Embed Size (px)
DESCRIPTION
Citation preview

506 | july 2009 | volume 39 | number 7 | journal of orthopaedic & sports physical therapy
[ RESEARCH REPORT ]
with any residual neuromuscular de-ficiency, may explain why a history ofligament injury is a strong risk factor forsubsequent injury.14,23 Some patients (upto a third) also continue to experiencesignificant symptoms even up to 3 yearsfollowing capsular or extracapsular liga-ment injury,25 and injuries to these liga-ments can contribute to the developmentof osteoarthritis.24
To address the short- and long-termconsequences of capsular and extracapsu-lar ligament injuries, there is a need forsimple interventions that facilitate earlyrecovery (accelerate healing) and/or resultin a better final outcome (augment heal-ing). By accelerating tissue-level healing,the injured tissue may be less susceptibleto reinjury during early rehabilitationand the individual may be able to returnto function quicker. By augmenting tissue-level healing, the final product of the heal-ing process may be enhanced such that thehealed tissue more closely approximatesthat of the native tissue.
Cross-fiber massage (CFM) may be amethod for accelerating and/or augment-ing capsular and extracapsular ligamenthealing. CFM refers to the application ofspecifically directed forces transverse tothe direction of the underlying collagensubstructure in order to induce physi-ological and/or structural tissue changes.
Ligament injuries account for up to 50% of sporting injuries,6
with the majority being to capsular and extracapsular ligaments(such as the knee and ankle collateral ligaments).11 Injuries tothese ligaments have traditionally been thought to heal in a
straightforward manner; however, preclinical studies have shown thatligament healing occurs by the formation of a reparative scar, rather thanvia regeneration, which leaves a deficiency in mechanical properties atthe completion of healing.7,29 This persistent tissue weakness, combined
1Associate Clinical Professor, Department of Physical Therapy, School of Health and Rehabilitation Sciences, Indiana University, Indianapolis, IN. 2Assistant Professor and Directorof Research, Department of Physical Therapy, School of Health and Rehabilitation Sciences, Indiana University, Indianapolis, IN. This study was supported in part by grants fromthe American Massage Therapy Foundation and TherapyCare Resources, Inc (Indianapolis, IN). The results presented herein represent the conclusions and opinions of the authors.Publication does not necessarily imply endorsement by the grant providers or endorsement of their products by the authors. No commercial party having a direct interest in theresults of the research supporting this article has or will confer a benefit on the authors or any organization with which the authors are associated. The study protocol for animal usewas approved a priori by the Institutional Animal Care and Use Committee at Indiana University. Address correspondence to M. Terry Loghmani, Department of Physical Therapy,School of Health and Rehabilitation Sciences, Indiana University, 1140 W Michigan St CF 326, Indianapolis, IN 46202. E-mail: [email protected].
M. TERRY LOGHMANI, PT, MS¹ PT, PhD²
Instrument-Assisted Cross-Fiber MassageAccelerates Knee Ligament Healing
Controlled laboratory study.
To investigate the effects ofinstrument-assisted cross-fiber massage (IACFM)on tissue-level healing of knee medial collateralligament (MCL) injuries.
Ligament injuries are commonand significant clinical problems for which thereare few established interventions. IACFM repre-sents an intervention that may mediate tissue-levelhealing following ligament injury.
Bilateral knee MCL injuries werecreated in 51 rodents, while 7 rodents weremaintained as ligament-intact, control animals.IACFM was commenced 1 week following injuryand introduced 3 sessions per week for 1 minuteper session. IACFM was introduced unilaterally(IACFM-treated), with the contralateral, injuredMCL serving as an internal control (nontreated).Thirty-one injured animals received 9 IACFMtreatments, while the remaining 20 injured animalsreceived 30 treatments. Ligament biomechani-cal properties and morphology were assessed ateither 4 or 12 weeks postinjury.
IACFM-treated ligaments were 43.1%
stronger (P .05), 39.7% stiffer (P .01), and couldabsorb 57.1% more energy before failure (P .05)than contralateral, injured, nontreated ligaments at4 weeks postinjury. On histological and scanningelectron microscopy assessment, IACFM-treatedligaments appeared to have improved collagenfiber bundle formation and orientation within thescar region than nontreated ligaments. There wereminimal differences between IACFM-treated andcontralateral, nontreated ligaments at 12 weekspostinjury, although IACFM-treated ligaments were15.4% stiffer (P .05).
IACFM-accelerated ligamenthealing, possibly via favorable effects on collagenformation and organization, but had minimal effecton the final outcome of healing. These findings areclinically interesting, as there are few establishedinterventions for ligament injuries, and IACFMis a simple and practical therapy technique. JOrthop Sports Phys Ther 2009;39(7):506-514.doi:10.2519/jospt.2009.2997
biomechanics, complementarytherapies, medial collateral ligament, physicaltherapy, sports medicine

journal of orthopaedic & sports physical therapy | volume 39 | number 7 | july 2009 | 507
tation. Animals had ad libitum access tostandard rat chow and water at all times,and were housed 2 per standard size cage(length, 40 cm; width, 20 cm; height, 20cm). All procedures were approved a pri-ori by The Institutional Animal Care andUse Committee of Indiana University.
