Embed Size (px)
Citation preview

MarinerMariner Health Care Health Care
QUALITY QUALITY ASSURANCE AND ASSURANCE AND MONITORING forMONITORING for
The HEALTH The HEALTH Information Information Management/Record Management/Record DepartmentDepartment

PRESENTED TO
February 15, 2010 (Northern Cal.)
February 16, 2010 (Southern Cal.)
Rhonda Anderson, RHIAPresident
Anderson Health Information Systems, Inc.940 W. 17th Street, Suite B
Santa Ana, CA 92706Tel. 714/558-3887 Fax 714/558-1302
OBJECTIVES
Participants will identify the key management principles for:– Managing the HIM/Record Department– Assuring a HIM/Record Department Evaluation is
followed up– Identifying those QA processes that are used as a
guiding principal for managing the facility.– Specifically reviewing the QA process as it relates
to managing audits
OBJECTIVES -2
Participants will…– Developing a plan for your own audit process and
follow up action plan – Identifying the ADM, MRD and HIM/Record
Consultant action/follow up.– Will review the HIPAA requirements – more
specific-- related to California Breaches regulations (SB541-SB337)
QI GOAL
Identify systems breakdown in audit process and develop and monitor interventions.
Identify those Health Information/Record Department requirements and how do you meet those.
Review of Consultant’s evaluation and what facility should do with the identified areas and recommendations.
QA PROCESS
Review of the QA Process Identify areas of concern/continuous quality
improvement processes, set out the goals, identify the criteria, collect data, identify measurement, evaluate and assess the information, analyze the causative factors, develop action plans and follow up – recycle!!

QA
Responsible for the overall direction of the facility’s quality improvement functions through a quality assessment/ improvement program/plan.
We will spend more time on this in the future workshops.
HIM/RECORD DEPARTMENT ORGANIZATION
Review of the HIM/Record Department organization and expectations.
HIM/Record Department Evaluation 1. Location of Items in the HIM/Record Dept
(H.O. #1)
2. The Basics of organization – what are some of the key areas to maintain organization? How? What to do? Discuss.

HIM/RECORD DEPARTMENT ORGANIZATION -2
HIM/Record Department Evaluation 3. Auditing and monitoring
policy/schedule/organization/follow – up – QA reports
4. What about HIPAA. Do you know the requirements. We will review later.
HIM/RECORD DEPARTMENT ORGANIZATION -3
Identify those Health Information Department items for improvement and documentation items from the HIM/Record Consultant.
WORKSHOP EXERCISE: – Determine for your facility those areas that need
improvement, then list them.– Reconcile for all the facilities.– Facility and Corporate action plan
TOP DEFICIENCIES & FOCUSED AUDITS
1. Quality of Care – identify those audits that would measure documentation, i.e., behavior drugs, falls, restraints, pain, etc.
2. Care Plans – Identify where the most deficiency is applicable to your facility; at C of Condition, after IT Team Quarterly Reviews with the MDS >> resultingin update of CP.
TOP 20 DEFICIENCIES & FOCUSED AUDITS -2
3. Pharmacy Procedures – results from the new pharmacy survey, RECAPS, med/tx Documentation, etc.
4. Measure against Unnecessary Drugs – Pharmacy QI include in QA process
5. Complete Records
H.O. #2 Top 20 Deficiencies
WHY PLAN FOR AUDITS AS WHY PLAN FOR AUDITS AS PART OF QAPART OF QA
In order to ensure that the documentation of the quality of care and services provided to all residents meets the needs of the residents and reflects high quality outcome of services and care process
Documentation supports those services and we can document the quality of services.
QA PROCESS
Identifies and addresses quality issues; including documentation items.
Provides a tool to coordinates the qualitative documentation activities of all departments.
Establishes assessment and improvement priorities for audits and follow up.
Sets expected outcomes for documentation of resident care, services and related administrative services;

