Embed Size (px)
Citation preview

� Mary Lou Sole� Oral care in reducing VAP
� Chris Winkelman� Mobility practices to prevent VAP, pressure ulcers and long term functional
limitations
� Kathleen M. Vollman� Bathing & other basics care activities to reduce spread of microorganisms
� Mary Beth Flynn Makic� Prevention of incontinence-associated dermatitis & pressure ulcers
� Pat J. Posa� Eliminating catheter-associated blood stream infections
� Ginger S. Pierson� Prevention of Sternal Wound Infections Following Cardiac Surgery
Mary Beth Flynn Makic RN PhD CNS CCNS
� Pressure ulcers (PUs) can be identified,
measured, and reported
� Usually preventable
� Result in adverse patient outcomes,
prolonged/additional care, increased costs
� Significant body of scientific evidence is available
to guide practice and prevent PUs
� October, 2008: Stage III and IV PUs acquired
after admission will not be reimbursed
www.cms.hhs.gov April 14, 2008 fact sheet; www.qualityforum.org Serious Adverse Events
Working Group March 19, 2008
� 4th leading preventable medical error in the U.S.
� 2.5 million patients are treated annually
� 1993-2003 PU prevalence ↑63% in acute care
� National acute care prevalence rates 7-16%
� NDNQI data base: critical care 7-14%
� ↑LOS ~ 4 days
� Cost to treat PU $40-70,000 per PU; estimated $11 billion annually in the U.S.
� Estimated 60,000 deaths per year associated with PUs
� 1995 ANA identified PU prevention as a nursing sensitive indicator� National Database of Nursing Quality Indicators (NDNQI)
� www.nursingworld.org
� 2004 National Quality Forum � National Voluntary Consensus Standards for Nursing-Sensitive Care
http://www.qualityforum.org/publications/reports/nurse_tracking.asp
� IHI 5 Million Lives Campaign� http:/www.ihi.org/IHI/Programs/Campaigns
� 1992/1994 AHRQ published guidelines for
assessment and treatment of PU
� www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.
chapter.4409
