Embed Size (px)
Citation preview

3/11/2015
1
Pathophysiology of the diseases of the blood:Pathophysiology of the diseases of the blood:
Anemias and haemorhagic Anemias and haemorhagic ggdiathesesdiatheses
Blagoi Marinov MD PhDBlagoi Marinov MD PhDBlagoi Marinov, MD, PhDBlagoi Marinov, MD, PhD
Pathophysiology DepartmentPathophysiology Department
Medical University of PlovdivMedical University of Plovdiv
Haemopietic system
Blood production
Blood wasting
3/11/2015
2
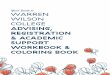
Haemopoiesis Haemopoiesis
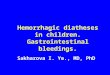
Blood Blood -- structure structure
4-5 L

3/11/2015
3
Characteristics of normal Characteristics of normal ErEr
Highly elastic bi concave discsHighly elastic bi concave discs ((55..10101212))..
Without nucleus and mitochondriaWithout nucleus and mitochondria(anaerobic metabolism).(anaerobic metabolism).
Contain large quantities of enzyme carbonic Contain large quantities of enzyme carbonic h dh danhydraseanhydrase
Lifecycle ~ 120 days.Lifecycle ~ 120 days.
Structure and function of Structure and function of HbHb
90% of the protein content of Ers is haemoglobin.90% of the protein content of Ers is haemoglobin.
•• transportstransports OO22 and part of the COand part of the CO22..•• represents mighty buffer systemrepresents mighty buffer system
3/11/2015
4
DefinitionDefinition
AnemiasAnemias are diseases of the blood having less are diseases of the blood having less than the normal number of red blood cells or less than the normal number of red blood cells or less than the normal quantity of hemoglobin in the than the normal quantity of hemoglobin in the blood. The oxygenblood. The oxygen--carrying capacity of the blood carrying capacity of the blood is, therefore, substantially decreased.is, therefore, substantially decreased.
ClassificationsClassifications
ClinicalClinical ClinicalClinical AcuteAcute SubacuteSubacute ChronicChronic
Erythrocytes morphologyErythrocytes morphology MicrocyticMicrocytic MacrocyticMacrocytic ((megaloblasticmegaloblastic)) SpherocyticSpherocytic
HaemoglobinHaemoglobin contentcontent HypochromicHypochromic HyperchromicHyperchromic

3/11/2015
5
PathogeneticPathogenetic classification classification of of anemiasanemias
HaemorrhagicHaemorrhagic anemiasanemiasHaemorrhagicHaemorrhagic anemiasanemias
Impaired Impaired erythroproductionerythroproduction((depressed erythropoiesisdepressed erythropoiesis))
IncreasedIncreased erythrodestructionerythrodestruction((pathologic pathologic haemolysishaemolysis))
Lab tests to consider in Lab tests to consider in anemic statesanemic states

3/11/2015
6
Hemorrhagic anemiasHemorrhagic anemias
HAEMORRHAGE SpeedQuantity HAEMORRHAGE pQ y
Hemodilution S
ANEMIA Time
Hb , Ers , Hct
Hyperkinetic circulation
Activated erythropoiesisC
OM
PEN
SATI
ON
S
Anemias due to impaired Anemias due to impaired erythroproductionerythroproduction
Impaired synthesis of haemoglobinImpaired synthesis of haemoglobin Impaired synthesis of haemoglobinImpaired synthesis of haemoglobinFeFe deficitdeficit
Altered DNA synthesisAltered DNA synthesisBB1212 defectdefectFolate deficitFolate deficit
HH dd l ti il ti i HypoHypo-- andand aplastic anemiasaplastic anemiasIdiopaticIdiopatic (ЕРО(ЕРО** insensitiveinsensitive))Erythropoietin deficitErythropoietin deficit
**ЕРОЕРО -- ErythropoietinErythropoietin

3/11/2015
7
Iron metabolismIron metabolism
FeFe--deficient anemias deficient anemias --etiologyetiology
Chronic haemorrhagesChronic haemorrhages Chronic haemorrhagesChronic haemorrhages Increased physiologic requirementsIncreased physiologic requirements Decreased FeDecreased Fe--uptakeuptake Altered FeAltered Fe--transformationtransformation
Decreased FeDecreased Fe absorptionabsorption Decreased FeDecreased Fe--absorptionabsorption Improper FeImproper Fe--transport to hemopoietic transport to hemopoietic
organsorgans