Ligament InjuryFifty-one animals underwent surgery onentry to the study to create bilateral kneeMCL injuries of their hindlimbs (injuredanimals). The remaining 7 animalsserved as age-matched, ligament-intactcage controls and were not operated on(control animals). Following a preopera-tive subcutaneous dose (0.05 mg/kg) ofbuprenorphine hydrochloride analgesia(Buprenex; Reckitt & Colman Pharma-ceuticals Ltd, Richmond, VA), surgicalanesthesia was achieved using a mixtureof ketamine (60-80 mg/kg) (Ketaset;Fort Dodge Animal Health, Fort Dodge,IA) and xylazine (7.5 mg/kg) (Sedazine;Fort Dodge Animal Health), introducedintraperitoneally. Using a sterile tech-nique, a 5-mm longitudinal incision wasmade over 1 knee’s medial joint line, andthe MCL sharply transected at the jointline using a size-11 scalpel blade. This re-sulted in complete disruption of the MCLat its midsubstance and transverse to theunderlying collagen fiber alignment. Noligament material was removed, and theligament ends were juxtaposed but notsutured prior to closing of the skin inci-sion with a single subcuticular absorb-able suture. The procedure was repeatedon the contralateral knee to create bilat-eral injuries. All animals demonstratednormal, symmetrical hindlimb use uponrecovery from surgery and were allowednormal cage activity (without access toexercise wheels) for the duration of thestudy.
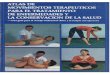
InterventionIACFM was performed using a rigid toolfabricated from stainless steel (GT6; Gras-ton Technique, TherapyCare Resources,Indianapolis, IN). The GT6 instrumentwas used because it is designed to apply
force through its tip to small structures,such as finger collateral ligaments in hu-mans (in the present study, rat knee-sizeligaments) ( ). IACFM was initiated1 week postoperatively (postinjury) to al-low the initial inflammatory response/phase of ligament healing to subside. Thisinitial delay in the introduction of IACFMis consistent with its suggested clinicaluse following an acute injury. IACFM wasadministered with the animals under iso-flurane anesthesia (3% at 1.5 L/min forinitial knockdown in a plastic container,and 1.5% at 1.5 L/min via a face mask formaintenance of anesthesia). Approximate-ly 250 to 300 g of instrument downwardforce was applied during treatment. This
It differs from other massage techniquesin that there is little motion between thetherapist’s contact and the patient’s skin.Instead, CFM involves moving the skinand subcutaneous tissues over deeper con-nective tissues to exert controlled mechan-ical forces on the latter. As the reparativecells (fibroblasts) responsible for produc-ing collagen and forming a scar followingligament injury are mechanosensitive,4,26
it is theorized that CFM facilitates matrixproduction and the restoration of tissue-level mechanical properties.
An addition to the practice of CFMhas been the use of rigid instruments,with the resultant technique referred toas instrument-assisted CFM (IACFM).IACFM appears to be effective in promot-ing tissue remodeling, with Davidson et al5
and Gehlsen et al8 having found increasedfibroblast recruitment and activation in ananimal model of Achilles tendon injury.Results of clinical pilot studies also suggestthat IACFM reduces symptoms in individ-uals with carpal tunnel syndrome, patellartendinopathy, and chronic ankle pain.1,17,30
Based on the hypothesized mechanicalmode of action of IACFM and preliminaryevidence demonstrating its potential effi-cacy, the aim of this study was to examinethe short- and long-term effects of IACFMon tissue-level healing of knee medialcollateral ligament (MCL) injuries in anestablished animal model. The primaryvariable of interest was ligament mechani-cal properties, as the ultimate outcome ofany healing process in a load-bearing tis-sue (such as a ligament) is the restorationof mechanical properties. The secondaryvariable of interest was ligament morphol-ogy, as this may explain differences in tis-sue mechanical properties.
Animals
Fifty-eight 6-month-old, virgin,female Sprague-Dawley rats (bodymass, 280-300 g) were purchased
from Harlan Sprague-Dawley, Inc (In-dianapolis, IN) and acclimated for aminimum of 7 days prior to experimen-
Instrument-assisted cross-fiber massage(IACFM) intervention. (A) The rigid Graston TechniqueGT6 tool fabricated from stainless steel has a taperedtip,* which permits treatment of small structures.IACFM of a (B) human finger, and (C) similar-sizerodent knee joint medial collateral ligament using theGT6 tool. Arrows indicate the direction of movement/force application perpendicular to the collagensubstructure of the ligament.

508 | july 2009 | volume 39 | number 7 | journal of orthopaedic & sports physical therapy
[ RESEARCH REPORT ]force is equivalent to that previously usedto demonstrate benefits of IACFM on in-jured rat Achilles tendons,8 and was deter-mined by using the massage instrumenton a force plate, with kinesthetically simi-lar pressure to that which would be usedclinically to treat a ligament of comparablesize at an equivalent tissue depth (eg, col-lateral ligament of a human interphalan-geal joint). Thirty-one injured animalswere treated 3 times per week for 3 weeks(total treatments, 9), while the other 20injured animals were treated 3 times perweek for 10 weeks (total treatments, 30).The number of treatments in the latteranimals is more than would typically beintroduced in a clinical setting; however,these were implemented to maximize thepotential of finding any long-term benefitof IACFM. IACFM was applied to the leftMCL in injured animals for 1 minute persession (IACFM-treated). This treatmentduration was based on the recommendedclinical use of IACFM for the treatment ofisolated tissue lesions3 and evidence fromprevious preclinical studies demonstrat-ing the efficacy of short-duration IACFMinterventions.5,8 The contralateral injuredMCL in these animals served as an inter-nal control and did not receive IACFM(nontreated). The 7 control animals werenot treated with IACFM.