RE-ADMISSION POLICY AND PROCEDURE
What is your procedure? Do you have a clear policy and procedure? Have you and the Consultant made sure it
meets requirements?
CALENDAR
Let us review the Calendar (H.O. #3) Identify items to ??? Yourself.
– Do you have all the required audits on the calendar?
– How do you schedule the monthly audits?– How do you schedule the treatment monitoring,
what days, what input from Nursing, etc.– Admission Audits

CALENDAR -2
Other required audits and timelines. – Have they changed?– Is the monitoring process in place.
What is the follow up process? What are your biggest challenges? How will you solve them? Who will you ask
to work with you?

QA AUDITS AND MONITORING
REVIEW of the Audit Compliance Grid– This is the ‘standard” (H.O. #4)
Let’s agree on a standard!– Get input from the facilities…
QA - PLANNING
Identify those standard audits that need to be carried out.
Identify the priorities for Mariner!– The rating of where Mariner stands against
those CMS identified areas where improvement is needed.
– Determine which audits will apply to your facility.

COLLECT INFORMATION
Establish the Medical Record Director’s schedule for auditing.
Standard Audits – those are the required audits as set by Mariner.
Determine the required without exception – identify those audits/monitoring
ADMISSION MONITORING
Most common admission audit findings:– Incomplete admission assessment– Incomplete or lack of documentation on the CP
that represents key problems for which the resident was admitted.
– Other key areas.– Review and discuss
ADMSSION MONITORING -2
Set an action plan for your facility List:
HOW TO CALCULATE COMPLIANCE
Counting the number of items that met compliance (denoted as “+”).
Dividing the number of “+”s (Met Compliance) by the total number of records reviewed in that category.
Multiplying by the result by 100 to obtain the percentage.
– Example: 5 records reviewed – 3 items met
3 divided by 5 = .6 x 100 = 60%

LET’S PRACTICE!
1. Count the number of items in compliance (1st column)
2. Count the total number of records reviewed
3. Divide the number of “Met” (answer to #1) into the total # of records (answer to #2)
4. Multiply the result (answer to #3) by 100
NEW ADMISSION AUDIT
What has changed???

24-HOUR AUDIT
CompleteFace SheetWith Dx
AllergySticker
Nursing Adm.Asmn'tcomplete
Tx Ordersmatch BodyAsmn't
VS/Ht/WT
MD andalternate MDon facesheet
MatchesHospitaland adm.Records
Body Asmn'tcomplete
Admission Ordersverified
I&OInitiated
***

