Embed Size (px)
Citation preview

Mass Chemical Incidents:Mass Chemical Incidents:Principles of Hospital Principles of Hospital
ManagementManagement
P. Halpern, MDChair, Emergency Department
Tel Aviv Medical Center

Granitville NC, Jan 2005, 0200am
The rail crew that parked 2 cars on the side rail by the Avondale Mills facility had not switched the diversion switch back and had gone home hours before an oncoming train with the chlorine railcars arrived.
The event killed nine and temporarily displaced thousands in Graniteville.

Responders from the local volunteer fire department responded to the train crash and subsequent chlorine release without first donning personal protective gear.
Neither law enforcement personnel nor emergency responders seemed trained/drilled/prepared for this scenario.

The area of evacuation was insufficient. A woman who lived 2.5 miles downwind was not evacuated. She awoke that morning feeling weak, and noticed “a strange fog” outside.
She learned about the disaster on TV. When her husband came home later, they left their home and went to relatives, but the chlorine came there also, so they went back home.

The woman did not go to an ED until 4 days after the incident.
There was no notification to her or others about health effects to watch out for. The hospital diagnosed her with pneumonia and gave her antibiotics, which did not help at all.
Conclusions
When a moderate-sized chemical event
occurred in the US, appropriate
procedures and capacity were in hand
locally or in relatively close proximity,
yet much of the available capacity was
never or sub optimally employed.
Why Should Civilian Doctors Know About Chemical Weapons ?
Agents potentially used by terrorists are involved in industrial and in transportation accidents (e.g. cyanide, acids, phosgene).
Some agents are generated in fires.Organophosphate insecticides act very much like military nerve gases.
The risk of terrorist incidents involving chemical weapons is now considered substantial.

Why should hospitals prepare for chemical mass incidents?
It may never happen, but probably WILL.
It is the hospital’s ethical duty to community to prepare;
It is an effective way to upgrade the entire system!
The Level of Awareness is Increasing
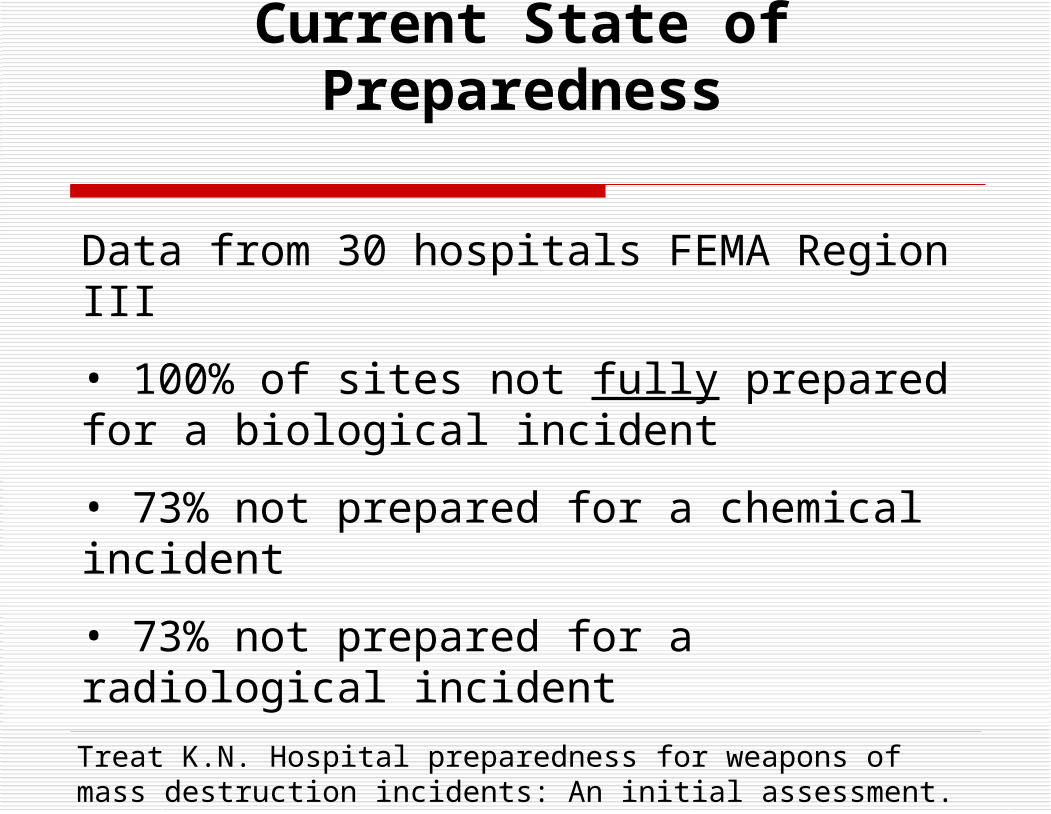
Current State of Preparedness
Data from 30 hospitals FEMA Region III
• 100% of sites not fully prepared for a biological incident
• 73% not prepared for a chemical incident
• 73% not prepared for a radiological incident
Treat K.N. Hospital preparedness for weapons of mass destruction incidents: An initial assessment. Annals of Emergency Medicine Nov. 2001

