Embed Size (px)
Citation preview
Massive traumatic bleeding:
The multi-factorial complex nature of
Institute of Thrombosis Hemostasis and The National Hemophilia Center, Sheba medical Center, Tel Hashomer,
Uri Martinowitz MDUri Martinowitz MD
Member, Hemorrhage Control Steering Committee , The U.S. Army Medical Research and Materiel Command USAMARC, The Combat Casualty Care
Research Program CCRP
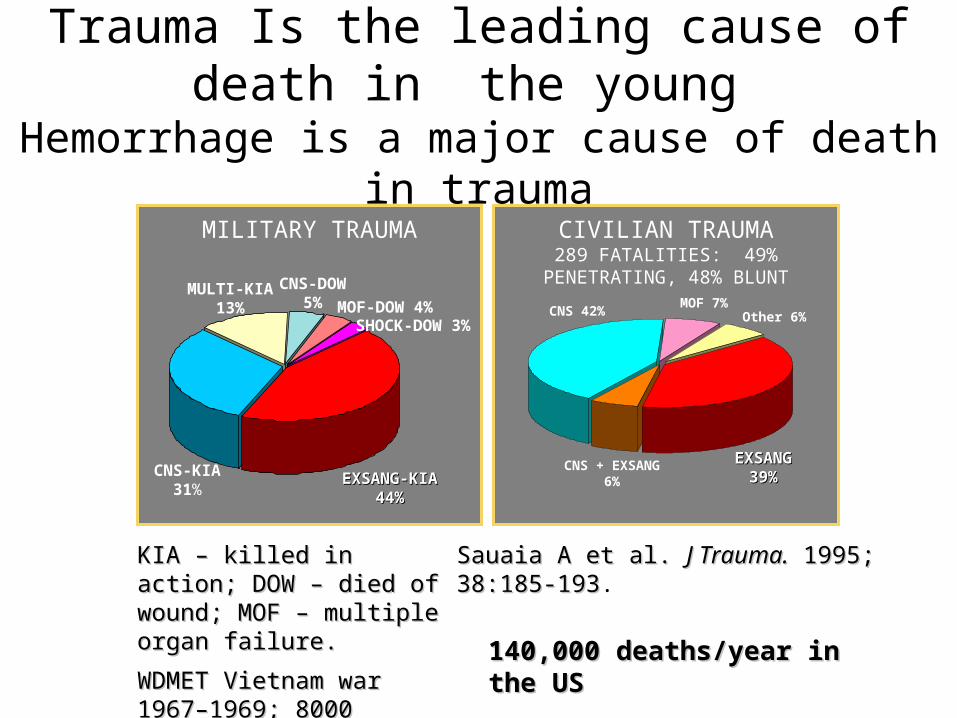
MILITARY TRAUMA
CNS-KIA31%
MULTI-KIA13% MOF-DOW 4%
CNS-DOW5%
SHOCK-DOW 3%
EXSANG-KIAEXSANG-KIA44%44%
KIA – killed in action; DOW KIA – killed in action; DOW – died of wound; MOF – – died of wound; MOF – multiple organ failure.multiple organ failure.
WDMET Vietnam war WDMET Vietnam war 1967–1969; 8000 1967–1969; 8000 CASUALTIESCASUALTIES. .
CNS 42%
EXSANGEXSANG39%39%
CNS + EXSANG6%
MOF 7%Other 6%
Sauaia A et al. Sauaia A et al. J Trauma.J Trauma. 1995; 1995;38:185-19338:185-193.
Trauma Is the leading cause of death in the young
Hemorrhage is a major cause of death in trauma
CIVILIAN TRAUMA289 FATALITIES: 49% PENETRATING, 48%
BLUNT
140,000 deaths/year in the US140,000 deaths/year in the US
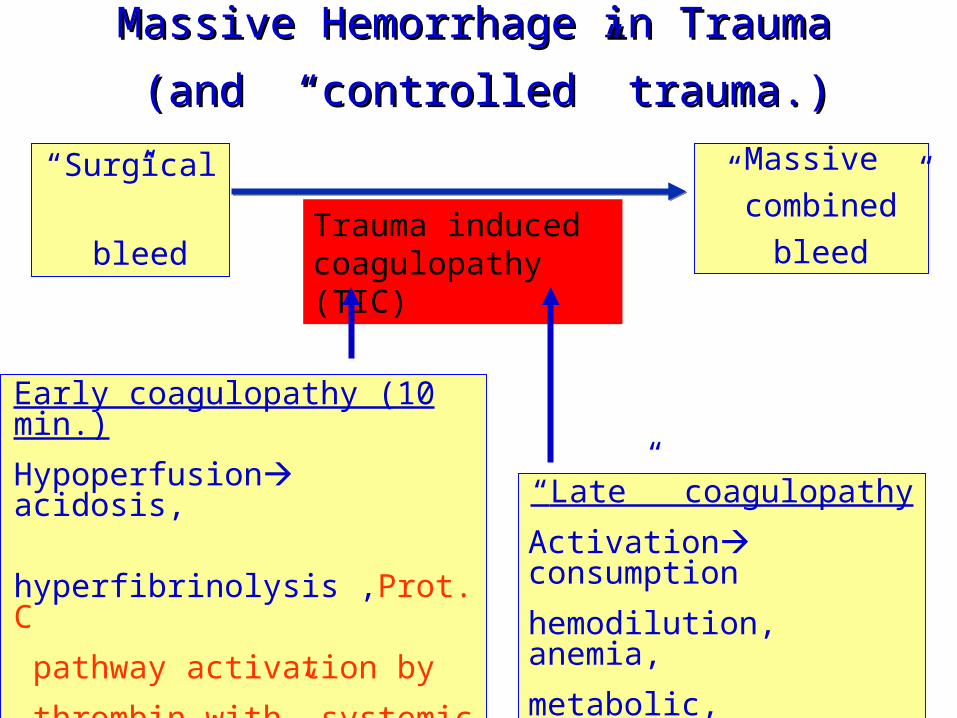
Massive Hemorrhage in Trauma Massive Hemorrhage in Trauma
(and “controlled” trauma.)(and “controlled” trauma.)
“Surgical”
bleed
Massive
” combined”
bleed
“Late” coagulopathy
Activation consumption
hemodilution, anemia,
metabolic, hypothermia
Early coagulopathy (10 min.)
Hypoperfusion acidosis,
hyperfibrinolysis ,Prot. C
pathway activation by
thrombin with” systemic
anticoagulation” ??? Brohi K. J. Trauma 2008: 64 :1211
Trauma induced coagulopathy (TIC)
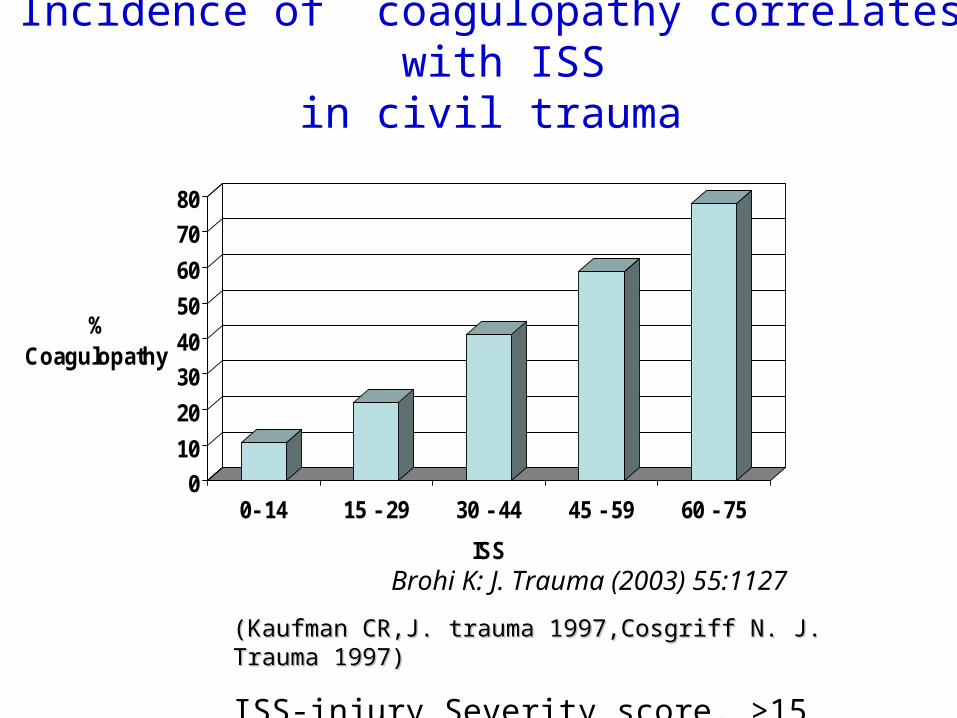
0
10
20
30
40
50
60
70
80
% Coagulopathy
0- 14 15 - 29 30 - 44 45 - 59 60 - 75
ISS
Brohi K: J. Trauma (2003) 55:1127
Incidence of coagulopathy correlates with ISSin civil trauma
(Kaufman CR,J. trauma 1997,Cosgriff N. J. Trauma 1997) (Kaufman CR,J. trauma 1997,Cosgriff N. J. Trauma 1997)
ISS-injury Severity score. >15 =severe injury
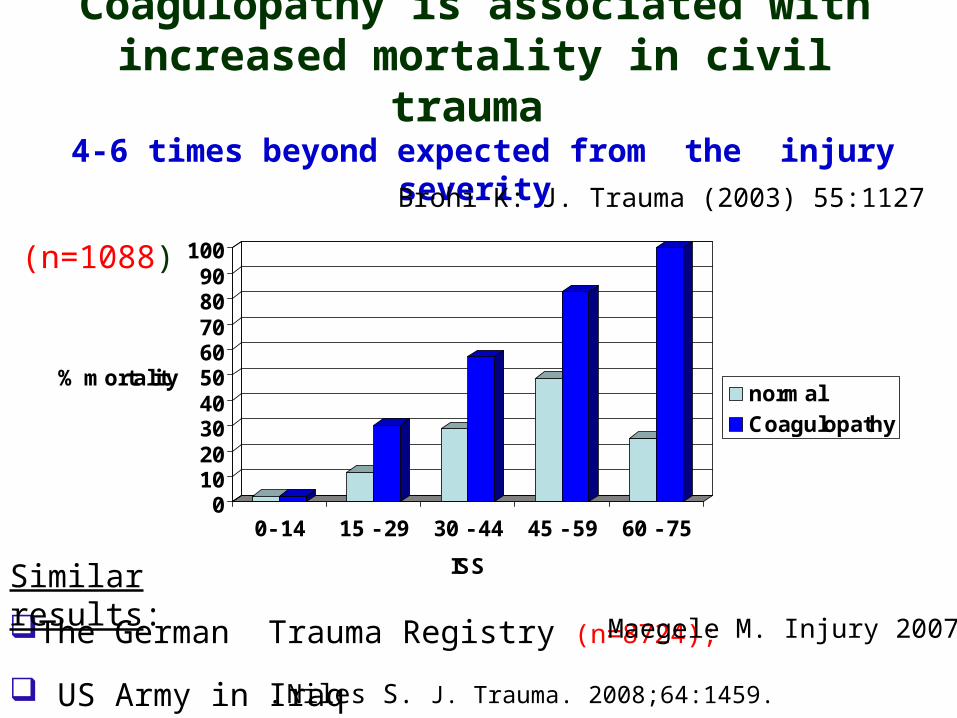
0102030405060708090
100
% mortality
0- 14 15 - 29 30 - 44 45 - 59 60 - 75
ISS
normalCoagulopathy
Coagulopathy is associated with increased mortality in civil trauma
4-6 times beyond expected from the injury severity
Brohi K: J. Trauma (2003) 55:1127
The German Trauma Registry (n=8724);
(n=1088)
Maegele M. Injury 2007 38:298
. Niles S. J. Trauma. 2008;64:1459. US Army in Iraq
Similar results:
