Embed Size (px)
Citation preview
1
Mark Levine MD Department of Oncology
McMaster University Hamilton Ontario Canada
2
Prevention of Cancer-Associated Thrombosis: Where Are We Today?
3
Risk of Thrombosis
• Rates of thrombosis reported in literature vary because of case selection
• Wide range - 1% to 20%
• Rate is influenced by tumor burden, as reflected by tumor stage
• Venous thrombosis is more common than arterial thrombosis
4
Primary Prevention: Clinical States on Cancer Continuum
• Hospitalized post surgery
• Hospitalized medical
• Ambulatory medical i.e. receiving anti-cancer treatment (chemotherapy, endocrine, molecular targeted, radiation)
• Palliative
5
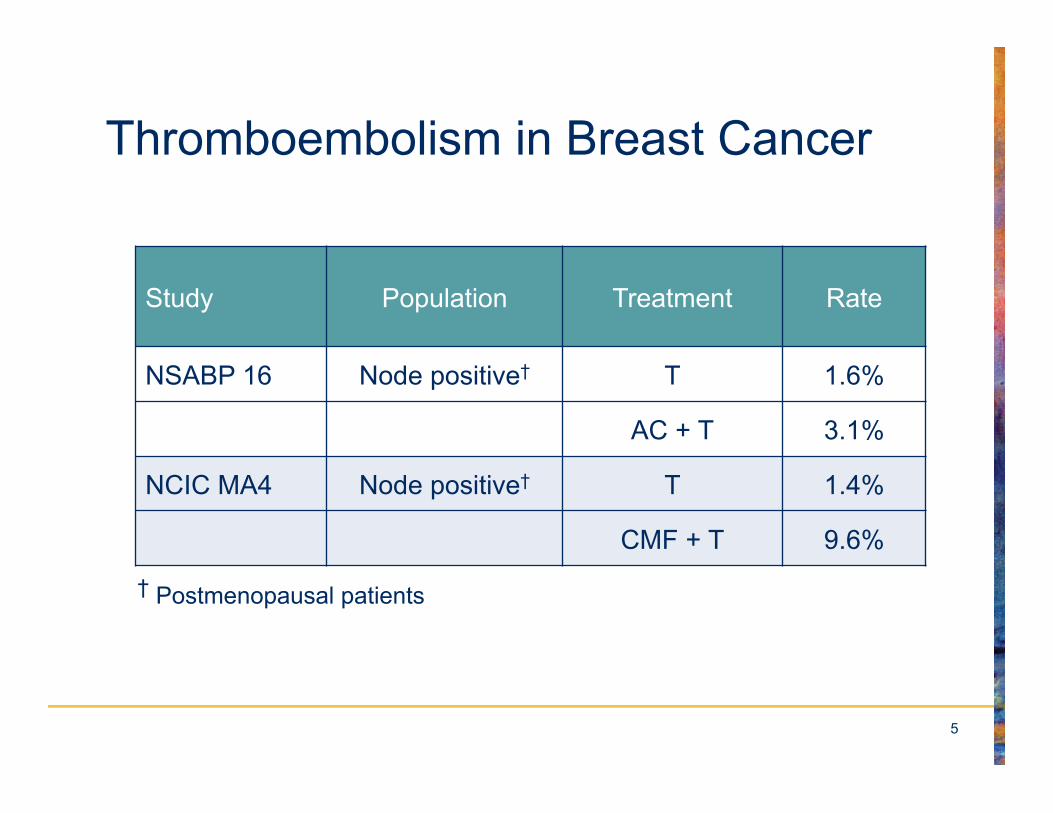
Thromboembolism in Breast Cancer
Study Population Treatment Rate
NSABP 16 Node positive† T 1.6%
AC + T 3.1%
NCIC MA4 Node positive† T 1.4%
CMF + T 9.6%
† Postmenopausal patients
6
