Embed Size (px)
Citation preview
Marijuana and theCannabinoids
14
14 Marijuana and the Cannabinoids
Background and History of Marijuana
Basic Pharmacology of Marijuana
Mechanisms of Action
Acute Behavioral and Physiological Effects of Cannabinoids
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Background and History of Marijuana
In the 1930s, the US Bureau of Narcotics launched a public relations campaign to portray marijuana as a social menace that could destroy the youth of America.
The propaganda included magazine articles and anti-marijuana films such as Reefer Madness.
Figure 14.1 Poster advertising the 1936 film Reefer Madness
Background and History of Marijuana
Marijuana remains a controversial subject in our society—castigated by many as a gateway to the so-called hard drugs, but praised by others as an unappreciated medical marvel.
Background and History of Marijuana
Marijuana is produced from flowering hemp (Cannabis sativa).
Hemp has been a major source of fiber in many cultures for rope, cloth, and paper.
Hemp seeds have been used for oil and bird food.
Figure 14.2 Cannabis plants
Background and History of Marijuana
Hemp also contains 70 unique compounds known as cannabinoids, plus more than 400 other identified compounds.
The psychoactive compound Δ9-tetrahydrocannabinol (THC), accounts for the use of cannabis as a drug.
Background and History of Marijuana
Marijuana is a mixture of dried and crumbled leaves, small stems, and flowering tops.
It can be consumed orally, as in cookies or brownies, but is usually smoked in rolled cigarettes known as “joints,” various kinds of pipes, or in hollowed-out cigars called “blunts.”
Background and History of Marijuana
Marijuana potency (in terms of THC content) varies widely, depending on the genetic strain of the plant and growing conditions.
Potency can be increased by preventing pollination and seed production by the female plants. This marijuana is called sinsemilla (“without seeds”).
Background and History of Marijuana
Hashish is a cannabis derivitive that can be smoked or eaten.
It can refer to a relatively pure resin preparation with very high cannabinoid content, or a solvent extract of leaves or resin.
Hash oil is an alcoholic extract. A drop is placed on a tobacco or marijuana cigarette.
Figure 14.3 The potent form of cannabis called hashish
Background and History of Marijuana
Cannabis probably originated in China. Medical and religious use can be traced to ancient China, India, and the Middle East, spreading to the Arab world.
Napoleon’s soldiers brought it to France from Egypt. It became popular with French writers and artists.
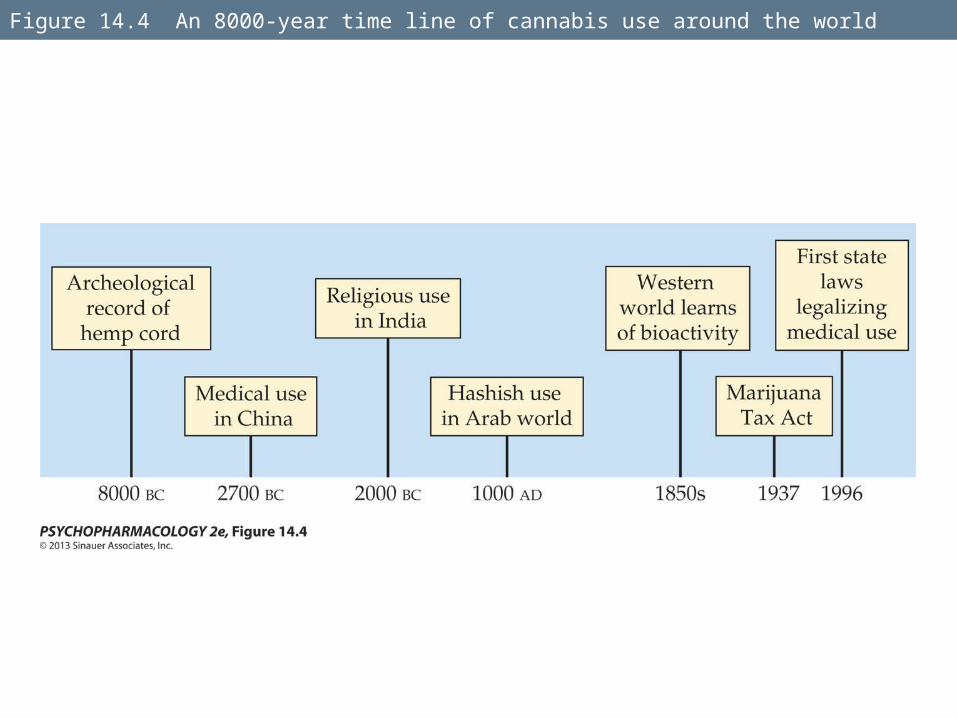
Figure 14.4 An 8000-year time line of cannabis use around the world
Background and History of Marijuana
Hemp was grown in colonial America, but marijuana smoking probably came to the U.S. with Mexican and Caribbean immigrants in the early 1900s.
In 1937, the Marijuana Tax Act instituted a national registration and taxation system aimed at discouraging all use of cannabis. It was overturned in 1969, but cannabis is still tightly controlled.
Background and History of Marijuana
THC was identified as the major active ingredient in 1964.
Burning marijuana causes the THC to vaporize and enter the smoker’s lungs in small particles.
Effective dose and latency to onset of effects are influenced by the amount and potency of the plant used, and patterns of smoking (e.g., breathhold duration).
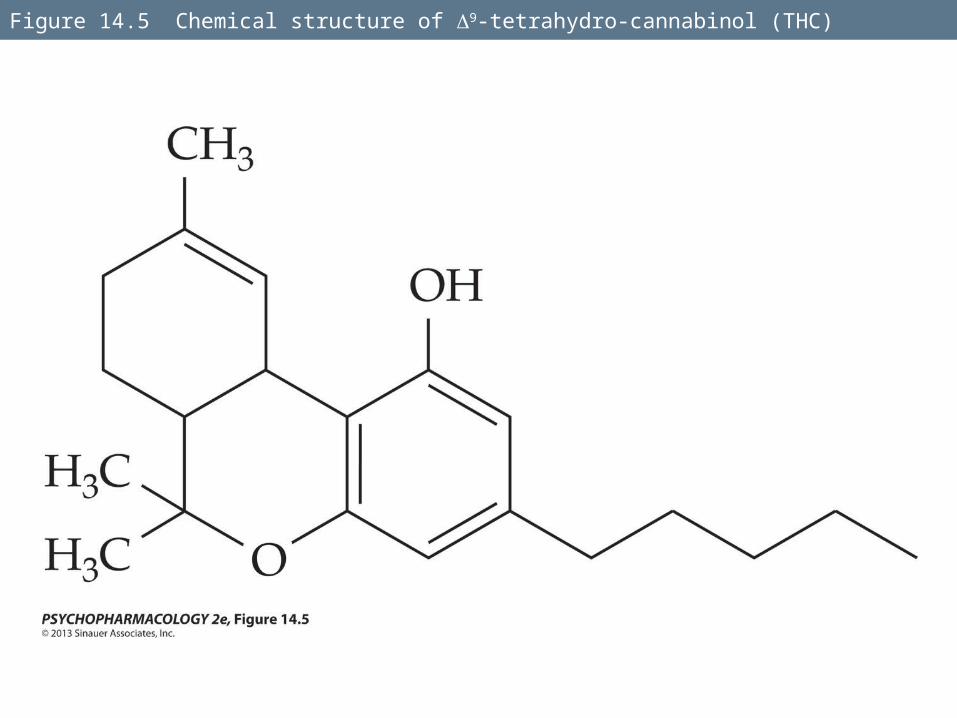
Figure 14.5 Chemical structure of 9-tetrahydro-cannabinol (THC)
Background and History of Marijuana
THC is easily absorbed by the lungs, and blood plasma levels rise quickly.
Concentrations begin to decline as a result of metabolism in the liver and accumulation in the body’s fat stores.
In oral use, poor absorption results in low and variable plasma levels, probably due to degradation in the stomach and first-pass metabolism.