3/11/2015
8
FeFe--deficient anemias deficient anemias --etiologyetiology
Stages
of Fe deficiency

3/11/2015
9
FeFe--deficient anemias deficient anemias --pathogenesispathogenesis
Decrease of the Fe stores in the organismDecrease of the Fe stores in the organismDecrease of the Fe stores in the organismDecrease of the Fe stores in the organism Prelatent FePrelatent Fe--deficitdeficit
FeritinFeritin Intestinal absorptionIntestinal absorption
Latent FeLatent Fe--deficitdeficit SerumSerum Fe Fe FeritinFeritin total iron binding capability (TIBC) total iron binding capability (TIBC)
Manifest FeManifest Fe--deficient anemiadeficient anemia Ers Ers ; Hb ; Hb ; MCV ; MCV ; ;
FeFe--deficient anemia :deficient anemia :Ers morphologyErs morphology
Fe-deficient anemia is microcytic and hypochromic !!!

3/11/2015
10
FeFe--deficient anemias deficient anemias --signs and symptomssigns and symptoms
Megaloblastic anemia Megaloblastic anemia --etiologyetiology
Autosomal recessive inheritance
Genetic predispositionGenetic predisposition –– HLAHLA--A3, A3, HLAHLA--B7B7
Autosomal-recessive inheritance (Addison-Biermer anemia)
Auto AB againstAuto AB against:: Parietal cells in the gastric mucosaParietal cells in the gastric mucosa
GastromucoproteinGastromucoprotein

3/11/2015
11
Vit BVit B1212 metabolismmetabolism
Megaloblastic anemia Megaloblastic anemia -- pathogenesispathogenesis
3/11/2015
12
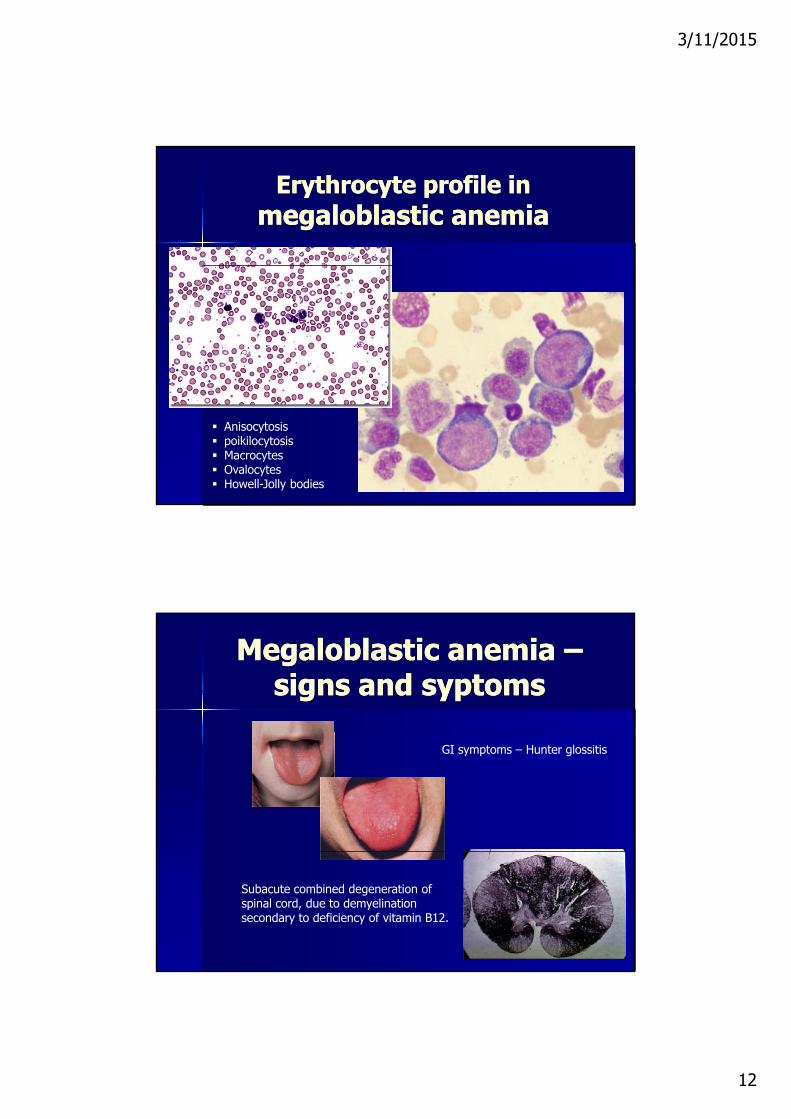
Erythrocyte profile in Erythrocyte profile in megaloblastic anemiamegaloblastic anemia
Anisocytosis poikilocytosis Macrocytes Ovalocytes Howell-Jolly bodies
Megaloblastic anemia Megaloblastic anemia ––signs and syptomssigns and syptoms
GI symptoms – Hunter glossitis
Subacute combined degeneration of spinal cord, due to demyelination secondary to deficiency of vitamin B12.