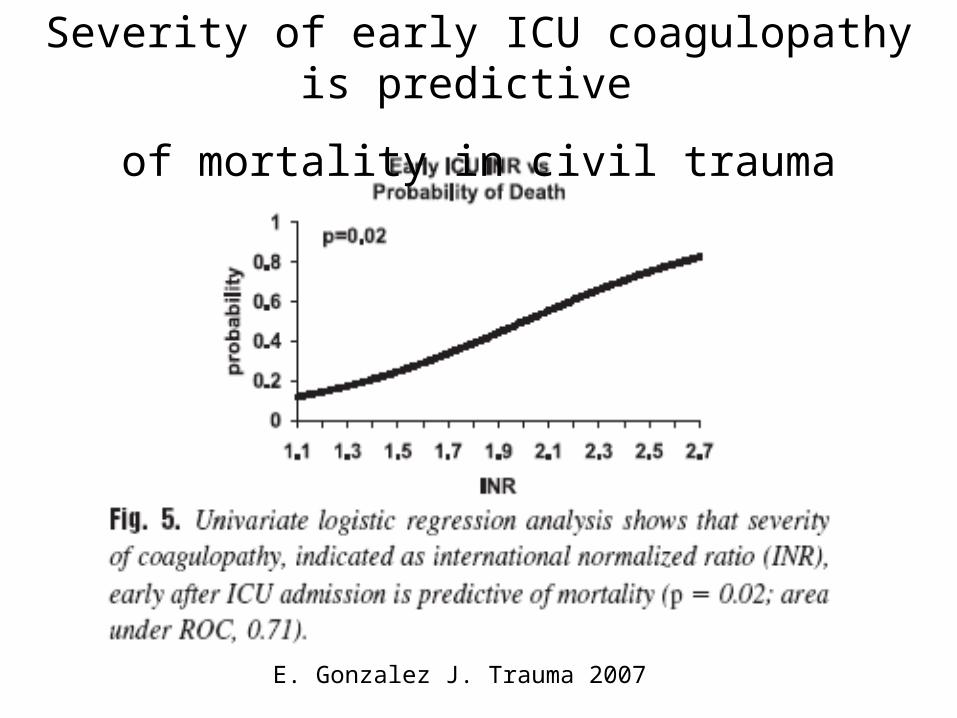
E. Gonzalez J. Trauma 2007
Severity of early ICU coagulopathy is predictive
of mortality in civil trauma
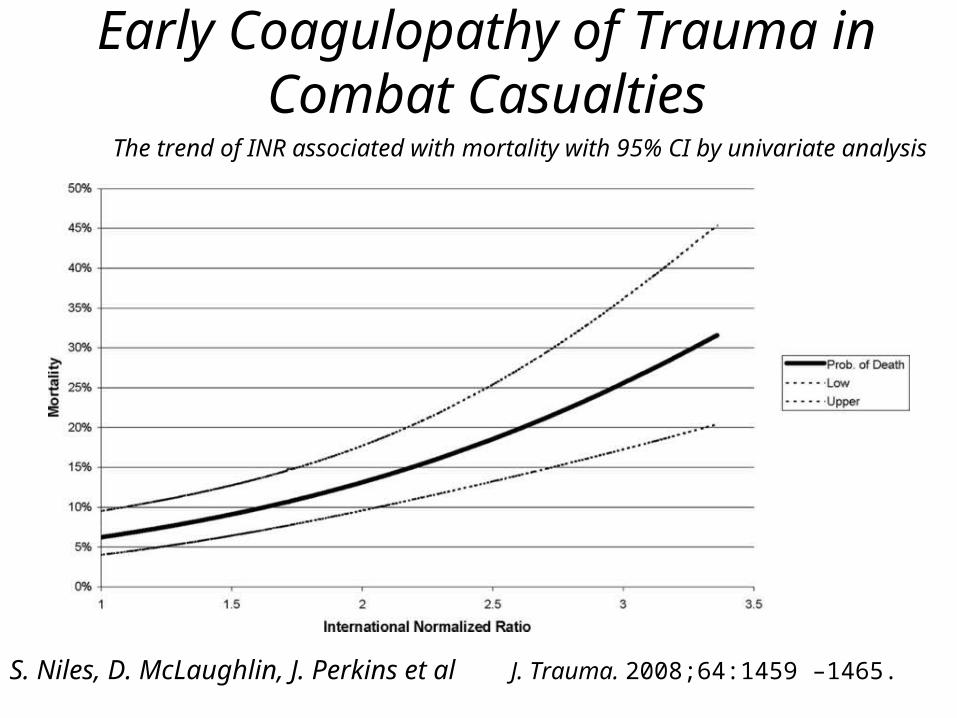
Early Coagulopathy of Trauma in Combat Casualties
The trend of INR associated with mortality with 95% CI by univariate analysis
S. Niles, D. McLaughlin, J. Perkins et al J. Trauma. 2008;64:1459 –1465.
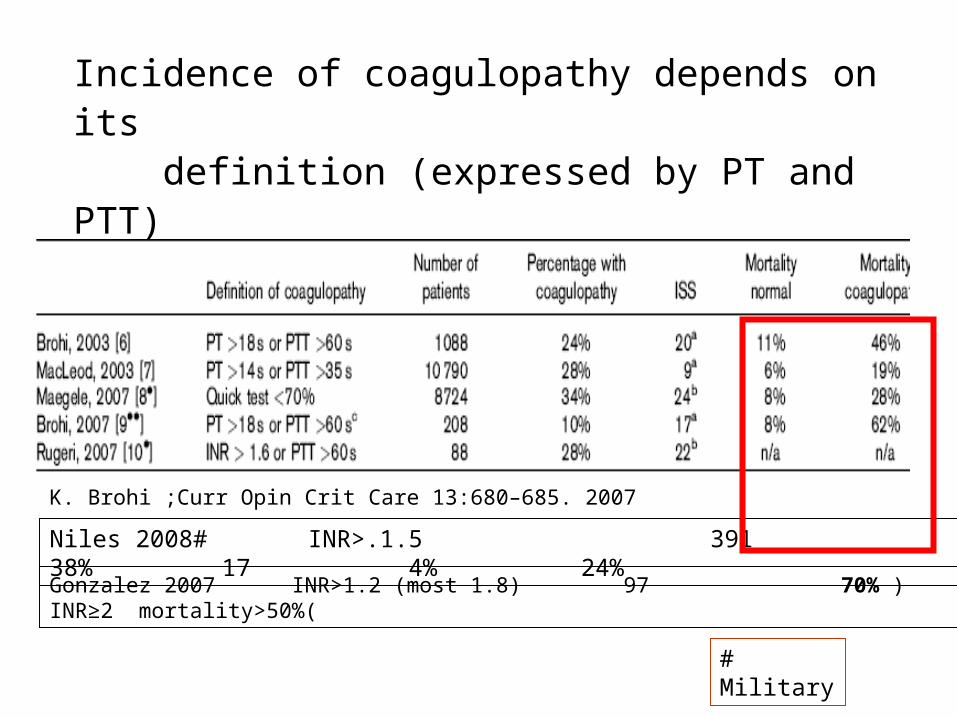
K. Brohi ;Curr Opin Crit Care 13:680–685. 2007
Gonzalez 2007 INR>1.2 (most 1.8) 97 70% ) INR≥2 mortality>50%(
Incidence of coagulopathy depends on its definition (expressed by PT and PTT)
Niles 2008# INR>.1.5 391 38% 17 4% 24%
# Military
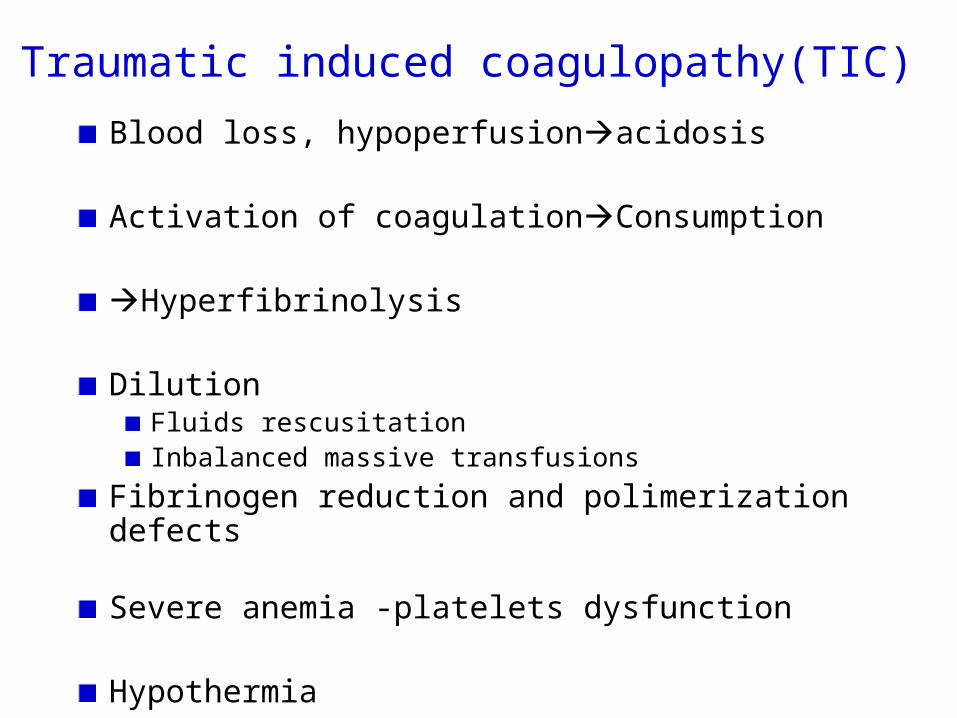
Traumatic induced coagulopathy(TIC)
Blood loss, hypoperfusionacidosis
Activation of coagulationConsumption
Hyperfibrinolysis
DilutionFluids rescusitationInbalanced massive transfusions
Fibrinogen reduction and polimerization defects
Severe anemia -platelets dysfunction
Hypothermia
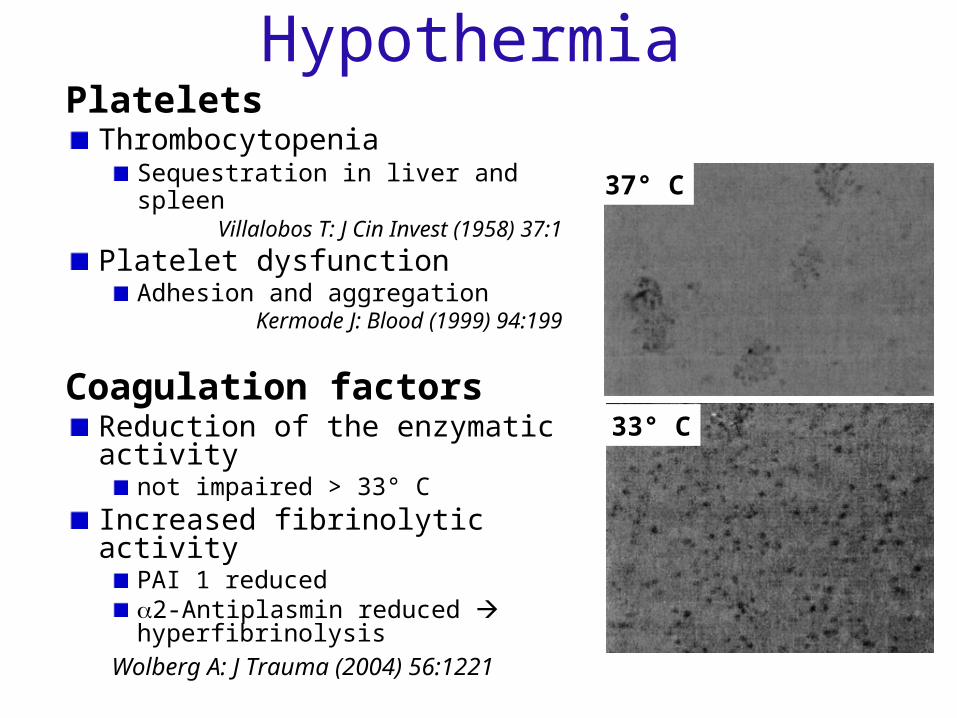
HypothermiaPlatelets
ThrombocytopeniaSequestration in liver and spleen
Villalobos T: J Cin Invest (1958) 37:1
