Embed Size (px)
Citation preview

MASTER SLIDES
NORWAY

The Diagnosis and Management of Auditory Neuropathy/Dys-
synchrony• Recently re-named at the Lake Como Consensus Conference:
Auditory Neuropathy Spectrum Disorders
• Charles I. Berlin, PhD, Professor• Benjamin A. Russell, Esteemed Colleague• University of South Florida Tampa FL. USA• [email protected]• [email protected]

Also: Fifty-three Years of Mistakes I have Made, and how
to avoid them.
Charles I. Berlin, PhD
Formerly Director of the Kresge Hearing Research Laboratory
LSU Health Sciences Center, Dept Otolaryngology, Head and Neck Surgery
Post-Katrina: Research Professor of CSD and Otolaryngology Head and Neck Surgery
University of South Florida
Tampa, FL

Sampling audience agendas
• The prepared materials are subject to improvisational change in response to your special interests and needs.
• Let’s review those first.
• The handouts will retain their utility as we cross various streams.

Stream 1
• The basic rules of speech and hearing and their interactions.
• F.I.T.• S===H • Demonstrations • Speech is in the ear of the listener not the
mouth of the speaker. Examples.• Rules and principles as they apply to
audiological assessment, hearing aid fitting and educational management.

Additional principles and rules
• Articulation Index
• Context vs. Intelligibility
• Language vs. Speech
• Luria effects.
• Other principles based on Speech Acoustics.




If you have no loss of outer hair
cells…this is what clear
speech sounds like to you. The
dot system assumes normal effort speech at roughly 50 dB
Hearing Level at
6 feet distance. From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

If you have a sharply sloping
high frequency loss and
hear mostly
voice but do not
understand
speech… this is
what the same
passage sounds
like to you
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group
Shortcut to 250 Hz Low Pass.lnk

If your loss begins at 500 Hz
you will hear more of the
speech signal but still have difficulty
understanding without lip
reading
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

If your loss begins at 1000 Hz you will
hear much more of
speech but still be
handicapped especially
in noisy situations

A hearing loss above 4000 Hz is often (incorrectly)
considered inconsequential.
Some people may still have trouble in
noise and in multiple
conversations and locating sound
sources.

.
Many people mistakenly believe that only high frequency losses cause listening problems; listen to this severe LOW frequency loss and seeif you agree!?
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group
Copy of 4k HIGH PASS.wma

Now the low frequency loss allows you to hear
sounds down to
2000 Hz. Notice the
sudden improvemen
t!
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

Now even more of the important
frequencies become
audible but the speech still sounds
“tinny”.From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

Now things are slightly
more natural but still “low
fidelity”.
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

Now even more natural
but still lacking full fidelity
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

And finally back to full
fidelity and a “normal
audiogram”.
From C.Berlin, HairCells and Hearing Aids, 1996 SingularPubl. Group

Real Time Demonstration of Speech Acoustics and Analysis
Sub question: Are Consonants really “high frequency” and vowels
really “low frequency”?

But first an exercise…
•Draw a sine wave.•You have probably drawn a picture in Time-by-amplitude as follows:

Time-by-amplitude sine wave

Continuing with the exercise
•Draw the same sine wave in a frequency-by-amplitude plot.

Frequency-by-amplitude (insert) compared to Time-by-amplitude
(background)

Now a time-by-frequency plot or spectrogram.

These exercises will help us better apply and understand the appearance
and…• …the nature of frequency response curves in
speakers, earphones, and hearing aids.• …the nature of otoacoustic emissions displays.• …the differences between DPOAE and TEOAE
recordings.• …cochlear microphonics, summating potentials,
and other electrical events recordable from the ear.
• How to display and analyze speech of the deaf and hard-of-hearing.

Stream 2
Examining our assumptions

The overall goals of this presentation
• To review 53 years of mistakes I personally have made in audiological management and how I would prevent them today.
• To review faulty assumptions I have made and both taught and been taught.
• To share techniques to both prevent errors, increase accuracy and validity, speed data collection, and predict success of various management strategies from hearing aids , to Audiory Verbal Therapy, to more visual strategies, etc.

To remind us that we are here to serve patients and meet their
needs
• And to do that we have to listen to them, with respect and dignity, and care…deeply…very deeply…about what happens to them and their family-members.