73% would set up a “single room” decontamination process.
13% had no decontamination process. Only 3% (1 hospital) had chemical
antidote stockpile 0% had prepared media statements 25% had “some” training in WMD
incidents
Current State of Preparedness

KA Candiotti: Anesth Analg 2005;101:1135-1140
Poll of all 135 US anesthesiology programs; 37% had any form of training, most did not
repeat training after initial sessions. 28% of programs east of the Mississippi reported
some training, whereas only 17% of programs west of it reported training available.
The majority of anesthesia residency programs in the US provide little or no training in the management of patients exposed to WMD 27

The Differences between non-conventional & conventional MCI
Number of casualties X 10, 100. Event may be overt or covert. Requirements for decontamination, staff
protection and site contamination disrupt normal facility response.
Disruption of external support may impede response (e.g. traffic jams).
Psychological effects on staff & victims.

ProcessTime for first walk-in victim to arrive (min)
Time for first victim to arrive by
ambulance (min)
Time for 500 more victims
to arrive (min)
Travel from attack site
to ED33 48 48-108
ProcessTime for first walk-in victim to arrive (min)
Time for first victim to arrive by
ambulance (min)
Time for 500 more victims
to arrive (min)
Travel from attack site
to ED33 48 48-108
Okumura T, et al: Report on 640 victims of the Tokyo Subway Sarin Attack. Ann Emerg Med 1996;28:129-135.
Time course of ED presentationafter Tokyo subway sarin attack
Vast majority of victims arrived within 2 hrVast majority of victims arrived within 2 hr

Tokyo Sarin eventTokyo Sarin event
TotalTotal 5,5105,510
Critically ill 17
Severely ill 37
Moderately ill 984
Required Mechanical Ventilation 54

