Embed Size (px)
DESCRIPTION
The Oncology Nurse
Citation preview

The Official Publication for the Hem/Onc Nurse & Advanced Practitioner
MARCH/APRIL 2011 www.TheOncologyNurse.com VOL 4, NO 2
©2011 Green Hill Healthcare Communications, LLC
At the 16th Annual Conference ofthe National ComprehensiveCancer Network (NCCN), chair-
persons of the various tumor panels pre-sented updates to the NCCN ClinicalPractice Guidelines and explained the rea-soning behind these changes. We reviewthe most important updates to the guide-lines for breast, prostate, and lung cancerand for various hematologic malignan-cies, including non-Hodgkin lymphoma
and chronic myelogenous leukemia(CML). This brief overview is for infor-mational purposes and is not intended toguide treatment decisions. You areencouraged to visit www.nccn.org toreview the complete guidelines and theirrespective references.
Breast CancerPivotal research and drug approvals in
the past year led to changes that are imme-
Clockwise from top left: Walter M. Sahijdak, MD; Philip J. Stella, MD; Lara Blair, RN; and Vita McCabe, MD; of the multidisciplinary lung clinic at St. Joseph Mercy Cancer Center.
St. Joseph Mercy Cancer Care CenterA Cancer Hospital in a Small Community Has Big PlansBy Dawn Lagrosa
Following a lung cancer diagnosis, patients typically embark on adizzying journey that takes them from one waiting room to anoth-er, as they follow their treatment plan from the medical oncologist
to the surgical oncologist to the radiation oncologist and back again.Coordinating these visits imposes yet another burden on the patientand often leads to delays in care. Six years ago, St. Joseph MercyCancer Center in Ypsilanti, Michigan, decided to simplify life for theirpatients by opening a multidisciplinary lung cancer clinic.
CANCER CENTER PROFILE
Continued on page 17
GUIDELINES
NCCN Updates TreatmentGuidelines Revisions Expected to Change PracticeBy Audrey Andrews
THE WHOLE PATIENT
Are You Talking to PatientsAbout Smoking Cessation?By Christin Melton
Continued on page 44
Continued on page 39
Despite aggressive campaigns toeducate Americans on the life-threatening risks of smoking,
nearly 500,000 people die each year inthe United States from smoking-relatedillness, according to a recent study inEpidemiology. Even patients with smok-ing-related cancers have trouble quitting,with about two-thirds of patients withlung cancer continuing to smoke.
At the annual meeting of theHematology/Oncology Pharmacy As -sociation, Jane Pruemer, PharmD,BCOP, FASHP, professor of clinicalpharmacy practice at the University ofCincinnati’s James L. Winkle College ofPharmacy in Ohio, suggested clinicianshave an obligation to encourage patientswith cancer who smoke to give up thehabit. “It is inconsistent to provide health-
COMPLIMENTARY CE . . . . . . . . . . . 32Follow-up Management of HodgkinLymphoma Survivors
DRUG SHORTAGES . . . . . . . . . . . . 13A Growing Crisis in Oncology
CONFERENCE NEWS
ASCO Gastrointestinal CancersSymposium . . . . . . . . . . . . . . . . . . . . . 18ASCO Genitourinary CancersSymposium . . . . . . . . . . . . . . . . . . . . . 22
SUPPORTIVE CARE . . . . . . . . . . . . 28Managing Anthracycline Extravasation
THE WHOLE PATIENT . . . . . . . . . . 42Cancer Treatment–Induced DiarrheaElderly Patients with Comorbidities
NEWS IN REVIEW . . . . . . . . . . . . . . 50Eribulin for Heavily PretreatedMetastatic Breast CancerAxillary Lymph Node DissectionUnnecessary for Some
I N S I D E©iStockphoto.com/Eduardo Jose Bernardino
For more CE Opportunities and to take the posttest for
the CE article in this issue, visit
www.TheOncologyNurse.com
VISIT US
TON_April2011_v7_TON 4/7/11 12:16 PM Page 1

D
T
f
a
T
v
T
v
H
s
‡
b
So. San Francisco, CA All rights reserved. 10581800 11/10
Announcingthe first and only monoclonal antibody indicated for use inHER2+ metastatic gastric and gastroesophageal junction (GEJ) cancer
to drive outcomes in HER2+ metastatic gastric/GEJ cancer
Boxed WARNINGS Herceptin administration can result in sub-clinical and clinical cardiac failure. The incidence and severity was highest in patients receiving Herceptin with anthracycline-containing chemotherapy regimens. In a pivotal adjuvant breast cancer trial, one patient who developed CHF died of cardiomyopathy
Evaluate cardiac function prior to and during treatment. Discontinue Herceptin for cardiomyopathy
Herceptin can result in serious and fatal infusion reactions and pulmonary toxicity. Discontinue Herceptin for anaphylaxis, angioedema, interstitial pneumonitis, or acute respiratory distress syndrome
Exposure to Herceptin during pregnancy can result in oligohydramnios, in some cases complicated by pulmonary hypoplasia and neonatal death
Indication Herceptin is indicated, in combination with cisplatin and capecitabine or 5-fluorouracil, for the treatment of patients with HER2 overexpressing metastatic gastric or gastroesophageal junction adenocarcinoma, who have not received prior treatment for metastatic disease.
S
TON_April2011_v7_TON 4/7/11 10:47 AM Page Cov2

Additional Important Safety Information Exacerbation of chemotherapy-induced neutropenia has also occurred
Detection of HER2 protein overexpression is necessary for selection of patients appropriate for Herceptin therapy
The most common adverse reactions associated with Herceptin were neutropenia, diarrhea, fatigue, anemia, stomatitis, weight loss, upper respiratory tract infections, fever, thrombocytopenia, mucosal inflammation, nasopharyngitis, and dysgeusia
Please see brief summary of full Prescribing Information, including Boxed WARNINGS and additional important safety information, on the following pages.
Reference: 1. Herceptin Prescribing Information. Genentech, Inc. October 29, 2010.
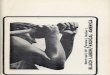
Months
Final Median Overall Survival Analysis1
Updated Median Overall Survival Analysis1‡
11.0
13.5
0 3 6 9 12 15
Herceptin plus chemotherapy* (n=298)
Chemotherapy alone* (n=296)
Hazard Ratio = 0.7395% CI: 0.60-0.91
P=0.0038
Hazard Ratio = 0.8095% CI: 0.67-0.97 11.7
13.1
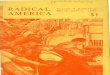
In the ToGA trial†:
• The final overall survival analysis demonstrated a 13.5-month median OS with Herceptin + chemotherapy (cisplatin and either capecitabine or 5-fluorouracil) vs an 11.0-month median OS with chemotherapy alone1
• The updated overall survival analysis demonstrated a 13.1-month median OS with Herceptin + chemotherapy (cisplatin and either capecitabine or 5-fluorouracil) vs an 11.7-month median OS with chemotherapy alone1
• Herceptin should be administered until disease progression or unacceptable toxicity in HER2+ metastatic gastric and GEJ cancer
Herceptin plus chemotherapy* extended median overall survival (OS) in HER2+ metastatic gastric and GEJ cancer1
*Chemotherapy was cisplatin and either capecitabine or 5-FU. ‡ The updated analysis was conducted one year after the final analysis. No P value
was associated with the updated analysis in the Herceptin Prescribing Information because there was no preplanned statistical testing for OS after the final analysis.
†Trastuzumab in gastric cancer.
©2010 Genentech USA, Inc. So. San Francisco, CA All rights reserved. 10581800 11/10
HER2+ metastatic gastric/GEJ cancer
B H
a c
E
H
a
E
t
TON_April2011_v7_TON 4/7/11 10:47 AM Page 3

HERCEPTIN® (trastuzumab)Brief Summary For full Prescribing Information, see package insert.
WARNING: CARDIOMYOPATHY, INFUSION REACTIONS, EMBRYO-FETAL TOXICITY, and PULMONARY TOXICITY Cardiomyopathy Herceptin administration can result in sub clinical and clinical cardiac failure. The incidence and severity was highest in patients receiving Herceptin with anthracycline containing chemotherapy regimens. Evaluate left ventricular function in all patients prior to and during treatment with Herceptin. Discontinue Herceptin treatment in patients receiving adjuvant therapy and withhold Herceptin in patients with metastatic disease for clinically significant decrease in left ventricular function. [see Warnings and Precautions and Dosage and Administration]Infusion Reactions; Pulmonary Toxicity Herceptin administration can result in serious and fatal infusion reactions and pulmonary toxicity. Symptoms usually occur during or within 24 hours of Herceptin administration. Interrupt Herceptin infusion for dyspnea or clinically significant hypotension. Monitor patients until symptoms completely resolve. Discontinue Herceptin for anaphylaxis, angioedema, interstitial pneumonitis, or acute respiratory distress syndrome. [see Warnings and Precautions] Embryo-Fetal Toxicity Exposure to Herceptin during pregnancy can result in oligohydramnios and oligohydramnios sequence manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. [see Warnings and Precautions, Use in Specific Populations]
INDICATIONS AND USAGE Adjuvant Breast Cancer Herceptin is indicated for adjuvant treatment of HER2 overexpressing node positive or node negative (ER/PR negative or with one high risk feature [see Clinical Studies] breast cancer • as part of a treatment regimen consisting of doxorubicin, cyclophosphamide, and either paclitaxel or docetaxel • with docetaxel and carboplatin • as a single agent following multi-modality anthracycline based therapy. Metastatic Breast Cancer Herceptin is indicated: • In combination with paclitaxel for first-line treatment of HER2-overexpressing metastatic breast cancer • As a single agent for treatment of HER2-overexpressing breast cancer in patients who have received one or more chemotherapy regimens for metastatic disease. Metastatic Gastric Cancer Herceptin is indicated, in combination with cisplatin and capecitabine or 5-fluorouracil, for the treatment of patients with HER2 overexpressing metastatic gastric or gastroesophageal junction adenocarcinoma, who have not received prior treatment for metastatic disease. CONTRAINDICATIONS None. WARNINGS AND PRECAUTIONS Cardiomyopathy Herceptin can cause left ventricular cardiac dysfunction, arrhythmias, hypertension, disabling cardiac failure, cardiomyopathy, and cardiac death [see Boxed Warning: Cardiomyopathy]. Herceptin can also cause asymptomatic decline in left ventricular ejection fraction (LVEF). There is a 4−6 fold increase in the incidence of symptomatic myocardial dysfunction among patients receiving Herceptin as a single agent or in combination therapy compared with those not receiving Herceptin. The highest absolute incidence occurs when Herceptin is administered with an anthracycline. Withhold Herceptin for 16% absolute decrease in LVEF from pre-treatment values or an LVEF value below institutional limits of normal and 10% absolute decrease in LVEF from pretreatment values [see Dosage and Administration]. The safety of continuation or resumption of Herceptin in patients with Herceptin-induced left ventricular cardiac dysfunction has not been studied. Cardiac Monitoring Conduct thorough cardiac assessment, including history, physical examination, and determination of LVEF by echocardiogram or MUGA scan. The following schedule is recommended: • Baseline LVEF measurement immediately prior to initiation of Herceptin • LVEF measurements every 3 months during and upon completion of Herceptin • Repeat LVEF measurement at 4 week intervals if Herceptin is withheld for significant left ventricular cardiac dysfunction [see Dosage and Administration] • LVEF measurements every 6 months for at least 2 years following completion of Herceptin as a component of adjuvant therapy. In Study 1, 16% (136/844) of patients discontinued Herceptin due to clinical evidence of myocardial dysfunction or significant decline in LVEF. In Study 3, the number of patients who discontinued Herceptin due to cardiac toxicity was 2.6% (44/1678). In Study 4, a total of 2.9% (31/1056) patients in the TCH arm (1.5% during the chemotherapy phase and 1.4% during the monotherapy phase) and 5.7% (61/1068) patients in the AC-TH arm (1.5% during the chemotherapy phase and 4.2% during the monotherapy phase) discontinued Herceptin due to cardiac toxicity. Among 32 patients receiving adjuvant chemotherapy (Studies 1 and 2) who developed congestive heart failure, one patient died of cardiomyopathy and all other patients were receiving cardiac medication at last follow-up. Approximately half of the surviving patients had recovery to a normal LVEF (defined as 50%) on continuing medical management at the time of last follow-up. Incidence of congestive heart failure is presented in Table 1. The safety of continuation or resumption of Herceptin in patients with Herceptin-induced left ventricular cardiac dysfunction has not been studied.Table 1 Incidence of Congestive Heart Failure in Adjuvant Breast Cancer Studies
Incidence of CHF Study Regimen Herceptin Control 1 & 2a ACb Paclitaxel+ Herceptin 2% (32/1677) 0.4% (7/1600) 3 Chemo Herceptin 2% (30/1678) 0.3% (5/1708) 4 ACb Docetaxel+ Herceptin 2% (20/1068) 0.3% (3/1050) 4 Docetaxel+Carbo+ Herceptin 0.4% (4/1056) 0.3% (3/1050)
a Includes 1 patient with fatal cardiomyopathy.b Anthracycline (doxorubicin) and cyclophosphamide
Table 2 Incidence of Cardiac Dysfunctiona in Metastatic Breast Cancer Studies
Incidence NYHA I−IV NYHA III−IV Study Event Herceptin Control Herceptin Control 5 Cardiac (AC)b Dysfunction 28% 7% 19% 3% 5 Cardiac (paclitaxel) Dysfunction 11% 1% 4% 1% 6 Cardiac Dysfunctionc 7% N/A 5% N/A
a Congestive heart failure or significant asymptomatic decrease in LVEF.
b Anthracycline (doxorubicin or epirubicin) and cyclophosphamide.
c Includes 1 patient with fatal cardiomyopathy.In Study 4, the incidence of NCI-CTC Grade 3/4 cardiac ischemia/infarction was higher in the Herceptin containing regimens: (AC-TH: 0.3% (3/1068) and TCH 0.2% (2/1056)) as compared to none in AC-T. Infusion Reactions Infusion reactions consist of a symptom complex characterized by fever and chills, and on occasion included nausea, vomiting, pain (in some cases at tumor sites), headache, dizziness, dyspnea, hypotension, rash, and asthenia. [see Adverse Reactions] In postmarketing reports, serious and fatal infusion reactions have been reported. Severe reactions which include bronchospasm, anaphylaxis, angioedema, hypoxia, and severe hypotension, were usually reported during or immediately following the initial infusion. However, the onset and clinical course were variable including progressive worsening, initial improvement followed by clinical deterioration, or delayed post-infusion events with rapid clinical deterioration. For fatal events, death occurred within hours to days following a serious infusion reaction. Interrupt Herceptin infusion in all patients experiencing dyspnea, clinically significant hypotension, and intervention of medical therapy administered, which may include: epinephrine, corticosteroids, diphenhydramine, bronchodilators, and oxygen. Patients should be evaluated and carefully monitored until complete resolution of signs and symptoms. Permanent discontinuation should be strongly considered in all patients with severe infusion reactions. There are no data regarding the most appropriate method of identification of patients who may safely be retreated with Herceptin after experiencing a severe infusion reaction. Prior to resumption of Herceptin infusion, the majority of patients who experienced a severe infusion reaction were pre-medicated with antihistamines and/or corticosteroids. While some patients tolerated Herceptin infusions, others had recurrent severe infusion reactions despite pre-medications. Embryo-Fetal Toxicity Herceptin can cause fetal harm when administered to a pregnant woman. In post-marketing reports, use of Herceptin during pregnancy resulted in cases of oligohydramnios and oligohydramnios sequence manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. Advise women of the potential hazard to the fetus resulting from Herceptin exposure during pregnancy and provide contraception counseling to women of childbearing potential. [see Use in Specific Populations, Patient Counseling Information]. Pulmonary Toxicity Herceptin use can result in serious and fatal pulmonary toxicity. Pulmonary toxicity includes dyspnea, interstitial pneumonitis, pulmonary infiltrates, pleural effusions, non-cardiogenic pulmonary edema, pulmonary insufficiency and hypoxia, acute respiratory distress syndrome, and pulmonary fibrosis. Such events can occur as sequelae of infusion reactions [see Warnings and Precautions]. Patients with symptomatic intrinsic lung disease or with extensive tumor involvement of the lungs, resulting in dyspnea at rest, appear to have more severe toxicity. Exacerbation of Chemotherapy-Induced Neutropenia In randomized, controlled clinical trials the per-patient incidences of NCI CTC Grade 3−4 neutropenia and of febrile neutropenia were higher in patients receiving Herceptin in combination with myelosuppressive chemotherapy as compared to those who received chemotherapy alone. The incidence of septic death was similar among patients who received Herceptin and those who did not. [see Adverse Reactions] HER2 Testing Detection of HER2 protein overexpression is necessary for selection of patients appropriate for Herceptin therapy because these are the only patients studied and for whom benefit has been shown. Due to differences in tumor histopathology, use FDA-approved tests for the specific tumor type (breast or gastric/gastroesophageal adenocarcinoma) to assess HER2 protein overexpression and HER2 gene amplification. Tests should be performed by laboratories with demonstrated proficiency in the specific technology being utilized. Improper assay performance, including use of suboptimally fixed tissue, failure to utilize specified reagents, deviation from specific assay instructions, and failure to include appropriate controls for assay validation, can lead to unreliable results. Several FDA-approved commercial assays are available to aid in the selection of breast cancer and metastatic gastric cancer patients for Herceptin therapy. Users should refer to the package inserts of specific assay kits for information on the Intended Use, and the validation and performance of each assay. Limitations in assay precision make it inadvisable to rely on a single method to rule out potential Herceptin benefit. Treatment outcomes for adjuvant breast cancer (Studies 2 and 3) and for metastatic breast cancer (Study 5) as a function of IHC and FISH testing are provided in Tables 8 and 10. Assessment of HER2 protein overexpression and HER2 gene amplification in metastatic gastric cancer should be performed using FDA-approved tests specifically for gastric cancers due to differences in gastric vs. breast histopathology, including incomplete membrane staining and more frequent heterogeneous expression of HER2 seen in gastric cancers. Study 7 demonstrated that gene amplification and protein overexpression were not as well correlated as with breast cancer. Treatment outcomes for metastatic gastric cancer (Study 7), based on HER2 gene amplification (FISH) and HER2 protein overexpression (IHC) test results are provided in Table 12. ADVERSE REACTIONS The following adverse reactions are discussed in greater detail in other sections of the label: • Cardiomyopathy [see Warnings and Precautions] • Infusion reactions [see Warnings and
Precautions] • Embryo-fetal Toxicity [see Warnings and Precautions] • Pulmonary toxicity [see Warnings and Precautions] • Exacerbation of chemotherapy-induced neutropenia [see Warnings and Precautions] The most common adverse reactions in patients receiving Herceptin in the adjuvant and metastatic breast cancer setting are fever, nausea, vomiting, infusion reactions, diarrhea, infections, increased cough, headache, fatigue, dyspnea, rash, neutropenia, anemia, and myalgia. Adverse reactions requiring interruption or discontinuation of Herceptin treatment include CHF, significant decline in left ventricular cardiac function, severe infusion reactions, and pulmonary toxicity [see Dosage and Administration]. In the metastatic gastric cancer setting, the most common adverse reactions ( 10%) that were increased ( 5% difference) in the Herceptin arm as compared to the chemotherapy alone arm were neutropenia, diarrhea, fatigue, anemia, stomatitis, weight loss, upper respiratory tract infections, fever, thrombocytopenia, mucosal inflammation, nasopharyngitis, and dysgeusia. The most common adverse reactions which resulted in discontinuation of treatment on the Herceptin-containing arm in the absence of disease progression were infection, diarrhea, and febrile neutropenia. Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Adjuvant Breast Cancer Studies The data below reflect exposure to Herceptin across three randomized, open-label studies, Studies 1, 2, and 3, with (n= 3355) or without (n= 3308) trastuzumab in the adjuvant treatment of breast cancer. The data summarized in Table 3 below, from Study 3, reflect exposure to Herceptin in 1678 patients; the median treatment duration was 51 weeks and median number of infusions was 18. Among the 3386 patients enrolled in Study 3, the median age was 49 years (range: 21 to 80 years), 83% of patients were Caucasian, and 13% were Asian.Table 3 Adverse Reactions for Study 3, All Gradesa:
1 Year Herceptin Observation Adverse Reaction (n= 1678) (n=1708)
CardiacHypertension 64 (4%) 35 (2%)Dizziness 60 (4%) 29 (2%)Ejection Fraction Decreased 58 (3.5%) 11 (0.6%)Palpitations 48 (3%) 12 (0.7%)Cardiac Arrhythmiasb 40 (3%) 17 (1%)Cardiac Failure Congestive 30 (2%) 5 (0.3%)Cardiac Failure 9 (0.5%) 4 (0.2%)Cardiac Disorder 5 (0.3%) 0 (0%)Ventricular Dysfunction 4 (0.2%) 0 (0%)Respiratory Thoracic Mediastinal DisordersCough 81 (5%) 34 (2%)Influenza 70 (4%) 9 (0.5%)Dyspnea 57 (3%) 26 (2%)URI 46 (3%) 20 (1%)Rhinitis 36 (2%) 6 (0.4%)Pharyngolaryngeal Pain 32 (2%) 8 (0.5%)Sinusitis 26 (2%) 5 (0.3%)Epistaxis 25 (2%) 1 (0.06%)Pulmonary Hypertension 4 (0.2%) 0 (0%)Interstitial Pneumonitis 4 (0.2%) 0 (0%)Gastrointestinal DisordersDiarrhea 123 (7%) 16 (1%)Nausea 108 (6%) 19 (1%)Vomiting 58 (3.5%) 10 (0.6%)Constipation 33 (2%) 17 (1%)Dyspepsia 30 (2%) 9 (0.5%)Upper Abdominal Pain 29 (2%) 15 (1%)Musculoskeletal & Connective Tissue DisordersArthralgia 137 (8%) 98 (6%)Back Pain 91 (5%) 58 (3%)Myalgia 63 (4%) 17 (1%)Bone Pain 49 (3%) 26 (2%)Muscle Spasm 46 (3%) 3 (0.2%)Nervous System DisordersHeadache 162 (10%) 49 (3%)Paraesthesia 29 (2%) 11 (0.6%)Skin & Subcutaneous Tissue DisordersRash 70 (4%) 10 (0.6%)Nail Disorders 43 (2%) 0 (0%)Pruritis 40 (2%) 10 (0.6%)General DisordersPyrexia 100 (6%) 6 (0.4%)Edema Peripheral 79 (5%) 37 (2%)Chills 85 (5%) 0 (0%)Aesthenia 75 (4.5%) 30 (2%)Influenza-like Illness 40 (2%) 3 (0.2%)Sudden Death 1 (0.06%) 0 (0%)InfectionsNasopharyngitis 135 (8%) 43 (3%)UTI 39 (3%) 13 (0.8%)Immune System DisordersHypersensitivity 10 (0.6%) 1 (0.06%)Autoimmune Thyroiditis 4 (0.3%) 0 (0%)
a The incidence of Grade 3/4 adverse reactions was <1% in both arms for each listed term.
b Higher level grouping term.The data from Studies 1 and 2 were obtained from 3206 patients, of whom 1635 received Herceptin; the median treatment duration was 50 weeks. The median age was 49 years (range: 24−80); 84% of patients were White, 7% Black, 4% Hispanic, and 4% Asian. In Study 1, only Grade 3−5 adverse events, treatment-related Grade 2 events, and Grade 2−5 dyspnea were collected during and for up to 3 months following protocol-specified treatment. The following non-cardiac adverse reactions of Grade 2−5 occurred at an incidence of at least 2% greater among patients randomized to Herceptin plus chemotherapy as compared to chemotherapy alone: arthralgia (31% vs. 28%), fatigue (28% vs. 22%), infection (22% vs. 14%), hot flashes (17% vs. 15%), anemia (13% vs. 7%), dyspnea (12% vs. 4%), rash/desquamation (11% vs. 7%), neutropenia (7% vs. 5%), headache (6% vs. 4%), and insomnia (3.7% vs. 1.5%). The majority of these events were Grade
2 in severity. In Study 2, data collection was limited to the following investigator-attributed treatment-related adverse reactions: NCI-CTC Grade 4 and 5 hematologic toxicities, Grade 3−5 non-hematologic toxicities, selected Grade 2−5 toxicities associated with taxanes (myalgia, arthralgias, nail changes, motor neuropathy, sensory neuropathy) and Grade 1−5 cardiac toxicities occurring during chemotherapy and/or Herceptin treatment. The following non-cardiac adverse reactions of Grade 2−5 occurred at an incidence of at least 2% greater among patients randomized to Herceptin plus chemotherapy as compared to chemotherapy alone: arthralgia (11% vs. 8.4%), myalgia (10% vs. 8%), nail changes (9% vs. 7%), and dyspnea (2.5% vs. 0.1%). The majority of these events were Grade 2 in severity. Safety data from Study 4 reflect exposure to Herceptin as part of an adjuvant treatment regimen from 2124 patients receiving at least one dose of study treatment [AC-TH: n = 1068; TCH: n = 1056]. The overall median treatment duration was 54 weeks in both the AC-TH and TCH arms. The median number of infusions was 26 in the AC-TH arm and 30 in the TCH arm, including weekly infusions during the chemotherapy phase and every three week dosing in the monotherapy period. Among these patients, the median age was 49 years (range 22 to 74 years). In Study 4, the toxicity profile was similar to that reported in Studies 1, 2, and 3 with the exception of a low incidence of CHF in the TCH arm. Metastatic Breast Cancer Studies The data below reflect exposure to Herceptin in one randomized, open-label study, Study 5, of chemotherapy with (n=235) or without (n=234) trastuzumab in patients with metastatic breast cancer, and one single-arm study (Study 6; n=222) in patients with metastatic breast cancer. Data in Table 4 are based on Studies 5 and 6. Among the 464 patients treated in Study 5, the median age was 52 years (range: 25−77 years). Eighty-nine percent were White, 5% Black, 1% Asian and 5% other racial/ethnic groups. All patients received 4 mg/kg initial dose of Herceptin followed by 2 mg/kg weekly. The percentages of patients who received Herceptin treatment for 6 months and 12 months were 58% and 9%, respectively. Among the 352 patients treated in single agent studies (213 patients from Study 6), the median age was 50 years (range 28−86 years), 86% were White, 3% were Black, 3% were Asian, and 8% in other racial/ethnic groups. Most of the patients received 4 mg/kg initial dose of Herceptin followed by 2 mg/kg weekly. The percentages of patients who received Herceptin treatment for 6 months and
12 months were 31% and 16%, respectively.Table 4 Per-Patient Incidence of Adverse Reactions Occurring in 5% of Patients in Uncontrolled Studies or at Increased Incidence in the Herceptin Arm (Studies 5 and 6)
Herceptin Single + Paclitaxel Herceptin ACb
Agenta Paclitaxel Alone + ACb Alone n = 352 n = 91 n = 95 n = 143 n = 135Body as a Whole Pain 47% 61% 62% 57% 42% Asthenia 42% 62% 57% 54% 55% Fever 36% 49% 23% 56% 34% Chills 32% 41% 4% 35% 11% Headache 26% 36% 28% 44% 31% Abdominal pain 22% 34% 22% 23% 18% Back pain 22% 34% 30% 27% 15% Infection 20% 47% 27% 47% 31% Flu syndrome 10% 12% 5% 12% 6% Accidental injury 6% 13% 3% 9% 4% Allergic reaction 3% 8% 2% 4% 2%Cardiovascular Tachycardia 5% 12% 4% 10% 5% Congestive 7% 11% 1% 28% 7% heart failureDigestive Nausea 33% 51% 9% 76% 77% Diarrhea 25% 45% 29% 45% 26% Vomiting 23% 37% 28% 53% 49% Nausea and vomiting 8% 14% 11% 18% 9% Anorexia 14% 24% 16% 31% 26% Heme & Lymphatic Anemia 4% 14% 9% 36% 26% Leukopenia 3% 24% 17% 52% 34%Metabolic Peripheral edema 10% 22% 20% 20% 17% Edema 8% 10% 8% 11% 5%Musculoskeletal Bone pain 7% 24% 18% 7% 7% Arthralgia 6% 37% 21% 8% 9%Nervous Insomnia 14% 25% 13% 29% 15% Dizziness 13% 22% 24% 24% 18% Paresthesia 9% 48% 39% 17% 11% Depression 6% 12% 13% 20% 12% Peripheral neuritis 2% 23% 16% 2% 2% Neuropathy 1% 13% 5% 4% 4%Respiratory Cough increased 26% 41% 22% 43% 29% Dyspnea 22% 27% 26% 42% 25% Rhinitis 14% 22% 5% 22% 16% Pharyngitis 12% 22% 14% 30% 18% Sinusitis 9% 21% 7% 13% 6%Skin Rash 18% 38% 18% 27% 17% Herpes simplex 2% 12% 3% 7% 9% Acne 2% 11% 3% 3% < 1%Urogenital Urinary tract infection 5% 18% 14% 13% 7%
a Data for Herceptin single agent were from 4 studies, including 213 patients from Study 6.
b Anthracycline (doxorubicin or epirubicin) and cyclophosphamide.
M
( In the Herceptin plus chemotherapy arm, the initial d
21 days until d
Herceptin +FC FC N (%)
B
2 (1) 43 (15) 6 (2) 7 (2) 10 ( 3) 1 (
Inflammation 37 (13) 6 (2) 18 (6) 2 (1)
Tract Infections 56 (19) 0 (0) 29 (10) 0 (0) (0) 17 (6) 0 (0)R
Impairment 53 (18) 8 (3) 42 (15) 5 (2)N
P
LVEF Decrease
LVEF <50% decrease decrease
For Studies 1, 2 and 3, events are counted from the beginning o
Studies 1 and 2 regimens: doxorubicin and cyclo-p
Study 4 regimens: doxorubicin and cyclophosphamide
f
S Cumulative Incidence of Time to First LVEF D
i
t
a o
Following the a
In Study 7 (
In a randomized, controlled trial in p N
The most common
p
An increased incidence of d
1
Samples for assessment of
H
t
D I
w
i
Pregnancy: Category D [s
If oligohydramnios occurs,
p a T
phone 1-800-690-6720. [s
Infant monkeys with detectable serum levels of t
Limitations in data collection and d
<
T
• Advise patients to contact a health care professional i
5 pounds in 24 hours, dizziness or loss of consciousness [s Cardiomyopathy]
(
TON_April2011_v7_TON 4/7/11 10:47 AM Page 4