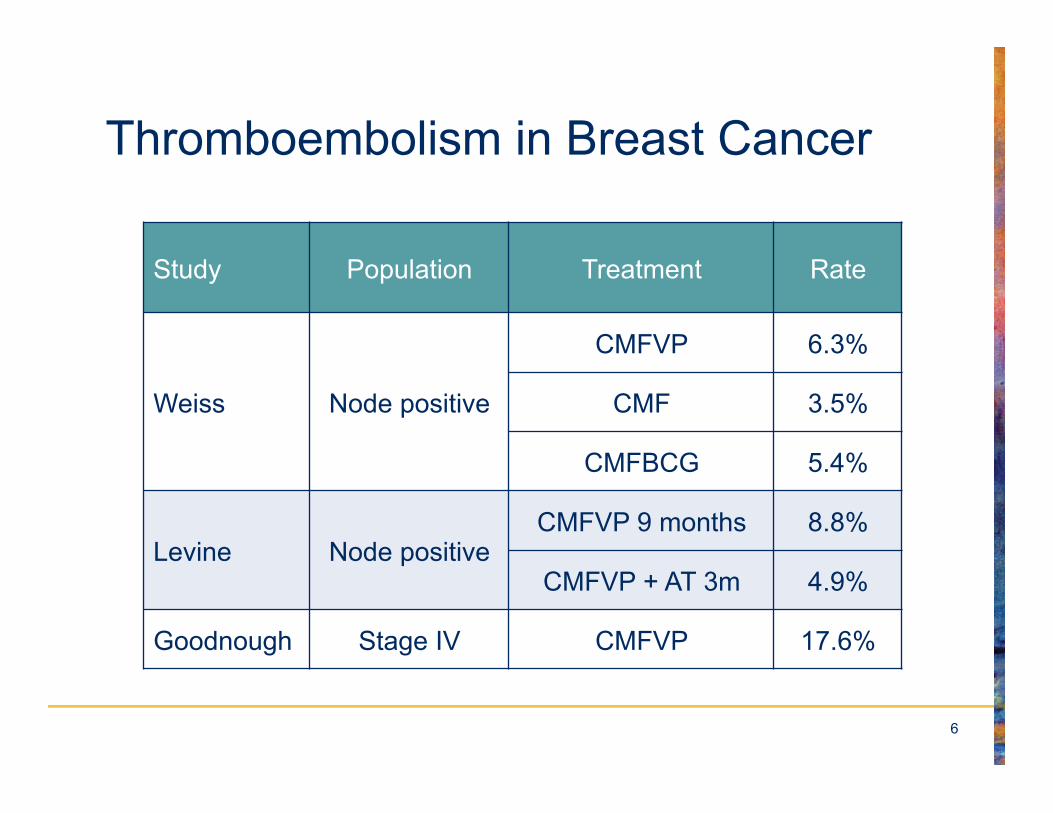
Thromboembolism in Breast Cancer
Study Population Treatment Rate
Weiss Node positive
CMFVP 6.3%
CMF 3.5%
CMFBCG 5.4%
Levine Node positive CMFVP 9 months 8.8%
CMFVP + AT 3m 4.9%
Goodnough Stage IV CMFVP 17.6%
7
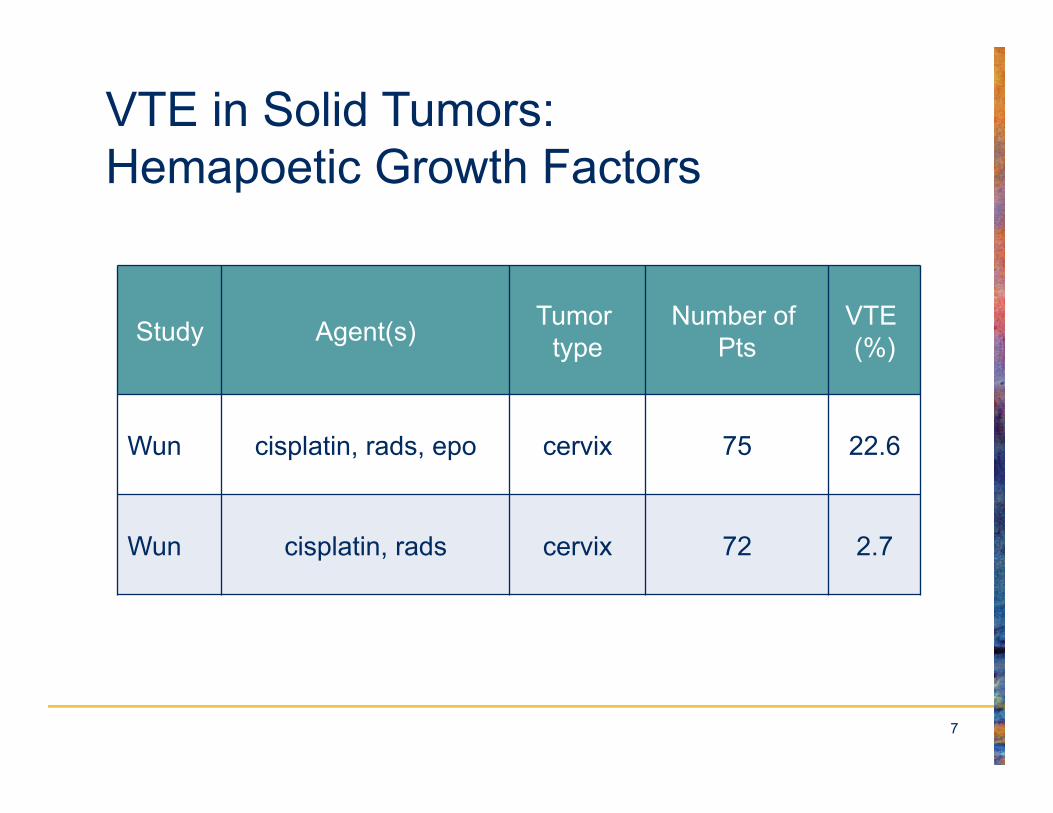
VTE in Solid Tumors: Hemapoetic Growth Factors
Study Agent(s) Tumor type
Number of Pts
VTE (%)
Wun cisplatin, rads, epo cervix 75 22.6
Wun cisplatin, rads cervix 72 2.7
8
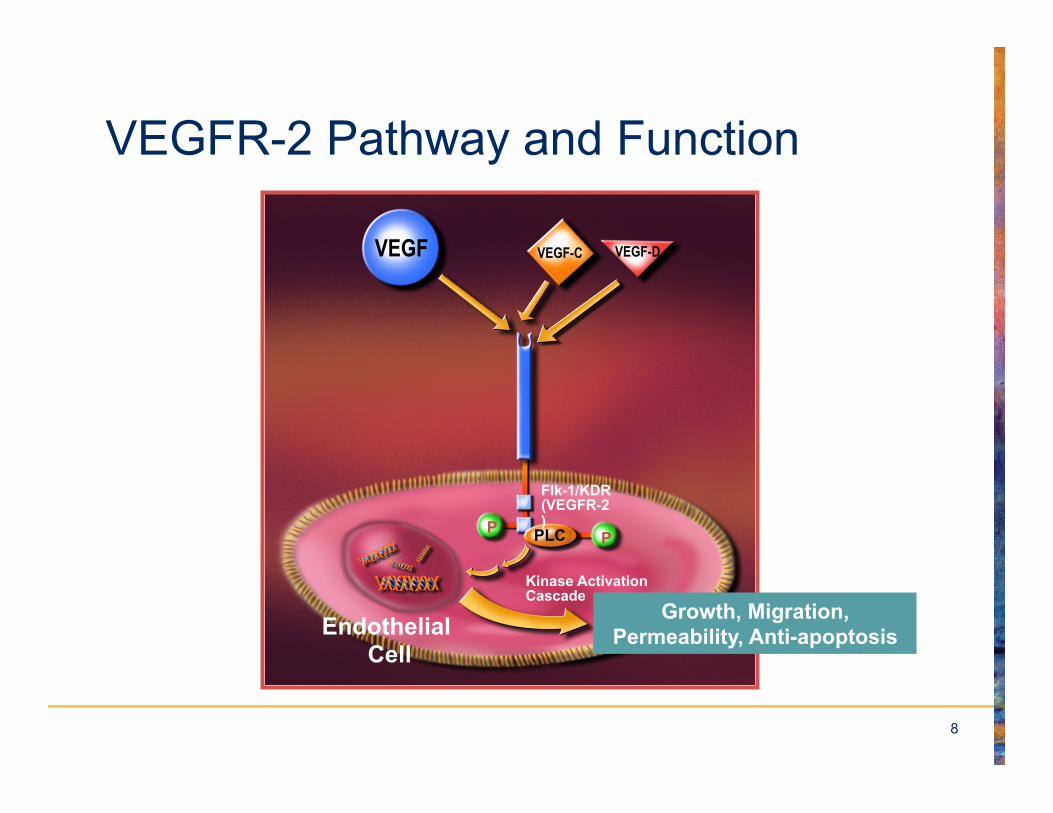
VEGFR-2 Pathway and Function
Endothelial Cell
Flk-1/KDR (VEGFR-2)
Growth, Migration, Permeability, Anti-apoptosis
VEGF
Kinase Activation Cascade
P PPLC
VEGF-C VEGF-D
9
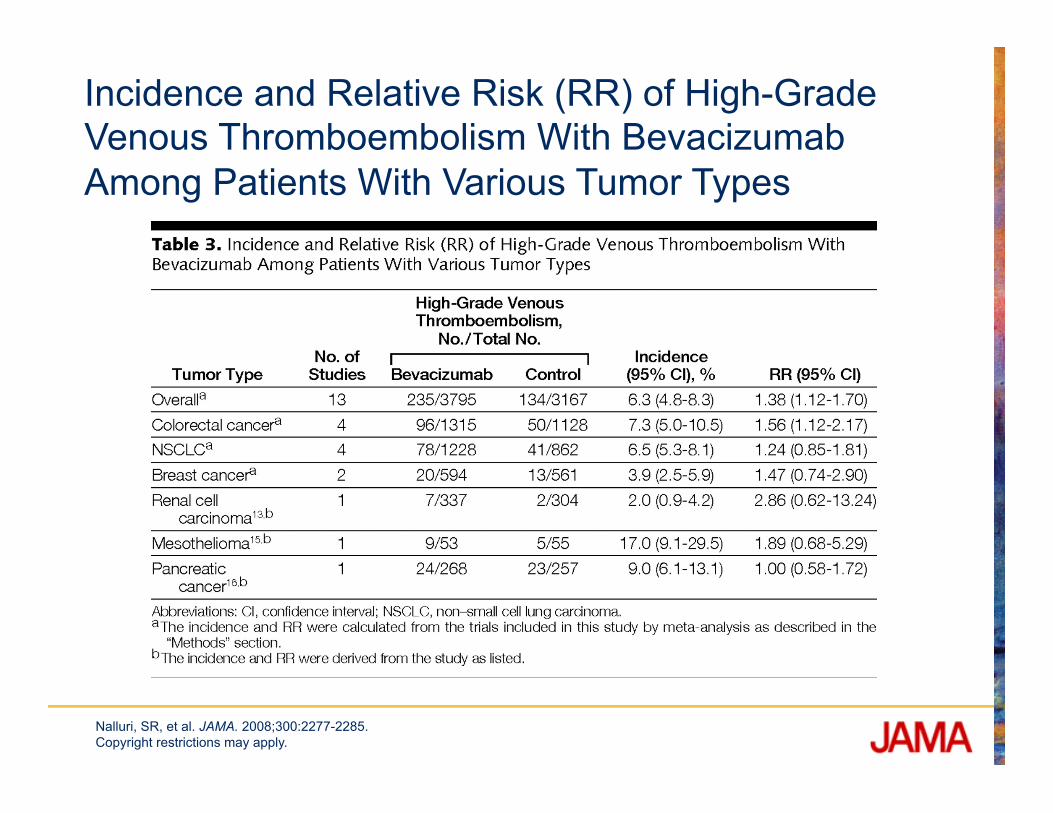
Incidence and Relative Risk (RR) of High-Grade Venous Thromboembolism With Bevacizumab Among Patients With Various Tumor Types
Nalluri, SR, et al. JAMA. 2008;300:2277-2285. Copyright restrictions may apply.
