Embed Size (px)
Citation preview

J Am Acad Audiol 15:29–46 (2004)
29
Masking Redux II: A RecommendedMasking Protocol
Robert G. Turner*
AbstractThis is the second in a series of two papers on masking. The objective of thesepapers is to develop a masking protocol that provides valid measures of thresh-old and is, in general, faster than the plateau method. In the first paper, amasking method was presented that can replace the traditional plateau methodin most masking situations. This new method is optimized to require fewermasking levels than the plateau method. As a result, this optimized methodis faster, sometimes significantly, than the plateau method. This paper evalu-ates the optimized method and compares the optimized method to the traditionalplateau method. This paper identifies specific masking situations in which theoptimized method is not appropriate. A variation on the plateau method isdescribed. When combined with the optimized method, these two maskingmethods constitute a recommended masking protocol that can be used in allmasking situations.
Key Words: Audiometry, auditory thresholds, masking, optimized method,plateau method
Abbreviations: A1 = initial masking level (air conduction) for the optimizedmethod; ABG = air-bone gap; ABGN: = actual air-bone gap in the nontest ear;ABGT = actual air-bone gap in the test ear; AC = air conduction; AMR = ade-quate masking range; ATN = air-conduction threshold in the nontest ear; B1= initial masking level (bone conduction) for the optimized method; BC = boneconduction; BTT = bone-conduction threshold of the test ear; IA = actual inter-aural attenuation; IM = initial masking level for the plateau method, either air-or bone-conduction testing; MIA = assumed minimum interaural attenuation;NTE = nontest ear; PWA = plateau width for air conduction; PWB = plateauwidth for bone conduction; TE = test ear
SumarioEste es el segundo de una serie de dos trabajos relacionados con el enmas-caramiento. El objetivo de estos trabajos es desarrollar un protocolo deenmascaramiento que proporcione mediciones válidas del umbral y que sea,en general, más rápido que el método del plateau. En el primer trabajo, sepresentó un método de enmascaramiento que puede reemplazar al métodotradicional del plateau en la mayor parte de las situaciones que lo requieren.Este nuevo método ha sido optimizado para necesitar menos niveles deenmascaramiento que el método del plateau. Como resultado, este métodoes significativamente más rápido que el tradicional. Este trabajo evalúa elmétodo optimizado y lo compara con el método del plateau. El trabajo iden-tifica situaciones específicas de enmascaramiento en las que el métodooptimizado no es apropiado. Se describe una variante del método del plateau.Cuando se combinan con el método optimizado, estos dos métodos consti-
*Louisiana State University Health Sciences Center
Reprint requests: Robert G. Turner, Department of Communication Disorders, Louisiana State University Health Sciences Center,1900 Gravier St., Box G6-2, New Orleans, LA 70112; Phone: 504-568-4339; Fax: 504-568-4352; E-mail: [email protected]
The material in this paper has been presented at the American Academy of Audiology 15th Annual Convention, Philadelphia, PA,April 2002 and the American Speech-Language-Hearing Association Convention, New Orleans, LA, November 2001.
90305 Cassidy text 2/12/04 10:23 AM Page 29
This is the second and final paper in aseries on masking. It is stronglyrecommended that the first paper be
read prior to this paper. The purpose of thesepapers is to develop a masking protocol thatyields valid measures of threshold and issufficiently fast to be acceptable in mostclinical environments. Hopefully, this protocolwill discourage audiologists from usingshortcut masking procedures because theplateau method is perceived as being tooslow. In the first paper (Turner, 2003), anoptimized masking method is described thatshould, in many masking situations, besignificantly faster than the traditionalplateau method. This paper has severalobjectives: (1) theoretically evaluate thevalidity of the optimized method for a varietyof audiometric configurations; (2) comparethe optimized method to the traditionalplateau method; (3) determine any limitationson the use of the optimized method; (4)provide a recommended masking protocolthat can be used in all masking situations.
MASKING METHODS
Plateau Method
The most common masking procedure isthe plateau method. There are severalvariations on the plateau method. For thispaper, the plateau method will be defined asthe following:
1. Measure an unmasked air-conduction (AC) threshold for each ear and an unmasked bone-conduction (BC) threshold.
2. At each frequency, determine if masking is required using conventional criteria.
3. Set the initial masking level (IM) 10dB above the AC threshold of the nontest ear (NTE) and reestablish threshold.
4. The masking level is increased 10 dB and threshold reestablished.
5. When the masking level is increasedtwice (20 dB range) with no change(poorer) in threshold, the masker isin the plateau, and the measured threshold is the actual threshold.
Optimized Method
The masking method developed in thefirst paper is as follows:
1. Measure an unmasked AC thresholdfor each ear and an unmasked BC threshold.
2. At each frequency, determine if masking is required using conventional criteria.
3. Set the initial masking level equal tothe AC threshold of the test ear (TE)minus 10 dB and reestablish the threshold.
4. Determine the dB shift in thresholddue to the masker.
5. Increase the masking level an amount equal to the threshold shiftand reestablish threshold.
6. If threshold improves or does not shift, the masker is in the plateau and the actual threshold has been determined. If the threshold shifts,repeat steps 5 and 6.
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
30
tuyen el protocolo recomendado de enmascaramiento, que puede ser uti-lizado en todas las situaciones que demandan enmascaramiento.
Palabras Clave: Audiometría, umbrales auditivos, enmascaramiento, métodooptimizado, método del plateau
Abreviaturas: A1 = nivel de enmascaramiento inicial (conducción aérea)para el método optimizado; ABG = brecha aéreo-ósea; ABGN = brecha aéreo-ósea real en el oído no evaluado; AC = conducción aérea; AMR = rangoadecuado de enmascaramiento; ATN = umbral de conducción aérea en eloído no evaluado; B1 = nivel de enmascaramiento inicial (conducción ósea)para el método optimizado; BC = conducción ósea; BTT = umbral de con-ducción ósea en el oído evaluado; IA = atenuación interaural real; IM = nivelinicial de enmascaramiento para el método del plateau, tanto para evalua-ciones por vía aérea u ósea; MIA = supuesta atenuación interaural mínima;NTE = oído no evaluado; PWA = ancho del plateau para la conducción aérea;PWB = ancho del plateau para la conducción ósea; TE = oído evaluado
90305 Cassidy text_blcx2 2/18/04 11:18 AM Page 30

Masking Redux II/Turner
31
MASKING AND FREQUENCYDIAGRAMS
Masking diagrams, which are describedin detail in the first paper, can be used
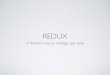
to illustrate the optimized method and theplateau method. Briefly, a masking diagramis a plot of masked threshold versus maskinglevel at a particular frequency. An examplefor AC testing is shown in Figure 1. In thisexample, the plateau is clearly evident inthe diagram, and both masking methods,optimized and plateau, have beenimplemented. The masking methods arerepresented by arrows on the maskingdiagram. The arrows indicate the masking
levels specified by the particular method.The black arrows (A1–A3) are the optimizedmethod, and the shaded arrows (IM andunlettered) are the plateau method.
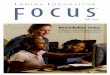
To the left of the masking diagram is afrequency diagram. This diagram representsone frequency on the audiogram and displaysa variety of information. To the left of the axisare unmasked, masked, and actualthresholds. (An explanation of theaudiometric symbols used in this and otherfigures is given in Figure 2.) If the unmaskedthreshold is the actual threshold, then onlythe unmasked threshold is shown. To theright of the axis are arrows corresponding tothe arrows in the masking diagram for the
optimized method. For the plateau method,only the arrow corresponding to the initialmasking level (IM) is shown on mostfrequency diagrams.
Based on the thresholds shown in Figure1, it is evident that there is a severe,unilateral, sensorineural loss in the rightear. We are assuming a minimum interauralattenuation (MIA) equal to 40 dB. The MIAis the criterion used to determine if maskingis required for AC thresholds. When theapparent ABG (air-bone gap) equals orexceeds the MIA, masking is needed. In allexamples in this paper, the MIA will be 40 dBfor AC testing, consistent with the use ofsupra-aural headphones. Supra-aural phones
Figure 1. Masking andfrequency diagrams forair-conduction testing ofthe right ear. The plateaumethod is represented byshaded arrows, the opti-mized method by blackarrows. See Figure 2 foran explanation of theaudiometric symbols. A1:initial masking level forthe optimized method;A2, A3: additional mask-ing levels for air-conduc-tion testing using theoptimized method. IA:actual interaural atten-uation; IM: initial mask-ing level for the plateaumethod.