Considerations for Hospital Preparedness Plan
Obtain commitment from management. It costs money, nobody likes the drills. Without authority and funding nothing will happen!
Designate a clear chain of command. Personnel must have incentives to train. Include field personnel in planning - not just
managers. Ensure continuing education for retention. Review plan periodically for changing threats,
environment, staff, equipment, concepts of care, hospital capabilities, funding.
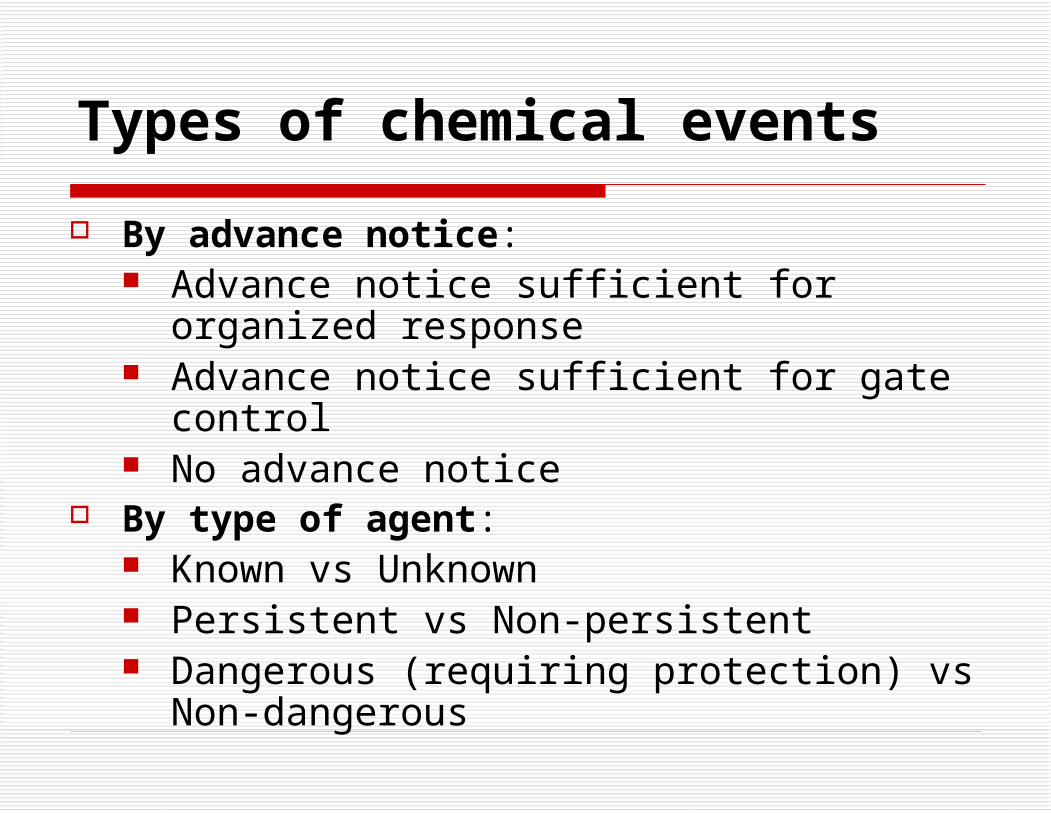
Types of chemical events
By advance notice: Advance notice sufficient for organized
response Advance notice sufficient for gate control No advance notice
By type of agent: Known vs Unknown Persistent vs Non-persistent Dangerous (requiring protection) vs Non-
dangerous
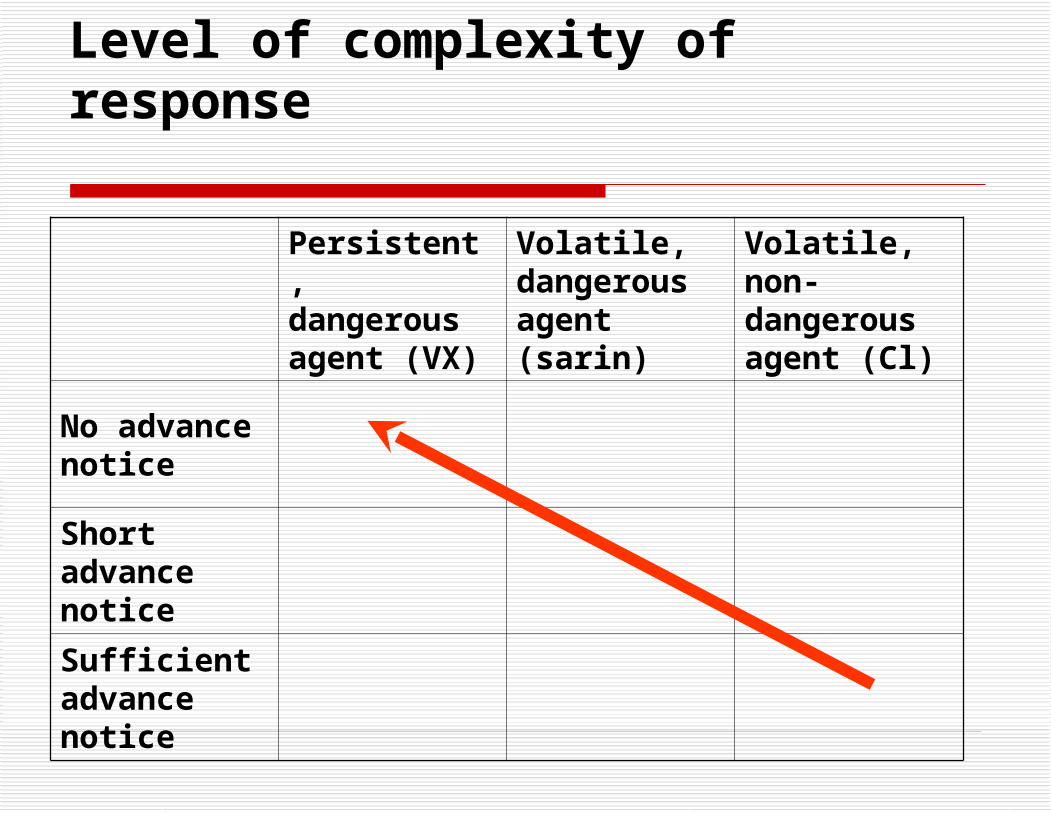
Level of complexity of response
Persistent, dangerous agent (VX)
Volatile, dangerous agent (sarin)
Volatile, non-dangerous agent (Cl)
No advance notice
Short advance notice
Sufficient advance notice