Platelet dysfunctionAdhesion and aggregation
Kermode J: Blood (1999) 94:199
Coagulation factorsReduction of the enzymatic activity
not impaired > 33° C
Increased fibrinolytic activityPAI 1 reduced2-Antiplasmin reduced hyperfibrinolysis
Wolberg A: J Trauma (2004) 56:1221
37° C
33° C
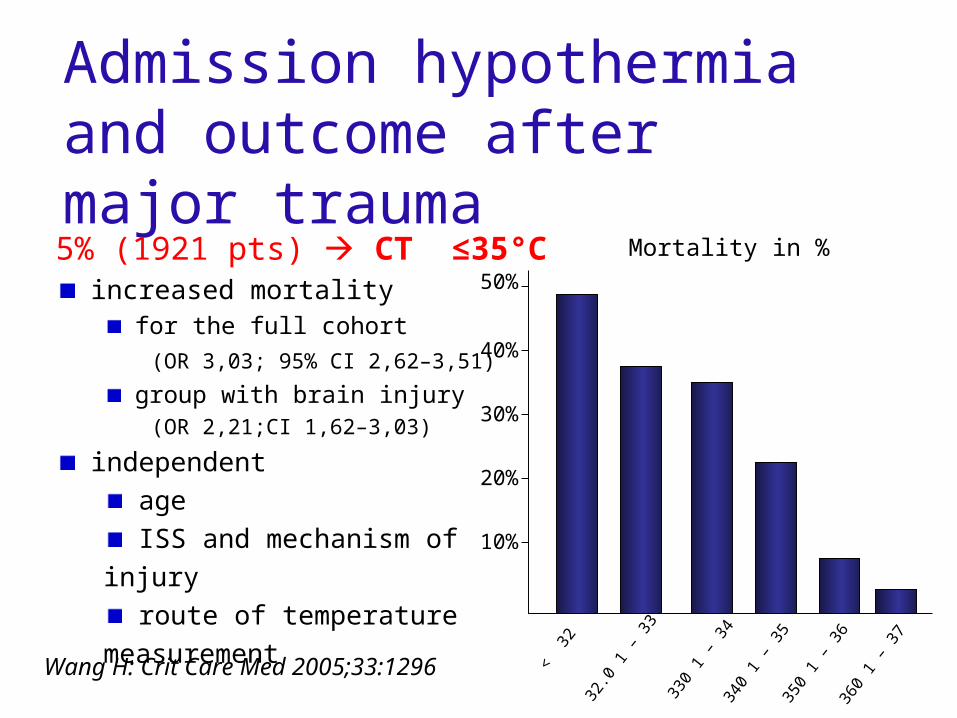
Admission hypothermia and outcome after major trauma
5% (1921 pts) CT ≤35°C increased mortality
for the full cohort
(OR 3,03; 95% CI 2,62–3,51)
group with brain injury (OR 2,21;CI 1,62–3,03)
independent
age
ISS and mechanism of injury
route of temperature measurement
Wang H: Crit Care Med 2005;33:1296 < 3
2
32.0
1 –
33
330
1 –
3434
0 1
– 35
350
1 –
3636
0 1
– 37
50%
40%
30%
20%
10%
Mortality in %
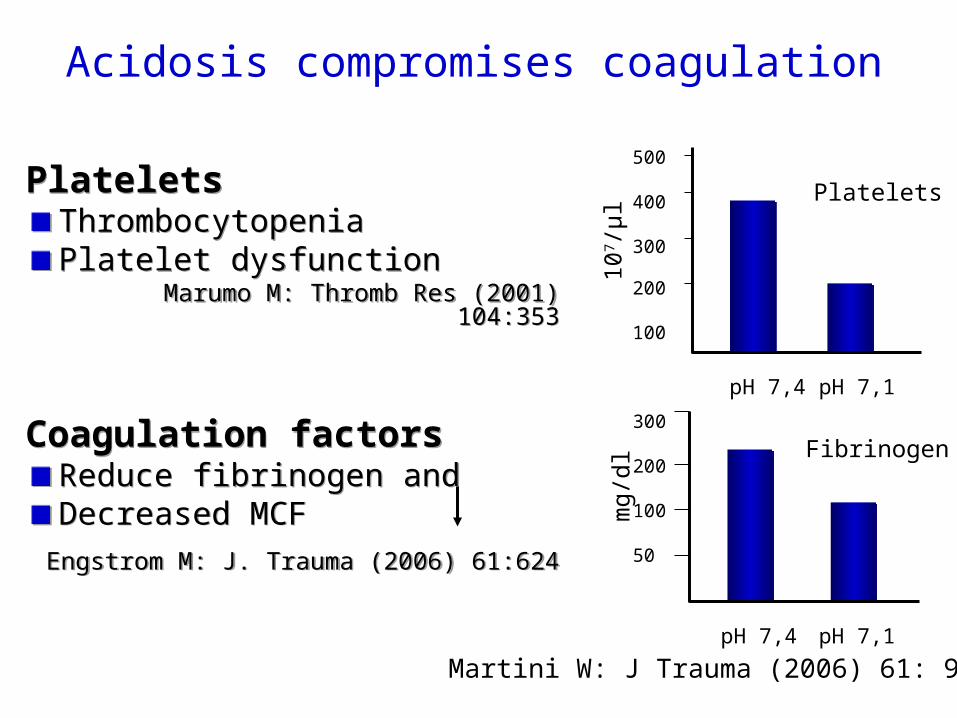
Acidosis compromises coagulation
PlateletsThrombocytopeniaPlatelet dysfunction
Marumo M: Thromb Res (2001) 104:353
Coagulation factorsReduce fibrinogen andDecreased MCF
Engstrom M: J. Trauma (2006) 61:624
PlateletsThrombocytopeniaPlatelet dysfunction
Marumo M: Thromb Res (2001) 104:353
Coagulation factorsReduce fibrinogen andDecreased MCF