The Value of “Knowing the Results Before You Get the Results” (Credit Edward de
Bono)
Read this word:
MOCK

Now Read It Again:
MOCKBA

Why is the Sky Dark at Night?
A question designed to awaken the process of re-
thinking a question to which you THINK you know the
answer

How about these? In your latitude…
• Where does the sun rise? Always?
• Where does it set? Always?
• Where does the moon rise?
• Where does it set?
• Is it always visible?

Similar questions:
• Why do we have middle ear muscle reflexes?
• How intense is your voice at your mouth when you say /a/?
• How intense it your voice at 6 feet?
• The vowels, the consonants?
• Are the vowels low frequency and the consonants high frequency?

STREAM 3 • KNOWING WHEN A HEARING AID WONT WORK... Without
asking your patient to “get used to it”. Research shows that you don’t need six weeks as an experienced adult to accommodate to a hearing aid. If it works well, the response is almost immediate. It is the patient’s attitude toward the aid from the beginning that should be considered. But in this stream we will discuss PHYSIOLOGIC predictors, not psychosocial ones.
• Reasons for referral and attitudes toward hearing aids: do they affect outcome?• Wilson C, Stephens D.• Clin Otolaryngol. 2003 Apr;28(2):81-4.
• Population study of the ability to benefit from amplification and the provision of a hearing aid in 55-74-year-old first-time hearing aid users.
• Davis A.• Int J Audiol. 2003 Jul;42 Suppl 2:2S39-52.
• Technology, expectations, and adjustment to hearing loss: predictors of hearing aid outcome.• Jerram JC, Purdy SC.• J Am Acad Audiol. 2001 Feb;12(2):64-79.

Think some more…
• Is a voluntary pure tone audiogram the gold standard for a hearing test?
• It must be, because we used to fit a hearing aid to it and design educational startegies around it.
• If not, why do we fit hearing aids and design educational strategies based on pure tone audiograms alone?
• What do I really need to know about a patient’s auditory system to habilitate him?

The secret lies in
•The Inner Hair Cell and•Its connections to and action with the primary nerve fibers.

What Does This Have to Do With Audiological Management and knowing
the validity of your Audiogram?
• About 10% of hearing impaired people have poor audiograms that look manageable but they have normal outer hair cells as evidenced by normal otoacoustic emissions
• Normal outer hair cells, which are nature’s low level preamplifiers, mitigate AGAINST hearing aid success…there is no need for amplifying faint sounds if the outer hair cells are already doing that job.
• The INNER HAIRCELLS AND NERVE FIBERS ARE COMPROMISED.

More…
• Putting hearing aids on someone with normal OAEs can destroy their emissions but still “improve their audiogram sensitivity”. It has never been shown to help them learn language auditorally.
• Tympanometry, reflexes and emissions should be done on all new patients to rule out AN/AD…if the reflexes are absent and the emissions are present, AN/AD is highly likely

Treat the Physiology, Not the Audiogram.
• Four cases of identical audiograms which require differing management strategies
• The proper differentiation is acquired through Triage with these tests. We recommend they be done BEFORE pure tone audiometry to speed data collection and reduce the need for re-checking and re-testing.
• They also reduce the intrusion of technical errors during pure tone audiometry.

The Tests for AUDIOLOGIC TRIAGE (classifying a PATIENT’S
CONDITION and predicting its outcome) . These are essential for planning an educational strategy.
• 1. Tympanometry
• 2. Middle Ear Muscle reflexes
• 3. Otoacoustic Emissions

Using multiple tests is not original with us…
• Probably the single most cited article on related principles was published by Jerger and Hayes. The cross-check principle in pediatric audiometry.Jerger JF, Hayes D.Arch Otolaryngol. 1976 Oct;102(10):614-20.
• Many other colleagues (Jay Hall, Frank Musiek, Michael Gorga, Mead Killion, Maureen Hannley,have made similar observations). E.g.
• Screening for and assessment of infant hearing impairment.
Hall JW 3rd J Perinatol. 2000 Dec;20(8 Pt 2):S113-21. Relationships among auditory brain stem responses, masking level differences and the acoustic reflex in multiple sclerosis .
Hannley M, Jerger JF, Rivera VM.Audiology. 1983;22(1):20-33.

View The Value of Triage (Sorting by Likely Outcomes)
From Book Chapter “The Physiological Basis of Audiologic Practice”
Berlin, CI, Ricci and Hood (Eds) Hair Cells Micomechanics and Otoacoustic Emissions Delmar-Thompson 2002.