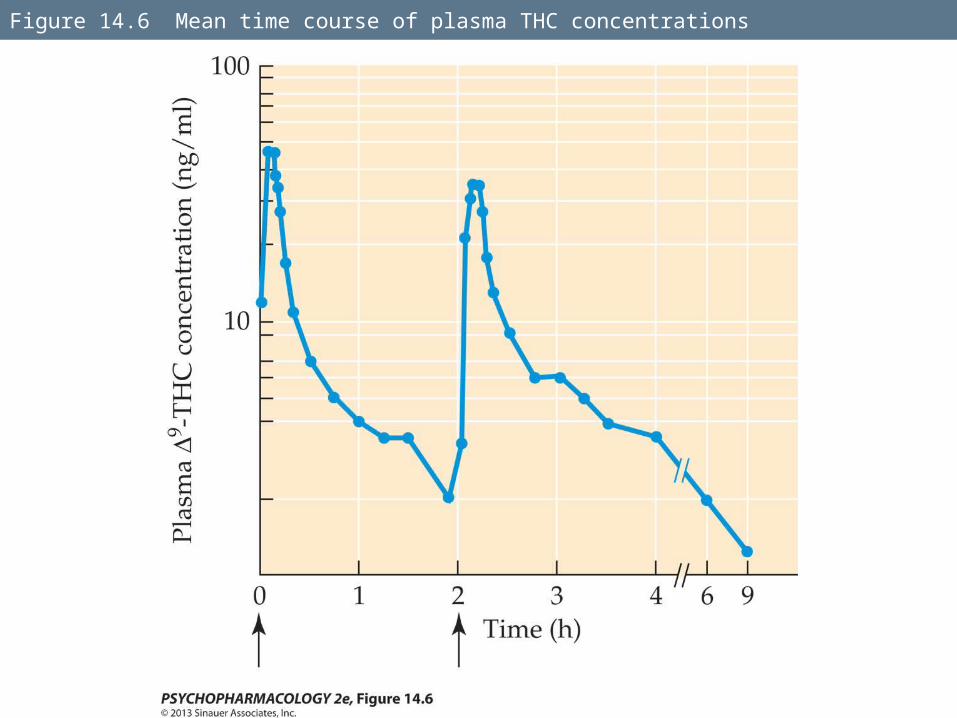
Figure 14.6 Mean time course of plasma THC concentrations
Background and History of Marijuana
Blood THC levels decline rapidly after smoking marijuana, but complete elimination from the body is much slower because of persistence in fat tissues.
The gradual movement of THC metabolites back out of fat stores means that urine screening tests can detect them more than 2 weeks after a single marijuana use.
Mechanisms of Action
A cannabinoid receptor in the CNS was identified in 1988.
Receptors occur in many brain areas.
CB1 is the receptor found in the CNS.
CB2 occurs in the immune system and other tissues such as bone, adipose (fat) cells, and the GI tract.
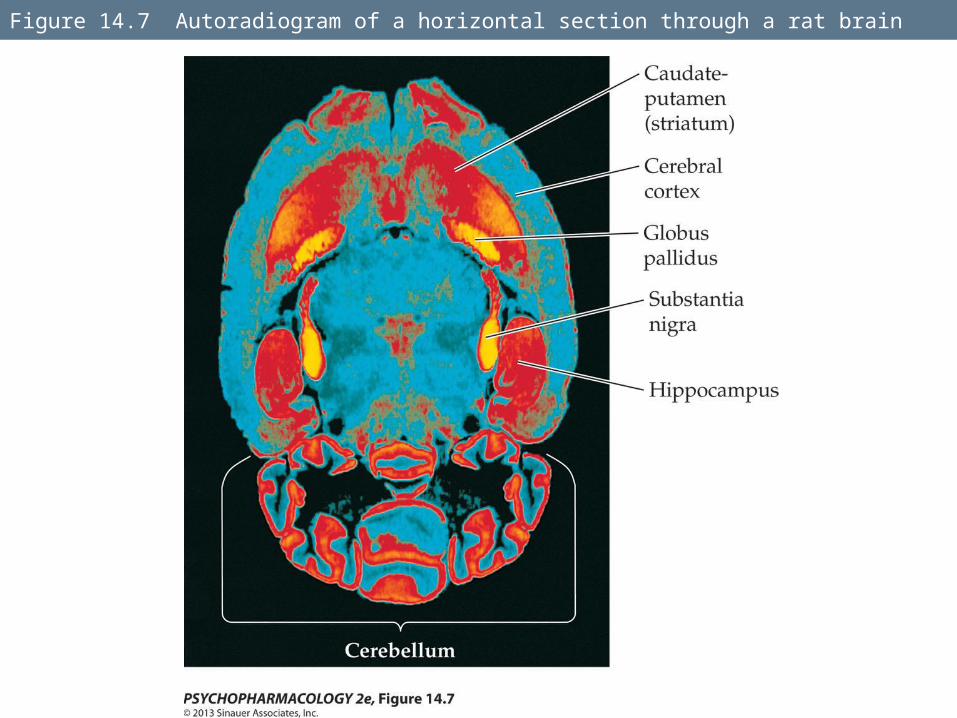
Figure 14.7 Autoradiogram of a horizontal section through a rat brain
Mechanisms of Action
Cannabinoid receptors are metabotropic; they work via G proteins to inhibit cAMP formation, inhibit voltage-sensitive Ca2+ channels, and open K+ channels.
CB1 receptors are located on axon terminals. By activating these presynaptic receptors, cannabinoids can inhibit the release of many neurotransmitters.
Mechanisms of Action
Synthetic cannabinoid agonists and antagonists have been developed for research and potential therapeutic use.
THC given to mice induces reduced locomotor activity, hypothermia, catelepsy, and hypoalgesia—mediated through CB1 receptors.
CB1 receptors also play an important role in the reward system.
Mechanisms of Action
Cannabinoids adversely affect cognitive function, which has been studied in animal models.
Microinjection of THC or the synthetic cannabinoid agonist CP-55,940 into the hippocampus produced memory deficits in the radial arm maze.
The effects can be completely blocked by the antagonist rimonabant.
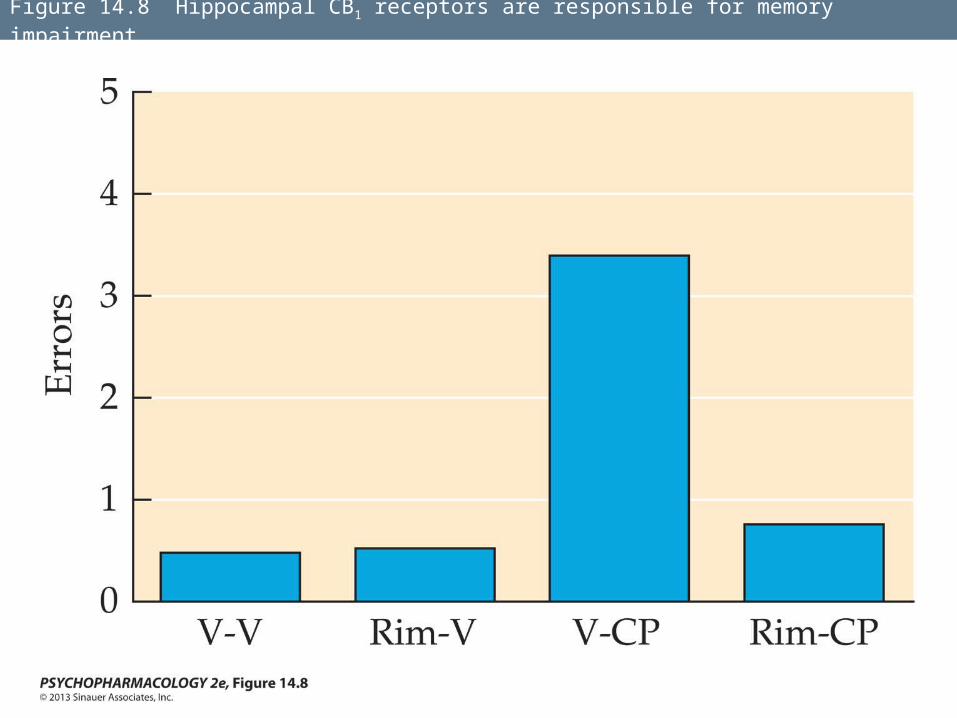
Figure 14.8 Hippocampal CB1 receptors are responsible for memory impairment
Mechanisms of Action
Other studies have shown that cannabinoids inhibit the induction of long-term potentiation (LTP) in the hippocampal CA1 area.
Mechanisms of Action
Why do human brains have receptors for a compound made by plants?