Engstrom M: J. Trauma (2006) 61:624
Fibrinogen
Platelets
mg/
dl10
7 /µ
l
300
200
100
50
500
400
300
200
100
pH 7,4 pH 7,1
pH 7,4 pH 7,1
Martini W: J Trauma (2006) 61: 99
0
0.5
1
1.5
2
2.5
3
6.2 6.6 7 7.4 7.8 8.2 8.6 9 pHRela
tive
Rate
of I
Ia G
ener
atio
n
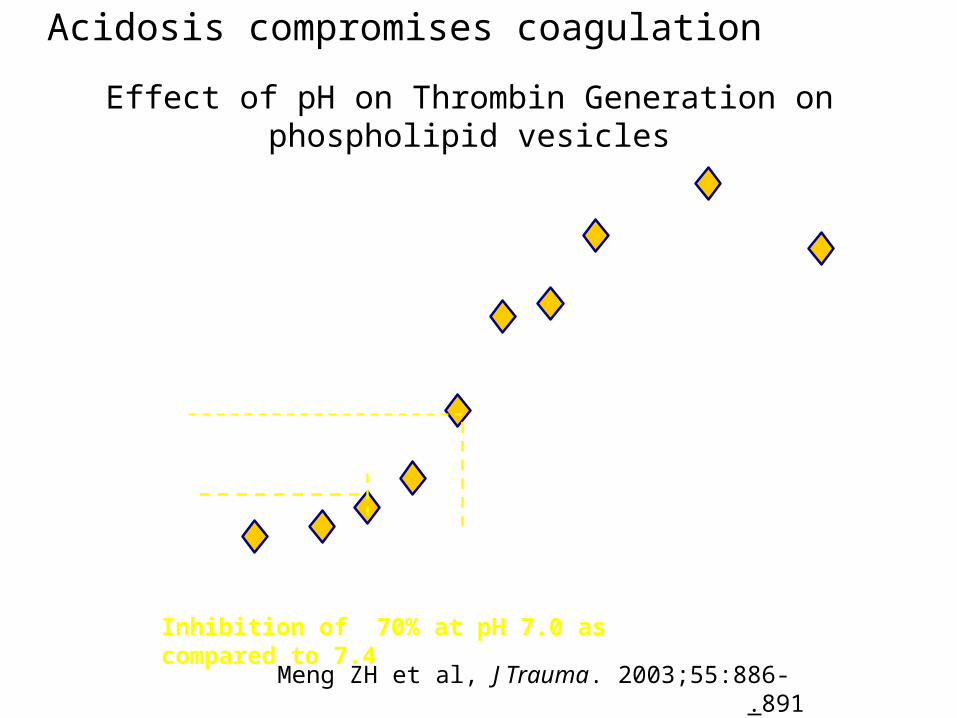
Inhibition of 70% at pH 7.0 as compared to 7.4
Effect of pH on Thrombin Generation on phospholipid vesicles
Meng ZH et al, J Trauma. 2003;55:886-891.
Acidosis compromises coagulation
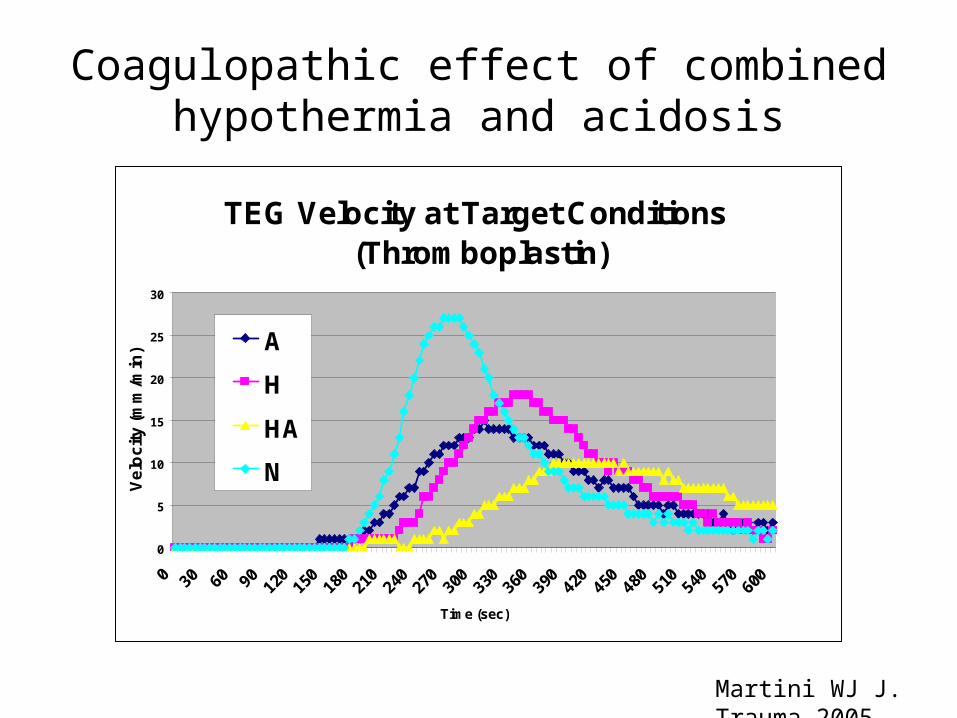
TEG Velocity at Target Conditions (Thromboplastin)
0
5
10
15
20
25
30
0 30 60 90 120
150
180
210
240
270
300
330
360
390
420
450
480
510
540
570
600
Time (sec)
Ve
loc
ity
(m
m/m
in) A
H
HA
N
Martini WJ J. Trauma 2005
Coagulopathic effect of combined hypothermia and acidosis
• Anemic patients tend to bleed more in surgery
• Ht 35 vs. 31 at end of CPB =blood loss X4-5
• Patients with bleeding diathesis (uremia, Glanzmans’ , irradiation colitis, angiodisplasia etc.) bleed less with correction of Hb (EPO).
• RBC transfusion is an important hemostatic treatment .In massive bleedings the goal is to achieve Ht 30-35,Hb 10-11.