� 2003 Wound Ostomy Continence Nurses Society
Guidelines for Prevention and Management of
PU
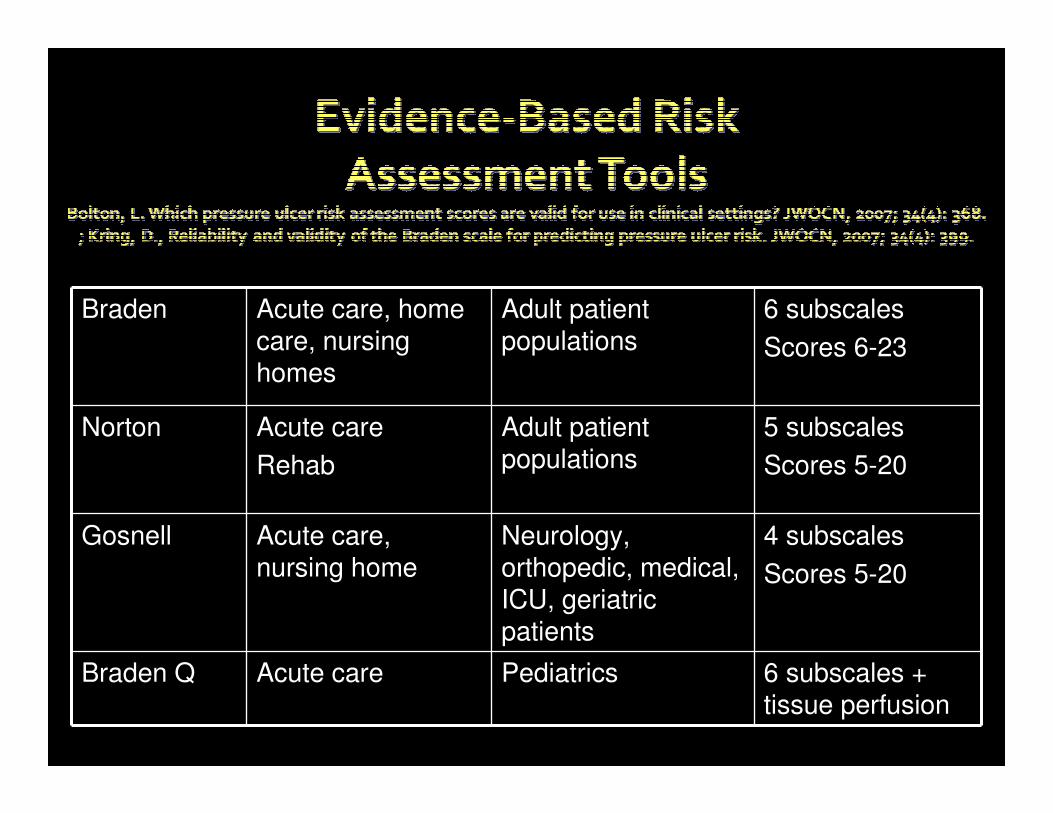
Braden Acute care, home care, nursing homes
Adult patient populations
6 subscales
Scores 6-23
Norton Acute care
Rehab
Adult patient populations
5 subscales
Scores 5-20
Gosnell Acute care, nursing home
Neurology, orthopedic, medical, ICU, geriatric patients
4 subscales
Scores 5-20
Braden Q Acute care Pediatrics 6 subscales + tissue perfusion
� Use standard EBP risk assessment tool
� Admission to hospital
� ?including ED
� Document PU present on admission (POA)
� Daily assessment throughout hospitalization
� Research has shown Risk Assessment Tools are more accurate than RN assessment alone.
� Braden Scale for Predicting Pressure Sore Risk
� 6 subscales
� Rated 1-4
� Pressure on tissues
� Mobility, sensory perception,
activity
� Tissue tolerance for pressure
� Nutrition, moisture,
shear/friction
� Score 6-23
� Frequent repositioning� CLRT and manual turning
� Managing moisture
� Developing and implementing a pressure ulcer prevent protocol� User friendly
� Products available
� RNs knowledge of protocol and products
�Assessment of risk�Other factors: age, vasopressors, instability, severe agitation, comorbidities, obesity
�Optimize nutrition & hydration
�Albumin, prealbumin
�Fluid balance
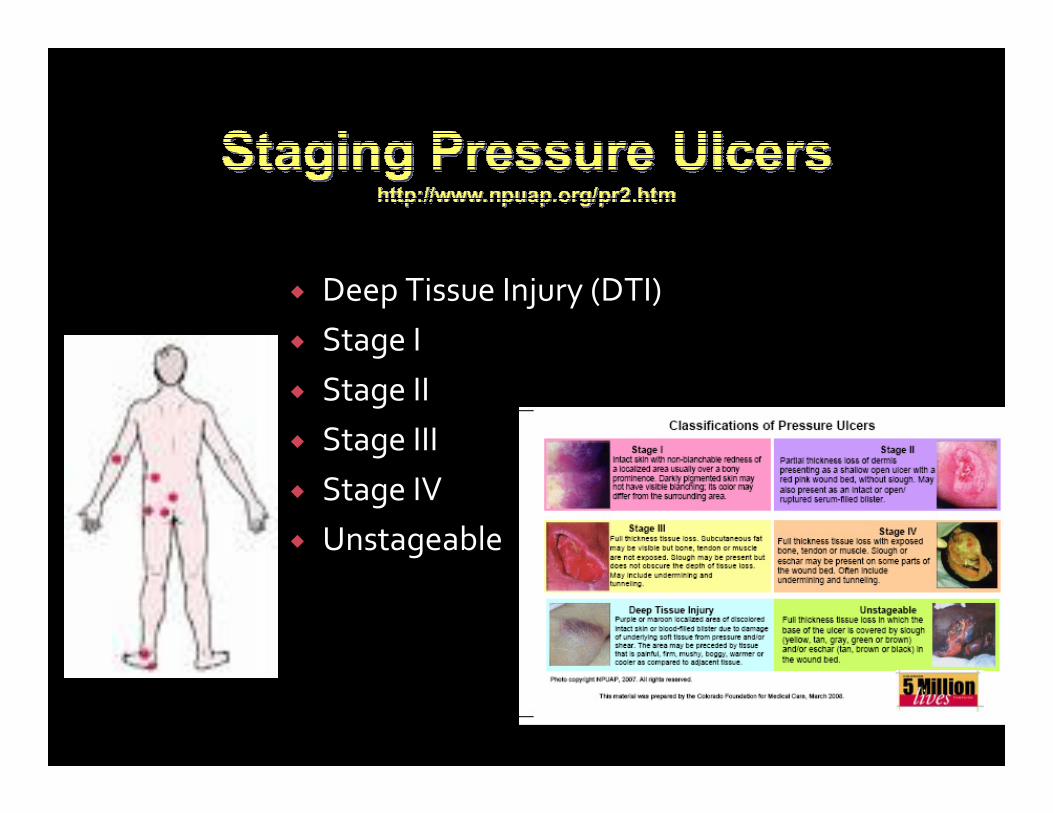
� Deep Tissue Injury (DTI)
� Stage I
� Stage II
� Stage III
� Stage IV
� Unstageable
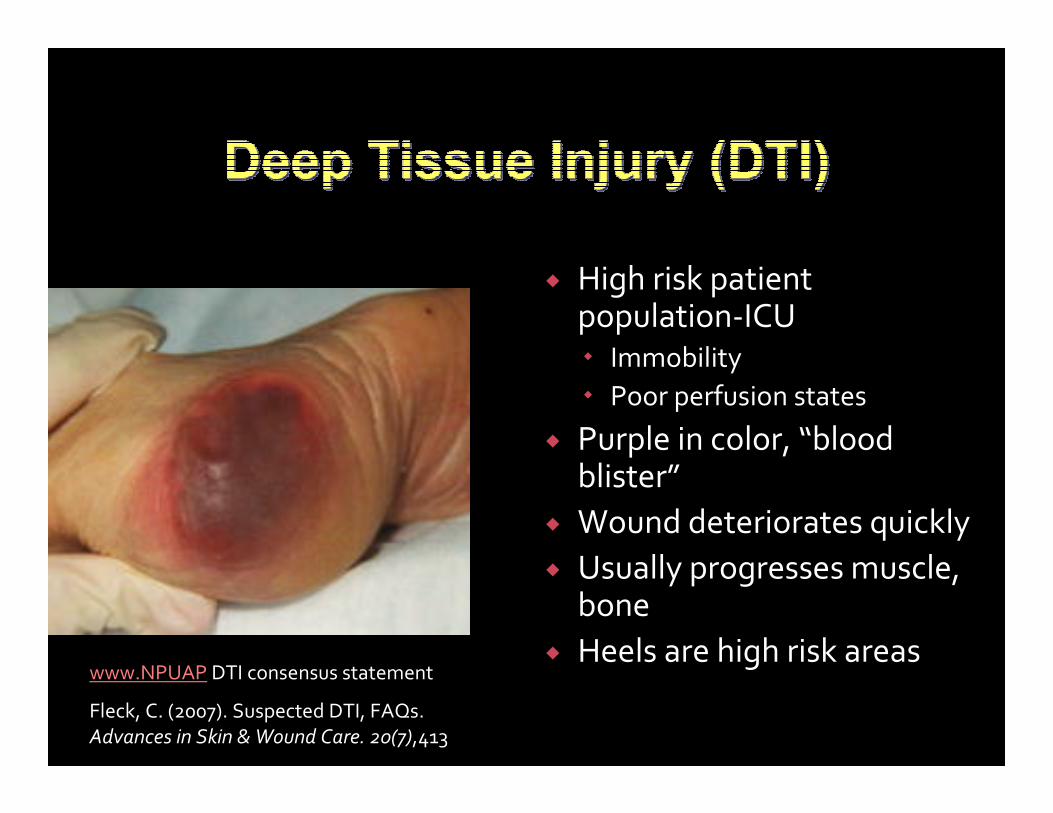
� High risk patient population-ICU� Immobility
� Poor perfusion states
� Purple in color, “blood blister”
� Wound deteriorates quickly
� Usually progresses muscle, bone
� Heels are high risk areaswww.NPUAP DTI consensus statement
Fleck, C. (2007). Suspected DTI, FAQs.
Advances in Skin & Wound Care. 20(7),413
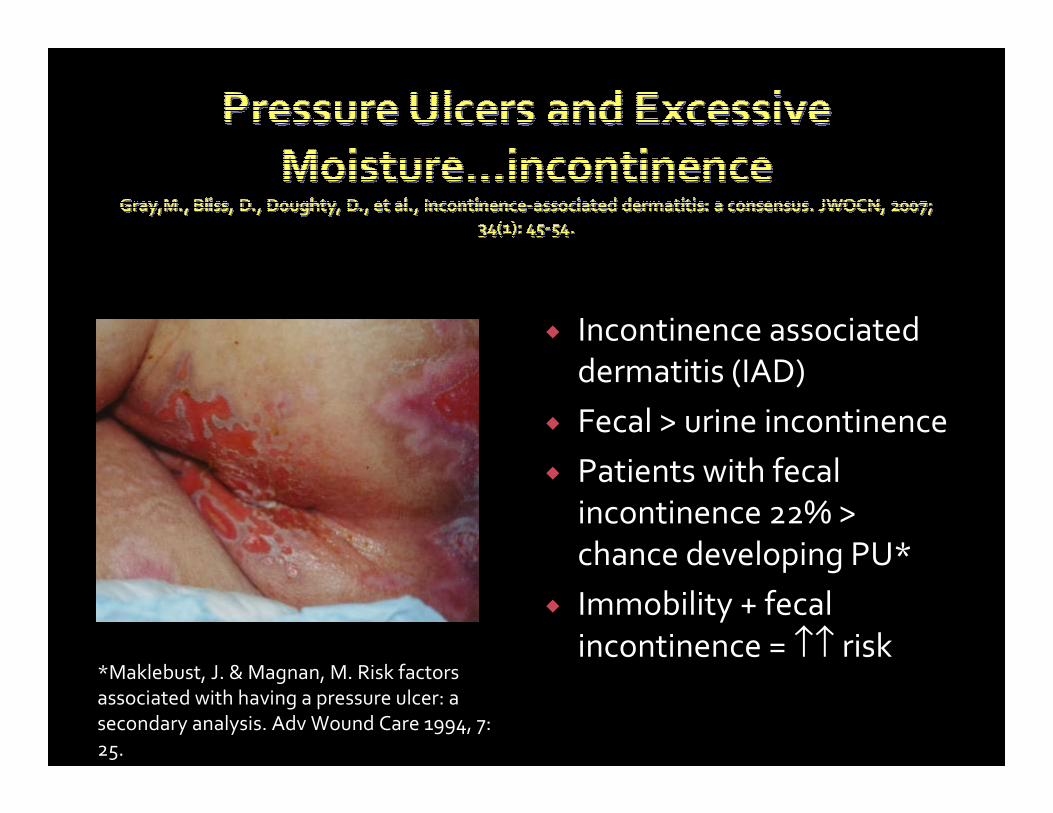
� Incontinence associated
dermatitis (IAD)
� Fecal > urine incontinence