Review of underlying principles behind the tests:
1. Middle Ear Muscle Reflexes2. Otoacoustic Emissions

Middle Ear Muscle Reflexes• Requires three pre-existing conditions to be seen:
– Normal middle ear mechanics– A “loud sound” …75-95 dB HL– An intact reflex arc and GOOD NEURAL
SYNCHRONY– Note that when one ear is stimulated
sufficiently, the reflex contraction of the stapedius muscle is obtained in BOTH ears
– MOVIE OF THE REFLEX IN ACTION.


Otoacoustic Emissions• Noises which come from the outer hair cells of the
cochlea• To see them you must have:
– 1. Normal Middle ears (measured by tympanometry)
– 2. Normal Cochlear Battery (Endocochlear Potential but reflected in CM)
– 3. Normal Outer Hair Cells (reflected in CM)– FILM of the moving hair cells.

Basic Review of Physiologic Principles Behind Middle Ear
Muscle Reflexes and Emissions
• The Four Electrical Events in the Cochlea– The endocochlear potential– The cochlear hair cell potential or cochlear
microphonic– The compound action potential or Wave I of
the ABR– The summating potential
• Oto-Acoustic Emissions Charles I. Berlin, Ph.D.
Staff of the Kresge Lab
at LSUMC Dept of ORL

AN/AD audiogram samples…all patients have NO ABR, no reflexes and normal emissions (lowest row right),.

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left
Rt Lt
Nr Nr
Nr Nr
SRT
Disc
Reflexes?:
Emissions?:
ABR?:

Brothers A and B
• Tymps Normal
• Reflexes absent
• Emissions not available at the time, absent when tested
• ABRs absent……
• Management…..


Siblings C and D
• Tympanometry normal
• Reflexes absent
• Emissions Present• ABR…
• Management…


What does a normal temporal bone in a premature baby look like:
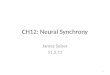
• Figure 1. Normal organ of Corti from the upper middle turn of a cochlea showing excellent preservation. From patient 15, a full-term baby who passed the auditory brainstem response screening on day 6 and died on day 8. Note stereocilia of the inner hair cell (short arrow) and outer hair cells (long arrows) (hematoxylin-eosin, original magnification ×250).

Normal Cochlea in a Premature

Temporal Bone of Premature, Courtesy of Mass. Eye and Ear Published in June 2001 Arch Otolaryngology

Temporal Bone of Premature, Courtesy of Mass. Eye and Ear Published in June 2001 Arch Otolaryngology
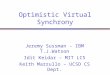
Normal nerve fiber count insidethe habenula perforata,

Temporal Bone of Premature, Courtesy of Mass. Eye and Ear Published in June 2001 Arch Otolaryngology
Note missing Inner Hair cell, Normal nerve fiber count insidethe habenula perforata,

Temporal Bone of Premature, Courtesy of Mass. Eye and Ear Published in June 2001 Arch Otolaryngology
Note missing Inner Hair cell, Normal nerve fiber count insidethe habenula perforata, and normal outer hair cells which would lead and normal outer hair cells which would lead to normal emissions and NO ABRto normal emissions and NO ABR

Alternatively, Starr et al. show this type of pathophysiology

Comparing a normal cochlea (right) to one with Auditory Neuropathy

ABR from two of Starr’s MPZ Gene subjects

From Starr et al. MPZ Gene paper

More from Starr paper

Patient E• History of normal hearing until she was beaten
unconscious by an abusive boyfriend• Claimed to be totally deaf to speech and pure tones• Tympanometry normal• Emissions normal• Initially diagnosed from emissions alone as
“hysterical” or “malingering”• Reflexes ABSENT

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left
Rt Lt
Nr Nr
Nr Nr
SRT
Disc
Reflexes?:
Emissions?:
ABR?:

Right Ear with 100,90 and 80 dB, opposite polarityClicks…all waves are CM
Cond100 dBRare
Cond90 dBRare
C & R 80 dB

Patient F• Normal hearing until after dental anesthesia, she
awoke totally deaf• She claimed to be unresponsive to speech and pure
tones and her voluntary audiograms and speech responses confirmed her symptoms
• Tympanometry normal• Emissions normal• Reflexes present• ABR and management...