F
Adjuvant Breast Cancer H
(
• as a single agent following multi-modality anthracycline b
N Cardiomyopathy H
o
Herceptin 2% (32/1677) 0.4% (7/1600) ACb
Herceptin 2% (20/1068) 0.3% (3/1050) Docetaxel+Carbo+ Herceptin 0.4% (4/1056) 0.3% (3/1050)
a
I
NYHA III−IV Congestive heart failure or significant asymptomatic
d Anthracycline (doxorubicin or epirubicin) and
c
Severe reactions which
i
Prior to resumption of Herceptin infusion, t
While some patients tolerated Herceptin
i
T
o
The most c
i
(
S
S
1 Year Herceptin Observation
The incidence of Grade 3/4 adverse reactions was <1% in b
received Herceptin; the median t
A
S
The percentages of p
Herceptin Single + Paclitaxel Herceptin ACb
Agenta
n = 352 n = 91 n = 95 n = 143 n = 135B pain 22% 34% 22% 23% 18% injury 6% 13% 3% 9% 4% reaction 3% 8% 2% 4% 2%C
vomiting 8% 14% 11% 18% 9%
edema 10% 22% 20% 20% 17%
neuritis 2% 23% 16% 2% 2%
increased 26% 41% 22% 43% 29%
simplex 2% 12% 3% 7% 9%
infection 5% 18% 14% 13% 7%
a Data for Herceptin single agent were from 4 studies, i
Anthracycline (doxorubicin or epirubicin) and c
Metastatic Gastric Cancer The data below are based on the exposure of 294 patients to Herceptin in combination with a fluoropyrimidine (capecitabine or 5-FU) and cisplatin (Study 7). In the Herceptin plus chemotherapy arm, the initial dose of Herceptin 8 mg/kg was administered on Day 1 (prior to chemotherapy) followed by 6 mg/kg every 21 days until disease progression. Cisplatin was administered at 80 mg/m2 on Day 1 and the fluoropyrimidine was administered as either capecitabine 1000 mg/m2 orally twice a day on Days 1-14 or 5-fluorouracil 800 mg/m2/day as a continuous intravenous infusion Days 1 through 5. Chemotherapy was administered for six 21-day cycles. Median duration of Herceptin treatment was 21 weeks; median number of Herceptin infusions administered was eight.Table 5 Study 7: Per Patient Incidence of Adverse Reactions of All Grades (Incidence 5% between Arms) or Grade 3 /4 (Incidence >1% between Arms) and Higher Incidence in Herceptin Arm
Herceptin +FC FC (N = 294) (N = 290) N (%) N (%)
Body System/ All Grades All GradesAdverse Event Grades 3 / 4 Grades 3/ 4
Investigations Neutropenia 230 (78) 101 (34) 212 (73) 83 (29) Hypokalemia 83 (28) 28 (10) 69 (24) 16 (6) Anemia 81 (28) 36 (12) 61 (21) 30 (10) Thrombocytopenia 47 (16) 14 (5) 33 (11) 8 (3)Blood And Lymphatic System Disorders Febrile Neutropenia _ 15 (5) _ 8 (3)Gastrointestinal Disorders Diarrhea 109 (37) 27 (9) 80 (28) 11 (4) Stomatitis 72 (24) 2 (1) 43 (15) 6 (2) Dysphagia 19 (6) 7 (2) 10 ( 3) 1 ( 1)Body as a Whole Fatigue 102 (35) 12 (4) 82 (28) 7 (2) Fever 54 (18) 3 (1) 36 (12) 0 (0) Mucosal Inflammation 37 (13) 6 (2) 18 (6) 2 (1) Chills 23 (8) 1 ( 1) 0 (0) 0 (0)Metabolism And Nutrition Disorders Weight Decrease 69 (23) 6 (2) 40 (14) 7 (2)Infections And Infestations Upper Respiratory Tract Infections 56 (19) 0 (0) 29 (10) 0 (0) Nasopharyngitis 37 (13) 0 (0) 17 (6) 0 (0)Renal And Urinary Disorders Renal Failure and Impairment 53 (18) 8 (3) 42 (15) 5 (2)Nervous System Disorders Dysgeusia 28 (10) 0 (0) 14 (5) 0 (0)
The following subsections provide additional detail regarding adverse reactions observed in clinical trials of adjuvant breast, metastatic breast cancer, metastatic gastric cancer, or post-marketing experience. Cardiomyopathy Serial measurement of cardiac function (LVEF) was obtained in clinical trials in the adjuvant treatment of breast cancer. In Study 3, the median duration of follow-up was 12.6 months (12.4 months in the observation arm; 12.6 months in the 1-year Herceptin arm); and in Studies 1 and 2, 23 months in the AC-T arm, 24 months in the AC-TH arm. In Studies 1 and 2, 6% of patients were not permitted to initiate Herceptin following completion of AC chemotherapy due to cardiac dysfunction (LVEF < 50% or
15 point decline in LVEF from baseline to end of AC). Following initiation of Herceptin therapy, the incidence of new-onset dose-limiting myocardial dysfunction was higher among patients receiving Herceptin and paclitaxel as compared to those receiving paclitaxel alone in Studies 1 and 2, and in patients receiving Herceptin monotherapy compared to observation in Study 3 (see Table 6, Figures 1 and 2).Table 6a Per-patient Incidence of New Onset Myocardial Dysfunction (by LVEF) Studies 1, 2, 3 and 4
LVEF <50% and Absolute Decrease Absolute from Baseline LVEF Decrease
LVEF 10% 16% <20% and <50% decrease decrease 10% 20%
Studies 1 & 2b AC TH 22.8% 18.3% 11.7% 33.4% 9.2% (n=1606) (366) (294) (188) (536) (148)
AC T 9.1% 5.4% 2.2% 18.3% 2.4% (n=1488) (136) (81) (33) (272) (36)
Study 3 Herceptin 8.6% 7.0% 3.8% 22.4% 3.5% (n=1678) (144) (118) (64) (376) (59)
Observation 2.7% 2.0% 1.2% 11.9% 1.2% (n=1708) (46) (35) (20) (204) (21)
Study 4c TCH 8.5% 5.9% 3.3% 34.5% 6.3% (n=1056) (90) (62) (35) (364) (67)
AC TH 17% 13.3% 9.8% 44.3% 13.2% (n=1068) (182) (142) (105) (473) (141)
AC T 9.5% 6.6% 3.3% 34% 5.5% (n=1050) (100) (69) (35) (357) (58)
a For Studies 1, 2 and 3, events are counted from the beginning of Herceptin treatment. For Study 4, events are counted from the date of randomization.
b Studies 1 and 2 regimens: doxorubicin and cyclo-phosphamide followed by paclitaxel (AC T) or paclitaxel plus Herceptin (AC TH).
c Study 4 regimens: doxorubicin and cyclophosphamide followed by docetaxel (AC T) or docetaxel plus Herceptin (AC TH); docetaxel and carboplatin plus Herceptin (TCH).
Figure 1 Studies 1 and 2: Cumulative Incidence of Time to First LVEF Decline of 10 Percentage Points from Baseline and to Below 50% with Death as a Competing Risk Event
Time 0 is initiation of paclitaxel or Herceptin + paclitaxel therapy.
Figure 2 Study 3: Cumulative Incidence of Time to First LVEF Decline of 10 Percentage Points from Baseline and to Below 50% with Death as a Competing Risk Event
Time 0 is the date of randomization.
Figure 3 Study 4: Cumulative Incidence of Time to First LVEF Decline of 10 Percentage Points from Baseline and to Below 50% with Death as a Competing Risk Event
Time 0 is the date of randomization.
The incidence of treatment emergent congestive heart failure among patients in the metastatic breast cancer trials was classified for severity using the New York Heart Association classification system (I−IV, where IV is the most severe level of cardiac failure) (see Table 2). In the metastatic breast cancer trials the probability of cardiac dysfunction was highest in patients who received Herceptin concurrently with anthracyclines. In Study 7, 5.0% of patients in the Herceptin plus chemotherapy arm compared to 1.1% of patients in the chemotherapy alone arm had LVEF value below 50% with a
10% absolute decrease in LVEF from pretreatment values. Infusion Reactions During the first infusion with Herceptin, the symptoms most commonly reported were chills and fever, occurring in approximately 40% of patients in clinical trials. Symptoms were treated with acetaminophen, diphenhydramine, and meperidine (with or without reduction in the rate of Herceptin infusion); permanent discontinuation of Herceptin for infusional toxicity was required in <1% of patients. Other signs and/or symptoms may include nausea, vomiting, pain (in some cases at tumor sites), rigors, headache, dizziness, dyspnea, hypotension, elevated blood pressure, rash, and asthenia. Infusional toxicity occurred in 21% and 35% of patients, and was severe in 1.4% and 9% of patients, on second or subsequent Herceptin infusions administered as monotherapy or in combination with chemotherapy, respectively. In the post-marketing setting, severe infusion reactions, including hypersensitivity, anaphylaxis, and angioedema have been reported. Anemia In randomized controlled clinical trials, the overall incidence of anemia (30% vs. 21% [Study 5]), of selected NCI-CTC Grade 2-5 anemia (12.5% vs. 6.6% [Study 1]), and of anemia requiring transfusions (0.1% vs. 0 patients [Study 2]) were increased in patients receiving Herceptin and chemotherapy compared with those receiving chemotherapy alone. Following the administration of Herceptin as a single agent (Study 6), the incidence of NCI-CTC Grade 3 anemia was < 1%. In Study 7 (metastatic gastric cancer) on the Herceptin containing arm as compared to the chemotherapy alone arm the overall incidence of anemia was 28% compared 21% and of NCI CTC Grade 3/4 anemia was 12.2% compared to 10.3%. Neutropenia In randomized controlled clinical trials in the adjuvant setting, the incidence of selected NCI-CTC Grade 4−5 neutropenia (2% vs. 0.7% [Study 2]) and of selected Grade 2−5 neutropenia (7.1% vs. 4.5% [Study 1]) were increased in patients receiving Herceptin and chemotherapy compared with those receiving chemotherapy alone. In a randomized, controlled trial in patients with metastatic breast cancer, the incidences of NCI-CTC Grade 3/4 neutropenia (32% vs. 22%) and of febrile neutropenia (23% vs. 17%) were also increased in patients randomized to Herceptin in combination with myelosuppressive chemotherapy as compared to chemotherapy alone. In Study 7 (metastatic gastric cancer) on the Herceptin containing arm as compared to the chemotherapy alone arm, the incidence of NCI CTC Grade 3/4 neutropenia was 36.8% compared to 28.9%; febrile neutropenia 5.1% compared to 2.8%. Infection The overall incidences of infection (46% vs. 30% [Study 5]), of selected NCI-CTC Grade 2−5 infection/febrile neutropenia
(22% vs. 14% [Study 1]) and of selected Grade 3−5 infection/febrile neutropenia (3.3% vs. 1.4%) [Study 2]), were higher in patients receiving Herceptin and chemotherapy compared with those receiving chemotherapy alone. The most common site of infections in the adjuvant setting involved the upper respiratory tract, skin, and urinary tract. In Study 4, the overall incidence of infection was higher with the addition of Herceptin to AC-T but not to TCH [44% (AC-TH), 37% (TCH), 38% (AC-T)]. The incidences of NCI-CTC Grade 3−4 infection were similar [25% (AC-TH), 21% (TCH), 23% (AC-T)] across the three arms. In a randomized, controlled trial in treatment of metastatic breast cancer, the reported incidence of febrile neutropenia was higher (23% vs. 17%) in patients receiving Herceptin in combination with myelo suppressive chemo-therapy as compared to chemo therapy alone. Pulmonary Toxicity Adjuvant Breast Cancer Among women receiving adjuvant therapy for breast cancer, the incidence of selected NCI-CTC Grade 2−5 pulmonary toxicity (14% vs. 5% [Study 1]) and of selected NCI-CTC Grade 3−5 pulmonary toxicity and spontaneous reported Grade 2 dyspnea (3.4% vs. 1% [Study 2]) was higher in patients receiving Herceptin and chemotherapy compared with chemotherapy alone. The most common pulmonary toxicity was dyspnea (NCI-CTC Grade 2−5: 12% vs. 4% [Study 1]; NCI-CTC Grade 2−5: 2.5% vs. 0.1% [Study 2]). Pneumonitis/pulmonary infiltrates occurred in 0.7% of patients receiving Herceptin compared with 0.3% of those receiving chemotherapy alone. Fatal respiratory failure occurred in 3 patients receiving Herceptin, one as a component of multi-organ system failure, as compared to 1 patient receiving chemotherapy alone. In Study 3, there were 4 cases of interstitial pneumonitis in Herceptin-treated patients compared to none in the control arm. Metastatic Breast Cancer Among women receiving Herceptin for treatment of metastatic breast cancer, the incidence of pulmonary toxicity was also increased. Pulmonary adverse events have been reported in the post-marketing experience as part of the symptom complex of infusion reactions. Pulmonary events include bronchospasm, hypoxia, dyspnea, pulmonary infiltrates, pleural effusions, non-cardiogenic pulmonary edema, and acute respiratory distress syndrome. For a detailed description, see Warnings and Precautions. Thrombosis/Embolism In 4 randomized, controlled clinical trials, the incidence of thrombotic adverse events was higher in patients receiving Herceptin and chemotherapy compared to chemotherapy alone in three studies (3.0% vs. 1.3% [Study 1], 2.5% and 3.7% vs. 2.2% [Study 4] and 2.1% vs. 0% [Study 5]). Diarrhea Among women receiving adjuvant therapy for breast cancer, the incidence of NCI-CTC Grade 2−5 diarrhea (6.2% vs. 4.8% [Study 1]) and of NCI-CTC Grade 3−5 diarrhea (1.6% vs. 0% [Study 2]), and of Grade 1−4 diarrhea (7% vs. 1% [Study 3]) were higher in patients receiving Herceptin as compared to controls. In Study 4, the incidence of Grade 3−4 diarrhea was higher [5.7% AC-TH, 5.5% TCH vs. 3.0% AC-T] and of Grade 1−4 was higher [51% AC-TH, 63% TCH vs. 43% AC-T] among women receiving Herceptin. Of patients receiving Herceptin as a single agent for the treatment of metastatic breast cancer, 25% experienced diarrhea. An increased incidence of diarrhea was observed in patients receiving Herceptin in combination with chemotherapy for treatment of metastatic breast cancer. Renal Toxicity In Study 7 (metastatic gastric cancer) on the Herceptin-containing arm as compared to the chemotherapy alone arm the incidence of renal impairment was 18% compared to 14.5%. Severe (Grade 3/4) renal failure was 2.7% on the Herceptin-containing arm compared to 1.7% on the chemotherapy only arm. Treatment discontinuation for renal insufficiency/failure was 2% on the Herceptin-containing arm and 0.3% on the chemotherapy only arm. In the postmarketing setting, rare cases of nephrotic syndrome with pathologic evidence of glomerulopathy have been reported. The time to onset ranged from 4 months to approximately 18 months from initiation of Herceptin therapy. Pathologic findings included membranous glomerulonephritis, focal glomerulosclerosis, and fibrillary glomerulonephritis. Complications included volume overload and congestive heart failure. Immunogenicity As with all therapeutic proteins, there is a potential for immunogenicity. Among 903 women with metastatic breast cancer, human anti-human antibody (HAHA) to Herceptin was detected in one patient using an enzyme-linked immunosorbent assay (ELISA). This patient did not experience an allergic reaction. Samples for assessment of HAHA were not collected in studies of adjuvant breast cancer. The incidence of antibody formation is highly dependent on the sensitivity and the specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to Herceptin with the incidence of antibodies to other products may be misleading. Post-Marketing Experience The following adverse reactions have been identified during post approval use of Herceptin. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. • Infusion reaction [see Warnings and Precautions] • Oligohydramnios or oligohydramnios sequence, including pulmonary hypoplasia, skeletal abnormalities, and neonatal death [see Warnings and Precautions] • Glomerulopathy [see Adverse Reactions] DRUG INTERACTIONS In Study 5, the mean serum trough concentration of trastuzumab was consistently elevated approximately 1.5-fold, when administered in combination with paclitaxel as compared to trough concentrations of trastuzumab when administered in combination with an anthracycline and cyclophosphamide. In other pharmacokinetic studies, where Herceptin was administered in combination with paclitaxel, docetaxel or doxorubicin, Herceptin did not alter the plasma concentrations of these chemotherapeutic agents, or the metabolites that were analyzed. In a drug interaction substudy conducted in patients in Study 7, the pharmacokinetics of cisplatin,
capecitabine and their metabolites were not altered when administered in combination with Herceptin. USE IN SPECIFIC POPULATIONS Pregnancy: Category D [see Warnings and Precautions, Nonclinical Toxicology] Herceptin can cause fetal harm when administered to a pregnant woman. In post-marketing reports use of Herceptin during pregnancy resulted in cases of oligohydramnios and of oligohydramnios sequence, manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. These case reports described oligohydramnios in pregnant women who received Herceptin either alone or in combination with chemotherapy. In some case reports, amniotic fluid index increased after Herceptin was stopped. In one case, Herceptin therapy resumed after the amniotic fluid index improved, and oligohydramnios recurred. Monitor women exposed to Herceptin during pregnancy for oligohydramnios. If oligohydramnios occurs, perform fetal testing that is appropriate for gestational age and consistent with community standards of care. The efficacy of IV hydration in management of oligohydramnios due to Herceptin exposure is not known. Advise women of the potential hazard to the fetus resulting from Herceptin exposure during pregnancy. Encourage pregnant women with breast cancer who are using Herceptin to enroll in MotHER-the Herceptin Pregnancy Registry: phone 1-800-690-6720. [see Patient Counseling Information]. No teratogenic effects were observed in offspring from reproduction studies in cynomolgus monkeys at doses up to 25 times the recommended weekly human dose of 2 mg/kg trastuzumab. In mutant mice lacking HER2, embryos died in early gestation. Trastuzumab exposure was reported at delivery in offspring of cynomolgus monkeys treated during the early (Days 20-50 of gestation) or late (Days 120-150 of gestation) fetal development periods, at levels of 15 to 28% of the maternal blood levels. Nursing Mothers It is not known whether Herceptin is excreted in human milk, but human IgG is excreted in human milk. Published data suggest that breast milk antibodies do not enter the neonatal and infant circulation in substantial amounts. Trastuzumab was present in the breast milk of lactating cynomolgus monkeys given 12.5 times the recommended weekly human dose of 2 mg/kg of Herceptin. Infant monkeys with detectable serum levels of trastuzumab did not have any adverse effects on growth or development from birth to 3 months of age; however, trastuzumab levels in animal breast milk may not accurately reflect human breast milk levels. Because many drugs are secreted in human milk and because of the potential for serious adverse reactions in nursing infants from Herceptin, a decision should be made whether to discontinue nursing, or discontinue drug, taking into account the elimination half-life of trastuzumab and the importance of the drug to the mother. Pediatric Use The safety and effectiveness of Herceptin in pediatric patients has not been established. Geriatric Use Herceptin has been administered to 386 patients who were 65 years of age or over (253 in the adjuvant treatment and 133 in metastatic breast cancer treatment settings). The risk of cardiac dysfunction was increased in geriatric patients as compared to younger patients in both those receiving treatment for metastatic disease in Studies 5 and 6, or adjuvant therapy in Studies 1 and 2. Limitations in data collection and differences in study design of the 4 studies of Herceptin in adjuvant treatment of breast cancer preclude a determination of whether the toxicity profile of Herceptin in older patients is different from younger patients. The reported clinical experience is not adequate to determine whether the efficacy improvements (ORR, TTP, OS, DFS) of Herceptin treatment in older patients is different from that observed in patients <65 years of age for metastatic disease and adjuvant treatment. In Study 7 (metastatic gastric cancer), of the 294 patients treated with Herceptin 108 (37%) were 65 years of age or older, while 13 (4.4%) were 75 and over. No overall differences in safety or effectiveness were observed. OVERDOSAGE There is no experience with overdosage in human clinical trials. Single doses higher than 8 mg/kg have not been tested. PATIENT COUNSELING INFORMATION • Advise patients to contact a health care professional immediately for any of the following: new onset or worsening shortness of breath, cough, swelling of the ankles/legs, swelling of the face, palpitations, weight gain of more than 5 pounds in 24 hours, dizziness or loss of consciousness [see Boxed Warning Cardiomyopathy]. • Advise pregnant women and women of childbearing potential that Herceptin exposure can result in fetal harm [see Warnings and Precautions and Use in Specific Populations]. • Advise women of childbearing potential to use effective contraceptive methods during treatment and for a minimum of six months following Herceptin [see Warnings and Precautions]. • Advise nursing mothers treated with Herceptin to discontinue nursing or discontinue Herceptin, taking into account the importance of the drug to the mother [see Use in Specific Populations]. • Encourage women who are exposed to Herceptin during pregnancy to enroll in MotHER- the Herceptin Pregnancy Registry (1-800-690-6720) [see Warnings and Precautions and Use in Specific Populations].
HERCEPTIN® [trastuzumab]Manufactured by:Genentech, Inc.A Member of the Roche Group1 DNA WaySouth San Francisco, CA 94080-4990
Initial US Approval: September 1998Revision Date: October 29, 2010Herceptin® is a registered trademark of Genentech, Inc.HER0000111000©2010 Genentech, Inc.
TON_April2011_v7_TON 4/7/11 10:47 AM Page 5