Animals were euthanized postinjury ateither 4 weeks (all animals treated for 9sessions [n = 31] and 2 control animals)or 12 weeks (all animals treated for 30sessions [n = 20] and 5 control animals).Animals euthanized at 4 weeks had bothhindlimbs harvested and prepared formechanical testing (injured animals, n= 18), scanning electron microscopy (in-jured, n = 11; control animals, n = 2), orhistological assessment (injured animals,n = 2). Animals euthanized at 12 weekshad both hindlimbs removed and pre-pared for mechanical testing (injured, n =17; control animals, n = 4) or histologicalassessment (injured, n = 3; control ani-mals, n = 1).
Ligament mechanical properties wereassessed as previously described.27,28
Hindlimbs destined for mechanical test-ing were initially stored at –80°C, withthe knee tissues intact. Postmortem stor-age of ligaments by freezing does notinfluence their mechanical properties.33
On the day of mechanical testing, thehindlimbs were allowed to thaw to roomtemperature in phosphate-buffered sa-line (PBS). Femoral-MCL-tibia (FMT)complexes were prepared by dissect-ing clear extraneous tissue (includingthe joint capsule and adherent medialmeniscus), while keeping the MCL andits insertion sites hydrated with PBS.The femoral and tibial insertions of theMCL were left intact, and the proximaltibia growth plate was removed to permitmore space within the knee joint duringtesting. MCL thickness and width weremeasured optically at the knee joint line,and MCL area estimated using an ellipti-cal geometry.20 Each FMT complex wasplaced in a customized testing jig, withthe knee joint positioned in 70° flexion,for MCL testing. This position appears toload all ligament fibers simultaneously.20
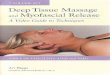
The femoral and tibial portions wereembedded in Wood’s low-melting-pointmetal (bismuth alloy LMA-117; SmallParts, Inc, Miami Lakes, FL) for fixation.The jig was coupled to an electromag-netic material testing device (TestBench200 N ELF LM-1; EnduraTEC SystemsGroup, Bose Corp, Minnetonka, MN),equipped with a 50-N load cell (2A). This system possesses a force anddisplacement resolution of 0.01 N and0.001 mm, respectively. A preload of 0.05N was applied and the ligaments werepreconditioned by cyclically loading at 1Hz for 10 cycles to 1% strain to reducethe effect of deep freezing on low-loadmechanical properties.33 The ligamentswere unloaded and allowed to recover for1.5 minutes, while being kept moist withPBS. Following tissue recovery, ligamentswere again preloaded (0.05 N) and pulledto tensile failure in displacement controlat a rate of 0.8 mm/s (~10%/s). Force and
displacement data were collected at 100Hz, and the mechanical properties of ul-timate force (N), stiffness (N/mm), andenergy to failure (mJ) obtained from theforce-displacement curves ( ).
Immediately after harvest, specimens forscanning electron microscopy were placedin a custom limb frame that held the kneepositioned in 70° flexion. The MCL wasexposed and drip fixed for 1 hour with2.5% glutaraldehyde in 0.1 mol sodiumcacodylate buffer (pH 7.4) (Electron Mi-croscopy Services, Hatfield, PA). Afterdrip fixation, the MCLs were removedusing a microsurgical scalpel, with thefemoral insertion marked by an angled
0
5
10
15
20
25
30
Displacement (mm)
Forc
e (N
)
35
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8
Ultimate force Stiffness
Energy to failure
70°
Femur
Medialcollateralligament
TibiaWood’s lowmelting-pointmetal
A
B
Tensile mechanical testing of rat kneemedial collateral ligament (MCL). (A) Representativeimage of the setup for testing. Femur-MCL-tibiacomplexes were placed in fixtures that supported("cupped") the distal femur and proximal tibia toprevent bone slippage, and fixed in place usingWood's low-melting-point metal. The knee jointwas positioned in 70° of flexion for testing. (B)Representative force displacement curve for a ratknee MCL tensile mechanical test. Derived propertiesinclude ultimate force (peak on the curve on they-axis), stiffness (slope of the linear portion of thecurve), and energy absorbed prior to failure (areaunder the curve).

journal of orthopaedic & sports physical therapy | volume 39 | number 7 | july 2009 | 509
plane thin (4 μm) sections were cut us-ing a rotary microtome (Reichert-JungModel 2050; Reichert-Jung, Heidelberg,Germany), mounted onto microscopeslides, and stained with Harris hematoxy-lin and eosin on a linear stainer (ShandonLinistain GLX; Thermo Electron Corp,Waltham, MA). Three sections per speci-men were qualitatively assessed underlight microscopy using a Nikon Optio-phot 2 microscope (Nikon, Inc, GardenCity, NY).