24-HOUR AUDIT -2
PCPStarted=Reasonadmit
Inv done w2 sig
Physical &Chem Rest
PhysicalRestraint
MatchesDevice Riskand BenefitsForm
Consent toTx
MedicareCert *
Informedconsent
RestraintAsmn't
All formscompleted
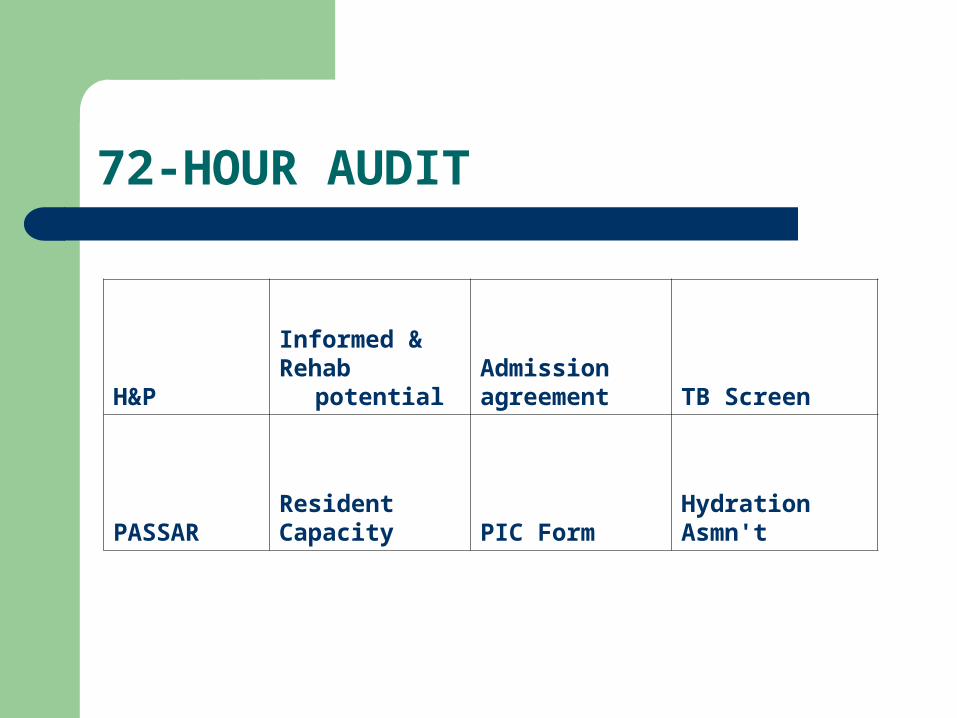
72-HOUR AUDIT
H&P Informed &Rehab potential
Admissionagreement TB Screen
PASSARResidentCapacity PIC Form
HydrationAsmn't
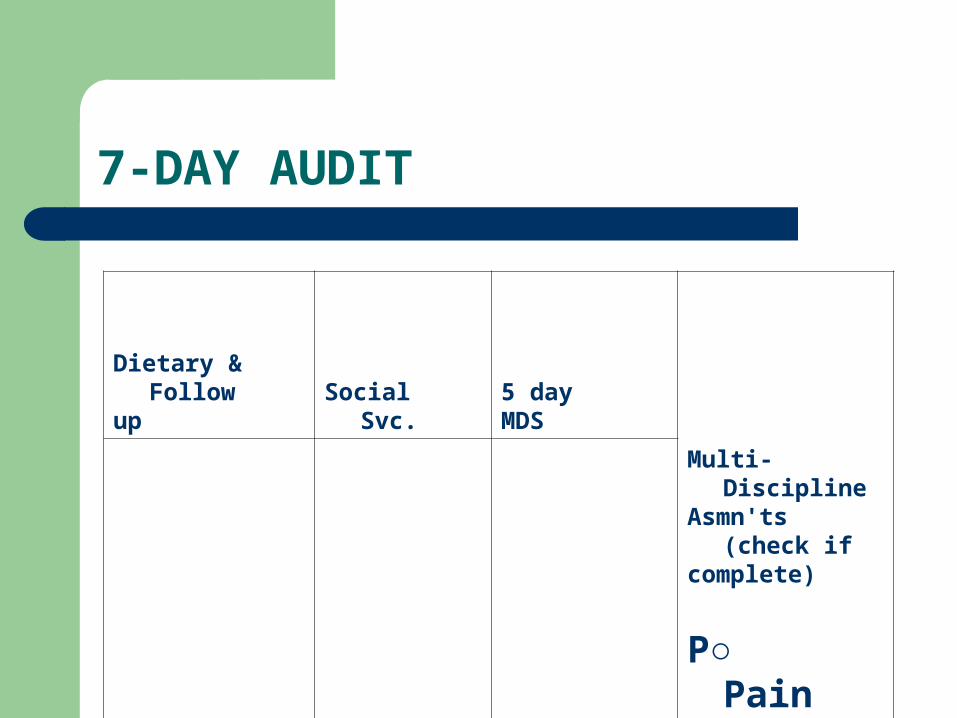
7-DAY AUDIT
Dietary & Followup Social Svc.
5 day MDS
Multi-DisciplineAsmn'ts (check ifcomplete)
P○ Pain
E○ Educ
R○ RestActivitiesDischplanning
SpiritualAsmn't(JCAHO)