� Patients with fecal
incontinence 22% >
chance developing PU*
� Immobility + fecal
incontinence = ↑↑ risk *Maklebust, J. & Magnan, M. Risk factors
associated with having a pressure ulcer: a
secondary analysis. Adv Wound Care 1994, 7:
25.
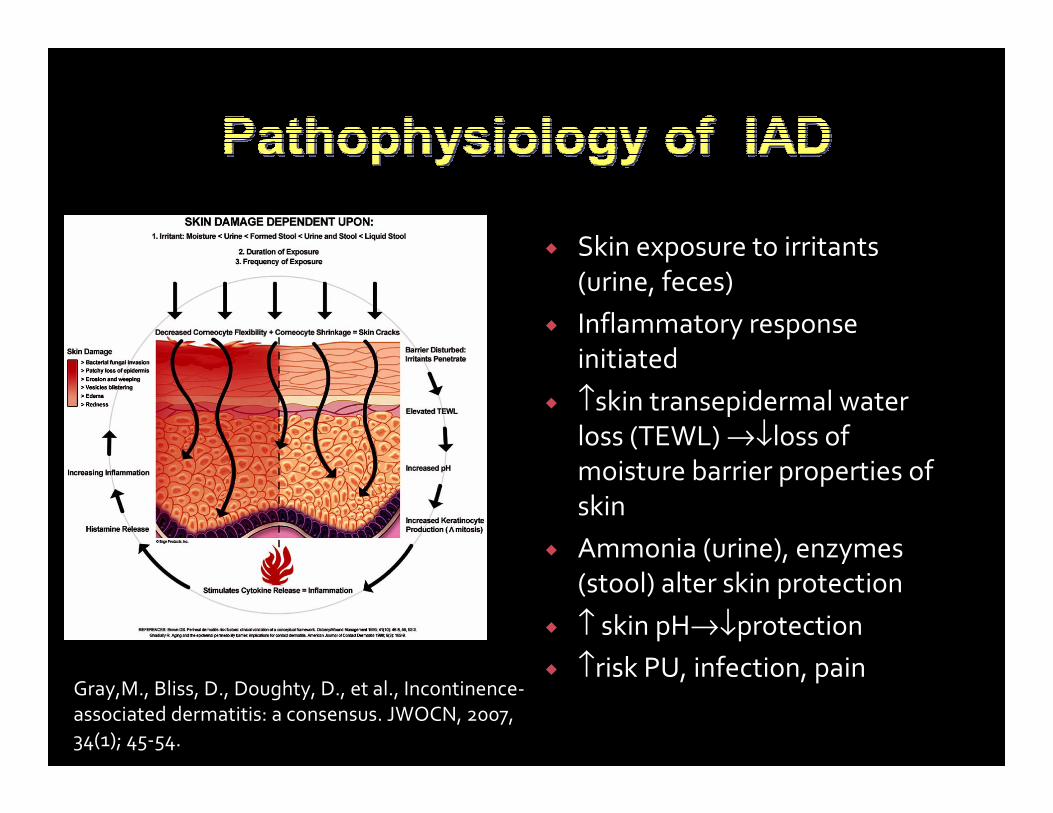
� Skin exposure to irritants
(urine, feces)
� Inflammatory response
initiated
� ↑skin transepidermal water loss (TEWL) →↓loss of moisture barrier properties of
skin
� Ammonia (urine), enzymes (stool) alter skin protection
� ↑ skin pH→↓protection
� ↑risk PU, infection, painGray,M., Bliss, D., Doughty, D., et al., Incontinence-
associated dermatitis: a consensus. JWOCN, 2007,
34(1); 45-54.
� 1st identify the source of IAD
� In ICU frequently it is antibiotics or tube feeding
� Consult nutritionist: evaluate osmolarity of tube feeding; add fiber to diet
� Consider medications to slow diarrhea
� Evaluate medications that
may be causing diarrhea
� Ace inhibitors, beta-blockers, digoxin, lasix, mannitol,
octreotide, lactulose
� Absorbent underpads,
changed frequently
� Low airloss therapeutic
mattress
� First, do no harm…
� Soaps ↑ skin pH
� Wash clothes rough-up already fragile skin
� Diapers keep moisture, enzymes in…
� Cleans frequently and avoid scrubbing
� Apply barrier creams that: moisturize and protect skin
� Polymer-based underpads; limit linensGray, M. Incontinence-related skin
damage: essential knowledge. OWM,
2007; www.o-wm.com/article/8161
� Skin pH is acidic (5.0 to 6.0)
� Cleansing products should be pH balanced or neutral (7)
� Soaps are alkaline →↑dryness, irritation, breakdown, ↓ barrier
� Soap pH
� Dove 7.0
� Dial 7.9
� Zest 10� Use pH balanced no-rinse
cleansing products
� Wash clothes irritate skin
� Perineal wipes
� Are pH balanced
� Contain moisturizers and emollients
� Skin protectant creams� Dimethicone, petrolatum,
zinc oxide� Use antifungal as indicated,
early
� Keep skin clean, dry, moisturized, protected