There must be an endogenous neurotransmitter-like substance that acts on the receptors.
Several of these have now been discovered—the endocannabinoids.
Mechanisms of Action
Two main endocannabinoids have been found: arachidonoyl ethanolamide (AEA), or anandamide, and 2-arachidonoylglycerol (2-AG).
They are retrograde messengers—carry information in the opposite direction from normal (i.e., postsynaptic to presynaptic).
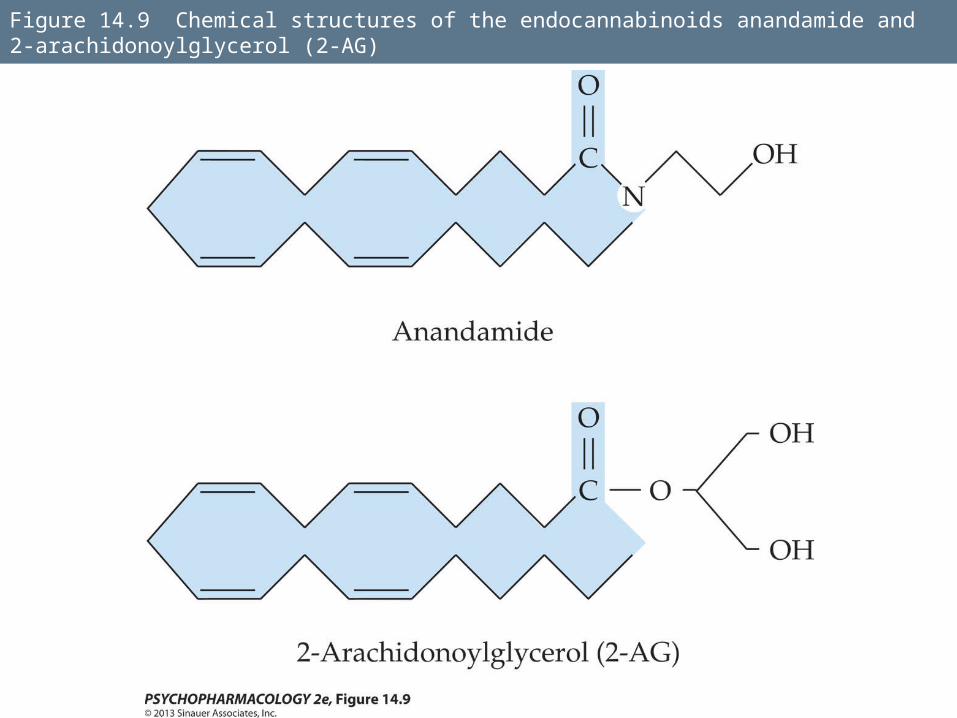
Figure 14.9 Chemical structures of the endocannabinoids anandamide and 2-arachidonoylglycerol (2-AG)
Mechanisms of Action
They are synthesized and released in response to depolarization of the postsynaptic cell due to the influx of Ca2+.
The endocannabinoids then cross the synaptic cleft, activate CB1 receptors on the nerve terminal, and inhibit Ca2+-mediated neurotransmitter release from the terminal.
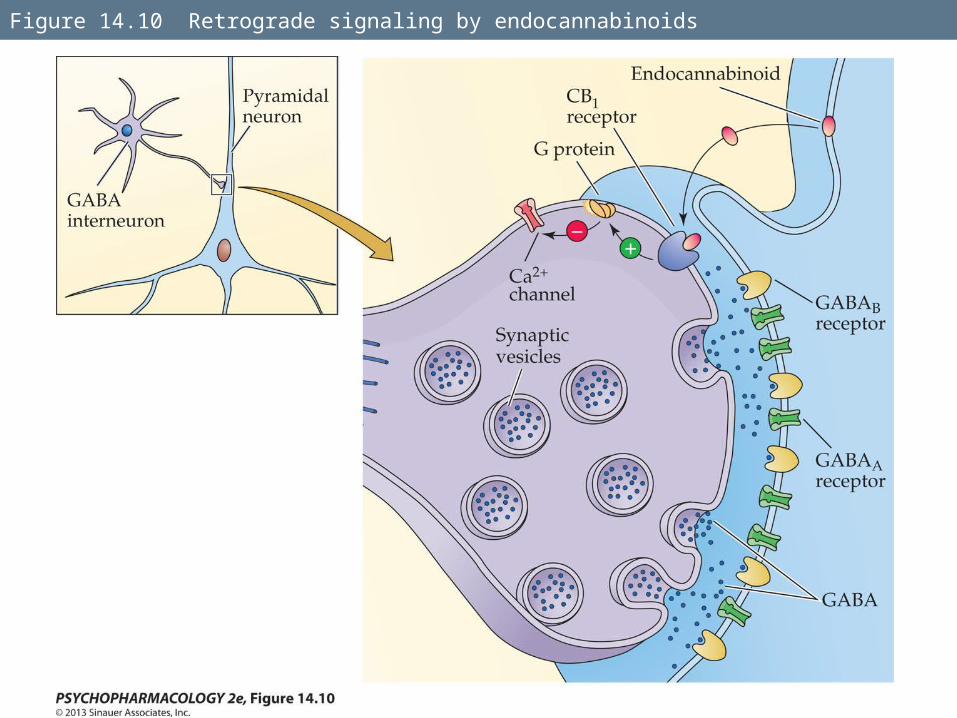
Figure 14.10 Retrograde signaling by endocannabinoids
Mechanisms of Action
To determine the roles of anandamide and 2-AG, researchers use the the CB1 receptor antagonist rimonabant, and CB1 and CB2 knockout mice.
Pain perception: both approaches produce mice with hyperalgesia (increased pain sensitivity).
Cannabinoid drugs have been used to treat pain and other medical conditions.
Mechanisms of Action
Dronabinol (Marinol), a synthetic form of THC and the THC analog nabilone (Cesamet) are used to treat nausea and emesis in cancer chemotherapy patients.
Nabiximols (Sativex) is a cannabis extract used to treat pain and spasticity in multiple sclerosis patients (not yet approved in the U.S.).
Mechanisms of Action
The anatomy and functioning of the endocannabinoid system is becoming well known.
A great deal of research is ongoing to develop cannabinoid medications to treat a variety of conditions, including GI disorders, pain, cancer, neurodegenerative diseases and psychiatric disorders.
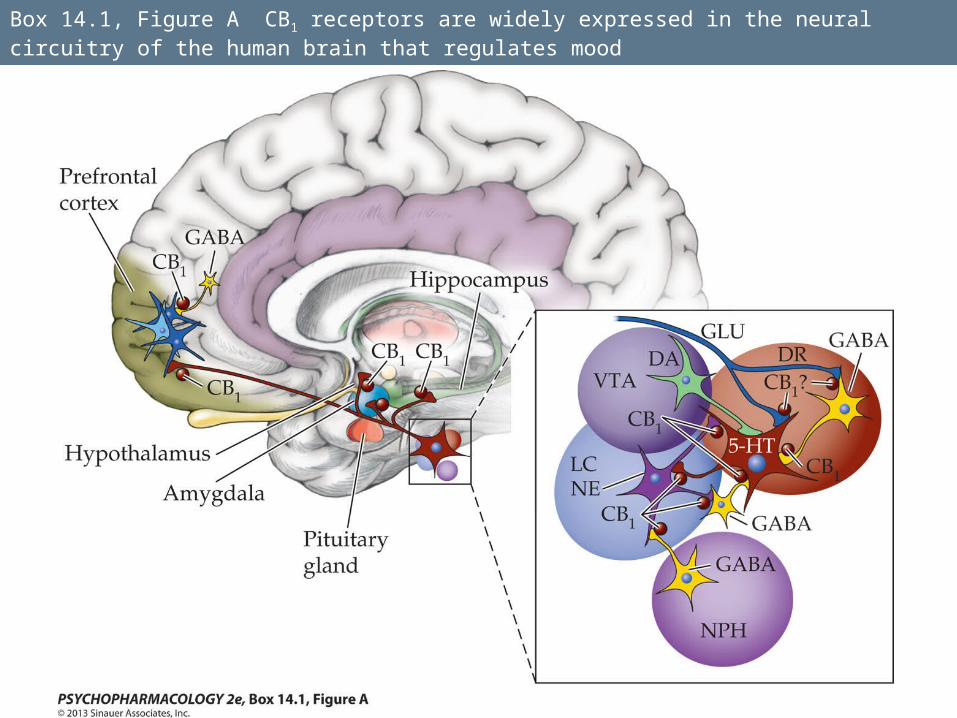
Box 14.1, Figure A CB1 receptors are widely expressed in the neural circuitry of the human brain that regulates mood
Mechanisms of Action
Medical marijuana—smoked marijuana as a medication.