Statistical analyses were performed usingSPSS, Version 16.0 (SPSS Inc, Chicago,IL). All comparisons were 2-tailed, witha level of significance set at 0.05. Un-paired t tests were performed to assesstime (4 versus 12 weeks postinjury) andgroup (injured versus control animals) ef-fects on body mass. IACFM effects wereprincipally determined using paired ttests to compare IACFM-treated and
cut. Any adherent tissue was removedunder a dissecting microscope. Liga-ments were then rinsed twice in bufferedsolution and dehydrated by immersingfor 15 minutes each in fresh solutions of70%, 95%, and 100% ethyl alcohol. Theywere subsequently immersed in liquid ni-trogen, placed on precooled microscopeslides, and fractured under a dissectingmicroscope in the sagittal plane from thefemoral to tibial end using one half of aprecooled, double-edged stainless steelrazor blade (Electron Microscopy Scienc-es, Hatfield, PA). The ligament sampleswere then critical point dried (Samdrimodel 780A; Tousimis Research Corp,Rockville, MA), mounted on 10-mmscanning electron microscopy specimenmount blocks using nonconductive adhe-sive tabs (Ted Pella, Inc, Redding, CA),and surrounded by colloidal silver paste(Electron Microscopy Sciences, Hatfield,PA). After drying overnight in a vacuumdessicator with dissecant, the sampleswere sputter coated with gold-palladium(Polaron, Energy Beam Sciences, EastGramby, CT) for 1.75 minutes, and storedin a vacuum dessicator with desiccant un-til imaged. The samples were imaged ona scanning electron microscope (JSM-6390LV; JEOL Ltd, Peabody, MA), usinga 5-kV accelerating voltage and workingdistance of 11 mm. The ligaments werealigned at low magnification (approxi-mately 25) by orienting the femoral endof the ligament to the top of the screen,and the residual and scar regions wereidentified. The morphology of collagenfibrils and fibers for each ligament inthe residual and scar tissue regions wereexamined at magnifications of 250 to
11000, and digitally imaged.
HistologyLigaments for histology were fixed undertension in 4% paraformaldehyde at 4°Cfor 48 hours. They were subsequentlydehydrated in graded alcohols, washedwith 2 changes of xylene, and infiltratedand embedded in paraffin, using a Shan-don automatic tissue processor (ThermoElectron Corp, Waltham, MA). Sagittal
contralateral nontreated MCLs. Paired ttest results were subsequently confirmedby calculating mean percent differencesbetween IACFM-treated and nontreatedMCLs [(IACFM-treated – IACFM-non-treated) ÷ nontreated 100%], whichwere analyzed using single sample t testswith a population mean of 0%.
There were no operative or post-operative complications. Animalsassessed at 12 weeks postinjury were
significantly heavier than those assessedat 4 weeks (mean SD, 291.4 13.2 gversus 313.5 22.6 g; P .05). Therewere no differences in weight betweeninjured and control animals (P = .76).
All surgically induced ligament defectswere bridged with scar tissue at the time
Representative images of surgically transected, untreated rat knee medial collateral ligaments (MCL)at (A) 4 and (B) 12 weeks following injury. Arrow indicates location of scar (initial injury). Abbreviations: F, femoralorigin of the MCL; T, tibial insertion of the MCL.

510 | july 2009 | volume 39 | number 7 | journal of orthopaedic & sports physical therapy
[ RESEARCH REPORT ]ligaments did not differ significantly ateither 4 (5.46 1.01 mm2 versus 5.16
1.55 mm2; P = .45) or 12 (3.80 1.02mm2 versus 4.09 0.79 mm2; P = .29)weeks postinjury.
Ligament Mechanical PropertiesAt 4 weeks postinjury, IACFM-treatedligaments could resist 6.4 N (95% con-fidence interval [CI], 1.6 to 11.2 N; P =.01) greater force than contralateral non-treated ligaments (FIGURE 4A). This wasreflected by IACFM-treated ligamentshaving 43.1% (95% CI, 8.2% to 78.0%;P = .02) greater mean difference in ten-sile strength than nontreated ligaments.Similarly, IACFM-treated ligaments had4.9 N/mm (95% CI, 2.4 to 7.4 N/mm; P= .001) (FIGURE 4B) and 5.8 mJ (95% CI,0.7 to 10.9 mJ; P .05) (FIGURE 4C) greaterstiffness and energy to failure at 4 weekspostinjury than nontreated ligaments, re-spectively. This was reflected by IACFM-treated ligaments being 39.7% (95% CI,15.9% to 63.5%; P .01) stiffer and beingable to absorb 57.1% (95% CI, 3.4% to110.9%; P = .04) greater energy beforefailure than nontreated ligaments.
At 12 weeks postinjury, IACFM-treat-IACFM-treat-ed ligaments had 2.6 N/mm (95% CI, 0.2to 5.0 N/mm; P .05) greater stiffnessthan nontreated ligaments, resulting inthe former being 15.4% (95% CI, 0.1%-30.7%; P .05) stiffer (FIGURE 5B). Howev-er, there were no differences at 12 weekspostinjury between IACFM-treated andnontreated ligaments in ultimate force(1.1 N; 95% CI, –2.6 to 4.7 N; P = .54)(FIGURE 5A) or energy to failure (–0.6 mJ;95% CI, –6.7 to 5.5 mJ; P = .84) (FIGURE
5C). Mechanical properties of ligamentsin injured animals at both 4 and 12 weekspostinjury remained inferior to intact,noninjured ligaments from control ani-mals (P .05).