14-DAY AUDIT
14 Day MDSRAPS/
CP Proceed
B&B Eval *Recert

21-DAY AUDIT
Care plan complete
Care Plan matches RAPs

STANDARD AUDITS
Weight audit – (may be done by others) Admission Audit Discharge Audits Psychotherapeutic drugs Specialized monitoring, i.e., review the
– H.O. #5 (Change of Condition)– H.O. #6 (Pressure Sore/Ulcer / Skin Conditions)

STANDARD AUDITS
Change of Condition – daily. Weekly skin report (done by the treatment
nurse and audited by the MRD for qualitative documentation) (HIM/Record Consultant may need to assist with the quality training).
Quantitative Reviews – is it or is it not there?
DISCHARGE AUDIT
A discharge form is not required on this record for one of the following reasons. Medical record staff is to check one reason and file this form on the front of the closed record.
Diagnoses are included in admission/discharge (face sheet) record, history and physical. In some cases a certification and re-certification form has the current diagnoses, progress notes includes condition on evaluation (if the resident was seen by the physician during the stay), physician’s orders include diagnoses to support medications/treatment.
DISCHARGE AUDIT -2
[ ] Resident was not discharged. He/she was transferred and is expected to return. See transfer form for current diagnoses, for the reason for transfer. Notations re: additional documents sent with resident.
[ ] Resident was released/discharged to home with an interdisciplinary discharge summary and post-discharge plan of care.

DISCHARGE AUDIT -3
[ ] Resident was transferred to another skilled or health care facility or assisted living. An interfacility transfer report was sent with the resident, including other identified record information, see notations of information sent.
[ ] Resident was not discharged. He/she expired. See death certificate.
[ ] Resident was not discharged. Resident left the facility { } ama-against medical advise { } left without discharge orders
{ } AWOL

AWAY WITHOUT LEAVE
Diagnoses are required by the California administrative code, Medicare/medical to identify the medical necessity for admission, specify the conditions supporting the stay and the condition at
discharge/death.
Provided based on information from Delores Galias, R.N., RHIT
AUDITS AND THE FOLLOW UP
Audit schedule with required audits and QA reporting and schedule.
Audit/Monitor Schedule (H.O. #3) on the Administrator’s and DNS desk. Follow up to assure MRD audits carried out as planned.
HIM/Record Consultants assist with above and provide training and monitoring to assist with the quality of the process.
OBJECTIVES
Participants will identify: The basic reason for physician’s orders The legal requirements for physician’s
orders The link between adequate/complete
orders and the medication and treatment records.
PHYSICIAN ORDERS
Purpose Gives clear direction in care of resident

PHYSICIAN
Orders given by physician Must be accepted by licensed nurse Must be documented on P.O. sheet Must be cosigned and dated by MD Must be maintained in chronological order Can be written by Licensed HC
professional Must be counter-initialed and dated by LN

PHYSICIAN -2
Orders received and signed via fax May be accepted Both physician office and facility to
maintain Part of Medical Record Must be clearly identified
With resident name and medical record number Every 30 days or as required reviewed and
signed by MD

RECEIVING A WRITTEN/FAXED ORDER
MD or state health care professional must write on PO or RX pad
Licensed Nurse receiving order must verify Date Time Physician signature Accurate dosage Accurate frequency Duration, as applicable Accurate route and/or site, if applicable Other info as may be necessary to carry out
order
TRANSCRIBING WRITTEN ORDER Licensed nurse (L.N.) verifies order Documents the word “noted” With his/her signature, title and date Transcribes to TAR, MAR or other document
Order not required to be documented on MAR/TAR must be followed up per facility policy*
Draw an error to box signifying the day and time
Order for limited time –Indicate the stop date Mark STOP DATE on Medication or Treatment
Record
RECEIVING A T.O./VERBAL ORDER
Repeat the order to physician/person giving order, clarify the order to be sure it is accurate
Information received should be Dosage Route of administration Time and/or frequency of administration Number of days or doses Diagnosis for medication
Write on T.O.
RECEIVING A T.O./VERBAL ORDER -2
LN records time, dates, and signs Notify pharmacy of new order, if
indicated Notify ancillary service if the order if for
a laboratory test, or other diagnostic test, consultation, etc.