Many states now permit legal use, but clinical studies of its efficacy have shown mixed results.
Smoked marijuana has the potential for adverse health effects and abuse; most researchers favor development of cannabinoid-based drugs instead.
Mechanisms of Action
Endocannabinoids enhance the incentive motivational properties of food and food-mediated reward.
CB1 receptor antagonists reduce food consumption in animals and human subjects.
AM6545, a peripherally-acting CB1 antagonist may be useful in treating obesity.
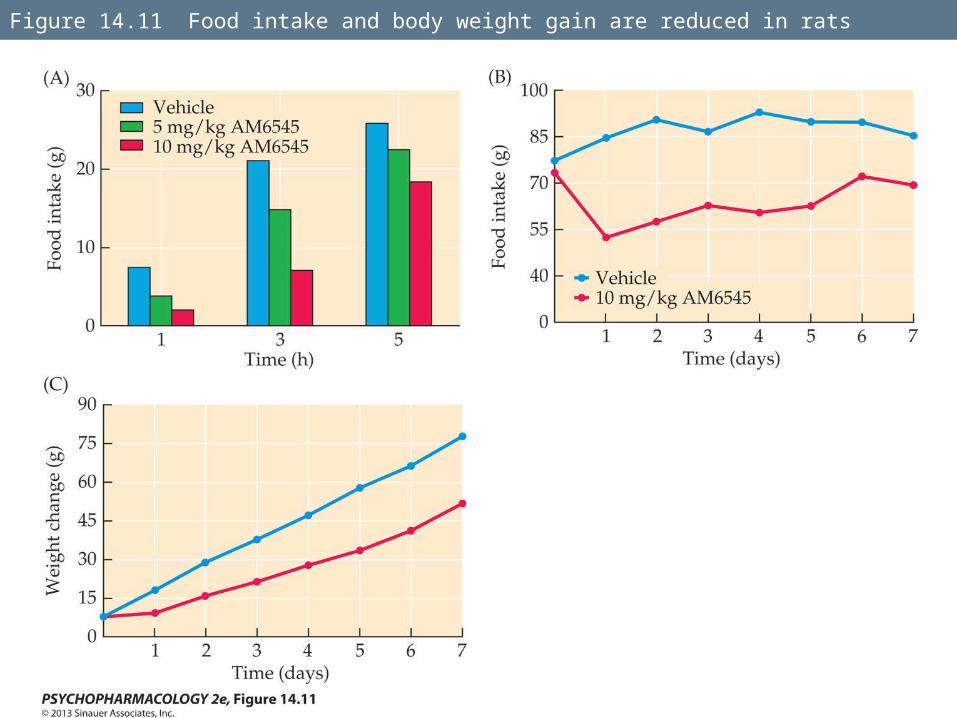
Figure 14.11 Food intake and body weight gain are reduced in rats
Mechanisms of Action
Learning and memory: some studies suggest endocannabinoids play a greater role in extinction of learned responses than in response acquisition.
This has been demonstrated with auditory fear conditioning of rats and mice. CB1 knockout mice do not show normal extinction of the freezing response.
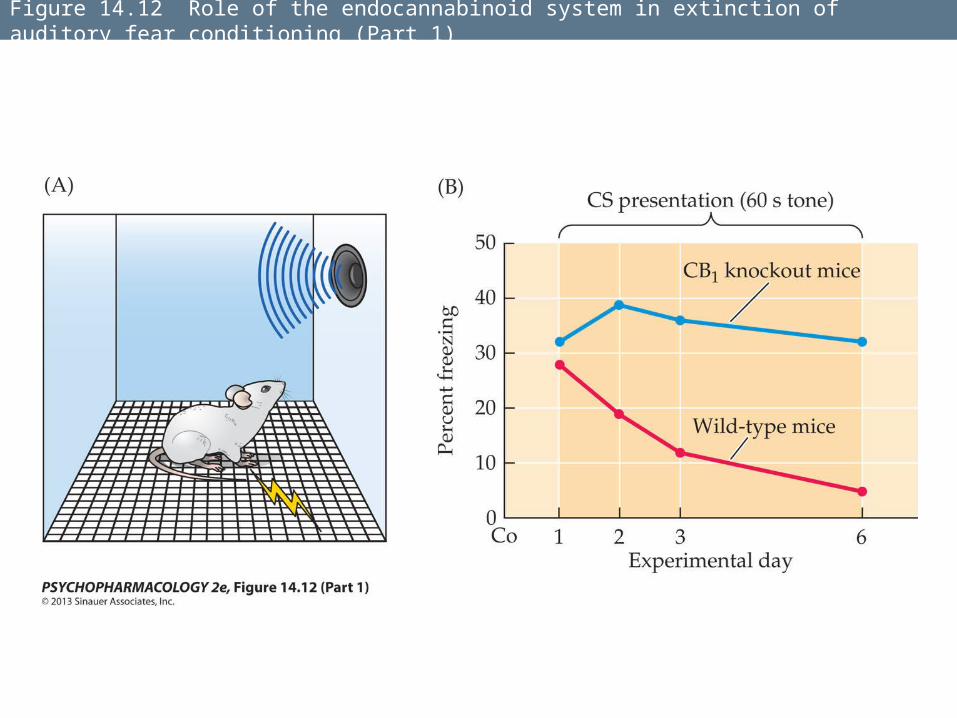
Figure 14.12 Role of the endocannabinoid system in extinction of auditory fear conditioning (Part 1)
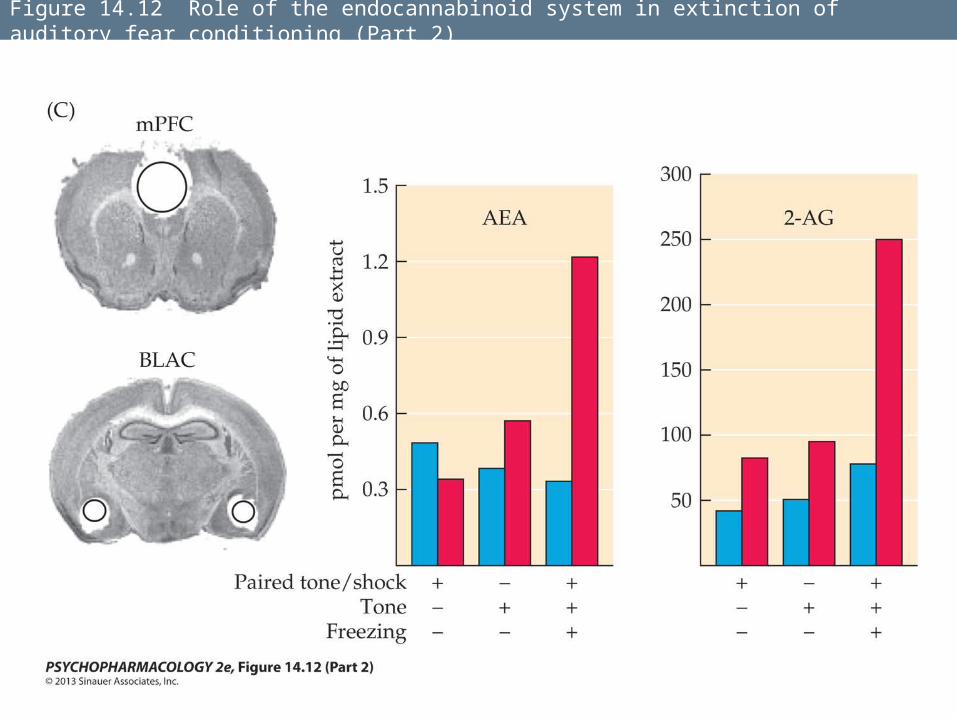
Figure 14.12 Role of the endocannabinoid system in extinction of auditory fear conditioning (Part 2)
Mechanisms of Action
In humans, a single nucleotide polymorphism in the FAAH gene has been discovered that results in increased endogenous anandamide levels.