Ligament Microscopic MorphologyLight microscopy of noninjured liga-ments from control animals revealed auniform appearance of tightly packed,well-aligned collagen fibrils with inter-spersed fibroblasts aligned parallel to
of harvest. At 4 weeks postinjury, theinjured region was clearly distinguishablefrom the uninjured ligament tissue bythe presence of a thickened, somewhattranslucent, pinkish scar (FIGURE 3A). Incomparison, ligaments at 12 weeks postin-postin-jury had difficult-to-see whitish scars thatwere relatively indistinguishable from theuninjured tissue, and the thickness of thescar region was continuous with that of
the uninjured portions of the ligament(FIGURE 3B). There were no grosslyobservable differences between IACFM-treated and nontreated ligaments at either4 or 12 weeks postinjury; however, non-postinjury; however, non-; however, non-non-treated ligaments often had more adhe-sions and granular tissue, and were moredifficult to harvest than IACFM-treatedligaments. Mean SD cross-sectionalarea of IACFM-treated and nontreated
0
10
20
30
40
50
Ener
gy to
failu
re (m
J)
0
5
10
15
20
25
30
Stiff
ness
(N/m
m)
0
10
20
30
40
50
Ultim
ate
forc
e (N
)
Nontreated IACFM-treated
†
* *
Noninjured ligament strengthNoninjured ligament stiffness
Noninjured ligament energy
A B C
FIGURE 4. Effect of 9 sessions (1 minute per session) of instrument-assisted cross-fiber massage (IACFM) onknee medial collateral ligament (MCL) mechanical properties assessed at 4 weeks following injury. IACFM-treatedligaments had greater (A) ultimate force, (B) stiffness, and (C) energy to ultimate force than contralateral,nontreated ligaments. *Indicates P .05. †Indicates P .01, as determined with paired t test. The dashed lineindicates mean mechanical properties within uninjured MCLs from age-matched, cage control animals. Error barsindicate SD.
0
10
20
30
40
50
Ener
gy to
Fai
lure
(mJ)
0
5
10
15
20
25
30
Stiff
ness
(N/m
m)
0
10
20
30
40
50
Ultim
ate
Forc
e (N
)
*Noninjured ligament strengthNoninjured ligament stiffness
Noninjured ligament energy
Nontreated IACFM-treated
A B C
FIGURE 5. Effect of 30 sessions (1 minute per session) of instrument-assisted cross-fiber massage (IACFM) onknee medial collateral ligament (MCL) mechanical properties assessed at 12 weeks following injury. IACFM-treatedligaments had (A) equivalent ultimate force, (B) enhanced stiffness, and (C) equivalent energy to failure thancontralateral, nontreated ligaments. *Indicates P .05, as determined with paired t test. The dashed line indicatesmean mechanical properties within uninjured MCLs from age-matched, cage-control animals. Error bars indicate SD.

journal of orthopaedic & sports physical therapy | volume 39 | number 7 | july 2009 | 511
the fibrils ( ). In contrast, liga-ments from injured animals appeared tohave scar morphology with extracellularmatrix disorganization and hypercellu-larity, particularly at 4 weeks postinjury( ). The scar region of IACFM-treated ligaments at 4 weeks postinjuryalso appeared to have greater cellularity,with collagen fiber bundles appearing tobe orientated more along the longitudi-nal axis of the ligament than observed incontralateral nontreated ligaments (FIG
). At 12 weeks postinjury, therewere limited histological differences be-tween IACFM-treated and nontreatedligaments ( ).
Ligaments from injured, but not con-trol, animals had granular tissue at lowmagnification ( 25) on scanning elec-tron microscopy and IACFM-treatedligaments appeared to have less sur-rounding granular tissue compared tonontreated ligaments, supporting themacroscopic observations ( ). Athigher scanning electron microscopymagnifications ( 250- 6500), the scarregion of IACFM-treated ligaments ap-peared to have improved collagen fiberbundle formation and orientation withinthe scar region compared to nontreatedligaments, supporting the light micros-copy observations ( ).
This study investigated the po-tential utility of manual therapy inthe form of IACFM on ligament
healing. Results indicate that IACFM-treated ligaments were 43% stronger,40% stiffer, and able to absorb 57% moreenergy than contralateral, nontreated, in-jured ligaments at 4 weeks following in-jury. These mechanical differences mayhave resulted from favorable effects ofIACFM on the organization of the under-lying collagen substructure, as suggestedby preliminary light microscopy andscanning electron microscopy analyses.The latter needs to be confirmed by wayof more in-depth quantitative analysesin future studies. In contrast, there was
Representative histological sections from (A) noninjured knee medial collateral ligament (MCL) ina cage-control animal, (B) scar region in a nontreated MCL at 4 weeks following injury, (C) scar region in aninstrument-assisted cross-fiber massage (IACFM)-treated MCL at 4 weeks following injury, (D) scar region in anontreated MCL at 12 weeks following injury, and (E) scar region in an IACFM-treated MCL at 12 weeks followinginjury. Black arrows indicate fibroblasts aligned parallel to the collagen fibrils in a noninjured ligament. Whitearrows indicate scar region in injured ligaments.
Representative scanning electron microscopy images taken from an (A) intact knee medial collateralligament (MCL) in a control animal, (B) nontreated MCL at 4 weeks following injury, and (C) instrument-assisted cross-fiber massage (IACFM)-treated MCL at 4 weeks following injury. Images were taken at low ( 25)magnification. Note the close appearance of the IACFM-treated ligament (C) to the noninjured ligament from acontrol animal (A). Also, note the large amount of surrounding granulation tissue in the nontreated, but injuredligament (C) relative to the other 2 ligaments.