Steps in response:
Notification Confirmation Activation (by senior management) Activation of plan: decide if event requires
decontamination and staff protection or not Establish command structure, based on
available personnel Agent recognition:
Initially clinical by medical staff and specialists Then by specialized local or regional or
national, civilian or military staff

Identifying a Chemical Event
Victim characteristics: Minimal wounds Strong odors Unidentified liquids on body Respiratory complaints Eye or mucous membrane complaints Chemical burns Neurologic complaints Rapidly decreasing LOC or unconsciousness Cardiac arrest

Identifying a Chemical Event
Event characteristics: Easy (!) chemical container event
recognized Minor explosion Multiple victims Odors noted Immediate complaints by initially uninjured
victims Victims come from large area

Hospital Deployment Scheme
for Chemical Events
DecontaminationIntubation
Flow Control Site
Initial Triage
Walking CasualtiesImmediate Casualties
Secondary Triage
Mild
Pediatric
Resuscitation
Severe
CombinedModerate
Disrobe

Worst Case Scenario: no advance notice, persistent, hazardous agent
Decision making (senior staff +/- in consultation with expert):
Chemical event ? (event and victim characteristics)
Dangerous chemical ? Persistent chemical (e.g. chlorine vs
terrorist release)? Specific therapy exists for chemical (e.g.
organophosphates)? Declare chemical event in the ED and
activate emergency plans.

Hospital and ED perimeter control (gate triage: allow in immediate ALS only);
Activate decontamination facility; Call up staff; Coordinate with EMS etc. Request support (antidotes, ventilators,
secondary transfers);
Activities in the Hospital

Activities in the ED Continue life-saving procedures by
unprotected staff; Initiate ED evacuation of “regular pts”; Disrobe all event casualties; Mark and isolate contaminated area; Protected personnel to relieve non-protected
teams; Contaminated staff – to self decontamination; Staff call-up

Deploy ventilators (human or mechanical). If antidote or specific meds available for
specific agent, bring forward.
Deploy O2 masks, IVs, intubation kits, meds.
Deploy and ensure staff read treatment cards or computer messages for specific agent.
Use public address system to communicate patient care and staff protection policy.
Activities in the ED

Medications and specific equipment: Nerve agent meds:
Atropine Pralidoxime Scopolamine Benzodiazepines Eye drops β1 agonist, inhaled
Cyanide meds: Na nitrite Na thiosulfate Bicarbonate
Mustard: Burn care meds and
dressings Eye drops β1 agonist, inhaled

Factors influencing medical management
Is the agent identified? Type of agent (toxicity, aging, persistence, specific
Rx availability). Route of exposure: inhalation/percutaneous. Presence and severity of clinical disease. Elapsed time after exposure. Number of victims and rate of arrival. Advance notification. Available resources (i.e. AM/PM, level of
preparedness of facility, available external support).

Decontamination of Victims: Principles
Decon site should be close to ED. Decon site should be operative within 20
min of event recognition. Clear demarcation and physical barriers
between “hot” and “cold” zones. Strict patient, staff and crowd control is
essential. Single-channel, one-way patient flow is
essential.