People homozygous for the allele did not habituate to images of threatening faces.
The endocannabinoid system may be involved in the alleviation of fear.
Acute Behavioral and Physiological Effects of Cannabinoids
Effects of cannabinoid use vary depending on dose, frequency of use, characteristics of the user, and the setting in which use occurs.
Subjective and behavioral effects of marijuana use can be separated into four stages: the “buzz,” the “high,” the stage of being “stoned,” and the “come-down.”
Acute Behavioral and Physiological Effects of Cannabinoids
The “high” is associated with feelings of euphoria and exhilaration, and a sense of disinhibition.
Relaxation is the most commonly reported effect of being “stoned.”
Acute Behavioral and Physiological Effects of Cannabinoids
Physical responses include increased blood flow to the skin and flushing, increased heart rate, and increased hunger.
Effects of marijuana are at least partially mediated by CB1 receptors—effects are significantly reduced by pretreatment with rimonabant.
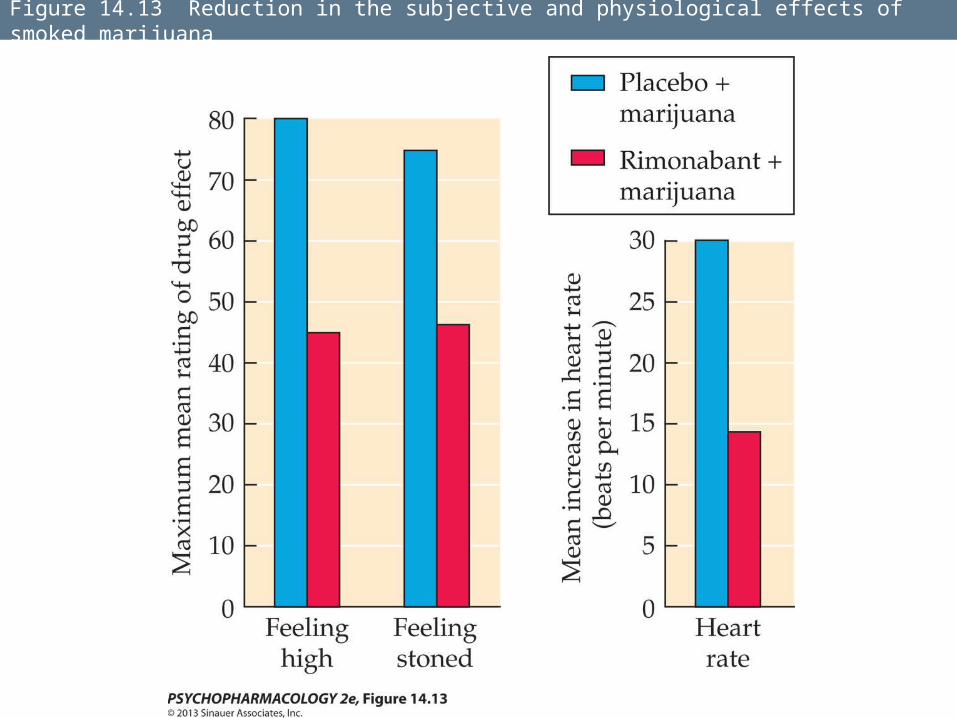
Figure 14.13 Reduction in the subjective and physiological effects of smoked marijuana
Acute Behavioral and Physiological Effects of Cannabinoids
Smoking marijuana can sometimes produce transient psychotic symptoms such as depersonalization, derealization, agitation, and paranoia.
Expectation also plays a role in what effects the drug will produce, as shown by placebo studies.
Acute Behavioral and Physiological Effects of Cannabinoids
Plasma THC levels peak much more rapidly after IV injection or marijuana smoking than after oral ingestion.
In smokers, maximum intoxication occurs some time after the cigarette has been finished, when plasma THC is already declining—brain and plasma THC concentrations are not yet equilibrated when the plasma level peaks.
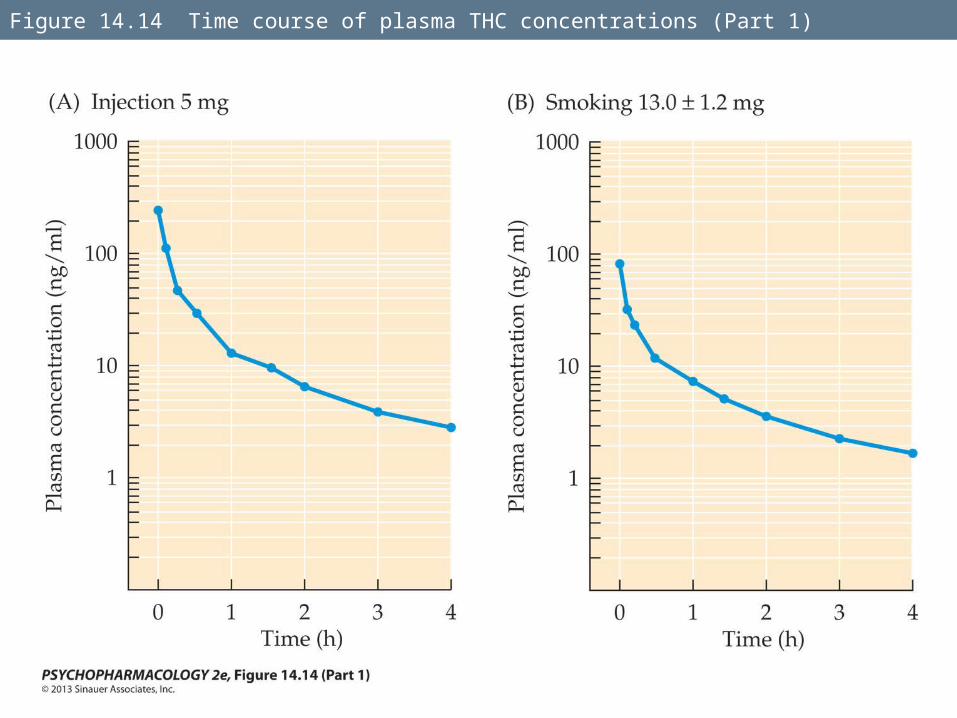
Figure 14.14 Time course of plasma THC concentrations (Part 1)
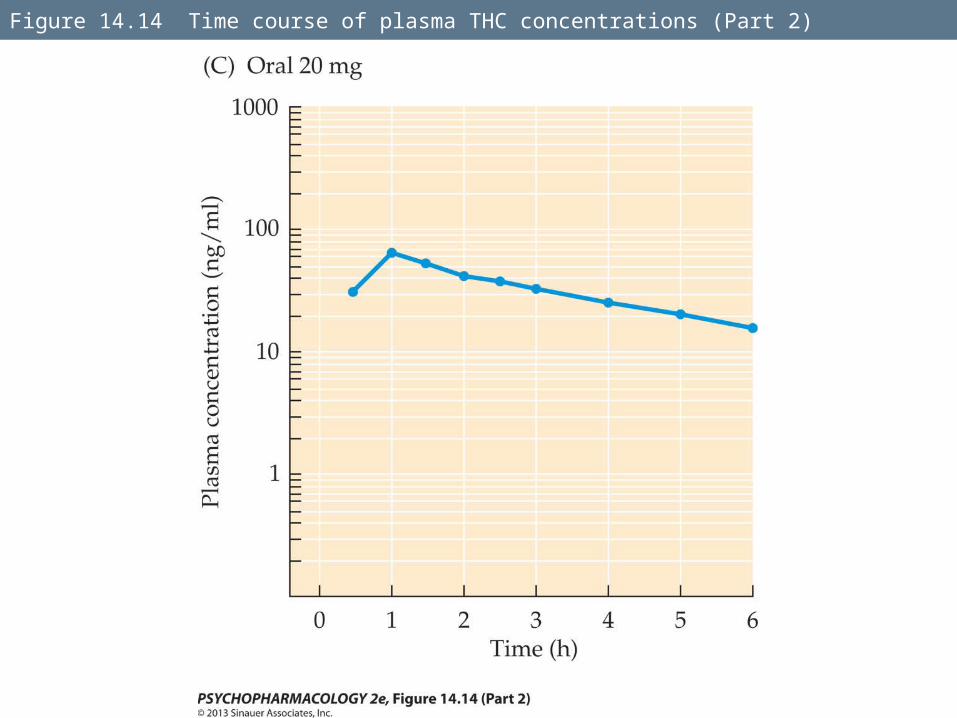
Figure 14.14 Time course of plasma THC concentrations (Part 2)
Acute Behavioral and Physiological Effects of Cannabinoids
Marijuana affects cognitive functions and psychomotor performance.