Anemia compromises coagulation
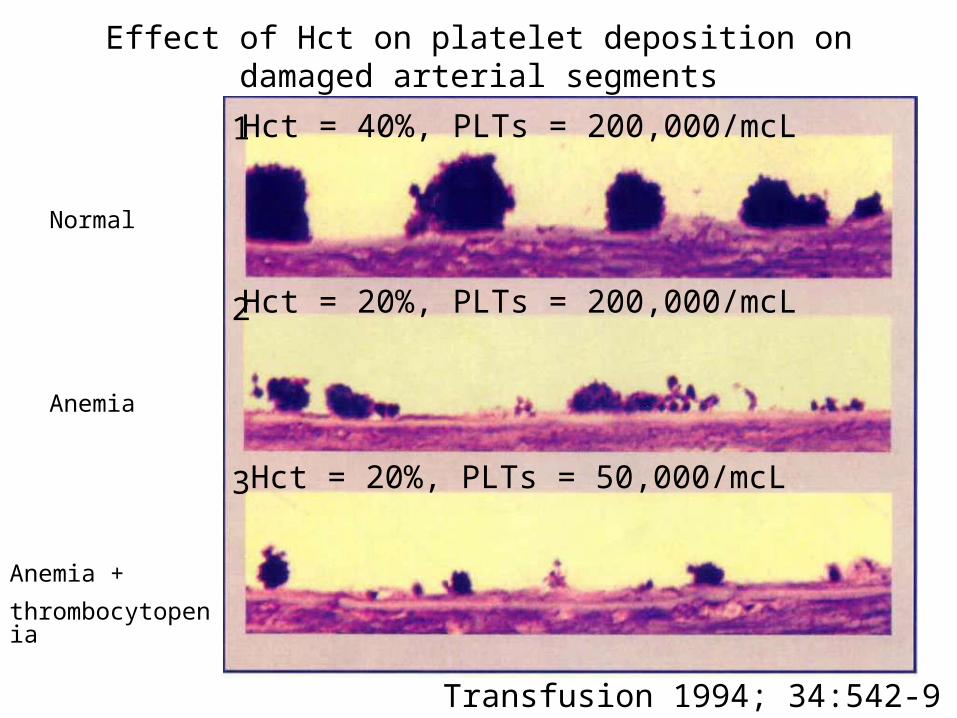
Effect of Hct on platelet deposition on damaged arterial segments
Hct = 40%, PLTs = 200,000/mcL
Hct = 20%, PLTs = 200,000/mcL
Hct = 20%, PLTs = 50,000/mcL
Transfusion 1994; 34:542-9
1
2
3
Anemia
Anemia +
thrombocytopenia
Normal
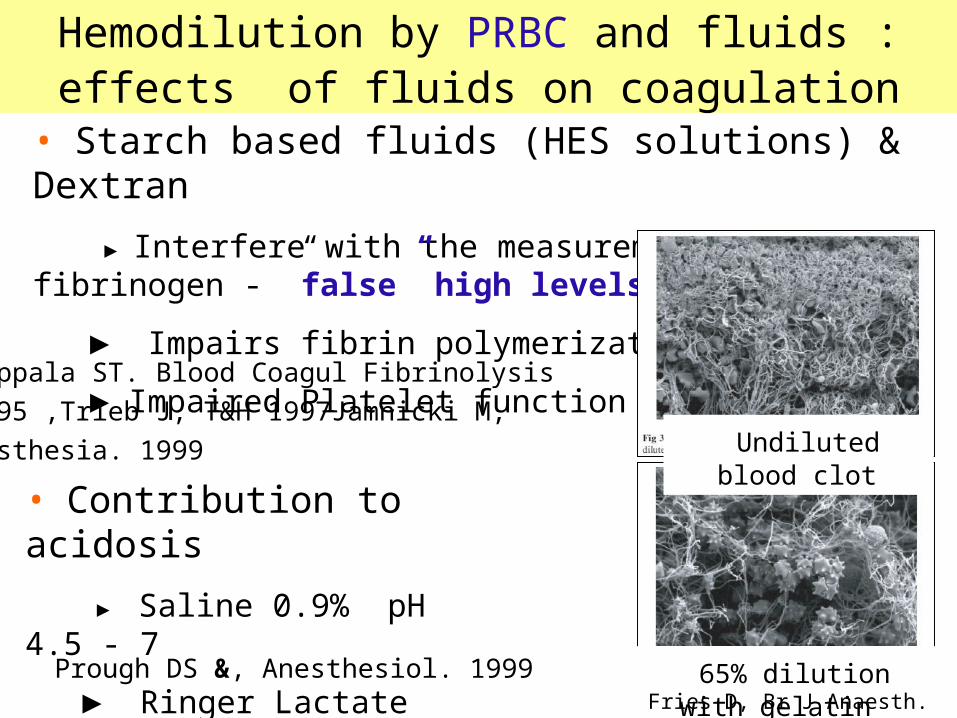
• Starch based fluids (HES solutions) & Dextran
► Interfere with the measurement of fibrinogen - ”false” high levels
► Impairs fibrin polymerization
► Impaired Platelet function
• Contribution to acidosis
► Saline 0.9% pH 4.5 - 7
► Ringer Lactate pH 6 - 7.5
Hemodilution by PRBC and fluids :effects of fluids on coagulation
Prough DS &, Anesthesiol. 1999
Hiippala ST. Blood Coagul Fibrinolysis
1995 ,Trieb J, T&H 1997Jamnicki M,
Anesthesia. 1999 Undiluted blood clot
65% dilution with gelatinFries D, Br J Anaesth. 2005
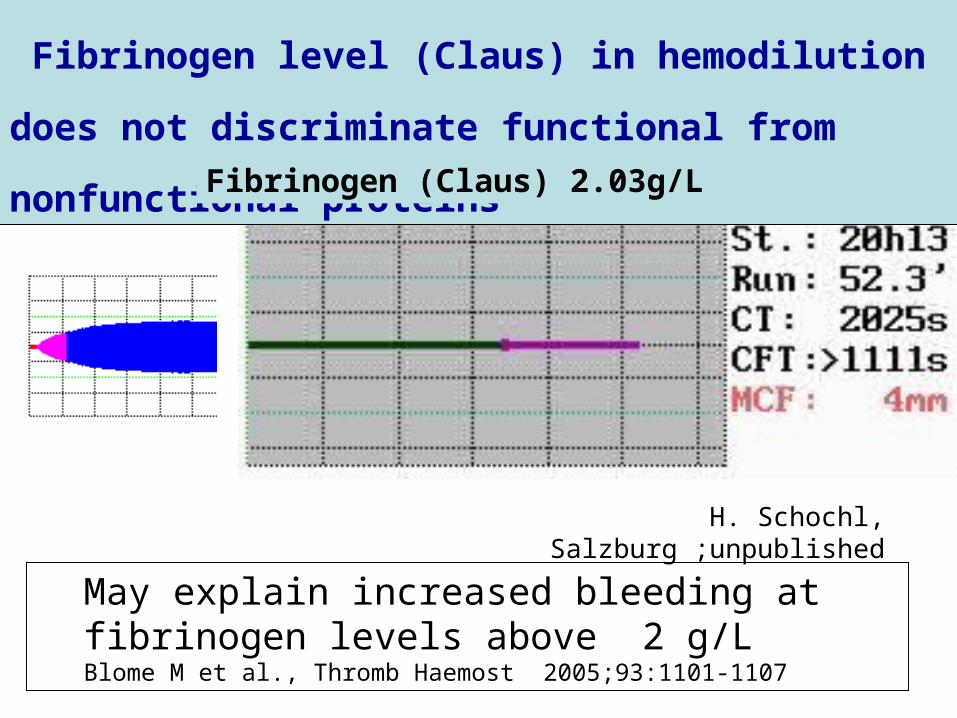
May explain increased bleeding at fibrinogen levels above 2 g/LBlome M et al., Thromb Haemost 2005;93:1101-1107
Fibrinogen level (Claus) in hemodilution does not
discriminate functional from nonfunctional proteinsFibrinogen (Claus) 2.03g/L
H. Schochl, Salzburg ;unpublished
Time [sec]
0 200 400 600 800 1000 1200 1400
Ve
loc
ity [
mm
*10
0 / s
ec
]
0
2
4
6
8
10
12
14
16
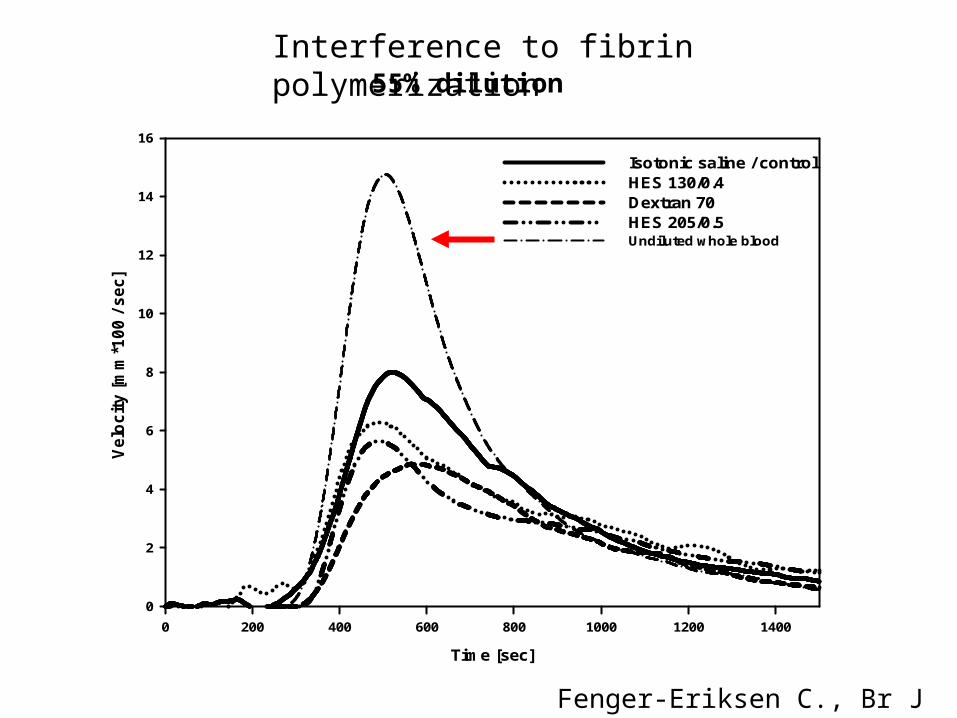
Isotonic saline / controlHES 130/0.4Dextran 70HES 205/0.5Undiluted whole blood
Fenger-Eriksen C., Br J Anaesth. 2005
Interference to fibrin polymerization 55% dilution
0 2 4 6 8 10 12 14 16 18
limp fr
abd
pelvis
brain injury
thoracic trauma
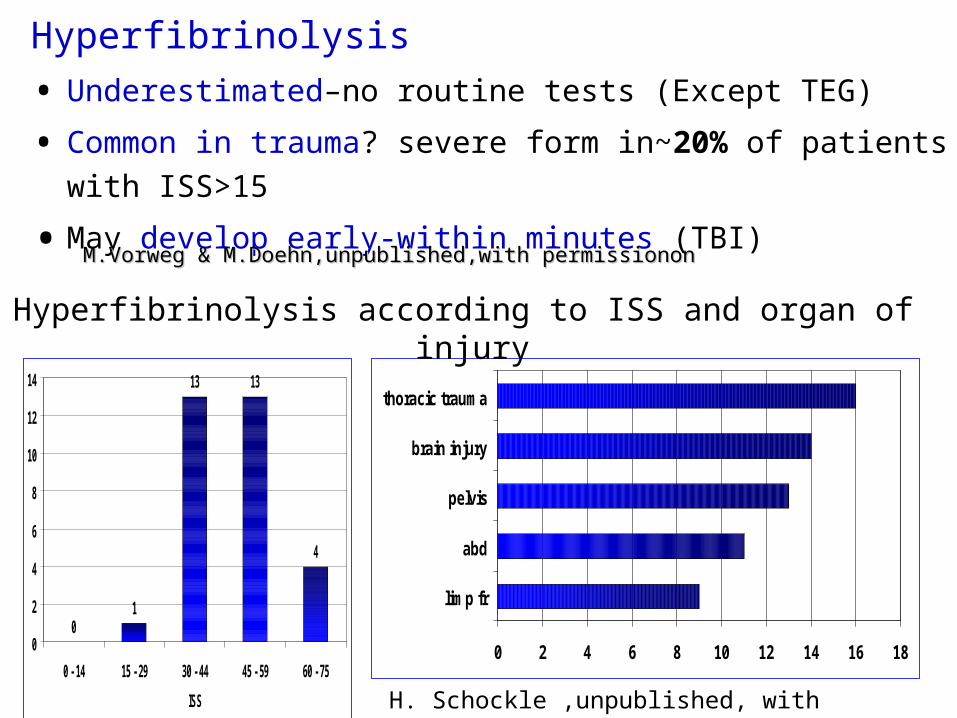
H. Schockle ,unpublished, with permission
Hyperfibrinolysis