MONTHLY PHYSICIAN ORDERS
Renewed every month, or as directed by law (California usually 30 days, or if facility has a 45 day stop order policy
Medical Record will conduct monthly audit To ensure signed by MD
AUDIT MONTHLY POs
MRD Care in entry of orders Follow up Review by Licensed Nursing Personnel Good time to review when you are
doing C of C for all new orders at least.

AUDIT PHYSICIAN ORDERS
Specific to drug strength and frequency “PRN” state reason and time frame TX order include site (1 per site) and
condition Diet order includes type of diet Admission activity order Orders verified with MD Orders not listed on transfer sheet – T.O. Recap of order is correct Review of orders indicated by
signature/initials
AUDIT P.O. ORDERS -2
MD signed and dated Foley order includes size Irrigation order includes type, amount of
solution and frequency (if used, not used much anymore)
NGT/GT order includes cc fluids, time period for intake
Enema order indicates type and frequency Laxative order include sequence criteria for
use

AUDIT P.O. ORDERS -3
Physical restraint order, includes medical reason and when to use
Behavior drug orders include specific behavior
Behavior control have behavior count set-up
Informed consent prior to usage (unless in effect prior to admit)
DISCONTINUATION OF ORDER
MD order required prior to discontinuation Any change in P.O. must be transcribed as
new order LN must transcribe order
Makes notation DC’d His/her initials Date

DAILY QUALITY ASSURANCE REVIEW SYSTEM
Used to identify problems, concerns and conditions where additional follow up, review or referral are needed or desired
A method of continuous quality care outcome review
Action/results oriented
SYSTEM BENEFITS
Reduces duplication of efforts– Follow up tasks identified and assigned to staff on
specified due dates Focus on
– Timely identification of deficiencies/problems– Prevention of repeat deficiencies/problems– Continued review of follow through until resolution
so that nothing “falls through the cracks”

SYSTEM BENEFITS -2
Utilizes time spent in daily stand up meeting to maximize results – quality outcomes
Promotes ID team involvement in problem identification and problem solving
SYSTEM COMPONENTS
24 hour report/shift report Incident reports Change of condition monitor Reports of
resident/family/concerns/complaints Daily quality assurance review form (log) Daily standup meeting
24-HOUR REPORT
Centralizes nursing communications on a shift by shift basis
Helps to ensure timely follow up from shift to shift or day to day
Usually the first documented indication of a new or impending problem or change of condition
An important link in the audit trail Important source of information for the IDT as well
as nursing
INCIDENT REPORTS
Another important link in the audit trail Provides detailed information that must be
carefully documented, reviewed and trended Must be integrated into the QA process
ongoing Daily review of reports to ensure quality
outcomes and timely follow up

CHANGE OF CONDITION MONITOR
Complete daily prior to the standup meeting Reviews information given in the 24 hour
report, incident reports and telephone orders Identifies changes and problems requiring
follow up in the last 24 hours (or 72 hrs. over the weekend)
Centralizes and identifies changes and any deficiencies or “loose ends” in documentation

RESIDENT/FAMILY CONCERNS AND COMPLAINTS
Frequently not picked up and processed in a methodical manner
An important source of information about the resident, impending or actual problems and changes of condition
Need to be identified and addressed by the IDT in a timely manner
IDT involvement and reporting is critical
WHAT MAY INDICATE A CHANGE OF CONDITION?
Changes can be physical, mental or psychosocial
Change can be– Slow to develop and show subtle signs or– Developed rapidly with more obvious signs
and symptoms