Decreased performance for a variety of verbal, spatial, time estimation, and reaction time tasks has been noted.
Cannabinoids appear to interfere with all aspects of memory processing.
Acute Behavioral and Physiological Effects of Cannabinoids
One study showed dose-dependent deficits in verbal memory tasks at 2 and 6 hours following oral THC administration to infrequent cannabis users.
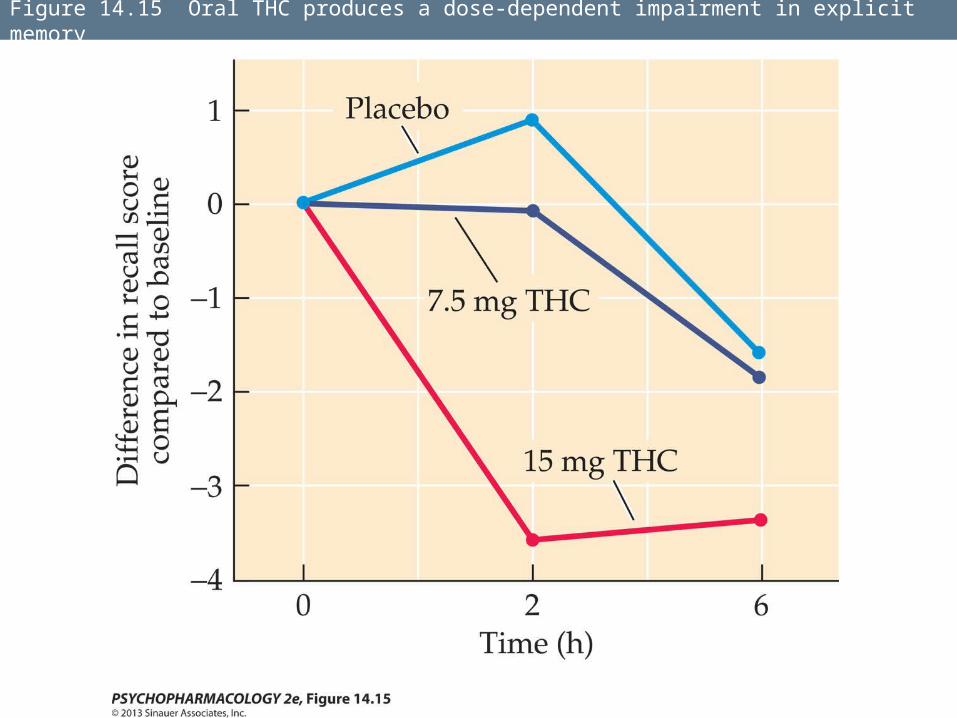
Figure 14.15 Oral THC produces a dose-dependent impairment in explicit memory
Acute Behavioral and Physiological Effects of Cannabinoids
Heavy cannabis use over a long period may lead to impaired executive functioning for at least 2 to 3 weeks following cessation of use.
Some data suggest that heavy, long-time users may continue to show impairment in decision-making, planning, and concept formation.
Acute Behavioral and Physiological Effects of Cannabinoids
Marijuana can affect psychomotor functioning under demanding task conditions, such as driving.
Use of cannabis with or without alcohol is a risk factor in automobile accidents.
Acute Behavioral and Physiological Effects of Cannabinoids
Cannabinoids are reinforcing:
In one study, regular marijuana users could discriminate THC-containing marijuana cigarettes from placebos with no THC, and all subjects preferred the marijuana with THC when given a choice.
Acute Behavioral and Physiological Effects of Cannabinoids
Animal studies have also demonstrated reinforcing properties.
Lever pressing by squirrel monkeys for THC stopped when placebos were used.
Lever pressing for THC was completely blocked by pretreatment with rimonabant, indicating that the reinforcing effect was dependent on CB1 receptor activation.
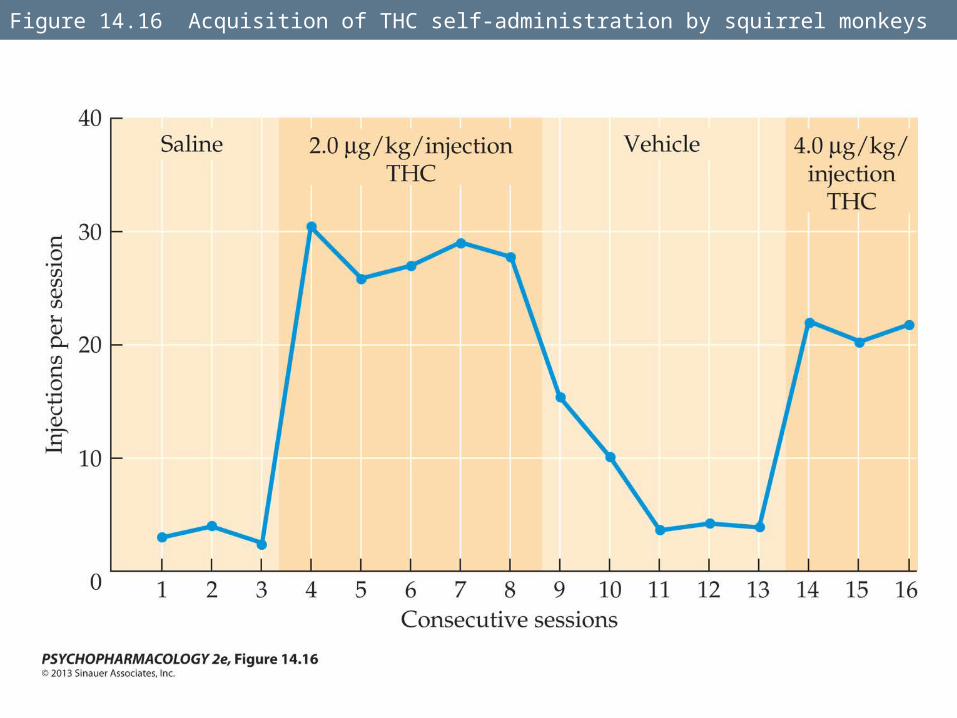
Figure 14.16 Acquisition of THC self-administration by squirrel monkeys
Acute Behavioral and Physiological Effects of Cannabinoids
Mechanisms for reinforcement:
Activation of the mesolimbic dopamine (DA) system.
Interactions between the cannabinoid and opioid systems may play a role in cannabinoid reward and reinforcement; opioid agonists enhance cannabinoid self-administration, and opioid antagonists have the opposite effect.
Acute Behavioral and Physiological Effects of Cannabinoids
The endocannabinoid system may play a role in reinforcement, dependence, and/or relapse for a number of other drugs, including ethanol.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Marijuana use typically begins in adolescence and peaks during young adulthood.
If an individual has not yet tried marijuana by his or her mid-twenties, he or she is unlikely to begin at a later age.