Figure 2. Explanation of the audiometric symbolsused in other figures.
90305 Cassidy text 2/12/04 10:23 AM Page 31

present a more difficult masking situationthan insert phones and are a better test of amasking procedure. Masked BC thresholdsare required when the apparent ABG exceeds10 dB.
In this example, there is an apparentABG in the right ear of 45 dB; therefore,masking is required for the AC and BCthresholds. The actual interaural attenuation(IA) is 45 dB. With the plateau method, theinitial masking level (IM) would be 10 dBHL, 10 dB greater than the unmasked ACthreshold of the NTE. The masking levelwould be increased in 10 dB steps until theplateau is defined by two increases in maskinglevel with no change in threshold. This isshown by the shaded arrows in Figure 1.
With the optimized method, initialmasking level (A1) is set at 35 dB HL, 10 dBless than the AC threshold of the TE. Thismasking level is 35 dB above the AC thresholdof the NTE. Thus, we would expect a shift inmasked threshold up to 35 dB. In this case,the right AC threshold shifts 35 dB from 45dB HL to 80 dB HL. Because the threshold hasshifted 35 dB, we increase the masking levelby the same amount, 35 dB. This level (A2)produces a 10 dB shift in threshold. Becausethe threshold shifted 10 dB, the maskinglevel is increased 10 dB (A3). The thresholdremains the same confirming that themaskers A2 and A3 are in the plateau region.
PLATEAU WIDTH AND AMR
Plateau Width
Before evaluating the two maskingprocedures, it is worthwhile to review theissue of plateau width. With any maskingprocedure, accurate thresholds will bemeasured when the masking level is withinthe plateau region. Thus, the ability to placethe masker within the plateau is related tothe width of the plateau. This width can varysignificantly depending upon several factors.Understanding the relationship betweenplateau width and audiogram configurationis important for anticipating maskingdifficulty and for selecting the appropriatemasking procedure.
The equations for plateau width areeasily derived from the equations of Liden etal (1959) for calculating minimum effective
masking and maximum usable masking. Theequations for plateau width are
PWA = 2IA - ABGT - ABGN (1)
PWB = IA - ABGN (2)
where PWA is plateau width for air-conduction testing, PWB is plateau widthfor bone-conduction testing, IA is the actualinteraural attenuation, ABGT is the actualair-bone gap (ABG) in the TE, and ABGN isthe actual air-bone gap in the NTE.
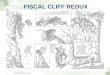
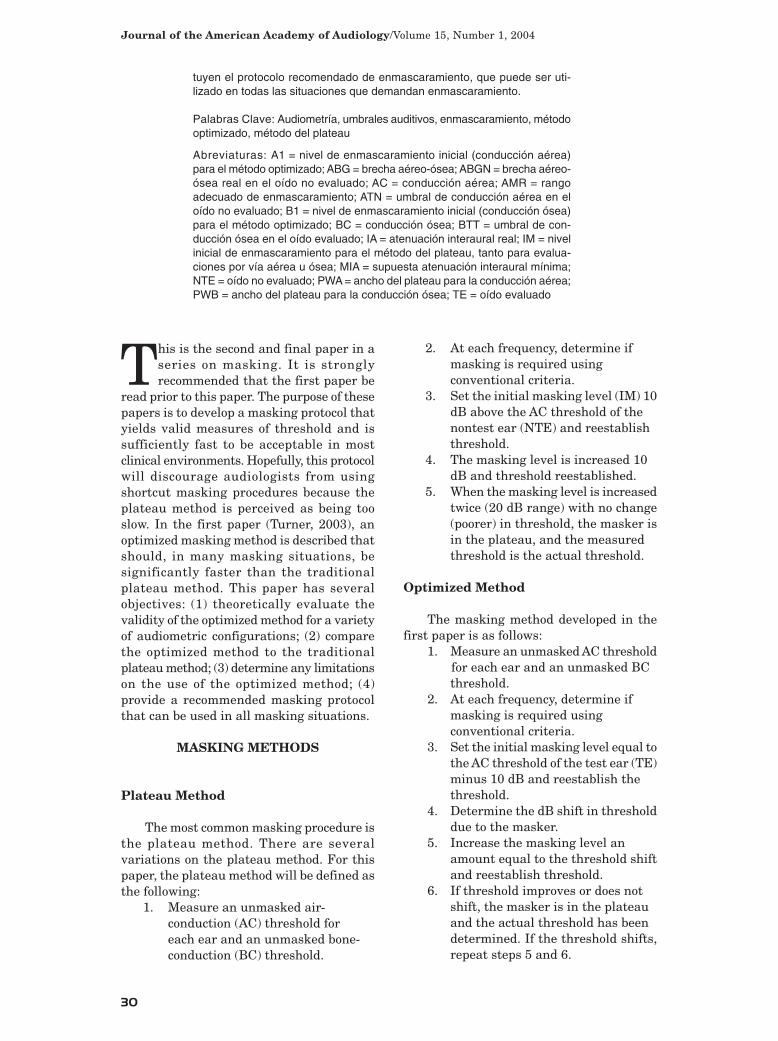
We can illustrate these equations usingFigure 3. In the frequency diagram, it isevident that the unmasked AC threshold inthe right ear (60 dB HL) is 50 dB greater thanthe unmasked BC threshold (10 dB HL). Theunmasked AC threshold is not the actualthreshold in the right ear and, therefore,must be due to crossover to the NTE. The IAmust be 50 dB. If IA was less than 50 dB, theunmasked AC threshold would have occurredat a lower (better) level. The actual thresholdsalso indicate a 40 dB ABG in the right ear (90dB HL minus 50 dB HL) and a 20 dB ABGin the left (30 dB HL minus 10 dB HL). UsingEquation 1, we have
PWA = 2IA - ABGT - ABGN = 100 - 40 - 20 = 40 dB
This value, 40 dB, agrees with the plateauwidth in the masking diagram. We can useEquation 2 to calculate plateau width for BCtesting.
PWB = IA - ABGN = 50 - 20 = 30 dB
This agrees with the BC plateau width in themasking diagram.
These equations are not particularlyuseful when measuring thresholds becausethe thresholds that you are trying to measuremust be known to evaluate the equations. Theequations do, however, provide useful insightinto plateau width. With AC testing, theplateau width can be as great as twice the IAand can easily exceed 100 dB. Plateau widthis reduced by conductive loss in either ear.Plateau width for BC testing is generallysmaller than for AC testing with a maximumwidth equal to the IA. This width is reducedby conductive loss in the NTE; conductive lossin the TE has no effect. As we will see, plateauwidth for AC and BC testing can be reduced
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
32
90305 Cassidy text 2/12/04 10:23 AM Page 32
Masking Redux II/Turner
33
to zero for certain conditions, producing theclassic masking dilemma.
With BC testing in the low frequencies,it may be necessary to correct for the occlusioneffect. This is an increase in bone-conductedsound in the NTE because the ear is occluded.When required, the initial masking level isincreased by an amount that depends on thefrequency of testing, the type of headphone,and the amount of conductive loss in theNTE. Also, the occlusion effect will increasethe minimum effective masking level, that is,the minimum masking required to reach theplateau. At first glance, this would indicatethat the occlusion effect would decreaseplateau width. In fact, data suggest that themaximum useable masking level will increasean equal amount and that plateau widthwould be relatively unchanged. (See Yacullo,1996, 65, for a more detailed explanation.)
Adequate Masking Range
Technically, the masking plateau onlyoccurs when the unmasked threshold in theTE is not the actual threshold but results fromcrossover to the NTE. If the unmaskedthreshold is the actual threshold, then therewill be no plateau. For all masking levels upto overmasking, the threshold will remain atthe actual threshold; there will be no regionof undermasking to help define a plateau. Wecan define, however, an adequate maskingrange (AMR) that is somewhat analogous tothe plateau. This is the range of maskinglevels from the minimum masking needed tomask the NTE to the maximum useablemasking before overmasking. When the
masking level is in this range, we know thatthe NTE is masked and is not responding tothe tone. Minimum masking for the AMR isnot the same as the minimum effectivemasking level for the plateau. For this paper,minimum masking is equal to the initialmasking level, IM, as defined by Martin(1974). That is, the AC threshold of the NTEplus 10 dB.