� Containment devices� What’s the evidence?
� Rectal pouches
� 1-2 days; 2 individuals to apply correctly
� May still tear intact skin upon removal
� Nasopharyngeal airway
� Mushroom catheter or balloon tipped catheter
� Bowel Management Systems (BMS)
BMS system
Balloon and nasal
trumpet system
� Assess on admission and daily
� Implement interventions
driven by your assessment
� Excessive moisture?
� Apply barrier cream
� NMBAs, Sedated, Intubated?
� Turn frequently, prop and tuck
bony prominences frequently,
assess pressure redistribution
bed/cushions
� Moisturize and hydrate the skin
� Critically evaluate your
bathing/skin care system
� Minimize friction and shear
� HOB 300, lift sheet, airpals
� Document POA and new
pressure ulcers
� Develop interprofessional plan of
care
� Preventing pressure ulcers and IAD through
evidence-based nursing practice…
Patricia J Posa RN, BSN MHA
Special Projects Coordinator-Keystone
St Joseph Mercy Health System
Ann Arbor, MI
� Incidence and risk factors
� Evidence based strategies to eliminate CLA-BSI
� Additional strategies
� Insertion process standardization, education and
evaluation
� Michigan Hospital Association Keystone ICU
Collaborative
� Incidence and risk factors
� Evidence based strategies to eliminate CLA-BSI
� Additional strategies
� Insertion process standardization, education and
evaluation
� Michigan Hospital Association Keystone ICU
Collaborative
� 80,000 CLA-BSI in U.S. ICUs annually
� Mortality: 18% (0-35%)
� Annual deaths: 500 - 28,000
� Cost per episode: $25,000-$45,000
� Annual cost: $296 million -$2.3 billion
CDC. MMWR 2002; Heiselman JAMA 1994; Dimick Arch Surg 2001
� Cutaneous colonization of insertion site
� Moisture under the dressing
� Prolonged catheter time
� Technique of care and placement
� Remove/Avoid unnecessary lines
� Hand hygiene
� Maximal barrier
� Chlorhexadine for skin prep
� Avoid femoral lines
CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]
www.ihi.org
What Does the ‘Bundle’ Evidence
Tell Us?

