Embed Size (px)
Citation preview

Massachuse(s General Hospital Center for Periopera6ve Care Re-‐design
Minakshi Raj, MPH; Caroline Horgan, RN; Kate Riddell, MD; Eden Brand, MPH Department of Anesthesia, Cri@cal Care and Pain Medicine
MassachuseCs General Hospital, Boston, MassachuseCs, USA
1. Improve Pa6ent Experience i. Reduce pa@ent processing @me and shorten
@me wai@ng in lines ii. Reduce pa@ent anxiety on the morning of
surgery 2. Reduce Delays
i. Reduce first case delays resul@ng from prep and transport delays
ii. Prevent delays in later case-‐starts resul@ng from first case delays
3. Increase Nursing and Admin Efficiency and Simplify Process
i. Reduce the @me OR staff spend wai@ng for pa@ents to arrive
ii. Reduce CPC check-‐in staff’s overwhelming workload between 5:30 and 6:30
A @me and mo@on study was conducted in June 2015 to iden@fy boClenecks in the current process. We created a current state process map (see Figure 4) and in collabora@on with CPC staff and leadership developed a future state process map. In the pilot a CPC administrator checked in pa@ents in the main hospital lobby from 5:00-‐5:25am (see Figure 6), and then returned to the CPC main desk to con@nue checking in pa@ents. Tools to support the CPC admin were created including: instruc@ons; conversa@on scripts; and colored pa@ent instruc@on cards. Some@mes, pa@ents who had a later case surgery also arrived at MGH prior to 5:30am. To ensure that the check-‐in process was fair and @mely for pa@ents who were scheduled for 1st case surgery, we created colored cards to triage pa@ents who checked in early (see Figure 5). The cards ensured CPC staff could easily iden@fy pa@ents based on @me of their surgery. Finally, we communicated and collaborated with mul@disciplinary teams throughout the hospital, including CPC leadership and administra@ve staff, security staff, and main lobby support staff, to ensure all groups were aware of and suppor@ve of the pilot and redefined process.
60
50.5
40
45
50
55
60
65
Monday
Time (M
inutes)
CPC Processing Time from Check -‐ In to Departure on Mondays
Pre -‐ Pilot
Pilot
IT Organiza6onal Issues
Pa6ent Percep6ons
Physical Resources
Hospital Policies Owned by Other Groups
Within Scope of Control Out of Scope of Control
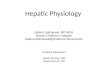
We observed the greatest reduc@on in processing @me on Mondays; on average, pa@ents were processed 9.5 minutes faster (see Figure 7). An overall average reduc@on in processing @me of 4 minutes was observed for each weekday. An average of eight pa@ents were checked in prior to 5:30am in the main hospital lobby each morning, allowing the morning shib CPC staff to experience a smoother workflow. We observed a number of addi@onal posi@ve outcomes of the pilot, including a reduc@on in @me wai@ng to check in. An improvement in pa@ent sa@sfac@on was also reported. The successful pilot process was suggested by a CPC staff member, and our adop@on of her sugges@on led to enhanced job sa@sfac@on and engagement between administra@ve staff and leadership. Feedback was sought from CPC staff resul@ng in collabora@on throughout the development and implementa@on of the pilot.
Based on our evalua@ons and results of the pilot, we recommend making the early check-‐in process standard for first case surgery pa@ents. We suggest designa@ng a member of the CPC staff to conduct future evalua@ons of the CPC process and to reassess the impact of the new process in 3-‐4 months. Other boClenecks were iden@fied during the ini@al shadowing process, such as in the transporta@on of pa@ents from the CPC to the opera@ng room. These boClenecks can be targeted next as areas for improvement. Finally, we recommend con@nuing to solicit feedback and sugges@ons from pa@ents and staff in order to con@nue improving the process and working towards achieving our goals of improving pa@ent experience, process and efficiency, and reducing delays in surgical start @me.
First case pa@ents arrive at MassachuseCs General Hospital’s (MGH) main lobby between 5:00-‐5:30am to check in for surgery at the Center for Periopera@ve Care (CPC). The CPC building does not open un@l 5:30am (see Figure 1). Pa@ents who arrive before 5:30am must wait in the main lobby un@l 5:30am. At 5:30am, 20+ pa@ents and their families proceed to the elevators and wait in the line to check-‐in (see Figures 2 and 3). Pa@ents experience very long wait lines to be processed for surgery, and CPC staff experience an overwhelming workflow un@l the majority of first-‐case pa@ents are checked in and processed.
Pa@ent Experience
On Time Surgical Starts
Improve Process and Efficiency
Figure 7. Note: Findings were not sta0s0cally significant due to limited sample size
Figure 3. Pa0ent View of CPC Entrance from Elevator
Figure 2. Pa0ent View of CPC Hallway
Surgical
Check In
Desks
Figure 1. CPC Check-‐In Desk
Security Staff Desks White Lobby Check-‐In Desk
Wai@ng Area
Wai@ng Area
Figure 6. Pilot: Main Lobby Check-‐In
Background
Evalua6on
Goals
Methods
Challenges
Results and Posi6ve Outcomes
Recommenda6ons
Time-‐Mo@on studies along with @me-‐stamps documented on EMR were collected and analyzed . Data was collected for eight days in July to measure current state, along with eight days of data during the pilot. We also evaluated the success of the pilot based on visual observa@ons, for example, shorter lines at 5:30am and a less overwhelming workflow. Our evalua@ons included feedback from staff on their experiences with the new workflow, and from pa@ents on their sa@sfac@on.
Figure 4. Current State Process Map
Figure 5. Colored Card