Interestingly, the AMR for AC testingequals that for BC testing and is given by thefollowing equation:
AMR = IA + BTT - ATN - 10 dB (3)
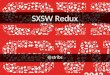
where BTT is the actual BC threshold in theTE and ATN is the actual AC threshold in theNTE. Figure 4 shows a masking diagram fora situation where the unmasked AC thresholdin the right ear is the actual threshold. In thisexample we assume that IA = 50 dB. ApplyingEquation 3 we have
AMR = IA + BTT - ATN - 10 dB = 50 + 10 - 20 - 10 = 30 dB
The value of 30 dB agrees with the AMRindicated in the masking diagram.
UNMASKED THRESHOLD PATTERNS
The decision to mask and the decision asto masking procedure are based on the
configuration of the unmasked thresholds. Itis useful to divide the unmaskedconfigurations into four patterns. In allpatterns, the TE is the “poorer ear.” That is,the unmasked AC threshold of the TE is
Figure 3. Masking and fre-quency diagrams illustratingplateau width for air-conductiontesting (PWA) and bone-con-duction testing (PWB). See Fig-ure 2 for an explanation of theaudiometric symbols. ABGN:actual air-bone gap in the non-test ear. ABGT: actual air-bonegap in the test ear. IA: actualinteraural attenuation.
90305 Cassidy text 2/12/04 10:23 AM Page 33

equal to, or poorer than, the unmasked ACthreshold of the NTE. The poorer ear wouldbe tested first for masked thresholds.
The first pattern (Figure 5a) is called“unilateral” because the unmasked thresholdsindicate the possibility of a unilateralconductive loss; that is, there is an apparentABG in the TE. The actual loss could beconductive with the actual ABG equal to theapparent ABG, mixed with an actual ABGsmaller than the apparent ABG, orsensorineural, in which case there would beno actual ABG. Note, the unmasked BCthreshold does not have to lie in the normalrange. It is the relationship between the twounmasked AC thresholds and the singleunspecified (as to ear) unmasked BCthreshold that is important, not the absolutelevels. For this pattern, the apparent ABG inthe TE must be sufficient to require masking.That is, the apparent ABG must equal or
exceed the MIA. In the NTE, the apparentABG must be 10 dB or less.
The second pattern (Figure 5b) is called“bilateral” because of the possibility ofbilateral conductive loss. Only one ear musthave conductive loss; the other could beconductive, sensorineural, or mixed. In theTE, the apparent ABG must be sufficient torequire masking. In the NTE, the ACthreshold must be, by definition, at least 25dB better than the AC threshold of the TE.
The third pattern (Figure 5c) is called“symmetrical” because of the possibility ofsymmetrical bilateral conductive loss. Onlyone ear must have conductive loss; the othercould be conductive, sensorineural, or mixed.In the TE, the apparent ABG must besufficient to require masking for the ACthreshold. By definition, the difference inunmasked AC thresholds must be 20 dB orless. In this pattern, there is a significantpossibility of overmasking.
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
34
Figure 4. Masking and fre-quency diagrams illustrat-ing adequate maskingrange (AMR). See Figure 2for an explanation of theaudiometric symbols. ATN:air-conduction threshold inthe nontest ear. BTT: bone-conduction thresholdof the test ear. IA: actualinteraural attenuation.
Figure 5. Four basicpatterns for unmaskedthreshold configurations.See Figure 2 for anexplanation of the audio-metric symbols. MIA:assumed minimuminteraural attenuation.
90305 Cassidy text 2/12/04 10:23 AM Page 34

The fourth pattern (Figure 5d) is called“bone-only” because only the BC thresholdsin one or both ears require masking. There isno need to mask AC thresholds because theapparent ABG is less than the MIA in bothears. If the apparent ABG is greater than 10dB, masking is required for BC. An apparentABG of 5 or 10 dB would not be maskedbecause the ABG could be closed with maskingdue to test variability and central masking.
EVALUATION OF MASKINGMETHODS
The plateau and optimized maskingmethods were evaluated using masking
diagrams for different threshold configurationsthat were derived from the unilateral,bilateral, symmetrical, and bone-onlypatterns. Obviously, a large number of actualaudiometric configurations can be derivedfrom any one pattern. Only a representativesample will be shown in this paper. Additionalconfigurations have been evaluated but arenot shown.
In all diagrams in this paper, the rightear will be the TE and the left the NTE. Theevaluation of the procedures will be based ontwo questions: (1) For a particular thresholdconfiguration, does the masking procedureplace the last masking level (arrow) within
the plateau and, thus, yield the validthreshold? (2) For a particular thresholdconfiguration, which procedure requires thefewest masking levels (arrows) to identifythe plateau? The two procedures will beevaluated for the four threshold patterns.
Unilateral Pattern
Consider the “best case” situation inFigure 6. The hearing loss in the TE isentirely sensorineural which results in thelargest plateau or AMR. Only conductive lossdiminishes plateau width. In fact, plateauwidth is 100 dB and 50 dB, respectively. Inthe unilateral pattern, the initial maskinglevel (A1) for the optimized method issignificantly greater than that (IM) for theplateau method. In this example, A1 is 40 dBabove the unmasked AC threshold of theNTE. Thus, we would expect a shift inmasked threshold up to 40 dB. In this case,threshold shifts 20 dB from 50 dB HL to 70dB HL. The actual threshold shift (20 dB) ismuch less than the maximum possible shift(40 dB), providing strong evidence that theinitial masking level (A1) is well into theplateau. Following the optimized method,the masking level is increased 20 dB (theamount of threshold shift) to 60 dB (A2). Thethreshold remains the same confirming the
Masking Redux II/Turner
35
Figure 6. Masking and fre-quency diagrams for a bestcase unilateral pattern.Test ear has sensorineuralloss. Note that the opti-mized method requiresfewer masking levels thanthe plateau method. SeeFigure 2 for an explanationof the audiometric symbols.A1: initial masking levelfor air-conduction testingusing the optimizedmethod; A2, A3: additionalmasking levels for air-con-duction testing using theoptimized method. B1: ini-tial masking level for bone-conduction testing usingthe optimized method; B2:additional masking levelfor bone-conduction testingusing the optimizedmethod. IA: actual inter-aural attenuation. IM: ini-tial masking level for theplateau method, either air-or bone-conduction testing.
90305 Cassidy text 2/12/04 10:23 AM Page 35

plateau. Thus, the optimized method requirestwo masking levels to identify plateau andyield the actual threshold. In contrast, theplateau method requires four masking levels.The difference between the procedures ismore dramatic for BC testing. For thisexample, and all future examples, we willassume that the BC limit for the audiometeris 60 dB HL, as indicated in Figure 6. Theoptimized method requires two maskinglevels to move threshold beyond the limit ofthe audiometer, whereas the plateau methodrequires eight levels.
For any unmasked threshold pattern,we can define a “worst case” situation thatwould yield the minimum plateau width orAMR. For this to occur, the IA must equal theMIA, for example, 40 dB for supra-auralphones. The apparent ABG in the unmaskedthresholds for the TE must represent theactual ABG, and that ABG must be maximumconductive, that is, the ABG equals the IA.It should be recognized that an ABG cannotexceed the IA. With this worst case, anyapparent ABG in the unmasked thresholdsfor the NTE must be the actual ABG in thatear. While this situation would rarely occur,it represents the most difficult maskingsituation. We can use the equations presentedearlier to calculate the worst case plateauwidth and AMR. For the unilateral pattern,the minimum plateau width is 30 dB andthe minimum AMR is 20 dB.
A worst case situation for the unilateralpattern is shown in Figure 7. We assume IAequals 40 dB, the ABG in the TE is maximum
conductive (40 dB), and there is a 10 dB ABGin the NTE. In this situation, there is noplateau, but there is an AMR. As stated above,the AMR equals 20 dB.