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left
Rt Lt
Nr Nr
Nr Nr
SRT
Disc
Reflexes?:
Emissions?:
ABR?:


The Take-Home Message: Testing in This Order Will Save Time Minimize the Need for Re-Test and Help Direct the Diagnostic Tree• Tympanometry• Middle ear muscle reflexes• Otoacoustic emissions then if adult• Speech audiometry…then either• Pure tone based tests including Stenger and
MLD if appropriate…or• ABR related physiological tests

The Triage (Division of Possible Outcomes) Prevents Mis-diagnosis of Ordinary Sensorineural Loss When
the Patient Might Really Have Auditory Neuropathy/Dys-synchrony
or You Have Some Audiological Errors

More Clinical Examples
• Consider how you would manage these patients if you ONLY had air-bone and speech, the usual request from our surgical colleagues and the maximal allowable by hearing instrument specialists.
• Look at these patients from a management point of view again:

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left bone
Rt Lt
45 55
40% 60%
SRT
Disc
Reflexes?:Emissions?:

How the Triage Works:• If emissions were normal and
reflexes were absent, while tymps are normal you would have expected…Auditory Neuropathy, and requested an ABR. If positive for AN, Hearing aids would not be likely to help teach language by ear to a child, or improve communication in an adult.
• If emissions were absent, and reflexes were present you would have expected hearing aids to help and communication to improve; spending time and money on the best possible aids and devices, doing real ear measures, etc., would be worthwhile.

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left
Rt Lt
25 30
80% 10%
SRT
Disc
Reflexes?:
Emissions?:

How the Triage Works:• If emissions were normal
and reflexes were absent in BOTH ears, while tymps are normal you would have expected AN/AD…if absent in only one ear, you might have suspected a vestibular Schwannoma. Either way an ABR is called for, not just an MRI.
• If emissions were absent, and reflexes were present you would have expected an aidable condition.

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left bone
Rt Lt
25 30
80% 76%
SRT
Disc
Note normal bone!! This Is an example of how audiological triage can help minimizeother errors.
Tympanometry?:Reflexes?:Emissions?:

How the Triage Works:
• If emissions were normal and reflexes were PRESENT, while tymps were normal you would NOT have expected a conductive loss, and should have suspected a collapsed canal or wax- clogged insert phones.
• If emissions were absent, and reflexes were ABSENT or ELEVATED you would have expected the mild conductive loss you see. Also other options.

0
10
20
30
40
50
60
70
80
90
100
110
250 500 1000 2000 4000 8000
Right Left
Rt Lt
25 NR
80% NR
SRT
Disc
WITH MAXIMUM NB MASKING IN RIGHT
Emissions?:
Reflexes BOTH IPSI andContra??:

How the Triage Works:• If emissions were
normal on both sides and reflexes were absent only when stimulating the poor ear, while tymps are normal you would have expected AN/AD, done an ABR in both ears and looked also for neural problems.
• If emissions were absent on the poor ear only, and reflexes were present when stimulating the good ear, you would have expected a dead ear and …

Key Questions About Auditory Dys-synchrony
• What is it?• What does it sound like and how does it differ from
regular hearing loss or Scheibe types of deafness?• What Causes it?• How many people are there like this?• What will happen to my child/our patients who have
this diagnosis?• What can I do to manage this disorder?

Interim Recommended Codes:
• Neuropathy 355.9
• Abnormal Auditory Perception: 388.4
• If present add:
–Peripheral Neuropathy: 356.9

What is it? The Combined Observation of...
• Absent or Abnormal Auditory Brainstem Responses WITH SALIENT Cochlear Microphonics.
• Normal Otoacoustic Emissions…WHICH SOMETIMES DISAPPEAR SPONTANEOUSLY AND MAY NOT BE PRESENT AT TIME OF TEST
• ABSENT MIDDLE EAR MUSCLE REFLEXES• Audiograms ranging from normal to totally deaf

Normal Emissions and Absent ABRs are a Paradox Only if You Already Thought You Knew Why the Sky
Was Dark at Night and...• ..were taught or told that
ABRs and Emissions are infallibly objective hearing tests
• THEY ARE NOT

Neither ABR Nor Otoacoustic Emissions Are Hearing Tests
• Let’s review the Physiology to dissect the physiologic basis of audiologic practice and to see how a “paradox” of normal emissions and absent ABRs occurs.