� For Provider:
� Hands hygiene
� Non-sterile cap and mask
� All hair should be under cap
� Mask should cover nose and mouth tightly
� Sterile gown and gloves
� For the Patient
� Cover patient’s head and body with a large sterile
drape


Minimal@ Maximum*
Local inf. 7.2% 2.3%
CVC-BSI 3.6% 0.6%
*cap, mask, sterile gloves, sterile gown, head/body of patient covered with
large sterile drape
@ sterile gloves, small sterile drape
Raad II, et al. Infect Control Hosp Epidemiol 1994;15:231-8


� Rapid bactericidal activity
� (affective after 30 sec vs. 2 min)
� Persistent activity on the skin & cumulative
� Maintains its activity in the presence of other organic
material
� Low allergic or toxic response
� None or mild systemic absorption
Chalyakunapruk N. et al. Ann Intern Med. 2002;136:792-801

� RCT of femoral and SC lines in the ICU� 145 pts femoral/144 pts SC
� Outcomes� Higher rate of infectious complications in femoral grp:
19.8% vs 4.5% (p<.001)
� Higher rate of thrombotic complications in femoral grp: 21.5% vs 1.9% (p<.001); complete thrombosis 6% vs 0%
� Similar rates of mechanical complications: 17.3% vs 18.8% (p=NS)
JAMA 2001,286: 700-7

� Replace all catheters inserted under emergency conditions within 48 hours
� Do not routinely replaced non-tunnelled CVC catheters
� PA catheters should be changed no more frequently than every 7 days.
� Use a guidewire assisted catheter exchange if infection is not suspected.
� Do not use guidewire technique to replace catheters if there is a clinical suspicion for CR-BSI.
� Routine culture of the tip is not recommended.
� For arterial lines: changed no more frequently than q 5 days along with the transducer and tubing.
CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]

� Use either sterile gauze or transparent dressing (High MVP rate) to cover the site (Cat 1A)
� If you place the 2x2 under the transparent it becomes a gauze dressing
� Change gauze q 2 days & transparent q 7 days (Cat 1A)
� Replace dressing if damp, loosened or soiled or inspection of the site is necessary
� Chlorhexidine/Alcohol skin prep recommended for every dressing change.
� Do not routinely apply antimicrobial ointments to the site (Cat 1A)
CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]

Additional Strategies:
� CHG Baths
� CHG Dressings
� Antimicrobial impregnated CVC

� 52 week, 2 arm, cross-over design clinical trial
� 22 bed MICU with 11 beds in 2 geographically
separate areas
� 836 MICU patients
� 1st 28 weeks: 1 hospital randomize to bathe with (Sage 2%) CHG cloths & the other unit bathe with
soap & water
� 2 week wash out period
� 2nd 24 weeks: methods were crossed over
� Measured: Primary outcomes: incidence of CA-BSI’s & clinical sepsis. Secondary: other infections
Bleasdale SC. et al. Arch Internal Med, 2007;167(19):2073-2079
CHG Bathing Reduces CLA-BSI