EDITOR-IN-CHIEFBeth Faiman,RN, MSN, APRN,BC, AOCNCleveland Clinic TaussigCancer InstituteCleveland, OH
Elizabeth Bilotti,RN, MSN, APRN,BC, OCNJohn Theurer Cancer CenterHackensack UniversityMedical CenterHackensack, NJ
Catherine Bishop,DNP, NP, AOCNPVirginia Cancer CareLansdowne, VA
Deena DamskyDell, RN, MSN,AOCN, BCFox Chase Cancer CenterPhiladelphia, PA
Wendy DiSalvo,DNP, APRN, AOCNGenentechNew London, NH
DeniceEconomou, RN,MN, CNS, AOCNCity of Hope NationalMedical CenterDuarte, CA
ConstanceEngelking, RN,MS, CNS, OCNThe CHE ConsultingGroup, Inc.Mt. Kisco, NY
Amy Ford, RN,BSN, OCNInnovexDallas, TX
Sharon S. Gentry,RN, MSN, AOCNDerrick L. Davis ForsythRegional Cancer CenterWinston-Salem, NC
Cassandra J.Hammond, RN,MSN, CRNPAvid Education Partners,LLCSharpsburg, MD
Shannon Hazen,RN, BSN, OCNNovant HealthPresbyterian CancerCenterCharlotte, NC
Patricia IrouerHughes, RN, MSN,BSN, OCNPiedmount HealthcareRex, GA
Taline Khoukaz,NP, MSN, ACNP-CUniversity of SouthernCaliforniaNorris Cancer Center &HospitalLos Angeles, CA
Sandra E. Kurtin,RN, MS, AOCN,ANP-CArizona Cancer CenterTucson, AZ
Elizabeth Lima,PA-CCleveland Clinic TaussigCancer InstituteCleveland, OH
Ann McNeill,MSN, RN, NP-C,OCNThe Cancer Center atHackensack University Medical CenterHackensack, NJ
Kena C. Miller,RN, MSN, FNPRoswell Park CancerInstituteBuffalo, NY
Patricia Molinelli,MS, RN, APN-C,AOCNSSomerset Medical CenterSomerville, NJ
Dolores “Jeff”Nordquist, RN, MS,CS, FNPMayo ClinicRochester, MN
MelindaOberleitner, RN,DNS, APRN, CNSCollege of Nursing andAllied Health ProfessionsUniversity of LouisianaLafayette, LA
Gary Shelton,MSN, ARNP,AOCNNYU Cancer InstituteNew York, NY
Lori Stover, RN,BSNWestern PennsylvaniaCancer Institute Pittsburgh, PA
Pamela HallquistViale, RN, MS,CS, ANP, AOCNSaratoga, CA
Connie Visovsky,RN, PhD, APRNUniversity of NebraskaCollege of NursingOmaha, NE
Rita Wickham,OCN, PhD, RNRush University College ofNursingRush-Presbyterian-St. Luke’s Medical CenterChicago, IL
Karla Wilson, RN,MSN, FNP-C, CPONCity of Hope NationalMedical CenterDuarte, CA
PharmacyJohn F. Aforismo,BSc Pharm, RPh,FASCPR. J. Health SystemsInternational, LLCWethersfield, CT
NutritionKaren Connelly,RD, CSOSomerset Medical CenterSomerville, NJ
Patient AdvocatePeg FordCoronado, CA
Social WorkCarolyn Messner,DSW, MSW, LCSW-R, BCDCancerCareNew York, NY
Managed Care andPharmaceuticalManagementBurt Zweigenhaft,BSBioPharma Partners LLCNew York, NY
Isabell Castellano, RNBristol-Myers Squibb Children’s HospitalRobert Wood Johnson University HospitalNew Brunswick, NJ
Jeanne Westphal, RNMeeker County Memorial HospitalLitchfield, MN
6 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Editorial Board
TON_April2011_v7_TON 4/7/11 10:47 AM Page 6

The challenges of multiple myeloma need new approaches
In multiple myeloma, median survival from the time of diagnosis has
been signicantly longer in the current decade than in previous years—
3.7 years vs 2.5 years.1 However, patients still face signicant challenges.
• Almost all patients eventually relapse2
• Patients may become refractory to multiple treatment options
Pursuing new treatment advances
Onyx Pharmaceuticals is pursuing potential new options for the treatment
of relapsed and refractory multiple myeloma, with the ultimate goal of
extending patients’ lives.
References: 1. Kumar SK, Rajkumar SV, Dispenzieri A, et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood. 2008;111:2516-2520. 2. Schwartz RN, Vozniak M. Current and emerging treatments for multiple myeloma. J Manag Care Pharm. 2008;14(suppl S):S12-S18.©2011 Onyx Pharmaceuticals, Inc., South San Francisco, CA 1210-CARF-051-R1 December 2010
In multiple myeloma
4:31 PM
TON_April2011_v7_TON 4/7/11 10:47 AM Page 7

PUBLISHING STAFFPublisherPhilip [email protected]
Editorial DirectorChristin [email protected]
Associate EditorDawn [email protected]
Quality Control DirectorBarbara Marino
Director, Client ServicesJohn W. [email protected]
Production ManagerStephanie Laudien
Business ManagerBlanche [email protected]
Executive AdministratorAndrea Boylston
Circulation [email protected]
Editorial Contact:Telephone: 732-992-1891 Fax: 732-656-7938
The Oncology Nurse®-APN/PA, ISSN 1944-9798 (print);ISSN 1944-9801 (online) is published 8 times a year byGreen Hill Healthcare Communications, LLC, 241Forsgate Drive, Suite 205C, Monroe Twp, NJ 08831.Telephone: 732.656.7935. Fax: 732.656.7938. Copyright©2011 by Green Hill Health care Com munications,LLC. All rights reserved. The Oncology Nurse®-APN/PAlogo is a registered trademark of Green Hill HealthcareCommunications, LLC. No part of this publication maybe reproduced or transmitted in any form or by anymeans now or hereafter known, electronic or mechan-ical, including photocopy, recording, or any informa-tional storage and retrieval system, without writtenpermission from the Publisher. Printed in the UnitedStates of America.
EDITORIAL CORRESPONDENCE should beaddressed to EDITORIAL DIRECTOR, The OncologyNurse®-APN/PA, 241 Forsgate Drive, Suite 205C,Monroe Twp, NJ 08831. E-mail: [email protected]. YEARLY SUBSCRIPTION RATES: UnitedStates and possessions: individuals, $105.00; institutions,$135.00; single issues, $17.00. Orders will be billed atindividual rate until proof of status is confirmed. Pricesare subject to change without notice. Correspondenceregarding permission to reprint all or part of any articlepublished in this journal should be addressed toREPRINT PERMISSIONS DEPARTMENT, GreenHill Healthcare Communications, LLC, 241 ForsgateDrive, Suite 205C, Monroe Twp, NJ 08831. The ideasand opinions expressed in The Oncology Nurse®-APN/PAdo not necessarily reflect those of the Editorial Board, theEditorial Director, or the Publisher. Publication of anadvertisement or other product mention in The OncologyNurse®-APN/PA should not be construed as an endorse-ment of the product or the manufacturer’s claims.Readers are encouraged to contact the manufacturer withquestions about the features or limitations of the productsmentioned. Neither the Editorial Board nor the Publisherassumes any responsibility for any injury and/or damageto persons or property arising out of or related to any useof the material contained in this periodical. The reader isadvised to check the appropriate medical literature andthe product information currently provided by the manu-facturer of each drug to be administered to verify thedosage, the method and duration of administration, orcontraindications. It is the responsibility of the treatingphysician or other healthcare professional, relying onindependent experience and knowledge of the patient, todetermine drug dosages and the best treatment for thepatient. Every effort has been made to check generic andtrade names, and to verify dosages. The ultimate respon-sibility, however, lies with the prescribing physician.Please convey any errors to the Editorial Director.
BPA Worldwide membership applied for April 2011.
Green Hill Healthcare Communications LLCGreen Hill Healthcare Communications, LLCHGYour Innovative Partners in Medical Media™
™
241 Forsgate Drive, Suite 205CMonroe Twp, NJ 08831
8 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
In This Issue
In Advanced Renal Cell Carcinoma...
IndicationVOTRIENT is indicated for the treatment of patients with advanced renal cell carcinoma (RCC).
Important Safety Information
WARNING: HEPATOTOXICITYSevere and fatal hepatotoxicity has been observed in clinical studies. Monitor hepatic function and interrupt, reduce, or discontinue dosing as recommended. See “Warnings and Precautions,”Section 5.1, in complete Prescribing Information.
Hepatic Effects: Patients with pre-existing hepatic impairment should use VOTRIENT with caution. Treatment with VOTRIENT is not recommended in patients with severe hepatic impairment. Increases in serum transaminase levels (ALT, AST) and bilirubin were observed. Severe and fatal hepatotoxicity has occurred. Transaminase elevations occur early in the course of treatment (92.5% of all transaminase elevations of any grade occurred in the fi rst 18 weeks). Before the initiation of treatment and regularly during treatment, monitor hepatic function and interrupt, reduce, or discontinue dosing as recommended.QT Prolongation and Torsades de Pointes: Prolonged QT intervals and arrhythmias, including torsades de pointes, have been observed with VOTRIENT. Use with caution in patients at higher risk of developing QT interval prolongation, in patients taking antiarrhythmics or other medications that may prolong QT interval,
and those with relevant pre-existing cardiac disease. Baseline and periodic monitoring of electrocardiograms and maintenance of electrolytes within the normal range should be performed. Hemorrhagic Events: Fatal hemorrhagic events have been reported (all grades [16%] and Grades 3 to 5 [2%]). VOTRIENT has not been studied in patients who have a history of hemoptysis, cerebral, or clinically signifi cant gastrointestinal hemorrhage in the past 6 months and should not be used in those patients. Arterial Thrombotic Events: Arterial thrombotic events have been observed and can be fatal. In clinical RCC studies of VOTRIENT, myocardial infarction, angina, ischemic stroke, and transient ischemic attack (all grades [3%] and Grades 3 to 5 [2%]) were observed. Use with caution in patients who are at increased risk for these events. Gastrointestinal Perforation and Fistula: Gastrointestinal perforation or fi stula has occurred. Fatal perforation events have occurred. Use with caution in patients at risk for gastrointestinal perforation or fi stula. Monitor for symptoms of gastrointestinal perforation or fi stula.Hypertension: Hypertension has been observed. Hypertension was observed in 47% of patients with RCC treated with VOTRIENT. Hypertension occurs early in the course of treatment (88% occurred in the fi rst 18 weeks). Blood pressure should be well-controlled prior to initiating VOTRIENT. Monitor for hypertension and treat as needed. If hypertension persists despite antihypertensive therapy, the dose of VOTRIENT may be reduced or discontinued as appropriate.
11:16 AM
13 FEATUREDrug Shortages: A Growing Crisis inOncology
18 CONFERENCE NEWSHighlights from the 2011 Gastrointestinal and Genitourinary Cancers Symposia
32 COMPLIMENTARY CEFollow-up Management of HodgkinLymphoma Survivors
42 THE WHOLE PATIENT• Considerations for CancerTreatment–Induced Diarrhea
• Managing Geriatric Patients
• Balloon Kyphoplasty Reduces VertebralCompression Pain
TON_April2011_v7_TON 4/7/11 1:18 PM Page 8