10
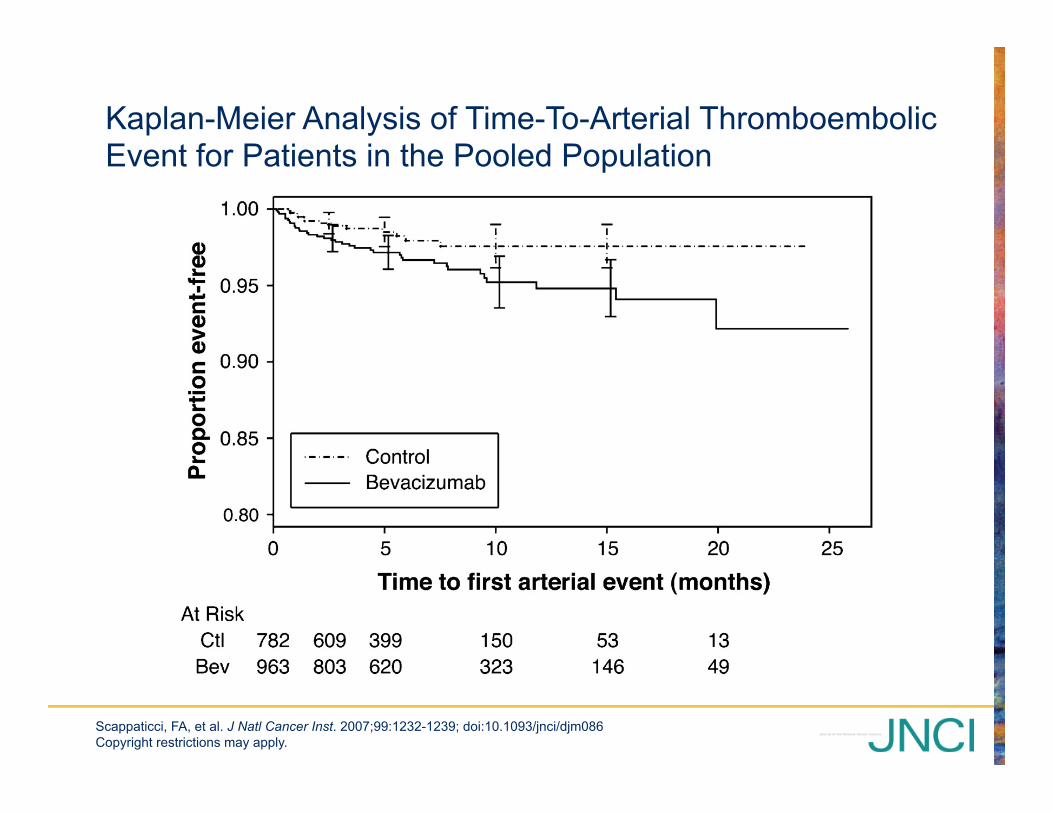
Kaplan-Meier Analysis of Time-To-Arterial Thromboembolic Event for Patients in the Pooled Population
Scappaticci, FA, et al. J Natl Cancer Inst. 2007;99:1232-1239; doi:10.1093/jnci/djm086 Copyright restrictions may apply.
11
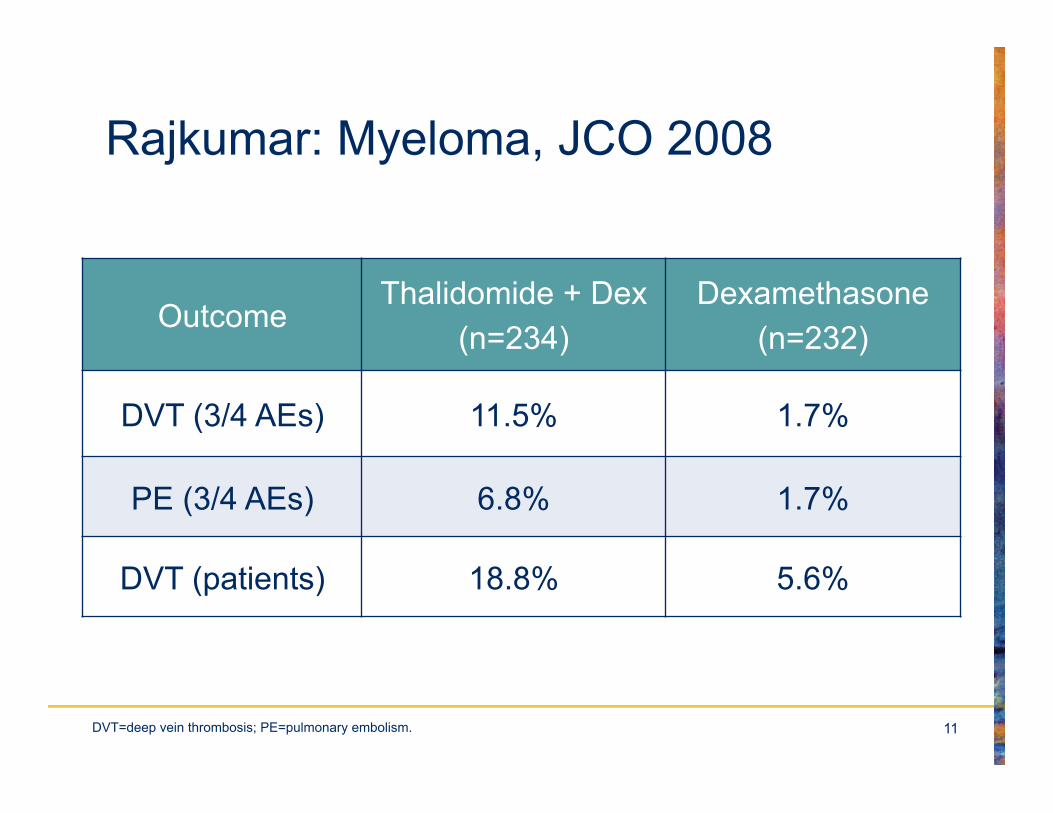
Rajkumar: Myeloma, JCO 2008
Outcome Thalidomide + Dex
(n=234) Dexamethasone
(n=232)
DVT (3/4 AEs) 11.5% 1.7%
PE (3/4 AEs) 6.8% 1.7%
DVT (patients) 18.8% 5.6%
DVT=deep vein thrombosis; PE=pulmonary embolism.