With the plateau method, three maskinglevels would be required for both AC and BCtesting. With the recommended method, only onelevel (A1, B1) is theoretically required. B1 is theinitial masking level specified by the optimizedmethod for BC testing. Both A1 and B1 wouldbe 20 dB above the unmasked AC threshold inthe NTE and should be sufficient to mask anycrossover to the NTE. If there is no change inthreshold, then the unmasked threshold is theactual threshold. If desired, it is generallyacceptable to use an additional masker, 5 dB to10 dB greater, to confirm the plateau. In thisexample, there should be no change in thresholdwith A1 or B1. If the threshold should shift(poorer) 5 to 10 dB because of test variabilityand/or central masking, the masking level canbe increased an equal amount. There should beno further change (poorer) in thresholdconfirming the AMR.
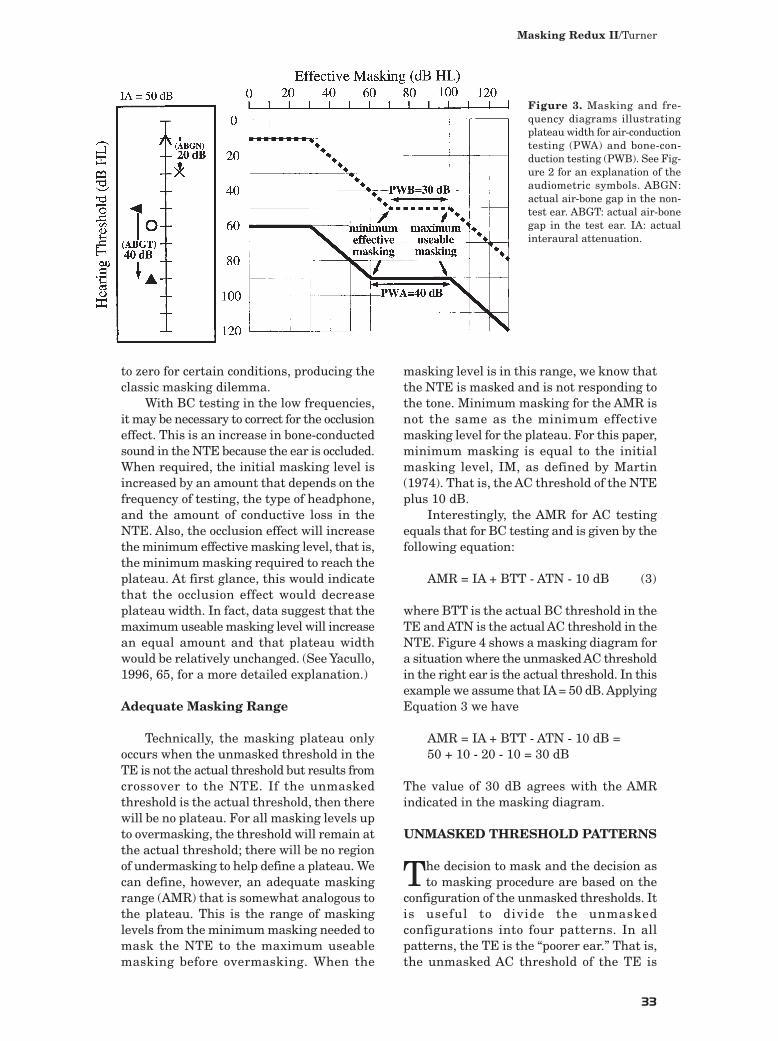
Another interesting thresholdconfiguration is the “Dead” ear (Figure 8).There is no plateau for AC or BC testing.The thresholds must be raised to the limitsof the audiometer. The optimized methodoffers a significant advantage over the plateaumethod. As shown in the figure, the optimizedmethod requires two masking levels to raisethe AC and BC thresholds beyondaudiometric limits, 60 dB for BC testing and120 dB for AC testing. The plateau method
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
36
Figure 7. Masking and fre-quency diagrams for a“worst case” unilateral pat-tern. Test ear has conduc-tive loss, and actual air-bone gap equals the actualinteraural attenuation (40dB). See Figure 2 for anexplanation of the audio-metric symbols. A1: initialmasking level for air-con-duction testing using theoptimized method. B1: Ini-tial masking level for bone-conduction testing usingthe optimized method. IA:actual interaural attenua-tion. IM: initial maskinglevel for the plateaumethod, either air- or bone-conduction testing.
90305 Cassidy text 2/12/04 10:23 AM Page 36
Masking Redux II/Turner
37
requires seven levels for AC testing and eightfor BC testing.
The final threshold configuration for theunilateral pattern is shown in Figure 9. Inthis example, the TE has a mixed loss. TheABG in the TE reduces AC and BC plateauwidth (compare to Figure 6). The optimizedmethod requires two masking levels toidentify the AC and BC plateaus. The plateau
method requires four levels for AC testing andsix for BC testing.
With the unilateral pattern, plateauwidth and the AMR are relatively large evenfor the worst case threshold configuration.Both masking procedures placed the lastmasker in the plateau, or AMR, and identifiedthe correct threshold. For all configurations,the optimized method required fewer masking
Figure 9. Masking and fre-quency diagrams for a unilateral pattern with amixed hearing loss in thetest ear. See Figure 2 foran explanation of the audio-metric symbols. A1: initialmasking level for air-con-duction testing using theoptimized method; A2:additional masking levelfor air-conduction testingusing the optimizedmethod. B1: initial maskinglevel for bone-conductiontesting using the optimizedmethod; B2: additionalmasking level for bone-con-duction testing using theoptimized method. IA:actual interaural attenua-tion. IM: initial maskinglevel for the plateaumethod, either air- or bone-conduction testing.
Figure 8. Masking and fre-quency diagrams for a uni-lateral pattern with a“Dead” test ear. Note thatthere is no plateau or ade-quate masking range. SeeFigure 2 for an explanationof the audiometric symbols.A1: initial masking level forair-conduction testing usingthe optimized method; A2:additional masking levelfor air-conduction testingusing the optimizedmethod. B1: initial maskinglevel for bone-conductiontesting using the optimizedmethod; B2: additionalmasking level for bone-con-duction testing using theoptimized method. IA:actual interaural attenua-tion. IM: initial maskinglevel for the plateaumethod, either air- or bone-conduction testing.
90305 Cassidy text 2/12/04 10:23 AM Page 37
levels than the plateau method, significantlyfewer for some threshold configurations.