March/april 2011 I VOl 4, NO 2 9www.TheOncologyNurse.com
In This Issue
Wound Healing: VOTRIENT may impair wound healing. Temporary interruption of therapy with VOTRIENT is recommended in patients undergoing surgical procedures. VOTRIENT should be discontinued in patients with wound dehiscence. Hypothyroidism: Hypothyroidism was reported as an adverse reaction in 26/586 (4%). Monitoring of thyroid function tests is recommended. Proteinuria: Monitor urine protein. Proteinuria was reported in 44/586 (8%) (Grade 3, 5/586 [<1%] and Grade 4, 1/586 [<1%]). Baseline and periodic urinalysis during treatment is recommended. Discontinue for Grade 4 proteinuria.Pregnancy Category D: VOTRIENT can cause fetal harm when administered to a pregnant woman. Women of childbearing potential should be advised of the potential hazard to the fetus and to avoidbecoming pregnant while taking VOTRIENT.Drug Interactions: CYP3A4 Inhibitors (eg, ketoconazole, ritonavir, clarithromycin): Avoid use of strong inhibitors. Consider dose reduction of VOTRIENT when administered with strong CYP3A4 inhibitors. CYP3A4 Inducers (such as rifampin): Consider an alternate concomitant medication with no or minimal enzyme induction potential or avoid VOTRIENT.CYP Substrates: Concomitant use of VOTRIENT with agents with narrow therapeutic windows that are metabolized by CYP3A4, CYP2D6, or CYP2C8 is not recommended.
Adverse Reactions: The most common adverse reactions (>20%) for VOTRIENT versus placebo were diarrhea (52% vs. 9%), hypertension (40% vs. 10%), hair color changes (depigmentation) (38% vs. 3%), nausea (26% vs. 9%), anorexia (22% vs. 10%), and vomiting (21% vs. 8%).Laboratory abnormalities occurring in >10% of patients and more commonly ( 5%) in the VOTRIENT arm versus placebo included increases in ALT (53% vs. 22%), AST (53% vs. 19%), glucose (41% vs. 33%), and total bilirubin (36% vs. 10%); decreases in phosphorus (34% vs. 11%), sodium (31% vs. 24%), magnesium (26% vs. 14%), and glucose (17% vs. 3%); leukopenia (37% vs. 6%), neutropenia (34% vs. 6%), thrombocytopenia (32% vs. 5%), and lymphocytopenia (31% vs. 24%).VOTRIENT has been associated with cardiac dysfunction (such as a decrease in ejection fraction and congestive heart failure) in patients with various cancer types, including RCC. In the overall safety population for RCC (N=586), cardiac dysfunction was observed in 4/586 patients (<1%).
Please see Brief Summary of Prescribing Information on adjacent pages.
www.VOTRIENT.com
NCCN Guidelines Category 1 recommendation4
• First-line therapy for relapsed or Stage IV unresectable RCC of predominant clear cell histology
Proven safety profi le1,2
• Most common adverse events observed with VOTRIENT (>20%) were diarrhea, hypertension, hair color changes(depigmentation), nausea, anorexia, and vomiting
— Grade 3/4 fatigue occurred in 2% of patients; all grades, 19%— Grade 3/4 asthenia occurred in 3% of patients; all grades, 14%
Most common laboratory abnormalities were ALT and AST increases1
• Grade 3 ALT increases occurred in 10% of patients; grade 4, 2%
• In clinical trials, 92.5% of all transaminase elevations of any grade occurred in the fi rst 18 weeks of treatment with VOTRIENT
• Monitor serum liver tests before initiation of treatment with VOTRIENT and at least once every 4 weeks for at least the fi rst4 months of treatment or as clinically indicated. Periodic monitoring should then continue after this time period
Once-daily oral dosing1
• The recommended dosage of VOTRIENT is 800 mg once daily without food (at least 1 hour before or 2 hours after a meal)
• Dose modifi cations, interruptions, and discontinuations may be required in patients with hepatic impairment, drug interactions, and following adverse events
• Forty-two percent of patients on VOTRIENT required a dose interruption; 36% of patients on VOTRIENT were dose-reduced
VOTRIENT is a multitargeted tyrosine kinase inhibitor that is indicated for the treatment of patients with advanced RCC.
Move Forward With VOTRIENTIn a phase 3, randomized, double-blind, placebo-controlled trial, VOTRIENT provided signifi cant improvement in progression-free survival (PFS) in both treatment-naïve and cytokine-pretreated patients with advanced RCC1,2
References: 1. VOTRIENT Prescribing Information. Research Triangle Park, NC: GlaxoSmith-Kline; 2010. 2. Sternberg CN, et al. J Clin Oncol. 2010;28(6):1061–1068. 3. Data on fi le, GlaxoSmithKline. 4. Referenced with permission from ©National Comprehensive Cancer Network, Inc 2010. All Rights Reserved. NCCN Guidelines™: Kidney Cancer, V.1.2011. NCCN.org Accessed January 12, 2011. NCCN® and NCCN GUIDELINES™ are trademarks owned by the National Comprehensive Cancer Network, Inc.
Cytokine-pretreated patients
7.4 months(95% CI, 5.6-12.9)
median PFS with VOTRIENT (n=135) vs 4.2 months (95% CI, 2.8-5.6) with placebo (n=67) (P<0.001)2,3
Treatment-naïve patients
11.1 months (95% CI, 7.4-14.8)
median PFS with VOTRIENT (n=155) vs 2.8 months (95% CI, 1.9-5.6) with placebo (n=78) (P<0.001)2,3
All patients9.2 months
(95% CI, 7.4-12.9) overall median PFS with VOTRIENT (n=290)
vs 4.2 months (95% CI, 2.8-4.2) with placebo (n=145) (P<0.001)2,3
V 11:16 AM
48 NEWS IN REVIEW• Voluntary Recall of Irinotecan• Tamoxifen Protective 10 Years After Treatment• Medicare Plans to Cover Provenge
58 NAVIGATION & SURVIVORSHIP• Azoospermic Survivors Not Necessarily Sterile• Navigators’ and Patients’ Perspectives on the NavigationExperience
60 NURSING LIFE• Nursing By the Numbers
• Do you Tweet?
• Can Alternative Medicine Prevent Burnout?
62 MEETINGS
TON_April2011_v7_TON 4/7/11 1:19 PM Page 9

BRIEF SUMMARYVOTRIENT™ (pazopanib) tabletsThe following is a brief summary only; see full prescribing information for complete product information.
WARNING: HEPATOTOXICITYSevere and fatal hepatotoxicity has been observed in clinical studies. Monitor hepatic function and interrupt, reduce, or discontinue dosing as recommended. [See Warnings and Precautions (5.1).]
1 INDICATIONS AND USAGEVOTRIENT™ is indicated for the treatment of patients with advanced renal cell carcinoma (RCC).
2 DOSAGE AND ADMINISTRATION2.1 Recommended Dosing: The recommended dose of VOTRIENT is 800 mg orally once daily without food (at least 1 hour before or 2 hours after a meal) [see Clinical Pharmacology (12.3) of full prescribing information]. The dose of VOTRIENT should not exceed 800 mg. Do not crush tablets due to the potential for increased rate of absorption which may affect systemic exposure. [See Clinical Pharmacology (12.3) of full prescribing information.] If a dose is missed, it should not be taken if it is less than 12 hours until the next dose. 2.2 Dose Modification Guidelines: Initial dose reduction should be 400 mg, and additional dose decrease or increase should be in 200 mg steps based on individual tolerability. The dose of VOTRIENT should not exceed 800 mg. Hepatic Impairment: The dosage of VOTRIENT in patients with moderate hepatic impairment should be reduced to 200 mg per day. There are no data in patients with severe hepatic impairment; therefore, use of VOTRIENT is not recommended in these patients. [See Use in Specific Populations (8.6).] Concomitant Strong CYP3A4 Inhibitors: The concomitant use of strong CYP3A4 inhibitors (e.g., ketoconazole, ritonavir, clarithromycin) may increase pazopanib concentrations and should be avoided. If coadministration of a strong CYP3A4 inhibitor is warranted, reduce the dose of VOTRIENT to 400 mg. Further dose reductions may be needed if adverse effects occur during therapy. This dose is predicted to adjust the pazopanib AUC to the range observed without inhibitors. However, there are no clinical data with this dose adjustment in patients receiving strong CYP3A4 inhibitors. [See Drug Interactions (7.1).] Concomitant Strong CYP3A4 Inducer: The concomitant use of strong CYP3A4 inducers (e.g., rifampin) may decrease pazopanib concentrations and should be avoided. VOTRIENT should not be used in patients who can not avoid chronic use of strong CYP3A4 inducers. [See Drug Interactions (7.1).]
4 CONTRAINDICATIONSNone.
5 WARNINGS AND PRECAUTIONS5.1 Hepatic Effects: In clinical trials with VOTRIENT, hepatotoxicity, manifested as increases in serum transaminases (ALT, AST) and bilirubin, was observed [see Adverse Reactions (6.1)]. This hepatotoxicity can be severe and fatal. Transaminase elevations occur early in the course of treatment (92.5% of all transaminase elevations of any grade occurred in the first 18 weeks). Across all monotherapy studies with VOTRIENT, ALT >3 X upper limit of normal (ULN) was reported in 138/977 (14%) and ALT >8 X ULN was reported in 40/977 (4%) of patients who received VOTRIENT. Concurrent elevations in ALT >3 X ULN and bilirubin >2 X ULN regardless of alkaline phosphatase levels were detected in 13/977 (1%) of patients. Four of the 13 patients had no other explanation for these elevations. Two of 977 (0.2%) patients died with disease progression and hepatic failure. Monitor serum liver tests before initiation of treatment with VOTRIENT and at least once every 4 weeks for at least the first 4 months of treatment or as clinically indicated. Periodic monitoring should then continue after this time period. Patients with isolated ALT elevations between 3 X ULN and 8 X ULN may be continued on VOTRIENT with weekly monitoring of liver function until ALT return to Grade 1 or baseline. Patients with isolated ALT elevations of >8 X ULN should have VOTRIENT interrupted until they return to Grade 1 or baseline. If the potential benefit for reinitiating treatment with VOTRIENT is considered to outweigh the risk for hepatotoxicity, then reintroduce VOTRIENT at a reduced dose of no more than 400 mg once daily and measure serum liver tests weekly for 8 weeks [see Dosage and Administration (2.2)]. Following reintroduction of VOTRIENT, if ALT elevations >3 X ULN recur, then VOTRIENT should be permanently discontinued. If ALT elevations >3 X ULN occur concurrently with bilirubin elevations >2 X ULN, VOTRIENT should be permanently discontinued. Patients should be monitored until resolution. VOTRIENT is a UGT1A1 inhibitor. Mild, indirect (unconjugated) hyperbilirubinemia may occur in patients with Gilbert’s syndrome [see Clinical Pharmacology (12.5) of full prescribing information]. Patients with only a mild indirect hyperbilirubinemia, known Gilbert’s syndrome, and elevation in ALT >3 X ULN should be managed as per the recommendations outlined for isolated ALT elevations. The safety of VOTRIENT in patients with pre-existing severe hepatic impairment, defined as total bilirubin >3 X ULN with any level of ALT, is unknown. Treatment with VOTRIENT is not recommended in patients with severe hepatic impairment. [See Dosage and Administration (2.2) and Use in Specific Populations (8.6).]
5.2 QT Prolongation and Torsades de Pointes: In clinical RCC studies of VOTRIENT, QT prolongation (≥500 msec) was identified on routine electrocardiogram monitoring in 11/558 (<2%) of patients. Torsades de pointes occurred in 2/977 (<1%) of patients who received VOTRIENT in the monotherapy studies. In the randomized clinical trial, 3 of the 290 patients receiving VOTRIENT had post-baseline values between 500 to 549 msec. None of the 145 patients receiving placebo had post-baseline QTc values ≥500 msec. VOTRIENT should be used with caution in patients with a history of QT interval prolongation, in patients taking antiarrhythmics or other medications that may prolong QT interval, and those with relevant pre-existing cardiac disease. When using VOTRIENT, baseline and periodic monitoring of electrocardiograms and maintenance of electrolytes (e.g., calcium, magnesium, potassium) within the normal range should be performed. 5.3 Hemorrhagic Events: In clinical RCC studies of VOTRIENT, hemorrhagic events have been reported [all Grades (16%) and Grades 3 to 5 (2%)]. Fatal hemorrhage has occurred in 5/586 (0.9%) [see Adverse Reactions (6.1)]. VOTRIENT has not been studied in patients who have a history of hemoptysis, cerebral, or clinically significant gastrointestinal hemorrhage in the past 6 months and should not be used in those patients. 5.4 Arterial Thrombotic Events: In clinical RCC studies of VOTRIENT, myocardial infarction, angina, ischemic stroke, and transient ischemic attack [all Grades (3%) and Grades 3 to 5 (2%)] were observed. Fatal events have been observed in 2/586 (0.3%). In the randomized study, these events were observed more frequently with VOTRIENT compared to placebo [see Adverse Reactions (6.1)]. VOTRIENT should be used with caution in patients who are at increased risk for these events or who have had a history of these events. VOTRIENT has not been studied in patients who have had an event within the previous 6 months and should not be used in those patients. 5.5 Gastrointestinal Perforation and Fistula: In clinical RCC studies of VOTRIENT, gastrointestinal perforation or fistula has been reported in 5 patients (0.9%). Fatal perforation events have occurred in 2/586 (0.3%). Monitor for symptoms of gastrointestinal perforation or fistula. 5.6 Hypertension: Blood pressure should be well-controlled prior to initiating VOTRIENT. Patients should be monitored for hypertension and treated as needed with anti-hypertensive therapy. Hypertension (systolic blood pressure ≥150 or diastolic blood pressure ≥100 mm Hg) was observed in 47% of patients with RCC treated with VOTRIENT. Hypertension occurs early in the course of treatment (88% occurred in the first 18 weeks). [See Adverse Reactions (6.1).] In the case of persistent hypertension despite anti-hypertensive therapy, the dose of VOTRIENT may be reduced [see Dosage and Administration (2.2)]. VOTRIENT should be discontinued if hypertension is severe and persistent despite anti-hypertensive therapy and dose reduction of VOTRIENT. 5.7 Wound Healing: No formal studies on the effect of VOTRIENT on wound healing have been conducted. Since vascular endothelial growth factor receptor (VEGFR) inhibitors such as pazopanib may impair wound healing, treatment with VOTRIENT should be stopped at least 7 days prior to scheduled surgery. The decision to resume VOTRIENT after surgery should be based on clinical judgment of adequate wound healing. VOTRIENT should be discontinued in patients with wound dehiscence. 5.8 Hypothyroidism: In clinical RCC studies of VOTRIENT, hypothyroidism reported as an adverse reaction in 26/586 (4%) [see Adverse Reactions (6.1)]. Proactive monitoring of thyroid function tests is recommended. 5.9 Proteinuria: In clinical RCC studies with VOTRIENT, proteinuria has been reported in 44/586 (8%) [Grade 3, 5/586 (<1%) and Grade 4, 1/586 (<1%)] [see Adverse Reactions (6.1)]. Baseline and periodic urinalysis during treatment is recommended. VOTRIENT should be discontinued if the patient develops Grade 4 proteinuria. 5.10 Pregnancy: VOTRIENT can cause fetal harm when administered to a pregnant woman. Based on its mechanism of action, VOTRIENT is expected to result in adverse reproductive effects. In pre-clinical studies in rats and rabbits, pazopanib was teratogenic, embryotoxic, fetotoxic, and abortifacient. There are no adequate and well-controlled studies of VOTRIENT in pregnant women. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant while taking VOTRIENT. [See Use in Specific Populations (8.1).]
6 ADVERSE REACTIONS6.1 Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The safety of VOTRIENT has been evaluated in 977 patients in the monotherapy studies which included 586 patients with RCC. With a median duration of treatment of 7.4 months (range 0.1 to 27.6), the most commonly observed adverse reactions (≥20%) in the 586 patients were diarrhea, hypertension, hair color change, nausea, fatigue, anorexia, and vomiting. The data described below reflect the safety profile of VOTRIENT in 290 RCC patients who participated in a randomized, double-blind, placebo-controlled study [see Clinical Studies (14) of full prescribing information]. The median duration of treatment was 7.4 months (range 0 to 23) for patients who received VOTRIENT and 3.8 months (range 0 to 22) for the placebo arm. Forty-two percent (42%) of patients on VOTRIENT required a dose interruption. Thirty-six percent (36%) of patients on VOTRIENT were dose reduced.
11:24 AM10 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
TON Notes
You can find them at www.TheOncologyNurse.com,by following the link to Continuing Education (CE).Topics range from supportive care issues, such as pre-
venting neuropathy and thromboembolic disease; to treat-ment concerns, like KRAS mutations and colorectal cancer;to practice matters, including bar coding as a strategy to pre-vent medication errors.
Additional CE is available at our preferred provider part-ner, Center of Excellence Media, LLC. At www.coexm.com,you will find a broad range of CE opportunities, on topics likemultiple myeloma and metastatic breast cancer.
If you have a CE topic you would like The Oncology Nurse-APN/PA to cover, forward your suggestion to us at [email protected] with CE in the subject line. �
Need More CE Credits?
TON_April2011_v7_TON 4/7/11 12:04 PM Page 10