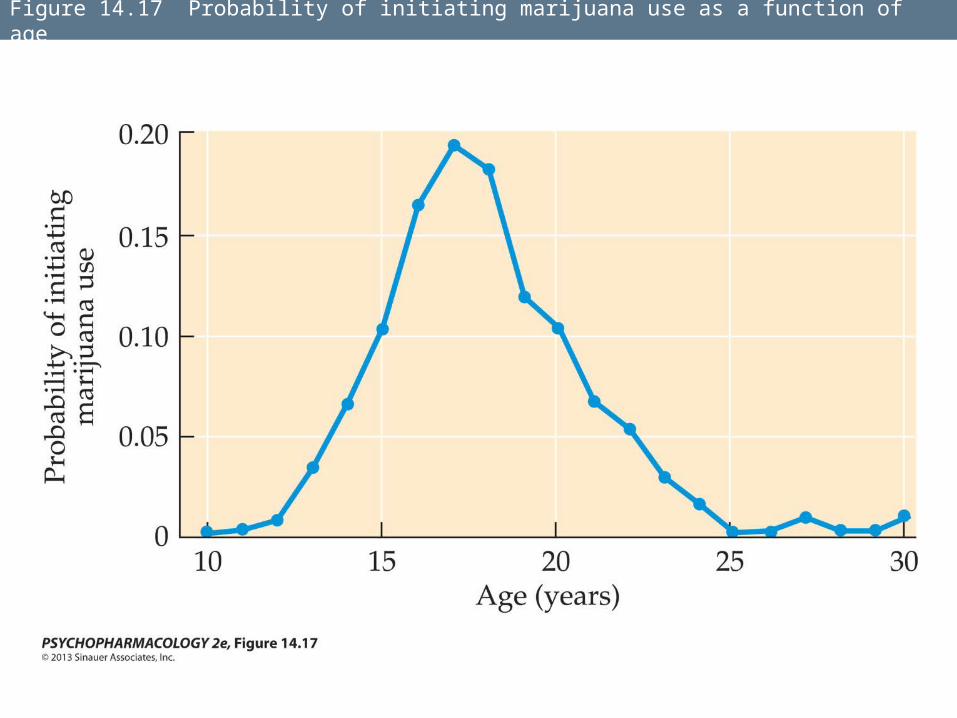
Figure 14.17 Probability of initiating marijuana use as a function of age
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Many adolescent users have already had experience with alcohol and/or cigarettes, leading to the hypothesis that alcohol and tobacco are “gateway” drugs to marijuana use, which in turn may serve as a gateway to other illicit drugs.
These hypotheses are very difficult to substantiate.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Risk factors in development of heavy marijuana use by adolescents include emotional problems in the family, heavy drug use in the household and/or by peers, dislike of school and poor school performance, and an early age of first use of marijuana.
Users that have more positive responses to early use have greater risk of becoming dependent.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Looking at usage from adolescence to age 37, investigators identified five patterns:
1. Non-users or experimenters
2. Occasional users
3. Quitters or decreasers
4. Chronic users
5. Increasing users
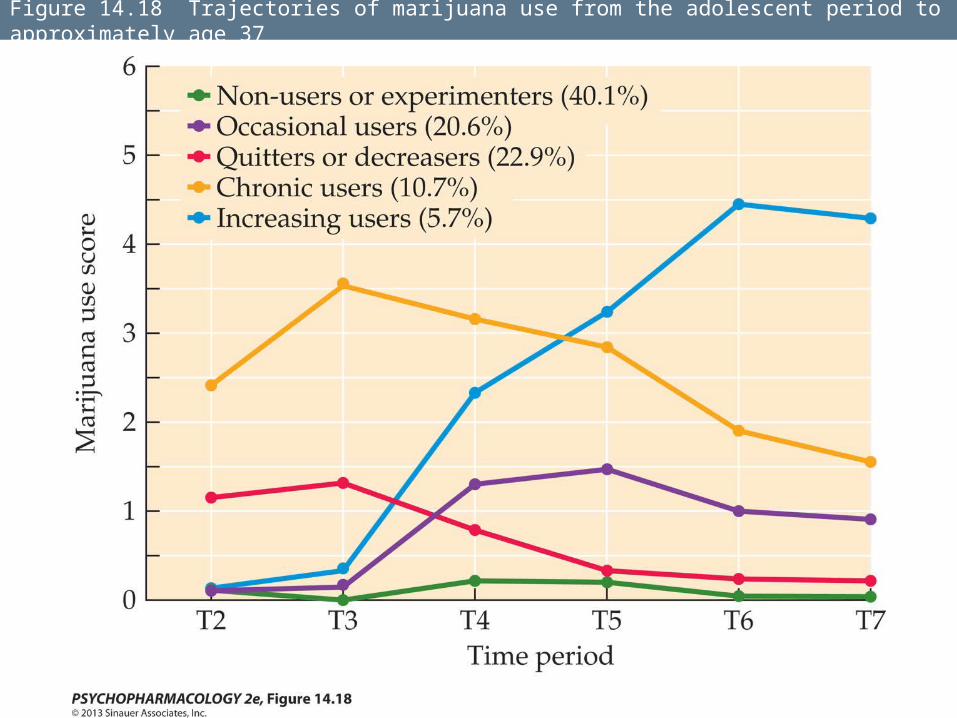
Figure 14.18 Trajectories of marijuana use from the adolescent period to approximately age 37
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Tolerance and Dependence
Animals exposed to THC or other CB1 agonists develop tolerance to the behavioral and physiological effects of these compounds.
It appears to involve a combination of desensitization and down-regulation of CB1 receptors.
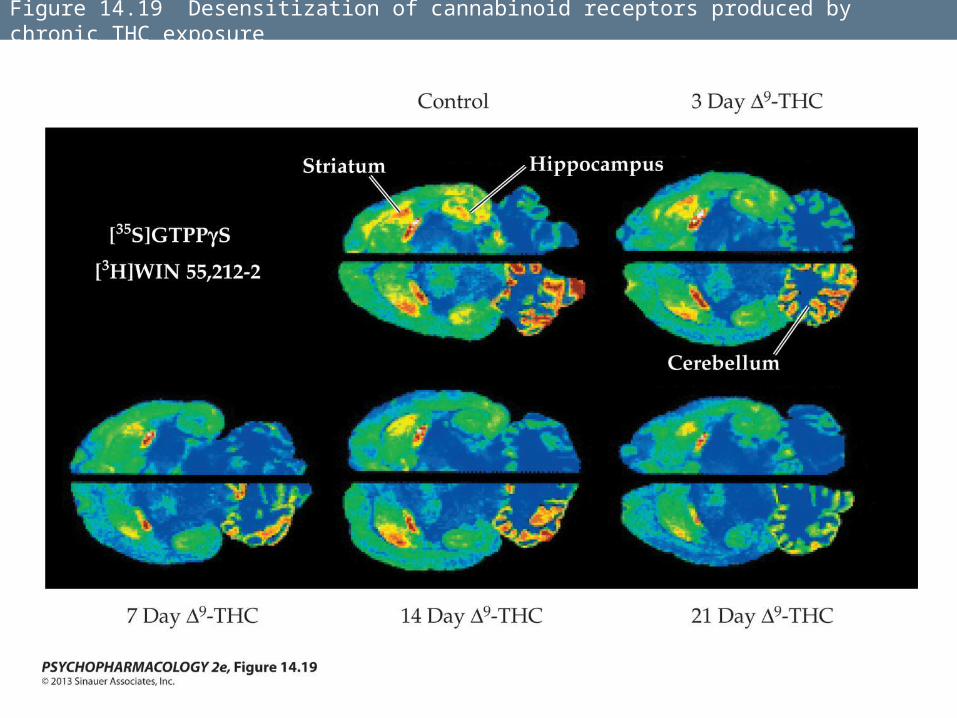
Figure 14.19 Desensitization of cannabinoid receptors produced by chronic THC exposure
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Risk of dependence is related to drug use patterns. People who progress to daily use have a 50% probability of become dependent.
Dependence is manifested as a difficulty in stopping one’s use, a craving for marijuana, and unpleasant withdrawal symptoms.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Withdrawal symptoms include irritability, increased anxiety, depressed mood, sleep disturbances, heightened aggressiveness, and decreased appetite.
These are similar to the symptoms of nicotine withdrawal.
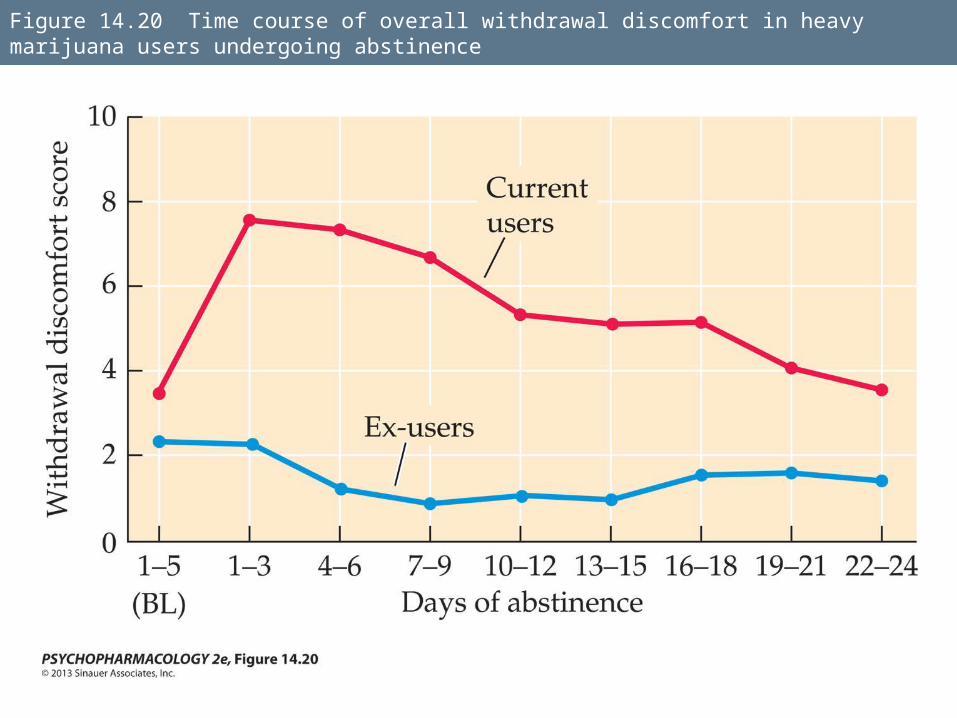
Figure 14.20 Time course of overall withdrawal discomfort in heavy marijuana users undergoing abstinence
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Development of the CB1 receptor antagonist rimonabant allowed researchers to test for dependence and withdrawal in animal models.