Basic Review of Physiologic Principles
• The Four Electrical Events in the Cochlea– The endocochlear potential– The cochlear hair cell potential or cochlear
microphonic– The compound action potential or Wave I of
the ABR– The summating potential
• Oto-Acoustic EmissionsCharles I. Berlin, Ph.D.
Staff of the Kresge Lab
at LSUMC Dept of ORL

TheThe EndocochlearEndocochlear PotentialPotential
1
2
34
5
Gene expressions #s

CM (AC) and Summating Potential DC

Pam Beck
• 216-292-6213
• Two organizations:
• National Cued Speech Association ny
• Cued Language Network of America utah

VIDEO DEMONSTRATIONS….
PRAY
FOR COMPUTER AND PROJECTOR
COMPATIBILITY.

Important reminders
• Many AN patients have already lost their emissions but can be diagnosed properly by the combined use of middle ear muscle reflexes with Cochlear Microphonics, ABR and EcochG.
• Everyone who has residual hair cell function will have a cochlear microphonic that inverts with polarity.
• THE PRESENCE OF THE INVERSION ALONE DOES NOT MAKE THE DIAGNOSIS.

Normal Polarity Inversion of the Cochlear Microphonic in a Newborn
Berlin, LSU Kresge 95
but not opposite polarityneural responses.

A Normal ABR on the Left, a Potential Trap or Misdiagnosis of Central Brain
Disorder on the Right

Reverse the Click Polarity and What Looked Like an ABR is Revealed as
a Cochlear Microphonic

Reverse the Click Polarity at Least Once IN A
SECOND COMPLETE AVERAGE to Separate CM
from AP

Hence Our Request of Our Colleagues to Consider ...
• Tympanometry
• Reflexes
• Emissions on all new diagnostic patients
• This yields 6 possible results, one of which raises a high index of suspicion for AN/AuDys: ABSENT REFLEXES AND NORMAL EMISSIONS
• PLEASE DON’T SKIP THE REFLEXES!!

So You Can See That Otoacoustic Emissions Only
Test Hair Cells…Not Hearing...• …and we can test neural synchrony and inner hair cells
with ABR and related tests.
• When both tests are normal, you are likely to have normal hearing, provided there are no upstream problems.
• If the two tests conflict, where the emissions are normal and the Neural Response can’t be well recorded, you have Auditory Dys-synchrony.
• If the emissions are gone, and you have large cochlear microphonics and absent ABR you are alos likely to have AN/AD but the reflexes should also be absent or severely elevated.

How Does Normal Outer Hair Cell Function Act Like a Biological Hearing Aid?

Human Middle Ear moving 1.25 mmIn response to 120 dB 200 Hz. StroboscopicIllumination (courtesy Prof. Kirikae)

Hair Cell in Action from Jonathan Lear Ashmore

Displacement of the Chinchilla Basilar Membrane Relative to the Stapes Adapted from Ruggero in Berlin, 1996
1
10
100
1000
10000
5k 6k 7k 8k 9k 10k
3dB20dB60dB80dB

Idealized Gain Function of a Hearing Aid Which Would Do Somewhat the Same Thing in the Intensity Domain and Whose Compression Knee Begins at 40 dB Input Adapted from Berlin, 1996
0
10
20
30
40
50
60
250Hz 500Hz 1000Hz 2000Hz 3000Hz 4000Hz 6000 Hz
40dB60dB90dB

Demonstrations of Splitting the study of the organ of Corti
by emissions and ABRFrom University of Wisconsin Web
Page

Demonstration of Polarity Sensitive Inner Hair Cell
From The University of Wisconsin Web Page

See Gateway.nlm.nih.govfor access to the National Library
of Medicineand visit our web page at
csd.bcs.usf.edu/berlin-russell for access to some of the patient films. Your FLASH
MEMORY will have the
animations.

Normal and Pathological Temporal Bones and a simulation of what speech might sound like through
their audiograms.
From University of Wisconsin Web Page and
Berlin, C. (1996) “Hair Cells and Hearing Aids”

Causes are Many and Might Include...
• The inner hair cells can be absent or disabled
• Jaundice…mild …probably coupled with a gene for hypersensitivity. The jaundice leads to a deposit, called kernicterus, which can interfere with inner hair cell access to the nerve fibers
• Genetic predisposition..this runs in families
• Let’s see more

The Final Common Path Probably Involves
Failure of inner hair cells to communicate synchronously to primary single units of the auditory nerve

Studying Inner vs. Outer Hair Cell function will reveal the nature of
the hearing loss
• The pure tone audiogram alone may often be insufficient to reveal the function of inner vs. outer hair cells without reference to reflexes, emissions and ABR.