Bleasdale SC. et al. Arch Internal Med, 2007;167(19):2073-2079
Results:�CHG arm were significantly less likely to acquire a CLA-BSI 6.4 vs. 16.8 infections per 1000 catheter days�Benefit against primary CLA-BSI’s by CHG cleansing after 5 days in MICU�No difference in clinical sepsis or other infections
CHG Bathing Reduces CLA-BSI

� BSI bundle implementation resulted in reduction of CA-BSI’s
from 24.8 to 3.1 per 1000 catheter days in 4 adult ICU’s (30
beds)
� 8 month implementation regarding addition of the
Chlorhexidine patch as part of site care
Results: Compared� 277 patients with CVC from May-April 2005 (Bundle)
� 226 patients with CVC from Sept- Dec 2005 (Bundle & Patch) with 98% compliance of patch
� CA-BSI went 3.1 to 0 per 1000 catheter days (p < 0.05)
� Cost savings estimate: $314, 678
Garcia R et al. AJIC, 2006;34(5):E42

� Prospective 2 year before and after study (1998-
2000 compared to 2000-2002)
� Use of chlorhexidine/silver-sulfadiazene catheter
in 6 ICUs at large teaching hospital
Results:
� CRBSI decreased from 8.2 per 1000 catheter days
to 5.4 per 1000 catheter days (p=.003)
� Prevention strategies used: maximal barrier
precautions (not using CHG for skin prep)
Borschel DM, et al Am Jo Infect Control 2006;34

CDC Recommendations:
� Use of an antimicrobial or antiseptic-
impregnated CVC in adults whose catheter is
expected to remain in place for > 5 days if,
after implementing a comprehensive strategy
to reduce rates of CRBSI, the CRBIS rate
remains above benchmarked goal (IE: 3.3/1000
catheter days)
Prevention of Catheter Infection: MMWR 2002;51

� Create Culture of Safety: � Completed unit education on patient safety� Training to senior medical staff and residents� Education to nurses and respiratory therapists� Empower nurses/RT to stop line placement� Pre-procedure Briefing
� Improve Processes� Reduce complexity: Line cart� Create independent checks for key processes: BSI
checklist� Nurse in room during line insertion� Sign on door: ‘Procedure in progress’ to decrease traffic in
room
� Automate:� Put checklist and standard documentation in new bedside
computer system
How to Implement the Evidence
Through a State-wide Collaborative

� Make introductions
� Discuss patient information and procedure
� Agree upon a time for line insertion
� Review best practice for line insertion(if necessary)
� Nurse defines their role to physician: provide equipment, monitor patient, provide patient comfort, observe for compliance with best practices and STOP procedure if sterile process compromised
� Establish communication expectation for sterile procedure breaks
� Examples include: your sleeve has touched the IV pole, the guidewire touched the headboard
� Identify any special supply or procedural needs
� Discuss any special patient issues (IE: patient confused, patient awake)
� Answer any additional questions
� TIME OUT: RIGHT PATIENT---RIGHT PROCEDURE


Are We Implementing the
Prevention Strategies and are
They Effective???

Use of CVC-Related Bloodstream Infection
Prevention Practices by US Hospitals
� National survey of infection control coordinators regarding CVC related BSI prevention practices
� Maximal Barrier Precautions, CHG prep or composite (MSP + CHG +
avoidance of routine central line changes)
� March 2005 to August 2005
� Random sample of non-federated hospitals with ICU and
more than 50 beds (n=600) and VA hospitals (n=119)
� 72% response rate (n=516):
� VA hospitals: n=95
� Non-VA hospitals: n=421
Krein SA, et al. Mayo Clin Proc. 2007;82(6):672-678

Use of CVC-Related Bloodstream Infection
Prevention Practices by US Hospitals
� Results:� Use of maximal barrier precautions: 84% for VA vs 71% non-VA (p=.01)
� Use of CHG for insertion site prep: 91% for VA vs 69% non-VA (p=.001)
� Use of Composite approach: 62% for VA vs 44% for non-VA (p=.003)
� Antimicrobial catheter use: 32% for VA vs 38% for non-VA (p=.30)
� Use of CHG dressing: 29% for VA vs 25% for non-VA (p=.47)
Hospitals with higher safety culture score, having a certified infection control professional and participating in an infection prevention collaborative were more
likely to use CR-BSI prevention practices
Krein SA, et al. Mayo Clin Proc. 2007;82(6):672-678

� 103 ICU’s in state of Michigan reported data
� Examine 375,757 catheter days
� Implementation of the BSI Bundle/checklist
Results�Median rate of CLA-BSI per 1000 catheter days
went 2.7 to 0 at 3 months ((p<0.002)
�Mean rate of CLA-BSI’s per 1000 catheter days
went 7.7 to 1.4 at 18 month follow up (p<0.002)
Pronovost P et al, N Engl J Med;2006;355:2725-2732
Intervention to Decrease CLA-BSI
Statewide Collaborative-Keystone ICU