Ready stores
Coherently arranged, clearly labeled, ready to use equipment, close to ED site

Decon area at the TASMC

Decontamination site during drillDecontamination site during drill
“Yellow line”

Decontamination procedure
Triage carried out by Level C-protected senior personnel:
Dead or dying Non-ambulatory, requires emergent
intubation Non-ambulatory, does not require emergent
intubation Ambulatory

Patients NOT requiring ventilatory support
Placed on wire-mesh gurneys
Given IM antidote (if nerve gas)
Decontaminated
Taken to “yellow line” and handed over as
above

Ambulatory pt decon
Disrobe down to underwear. No decontamination is performed,
except for vesicant agents. Anxiety victims are reassured and
discharged.

Non-ambulatory pt decon Full disrobing; Privacy provided as best possible; Warm water + liquid soap: head to toe, toe to
head x2, or 6 minutes. Bleach (0.5%) controversial (open wounds,
eyes). Decon staff wear Level C PPE. Decon staff are nurses or paramedical
personnel, who can recognize patient deterioration during decon.

Decontamination for Vesicants
Initial “dry decontamination” No scrubbing of skin Followed by wet decontamination Emphasis on irrigation of the eyes Consider using dilute bleach for
extreme skin exposure.

Care of Multiple Ventilator-Dependent Patients
Large numbers of ventilated pts anticipated
Designate alternate Intensive Care areas
Ensure O2 supply
Ensure supply of mechanical ventilators
and/or manual resuscitators
Train personnel to care for ventilated
patients and to ventilate manually

Identify and designate MD & RN trained in mechanical ventilation.
Ensure supplies of disposables and drugs (e.g. HMEs, tubing, sedatives, paralytics).
Prepare data management system (appropriate forms or computerized system).
Standardize care! Disallow multiple protocols and experimental or unproven therapies.
Ensure staff coordination and information dissemination (daily meetings, bulletins etc.)
Care of Multiple Ventilator-Dependent Patients

Summary
Preparing medical centers for chemical mass events is critical to successful event management, but also ethically and practically correct.
The unique features of a chemical attack make it probably the most challenging event any hospital may ever face.

Addendum: Hospital oxygen supplies:
Assume victims=50% of hospital capacity; 25% ventilated, i.e. for 1,000 bed hospital 500 victims, 125 ventilated pts.
Assume 15 lpm/pt, 21,600 liters/24hr/pt, 2,700,000 liters/24 hr/hospital.
Assume 50% require O2 by mask at 10 lpm/pt, i.e. 250x10x60x24=3,600,000 liters/24hr.
Assume 2,000,000 for rest of hospital use. Total: 8,300,000 liters/24 hr. My hospital’s total storage capacity: ______

Assume 40-bed ward, 20 ventilators @ 15lpm. Assume ventilators require pressure > 3.5 Atm. Assume 18 mask O2 pts @ 10 lpm.
Assume 2 CPAP pts @ 100 lpm. Assume 100 lpm surge flow (sudden opening of flow
meter, new patient connected to CPAP) Total required FLOW: 680 lpm. Assume pressure drop along tubing and check most
distant room!
Addendum: Hospital oxygen supplies:
![DANIEL HALPERN-LEISTNER - Columbia Universitydanhl/derived_equivalences... · DANIEL HALPERN-LEISTNER In [BO], Bondal and Orlov made the following Conjecture 0.1 (D-equivalence)](https://img.pdfslide.us/doc/110x75/6057dbfe94cc0e1ab62d2580/daniel-halpern-leistner-columbia-danhlderivedequivalences-daniel-halpern-leistner.jpg)






![Game Theory with Costly Computation - arxiv.org filearXiv:0809.0024v1 [cs.GT] 29 Aug 2008 Game Theory with Costly Computation Joseph Halpern Cornell University halpern@cs.cornell.edu](https://img.pdfslide.us/doc/110x75/5cea570788c9935c028c13cb/game-theory-with-costly-computation-arxivorg-08090024v1-csgt-29-aug-2008.jpg)