12
Incidental PE on Imaging for Staging
13
Should I Give Prophylaxis?
Reduction in thrombosis
Increase in bleeding
14
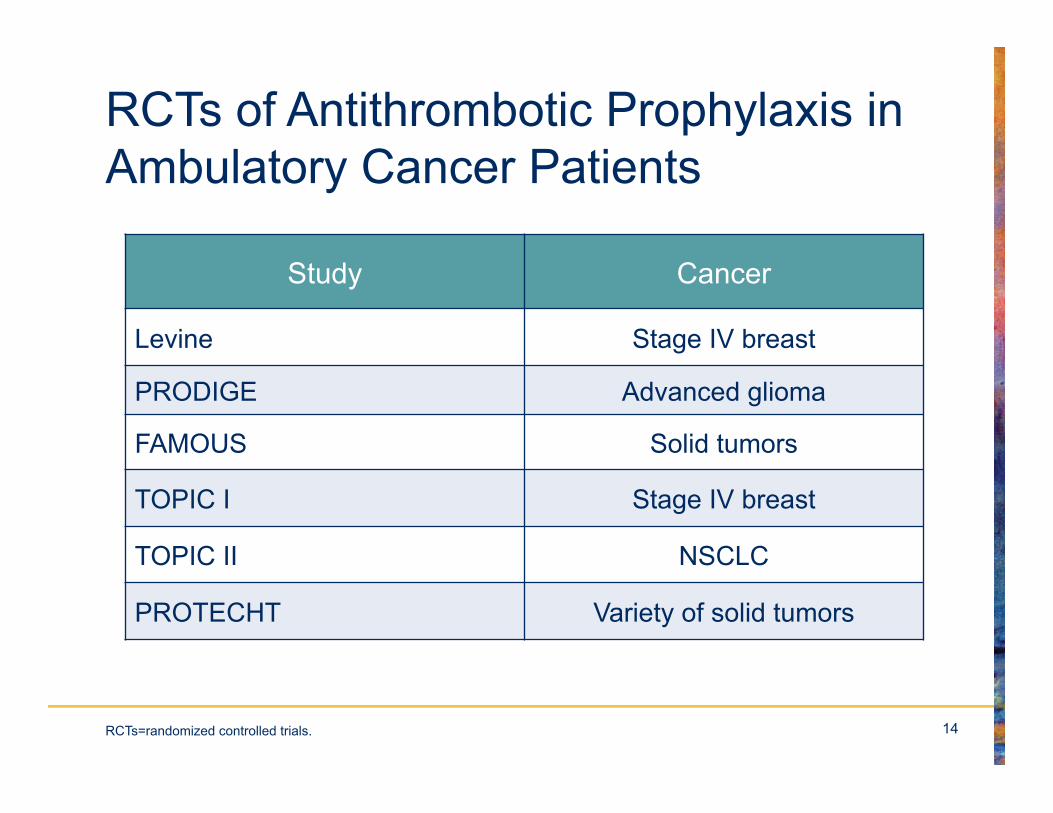
RCTs of Antithrombotic Prophylaxis in Ambulatory Cancer Patients
Study Cancer
Levine Stage IV breast
PRODIGE Advanced glioma
FAMOUS Solid tumors
TOPIC I Stage IV breast
TOPIC II NSCLC
PROTECHT Variety of solid tumors
RCTs=randomized controlled trials.
15
Thromboprophylaxis Levine et al. Lancet 1994; 343, 886-9
• 311 women with metastatic breast cancer on 1st or 2nd line chemotherapy
• Randomized to 1 mg warfarin for 6 weeks, then warfarin titrated to INR 1.3-1.9 or placebo
• 7 events vs.1 (85% risk reduction, P=0.03 with no increased bleeding)
INR=international normalized ratio.
16
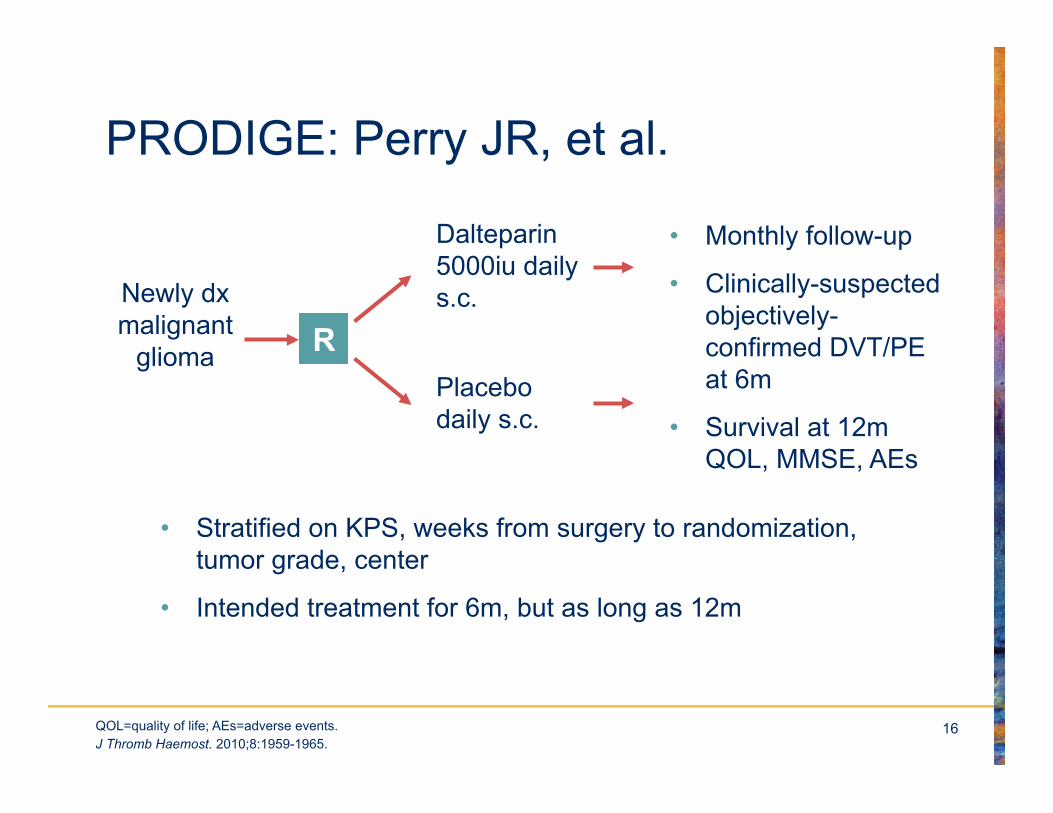
PRODIGE: Perry JR, et al.