� 3 hospital system: 2 hospital having 4 ICUs
� Implemented BSI Bundle in July 2004� 5 best practices
� BSI checklist
� Line cart
� Empower nurses to stop line placement if procedure not followed
� Nurse in room during line insertion
� Education—Education --Education
� Share data monthly and chart review each of CLA-BSI (Learn from a Defect)
Posa, P Harrison, D & Vollman, K AACN Advanced Critical Care, 2006; 17(4):446-454
St. Joseph Mercy Health System
Ann Arbor, MI

Results:
� Baseline rate: 7.6 per 1000 catheter days
� 2005: 2.12 per 1000 catheter days
� 2006: 1.11 per 1000 catheter days
� 2007: 1.12 per 1000 catheter days
St. Joseph Mercy Health System
Ann Arbor, MI

Results::� Livingston CCU: 38 months without a BSI
� MICU: 29 months without a BSI
� CCU: 17 months without a BSI
� SICU: 6 months without a BSI
St. Joseph Mercy Health System
Ann Arbor, MI

Results:� Marginal cost avoidance of $8,800 per BSI prevented
� 2004: 38 BSIs
� 2005: 13 BSIs
� 2006: 8 BSIs
� 2007: 8 BSIs
St. Joseph Mercy Health SystemJuly 2004 to December 2007
$ 220,000 marginal cost avoidance
between 2004 and 2005

Our Next Steps
� Implement the CHG Bath in all ICUs
� Explore the use of the CHG dressing
� Explore use of antimicrobial/antiseptic CVC
catheters in certain high risk populations

Keys to Success
� Team in place with key stakeholders overseeing implementation
� Project coordinator with lead clinical staff on each unit
� Strong physician leadership on team
� Education of staff through use of BSI checklist
� Empowerment of nursing staff to prevent errors
� Administrative support to help manage barriers
� Review data monthly for opportunities for improvement (if further analysis is needed can use Learn from a Defect Tool )
� Support from state-wide collaborative

Prevention of Sternal Wound Infections Following Cardiac Surgery
Ginger S. Pierson MSN, RN, CCRN, CNSCardiovascular & Critical Care CNS
CNS, New Grad RN Program
Hoag Hospital,
Newport Beach, California

Surgical Site Infections
� Post-operative infection is a major cause of patient injury, mortality and healthcare costs
� A surgical site infection (SSI) is defined as:� An infection that develops within 30 days after an operation
� Occurs within one year, if an implant was placed, and relates to the surgery
� It is estimated that approximately 500,ooo to 750,000 surgical site infections (SSI) occur annually in the USA
Rhee, H. & Harris, B., Infection Control Today, March, 2008

Surgical Site Infections (SSI)
� Patients who develop an SSI –� Require significantly more medical care
� Are 60% more likely to spend time in ICU
� May have an ↑ LOS by ~ 2 weeks
� Have twice the mortality (cardiac surgery patients ↑↑)
� SSIs develop in almost 2% of patients after discharge and are five times as likely to be readmitted
Rhee, H. & Harris, B., Infection Control Today, March, 2008

� Surgical Infection Prevention (SIP) Project developed in 2002
� National, collaborative quality initiative to substantially reduce surgical mortality and morbidity through collaborative efforts
� SCIP became the expanded project to include surgical complications in 2005 by CMS and the CDC
Fitzgerald, J. et. al, Nursing Management, Nov, 2007, 35

SCIP Steering Committee
� American College of
Surgeons
� American Hospital
Association
� American Society of
Anesthesiologists
� Association of
Peri-Operative RNs
� Agency for Healthcare
Research and Quality
� Centers for Medicare &
Medicaid Services
� Centers for Disease Control
and Prevention
� Department of Veteran’s
Affairs
� Institute for Healthcare
Improvement
� Joint Commission on
Accreditation of Healthcare
Organizations

SIP/SCIP National Expert Panel
� Society for Healthcare Epidemiology of America
� Association of Peri-Operative Registered Nurses
� American Association of Critical Care Nurses
� American College of Obstetricians & Gynecologists
� Society of Thoracic Surgeons
� Surgical Infection Society
� VHA, Inc.
� American Academy of Orthopedic Surgeons
� American Society of Anesthesiologists
� American Society of Health System Pharmacists
� American Geriatrics Society
� And more………..

SCIP- Opportunity to Prevent
Surgical Site Infections
� Evidence shows that approximately 40 – 60% of SSIs can be prevented
� GOAL: To reduce incidence of surgical complications by 25% by the year 2010*(*in selected surgical procedure patients)

SCIP Selected Surgical Procedures
� Cardiac Surgery
♥ Coronary Artery Bypass Graft (CABG)
� Colon
� Hip & Knee Arthroplasty
� Abdominal & Vaginal Hysterectomy
� Vascular Surgery:
� Aneurysm repair
� Thromboendarterectomy
� Vein Bypass

SCIP Quality Initiatives and Application to
Cardiac Surgery Patients
� Appropriate use of prophylactic antibiotics� Antibiotic selection
� Timing of administration
� Timing for discontinuation post-op
� Appropriate hair removal and skin prep
� Controlled post-operative serum glucose