• Underestimated–no routine tests (Except TEG)
• Common in trauma? severe form in~20% of patients with
ISS>15
• May develop early-within minutes (TBI) M.Vorweg & M.Doehn,unpublished,with permissiononM.Vorweg & M.Doehn,unpublished,with permissionon
01
13 13
4
0
2
4
6
8
10
12
14
0 - 14 15 - 29 30 - 44 45 - 59 60 - 75
ISS
Hyperfibrinolysis according to ISS and organ of injury
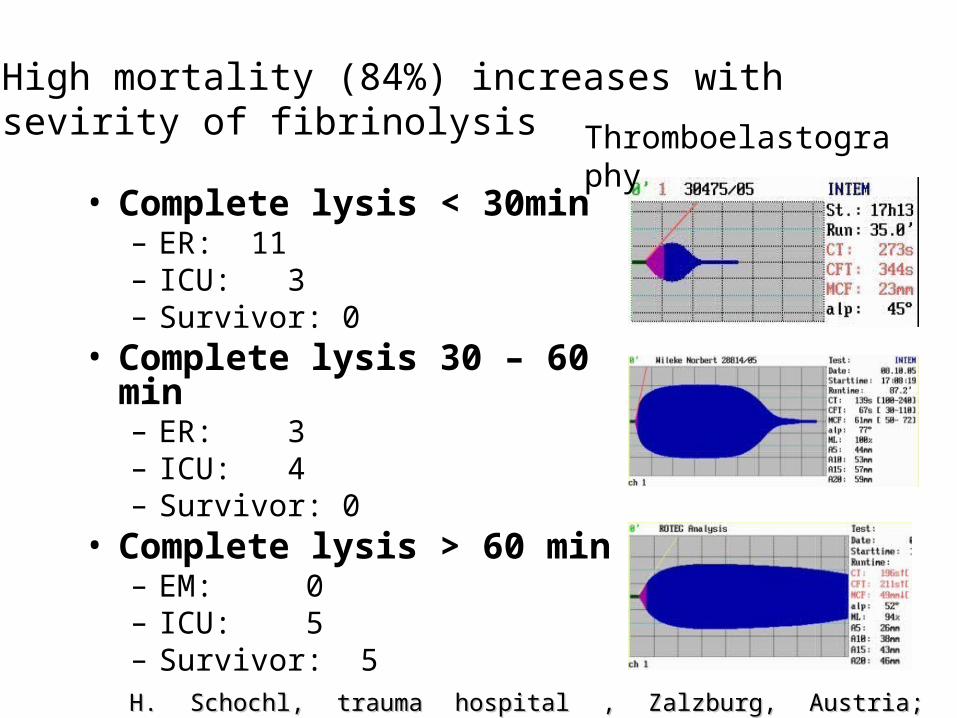
• Complete lysis < 30min– ER: 11– ICU: 3– Survivor: 0
• Complete lysis 30 – 60 min– ER: 3– ICU: 4– Survivor: 0
• Complete lysis > 60 min– EM: 0– ICU: 5– Survivor: 5
High mortality (84%) increases with sevirity of fibrinolysis
H. Schochl, trauma hospital , Zalzburg, Austria; unpublishedH. Schochl, trauma hospital , Zalzburg, Austria; unpublished
Thromboelastography
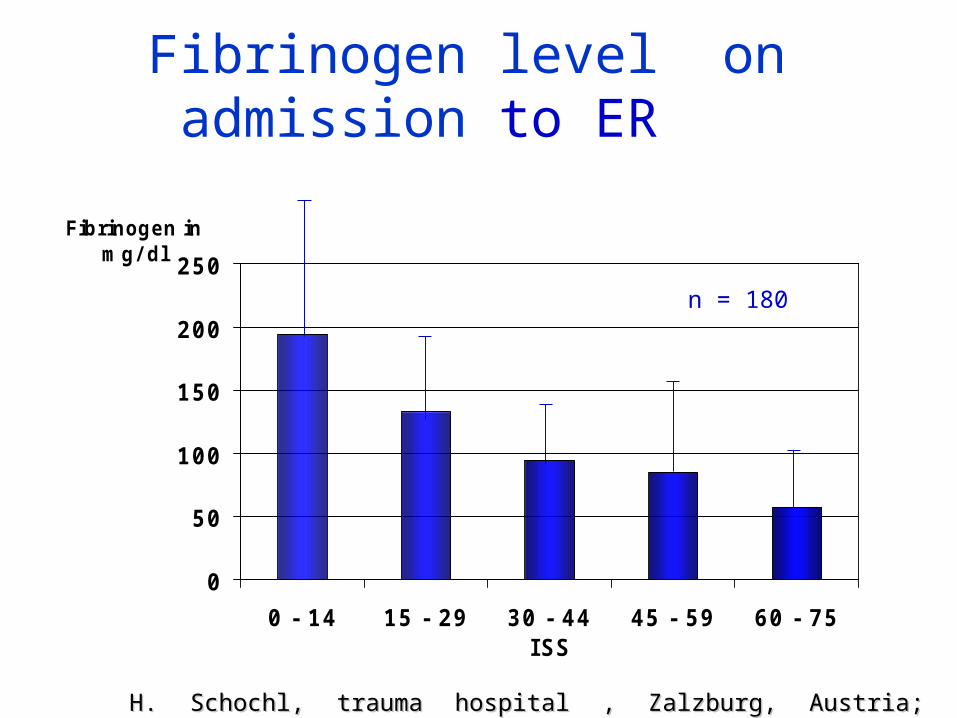
Fibrinogen level on admission to ER
0
50
100
150
200
250
0 - 14 15 - 29 30 - 44 45 - 59 60 - 75ISS
Fibrinogen in mg/ dl
H. Schochl, trauma hospital , Zalzburg, Austria; unpublishedH. Schochl, trauma hospital , Zalzburg, Austria; unpublished
n = 180
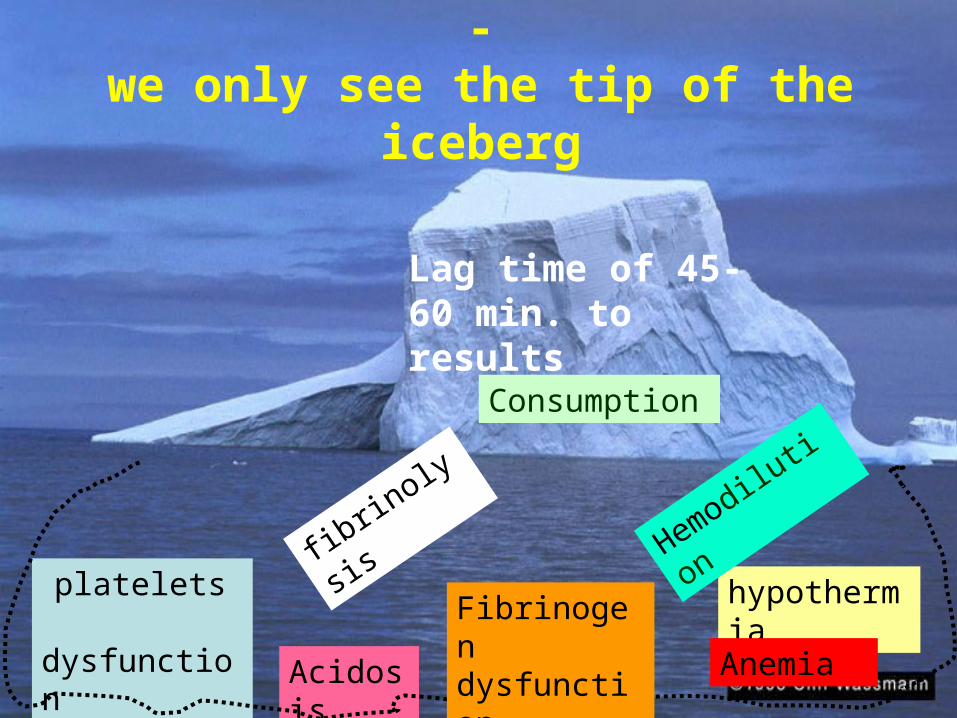
Coagulopathy is underestimated -we only see the tip of the iceberg
Acidosis
hypothermia
platelets dysfunction
fibrinolysis
Hemodilutio
n
Anemia
Consumption
Lag time of 45-60 min. to results
Fibrinogen dysfunction
1111
1212
1313
1414
1515
1616
1717
2626 2828 3030 3232 3434 3636 3838 4040 4242
Temperature (°C)Temperature (Temperature (°°CC))
PT (S
ec)
PT (S
ec)
PT (S
ec)
3434
3939
4444
4949
5454
5959
2626 2828 3030 3232 3434 3636 3838 4040 4242
Temperature (°C)Temperature (Temperature (°°C)C)PT
T (Se
c)
PTT (
Sec
PTT (
Sec
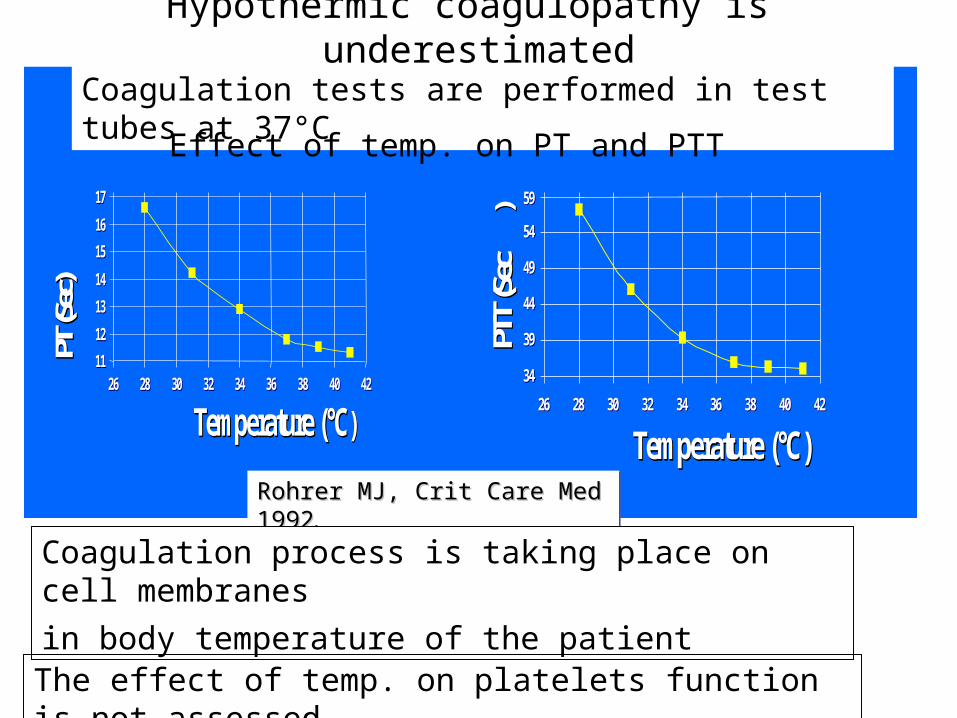