3/11/2015
13
SecondarySecondary mmegaloblastic egaloblastic anemiaanemiass
Primary liver diseasePrimary liver disease
Surgical interventions on the stomach Surgical interventions on the stomach and intestinesand intestines
Neoplastic processesNeoplastic processes
Parasitic diseasesParasitic diseases
MedicationsMedications ((cytostatics, cytostatics, immunosuppressors, antiepilepticsimmunosuppressors, antiepileptics))
Hypo- and aplastic anemias
Pluripotentstem cell
Radiation
Cytostatics
A ibi i
Replicationdefects
StimulatoryIL 1Antibiotics
Antithyroid drugs
Benzol derivatives
Viral infections
Metastases
Genetic defects
Stimulatorydefficit
Inhibitory effect
T-suppressormechanism
Apoptosismechanism
IL - 1
IL - 6
IL - 3
STEMCELLS
Leukopoesis Erythropoesis
Thrombopoesis
Bone marrow insufficiency (PANCYTOPENIA)

3/11/2015
14
Anemias due to iAnemias due to increased ncreased erythrodestructionerythrodestruction
InbornInborn ((inheritedinherited))InbornInborn ((inheritedinherited))Disorders in the structure of Er membraneDisorders in the structure of Er membraneDisorders in Ers enzymatic contentDisorders in Ers enzymatic contentDisorders in the synthesis of the globin moleculeDisorders in the synthesis of the globin molecule
HaemoglobinosesHaemoglobinoses ThalassemiasThalassemias
AcquiredAcquiredImmunologic mechanismsImmunologic mechanisms
IsoimmuneIsoimmune Drug inducedDrug induced ((haptenshaptens)) AutoimmuneAutoimmune
SymptomaticSymptomatic ((secondarysecondary) )
Anemias due to disorders in Anemias due to disorders in the structure of Er membranethe structure of Er membrane
Microspherocytosis (M Minkowski Chauffard)
Quantitative and qualitative changes of Quantitative and qualitative changes of membrane protein membrane protein spectrin spectrin ((autosomal dominant trait)