Due to the enthusiastic response our OncologyNurse Excellence Award campaign hasreceived, we have decided to extend voting
until April 30. We will announce the winner in theJune issue of The Oncology Nurse-APN/PA. If youhave not voted already, we encourage you to visit theWebsite at the URL above and tell us whether youwould like Lisa K. Rioux, RN, BSN, OCN; Martha
Polovich, PhD, RN, AOCN; Janet C. Stocker, RN,MS, NP-C, AOCNS, or Patricia Shearburn, RN,MSN, AOCN, to receive this award.
If you no longer have the February issue availableto read up on the nominees, you will find all theirprofiles at www.TheOncologyNurse.com/award.There are only a few more weeks left to make yourselection, so don’t forget! �
Table 1. Adverse Reactions Occurring in ≥10% of Patients who Received VOTRIENT
VOTRIENT Placebo
(N = 290) (N = 145)
Adverse Reactions
All Gradesa
%Grade 3
%Grade 4
%
All Gradesa
%Grade 3
%Grade 4
%Diarrhea 52 3 <1 9 <1 0Hypertension 40 4 0 10 <1 0Hair color changes 38 <1 0 3 0 0Nausea 26 <1 0 9 0 0Anorexia 22 2 0 10 <1 0Vomiting 21 2 <1 8 2 0Fatigue 19 2 0 8 1 1Asthenia 14 3 0 8 0 0Abdominal pain 11 2 0 1 0 0Headache 10 0 0 5 0 0
a National Cancer Institute Common Terminology Criteria for Adverse Events, version 3.
Other adverse reactions observed more commonly in patients treated with VOTRIENT than placebo and that occurred in <10% (any grade) were alopecia (8% versus <1%), chest pain (5% versus 1%), dysgeusia (altered taste) (8% versus <1%), dyspepsia (5% versus <1%), facial edema (1% versus 0%), palmar-plantar erythrodysesthesia (hand-foot syndrome) (6% versus <1%), proteinuria (9% versus 0%), rash (8% versus 3%), skin depigmentation (3% versus 0%), and weight decreased (9% versus 3%).
Table 2. Selected Laboratory Abnormalities Occurring in >10% of Patients who Received VOTRIENT and More Commonly (≥5%) in Patients who Received VOTRIENT Versus Placebo
VOTRIENT(N = 290)
Placebo(N = 145)
Parameters
All Gradesa
%Grade 3
%Grade 4
%
All Gradesa
%Grade 3
%Grade 4
% Hematologic
Leukopenia 37 0 0 6 0 0Neutropenia 34 1 <1 6 0 0Thrombocytopenia 32 <1 <1 5 0 <1Lymphocytopenia 31 4 <1 24 1 0
ChemistryALT increased 53 10 2 22 1 0AST increased 53 7 <1 19 <1 0Glucose increased 41 <1 0 33 1 0
Total bilirubin increased 36 3 <1 10 1 <1
Phosphorus decreased 34 4 0 11 0 0
Sodium decreased 31 4 1 24 4 0
Magnesium decreased 26 <1 1 14 0 0
Glucose decreased 17 0 <1 3 0 0
a National Cancer Institute Common Terminology Criteria for Adverse Events, version 3.
Hepatic Toxicity: In a controlled clinical study with VOTRIENT for the treatment of RCC, ALT >3 X ULN was reported in 18% and 3% of the VOTRIENT and placebo groups, respectively. ALT >10 X ULN was reported in 4% of patients who received VOTRIENT and in <1% of patients who received placebo. Concurrent elevation in ALT >3 X ULN and bilirubin >2 X ULN in the absence of significant alkaline phosphatase >3 X ULN occurred in 5/290 (2%) of patients on VOTRIENT and 2/145 (1%) on placebo. [See Dosage and Administration (2.2) and Warnings and Precautions (5.1).] Hypertension: In a controlled clinical study with VOTRIENT for the treatment of RCC, 115/290 patients (40%) receiving VOTRIENT compared with 15/145 patients (10%) on placebo experienced hypertension. Grade 3 hypertension was reported in 13/290 patients (4%) receiving VOTRIENT compared with 1/145 patients (<1%) on placebo. The majority of cases of hypertension
were manageable with anti-hypertensive agents or dose reductions with 2/290 patients (<1%) permanently discontinuing treatment with VOTRIENT because of hypertension. In the overall safety population for RCC (N = 586), one patient had hypertensive crisis on VOTRIENT. [See Warnings and Precautions (5.2).] QT Prolongation and Torsades de Pointes: In a controlled clinical study with VOTRIENT, QT prolongation (≥500 msec) was identified on routine electrocardiogram monitoring in 3/290 (1%) of patients treated with VOTRIENT compared with no patients on placebo. Torsades de pointes was reported in 2/586 (<1%) patients treated with VOTRIENT in the RCC studies. [See Warnings and Precautions (5.3).] Arterial Thrombotic Events: In a controlled clinical study with VOTRIENT, the incidences of arterial thrombotic events such as myocardial infarction/ischemia [5/290 (2%)], cerebral vascular accident [1/290 (<1%)], and transient ischemic attack [4/290 (1%)] were higher in patients treated with VOTRIENT compared to the placebo arm (0/145 for each event). [See Warnings and Precautions (5.4).] Hemorrhagic Events: In a controlled clinical study with VOTRIENT, 37/290 patients (13%) treated with VOTRIENT and 7/145 patients (5%) on placebo experienced at least 1 hemorrhagic event. The most common hemorrhagic events in the patients treated with VOTRIENT were hematuria (4%), epistaxis (2%), hemoptysis (2%), and rectal hemorrhage (1%). Nine (9/37) patients treated with VOTRIENT who had hemorrhagic events experienced serious events including pulmonary, gastrointestinal, and genitourinary hemorrhage. Four (4/290) (1%) patients treated with VOTRIENT died from hemorrhage compared with no (0/145) (0%) patients on placebo. [See Warnings and Precautions (5.5).] In the overall safety population in RCC (N = 586), cerebral/intracranial hemorrhage was observed in 2/586 (<1%) patients treated with VOTRIENT. Hypothyroidism: In a controlled clinical study with VOTRIENT, more patients had a shift from thyroid stimulating hormone (TSH) within the normal range at baseline to above the normal range at any post-baseline visit in VOTRIENT compared with the placebo arm (27% compared with 5%, respectively). Hypothyroidism was reported as an adverse reaction in 19 patients (7%) treated with VOTRIENT and no patients (0%) in the placebo arm. [See Warnings and Precautions (5.7).] Diarrhea: Diarrhea occurred frequently and was predominantly mild to moderate in severity. Patients should be advised how to manage mild diarrhea and to notify their healthcare provider if moderate to severe diarrhea occurs so appropriate management can be implemented to minimize its impact. Proteinuria: In the controlled clinical study with VOTRIENT, proteinuria has been reported as an adverse reaction in 27 patients (9%) treated with VOTRIENT. In 2 patients, proteinuria led to discontinuation of treatment with VOTRIENT.Lipase Elevations: In a single-arm clinical study, increases in lipase values were observed for 48/181 patients (27%). Elevations in lipase as an adverse reaction were reported for 10 patients (4%) and were Grade 3 for 6 patients and Grade 4 for 1 patient. In clinical RCC studies of VOTRIENT, clinical pancreatitis was observed in 4/586 patients (<1%). Cardiac Dysfunction: Pazopanib has been associated with cardiac dysfunction (such as a decrease in ejection fraction and congestive heart failure) in patients with various cancer types, including RCC. In the overall safety population for RCC (N = 586), cardiac dysfunction was observed in 4/586 patients (<1%).
7 DRUG INTERACTIONS7.1 Drugs That Inhibit or Induce Cytochrome P450 3A4 Enzymes: In vitro studies suggested that the oxidative metabolism of pazopanib in human liver microsomes is mediated primarily by CYP3A4, with minor contributions from CYP1A2 and CYP2C8. Therefore, inhibitors and inducers of CYP3A4 may alter the metabolism of pazopanib. CYP3A4 Inhibitors: Coadministration of pazopanib with strong inhibitors of CYP3A4 (e.g., ketoconazole, ritonavir, clarithromycin) may increase pazopanib concentrations. A dose reduction for VOTRIENT should be considered when it must be coadministered with strong CYP3A4 inhibitors [see Dosage and Administration (2.2)]. Grapefruit juice should be avoided as it inhibits CYP3A4 activity and may also increase plasma concentrations of pazopanib. CYP3A4 Inducers: CYP3A4 inducers such as rifampin may decrease plasma pazopanib concentrations. VOTRIENT should not be used if chronic use of strong CYP3A4 inducers can not be avoided [see Dosage and Administration (2.2)]. 7.2 Effects of Pazopanib on CYP Substrates: Results from drug-drug interaction studies conducted in cancer patients suggest that pazopanib is a weak inhibitor of CYP3A4, CYP2C8, and CYP2D6 in vivo, but had no effect on CYP1A2, CYP2C9, or CYP2C19 [see Clinical Pharmacology (12.3) of full prescribing information]. Concomitant use of VOTRIENT with agents with narrow therapeutic windows that are metabolized by CYP3A4, CYP2D6, or CYP2C8 is not recommended. Coadministration may result in inhibition of the metabolism of these products and create the potential for serious adverse events. [See Clinical Pharmacology (12.3) of full prescribing information.]
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy: Pregnancy Category D [see Warnings and Precautions (5.10)]. VOTRIENT can cause fetal harm when administered to a pregnant woman. There are no adequate and well-controlled studies of VOTRIENT in pregnant women. In pre-clinical studies in rats and rabbits, pazopanib was teratogenic, embryotoxic, fetotoxic, and abortifacient. Administration of pazopanib to pregnant rats during organogenesis at a dose level of ≥3 mg/kg/day (approximately 0.1 times the human clinical exposure based on AUC) resulted in teratogenic effects including cardiovascular malformations (retroesophageal subclavian artery, missing innominate artery, changes in the aortic arch) and incomplete or absent ossification. In addition, there was
11:24 AM
www.TheOncologyNurse.com March/april 2011 I VOl 4, NO 2 11
TON Notes
Don’t Forget to Vote at www.TheOncologyNurse.com/award.
TON_April2011_v7_TON 4/7/11 1:56 PM Page 11

The “Annual Report to the Nationon the Status of Cancer,” emerg-ing from a collaboration of the
North American Association of CentralCancer Registries, the National CancerInstitute (NCI), the Centers for DiseaseControl and Prevention, and theAmerican Cancer Society, shows
declines in cancer rates and improvedsurvival. It helps reassure us that theresources invested to fight cancer havenot been misplaced. Yet those resources are threatened.
Toward the end of the Bush adminis-tration, NCI funding flat-lined. In2009, the American Recovery and
Reinvestment Act provided a welcomeboost allocating millions for NCIresearch grants. Last month, the Housepassed a budget plan that would cutNational Institutes of Health funding by$1.6 billion, leading to fewer grants fromthe NCI. In February, Stevens and colleagues
wrote in the New England Journal ofMedicine that 1 of 5 major medicaladvances approved by the US Food andDrug Administration between 1990 and
2007 originated in a federally funded lab-oratory. This includes more than 40 anti-cancer drugs, some of which you proba-bly recognize: bortezomib, carboplatin,cisplatin, doxorubicin, imatinib, pacli-taxel, sunitinib. How many lives havethese drugs saved or prolonged?Not everyone agrees about what to
leave in the federal budget and what toremove, but we healthcare workers tendto divorce spending on cancer researchor patient programs from our politicalleanings. For us, it is an issue of protect-ing our patients, who are not just a num-ber in a report. With so much promisingresearch under way and such great need,it is painful to imagine what might beaccomplished for the want of a sliver ofthe federal budget. Some say we have pushed billions at
the cancer problem without solvingit—but the money hasn’t been wasted.In the Journal of the NCI last month,Gambacorti-Passerini and associateswrote that patients with chronicmyeloid leukemia (CML) in remissionafter imatinib therapy have a normallife expectancy. Before imatinib, lifeexpectancy for patients with CML was3 to 5 years. Last year, M. D. AndersonCancer Center researchers reportedthat 3 of every 4 women diagnosedwith breast cancer at their institutionin 1944 died within 10 years. In 2004,3 out of 4 patients diagnosed survived10 years! The declines in cancer incidence and
mortality are heartening, but as the pro-portion of our population aged ≥65 yearsgrows, cancer rates will grow, too.Childhood cancers continue to increase.As nurses, we know cancer research is
not only about helping patients livelonger, but also about helping them livebetter. If everyone spent 1 week as anurse on a pediatric cancer ward, we’dsee a unanimous call to increase cancerresearch funding, with everyone agreedthat curing cancer and stopping its bur-den outweighs anyone’s political points.Funding is, of course, only part of
the equation for improving outcomes.Nurses are another important part.Our goal with every issue of TheOncology Nurse-APN/PA is to providethe information you need to play thatpart. This issue includes studies thathad federal funding and others thatwere privately funded. All signalpromise to improve care. We are also introducing two new
departments: The Whole Patient, focus-ing on quality-of-life issues; and News inReview, keeping you current on preva-lent research taking place outside theconference setting, along with regulatoryand legislative news. We will still providecontinuing education, conference high-lights, and advice from peers.Please take a moment to let us know
your thoughts about these changes! �
We Are All in This TogetherBy Editor-in-Chief Beth Faiman, RN, MSN, APRN, BC, AOCN
©2011 The GlaxoSmithKline Group of Companies.All rights reserved. Printed in USA. VOT234R0 January 2011
reduced fetal body weight, and pre- and post-implantation embryolethality in rats administered pazopanib at doses ≥3 mg/kg/day. In rabbits, maternal toxicity (reduced food consumption, increased post-implantation loss, and abortion) was observed at doses ≥30 mg/kg/day (approximately 0.007 times the human clinical exposure). In addition, severe maternal body weight loss and 100% litter loss were observed at doses ≥100 mg/kg/day (0.02 times the human clinical exposure), while fetal weight was reduced at doses ≥3 mg/kg/day (AUC not calculated). 8.3 Nursing Mothers: It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from VOTRIENT, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. 8.4 Pediatric Use: The safety and effectiveness of VOTRIENT in pediatric patients have not been established. In repeat-dose toxicology studies in rats including 4-week, 13-week, and 26-week administration, toxicities in bone, teeth, and nail beds were observed at doses ≥3 mg/kg/day (approximately 0.07 times the human clinical exposure based on AUC). Doses of 300 mg/kg/day (approximately 0.8 times the human clinical exposure based on AUC) were not tolerated in 13- and 26-week studies with rats. Body weight loss and morbidity were observed at these doses. Hypertrophy of epiphyseal growth plates, nail abnormalities (including broken, overgrown, or absent nails) and tooth abnormalities in growing incisor teeth (including excessively long, brittle, broken and missing teeth, and dentine and enamel degeneration and thinning) were observed in rats at ≥30 mg/kg/day (approximately 0.35 times the human clinical exposure based on AUC) at 26 weeks, with the onset of tooth and nail bed alterations noted clinically after 4 to 6 weeks. 8.5 Geriatric Use: In clinical trials with VOTRIENT for the treatment of RCC, 196 subjects (33%) were aged ≥65 years, and 34 subjects (6%) were aged >75 years. No overall differences in safety or effectiveness of VOTRIENT were observed between these subjects and younger subjects. However, patients >60 years of age may be at greater risk for an ALT >3 X ULN. Other reported clinical experience has not identified differences in responses between elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. 8.6 Hepatic Impairment: The safety and pharmacokinetics of pazopanib in patients with hepatic impairment have not been fully established. In clinical studies for VOTRIENT, patients with total bilirubin ≤1.5 X ULN and AST and ALT ≤2 X ULN were included [see Warnings and Precautions (5.1)]. An interim analysis of data from 12 patients with normal hepatic function and 9 with moderate hepatic impairment showed that the maximum tolerated dose in patients with moderate hepatic impairment was 200 mg per day [see Clinical Pharmacology (12.3) of full prescribing information]. There are no data on patients with severe hepatic impairment [see Dosage and Administration (2.2)]. 8.7 Renal Impairment: Patients with renal cell cancer and mild/moderate renal impairment (creatinine clearance ≥30 mL/min) were included in clinical studies for VOTRIENT. There are no clinical or pharmacokinetic data in patients with severe renal impairment or in patients undergoing peritoneal dialysis or hemodialysis. However, renal impairment is unlikely to significantly affect the pharmacokinetics of pazopanib since <4% of a radiolabeled oral dose was recovered in the urine. In a population pharmacokinetic analysis using 408 subjects with various cancers, creatinine clearance (30-150 mL/min) did not influence clearance of pazopanib. Therefore, renal impairment is not expected to influence pazopanib exposure, and dose adjustment is not necessary.
10 OVERDOSAGEPazopanib doses up to 2,000 mg have been evaluated in clinical trials. Dose-limiting toxicity (Grade 3 fatigue) and Grade 3 hypertension were each observed in 1 of 3 patients dosed at 2,000 mg daily and 1,000 mg daily, respectively. Treatment of overdose with VOTRIENT should consist of general supportive measures. There is no specific antidote for overdosage of VOTRIENT. Hemodialysis is not expected to enhance the elimination of VOTRIENT because pazopanib is not significantly renally excreted and is highly bound to plasma proteins.
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenicity studies with pazopanib have not been conducted. However, in a 13-week study in mice, proliferative lesions in the liver including eosinophilic foci in 2 females and a single case of adenoma in another female was observed at doses of 1,000 mg/kg/day (approximately 2.5 times the human clinical exposure based on AUC). Pazopanib did not induce mutations in the microbial mutagenesis (Ames) assay and was not clastogenic in both the in vitro cytogenetic assay using primary human lymphocytes and in the in vivo rat micronucleus assay. Pazopanib may impair fertility in humans. In female rats, reduced fertility including increased pre-implantation loss and early resorptions were noted at dosages ≥30 mg/kg/day (approximately 0.4 times the human clinical exposure based on AUC). Total litter resorption was seen at 300 mg/kg/day (approximately 0.8 times the human clinical exposure based on AUC). Post-implantation loss, embryolethality, and decreased fetal body weight were noted in females administered doses ≥10 mg/kg/day (approximately 0.3 times the human clinical exposure based on AUC). Decreased corpora lutea and increased cysts were noted in mice given ≥100 mg/kg/day for 13 weeks and ovarian atrophy was noted in rats given ≥300 mg/kg/day for
26 weeks (approximately 1.3 and 0.85 times the human clinical exposure based on AUC, respectively). Decreased corpora lutea was also noted in monkeys given 500 mg/kg/day for up to 34 weeks (approximately 0.4 times the human clinical exposure based on AUC). Pazopanib did not affect mating or fertility in male rats. However, there were reductions in sperm production rates and testicular sperm concentrations at doses ≥3 mg/kg/day, epididymal sperm concentrations at doses ≥30 mg/kg/day, and sperm motility at ≥100 mg/kg/day following 15 weeks of dosing. Following 15 and 26 weeks of dosing, there were decreased testicular and epididymal weights at doses of ≥30 mg/kg/day (approximately 0.35 times the human clinical exposure based on AUC); atrophy and degeneration of the testes with aspermia, hypospermia and cribiform change in the epididymis was also observed at this dose in the 6-month toxicity studies in male rats.
17 PATIENT COUNSELING INFORMATION See Medication Guide. The Medication Guide is contained in a separate leaflet that accompanies the product. However, inform patients of the following:• Therapy with VOTRIENT may result in hepatobiliary laboratory
abnormalities. Monitor serum liver tests (ALT, AST, and bilirubin) prior to initiation of VOTRIENT and at least once every 4 weeks for the first 4 months of treatment or as clinically indicated. Inform patients that they should report any of the following signs and symptoms of liver problems to their healthcare provider right away.
• yellowing of the skin or the whites of the eyes (jaundice), • unusual darkening of the urine, • unusual tiredness, • right upper stomach area pain.• Gastrointestinal adverse reactions such as diarrhea, nausea, and vomiting
have been reported with VOTRIENT. Patients should be advised how to manage diarrhea and to notify their healthcare provider if moderate to severe diarrhea occurs.
• Women of childbearing potential should be advised of the potential hazard to the fetus and to avoid becoming pregnant.
• Patients should be advised to inform their healthcare providers of all concomitant medications, vitamins, or dietary and herbal supplements.
• Patients should be advised that depigmentation of the hair or skin may occur during treatment with VOTRIENT.
• Patients should be advised to take VOTRIENT without food (at least 1 hour before or 2 hours after a meal).
VOTRIENT is a trademark of GlaxoSmithKline.
©2010, GlaxoSmithKline. All rights reserved.VTR:3BRS
12 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
From the Editor
TON_April2011_v7_TON 4/7/11 10:48 AM Page 12

