Embed Size (px)
Citation preview

Mark Wallace-Bell PhD RN
Heart Foundation
University of Canterbury
Health Sciences Centre

Income gapsHow many times richer are the richest fifth than the poorest fifth?
Wilkinson & Pickett, The Spirit Level www.equalitytrust.org.uk
Inequality...How much richer are the richest 20% in each country than the poorest 20%?

Wilkinson & Pickett, The Spirit Level
Index of: •Life expectancy•Math & Literacy
•Infant mortality•Homicides•Imprisonment•Teenage births •Trust•Obesity•Mental illness – including drug & alcohol addiction
•Social mobility
www.equalitytrust.org.uk
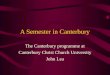
Health and social problems are worse in more unequal countries
Ind
ex
of h
ea
lth a
nd
so
cia
l pro
ble
ms

Social Relations
• Child conflict• Homicide• Imprisonment• Social capital• Trust
Bigger income gaps lead to deteriorations in:-
Human Capital
• Child wellbeing• High school drop outs• Math & literacy scores• Social mobility• Teenage births
Health
• Drug abuse• Infant mortality• Life expectancy• Mental illness• Smoking• Obesity

More inequality
• More superiority and inferiority• More status competition and
consumerism• More status insecurity
• More worry about how we are seen and judged
• More “social evaluation anxiety”(threats to self-esteem & social
status, fear of negative judgements
Valued or Devalued?
Smoking as a response to stress
caused by inequality?

The cycle of smoking and disadvantage
Social disadvantage and deprivation:
adverse circumstances (Unemployment, lone parenthood, transience etc)
stress isolation smoking as “normal” unsafe neighbourhoods limited recreation
Smoking prevalence: increased smoking less successful quitting higher relapse
Creates vulnerability to smoking:
as a means of coping with difficult circumstances
as a response to stress and exclusion
as an ‘affordable’ recreation
Makes circumstances worse: less money for essentials greater financial stress poorer health and wellbeing
Source: Cancer Council NSW

7
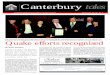
Health inequalities in NZ
50
55
60
65
70
75
80
85
1950 1960 1970 1980 1990 2000 2010
Lif
e e
xp
ec
tan
cy
in
ye
ars
Non-Mäori (SNZ) Male Non-Mäori (SNZ) Female
Mäori (SNZ) Male Mäori (SNZ) Female
Mäori (NZCMS) Male Mäori (NZCMS) Female
Māori (MoH latest) Male Māori (MoH latest) Female
Source: Blakely T, et al. Soc Sci Med 2005:2233-2251. N Z Med J 2008;121:7-11.

8
Changes in life expectancy in 2040 if everyone stopped smoking in Aotearoa by 2020?
Compared to the 2006 census smoking rates continuing into the future, if nobody smokes tobacco from 2020 onwards we estimate that by 2040 there will be:
about 5 years of additional life expectancy for Māori (range 2.5 to 7.9 years)
about 3 years of additional life expectancy for non-Māori (range 1.2 to 5.4 years)
and therefore about a 2 year closing in ethnic gaps in life expectancy (range 0.3 to 4.6 years)
Blakely, Carter, Wilson, Edwards, Woodward, Thomson, Sarfati. In press. NMZJ

9
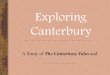
20/20 vision on 2040: Achieving health equity
0
10
20
30
40
50
60
70
80
90
1840 1860 1880 1900 1920 1940 1960 1980 2000 2020 2040
Non-Mäori (SNZ) Male
Non-Mäori (SNZ)Female
Māori pre WWII Male
Māori pre WWIIFemale
Mäori (SNZ) Male
Mäori (SNZ) Female
Māori (correcting forundercount) Male
Māori (correcting forundercount) Female
Projected non-Māori2.0% Male
Projected non-Māori2.0% Female
Projected Māori 3.5%Male
Projected Māori 3.5%Female
Going smokefree as a nation by 2025 is
an important step to achieving health equity by 2040

10
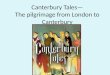
Smoker support for change
0 10 20 30 40 50 60 70 80
Regulating tobaccocompanies more tightly
Government doing more totackle the harm done by
smoking
Increasing the tax ontobacco**
Government setting a dateto ban cigarette sales in 10
years time*
% Support
Maori European/Other
Edwards et al NZ Med J 2009
Views on tobacco control policies

11
An endgame strategy
The endgame plan should include:
Community engagement to build support
A clear end date for commercial sales – sinking lid
Clear adjunct policies to reduce both supply and demand of tobacco – to ensure equity and facilitate impact
Built-in reviews at crucial stages (eg, at 1% prevalence for all groups)

12
Community engagement Essential at risk communities part of the
process Strategies:
Working with communitiesRecognise leadership and advocates for
EndgameMass media

The Vision
Future generations of New Zealand children will be free from exposure
to tobacco and will enjoy tobacco free lives

What’s happening
1 January 2012 tax increase
Removal of displays
Increasing smokefree out-door environments
Reduction in supply, improvements in cessation support

Roll on plain packaging!!

Why it matters Fifty percent of all smokers die from diseases directly
caused by smoking – that's means over 300,000 New Zealanders will die before their time.
Of those who die, they die on average 15 years earlier than their non-smoking peers, and most with deteriorating quality of life.
According to the WHO, between 80,000 and 100,000 children worldwide start smoking each day – and approximately a quarter of the children alive in the Western Pacific region will die from smoking.
Smoking is directly responsible for a quarter of all cancer deaths in New Zealand.

The difference you make
The ABC approach is endorsed because of its strong evidence base when linked with the role of health professionals. Evidence shows:– an estimated 20 percent of smokers will
go on to make a quit attempt in a six month period following a GP visit
– if all smokers were given brief advice to quit then the proportion of smokers making a quit attempt would increase to 25 percent

The difference you make– this can be further increased (by 40
percent) to 35 percent if this advice to quit is followed up with an offer of support to quit
– furthermore, people seem to be willing to accept this offer.
– The evidence is clear: even just a brief offer of support is enough to prompt people to quit.

The influence you have
You advise just one smoker every day to quit (time taken = 30 seconds)
Over 40 days this would have taken up 20 minutes of your time, but one of those 40 people will quit long term*
Over 1 year and you will have prompted six people to stop smoking, using about 2 hours effort from you
Consider that by investing two hours of your time in that year, you’ve saved three of those people’s lives!
*Silagy C, Stead LF. Physician advice for smoking cessation. Cochrane Database Syst Rev

Take home messages
You have an important influence in prompting people to quit
You can help people stop smoking
Medicines work but are not magic cures
Medicines work even better with ‘wrap around’ behavioural support
Don’t give up helping your patients to give up