512 | july 2009 | volume 39 | number 7 | journal of orthopaedic & sports physical therapy
[ RESEARCH REPORT ]How IACFM facilitates the restoration
of ligament tensile mechanical propertiesfollowing injury was not investigated indetail in the current study, as the primarypurpose was to provide proof-of-conceptevidence for the utility of IACFM. How-ever, preliminary light microscope andscanning electron microscopy assess-ments suggest that IACFM may enhancerestoration of ligament biomechanicalhealing by optimizing the organizationof the collagen substructure. Collagen (inparticular, type 1 collagen) is the primaryload-bearing molecule in ligament thatendows tensile strength, and is orderedhierarchically into fibrils and fibers.21
The alignment and organization of newlyformed collagen fibers in the direction oftensile loads during healing influencesligament mechanical properties.19,20 Thequalitatively improved collagen fiber or-ganization observed within the scar re-gion of IACFM-treated ligaments in thecurrent study is a possible explanationfor why IACFM-treated ligaments hadenhanced tensile mechanical properties.This will be the focus of future quantita-tive studies into IACFM effects on liga-ment morphology.
In addition to more detailed studiesinto IACFM effects on ligament mor-phology, studies are planned to explorepotential molecular mechanisms bywhich IACFM generates its biomechani-cal effects. Our working hypothesis is thatIACFM has an underlying effect on colla-gen, which may include effects on its syn-thesis, maturation, and/or cross-linking.To have such effects, IACFM must influ-ence the fibroblastic cells responsible forproducing collagen. This potential effectis supported by previous work that foundthat IACFM increases fibroblast recruit-ment and activation in a rodent Achillestendon injury model.5,8 It is plausiblethat IACFM presents a direct mechani-cal stimulus to the extracellular matrix,which is subsequently transduced into acellular response. A candidate mechan-otransduction pathway for this responsedeserving of future investigation is the ex-tracellular matrix-integrin-cytoskeleton
servative treatment and surgical repairproducing similar outcomes irrespec-tive of the extent of the initial ligamentdamage.9,13,22 Consequently, there is aneed to establish interventions otherthan surgery for influencing ligamenthealing. Numerous preclinical studieshave investigated the utility of novelinterventions targeting ligament heal-ing, including the use of gene therapies,growth factors, biological scaffolds, stemcell therapies, and biophysical modali-ties.10,15,18,32 While each of these direc-tions has shown promise in influencingligament healing, the techniques arefar from being translated into the clini-cal realm and their eventual costs mayprohibit wide use in mainstream clinicalpractice. In contrast, IACFM may haveclinical utility, as it is currently readilyavailable and practical from the sensethat gains in ligament biomechanicalproperties were produced in the currentstudy using a relatively limited numberof short treatment sessions (9 total ses-sions of 1-minute duration each).
minimal to no effect of IACFM on liga-ment healing when assessed at 12 weeksfollowing injury, with the only differencebetween IACFM-treated and nontreatedligaments being 15% greater stiffness inthe former. Overall, the findings of thisstudy suggest that IACFM acceleratesearly tissue-level healing following liga-ment injury, but does little in terms ofaugmenting healing.
The findings of the current study areinteresting in that a relatively simple andpractical manual therapy technique wasfound to enhance early recovery of liga-ment biomechanical properties follow-ing acute injury. This may be clinicallyrelevant, as there are currently limitedestablished treatment options for me-diating tissue-level ligament healing.It is clear from preclinical and clinicalstudies that surgery with or without im-mobilization is not indicated for mostcapsular and extracapsular ligamentinjuries. This holds true for both par-tial- and full-thickness ligament tears,with comparative studies showing con-
Representative scanning electron microscopy images taken from the scar region of a nontreated (A,B), and instrument-assisted cross-fiber massage (IACFM) treated ligament (C, D) at 4 weeks following injury.Images were taken at medium ( 250) (A, C), and high ( 6500) (B, D) magnification. Note the improved collagenfiber bundle formation and orientation within the scar region of the IACFM-treated ligament (C, D) relative to thenontreated ligament (A, B).

journal of orthopaedic & sports physical therapy | volume 39 | number 7 | july 2009 | 513
axis. Integrins are a family of glycoproteinmolecules that connect extracellularlywith the extracellular matrix and intrac-ellularly with the cytoskeleton and othercytoplasmic constituents.12 This creates atransmembrane axis that mechanicallylinks the extracellular matrix with thecytoplasmic constituents of the cell totransmit external stimuli (such as thoseassociated with IACFM) directly to theinternal environment of the cell to altergene expression and protein synthesis.
The current study provides supportiveevidence for the potential clinical use ofIACFM in the treatment of capsular andextracapsular ligament injuries; however,the findings need to be carefully inter-preted in light of acknowledged limita-tions. First, the study was performed inan animal model, wherein the knee MCLwas injured via surgical transection. Thisis a highly reproducible and establishedmodel for the preclinical testing of in-terventions for ligament injuries16,20,29,31;however, the ability of the model to pre-dict the clinical scenario wherein liga-ments are injured via excessive tensileload has not been established. Second, thesize of rodent tissues in relation to thoseof humans raises scaling issues in termsof intervention application and response.We addressed this issue by performingIACFM to rodent ligaments with thesame tool and force as those used clinical-ly to treat similar-size ligaments (fingercollateral ligaments). Third, between-animal differences in activity levels mayhave influenced ligament-healing rates,as activity has previously been shownto mediate healing of isolated MCL in-juries in rodents.2 We controlled for thispossibility in the current study by estab-lishing within-animal IACFM effects,wherein IACFM-treated ligaments werecompared to contralateral nontreatedligaments that were presumably exposedto equivalent activity levels. Fourth, thecurrent study did not consider IACFM ef-fects on clinically measurable outcomes,such as recovery from symptoms such aspain. The restoration of mechanical prop-erties is the ultimate tissue-level outcome
of the ligament-healing process and is animportant preclinical outcome; however,it is plausible that IACFM acceleratesligament biomechanical healing withoutinfluencing symptom recovery. Also, theestablishment of IACFM benefits via theex vivo testing of MCL tensile proper-ties with the knee at 70° flexion may notrepresent the most clinically translatableoutcome. While testing at 70° knee flex-ion is reported to load all fibers of the ratMCL simultaneously,20 it is plausible thatalternative joint positions provide bet-ter tests of functionally important por-tions of the ligament. Similarly, as theMCL was isolated for mechanical test-ing, the contribution of other structuresthat contribute to the in vivo resistanceof knee valgus forces were not assessed.It is possible that other passive and ac-tive restraints are able to compensate forinjury to the MCL in the clinical setting,reducing the potential clinical effect sizeof IACFM during ligament healing.