WHAT MAY INDICATE A CHANGE OF CONDITION? -2
When reviewing the 24 hr. Report look for:– Reports to nursing by family, C.N.A.’S, R.N.A.’S, ancillary
services that something has occurred or is changing in the resident’s condition
– Don’t overlook resident/family complaints– New orders for
An antibiotic, Treatment, Physical or chemical restraint, New support or assistive device, Weight loss or gain, X-rays and labs
WHAT MAY INDICATE A CHANGE OF CONDITION? -3
Changes in orders can also indicate a change of condition. For example:– Increase in dose of psychotropic medication– A change from one type of physical restraint to
another type– A change in type of assistive device used to treat
a condition or maintain mobility– Change in treatment order because the site is not
responding

WHAT MAY INDICATE A CHANGE OF CONDITION? -4
When reviewing incident reports look for– Falls– Medication errors– Injuries/death resulting from defective equipment– Resident to resident or resident to staff
altercations
COMPLETING THE COC MONITOR
Work Session – Review of the last 5 change of condition monitors from each facility (work as a group).
Summarize issues Plan for facility and Corporate-wide

COMPLETING THE COC MONITOR -2
Look at the audit form (H.O. #5) Review the Legend at the bottom of the form
– These are the codes used to complete the form
Review the Incidents and Accidents box– These are some general related guidelines
COMPLETING THE COC MONITOR -3
Reviews information given in the 24 hour report, incident reports and telephone orders
Identifies changes and problems requiring follow up in the last 24 hours (or 72 hrs. over the weekend)
Centralizes and identifies changes and any deficiencies or “loose ends” in documentation

HITECH and HIPAA
SB541 – SB337 BREACHES
HITECH and HIPAA
SB541 – SB337 BREACHES

HITECH & HIPAA HITECH & HIPAA
ACCESS
HITECH HIPAA
SB 541
BREACHES
Privacy and Security
Privacy and Security

BreachesBreaches
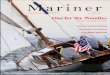
Part of the American Recovery and
Reinvestment Act of 2009
Applies the HIPAA privacy and security rules and
their penalties to HIPAA business associates
Creates a new breach reporting requirement for
HIPPA CEs and BAs
Effective Date February 2009
Part of the American Recovery and
Reinvestment Act of 2009
Applies the HIPAA privacy and security rules and
their penalties to HIPAA business associates
Creates a new breach reporting requirement for
HIPPA CEs and BAs
Effective Date February 2009
California legislature that enforces reporting
requirements for unlawful or
unauthorized access, use or disclosure of a
patient’s medical information
Reporting requirement within 5 days of
discovery
Effective Date 2009
California legislature that enforces reporting
requirements for unlawful or
unauthorized access, use or disclosure of a
patient’s medical information
Reporting requirement within 5 days of
discovery
Effective Date 2009
Health Insurance Portability and
Accountability Act
Guidance for Privacy and Security of protected health
information
45CFR 160 -164
Effective Date 2003
Health Insurance Portability and
Accountability Act
Guidance for Privacy and Security of protected health
information
45CFR 160 -164
Effective Date 2003
HIPAA HIPAA
SB 541SB 541HITECH ACT HITECH ACT

HITECH STATE LAW Vocabulary HITECH STATE LAW Vocabulary
• Breach – the unauthorized acquisition, access, use or disclosure of protected health information which compromises the security or privacy of such information

Breaches ElectronicBreaches Electronic
• The notice to individuals must contain a description of what happened and the PHI involved, efforts to investigate, mitigate and prevent further breaches and contact information.