Bilateral Pattern
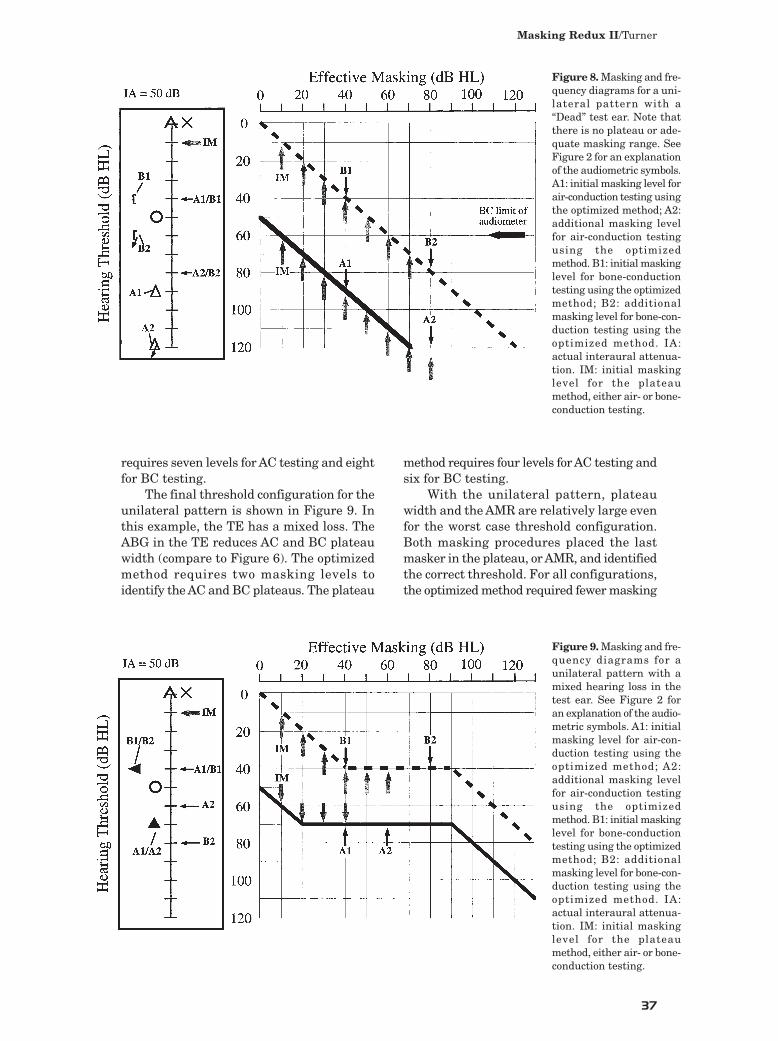
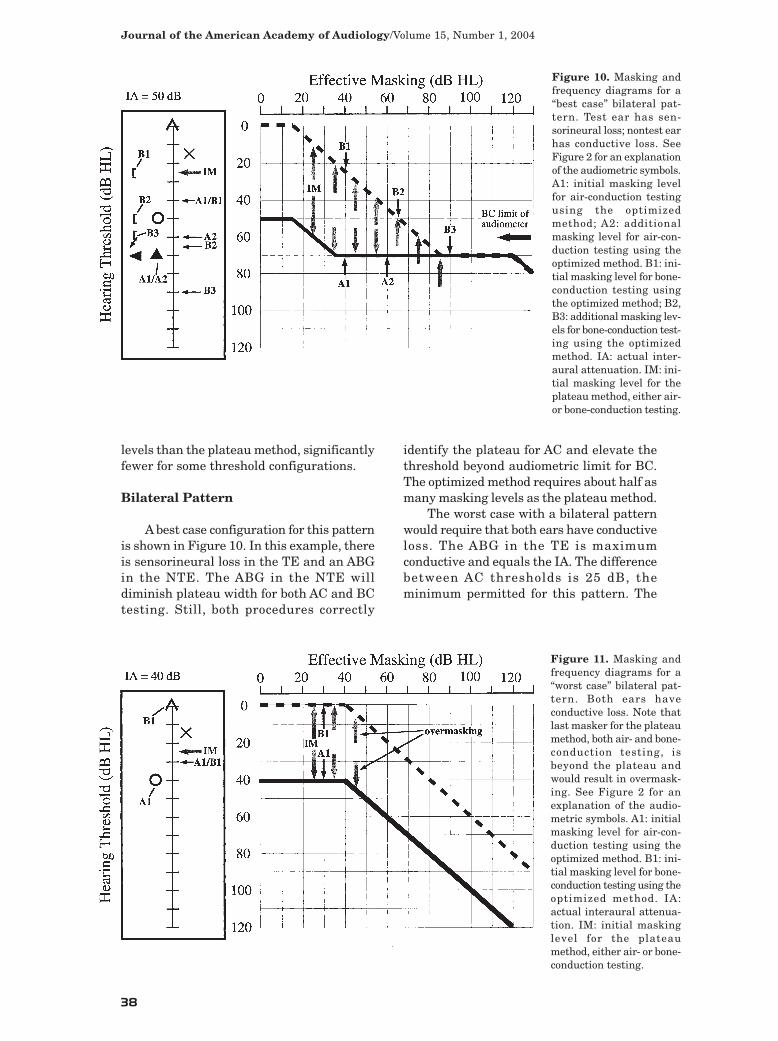
A best case configuration for this patternis shown in Figure 10. In this example, thereis sensorineural loss in the TE and an ABGin the NTE. The ABG in the NTE willdiminish plateau width for both AC and BCtesting. Still, both procedures correctly
identify the plateau for AC and elevate thethreshold beyond audiometric limit for BC.The optimized method requires about half asmany masking levels as the plateau method.
The worst case with a bilateral patternwould require that both ears have conductiveloss. The ABG in the TE is maximumconductive and equals the IA. The differencebetween AC thresholds is 25 dB, theminimum permitted for this pattern. The
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
38
Figure 10. Masking andfrequency diagrams for a“best case” bilateral pat-tern. Test ear has sen-sorineural loss; nontest earhas conductive loss. SeeFigure 2 for an explanationof the audiometric symbols.A1: initial masking levelfor air-conduction testingusing the optimizedmethod; A2: additionalmasking level for air-con-duction testing using theoptimized method. B1: ini-tial masking level for bone-conduction testing usingthe optimized method; B2,B3: additional masking lev-els for bone-conduction test-ing using the optimizedmethod. IA: actual inter-aural attenuation. IM: ini-tial masking level for theplateau method, either air-or bone-conduction testing.
Figure 11. Masking andfrequency diagrams for a“worst case” bilateral pat-tern. Both ears have conductive loss. Note thatlast masker for the plateaumethod, both air- and bone-conduction testing, isbeyond the plateau andwould result in overmask-ing. See Figure 2 for anexplanation of the audio-metric symbols. A1: initialmasking level for air-con-duction testing using theoptimized method. B1: ini-tial masking level for bone-conduction testing using theoptimized method. IA:actual interaural attenua-tion. IM: initial maskinglevel for the plateaumethod, either air- or bone-conduction testing.
90305 Cassidy text 2/12/04 10:23 AM Page 38
calculated minimum plateau width is 25 dB,and the AMR is 15 dB.
A worst case configuration is shown inFigure 11. Note that the initial masking levelfor the optimized method (A1, B1) is only 5dB greater than for the plateau method (IM).Theoretically, only one masking level shouldbe required with the optimized method. The
initial masking level (A1, B1) is 15 dB abovethe unmasked AC threshold of the NTE andshould be sufficient to mask the NTE. Asdiscussed above, an additional masker couldbe used to confirm the plateau. With thebilateral pattern, it would be best to use a 5dB masker increase. In addition, a secondlevel may be needed if threshold shifts dueto test variability or central masking. By ourdefinition, the plateau method requires threelevels, 10 dB apart, to establish plateau orAMR. In this example, the third maskinglevel for the plateau method would result inovermasking.
With the bilateral pattern, plateau widthand AMR tend to be smaller than in theunilateral pattern because of a possibleconductive loss in the NTE. Even so, theoptimized method correctly identifies theplateau and should yield valid measures ofthreshold. Consistently, the optimized methodrequired fewer masking levels than theplateau method, but the advantage is not asgreat as with the unilateral pattern. Thesuccess of the plateau method depends on theparticular definition. As shown in Figure 11,if the masking level must be increased twicein 10 dB increments to identify the plateauor AMR, then overmasking can occur in somethreshold configurations. The masking levelsmay pass through the plateau intoovermasking. This is not a fatal flaw butcould result in some confusion.