Drug shortages continue to plaguethe United States, compromis-ing patient safety and placing
additional strain on healthcare re -sources. The shortages encompass com-mon drugs used to treat a range of con-ditions, from everyday infections toheart attacks. The problem has escalated in recent
years, with the number of drugsdeemed unavailable or scarce jumpingfrom 74 in 2005 to more than 240 in2010, according to the Drug Info -rmation Service (DIS) at the Uni -versity of Utah Hospitals & Clinics.DIS, which started tracking drug short-ages in January 2001, is among the firstgroups to recognize the problem. ErinFox, PharmD, manages DIS and said inan interview, “I believe the currentstate of shortages is a crisis for theUnited States.” The shortages have hit oncology
hard. “In so many cases there are nogood alternative agents, particularly forchemotherapy agents. We have seenover 20 different chemotherapy drugs inshort supply during 2010 and continu-ing into 2011,” Fox explained. Thenonprofit Institute for Safe MedicationPractices (ISMP) warns “there is littlerelief in sight.”
Providers See the Effects of Drug Shortages Local news reports from Alaska,
California, Maryland, Pennsylvania,Texas, Tennessee, Virginia, and else-where show that hospitals in virtuallyevery state are struggling to managethe growing list of hard-to-get drugs.A hospital administrator in Tennesseetold her local paper that drug short-ages were “the new norm.” Small hos-pitals feel the burden more than largehospitals, which can use their pur-chasing power to stockpile drugs onthe shortage list. Many hospitals innetworks manage shortages by shiftingsupplies to whichever sister facilityneeds them. In 2010, ISMP surveyed 1800 phar-
macists, physicians, nurses, and health-care administrators at hospitals andlong-term care facilities and found thatnearly all had been affected by drugshortages. More than 80% complainedthat they were never warned of a loom-ing drug shortage nor told how long itmight last, and 82% said it requiredconsiderable resources to come up witha management plan. Shortages havealso affected providers on a personallevel, with 55% of physicians surveyedsaying they felt anger toward otherstaff or the hospital when a drug wasnot available.
Three-quarters of respondents toldISMP that drug shortages had costtheir facility money. This correspondswith results of a survey by Premier, Inc,an alliance of 200 hospitals and healthsystems in the United States. From Julyto December 2010, Premier questioned311 pharmacy experts about the effectof drug shortages on their practice. Atleast 98% acknowledged substituting amore expensive drug 1 or more times,and 40% said they had done so morethan 21 times. Premier estimates oncology providers
shelled out an additional $10.5 millionin 2010 for the generic equivalents ofdrugs on the shortage list. Not everydrug in short supply has a generic equiv-alent, and Premier says using the besttherapeutic alternative increases treat-ment costs an average of 11%. Acrossall areas of care, hospitals paid an extra$200 million in 2010 for therapeuticsubstitutions.
More than Dollars and CentsThe highest costs of drug shortages
have been borne by patients. Health -care providers have only a few optionswhen they are unable to give thepatient the drug he or she needs: theycan substitute an equivalent or near-equivalent agent, give nothing, or delaytreatment until the drug becomes avail-able. All these options could lead toworse outcomes.Respondents to the ISMP survey
reported “more than 1000 near misses,errors, and adverse outcomes” attribut-able to drug shortages. Some errors ledto a patient’s death. At one facility,hydromorphone was substituted formorphine, which was not available dueto shortages. The provider adminis-tered the hydromorphone at the doseoriginally indicated for the morphineprescription, leading to the deaths of 2patients and nonfatal overdose inanother. Whenever a drug has beensubstituted for another, it is essential toensure that the new drug is correctlydosed or that the correct infusion rateis used.Other dosing errors occur when the
only way the hospital can get the drugis by ordering a different concentra-tion. For example, when preloadedsyringes of epinephrine were difficultto get, some hospitals ordered the drugin vials. Because epinephrine is typi-cally used in emergencies, the nurse ispressured to draw the dose from thevial quickly, increasing the risk ofdelivering an underdose or overdose.Institutions might try to conserve
supplies of a hard-to-get drug by usingsmaller doses. ISMP said attempts to
conserve propofol by cutting the doseat some hospitals led to inadequatesedation or anesthesia awareness.Some hospitals are shortening theduration of therapy when prescribingmedications in short supply. Forpatients with cancer, both approachescould lead to worse outcomes. Substituting one drug for another
compromises outcomes if the replace-ment drug proves to be less effective orless tolerable. Not every drug has asuitable replacement, such as amikacinand acyclovir. As Beth Faiman, RN,MSN, APRN, BC, AOCN, a nursepractitioner at the Cleveland ClinicTaussig Cancer Institute in Ohio and
editor-in-chief of The Oncology Nurse-APN/PA, explained, “Last year, acy-clovir was virtually unavailable for afew months, which put our patients atrisk to develop viral infections.”In addition to the detrimental phys-
ical effects of drug shortages onpatients with cancer, CatherineBishop, DNP, NP, AOCNP, doctor ofnursing practice and an oncology nursepractitioner at Virginia Cancer Care,Inc, pointed out that there are also psy-chological considerations. “Some ofthe issues patients face are the likeli-hood or need to discontinue a certainmedication, such as leucovorin oretoposide. For patients in the metasta-
www.TheOncologyNurse.com March/april 2011 I VOl 4, NO 2 13
Drug Shortages
Continued on page 14
Drug Shortages: A Growing Crisis in OncologyBy Christin Melton
Common Cancer Drugs in Short SupplyThe following is a list of drugs commonly used for patients with cancer that theAmerican Society of Health-System Pharmacists (ASHP) classified as being inshort supply in March. For some drugs, only certain doses or preparations areunavailable. Most shortages are attributable to manufacturing delays and/orincreased demand. In some cases, the manufacturer discontinued the drug oroffered no explanation for the short supply. A couple (ie, capecitabine [Xeloda]tablets and dexamethasone sodium phosphate) have been voluntarily recalledbecause of contamination concerns. To alleviate the shortage of capecitabine,the US Food and Drug Administration has granted the manufacturer permissionto import the drug from the European Union. The ASHP Website provides sug-gestions for managing care when your facility does not have one of the productslisted below.
• Acyclovir injection
• Acyclovir capsules and tablets
• Amikacin injection
• Capecitabine tablets
• Carboplatin
• Cisplatin injection
• Cytarabine
• Dacarbazine powder for injection
• Daunorubicin hydrochloride
• Dexamethasone sodium phosphate
• Doxorubicin injection
• Etoposide injection
• Fentanyl injection
• Fludarabine injection
• Granisetron hydrochloride injection
• Idarubicin hydrochloride injection
• Leucovorin calcium injection
• Melphalan injection
• Morphine injection
• Vancomycin hydrochloride injection
• Vincristine injection
“Last year, acyclovir was virtuallyunavailable for a few months,which put our patients at risk todevelop viral infections.”
—Beth Faiman, RN, MSN,
APRN, BC, AOCN
TON_April2011_v7_TON 4/7/11 10:48 AM Page 13

14 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Drug Shortages
tic setting, this can produce a greatdeal of anxiety,” she said. Talking topatients about drug shortages is alsotough on the practitioner. “For anyprovider to tell a patient that the drugthat may benefit them the most is notcurrently available is difficult andalmost impossible to explain,” she said.
Why Are So Many Drugs in Short Supply?The drug shortage crisis has emerged
from a confluence of factors. “Ourcountry depends on just a few genericmanufacturers to make the majority ofthe critical drugs we need in our hospi-tals and operating rooms each day,”said Fox. A problem at one facility or adecision by one manufacturer toreduce production is ultimately felt atthe clinic. The Pharmaceutical Research and
Manufacturers of America (PhRMA)released a statement on drug shortages inMarch, noting that “according to theFDA [US Food and Drug Administra -tion] and other experts, drug shortagescan occur for any number of reasons.”PhRMA cited “natural disasters; shifts inclinical practices; wholesaler and phar-macy inventory practices; raw materialshortages; changes in hospital andpharmacy contractual relationshipswith suppliers and wholesalers that cancause fluctuations in the availability ofcertain products; adherence to FDA-mandated distribution protocols,which can impact patients’ timelyaccess to medicines; individual compa-ny decisions to discontinue specificmedicines; and manufacturing chal-lenges” as some of the causes of thecountry’s drug shortage problem.In 2010, the FDA reported that 40%
of drug shortages were caused by man-ufacturing issues, which includes diffi-culty obtaining the drug’s raw materi-als or containers and quality controlissues. Another 20% of shortages
occurred when the manufacturerdecided to stop making the drug, oftenbecause it was no longer profitable, and20% resulted from production delays.Premier notes that foreign companiesprovide nearly 80% of the raw materi-als for drug manufacture in the UnitedStates. In 2010, concerns over theintegrity of ingredients from China ledsome drug companies to look for a newsupplier, disrupting production forsome drugs and landing them on theshortage list.
At the Drug Shortages Summit con-vened in November 2010 by theAmerican Society of Health-SystemPharmacists (ASHP), the AmericanSociety of Anesthesiologists, theAmerican Society of ClinicalOncology, and the ISMP, participantsrecognized that regulatory issues cancause shortages. As part of the 2006Unapproved Drugs Initiative, the
FDA is requiring manufacturers ofdrugs approved prior to the adoptionof stricter drug regulations in 1938 toconduct trials and file a New DrugApplication for their generic product.Some drug companies balked at theexpense of complying with the initia-tive and instead elected to stop mak-ing the drug. A drugmaker must alsofile an application with the FDAwhen it wants to change suppliers foractive ingredients, and several havecomplained that the agency is slow toapprove these applications. Complexpackaging re quirements and demandsfor risk evaluation and mitigationstrategies for certain drugs have alsocontributed to delays.Premier outlines other potential caus-
es for drug shortages. When the econo-my was in recession, many companies inthe drug production chain scaled downthe quantity of supplies kept on hand.Any disruption in one company’s abili-ty to restock supplies has a ripple effecton the manufacturer’s ability to get thedrug to market.Some pharmacists complain that
“gray market distributors” are causingartificial drug shortages by buying largequantities of important, inexpensivedrugs and reselling them at greatlyinflated prices once the drugs are diffi-cult to obtain. This is a bit like when aticket outlet purchases all the premiumtickets for a major rock concert or pop-ular Broadway show and offers them ata high markup once the show has soldout. Providers who stockpile drugs forfear that they might become hard to getalso contribute to artificial shortages.Temporary shortages occur when onedrug is discontinued, everyone switchesto the same alternative, and the manu-facturer cannot keep up with supply.
Is Anything Being Done?Fox expressed optimism about a few
recent developments reguarding thedrug shortage. “I am hopeful the prob-lem may subside in part because 2 of thelargest generic companies with multipleshortages seem to be resolving theirmanufacturing problems,” she said. If
this happens, Fox said the number ofshortages might fall to 2009 levels,which she notes were still too high. Congressional legislators have intro-
duced US Senate Bill 296, thePreserving Access to Life-SavingsMedications Act. The bill requiresdrugmakers to notify the FDA at least6 months before stopping or delayingproduction for a drug. Many in themedical community support the bill.“There is widespread belief by many inthe medical community that thereneeds to be oversight and regulations,which should be strictly enforced, somanufacturers cannot just decide tostop the manufacturing of a drug with-out significant notice,” said Bishop.Bill 296 also requires the FDA to iden-tify drugs vulnerable to shortages andtake steps to ensure that the supply isnot interrupted.“The bill won’t solve all shortage
problems, but it is a great start,” saidFox. She encouraged clinicians to con-tact their congressional officials andurge them to support the bill.Some patients are not waiting for leg-
islation to resolve the problem and havedecided to head to court. Genzyme,which has been plagued with problemsat its manufacturing facilities, has beennamed in a civil lawsuit by a group ofpatients with Fabry disease. Genzymemanufactures Fabrazyme, the primarydrug used to treat the genetic disor-der. In the past year, the companystarted rationing access to the drugand cutting dosages; the lawsuitclaims at least 3 patients have diedfrom this approach. Genzyme hadsimilar manufacturing problems withCerezyme, its drug for Gaucher dis-ease, but believes it will soon havethe situation corrected.As the Drug Shortages Summit
participants pointed out, the FDAcannot require a drug manufacturerto keep making a product. They saidCongress can and should, however,offer incentives to companies thatmanufacture life-saving generic medi -cations, such as tax breaks and ex -tended exclusivity rights.
Taking Steps to Protect PatientsFox listed a few steps hospitals can
take to minimize the effects of drugshortages on their patients. “Phar -macists can discuss shortages with clini-cians as far ahead as possible.” Shenoted that sometimes this is not possi-ble, but “as much advance notice as pos-sible can help when decisions abouttherapy are being made, particularly ifanother treatment choice is availableand will work well for the patient.”She recommended that clinicians
Drug Shortages: A Growing Crisis in Oncology Continued from page 13
Continued on page 16
“Some of the issues patientsface are the likelihood or needto discontinue a certainmedication, such as leucovorinor etoposide. For patients in themetastatic setting, this canproduce a great deal of anxiety.”—Catherine Bishop, DNP, NP, AOCNP
175
150
125
100
75
50
25
02005
Year
Num
ber
2006 2007 2008 2009
Total drugshortages
Drug shortagesinvolving sterileinjectables
Figure. Drug shortages per year.
Clinicians shouldconsider centralizing theirsupply of medicationsand tracking what theyneed based on theirpatient roster.
TON_April2011_v7_TON 4/7/11 10:48 AM Page 14

STARTS STRONG. LASTS LONG.
IndicationALOXI® (palonosetron HCl) injection 0.25 mg is indicated in adults for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of moderately emetogenic chemotherapy, and acute nausea and vomiting associated with initial and repeat courses of highly emetogenic chemotherapy.
Important Safety Information
of its components
include headache (9%) and constipation (5%)
Please see the brief summary of the Full Prescribing Information on the adjacent page.
References: 1. Gralla R, Lichinitser M, Van der Vegt S, et al. Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy: results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron. Ann Oncol. 2003;14:1570-1577. 2. Eisenberg P, Figueroa-Vadillo J, Zamora R, et al. Improved prevention of moderately emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmacologically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus dolasetron. Cancer. 2003;98:2473-2482. 3. Data on fi le. Eisai Inc., Woodcliff Lake, NJ. 4. Aapro MS, Grunberg SM, Manikhas GM, et al. A phase III, double-blind, randomized trial of palonosetron compared with ondansetron in preventing chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy. Ann Oncol. 2006;17:1441-1449.
ALOXI®
Help support your patients’ chemotherapy treatment goals Powerful CINV prevention in the fi rst 24 hours and up to 5 days following
moderately emetogenic chemotherapy1,2
Lasts long against nausea following moderately emetogenic chemotherapy
Powerful acute CINV prevention following highly emetogenic chemotherapy4
ALOXI® provides powerful CINV prevention that can’t be ignored.
TON_April2011_v7_TON 4/7/11 10:48 AM Page 15

consider centralizing their supply ofmedications and tracking what theyneed based on their patient roster. “Thisstrategy is particularly helpful withchemotherapy shortages,” Fox said.“Track out the needs of the patients andthen, if insufficient drug is available, thephysicians can decide the best action.”
In some cases that might be not accept-ing a new patient, delaying treatment,or altering the treatment plan.
ISMP recommends “establishing ashortage network” with other health-care providers. The organization alsosuggests adopting strategies to preventerrors when using substitutes and con-
sulting the ethics committee about anydecisions to prioritize or place limits onmedications in short supply.
Several online resources are avail-able to identify ongoing and poten-tial shortages and ways to manage adrug shortage. Fox recommended vis-iting www.ashp.org/shortage, which
maintains a list of current shortages,resolved shortages, and drugs no longeravailable. The site also contains severalresources on managing drug shortagesand encourages clinicians to report pos-sible shortages to ASHP.
Because the vast majority of drugs inshort supply or no longer available areinjectables, nurses often have the finalopportunity to ensure that the substi-tute drug provided is being used at thecorrect dose. The ASHP Website offershelp with this, by highlighting the pos-sibility of confusion or dosing errorswith some substitute medications. Forexample, ASHP warns providers of the“potential for dosing errors when inter- changing leucovorin and levoleuco- vorin (Fusilev),” noting that the levo -leucovorin dose should be one-half theracemic leucovorin injection dose.
Etoposide for injection is anotherdrug in short supply, and many hospi-tals are substituting oral etoposide. Theoral version has only half the bioavail-ability of the injectable. This meansthat the oral dose needs to be doublethat of the intravenous dose.
As the ISMP study indicates, problemshave also occurred with epinephrine dos-ing. Miscalculations have been madewhen switching be tween the 1-mg/mLstrength of epinephrine and the 0.1-mg/mL dose. In addition, some hos-pitals are using the 1-mg/mL syringe thathas an intracardiac needle permanentlyaffixed. The ISMP warns providers notto attempt to remove this needle.
To prevent errors due to confusionabout differences in dosing, activity,adverse effects, etc, between the intend-ed drug and its substitution, ASHP rec-ommends updating automated systemsand order-entry systems. Pharmacy staffshould also communicate with nursingstaff about alternative therapies and anyspecial considerations.
Talking to patients or caregiversabout why you have to delay their sur-gery, interrupt their treatment, or can-not give them the most effective drugfor their disease is probably one of thegreatest difficulties providers face indealing with the shortages. It is also oneproblem for which the organizationsadvising hospitals on how to managedrug shortages have few suggestions. �
ALOXI® (palonosetron HCl) injection
BRIEF SUMMARY OF PRESCRIBING INFORMATION
INDICATIONS AND USAGE
Chemotherapy-Induced Nausea and VomitingALOXI is indicated for:
DOSAGE AND ADMINISTRATIONRecommended DosingChemotherapy-Induced Nausea and Vomiting
Instructions for I.V. Administration
CONTRAINDICATIONS
[see Adverse Reactions (6) ]
WARNINGS AND PRECAUTIONSHypersensitivity
ADVERSE REACTIONS
≥
Table 1: Adverse Reactions from Chemotherapy-Induced Nausea and Vomiting Studies ≥ 2% in any Treatment Group
Postmarketing Experience
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONSPregnancy
Labor and Delivery
Nursing Mothers
Pediatric Use
Geriatric Use
≥
≥ ≥
≥
Renal Impairment
Hepatic Impairment
Race
OVERDOSAGE
PATIENT COUNSELING INFORMATION FDA-Approved Patient Labeling (17.2) in
Instructions for Patients
see Adverse Reactions (6)
ALOXI®
EventALOXI
0.25 mg (N=633)
Ondansetron 32 mg I.V. (N=410)
Dolasetron 100 mg I.V.
(N=194)
16 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Drug Shortages
Drug Shortages: A Growing Crisis in Oncology Continued from page 14
The pharmacy staffshould also communicatewith the nursing staffabout alternativetherapies and any specialconsiderations.
TON_April2011_v7_TON 4/7/11 12:27 PM Page 16