• Monthly follow-up
• Clinically-suspected objectively-confirmed DVT/PE at 6m
• Survival at 12m QOL, MMSE, AEs
Newly dx malignant
glioma R
Dalteparin 5000iu daily s.c.
Placebo daily s.c.
• Stratified on KPS, weeks from surgery to randomization, tumor grade, center
• Intended treatment for 6m, but as long as 12m
J Thromb Haemost. 2010;8:1959-1965. QOL=quality of life; AEs=adverse events.
17
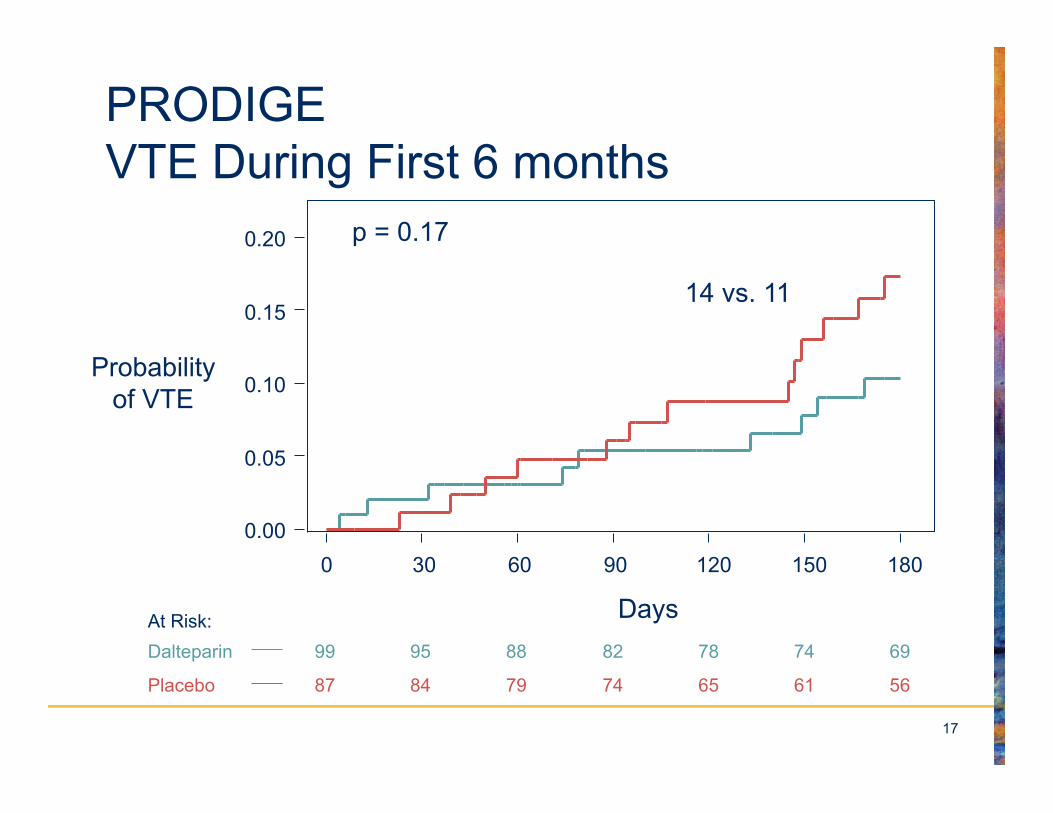
PRODIGE VTE During First 6 months
Placebo 87 84 79 74 65 61 56
Dalteparin 99 95 88 82 78 74 69 At Risk:
0.00
0.05
0.10
0.15
0.20
Days 0 30 60 90 120 150 180
Probability of VTE
p = 0.17
14 vs. 11
18
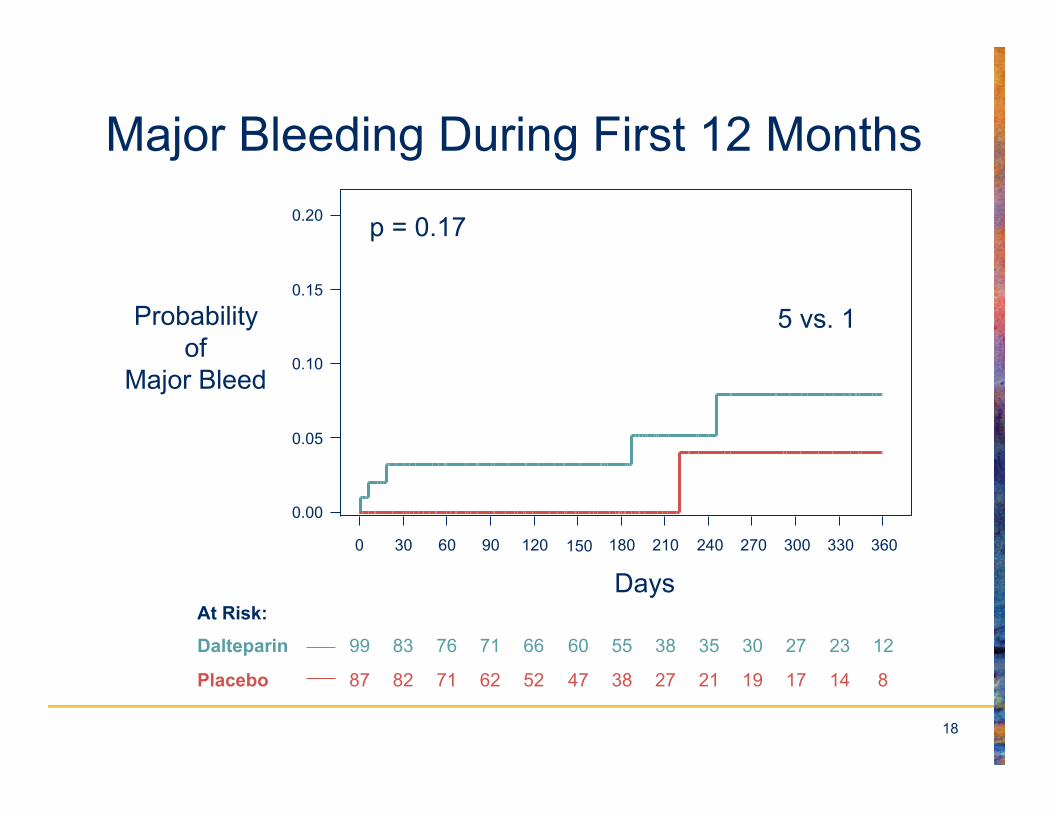
Major Bleeding During First 12 Months
240
Placebo 87 82 71 62 52 47 38 27 21 19 17 14 8
Dalteparin 99 83 76 71 66 60 55 38 35 30 27 23 12
At Risk:
0.00
0.05
0.10
0.15
0.20
0 30 60 90 120 180 210 270 300 330 360
Probability of
Major Bleed
p = 0.17
5 vs. 1
150
Days
19
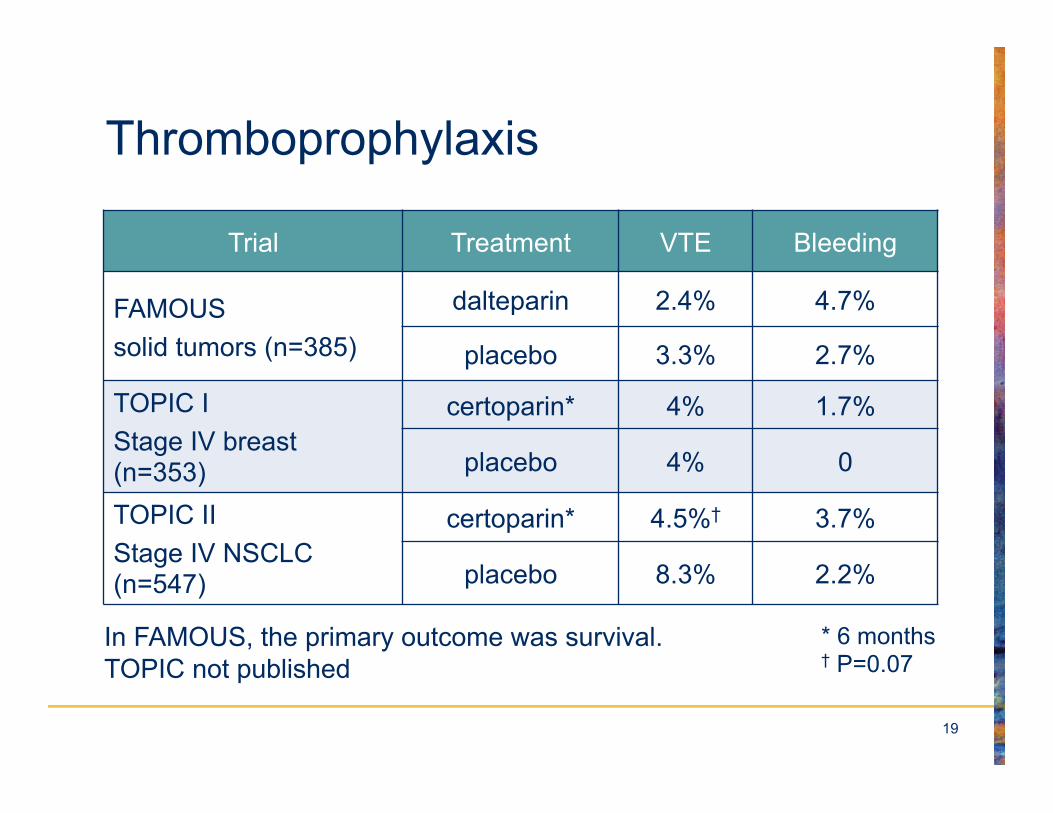
Thromboprophylaxis
Trial Treatment VTE Bleeding
FAMOUS solid tumors (n=385)
dalteparin 2.4% 4.7%
placebo 3.3% 2.7%
TOPIC I Stage IV breast (n=353)
certoparin* 4% 1.7%
placebo 4% 0
TOPIC II Stage IV NSCLC (n=547)
certoparin* 4.5%† 3.7%
placebo 8.3% 2.2%
In FAMOUS, the primary outcome was survival. TOPIC not published
* 6 months † P=0.07
20
PROTECHT: Agnelli et al.
• Ambulatory patients with lung, GI, pancreas, breast, ovarian, head & neck cancer