Disturbance in ATP metabolismDisturbance in ATP metabolism
Decreased activity of the enzyme Decreased activity of the enzyme proteinkinaseproteinkinase
Microspherocytosis (M. Minkowski-Chauffard)
Spectrin deficit
Increased permeability
Shortened life cycle
Haemolytic anemia
3/11/2015
15
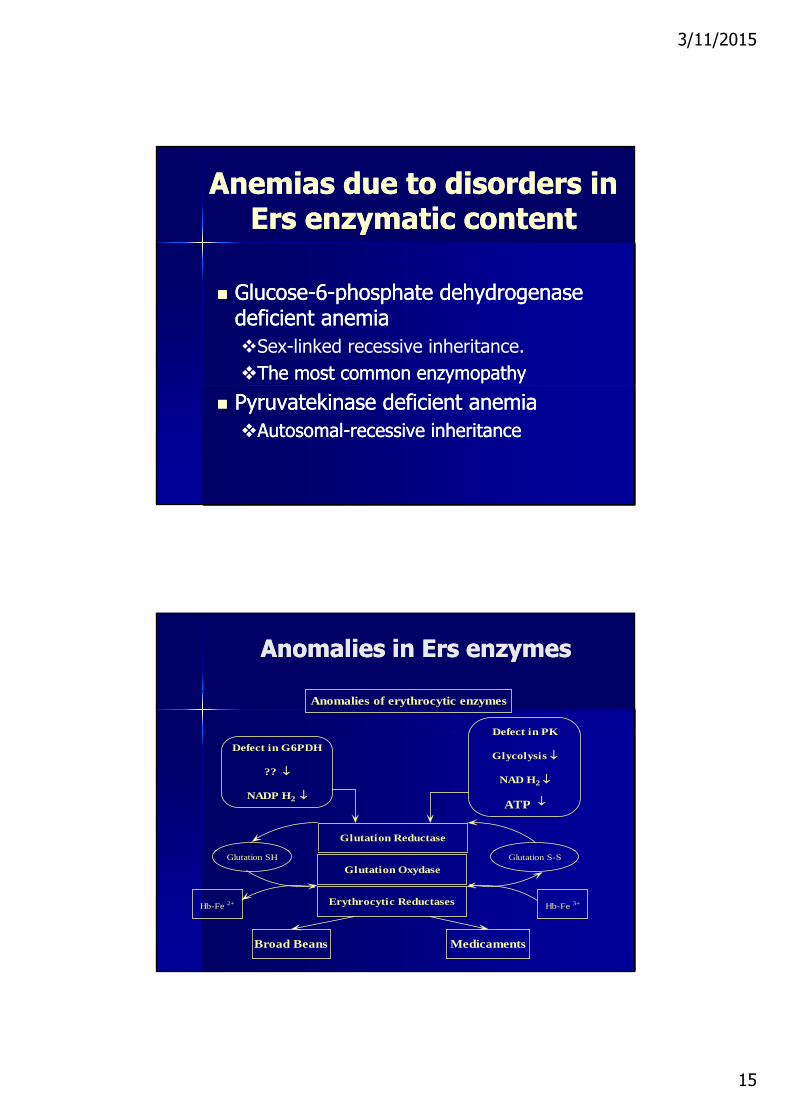
Anemias due to dAnemias due to disorders in isorders in Ers enzymatic contentErs enzymatic content
GlucoseGlucose--66--phosphate dehydrogenase phosphate dehydrogenase deficient anemiadeficient anemiaSex-linked recessive inheritance.The most common enzymopathyThe most common enzymopathy
Pyruvatekinase deficient anemiaPyruvatekinase deficient anemiaAutosomalAutosomal--recessive inheritancerecessive inheritance
Anomalies in Ers enzymesAnomalies in Ers enzymes
Anomalies of erythrocytic enzymes
Defect in PK
Glutation Reductase
Defect in G6PDH
??
NADP H2
Defect in PK
Glycolysis
NAD H2
ATP
Glutation Oxydase
Erythrocytic Reductases
Broad Beans Medicaments
Glutation SH
Hb-Fe 2+
Glutation S-S
Hb-Fe 3+
3/11/2015
16
G6PD
Genetic defectsGenetic defects Deficit of Deficit of G6PD Impaired glutathione synthesisImpaired glutathione synthesis Oxygen stressOxygen stressygyg Denaturation of hemoglobinDenaturation of hemoglobin Hemolysis of Ers with enzyme defectsHemolysis of Ers with enzyme defects
ThalassemiasThalassemias
Beta thalassemiasBeta thalassemias Beta thalassemiasBeta thalassemiasHomozygotic formHomozygotic form ((--thalassemia mayor, thalassemia mayor,
Morbus Cooley)Morbus Cooley)Heterozygotic forms (Heterozygotic forms (--thalassemia minor)thalassemia minor)
Alpha thalassemiasAlpha thalassemiasHomozygotic formHomozygotic formHeterozygotic formsHeterozygotic forms