Masking Redux II/Turner
39
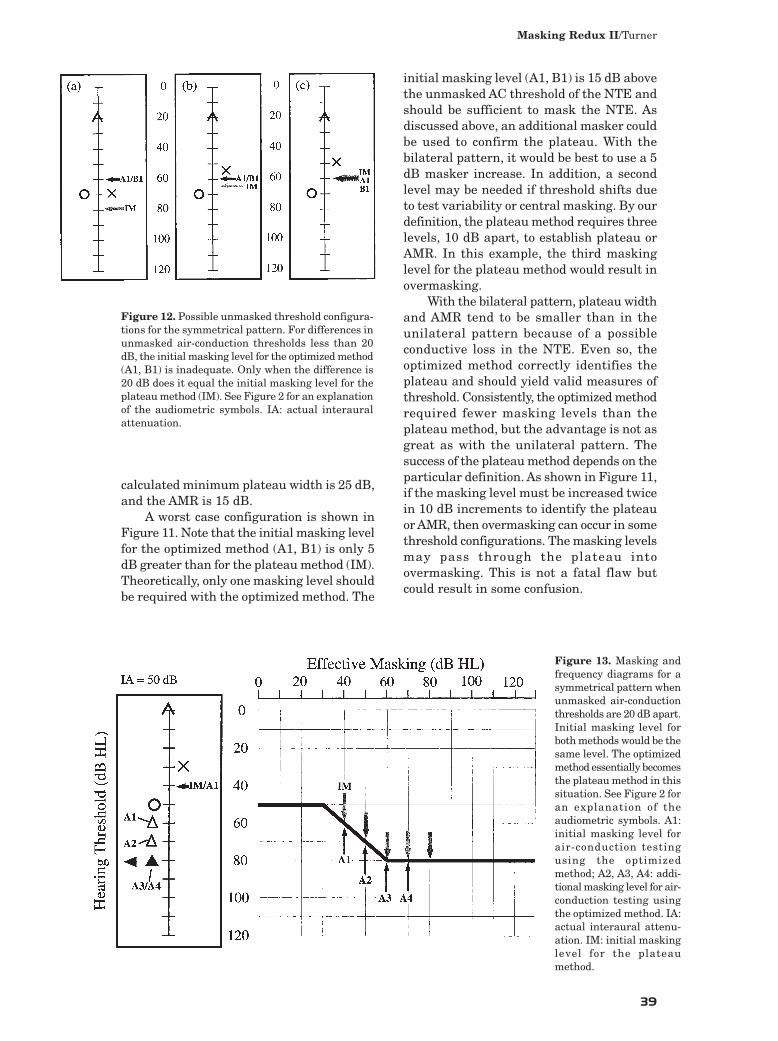
Figure 12. Possible unmasked threshold configura-tions for the symmetrical pattern. For differences inunmasked air-conduction thresholds less than 20dB, the initial masking level for the optimized method(A1, B1) is inadequate. Only when the difference is20 dB does it equal the initial masking level for theplateau method (IM). See Figure 2 for an explanationof the audiometric symbols. IA: actual interauralattenuation.
Figure 13. Masking andfrequency diagrams for asymmetrical pattern whenunmasked air-conductionthresholds are 20 dB apart.Initial masking level forboth methods would be thesame level. The optimizedmethod essentially becomesthe plateau method in thissituation. See Figure 2 foran explanation of theaudiometric symbols. A1:initial masking level forair-conduction testingusing the optimizedmethod; A2, A3, A4: addi-tional masking level for air-conduction testing usingthe optimized method. IA:actual interaural attenu-ation. IM: initial maskinglevel for the plateaumethod.
90305 Cassidy text 2/12/04 10:23 AM Page 39

Symmetrical Pattern
With the symmetrical pattern, thedifference in unmasked AC thresholds mustbe less than 25 dB. Figure 12 shows threeunmasked patterns that meet the definitionof a symmetrical pattern. In Figure 12a, theunmasked AC thresholds are equal (70 dBHL). The optimized method would specifyan initial masking level (A1, B1) at 60 dB HL.This is below the threshold of the NTE andobviously would not mask the NTE. Theoptimized method could not be used. Theplateau method specifies an initial maskinglevel (IM) of 80 dB HL. This level should
mask the NTE, although overmasking is apossibility. In Figure 12b, the unmasked ACthresholds differ by 15 dB. The initialmasking level (A1, B1) is only 5 dB above thelevel of the unmasked AC threshold of theNTE. We could not be certain that this levelwould provide adequate masking. Again, theoptimized method should not be used. Thus,as the difference between unmasked ACthresholds varies from 0 dB to 15 dB, theinitial masking level (A1, B1) of the optimizedmethod may not be sufficient to ensureadequate masking. An initial masking levelof at least 10 dB above the unmasked AC
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
40
Figure 14. Masking andfrequency diagrams for asymmetrical pattern whenplateau width is only 10dB. With 10 dB maskersteps, the masking levelsfor the plateau method canfail to clearly identify theplateau. See Figure 2 foran explanation of theaudiometric symbols. IA:actual interaural attenua-tion. IM: initial maskinglevel for the plateaumethod.
Figure 15. Masking andfrequency diagrams for theclassic masking dilemma.Hearing loss is bilateralconductive, and the air-bone gaps (40 dB) equal theactual interaural attenua-tion (IA). There is noplateau or adequate mask-ing range so that even theinitial masking level (IM)causes overmasking. SeeFigure 2 for an explanationof the audiometric symbols.
90305 Cassidy text 2/12/04 10:23 AM Page 40

threshold of the NTE, as specified by theplateau method, should be used.
In Figure 12c, the unmasked AC thresholdsdiffer by 20 dB, the maximum for thesymmetrical pattern. In this case, the initialmasking level (A1) for the optimized method isat the same level (60 dB HL) as the initialmasking level (IM) for the plateau method.When this occurs, the optimized methodessentially becomes the plateau method. Bothprocedures use the same initial masking leveland would theoretically increase the maskinglevel in 10 dB steps. This is illustrated by theexample in Figure 13. Note that the maskinglevels are the same for both masking methods,although the optimized method maytheoretically require one fewer masking level.
These results suggest that for asymmetrical pattern the optimized methodshould not be used but that the plateaumethod may be an acceptable maskingprocedure. However, the plateau method asdefined for this paper may not always beappropriate. In particular, the use of 10 dBmasker steps may not be adequate to definea small plateau or AMR. This limitation isillustrated in Figure 14, where the 10 dBsteps cause the masker to pass through theplateau without the plateau being evident. Abetter solution would be to use the plateaumethod with 5 dB steps. The small step sizeprovides the resolution needed to define asmall plateau or AMR.
With a symmetrical pattern, there is thepotential for the plateau or AMR to be quitesmall. That is the basis for recommending a5 dB masker step. Just because the plateau
can be small, however, does not mean that ithas to be small. If the IA is much larger thanthe actual ABGs, then the plateau or AMRcould be of reasonable size. In this situation,using a 5 dB step would be inefficient. Areasonable option would be to test with themore traditional 10 dB step. In manysituations, this may be sufficient to identifythe plateau and, thus, save time relative tothe use of 5 dB steps. If no plateau isidentified with 10 dB steps, then it isnecessary to retest with 5 dB steps.
Consider the worst case situation shownin Figure 15. Both ears have maximumconductive loss; that is, the actual ABG in bothears equals the MIA. In this situation, thereis no plateau or AMR. This is the classicmasking dilemma. The initial masker (IM)will overmask and even using the plateaumethod with 5 dB masker steps will not identifya plateau. However, masking should always beattempted with the symmetrical pattern evenif the unmasked thresholds suggest thepossibility of a masking dilemma. If the IA isgreater than the MIA, it may be possible todefine a plateau or AMR, as in Figure 16. Inthis example, the IA is 20 dB greater than theMIA, resulting in an AMR of 10 dB. This couldbe identified using 5 dB masker steps.
Bone-Only Pattern
In this pattern, masking is required onlyfor BC thresholds, never for AC thresholds foreither ear. The strategy developed for theother patterns will work for this pattern. Ifthe AC thresholds differ by more than 20
Masking Redux II/Turner
41
Figure 16. Masking andfrequency diagrams for asymmetrical pattern thatappears to be a maskingdilemma, but is not. Theair-bone gaps (40 dB) areless than the actual inter-aural attenuation (60 dB).There is a small adequatemasking range (AMR) thatcan be identified using 5dB masker steps. See Fig-ure 2 for an explanation ofthe audiometric symbols.IA: actual interaural atten-uation. IM: initial maskinglevel for the plateaumethod, either air- or bone-conduction testing.
90305 Cassidy text 2/12/04 10:23 AM Page 41

dB, the optimized method should be used.Otherwise, use the plateau method with 5 or10 dB steps, as discussed above. In thispattern, masking is required only for BCthresholds because the apparent ABG in bothears is less than the MIA. This means thatthe apparent ABG will always be smallerthan the IA. The plateau or AMR for thispattern will tend to be larger than for thesymmetrical pattern, so there may be moresuccess using 10 dB masker steps.
RELATED ISSUES
Reestablishing Threshold
Both the plateau method and theoptimized method require that thresholdsbe reestablished. As discussed in the firstpaper, there are two techniques that can beused. The traditional procedure is the up-down search for threshold. An alternatestrategy is the “single-tone” procedure inwhich the tone is presented once at eachmasking level. If there is a response to thetone, the tone is considered to be at thresholdat that masking level, and the masking levelis increased. If there is no response, then thetone is increased in 5 or 10 dB steps andpresented once at each level until there is aresponse. This response indicates thethreshold at that masking level. If this single-tone procedure is used to reestablish
threshold and identify the plateau, then thethreshold in the plateau, which is the actualthreshold of the ear, should be measuredusing the more accurate up-down procedure.