Precipitated withdrawal—rimonabant blocks the receptors and even with THC present, the animals showed abstinence symptoms.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Most cannabis users do not become dependent and do not seek treatment.
Treatment in outpatient programs involves cognitive-behavioral therapy, relapse prevention training, and/or motivational enhancement therapy, but patients are very vulnerable to relapse.
Some research on medications to relieve withdrawal symptons has been done.
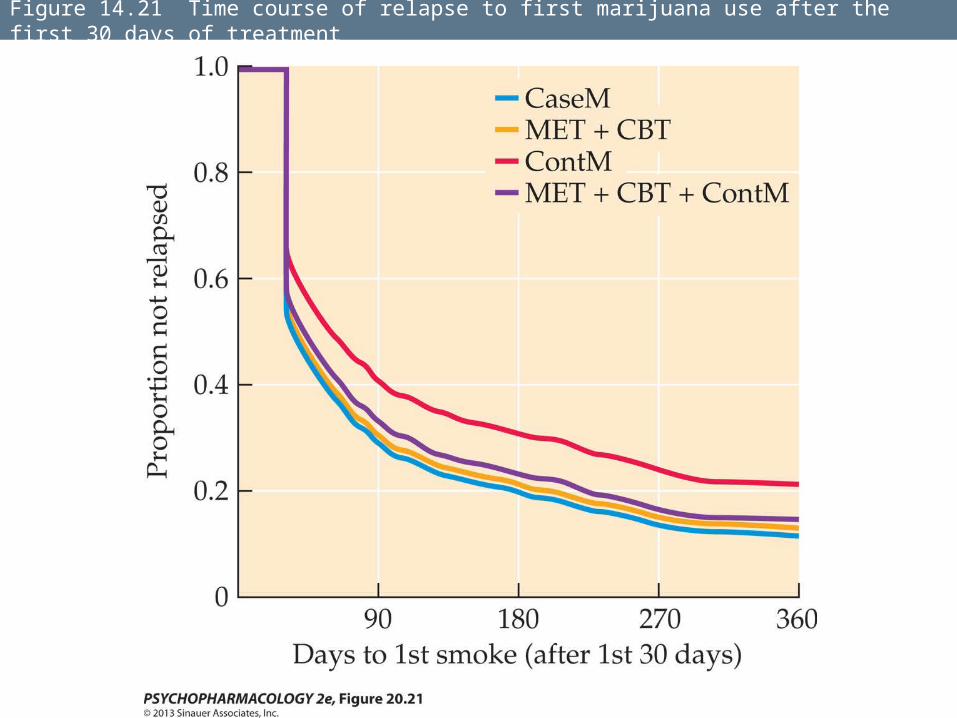
Figure 14.21 Time course of relapse to first marijuana use after the first 30 days of treatment
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Effects of chronic cannabis use
In young people, amount of cannabis use is inversely related to educational performance.
Some research supports the hypothesis that heavy cannabis use leads to persistent cognitive deficits, impairing school performance.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Alternatively, poor school performance and rejection of mainstream values such as educational achievement may increase cannabis use.
Chronic cannabis use can also result in aimlessness, decreased motivation, lack of planning, and decreased productivity—amotivational syndrome.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Imaging studies suggest that chronic marijuana use is associated with several kinds of abnormalities in the brain.
Several studies have found a significant relationship between early heavy marijuana smoking and increased risk for later development of psychotic disorders such as schizophrenia.
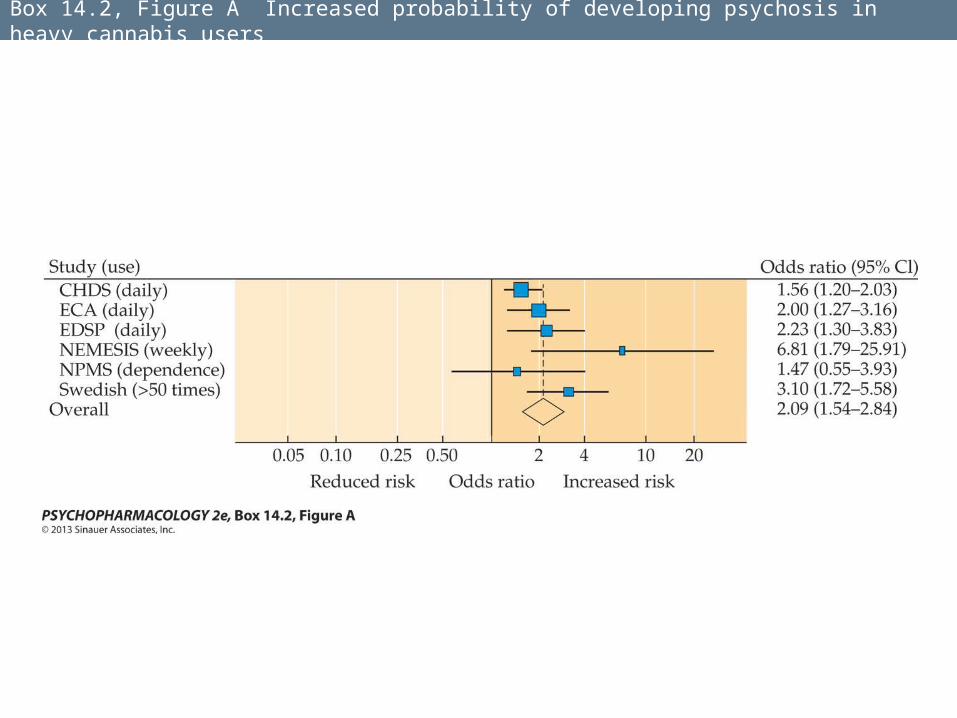
Box 14.2, Figure A Increased probability of developing psychosis in heavy cannabis users
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Other researchers question some of these results and suggest other interpretations of the relationship.
1. Association model—individuals who are already vulnerable to developing psychosis have an increased likelihood of using cannabis when they are young
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
2. Causal model—heavy use predisposes individuals to develop psychosis later in life.
3. Indicator-variable model—one or more other factors lead jointly to cannabis use and psychosis proneness.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Health effects:
There are no reports of death from overdose.
Smoking marijuana can damage lungs—smoke contains tar, carcinogens, carbon monoxide, etc.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
THC has been found to impair resistance to bacterial and viral infections under controlled experimental conditions, but it is not clear yet whether this occurs in real-life conditions.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
THC may affect reproductive functions:• Supresses release of LH (luteinizing
hormone).
Other animal work has demonstrated pregnancy failure, retarded embryonic development, and even fetal death with THC administration, but this has not yet been reported in controlled human studies.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
In men, regular smoking has been shown to decrease testosterone levels and sperm counts.
Smoking during pregnancy: cognitive deficits, poor school achievement, and increased risk for tobacco and/or marijuana use later in life have all been associated with prenatal marijuana exposure.
Cannabis Abuse and the Effects of Chronic Cannabis Exposure
Synthetic designer cannabinoids – “K2” or “Spice.”
Appeared in 2004 on the Internet; produce several adverse physiological and psychological effects.
They have been placed under Schedule I, which bans recreational use.