We have all seen these cases and often mis-diagnosed many of them
as having…
• CENTRAL AUDITORY PROCESSING DISORDERS
• VERBAL AGNOSIA
• WORD DEAFNESS.
• We must check all of these patients for missing reflexes and absent ABRs but present emissions or at least large cochlear microphonics.

•What will happen to my child or patient when they get this diagnosis?

A Continuum of Auditory Dys-Synchrony
No overt delays or auditory complaints until adulthood or until first ABR
Bizarrely inconsistent auditory responses, best in quiet, poorest
in noise. Audiograms can be misleading or fluctuate. ABR
always desynchronized, reflexes absent. Visual phonetic
language usually works best until implantation, unless family
prefers cultural Deafness
Total Lack of Sound
Awareness
1 5 10

How do cochlear implants help?
• Watch post-op movie.

We all have these patients…
• Find them before it’s too late to be sure by using….
• A.• B.• C.• D.• Before behavioral audiometry which can
often be misleading or delay accurate diagnosis or proper management.

Modify Your ABR Protocol • Use one positive and one negative polarity
click to isolate and identify the CM• The presence of a CM inversion alone does
not make the diagnosis. You need to show absence of Latency-Intensity Function, and ABSENT MIDDLE EAR MUSCLE REFLEXES as well as normal emissions

Using one positive and one negative polarity click to uncover AN/AuDys . Note Normal auditory function with CM reversal and Normal Latency -Intensity Function on the Left... Auditory Dys-synchrony with only CM reversal and no latency-intensity function on the Right.
ONLY CMNormal

Twin JO’s ABR at LSU in 1993 Shows All
Waves Are Cochlear Microphonics
Note polarity inversionand no latency shiftshowingthis to bea CM

Twin JO Compared to His Brother JA Twin JO Compared to His Brother JA
0
10
20
30
40
50
60
70
80
90
100
250 500 1000 1500 2000 4000 8000
JO right
JO left
JA right
JA left
JO’s SRT was 10 dB
JA’s SRTwas 55-60 dB

Patient Whose Cochlear Microphonic Masqueraded as an ABR and Gradually Disappeared

Type PL...Loss of CM Over Time
9595
8585
8585
9595
8585
8/948/94
4/934/93
3/933/93

Type M Patient Who Maintains Emissions But Behaves Deaf

Patient FB: ABR absent at birth, Emissions not available. Diagnosed as Deaf
and reportedly raised at a school for the Deaf without speech and with ASL
only. No ABR at age 12, but a normal emissions, immittance, pure tone
audiogram and awareness of many sounds. Limited speech, language and
reading skills.
0102030405060708090
100
Frequency
dB H
eari
ng L
evel
FB Age 5RightFB Age 5LeftFB Age 8RightFB Age 8LeftFB Age 12RightFB Age 12Left
FB Age 5Right
75 85 95 95 95
FB Age 5Left
80 90 90 95 95
FB Age 8Right
65 65 70 65 70 75 65 60 55
FB Age 8Left
60 60 65 70 65 60 55 50 65
FB Age 12Right
15 10 5 5 10 15 10 15 15
125 250 500100
0200
0300
0400
0600
0800
0
Latest Data courtesy of parents and Jack Katz Ph.D. With the University of Buffalo Audiology Service
Type PR

Patient DVPatient DV: No ABR, Normal Otoacoustic Emissions, No Middle Ear Muscle Reflexes. : No ABR, Normal Otoacoustic Emissions, No Middle Ear Muscle Reflexes.
Audiogram shifts but emissions remain normal and ABR remains absent. Patient Audiogram shifts but emissions remain normal and ABR remains absent. Patient
Developed Charcot-Marie Tooth Disease; sister has normal audiogram, abnormal ABR, Developed Charcot-Marie Tooth Disease; sister has normal audiogram, abnormal ABR,
no efferent suppression, but no symptoms as yet.no efferent suppression, but no symptoms as yet.
0
10
20
30
40
50
60
70
80
90
100
Frequency
dB
Hea
rin
g L
ev
el
LEFTAGE 13
RIGHTAGE 13
LEFTAGE 21
RIGHTAGE 21
LEFT AGE13
10 20 20 25 35 65
RIGHTAGE 13
10 10 10 10 40 65
LEFT AGE21
55 50 20 80 30 75
RIGHTAGE 21
20 40 50 40 95 85
250 500 1000 2000 4000 8000
Type WPNType WPN

How Many People Are There Like This?
Roughly 1 in 1000 are born Deaf.
At least 10-12% of the Deaf have Auditory Dys-Synchrony from our survey of close to 1,000 students in schools for the Deaf. Probably there are many more because the results undergo change over time.