Deep Sternal Wound
Following Cardiac SurgeryCDC and DHS definition:� Infection occurs within 30 days of surgery AND
� Involves the deep, soft tissues (fascial and muscle layers) of the incision AND
� Patient has at least ONE of the following:� Purulent drainage from the deep incision
� Incision spontaneously dehisces or is deliberately opened by the surgeon and is culture +, or fever, pain or tenderness
� Abscess/ infection found on exam, re-operation, histopathology or radiologic exam
� Diagnosis of deep incisional SSI is made by the surgeon/attending MD
CDC& DHS, National Healthcare Safety Network Manual, October, 2007

Who is at Risk for Sternal SSI?
Host Risk Factors:
� Obesity
� Diabetes Mellitus
� Use of IMA grafts
� Advanced age
� Male gender
� COPD
� Smoking
� Prolonged mechanical ventilation
� Steroids
� Pre-op hospital stay > 5 days
Surgical Risk Factors:
� Duration of surgery and perfusion time
� Use of an IABP
� Post-operative bleeding
� Re-operation
� Sternal re-wiring
� Extensive electrocautery
� Shaving with razors
� Use of bone wax
Hollenbeak, C. et. al., Chest, 2000, 118(20):397

Prophylactic Antibiotic Selection
and Timing for Cardiac Surgery
� Pre-op dose of 2 gm IV Cefazolin for a patient >60 kg body weight
� Repeat dose every 3- 4 hours (while surgical incision remains open)-if normal renal function
� If IgEIgE allergy to Penicillin or Cephalosporin: give Vancomycin
� Vancomycin dose of 1 to 1.5 gm IV or a weight-adjusted dose of 15 mg/kg administered IV slowly over 1 hour, with completion within 1 hour of skin incision
� A 2nd dose of Vanco 7.5 mg/kg can be considered during CPB
� Mupirocin topical antibiotic in nares pre-op and post-op
Engleman, R. et. al., STS, Annals of Thoracic Surgery, 2007;83: 1569-1576

Perioperative AntibioticsTiming of Administration
14/ 369
5/ 6995/ 1009
2/ 180
1/ 81
1/ 41
1/ 47
15/ 441
Classen, et al., N England J Med., 1992;328:281

Discontinuation of Antibiotics
SCIP Guidelines:
� Most surgical procedures- D/C antibiotics within
24 hours of surgery end time
� Cardiac surgery- may D/C antibiotics within 48 hours of
surgery end time
STS Guidelines: do not favor 24 hours over 48 hours for
discontinuation (surgeon/ team preference)
Hall, M., SCIP: Medscape.com, Module 1, May, 2006

Serum Glucose Control
� Strong relationship between hyperglycemia and surgical site infections
� Latham (2001) found that any cardiac surgery patient who had a serum glucose > 300 mg/dl within 48 hours post-op, was 3.3 times more likely to develop SSI than if glucose was kept < 200 mg/dl
� Evidence supports keeping serum glucose levels
< 200 mg/dl in the peri-op and post-op phases
Latham, R, et. Al., Infection Control Hosp Epidemiol, 2001

Other Strategies
� Appropriate hair removal
� Clipped (never shave), just before surgery
� Adequate skin antisepsis/ pre-op skin preparation
� Agent with broad spectrum of activity
� Rapid onset
� Persistent effects
* Most common- Iodine, alcohol-based products and chlorhexidine (2% vs. 4%)
Rhee, H. & Harris, B., Infection Control Today, March, 2008
Hall, M., SCIP: Medscape.com, Module 1, May, 2006

Harris H et al Infection Control Today. March 2008: www.infecctioncontroltoday.com
� Methodology� Observational study with a pre & post intervention
period
� Baseline: Actively part of National SCIP program
� Pre-intervention pre-op prep was night before in home
showering or washing with 4% CHG solution
� Post intervention: Pre-op prep preformed with a pre-
packaged 2% CHG prep product with instructions on its
use
� Pre-package prep preformed at hospital prior to surgery
� Measured:
� Change in baseline SSI would occur with new prep
process

Harris H et al Infection Control Today. March 2008: www.infecctioncontroltoday.com
� Results:
� 25 SSI’s during
historical period out of
5174 procedures (rate
of 2.1%)
� 11 SSI’s during
interventional period
out of 4266
procedure(rate 0 .7%)
� 72% reduction

Other Strategies- Continued
� Mupirocin (Bactroban)-intranasal-recommended as a routine prophylactic measure to eradicate the nasal colonization of S. Aureus-including MRSA:
� Begin at least the day before surgery
� Continue for 2 – 5 days post-op
� Post-op wound care and dressing changes� No concensus on best practice
Engleman, R. et. al., STS, Annals of Thoracic Surgery, 2007;83: 1569-1576
Haycock, C., et. al, Journal of Cardiovascular Nursing, 2005, 20(5): 299-305

In Summary � Antibiotics selection: Give Cefazolin, if allergic- give
Vancomycin (and may consider aminoglycoside 1-2 doses)
� Antibiotics are infused/completed within 1 hour of surgical incision
� D/C antibiotics within 48 hours of end of surgery
� Maintain serum glucose < 200mg/dl peri-op & post-op
� Appropriate hair removal just before surgery; complete skin antisepsis
� Mupirocin intranasally pre-op and post-op

Project overview available at: www.medqic.org/scip






