• Randomized in a 2:1 ratio to nadroparin (779) or placebo (387) for up to 4 months
• Rate of VTE, 2% versus 3.9%, P= 0.02 1-tailed
• 5 (0.7%) major bleeds vs. 0, P=0.18 2-tailed
The Lancet Oncology, Volume 10, Issue 10, Pages 943 - 949, October 2009
21
Myeloma
• Many observational studies of prophylaxis
• 2 RCTs
– 659 on thalidomide randomized to ASA, Warfarin and LMWH (thrombosis = 6.4%, 8.2%, 5.0%, respectively)
– 342 patients treated with lenalidomide-based chemotherapy randomized to low-dose ASA (100 mg) or enoxaparin (VTE = 2.3% vs.1.2%)
Palumbo A, et al. J Clin Oncol. 2011;29:986-993. Larocca A, et al. Blood. 2012;119:933-939.
ASA=acetylsalicylic acid (aspirin); LMWH=low molecular weight heparin.

22
Direct Thrombin & Anti Factor Xa Inhibitors
*Direct thrombin inhibitor
a TF VII
IX
Xa X
IXa
II Va
IIa
VIIIa
Fibrinogen Fibrin
IIa
DTI*
Anti Xa
23
ABLE Trial
• A multi-center, randomized, double-blind, phase II 4-arm trial was conducted.
• Patients with metastatic cancer on 1st or 2nd line chemotherapy received study drug once daily for 12 weeks
• dose of 5, 10 or 20 mg of Apixaban or placebo.
Levine MN, et al. J Thromb Haemost. 2012;10:807-814.
24
ABLE
• The primary outcome measure was:
– proportion of patients remaining free of major bleeding (MB), clinically relevant non-major bleeding (CRNMB), VTE, and grade >3 adverse events (AE) considered to be probably/definitely related to study drug.