))Rohrer MJ, Crit Care Med 1992Rohrer MJ, Crit Care Med 1992..Rohrer MJ, Crit Care Med 1992Rohrer MJ, Crit Care Med 1992..
Hypothermic coagulopathy is underestimated
Coagulation tests are performed in test tubes at 37°C
Coagulation process is taking place on cell membranes
in body temperature of the patient
Effect of temp. on PT and PTT
The effect of temp. on platelets function is not assessed
Time [sec]
0 1000 2000 3000 4000 5000 6000
Coagulation
Fluid
Time [sec]
0 1000 2000 3000 4000 5000 6000
Clot
Time [sec]
0 1000 2000 3000 4000 5000 6000
FluidFibrinolysis
Time [sec]
0 1000 2000 3000 4000 5000 6000
Clo
t fo
rma
tion
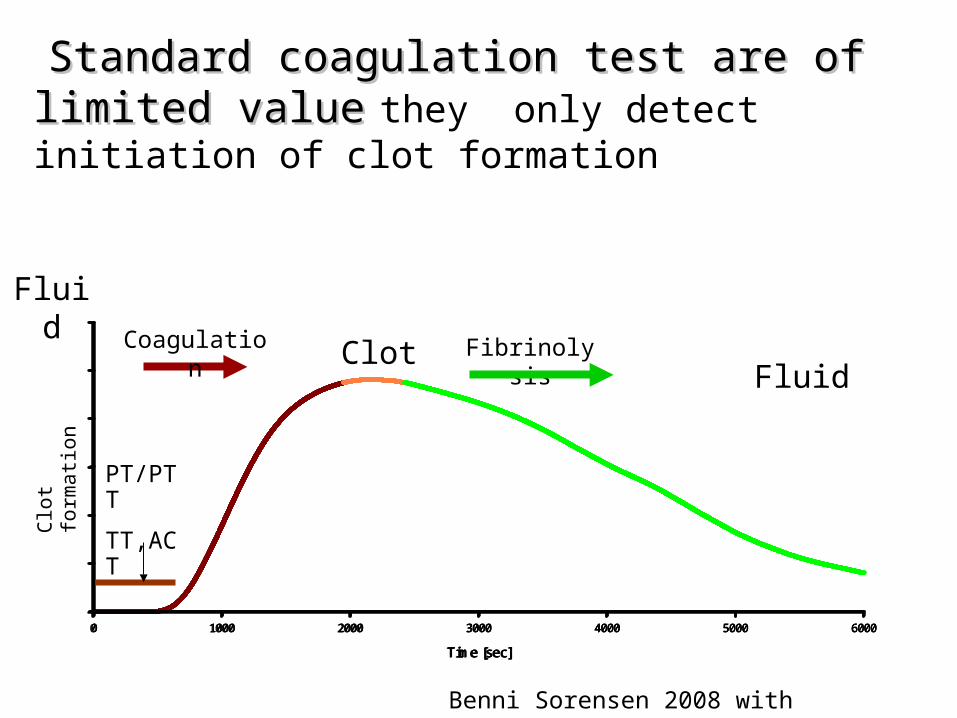
Benni Sorensen 2008 with permission
Standard coagulation test are of limited valueStandard coagulation test are of limited value
they only detect initiation of clot formation
PT/PTT
TT,ACT
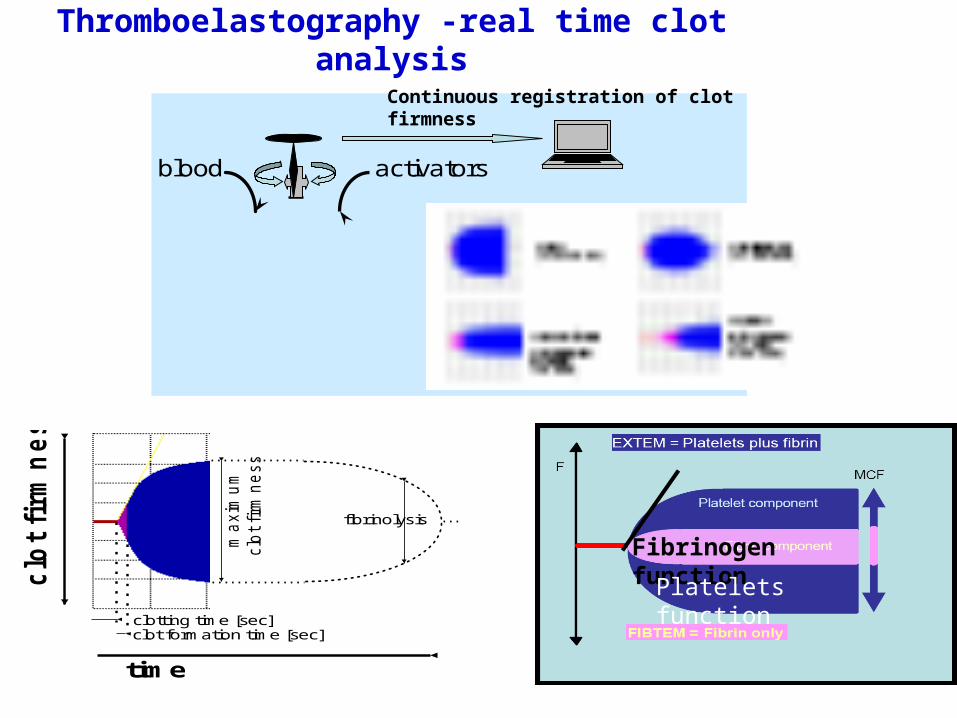
Thromboelastography -real time clot analysis
clotting time [sec]clot formation time [sec]
ma
xim
um
clo
t firm
ne
ss
fibrinolysis
clo
t fi
rmn
ess
time
blood activators
Continuous registration of clot firmness
Fibrinogen function
Platelets function
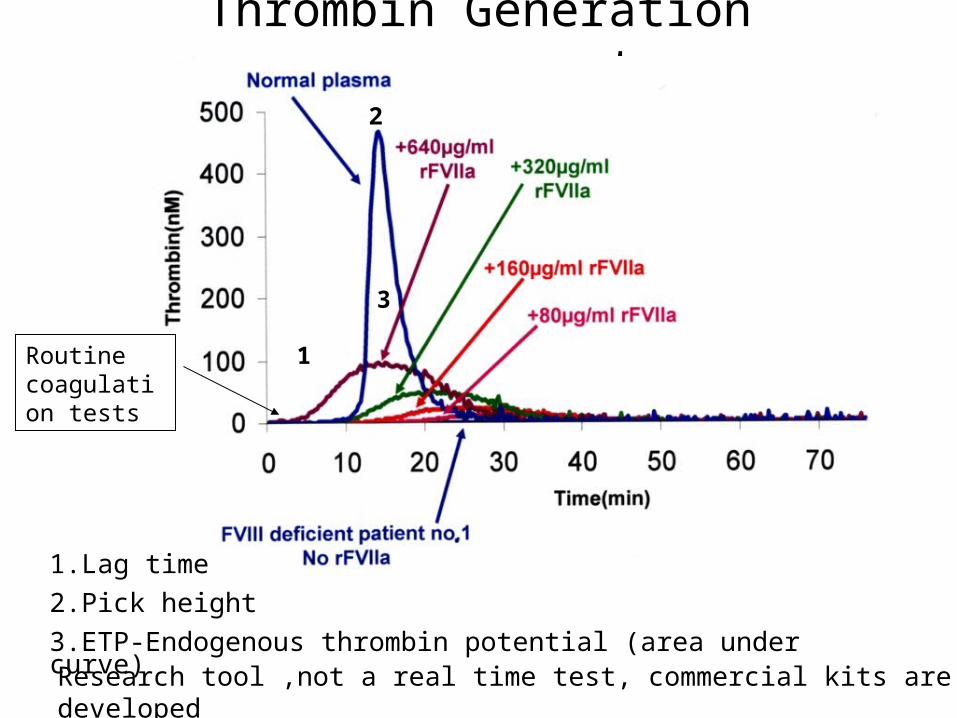
Thrombin Generation measurement
1.Lag time
2.Pick height
3.ETP-Endogenous thrombin potential (area under curve)
1
3
2
Research tool ,not a real time test, commercial kits are developed
Routine coagulation tests
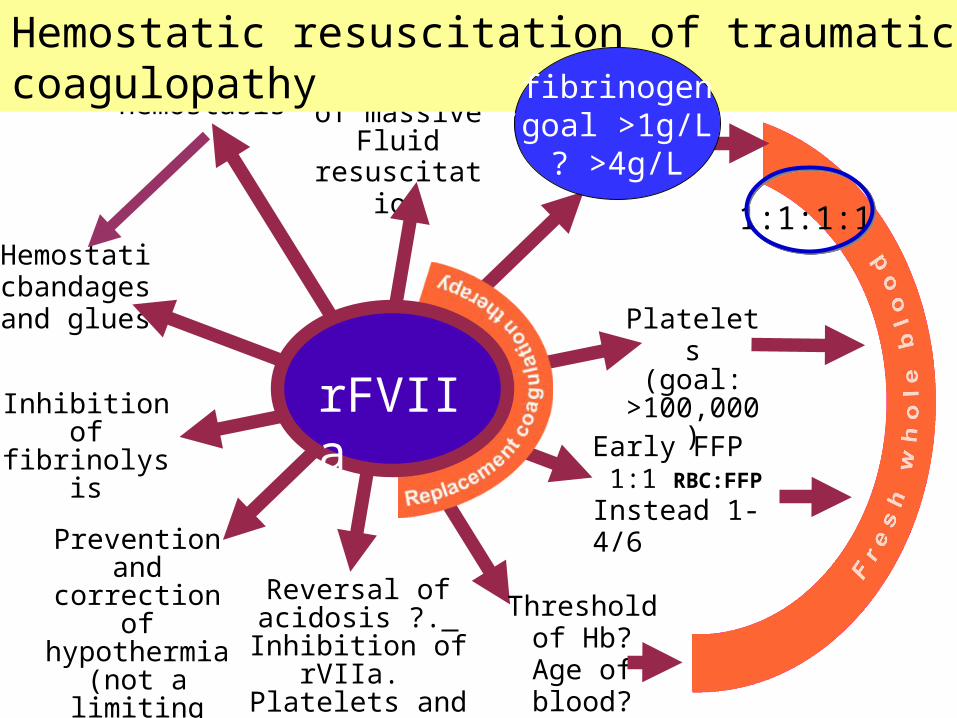
Surgicalhemostasis
Reversal ofacidosis ?. Inhibition of
rVIIa. Platelets and Fib. may be
needed
Inhibitionof
fibrinolysis
Avoidanceof massive
Fluidresuscitatio
n
Hemostaticbandage
sand glues
Preventionand correction
of hypothermia