In summary, this study suggeststhat IACFM may accelerate earlytissue-level healing following acute
capsular/extracapsular ligament injurybut it has minimal to no effect in termsof augmenting the overall outcome of theligament-healing process. This findingsupports a theoretically sound argumentfor the use of IACFM after acute ligamentinjury; however, careful interpretation ofthis controlled laboratory study is war-ranted until its findings are confirmed byclinical studies.
IACFM accelerated earlytissue-level healing following acutecapsular/extracapsular ligament injurybut had minimal to no effect in terms ofaugmenting the overall outcome of theligament-healing process.
IACFM is a relatively simpleand practical therapy technique thatmay facilitate earlier return of ligamenttissue-level biomechanical properties,
enabling quicker return to function withless susceptibility to reinjury.
Careful interpretation of thiscontrolled animal study is warranteduntil its findings are confirmed by clini-cal studies.
ACKNOWLEDGEMENTS: The authors wouldlike to acknowledge the following student re-search assistants from the Doctor of PhysicalTherapy Program at Indiana University whocontributed to this study: Keith Avin, MonicaBeaman, Marie DeWolf, Monica Eberle, Ja-mie Grogg, Allison Herriot, Kristen Kastner,John Kiesel, Jessica Lassiter, Kristen Meade,Kory Risner, Heidi Streeter, Lynn Taylor, andMark Watson. We also appreciate the supportreceived from the Histology Laboratory andElectron Microscopy Center, Department ofAnatomy and Cell Biology, Indiana Univer-sity School of Medicine.
1. Burke J, Buchberger DJ, Carey-Loghmani MT,Dougherty PE, Greco DS, Dishman JD. A pilotstudy comparing two manual therapy interven-tions for carpal tunnel syndrome. J ManipulativePhysiol Ther. 2007;30:50-61. http://dx.doi.org/10.1016/j.jmpt.2006.11.014
2. Burroughs P, Dahners LE. The effect of enforcedexercise on the healing of ligament injuries. AmJ Sports Med. 1990;18:376-378.Carey-Loghmani M, Hyde T. The Grastontechnique of instrumented-assisted soft tissuemobilization. In: Hyde T, Genenbach M, eds.Conservative Management of Sports Injuries.Sudbury, MA: Jones & Bartlett Publishers;2005:300-310.Chiquet M, Tunc-Civelek V, Sarasa-RenedoA. Gene regulation by mechanotransduc-tion in fibroblasts. Appl Physiol Nutr Metab.2007;32:967-973. http://dx.doi.org/10.1139/h07-053Davidson CJ, Ganion LR, Gehlsen GM, Verhoe-stra B, Roepke JE, Sevier TL. Rat tendon mor-phologic and functional changes resulting fromsoft tissue mobilization. Med Sci Sports Exerc.1997;29:313-319.Fernandez WG, Yard EE, Comstock RD. Epi-demiology of lower extremity injuries amongU.S. high school athletes. Acad Emerg Med.2007;14:641-645. http://dx.doi.org/10.1197/j.aem.2007.03.1354Frank C, Woo SL, Amiel D, Harwood F, Gomez M,Akeson W. Medial collateral ligament healing. Amultidisciplinary assessment in rabbits. Am JSports Med. 1983;11:379-389.

514 | july 2009 | volume 39 | number 7 | journal of orthopaedic & sports physical therapy
[ RESEARCH REPORT ]
@ MORE INFORMATIONWWW.JOSPT.ORG
Gehlsen GM, Ganion LR, Helfst R. Fibroblastresponses to variation in soft tissue mobilizationpressure. Med Sci Sports Exerc. 1999;31:531-535.
9. Gomez MA, Woo SL, Inoue M, Amiel D, HarwoodFL, Kitabayashi L. Medical collateral ligamenthealing subsequent to different treatment regi-mens. J Appl Physiol. 1989;66:245-252.
10. Hoffmann A, Gross G. Tendon and ligamentengineering: from cell biology to in vivo applica-tion. Regen Med. 2006;1:563-574. http://dx.doi.org/10.2217/17460751.1.4.563
11. Hootman JM, Dick R, Agel J. Epidemiology ofcollegiate injuries for 15 sports: summary andrecommendations for injury prevention initia-tives. J Athl Train. 2007;42:311-319.