25
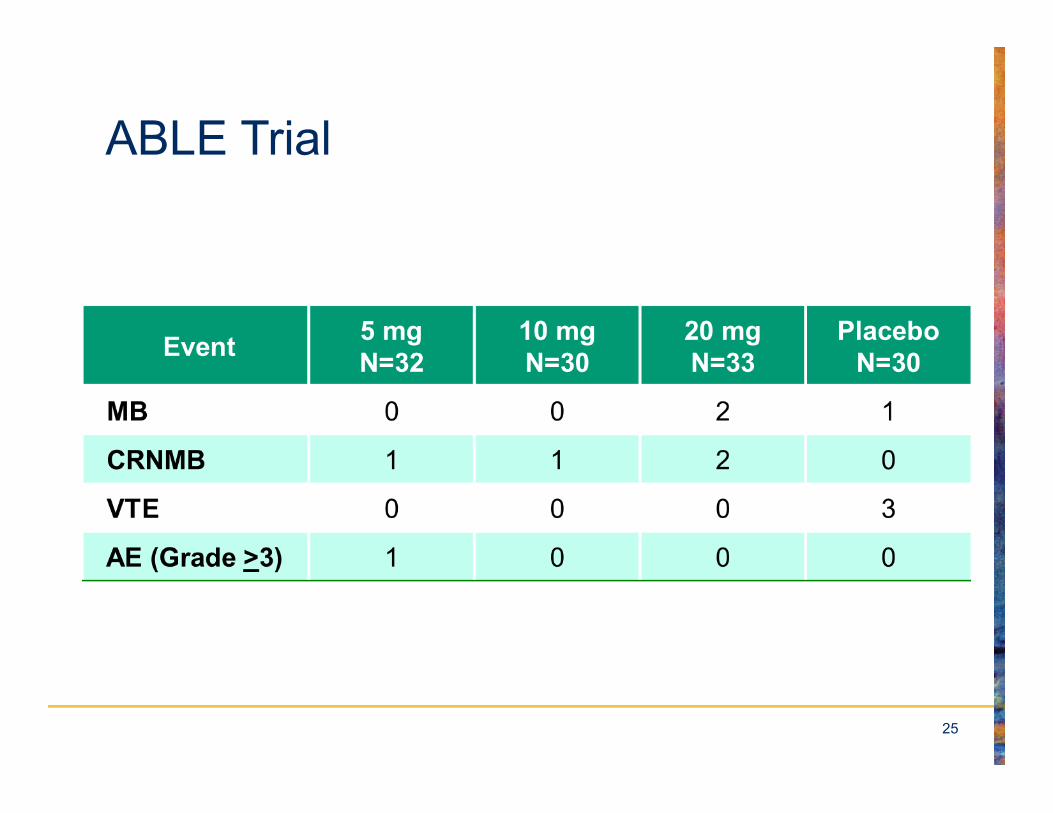
ABLE Trial
26
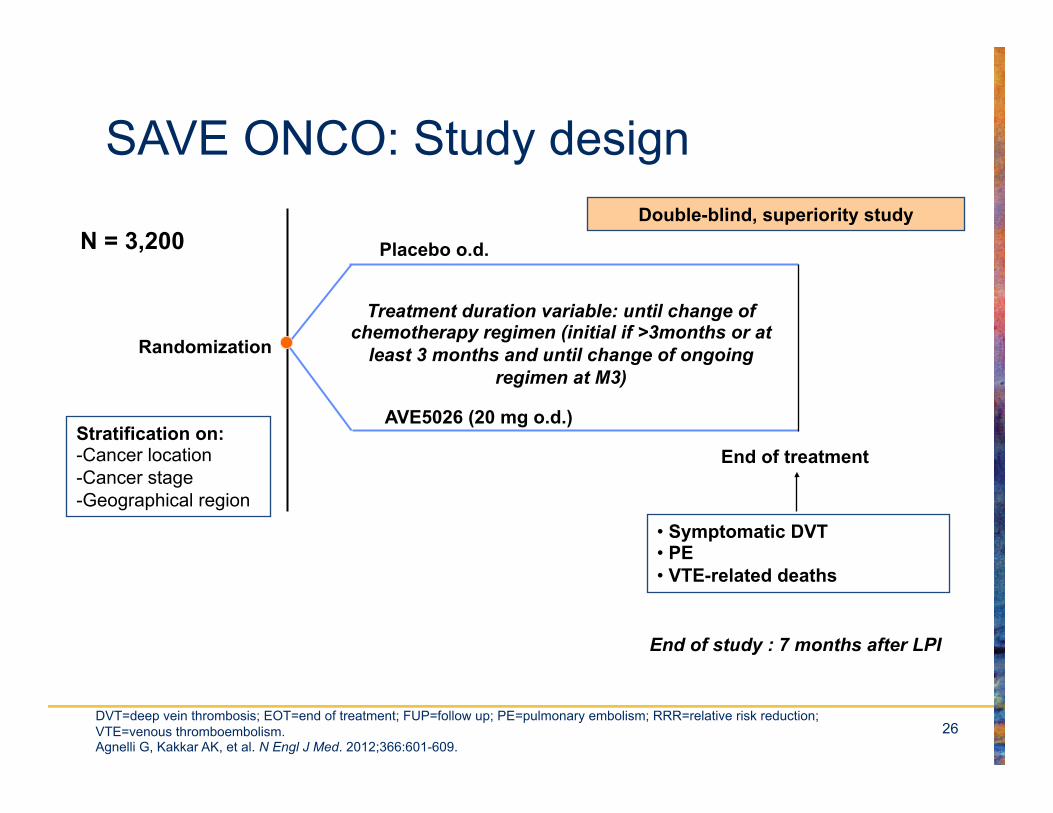
SAVE ONCO: Study design
Randomization
Placebo o.d.
AVE5026 (20 mg o.d.)
End of treatment
Treatment duration variable: until change of chemotherapy regimen (initial if >3months or at
least 3 months and until change of ongoing regimen at M3)
• Symptomatic DVT • PE • VTE-related deaths
End of study : 7 months after LPI
Stratification on: - Cancer location - Cancer stage - Geographical region
Double-blind, superiority study N = 3,200
DVT=deep vein thrombosis; EOT=end of treatment; FUP=follow up; PE=pulmonary embolism; RRR=relative risk reduction; VTE=venous thromboembolism. Agnelli G, Kakkar AK, et al. N Engl J Med. 2012;366:601-609.
27
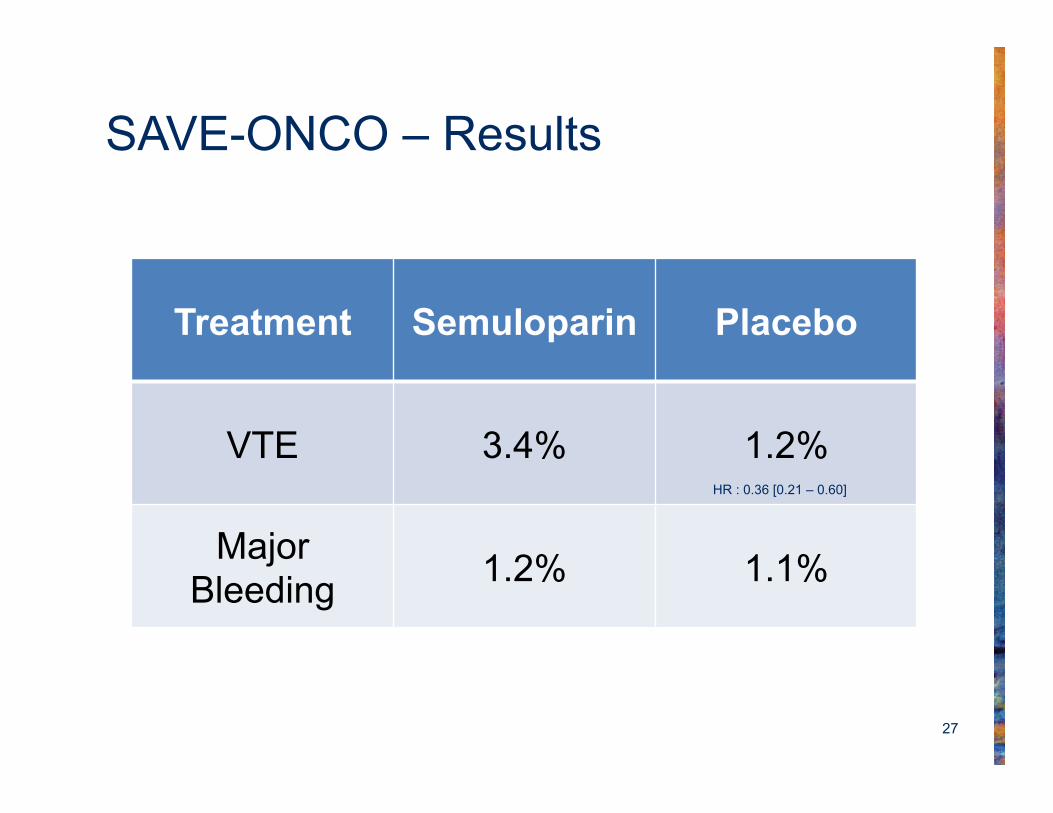
SAVE-ONCO – Results
Treatment Semuloparin Placebo
VTE 3.4% 1.2%
Major Bleeding 1.2% 1.1%
HR : 0.36 [0.21 – 0.60]
28
Biomarkers to Predict Thrombosis
• Elevated WBC
• Elevated platelets
• D-dimer
• P-selectin
• F1+2
• TF micro particles
Pabinger I, et al. Blood. 2013;122:2011-2018. WBC=white blood cell count.