“They can come in the morning andsee everybody and come out with aplan,” explained Philip J. Stella, MD,the clinic’s medical director and med-ical oncologist. The multidisciplinaryapproach seems to be working. Notonly has the program shaved morethan two-thirds off the time betweenwhen lung cancer is suspected to initi-ation of a treatment plan, “We havevery high rates of satisfaction from thepatients and their families,” said Stella.Patients are not the only ones who
appreciate St. Joseph Mercy’s efforts.Primary care physicians in the regionhave shown their satisfaction with theprogram by referring more patients tothe lung cancer clinic. “We try to makeit easy for them, so [that] when theyhave a patient with lung cancer, theydon’t have to call 3 different offices. …Just 1 call will get the patient seen in atimely fashion,” said Stella. The lung cancer clinic’s reputation
continues to spread. Stella said thepositive reception for the multidisci-plinary approach has led to patientreferrals from physicians outside theSt. Joseph Mercy system and the needto expand.
A Model in the MakingLike other multidisciplinary clinics at
St. Joseph Mercy, the lung cancer clinicis spearheaded by an advisory committee,which consists of physicians and otherproviders who tend to patients at theclinic and participate in tumor boards.Vita McCabe, MD, a cardiothoracic sur-geon, chairs the committee and helpssteer the program. McCabe described her philosophy of
care: “When you are a cancer patient,you need to feel that you are in a high-end department store, that you are com-pletely cared for from every direction—[that] this is not a discount-shoppingsituation.” Department stores claim tooperate according to the principle thatthe “customer is always right.” Althoughthe patient might not always be right atSt. Joseph Mercy, the lung cancer clin- ic’s multidisciplinary team factors thepatient’s perspective into each decision.In developing the program from the
perspective of the patient, it becameclear that it would be important to assigneach patient to a nurse navigator. Thenavigator serves as the point person forarranging visits and facilitating commu-nication between the patient or thepatient’s caregivers and the individualson his or her care team. This is useful forcoordinating not only anticancer treat-ment, but also support services. Alongwith medical oncologists, surgeons, andradiologists, many patients meet withresearchers, social workers, and nutri-tionists at the clinic.
Lara Blair, RN, is one of the program’snurse navigators. “Even if someone justhas a small question, when you have ateam of 3 or 4 different doctors and otherspecialists, that can mean 20 phonecalls,” said Blair. “One of my biggest jobsis cutting that process down and stream-lining it for [the patients].”Benefits of this system are that
“patients don’t have to wait for care,nor are they confused,” said McCabe.The clinic strives to stay at the fore-
front of lung cancer care, offering anarray of advanced surgical and radio-therapy techniques. To handle growingdemand, a second surgeon was recentlyadded to the staff. With 2 surgeons on-board, the clinic has been able toexpand the number of minimally inva-sive approaches available, to includevideo-assisted and robotic surgery andthoracoscopic procedures. St. Joseph Mercy became the first
hospital in Michigan to offer theCyberKnife system for stereotacticbody radiation therapy. As a result,“Medically inoperable patients arebeing treated for their lung cancerswith a high degree of success and withminimal complications and sideeffects,” said Walter M. Sahijdak, MD,a radiation oncologist at the clinic. As a member of the Community
Clinical Oncology Program (CCOP)network for the past 20 years, St.Joseph Mercy has actively recruitedpatients with cancer for a number ofclinical trials. The CCOP affiliationallows patients treated at St. JosephMercy, including those seen in thelung cancer clinic, to enroll in trialsconducted by major national researchgroups, such as the Mayo Clinic andthe M. D. Anderson Cancer Center.The lung program currently haspatients enrolled in several innova-tive studies its researchers are con-ducting, including trials comparingoutcomes with CyberKnife versusstandard resection in patients withsolitary lung nodules.The lung cancer clinic recently
moved into new space, which houses anurse navigation office and the adviso-ry committees for each of St. JosephMercy’s multidisciplinary clinics. Stellasaid the lung cancer program has beenso successful he expects it to serve as amodel for future multidisciplinary clin-ics focused on other tumor types.
Success Paves the WayThe success of the lung cancer pro-
gram no doubt factored into last year’sdecision by the National CancerInstitute’s Community Cancer CentersProgram (NCCCP) to designate St.Joseph Mercy as one of only 30 NCCCPsites in the nation. The NCCCP ini-tiative seeks to develop a network ofcommunity hospitals tasked with re -searching ways to improve the qualityof cancer care and prevention, as wellas to reduce disparities in access to careand outcomes.
An accompanying $2.5-million grantwill allow St. Joseph Mercy to add sever-al cancer specialists to its staff and devel-op new programs. In a press releaseannouncing the designation, Stella, the
grant’s principal investigator, said, “Thisprogram allows St. Joseph Mercy AnnArbor to accelerate the tempo of scien-tific research and advancement of cancercare. … St. Joe’s is already recognized forour cancer research; this contract allowsus to take our program to the next leveland expand other areas of research andcare. It underscores our dedication toproviding our patients with the latestand most state-of-the-art care.” The NCCCP contract calls for St.
Joseph Mercy to develop a tissue bank.Stella said while St. Joseph Mercy typi-cally submits tissue from patients in itsclinical trials for translational research,the center will now be preserving tumortissue samples for all their patients withcancer. “We are going to…be able toprovide that to investigators at academiccenters around the country that wantaccess to fresh tissue or paraffin-embed-ded tissue to do their translational work,”said Stella. “This is a very important partof this grant and the network as awhole,” he explained. “So much of whatwe are going to be learning about canceris going to be through translationalresearch. Other plans include hiring a geneti-
cist to counsel patients and evaluatethose considered high risk and expand-ing outreach efforts to underservedcommunities. This will require hiring aminority coordinator to reach out toethnic minority populations andadding a financial counselor to thestaff to help low-income and indigentpatients with obtaining oncologic care.“There is no way in this economic
environment that the hospital wouldever be able to provide these posi-tions,” Stella said. “If it had not beenfor this grant, we absolutely would notbe able to provide many of the servicesthat I think we should be doing as acancer program.” And had it not beenfor the stellar multidisciplinary lungcancer clinic at St. Joseph Mercy, itmight have taken the NCCCP longerto recognize just how determined thecenter is to ensure that people withcancer have the best care possible. �
www.TheOncologyNurse.com March/april 2011 I VOl 4, NO 2 17
Cancer Center Profile
St. Joseph Mercy Cancer Care Center... Continued from cover
• Access daily news impacting you and your patients
• Easily share and post to social media sites
• Earn continuing education credits
Oncology News
YOUR Way
www.TheOncologyNurse.com
“Medically inoperablepatients are being treatedfor their lung cancers witha high degree of successand with minimalcomplications and sideeffects.”
—Walter M. Sahijdak, MD
“They can come in the morning and seeeverybody and come out with a plan.”
—Philip J. Stella, MD
TON_April2011_v7_TON 4/7/11 10:48 AM Page 17

www.TheOncologyNurse.com18 March/april 2011 I VOl 4, NO 2
Conference News
©ASCO/Todd Buchanan 2011.
The somatostatin analog lan-reotide (Somatuline) reducedthe frequency of vomiting for
patients with inoperable malignantbowel obstruction (MBO) in what pre-senter Pascale Mariani, MD, at the Institut Curie in Paris, France,called the first randomized, double-blind, placebo-controlled study onpalliative care in this patient popula-tion. “We showed that lanreotide mayreduce the frequency of vomiting andallow for nasogastric tube [NGT]removal, which makes hospital dis-charge possible,” said Mariani, whopresented the findings. Investigators at 22 European centers
enrolled symptomatic patients withinoperable MBO who were experiencing≥2 vomiting episodes per day or had anNGT. Most patients were severelyimpaired; 63.8% had an ECOG perform-ance status of 3 or 4, and 80% were fedby central parenteral route. Patients wererandomly assigned to receive 1 injectionwith 30 mg of lanreotide microparticles(n = 43) or placebo (n = 37). The trial’sprimary end point was response rate(RR), defined as the proportion ofpatients at 7 days who, for 3 consecutivedays, recorded ≤1 episode of vomiting orno vomiting after NGT removal.
In the intent-to-treat (ITT) popula-tion, RR was 41.9% for patients injectedwith lanreotide compared with 29.7%for those given placebo, a difference thatwas not significant (odds ratio [OR],1.75; 95% confidence interval [CI], 0.68-4.49; P = .24). A per protocol analysisfound a statistically significant benefitassociated with lanreotide use, with an
RR of 57.7% in the treatment arm versus30.4% in the control group (OR, 3.60;95% CI, 1.03-12.62; P = .045). Marianisaid investigator assessment of data forthe ITT population also found a signifi-cant difference in RR between thegroups, favoring lanreotide over pla -cebo (50.0% vs 28.6%, respectively; P = .0481). By day 7, the frequency ofvomiting had declined by a median of2.3 episodes for patients in the lanreotidegroup and 1.3 episodes for patients in theplacebo arm (P = .4510).
On most secondary end points, no significant differences were observed be -tween the groups. The mean number ofdays without vomiting and the meanchange in episodes of nausea from base-line to day 7 were similar, as was thedecline in the abdominal pain score.Well-being, which investigators assessedon day 7 using a visual analog scale,
was the only secondary end point thatsignificantly favored lanreotide. Pa -tients treated with lanreotide experi-enced significant im provement inwell-being, which declined for patientsgiven placebo.Mariani said treatment-emergent
adverse events were similar in bothgroups and as expected for patients with inoperable MBO. None of the serious adverse events appeared to betreatment-related. Robert S. Krouse, MD, a surgery
professor at the University of Arizonaand staff general and oncologic sur-geon at Southern Arizona VA HealthCare System in Tuscon, discussed thefindings at the session. He observedhow challenging it is to treat MBO,which occurs in approximately one-quarter of patients with colorectalcancer and half of patients with ovar-ian cancer. “There is no defined algo-rithm for the management of thesepatients,” said Krouse, but he notedthat somatostatin analogs are thestandard of care, with multiple stud-ies showing some benefit withoctreotide (Sandostatin LAR) use.“This study suggests that lanreotidemay also have a role in the treatmentalgorithm for MBO.” Krouse said medical treatment is
often preferred to surgery even forpatients with operable MBO becausenearly 20% “just get postoperativepain without benefit.” The patientswho undergo surgery have higher risksof morbidity and mortality and worsequality of life and up to 50% experi-ence recurrence. Krouse said nearlyone-third of patients with MBO ben-efit from nonsurgical interventionssuch as nasogastric compression andsymptom management. �
Lanreotide Reduces Vomiting in Patients with Malignant Bowel ObstructionBy Caroline Helwick
The following articles are based on presentations at the 2011 Gastrointestinal CancersSymposium held January 20-22, 2011, in San Francisco, California.
“We showed that lanreotide may reducethe frequency of vomiting and allow fornasogastric tube removal, which makeshospital discharge possible.”
—Pascale Mariani, MD
New Radiotherapy Technique Less Toxic for Patients with Anal Cancer
Using dose-painted intensity-modulated radiation therapy(DP-IMRT) to treat cancer in
the anal canal reduces the risk of seri-ous adverse events associated withstandard radiation therapy withoutcompromising survival according todata presented by Lisa Kachnic, MD,chief of radiation oncology at BostonMedical Center and an associate pro-fessor with Boston University Schoolof Medicine, Massachusetts. Shereported results from the phase 2Radiation Therapy Oncology Group(RTOG)-0529 trial at a press briefing. Kachnic said although the study did
not achieve its goal of a 15% reduc-tion in the rate of gastrointestinal(GI) and genitourinary toxicities≥grade 2 observed in RTOG-9811,which used standard external beam
radiation, DP-IMRT demonstratedenough benefit to become the “stan-dard radiation technique in futureRTOG anal cancer trials assessingnovel agents in combination withradiation.” With DP-IMRT, the radia-tion dose is “painted” to conform tothe shape of the targeted tissue andspares nearby healthy tissue. Investigators analyzed data for 52
patients with stage II and stage III analcancer enrolled in RTOG-0529 whoreceived standard 5-fluorouracil/mito-mycin-C chemotherapy plus DP-IMRT. Patients with T2 diseasereceived a total radiation dose of 50.4Gy targeted to the tumor and 42 Gydelivered to elective lymph nodes in28 fractions over 5.5 weeks. Patientswith T3 to T4 disease received 54 Gyto the tumor and 45 Gy to the nodes,
delivered in 30 fractions over 6 weeks.Findings were compared with resultsfor the patients in RTOG-9811 whohad received the same chemotherapyregimen plus conventional radiothera-py (n = 325).The RTOG-0529 patients had sig-
nificantly lower rates of acute GI anddermatologic toxicities. Nearly 20% ofpatients given DP-IMRT developedGI toxicities ≥grade 3 versus 35% ofthe selected RTOG-9811 patients (P = .0082). Whereas skin toxicities≥grade 3 were observed in ~50% ofthe RTOG-9811 patients, the ratedropped to ~20% for patients in theDP-IMRT group (P <.0001). Kachnicsaid investigators were surprised bythe significant 10% reduction inhematologic toxicities ≥grade 2 seenwith DP-IMRT (P = .032).
At median follow-up of 27 months,the trials demonstrated similar 2-yearrates of locoregional and distant failureand survival outcomes, even thoughRTOG-0529 had a higher proportion ofnode-positive patients. The medianduration of DP-IMRT was 43 days ver-sus 49 days for the conventional arm,and patients in RTOG-0529 experi-enced fewer treatment breaks, whichKachnic said was an important benefit.Kachnic acknowledged DP-IMRT
involved a learning curve and that“real-time quality assurance” is essen-tial for safety and efficacy. She said theRTOG-0529 researchers concludedthat “DP-IMRT is feasible with rigor-ous quality assurance and continuededucation...and may allow for furtherradiation dose escalation in advanced-stage disease.” —CH �
TON_April2011_v7_TON 4/7/11 10:48 AM Page 18

THE 5-YEAR SURVIVAL RATEIS 17% FOR PATIENTS WITHMETASTATIC SOFT TISSUE SARCOMA,YET SIGNIFICANT THERAPEUTICADVANCEMENTS ARE LAGGING.1
NEW TREATMENTS ARE URGENTLY NEEDED.
Reference: 1. National Cancer Institute. Surveillance Epidemiology and End Results. seer.cancer.gov/statfacts/html/soft.html. Accessed March 19, 2010.
Copyright © 2010 Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc.All rights reserved. 21003100(5)-ARI
SARCOMA: THE ONLY THING PROGRESSING IS THE DISEASE
TON_April2011_v7_TON 4/7/11 10:48 AM Page 19

In a study funded by PathworkDiagnostics, Inc., researchers foundthat using the company’s tissue of
origin test for patients with hard-to-identify primary cancers enabledaccurate diagnosis of the tumor inseveral cases and led to changes intreatment. Patients whose diagnosiswas confirmed appeared less anxious. Data were collected for 59 patients
whose physician used the test to
identify their primary cancers. Thephysicians (n = 48) completed anonline survey about the patient’sdiagnosis, diagnostic proceduresused, and recommended treatmentsbefore and after tissue of origin test-ing. Responses were confirmed bytelephone.The physicians indicated that
prior to performing the test, patientsunderwent a median of 6 imaging
tests and 10 immunohistochemistrytests. In 54% of patients, the tissue oforigin test results led to changes indiagnosis. Treatment changed for68% of patients. Nearly two-thirds ofphysicians said the test was “clinical-ly useful” in informing disease man-agement. In addition, 62% patientswere ob served to have less anxietyafter receiving results.The authors wrote, “In patients
with difficult-to-diagnose primarycancers, extensive baseline diagnos-tics is not uncommon and less thanhalf of the patients have an estab-lished working diagnosis.” The test,which compares >2000 genes in thepatient’s tumor against a control setof gene expression patterns from 15tumor types, received clearance in2010 from the US Food and DrugAdministration. �
20 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Conference News
2011 GASTROINTESTINAL CANCERS SYMPOSIUM
A Wealth of Targets Identified in Colorectal CancerBy Caroline Helwick
For patients with colorectal cancer(CRC), advances in molecularprofiling have led to an explosion
in novel agents specific for targets aboveand beyond the epidermal growth factorreceptor (EGFR). Joseph Tabernero,MD, director of clinical research at Valld’Hebron Institute of Oncology inBarcelona, Spain, previewed the futureof treatment for CRC.“The good news is there are lots of
new compounds. The challenge will beto profile patients accurately and toidentify the gene signatures of thosewho will benefit from the individualdrugs and combinations of agents,” saidTabernero.
EGFR Remains a TargetMany patients with CRC are resist-
ant to the currently approved EGFRinhibitors cetuximab (Erbitux) andpanitumumab (Vectibix). The KRASgene has already been identified as play-ing an important role in CRC, withconstitutive mutations of KRAS servingas predictors of resistance to anti-EGFRmonoclonal antibodies.
Researchers are examining the role ofgenetic mutations associated with othersignal transducer proteins, includingmutations in BRAF, NRAS, PIK3CA,AKT, PTEN, and TP53. Tabernero saidany of these might prove to be a useful“on/off” biomarker for EGFR expressionin metastatic CRC. “More effective monoclonal antibod-
ies are coming,” Tabernero promised.Encouraging results have been observedwith the investigational compoundsGA201 and SYM004, including seem-ingly durable responses. “Objectiveresponse rates have been achieved invery refractory patients,” he noted. HER3 is a new target in CRC. It has
been implicated as a potential mecha-nism of resistance to EGFR inhibitors. Ahandful of anti-HER3 compounds are indevelopment, including the monoclonalantibody MEHD7945A (a dual anti-EGFR and HER3 inhibitor), MM121,and U3-1287-AMG888.
Other Targets Under StudyResearchers are developing mono-
clonal antibodies specific for receptorsother than EGFR. One target isinsulin-like growth factor-1 receptor(IGF-1R) protein, which is expressedin 90% of colon cancers but not foundat all in normal mucosa. Expressionlevels correspond with proliferationand tumor stage. Overexpression ofIGF-1R, observed in ~50% of patients,is an independent prognostic factor forworse survival. Research into therapeutics for this
novel target took a step back when a ran-domized phase 2 clinical trial of IMC-A12, an investigative inhibitor of IGF-1R, failed to improve outcomes inpatients with CRC refractory to EGFRinhibitors. Ongoing studies are attempt-ing to refine the gene signature anddevelop effective agents.
Two possible new targets are the li -gand of the c-Met receptor and hepato-cyte growth factor (HGF) receptor.Both have been implicated in tumorinvasiveness, metastasis, and prolifera-tion; angiogenesis; and resistance totreatment. The HGF inhibitor rilotu-mumab (AMG102) showed promisingefficacy in metastatic CRC when com-bined with panitumumab. Eric VanCutsem, MD, University of Leuven,Belgium, presented data from an inter-national, randomized, phase 1/2 trialinvolving 142 patients that comparedpanitumumab alone; rilotumumabplus panitumumab; and ganitumumab(AMG479), a novel IGF-IR inhibitor,plus panitumumab. Van Cutsem saidthe doublet of rilotumumab and panitu-mumab was promising, producing anoverall response rate (ORR) of 31%compared with an ORR of 22% in theganitumumab arm and 21% in the pan-itumumab monotherapy group. Medianprogression-free survival was 5.2months with rilotumumab plus panitu-mumab, 5.3 months with the ganitu-mumab combination, and 3.7 monthswith panitumumab alone.Another avenue being pursued in -
volves the tumor necrosis factor–relatedapoptosis-inducing ligand (TRAIL) andits receptors. TRAIL inhibits the growthof colon cancer cells, and TRAIL-R1expression correlates with improved disease-free survival. Conatumumab(AMG655) is a monoclonal antibodythat binds to TRAIL-R2 and has pro-duced partial responses in early trials. It isalso being studied in combination withstandard chemotherapy regimens.
Looking at Downstream PathwaysSome researchers are looking into
inhibiting critical downstream path-ways, such as the mitogen-activatedprotein kinase (MAPK)/extracellular
signal-regulated kinase (ERK) path-way. Protein kinases along this path-way regulate cell proliferation, differ-entiation, and survival and respond toexternal stimuli. Tabernero said inves-tigators have identified at least 2 ther-apeutic targets in the MAPK/ERKpathway, namely RAF and MEK.Already more than a dozen inhibitorsare in development.In 50% of patients with advanced
disease, PIK3CA is dysregulated.PIK3CA activation triggers a signaltransduction cascade that promotescell growth and survival. Druggabletargets in this pathway includePIK3CA, AKT, mTOR, TORC 1/2,and pS6K. Nearly 20 relevant com-pounds are being investigated, includ-ing some multikinase inhibitors. It is thought that many novel agents
might be most effective when combined.Promising marriages are between 2 ERKpathway inhibitors (ie, a RAF inhibitorand a MEK inhibitor); 2 PIK3CA path-way inhibitors (ie, a dual PIK3CAinhibitor and a TORC 1/2 inhibitor); 1 ERK pathway inhibitor and 1 PI3Kpathway inhibitor (ie, a MEK inhibitorwith either an AKT, TORC 1/2, orPIK3CA inhibitor). Any of these agentscould potentially be combined with acytotoxic agent, as well.Despite an apparent plethora of
opportunities for arresting proliferationof CRC cells, Tabernero cautioned thathuge challenges lie ahead. The molecu-lar profile of a specific cancer cell influ-ences its behavior, and cancer cells oper-ate under “plastic and evolutivephenomena” that extend to the genelevel (expression, mutation, amplifica-tion/deletion, etc) and the proteomiclevel (activation, phosphorylation).“Cells change under the pressure ofstress,” he said, noting that treatmentinduces stress. �
Novel Strategiesfor Treating CRC• More efficient anti-EGFR mono-clonal antibodies
• Monoclonal antibodies directed toother members of the EGFR/HERfamily
• Monoclonal antibodies directed toother receptors (c-MET, IGF-1R)
• Inhibitors of downstream effectors(MAPK/ERK)
• Rationally based combinations• Identification of populations likelyto benefit from specific therapies
Tissue of Origin Test Leads to Changes in TreatmentBy Christin Melton
TON_April2011_v7_TON 4/7/11 10:49 AM Page 20