3/11/2015
17
Thalassemia mayor Thalassemia mayor (M. Cooley)(M. Cooley)
Abnormally high quantity of Hb FAbnormally high quantity of Hb F and and Hb AHb A2 2 is synthesisedis synthesised
Due to deficit or inappropriate Due to deficit or inappropriate synthesis of synthesis of --chains in Ers there is an chains in Ers there is an excess of uncoupledexcess of uncoupled --chainschainsexcess of uncoupled excess of uncoupled chainschains
The uncoupled The uncoupled --chains precipitatechains precipitate The permeability of Ers is increasedThe permeability of Ers is increased HemolysisHemolysis
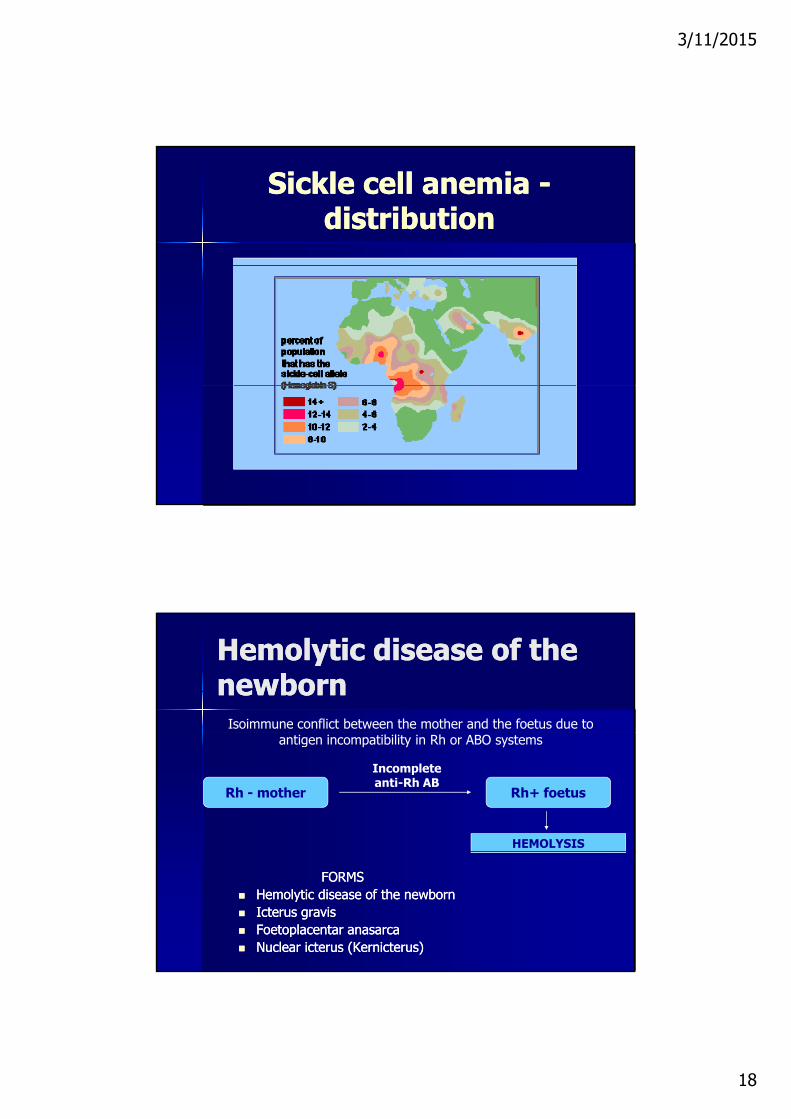
Sickle cell anemiaSickle cell anemia
I i d h i th i ith f ti fImpaired -chain synthesis, with formation ofpathologic haemoglobin S
Hardly soluble in liquids
homozygote
OXY-state DEOXY- state
Haemoglobin crystals in hypoxic environment
heterozygote
3/11/2015
18
Sickle cell anemia Sickle cell anemia --distributiondistribution
Hemolytic disease of the Hemolytic disease of the newbornnewborn
Isoimmune conflict between the mother and the foetus due to antigen incompatibility in Rh or АВО systems
Rh - mother Rh+ foetus
Incompleteanti-Rh АB
HEMOLYSIS
FORMSFORMS Hemolytic disease of the newbornHemolytic disease of the newborn Icterus gravisIcterus gravis Foetoplacentar anasarcaFoetoplacentar anasarca Nuclear icterus (Kernicterus)Nuclear icterus (Kernicterus)