12. Hynes RO. Integrins: bidirectional, allostericsignaling machines. Cell. 2002;110:673-687.Inoue M, Woo SL, Gomez MA, Amiel D, OhlandKJ, Kitabayashi LR. Effects of surgical treatmentand immobilization on the healing of the medialcollateral ligament: a long-term multidisciplinarystudy. Connect Tissue Res. 1990;25:13-26.Kofotolis ND, Kellis E, Vlachopoulos SP. Anklesprain injuries and risk factors in amateursoccer players during a 2-year period. Am JSports Med. 2007;35:458-466. http://dx.doi.org/10.1177/0363546506294857Laurencin CT, Khan Y, Kofron M, et al. The ABJSNicolas Andry Award: Tissue engineering ofbone and ligament: a 15-year perspective. ClinOrthop Relat Res. 2006;447:221-236. http://dx.doi.org/10.1097/01.blo.0000194677.02506.45Lechner CT, Dahners LE. Healing of the medialcollateral ligament in unstable rat knees. Am JSports Med. 1991;19:508-512.Melham TJ, Sevier TL, Malnofski MJ, Wilson JK,Helfst RH, Jr. Chronic ankle pain and fibrosissuccessfully treated with a new noninvasiveaugmented soft tissue mobilization technique(ASTM): a case report. Med Sci Sports Exerc.1998;30:801-804.Molloy T, Wang Y, Murrell G. The roles of growth
factors in tendon and ligament healing. SportsMed. 2003;33:381-394.
19. Provenzano PP, Alejandro-Osorio AL, GrorudKW, et al. Systemic administration of IGF-Ienhances healing in collagenous extracellularmatrices: evaluation of loaded and unloadedligaments. BMC Physiol. 2007;7:2. http://dx.doi.org/10.1186/1472-6793-7-2
20. Provenzano PP, Martinez DA, Grindeland RE, etal. Hindlimb unloading alters ligament healing.J Appl Physiol. 2003;94:314-324. http://dx.doi.org/10.1152/japplphysiol.00340.2002
21. Provenzano PP, Vanderby R, Jr. Collagen fibrilmorphology and organization: implications forforce transmission in ligament and tendon.Matrix Biol. 2006;25:71-84. http://dx.doi.org/10.1016/j.matbio.2005.09.005
22. Reider B, Sathy MR, Talkington J, Blyznak N,Kollias S. Treatment of isolated medial collateralligament injuries in athletes with early func-tional rehabilitation. A five-year follow-up study.Am J Sports Med. 1994;22:470-477.Tyler TF, McHugh MP, Mirabella MR, MullaneyMJ, Nicholas SJ. Risk factors for noncontactankle sprains in high school football players: therole of previous ankle sprains and body mass in-dex. Am J Sports Med. 2006;34:471-475. http://dx.doi.org/10.1177/0363546505280429Valderrabano V, Hintermann B, Horis-berger M, Fung TS. Ligamentous post-traumatic ankle osteoarthritis. Am J SportsMed. 2006;34:612-620. http://dx.doi.org/10.1177/0363546505281813van Rijn RM, van Os AG, Bernsen RM, Lui-jsterburg PA, Koes BW, Bierma-Zeinstra SM.What is the clinical course of acute anklesprains? A systematic literature review. Am JMed. 2008;121:324-331 e326. http://dx.doi.org/10.1016/j.amjmed.2007.11.018Wang JH, Thampatty BP, Lin JS, Im HJ. Mecha-noregulation of gene expression in fibroblasts.Gene. 2007;391:1-15. http://dx.doi.org/10.1016/j.gene.2007.01.014
Warden S, Saxon L, Castillo A, Turner C. Knee
ligament mechanical properties are not influ-
enced by estrogen or its receptors. Am J Physiol
Endocrinol Metab. 2006;290:E1034-1040.
Warden SJ, Avin KG, Beck EM, DeWolf ME,
Hagemeier MA, Martin KM. Low-intensity pulsed
ultrasound accelerates and a nonsteroidal
anti-inflammatory drug delays knee ligament
healing. Am J Sports Med. 2006;34:1094-1102.
http://dx.doi.org/10.1177/0363546505286139
29. Weiss JA, Woo SL, Ohland KJ, Horibe S, Newton
PO. Evaluation of a new injury model to study
medial collateral ligament healing: primary
repair versus nonoperative treatment. J Orthop
Res. 1991;9:516-528. http://dx.doi.org/10.1002/
jor.1100090407
Wilson JK, Sevier TL, Helfst RH, Honing EW,
Thomann AL. Comparison of rehabilitation
methods in the treatment of patellar tendonitis.
J Sports Rehab. 2000;15:9-14.
Woo SL, Debski RE, Zeminski J, Abramowitch
SD, Saw SS, Fenwick JA. Injury and repair of
ligaments and tendons. Annu Rev Biomed Eng.
2000;2:83-118. http://dx.doi.org/10.1146/an-
nurev.bioeng.2.1.83
Woo SL, Jia F, Zou L, Gabriel MT. Functional tis-
sue engineering for ligament healing: potential
of antisense gene therapy. Ann Biomed Eng.
2004;32:342-351.
Woo SL, Orlando CA, Camp JF, Akeson WH.
Effects of postmortem storage by freezing
on ligament tensile behavior. J Biomech.
1986;19:399-404.
DOWNLOAD PowerPoint Slides of JOSPT Figures & Tables
JOSPT PowerPoint slides of figures and tablesJournal www.jospt.org
“View Slides”“Save Target As”






![INDEX [] · 2021. 3. 16. · Masaje personalizado con aceites medicados. Ayurveda - Pinda Swedana 60 min Masaje realizado con saquitos de semillas y aceites esenciales. Beauty Back](https://img.pdfslide.us/doc/110x75/6133c2abdfd10f4dd73b4c1c/index-2021-3-16-masaje-personalizado-con-aceites-medicados-ayurveda-.jpg)