High Masking Levels
There is one caution when using theoptimized method. In certain situations, themethod can specify a masking level that isextremely high. An example is shown in Figure17. The left ear is normal, and the right earhas a profound sensorineural loss. The secondmasker (A2) is in the plateau, but the methodspecifies a third masker (A3) at 105 dB HL toconfirm the plateau. It would be undesirableto subject a normal ear to this level of masking,and it is not necessary to identify the plateau.Once a relatively high level is reached, forexample, greater than 80 dB HL, it would bebetter to increase the masker in smaller stepsof 5 dB or 10 dB (A3’) until the plateau isidentified or the masked threshold reachesthe limit of the audiometer.
A more likely situation is shown in Figure18 for BC testing. The left ear is normal, andthe right ear has a moderate sensorineuralloss. It has been determined that the rightunmasked AC threshold is the actualthreshold. A masked BC threshold is requiredbecause the apparent ABG is greater than 10dB. The initial masking level (B1) elevates thethreshold, but the plateau has not beenidentified. The method specifies a second
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
42
Figure 17. Masking andfrequency diagrams for asituation where the opti-mized method specifies ahigh masking level (A3) ina normal ear. The plateaucan be identified usingsmaller steps, for example,5 dB to 10 dB, as illustratedby the dashed arrow (A3’).See Figure 2 for an expla-nation of the audiometricsymbols. A1: initial mask-ing level for air-conductiontesting using the optimizedmethod; A2, A3: additionalmasking levels for air-con-duction testing using theoptimized method. IA:actual interaural attenua-tion.
90305 Cassidy text 2/12/04 10:23 AM Page 42
Masking Redux II/Turner
43
masker at 90 dB HL (B2). This level could beuncomfortable to a normal ear and isunnecessary. A smaller masking level increase(B2’), 20 dB in this case, would be adequateto raise the masked threshold to the ACthreshold, which is sufficient since BCthresholds should not, in theory, be poorerthan AC thresholds. In this example, hadthe actual AC and BC thresholds been poorer,for example, 80 dB HL, it would only benecessary to demonstrate no BC response atthe BC limit of the audiometer. Again asmaller masking level increase could be used.
Masked Thresholds in the Better Ear
The four patterns used to evaluate thetwo masking methods all assume that the TEis the poorer ear. For AC testing, it is seldomnecessary to obtain masked thresholds in
the better ear. The only possible exceptionoccurs with the Symmetrical Pattern whenthe unmasked AC thresholds are similar,and it is difficult to be certain as to which earis actually the poorer ear. In this situation,it may be necessary to test both ears. WithBC testing, testing the better ear is morecommon, particularly with the bone-onlypattern. If it is necessary to measure maskedthresholds in the better ear, then whichmasking method should be used? Theoptimized method is never appropriate whentesting the better ear even if the unmaskedAC thresholds differ by more than 20 dB. Inthis situation, the unmasked AC threshold ofthe TE would be better than the unmaskedAC threshold of the NTE. A masking level set10 dB below the unmasked AC threshold ofthe test (better) ear would be below thethreshold of the nontest (poorer) ear and
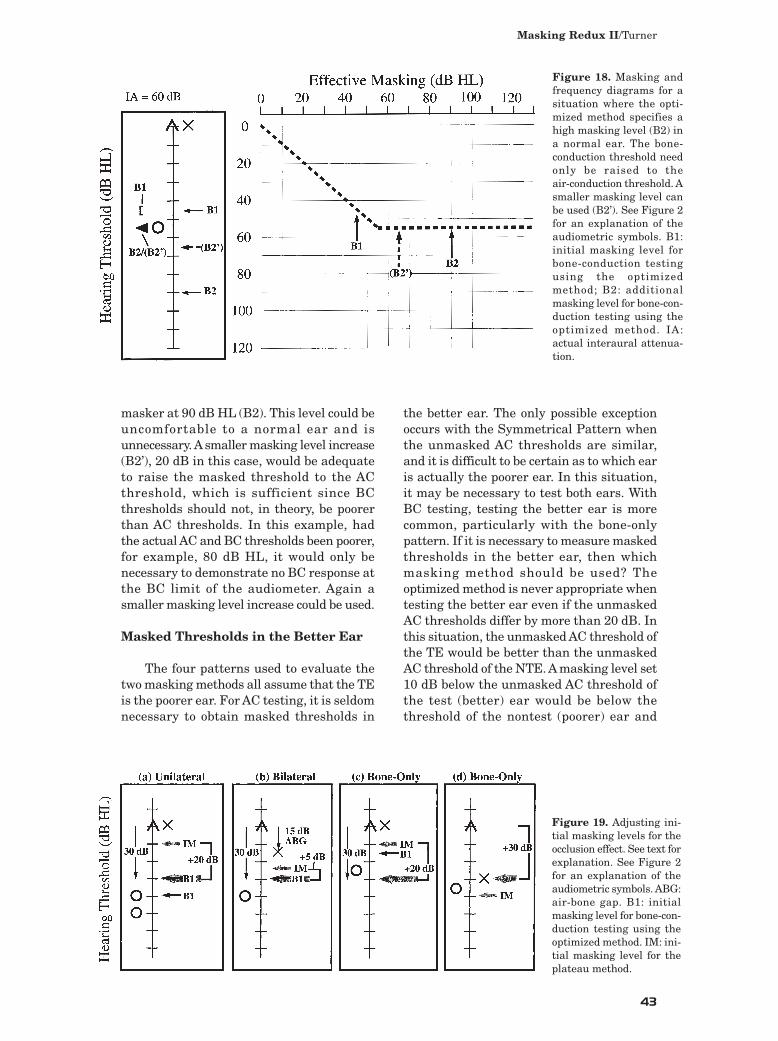
Figure 18. Masking andfrequency diagrams for asituation where the opti-mized method specifies ahigh masking level (B2) ina normal ear. The bone-conduction threshold needonly be raised to the air-conduction threshold. Asmaller masking level canbe used (B2’). See Figure 2for an explanation of theaudiometric symbols. B1:initial masking level forbone-conduction testingusing the optimizedmethod; B2: additionalmasking level for bone-con-duction testing using theoptimized method. IA:actual interaural attenua-tion.
Figure 19. Adjusting ini-tial masking levels for theocclusion effect. See text forexplanation. See Figure 2for an explanation of theaudiometric symbols. ABG:air-bone gap. B1: initialmasking level for bone-con-duction testing using theoptimized method. IM: ini-tial masking level for theplateau method.
90305 Cassidy text 2/12/04 10:23 AM Page 43

would not be audible. Overmasking is alwaysa potential problem when testing the betterear. The safest approach is to use the plateaumethod with 5 dB masker steps.
Occlusion Effect
When using the plateau method andtesting BC thresholds in the lowerfrequencies, it is necessary to increase themasking level to compensate for the occlusioneffect. A variety of values have been proposedfor supra-aural phones. Yacullo (1996, 63)recommends correction factors of 30 dB for250 Hz, 20 dB for 500 Hz, 10 dB for 1000 Hz,and no correction for higher frequencies.These values are in addition to the usual 10dB that is added to the AC threshold of theNTE. Roeser and Clark (2000) recommend 20dB, 15 dB, and 5 dB. Goldstein and Newman(1994) recommend 15 dB, 15 dB, and 10 dB.The values for insert phones, when properlyinserted, are significantly smaller than forsupra-aural phones. For example, Yacullo(1996, 128) recommends 10 dB at 250 Hzand no correction at any other frequency.