3/11/2015
19
Acquired autoimmune Acquired autoimmune anemiasanemias
Types of antibodiesTypes of antibodies
I l t h t l ti iI l t h t l ti i
Autoimmune conflict between specific AB and body’s own unchanged erythrocyte antigens
Incomplete heat agglutininsIncomplete heat agglutinins
Heat hemolysisnsHeat hemolysisns
Complete cold agglutininsComplete cold agglutinins
BiBi--phase hemolysinsphase hemolysins
Bone marow transplantationBone marow transplantation

3/11/2015
20
Hemorrhagic diatheses
IntrinsicPathway
ExtrinsicPathway
CommonPathway

3/11/2015
21
Hemorrhagic diatheses
Coagulation abnormalities Coagulation abnormalities
Quantitative and qualitative platlet abnormalities (thrombocitopenias & thrombocitopathias)thrombocitopathias)
Damage to the vascular wall(vasopathies)
Hemophilia
Disorder of hemostasis a coagulopathy Disorder of hemostasis, a coagulopathy Hemophilia A - Factor VIII deficiency Hemophilia B – Factor IX deficiency
Hemophilia C – Factor XI, XII
Prevalence: 13.4 cases per 100,000 males Incidence: 1 in 5032 live male births

3/11/2015
22
Queen Victoria
How do you get it? Hemophilia is a genetic disease and is passed on by the X
chromosome (the chromosome that carries the clotting factor)chromosome (the chromosome that carries the clotting factor). If a boy gets the X chromosome that carries the hemophilia
gene he will become a hemophiliac. If a girl get the gene, she will become the carrier of the gene,

3/11/2015
23
Severity of Factor Deficiencies
Severe: <1% Severe: <1%– Hemarthrosis with minimal trauma or ADLs
Moderate: 1 to 5%– Intermediate symptoms with fewer
hemarthroses
Mild: >5% Mild: >5%– Joint bleeds rarely develop except with
significant trauma
Hemophilic Arthropathy
As blood is catabolized it is absorbed by As blood is catabolized, it is absorbed by synovium
Iron is toxic to cells – synovial cells disintegrate releasing lysosomes which destroy cartilage and inflame synovium
Chondrocytes also affected
FIBROSIS

3/11/2015
24
1/3 of all Hospital Hematology Consults are1/3 of all Hospital Hematology Consults are
Thrombocitopenia
1/3 of all Hospital Hematology Consults are 1/3 of all Hospital Hematology Consults are for thrombocytopeniafor thrombocytopenia
5 to 10% of all hospitalized patients are 5 to 10% of all hospitalized patients are thrombocytopenic in the ICU the number thrombocytopenic in the ICU the number increases to 35%increases to 35%increases to 35%increases to 35%
Thrombocytopenic patients in the hospital Thrombocytopenic patients in the hospital suffer a twofold greater mortality rate than suffer a twofold greater mortality rate than those who are notthose who are not
Echymoses

3/11/2015
25
Platelet count Symptoms
Thrombocytopenia
Platelet count Symptoms
50-100,000 Prolonged bleeding following trauma
< 50,000 Easy bruisingPurpura following minor traumap g
< 20,000 Spontaneous bleedingPetechiaeMay suffer spontaneous internal and intracranial bleeding
Mechanisms of Thrombocytopenia
Decreased platelet production Decreased platelet production Increased platelet destruction Dilutional Thrombocytopenia Splenomegaly or splenic sequestration
Pseudothrombocytopenia Pseudothrombocytopenia
The primary reason for evaluating thrombocytopenia is to assess the The primary reason for evaluating thrombocytopenia is to assess the risk of bleeding and assess the presence of underlying disordersrisk of bleeding and assess the presence of underlying disorders
3/11/2015
26
Decreased Platelet Production
Factors causing bone marrow suppression Factors causing bone marrow suppression or damage
Viral illness HIV (direct damage to Megakaryocytes) Chemo- or radiation therapy Congenital or acquired bone marrow aplasia
or hypoplasia Vit. B12 or Folate deficiency
Increased Platelet Destruction
Idiopathic (Immune) Thrombocytopenic Purpura
Alloimmune destruction—Posttransfusion, Post-transplantation
Disseminated Intravascular Coagulation Disseminated Intravascular Coagulation Thrombotic Thrombocytopenic Purpura Antiphospholipid Antibody Syndrome Certain drugs—Heparin, quinidine, valproate