No Safe HarborNo Safe Harbor
• California covered entities are still required to report unlawful or unauthorized access, use or disclosure of a patient’s medical information within 5 days to comply with SB 541 – which has been in effect since January 2009

Penalties Penalties
• SB-541 – failure to report within 5 days
$100 per day for each day that the unlawful or unauthorized access, use or disclosure is not reported up to a maximum of $250,000.
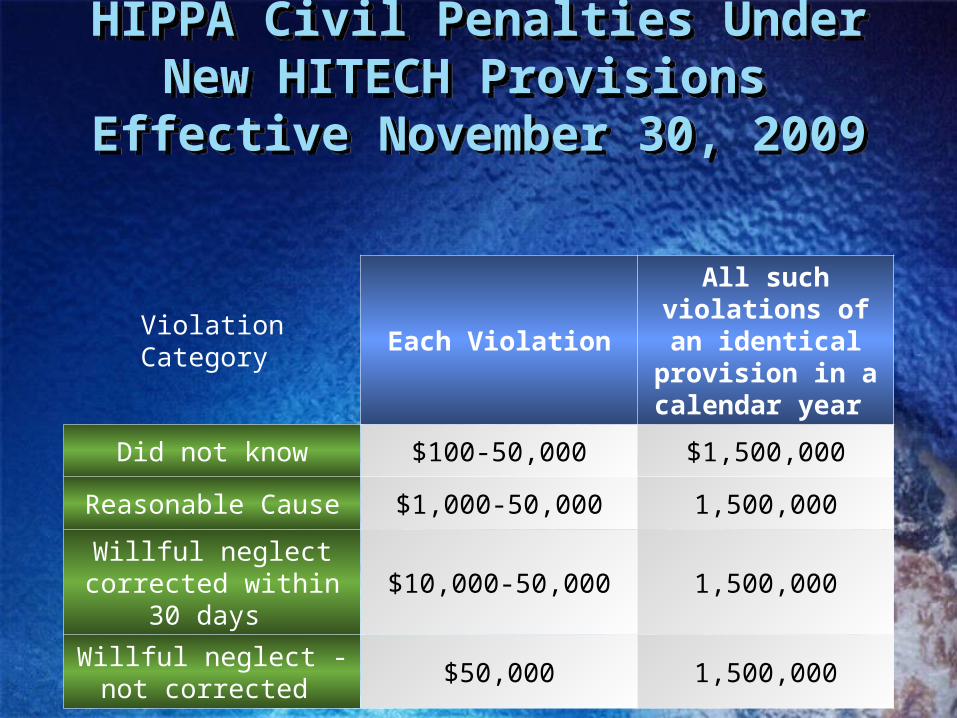
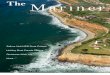
HIPPA Civil Penalties Under New HITECH Provisions
Effective November 30, 2009
HIPPA Civil Penalties Under New HITECH Provisions
Effective November 30, 2009
Violation Category Each Violation
All such violations of an identical provision in a calendar year
Did not know $100-50,000 $1,500,000
Reasonable Cause $1,000-50,000 1,500,000
Willful neglect corrected within 30
days $10,000-50,000 1,500,000
Willful neglect - not corrected
$50,000 1,500,000
Risk Analysis and Implementation Risk Analysis and Implementation
• AHIS will help you analyze possible areas of risk
• Provide you with guidance on documentation of investigation and notification of breaches

AHIS As Your Partner AHIS As Your Partner
Implementation Plan
Risk Analysis
Policy and Procedure
Current system review
Action as needed

RECORD DEPARTMENT NEEDS
1.
2.
3.
4.
5.
6.
7.
RECORD DEPARTMENT NEEDS -2
8.
9.
10.
11.
12.
13.
14.

FORMS
Who orders and sign up. One sign in sheet for forms, include name,
facility, address, phone and email address.

OFFSITE STORAGE
When? What is required – reference to the
HIM/Record Manual? YOUR ACTION PLAN!

Follow up
1.
2.
3.
4.
5.
6.
7.
THANK YOU FOR ATTENDING!
Please Complete and Leave the Evaluation with the Instructor