After Cochlear Implantation (45 of 50 Verified as Successful So Far in Our Data Base as of March
2009)...• Auditory verbal and oral therapies are ideal• Total and sudden removal of any and all prior manual
assistance is generally counterproductive• Children who depend upon vision for language can
benefit from interleaving of auditory with visual support
• This is what makes Cued Speech so valuable…it supports spoken language phonology which allows CI users to know what it was they missed

SELF-DESCRIBED “PROFOUNDLY DEAF” FRENCH-BORN USER OF CUED SPEECH, AS YET UNCONFIRMED AN/AD. NOTE GOOD PROSODY AND VOICE CONTROLFRENCH ACCENT, ETC. COURTESY JUDY CURTIN.

How to Guide Families Through Such an Unpredictable Course?
• What is your Goal?• Mine is to help parents raise a literate
taxpayer and position them so that whatever choices they make for their child, they cannot have made a serious error
• Parents are in charge and must become expert in their child’s management

No Matter What Choices You Make…Remember That...
• Children learn language by eavesdropping and imitating Language here means receptive vocabulary and comprehension much more than speaking
• So you must offer systems and tools that the parents and other family members can use easily and will facilitate language learning

What Has NOT Worked and What Mistakes Have I Made Since I Saw
My First AN Patient in 1982• Hearing aids and Auditory Verbal Therapy have been
disproportionately unsuccessful with these children ESPECIALLY IF ONE ADHERES TO THE AVT PRINCIPLES YEAR AFTER YEAR (blocking the face) BECAUSE THE AUDIOGRAM IS SO GOOD AND THE TRAINING “SHOULD WORK”.
• FM systems have been at best marginal • Trying to teach these most (BUT NOT ALL) of these
patients to talk without some form of visual language has been singularly unsuccessful despite their “normal hearing” by otoacoustic emissions

What Has Been Effective For the Families With Whom I Have
Worked• Sign language, with or without the adoption of
Deaf Culture values, is very useful but rarely produces good spoken language.
• Sign language with speech, while difficult, will help because of the hearing the child has and will facilitate two-way communication
• Cued Speech has great benefits, for teaching sounds OF ANY LANGUAGE and phonology and will not conflict with signs.
• Auditory Verbal Therapy is ideal AFTER implantation, but may cause serious problems before.

For Children Who Get Implants and Need to “Catch Up” On
English Phonology and Reading...
• The Fast ForWord™ series of programs, designed around Neuroscience Training Principles, has been remarkably effective (here and with CAPD as well)

Final Take Home Message to My Audiology , Otolaryngology AND
EDUCATIONAL Colleagues
• Check Tympanometry, Emissions and reflexes on all new or difficult diagnostic patients. Normal emissions and ABSENT reflexes should be a red flag calling for ABR regardless of the behavior.
• Emissions and reflexes which are not coherent with audiological data require re-examination.
• During the ABR use one positive and one negative polarity click to isolate and identify the CM.
• Parents will report “surprising hearing moments”…honor and respect their reports and learn from them.
• Parents “IN DENIAL” of their child’s hearing loss may really have children with AN/AD

Acknowledgments
• Colleagues who participated in these studies include:
• Linda Hood, PhD., Bronya Keats, PhD, Li Li, MD, Diane Wilensky, M.S., Shanda Brashears, MCD, Patti St. John, MCD, Liz Montgomery, MA, Harriet Berlin , MS, Thierry Morlet, PhD, Jennifer Jeanfreau-Taylor, MCD, Kelly Rose, MA.,, JM Huang MD. Stefan Frisch, PhD, Jon Shallop, PhD, Ben Russell, Michelle Arnold.
• Support from NIH, BMDR 1549, and Private Foundations, including Marriott, Oberkotter, Lions, LSUHSC, and others.