3/11/2015
27
Splenic Sequestration
Normally ~1/3 of platelets are sequestered Normally, 1/3 of platelets are sequestered in the spleen in any given time
In extreme splenomegaly, up to 90% of platelets can be trapped in the spleen
Cirrhosis, Portal HTN, splenomegaly can all present with apparent thrombocytopenia, although these pts are not usually at risk for clinical bleeding
Qualitative platelet disorders -thrombocytopathy
Hereditary Aquired
Glanzmann Drugs (aspirin)Thrombasthenia
Bernard Soulier disease
Plt granules deficiency
Inhibitors (Ab)
3/11/2015
28
Vasopathias
Schönlein-Henoch Purpura Schönlein-Henoch Purpura
Sympthomatic hemorrhagic vasculites Krimean hemorrhagic fever Measels
Hereditary vasopathias Rendu-Osler-Weber
Schönlein-Henoch Purpura anaphylactoid purpura
Schönlein-Henoch Purpura is a common vasculitis with cutaneous and systemic complications.
The usual location of the acute small vessel damage is primarily in the skin GI tract anddamage is primarily in the skin, GI tract, and kidneys
It is the most common cause of nonthrombocytopenic purpura in children.

3/11/2015
29
History
First described in 1801 by William Heberden, y ,a physician in London, who wrote about a case of a 5 year old boy with hematuria, abdominal pain, joint pains and a skin rash.
In 1837, Johann Schönlein and later in 1874, Edouard Henoch described multiple case reports of similar cases. They also showed an association of an upper respiratory infection preceding development of symptoms.
Pathogenesis
Likely mechanism thought to be an immune- Likely mechanism thought to be an immunecomplex mediated disease with deposits in the glomerular capillaries, dermal capillaries and GI tract.
Mesangial deposits of IgA are the same as Mesangial deposits of IgA are the same as those seen in IgA nephropathy

3/11/2015
30
Epidemiology
More frequent in children than adults, with More frequent in children than adults, with most cases occurring between 2 and 8 yr of age,
Most frequently in the winter months. The overall incidence is estimated to be
9/100 000 population9/100,000 population. Males are affected twice as frequently as
females.
Rash (95-100%) especially involving the
Clinical manifestations
Rash (95 100%), especially involving the legs, may not be present on initial presentation
Subcutaneous edema (20-50%) Abdominal pain and vomiting (85%)
Joint pain (60 80%) especiall in ol ing the Joint pain (60-80%), especially involving the knees and ankles
Scrotal edema (2-35%) Bloody stools

3/11/2015
31
Clinical Presentation
Petechiae Petechiae Purpura Ecchymoses
Arthritis
Present in more than ⅔ of children with HSP,
Is usually localized to the knees and ankles and appears to be concomitant with edema.
The effusions are serous, not hemorrhagic,
Resolve after a few days without residual deformity or Resolve after a few days without residual deformity or articular damage.
They may recur during a subsequent reactive phase of the disease.
3/11/2015
32
Gastrointestinal tract
Intermittent abdominal pain that is often colicky in tnature.
There may be peritoneal exudate, enlarged mesenteric lymph nodes, segmental edema, and hemorrhage into the bowel.
More than half of patients have occult heme-positive stools,
Diarrhea (with or without visible blood) or hematemesis Diarrhea (with or without visible blood), or hematemesis. Complete bowel obstruction or infarction with bowel
perforation.
Renal involvement
occurs in 25-50% of children
may manifest with: hematuria, proteinuria, or both; nephritis or nephrosis; acute renal failure acute renal failure.
Renal involvement at presentation may lead to chronic hypertension or end-stage renal disease in the future

3/11/2015
33
The ENDThe END
Have a wonderful day!