29
30
Questions & Challenges
• What is the baseline rate of thrombosis that would warrant prophylaxis? – Don’t know
– Very difficult to predict rate for an individual patient
– Risk changes over time
– Duration of prophylaxis could be many months
31
Questions & Challenges
• What is the magnitude of thrombosis reduction with prophylaxis?
• Is there Level I evidence?
– Levine 85% RR but baseline rate 4%
– Agnelli 50% RR but baseline rate 3.9%
RR=relative risk.
32
Questions & Challenges
• What is the down-side (“hassle factor”) of prophylaxis?
– Bleeding
– Monitoring test of coagulation
– Subcutaneous injections
33
Questions & Challenges
• What is the ideal prophylactic agent? – Warfarin is inexpensive but requires laboratory
monitoring
– LMWH requires daily subcutaneous injection and is expensive in North America
– Both warfarin and LMWH may cause bleeding
– Lack of data on new anti-thrombotics
– No ideal agent
34
Stick Factors
• VTE Prophylaxis for the patient on chemotherapy:
– Safe
– Effective
– Hassle-free
– Cheap
35
Prevention of Cancer-Associated Thrombosis: Where are we Today?
I Don’t Know
36
Recommendation: ASCO 2013
• Thromboprophylaxis is not routinely recommended for outpatients with cancer, but may be considered for selected high-risk patients.
• Patients with multiple myeloma receiving thalidomide- or lenalidomide-based regimens with chemotherapy and/or dexamethasone should receive pharmacologic prophylaxis with either aspirin or LMWH for lower risk patients and LMWH for higher-risk patient
J Clin Oncol 2013: 31,2189-2204.
37
What is Central Vein Catheter-Associated Thrombosis (CVCAT)?
• No venous flow
• Fibrin sheath
• Ball valve clot
• Venous thrombosis of large vein (subclavian, axillary vein)
• We don’t even know what it is!
38
Is it a Frequent Problem?
• Lee et al. conducted a prospective study (JCO 2006;24,404)
• 444 cancer patients with CVCs were followed for 12 months (76,713 patient days)
• 19 (4.3%) developed symptomatic CVCT
• 0.3 per 1000 catheter days
CVCs=central venous catheters; CVCT=central venous catheter thrombosis.
39
Is it Clinically Important?
• Post phlebitic syndrome is not a problem in this population
• If CVC is still working, then it is still used
• Symptomatic pulmonary embolism is a rare occurrence
40
What is the Most Appropriate Outcome of Prevention of CVCAT?
• It must be a clinical outcome, e.g. painful swollen arm with or without CVC obstruction
• It is not asymptomatic obstruction on screening venogram
41
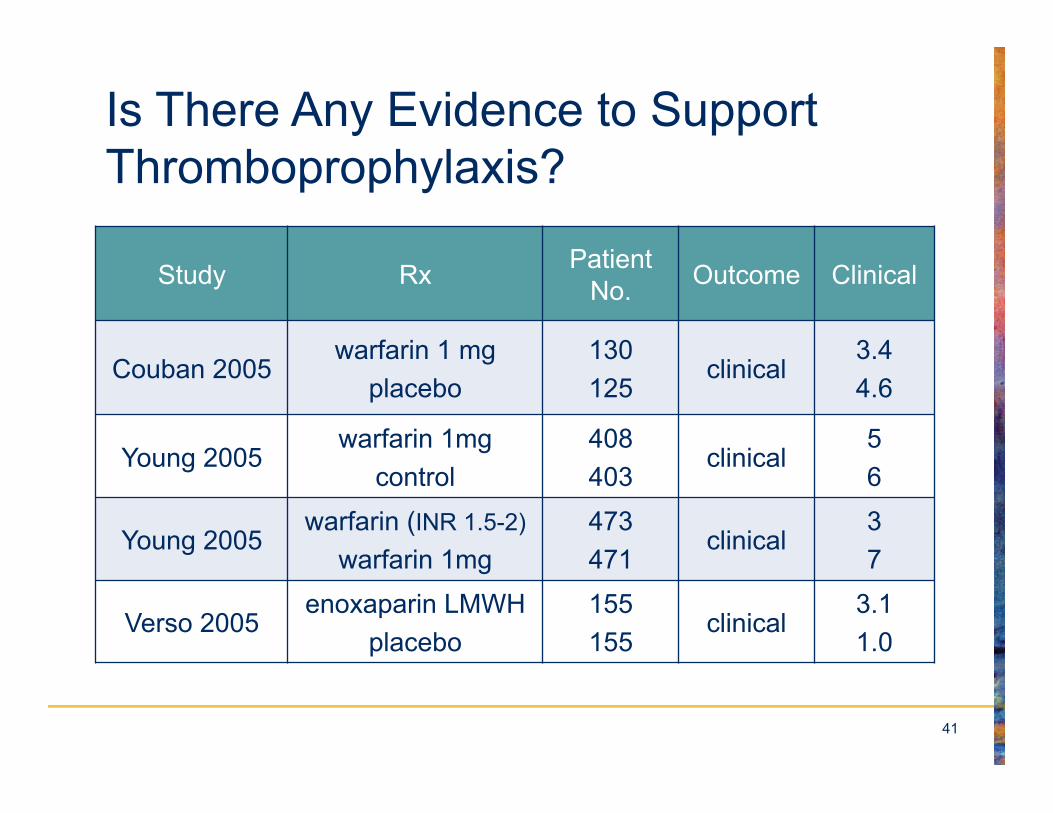
Is There Any Evidence to Support Thromboprophylaxis?
Study Rx Patient No. Outcome Clinical
Couban 2005 warfarin 1 mg
placebo 130 125
clinical 3.4 4.6
Young 2005 warfarin 1mg
control 408 403
clinical 5 6
Young 2005 warfarin (INR 1.5-2)
warfarin 1mg 473 471
clinical 3
7
Verso 2005 enoxaparin LMWH
placebo 155 155
clinical 3.1 1.0
42
ASCO Catheter Guideline
• Prophylactic use of warfarin or low–molecular weight heparin is not recommended
Schiffer CA, et al. J Clin Oncol. 2013:31;1357-1370.
43
Recommendation: ASCO 2013
• Most hospitalized patients with cancer require thromboprophylaxis throughout hospitalization
• Patients undergoing major cancer surgery should receive prophylaxis, starting before surgery and continuing for at least 7 to 10 days.
• Extending prophylaxis up to 4 weeks should be considered in those with high-risk features. LMWH
Lyman GH, et al. J Clin Oncol. 2013;31:2189-2204.