(not a limitingfactor for
rFVIIa)
Threshold of Hb? Age of blood?
Early FFP 1:1 RBC:FFP
Instead 1-4/6
Platelets(goal:
>100,000)rFVIIa
Hemostatic resuscitation of traumatic coagulopathy
1:1:1:1
fibrinogen(goal >1g/L
? >4g/L
The blood bank: from (problematic) provider to partner in massively bleeding patients
Pär I. Johansson, Transfusion 2007 Aug. 47:176-181s (Anesth.+transfus
Early hemostatic rescusitation
Pro-hemostatic agents :
Extra-vascular (surgical):
● Fibrin glues ● New hemostatic polymers Intravascular - ● Fibrinolytic / proteolytic inhibitors ● Coagulation factors (cryo, FFP) and platelets ● Coagulation factor concentrates PCC, APCC, fibrinogrn FXIII , platelets substitutes ● DDAVP … ● New generation of Injury-specific hemostatic agents . (rFVIIa, Xa / PL, pdVIIa/Xa ,mutants rFVIIa)
ConclusionCoagulopathy is common in major trauma, its Coagulopathy is common in major trauma, its severity correlates with bleeding and mortalityseverity correlates with bleeding and mortality
Hypothermia , acidosis, hemodilution are Hypothermia , acidosis, hemodilution are important confounders of the coagulation important confounders of the coagulation processprocess
Hyperfibrinolysis is underestimatedHyperfibrinolysis is underestimated
Fibrinogen depletes early in severe trauma Fibrinogen depletes early in severe trauma
Standard coagulation test are of limited valueStandard coagulation test are of limited value
Thrombelastography could be helpful in Thrombelastography could be helpful in detecting coagulopathy and monitor treatmentdetecting coagulopathy and monitor treatment
• Overview of rFVIIa
Thank you for your participation,I hope it was usefull