Consider the unilateral pattern in Figure19a. This is a worst case in that the apparentABG equals the MIA (40 dB), the smallestpossible for this pattern. We are using theplateau method and testing BC in the lowfrequencies. A correction factor of 20 dB isadded to the initial masking level (IM)resulting in a masking level 30 dB greaterthan the unmasked BC threshold. If we wereto use the optimized method, the initialmasking level (B1) would be 10 dB below theAC threshold of the NTE, which would alsobe 30 greater than the unmasked BCthreshold. Thus, the optimized methodautomatically adjusts for a correction factor upto at least 20 dB. If the apparent ABG is biggerthan 40 dB (shaded circle), then the initialmasking level (shaded B1) would compensatefor an even larger correction factor.
The situation for a bilateral pattern isshown in Figure 19b. In this case, there is anapparent ABG of 15 dB in the NTE. Aconductive hearing loss reduces the occlusioneffect and essentially eliminates it when theABG reaches 20 dB (Martin et al, 1974). Thus,the correction factor is reduced by the ABG.If the loss in the NTE is conductive, then the20 dB correction factor would be reduced by15 dB. It would only be necessary to add 5 dBto the initial masking level (IM). This results
in a masking level 30 dB above the unmaskedBC threshold. If we used the optimizedmethod, the initial masking level (B1) wouldbe placed at the same level, automaticallycompensating for the correction factor.
What if the loss in the NTE issensorineural? The unmasked BC thresholdcould not be due to crossover to the NTE andwould represent the actual BC threshold ofthe TE. Even if a tone at the BC threshold ofthe TE (assume 10 dB HL) was increased 20dB by the occlusion effect, it would arrive atthe NTE (at 30 dB HL), only 5 dB greaterthan the actual BC threshold of the NTE (25dB HL). Increasing the initial masking level5 dB (from 35 dB HL to 40 dB HL) would besufficient to keep the masker 10 dB greaterthan the signal in the NTE. This places themasker at the same level as the initialmasking level (B1) for the optimized method.Thus, it does not matter if the apparent ABGis actually conductive or sensorineural; theoptimized method would automaticallycompensate for a correction factor up to 20 dB.
The symmetrical pattern is not shown inFigure 19. By definition, the symmetricalpattern requires an apparent ABG of at least20 dB. This eliminates the need to adjust forany correction factor up to 20 dB. When usingthe plateau method with the symmetricalpattern, no modification to the initial maskinglevel is required.
There is a potential problem with thebone-only pattern. The optimized methodwould be used with the thresholdconfiguration in Figure 19c. The initialmasking level (B1) would be significantlybelow the required masking level when usinga 20 dB correction factor. Note, however, thatthe required masking level is 30 dB greaterthan the unmasked BC threshold, as wasthe case with the unilateral and bilateralpatterns (Figures 19a, 19b). One strategywould be to always place the initial maskinglevel at a level 30 dB greater than theunmasked BC threshold. This level wouldnever cause overmasking because theminimum interaural attenuation is 40 dBfor supra-aural headphones. Sometimes, therequired initial masking level (IM) may begreater than 30 dB above the unmasked BCthreshold. This can occur if the unmasked ACthresholds are close and the plateau methodis being used (Figure 19d). In this situation,the greater masking level specified by theplateau method should be used.
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
44
90305 Cassidy text 2/12/04 10:23 AM Page 44

MASKING PROTOCOL
Based on the evaluations of the optimizedand plateau methods, a protocol can be
constructed that is suitable for all maskingsituations. The optimized method should beused when the unmasked thresholds meet therequirements for a unilateral or a bilateralpattern. The key requirement is that theunmasked AC thresholds differ by at least 25dB. For audiometric configurationscorresponding to these two patterns, theoptimized method correctly placed the lastmasking level in the plateau (or AMR) andyielded the actual threshold. The traditionplateau method, as defined for this paper,used 10 dB masker steps and required twoincreases in masking level (20 dB range) todefine a plateau. With this definition, theplateau method could produce overmaskingfor certain audiometric configurations. Theoptimized method never required moremasking levels than the plateau method andfrequently required significantly fewer levels.In general, this advantage is greater for theunilateral pattern than the bilateral pattern.
The optimized method is neverappropriate for the symmetrical patternbecause unmasked AC thresholds, bydefinition, differ by less than 25 dB. With thispattern, the plateau or AMR can be small. Theplateau method should be used with a 5 dBmasker step to help identify a small plateau.An alternative strategy is to test first using10 dB masker steps and retest with 5 dBsteps if no plateau or AMR can be identified.There is still the possibility that maskingwill not be successful, even with 5 dB steps,in the case of the classic masking dilemma.
The optimized method can be used withthe bone-only pattern when unmasked ACthresholds differ by more than 20 dB. When thedifference is 20 dB or less, the plateau methodshould be used. Either use 5 dB masker steps ortest first with 10 dB steps and retest with 5 dBsteps if a plateau or an AMR cannot be identified.
If we use correction factors up to 20 dBfor the occlusion effect, as specified by Roeserand Clark or Goldstein and Newman, thenlittle modification to procedure is needed.For properly inserted insert phones, thecorrection factor is only 10 dB at 250 Hz,and, again, little modification is needed. Forcorrection factors up to 20 dB, the optimizedmethod automatically compensates for theunilateral and bilateral patterns. There is no
need to make any adjustment when using theplateau method with the symmetricalpattern. The only exception would be thebone-only pattern. The initial masking levelspecified by the protocol may not always beadequate. A simple solution is to use theinitial masking level specified by the protocol,or 30 dB greater than the unmasked BCthreshold, whichever is larger. There isanother advantage to setting the initialmasking level no less than 30 dB greaterthan the unmasked BC threshold, even in thehigher frequencies where the occlusion effectis not an issue. The higher masking levelwill help reduce testing time.
If a correction factor of 30 dB is being usedfor 250 Hz, as recommended by Yacullo, thereis a solution. When testing 250 Hz, always setthe initial masking level at least 40 dB greaterthan the unmasked BC threshold, althoughthis may increase the possibility ofovermasking. If the masking method beingused specifies a larger value, use that.
Recommended Protocol
The following protocol can be used in allmasking situations with supra-aural or insertphones.
When testing the poorer ear:
• If the unmasked AC thresholds differby more than 20 dB, then use the optimized masking method.
• If the difference in unmasked AC thresholds is 20 dB or less, then there are two options:1. Use the plateau method with 5
dB masker stepsor
2. Initially use the plateau methodwith 10 dB steps. If no plateauor AMR can be identified, thenretest using 5 dB steps.
When testing bone-conductionthresholds:
• Always set the initial masking level at least 30 dB greater than theunmasked BC threshold. If the masking method being used specifiesa greater value, use that. This strategy automatically compensates
Masking Redux II/Turner
45
90305 Cassidy text 2/12/04 10:23 AM Page 45
for occlusion effect correction factorsup to 20 dB.
When testing the better ear (this isseldom necessary for AC thresholds):
• Use the plateau method with 5 dB masker steps.
Note:
• Thresholds can be reestablished using the traditional up-down search or the single-tone procedure. The single-tone procedure will reduce testing time.
• Try to avoid high masking levels. Occasionally, the optimized methodmay specify a large increase in masking level, and that increase may produce a masker greater than 80 dB HL. When this occurs, consider using smaller increases inmasking level to identify plateau.
REFERENCES
Goldstein B, Newman C. (1994). Clinical masking: adecision making process. In: Katz J, ed. Handbook ofClinical Audiology. Baltimore, MD: Williams andWilkins, 109–131.
Liden G, Nilsson G, Anderson H. (1959). Masking inclinical audiometry. Acta Otolaryngol 50:25–136.
Martin F. (1974). Minimum effective masking levelsin threshold audiometry. J Speech Hear Dis39:280–285.
Martin F, Butler E, Burns P. (1974). Audiometric Bingtest for determination of minimum masking levelsfor bone conduction tests. J Speech Hear Disord39:148–152.
Roeser R, Clark J. (2000). Clinical masking. In: RoeserR, Valente M, Hosford-Dunn H, eds. AudiologyDiagnosis. New York: Thieme, 253–279.
Turner R. (2003). Masking Redux I: an optimizedmasking method. J Am Acad Audiol 15:17–28.
Yacullo W. (1996). Clinical Masking Procedures.Needham Heights, MA: Allyn and Bacon.
Journal of the American Academy of Audiology/Volume 15, Number 1, 2004
46
90305 Cassidy text 2/12/04 10:23 AM Page 46