Numoisyn Liquid
Prescribing Information
Ingredients:Water, sorbitol, linseed (flaxseed) extract, Chondrus crispus, methylparaben, sodiumbenzoate, potassium sorbate, dipotassium phosphate, propylparaben.
How Supplied: 30 mL per bottle or 300 mL per bottle.
Therapeutic Group: Numoisyn Liquid is an oral solution formulated for the relief of chronic and tempraryxerostomia (dry mouth), which may be a result of disease, medication, oncology therapy, stress, or aging.
Indications: Numoisyn Liquid is indicated for the treatment of symptoms of dry mouth. NumoisynLiquid relieves the symptoms of dry mouth by enhancing swallowing, improving speech mechanics, andlubricating the oral cavity like natural saliva. Numoisyn Liquid may be used to replace natural salivawhen salivary glands are damaged or not functioning. The viscosity is similar to that of natural saliva.
Contraindications: Numoisyn Liquid are contraindicated in patients with a known history ofhypersensitivity to any of the ingredients.
Special Precautions for Use: As Numoisyn Liquid contains linseed (flaxseed) extract, patients withirritable bowel syndrome or diverticular disease or those on a high linseed diet may experienceabdominal discomfort.
Warning: Federal law restricts Numoisyn Liquid to sale by, or on the order of, a physician or properlylicensed practitioner.
Interactions: There are no known interactions between Numoisyn Liquid and any medicinal orother products.
Directions for Use: Shake bottle well. Take 2 mL (about 1/2 teaspoon) of Numoisyn Liquid and rinsearound in the mouth before swallowing. Use as needed.
Side Effects: Patients may experience difficulty in swallowing, altered speech, and changes in taste.If side effects persist or become severe, patients should contact a physician.
Storage: Store at room temperature. Do not refrigerate. Use within 3 months of first opening.KEEP OUT OF REACH OF CHILDREN.
Please Note: Numoisyn Liquid is translucent and may contain some natural particles that do notaffect the quality of the product.
Hydrate.Soothe.Protect.
Hydrate.Soothe.Protect.
Works Fast...And Lasts.
Numoisyn Lozenges
Prescribing Information
Ingredients: Sorbitol (0.3 g per lozenge), polyethylene glycol, malic acid, sodium citrate,calcium phosphate dibasic, hydrogenated cottonseed oil, citric acid, magnesium stearate,and silicon dioxide.
Pharmaceutical Form: Oral lozenge
Contents: 100 lozenges per bottle. Net weight of 40 g (0.4 g per lozenge).
Therapeutic Group: Numoisyn Lozenges are oral lozenges formulated to promote lubricationof oral mucosa that may be dry due to a variety of circumstances, including medication,chemotherapy or radiotherapy, Sj˙ogren’s syndrome, or oral inflammation.
Indications: Numoisyn Lozenges are indicated for the treatment of xerostomia (dry mouth).Numoisyn Lozenges provide temporary relief of dry mouth due to damaged salivary function.Numoisyn Lozenges are formulated to support the natural protection of teeth provided by salivaso that no damage occurs to teeth with repeated use of the lozenges.
Contraindications: Numoisyn Lozenges are contraindicated in patients with fructose intoleranceor a known history of hypersensitivity to any of the ingredients.
Warning: Federal law restricts Numoisyn Lozenges to sale by, or on the order of, a physician orproperly licensed practitioner.
Interactions: There are no known interactions between Numoisyn Lozenges and any medicinalor other products.
Directions for Use: Let one Numoisyn Lozenge dissolve slowly in the mouth when needed.To obtain optimal effect, move the lozenge around in the mouth. Repeat as necessary. Do notexceed 16 lozenges in 24 hours.
Side Effects: Excessive consumption can cause minor digestive problems.
Storage: Store at room temperature. KEEP OUT OF REACH OF CHILDREN.
Overdose: No overdoses have been reported to date.
Xclair Cream
Prescribing Information
Ingredients:Water, isohexadecane, butyrospermum parkii, pentylene glycol, ethylhexyl palmitate,glycyrrhetinic acid, cera alba, peg-30 dipolyhydroxystearate, bisabolol, polyglyceryl-6polyricinoleate, tocopheryl acetate (antioxidant), hydrogenated castor oil, sodium hyaluronatenylon 12, butylene glycol, magnesium sulfate, piroctone olamine, allantoin, magnesium stearate,disodium EDTA, vitis vinifera, ascorbyl tetraisopalmitate, propyl gallate, and telmesteine.
Contents: 75 mL per tube
Therapeutic Group: Xclair Cream is formulated for symptom relief in radiation dermatitis.
Indications: Xclair Cream is indicated to manage and relieve the burning, itching, and painexperienced with radiation dermatitis. Xclair Cream may be used to relieve the pain of first-and second-degree burns.
Contraindications: Xclair Cream is contraindicated in patients with a known history ofhypersensitivity to any of the ingredients.
Special Precautions for Use: Xclair Cream contains a nut oil, and patients with a knownallergy to nuts or nut oils should consult their physician before using this topical preparation.
Warning: Federal law restricts Xclair Cream to sale by, or on the order of, a physician orproperly licensed practitioner.
Interactions: There are no known interactions between Xclair Cream and any medicinal orother products.
Directions for Use: Apply Xclair Cream to the affected skin area 3 times per day (or as needed),and massage gently into the skin. If the skin is broken, cover the affected area with a steriledressing after application of Xclair Cream.
Storage: Store at room temperature. KEEP OUT OF REACH OF CHILDREN.
Manufactured in Italy under license from Sinclair Pharmaceuticals Ltd., Godalming, Surrey GU7 1XW UK. Distributed by ALIGN Pharmaceuticals, LLC, Berkeley Heights, NJ 07922 USA www.alignpharma.com
1.Primavera G., et al.A double-blind, vehicle-controlled clinical study to evaluate the efficacy of MAS065D (Xclair), a hyaluronic acid-based formulation, in the management of radiation-induced dermatitis. Cutaneous and Ocular Toxicology, 25: 1–7, 2006.
©2011 ALIGN Pharmaceuticals, LLC All rights reserved.
ALIGN PharmaceuticalsProviding Supportive Care Solutions for Your PatientsXclair®Cream, the preferred treatment option for radiationdermatitis by both physicians and patients.1
Numoisyn® Liquid and Numoisyn®Lozenges,for dry mouth relief with less side effects.
www.alignpharma.com Customer Service: 908-834-0960All three ALIGN Pharmaceuticals products are FDA approved prescription products andare available at your major wholesalers. For Direct Purchases, please call 866-231-5020.
A TON_April2011_v7_TON 4/7/11 1:59 PM Page 21

Investigators of a phase 2 study com-paring 2 dosing schedules of suni-tinib (Sutent) as first-line therapy
for patients with advanced renal cellcarcinoma (RCC) concluded that clini-cians should stay with the currentlyapproved dosing regimen of 50 mg dailyfor 4 weeks followed by a 2-week break.Robert Motzer, MD, attending physi-cian, Memorial Sloan-Kettering CancerCenter, New York, who presented the
findings, said the data add to a growingbody of evidence favoring the dosingregimen that the US Food and DrugAdministration approved for sunitinib.
From January 2007 to June 2008,Motzer and colleagues recruited 292patients (median age, 62 years) withlocally recurrent or metastatic RCC ofclear cell histology to participate in thephase 2 Renal EFFECT trial. Patientswere assigned randomly to receive the
conventional 50-mg dose, 4 weeks on/2-weeks off (4/2) regimen of sunitinib ora 37.5-mg continuous daily dose (CDD).Treatment continued for up to 2 years,with patients who experienced diseaseprogression or unacceptable toxicity dis-continuing earlier. The study’s primaryend point was time to tumor progression(TTP), with secondary end points ofoverall response rate (ORR), overall sur-vival (OS), time to deterioration, andadverse events.
Patients in the 4/2 group received amedian of 5 months of treatment com-pared with 6 months in the CDD arm.On the primary end point of TTP,Motzer said, “There wasn’t a statistical-ly significant difference be tween the 2 arms, but there was a strong trendfavoring the 4/2 schedule over contin-uous dosing.”
Median TTP was 9.9 months forpatients treated with the 4/2 regimencompared with 7.1 months for thoseassigned to the CDD schedule (hazardratio, 0.77; 95% confidence interval,0.57-1.04; P = .090). ORR and OSwere similar between the study arms.ORR in the 4/2 arm was 32.2% versus28.1% in the CDD group (P = .044) andOS reached a median of 23.1 months inthe 4/2 group compared with 23.5months in the CDD arm. Time to deteri-oration and death were significantlyimproved with the 4/2 schedule versusthe CDD regimen (4.0 months vs 2.9months; P = .034).
No statistically significant differencewas observed between the groups inthe proportion of patients experienc-ing all-grade or grade 3/4 adverseevents (P >.05). The most commondrug-related adverse events overallwere fatigue, nausea, diarrhea, dysgeu-sia, and vomiting (Figure). Hand-footsyndrome was the most frequent grade3/4 adverse event, observed in 10% ofpatients in each arm.
Motzer told The Oncology Nurse-APN/PA that patient-reported out-comes suggested the regimens had anequal effect on quality of life and kid-ney cancer symptoms, but patients onthe 4/2 schedule reported better quali-ty of life during the 2 weeks off thera-py. “I think this is important in coun-seling patients on the 4/2 schedule,”Motzer said.
Although previous studies compar-ing these regimens have found themequally active, Motzer said those stud-ies generally excluded patients with apoor performance score. This studyallowed patients with a Karnofsky per-formance score as low as 70% andenrolled fewer patients (~80%) whohad a nephrectomy. Based on thesedata, Motzer concluded, “The treat-ment goal, therefore, should be toadhere to the approved dose andschedule.”
Motzer disclosed that funding for thestudy was provided by Pfizer and he hasreceived compensation from Pfizer. �
www.TheOncologyNurse.com22 March/april 2011 I VOl 4, NO 2
Conference News
70
60
50
40
30
20
10
0
62 62
56
49
56
38
34 34 34
Fatigue Nausea Diarrhea Dysgeusia Vomiting
Adverse Event
Patients, %
4/2 indicates 50 mg daily for 4 weeks followed by a 2-week break; CDD, 37.5-mg continuous daily dosing.
4/2
CDD
©ASCO/Todd Buchanan 2011.
The following articles are based on presentations at the 2011 Genitourinary CancersSymposium held February 17-19, 2011, in Orlando, Florida.
Approved Sunitinib Dosing ScheduleRecommended for Patients withMetastatic Renal Cell CarcinomaBy John Schieszer
Figure. Rate of Adverse Events
Interim results of a randomized, con-trolled, phase 3 trial showed that abi-raterone acetate significantly pro-
longed overall survival (OS) in patientswith metastatic castration-resistantprostate cancer (CRPC) who progressedafter docetaxel-based chemotherapy.The survival benefit was consistentacross all prespecified subgroups. Leadauthor Howard Scher, MD, MemorialSloan-Kettering Cancer Center, NewYork, said abiraterone is poised tobecome a new standard of care.
The study enrolled 1200 patientswith metastatic CRPC who failed on
docetaxel and ≤1 additional chemo -therapy regimen. Patients were ran-domized to abiraterone and prednisoneor prednisone and placebo. Groupswere well balanced for demographicand disease characteristics.
Patients on abiraterone achieved sig-nificantly superior median OS versusplacebo (14.8 months vs 10.9 months; P <.001), representing a 35% reductionin the relative risk of mortality. Pre -planned analyses found survival benefitconsistent across all subgroups, regardlessof prior chemotherapy lines, perform-ance status, pain scores, and radiograph-
ic progression-free survival. The abi-raterone group also had higher rates oftotal and confirmed responses accordingto prostate-specific antigen (PSA) test-ing. Rates of overall and serious adverseevents were similar between both groupsand considered manageable.
Oliver Sartor, MD, Tulane UniversitySchool of Medicine, New Orleans,Louisiana, moderated the prostate can-cer session. “This is a game-changer. Tome this will change practice,” he said.
Positive 42-month data were also pre-sented for MDV3100, a novel, triple-acting, oral androgen-receptor antago-nist for CRPC. In a phase 1/2 study,MDV3100 demonstrated durable anti- tumor activity, based on median times toPSA and radiographic progression.
Higano and associates enrolled 140men with progressive disease resistant tostandard antiandrogen treatments, suchas bicalutamide. As of the meeting, 18men remained on active treatment.Median time to PSA progression was 316days in the postchemotherapy group andnot yet reached in the chemotherapy-naïve cohort. Median time to radio -graphic progression was 392 days versus175 days, respectively. Circulating tumorcell counts remained favorable for 91%of patients with favorable counts at base-line, and counts for 15 patients wentfrom unfavorable to favorable.
MDV3100 is currently being studiedin the randomized phase 3 AFFIRM andPREVAIL trials. Both trials are activelyrecruiting patients. �
Novel Drugs in Prostate CancerBy Alice Goodman
TON_April2011_v7_TON 4/7/11 10:49 AM Page 22

Some men with prostate cancer whoundergo external beam radiothera-py (EBRT), interstitial brachyther-
apy, or radical prostatectomy show evi-dence of toxicity for at least a decadeafter the procedure. Grant Hunter, MD,a third-year urology resident at theCleveland Clinic in Ohio, led the retro-spective study and presented findings atthe meeting. He said all 3 modalitiesresulted in gastrointestinal (GI) and/orgenitourinary (GU) toxicities up to 10years later, with the most severe profilesobserved in patients with diabetes melli-tus (Table). “The findings from this studyshould be of special interest to oncologynurses,” said Hunter, who noted thatmany clinicians might not be aware ofthe potential for late-term effects relatedto these therapies. Hunter and colleagues reviewed
records for 483 patients who receivedEBRT (36%), interstitial brachytherapy(24%), or radical prostatectomy (40%)for prostate cancer in 1999. They exam-ined the incidences of late GI and GUtreatment-related adverse effects duringa mean follow-up of 8.6 years (range, 0.2-11.5 years) and graded their severity
according to the Radiation TherapyOncology Group scoring criteria foracute and late effects. Other factorsweighed in the analyses include patient’sage; body mass index; smoking history;and medical comorbidities, such as dia-betes mellitus, peripheral vascular dis-ease, and connective tissue disease. The rates of late GI and GU toxici-
ties were low, which Hunter said wasreassuring. A competing risk regressionanalysis found that patients whounderwent EBRT were most likely toexperience GU toxicities ≥grade 2 in10 years of follow-up and patients whoreceived brachytherapy were least like-ly (11.2% vs 4.3%, respectively). Inthe 10 years after radical prostatecto-
my, 5.5% of patients had GU toxicities≥grade 2. The risk of GU toxicity≥grade 2 was 2.35-fold greater for menwith diabetes at treatment outset thanmen who did not have diabetes whenbeginning therapy (P = .043).Nobody in the radical prostatectomy
group experienced late GI toxicity≥grade 2, but the 10-year cumulative ratewas 1.7 for patients in the brachytherapyarm and 7.8% for the EBRT group.According to Hunter, EBRT (P = .038)and diabetes (P = .008) were the onlyindependent variables found to signifi-cantly increase patients’ risk of late GItoxicity of ≥grade 2. “This is the first study of this kind
to look at all 3 treatment modalities
in patients treated for prostate can-cer,” said Hunter in an interview withThe Oncology Nurse-APN/PA. “Wethought this was something to look atbecause patients treated for prostatecancer tend to live a very long timeand so the potential toxicity profilesare relevant.”Hunter said it is important for
oncology nursing professionals to becognizant of the possibility for patientstreated 7 or 8 years ago to experiencelate GI and GU toxicity. Thesepatients have a “need for follow-up andneed for care because of toxicity issuesthat are late, especially in patients whohave diabetes when they undergotreatment,” he said.—JS �
www.TheOncologyNurse.com March/april 2011 I VOl 4, NO 2 23
Conference News
Adding androgen-deprivation ther- apy (ADT) to dose-escalatedexternal beam radiotherapy
(EBRT) for men with intermediate-riskprostate cancer improves biochemicalfailure-free survival but not overall sur-vival (OS), according to a retrospectivestudy. Researchers from Emory Uni -versity School of Medicine and theAtlanta Veterans Administration inGeorgia conducted the study. Althoughprevious trials have found that combin-ing ADT with EBRT improves biochem-ical failure-free survival and OS in menwith high-risk prostate cancer, the dualtherapy has never been thoroughlyinvestigated in men with intermediate-risk disease.Using a database of 850 men treated at
multiple institutions, investigators iden-tified 251 with intermediate-risk prostatecancer, which they defined as stage ≥T2bdisease or a prostate-specific antigen(PSA) level >10 ng/mL or a Gleasonscore (GS) of 7. Patients meeting any ofthe following criteria were excluded:stage ≥T3 disease, PSA level >20 ng/mL,GS ≥8, positive nodes, or distant metas-tases. All patients in the study hadreceived EBRT to a dose ≥70 Gy but
none had undergone brachytherapy orprostatectomy; 87 were given ADT. Mean PSA score was higher for men
in the ADT group than for those in theEBRT-only arm (12.0 ng/mL vs 8.9ng/mL, respectively), and more men inthe ADT group than the EBRT-only armunderwent pelvic radiography (49% vs22%, respectively). The study arms werewell balanced in terms of age, race, mean
EBRT dose, and the proportion ofpatients who had intensity-modulatedradiation therapy (IMRT). Median fol-low-up was 47 months.The 5-year rate of biochemical failure-
free survival was 80% for the ADT groupcompared with 76% for the EBRT-onlygroup (P = .017). At 5 years, 84% ofpatients in the ADT group were alive
compared with 76% of patients not givenADT (P = .028). Multi variate analysesfound that ADT use and GS were theonly significant independent predictorsof biochemical failure-free survival andthat PSA level and IMRT were the onlysignificant independent predictors of OS.Adding ADT to EBRT did not increasethe incidence or severity of gastrointesti-nal and genitourinary toxicities.
In an interview with The OncologyNurse-APN/PA, lead investigator ScottEdelman, MD, assistant professor ofradiation oncology at Emory Uni -versity, said although the data supportnurses counseling their patients withintermediate-risk prostate cancer that“if you take hormonal therapy [for 6months], there is a really good chance
that 3 or 4 years down the road, yourPSA will be under control,” it is prema-ture to suggest adding ADT improvessurvival. Edelman said the findingsmight reassure some men contemplatingit, but they need to know about the sig-nificant side effects associated with thetherapy before deciding on treatment.“Hormonal therapy gives you hot
flashes and breast tenderness. It maygive you a little breast enlargementand may make you more emotional. Italso may take away your sex drive inthe short term and give you problemswith erections, and increase your riskfor osteoporosis and bone fractures,” heexplained. Edelman said it comes down to what
matters most to the patient. “If thepatient is someone who wants a cure—based on his PSA level—and that isthe most important thing for him, thenhe should go on hormonal therapy.However, if quality of life is the mostimportant issue, then it would probablybe best to tell them not to go on hor-monal therapy.” A randomized trial iscurrently investigating combinationtherapy in men with intermediate-riskprostate cancer.—JS �
Prostate Cancer Therapies Cause Toxicities Up to 10 Years Later
ADT for Intermediate-Risk Prostate Cancer Does Not Appear to Improve Overall Survival
Table Cumulative Rates of GI and GU Effects 5 and 10 Years After Therapy
ModalityGI Toxicity ≥Grade 2, % GU Toxicity ≥Grade 2, %
5 Years 10 Years 5 Years 10 Years
EBRT 7.8 7.8 8.6 11.2
Brachytherapy 1.7 1.7 4.3 4.3
Prostatectomy 0 0 3.1 5.5
EBRT indicates external beam radiotherapy; GI, gastrointestinal; GU, genitourinary.Source: Hunter G, et al. J Clin Oncol. 2011;29(suppl 17):65.
Edelman said the findings might reassure some mencontemplating ADT, but they need to know about thesignificant side effects associated with the therapybefore deciding on treatment.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 23

Adjuvant indicationsHerceptin is indicated for adjuvant treatment of HER2-overexpressing node-positive or node-negative (ER/PR-negative or with one high-risk feature*) breast cancer: As part of a treatment regimen containing doxorubicin, cyclophosphamide, and either
paclitaxel or docetaxel With docetaxel and carboplatin As a single agent following multi-modality anthracycline-based therapy
* High-risk is defi ned as ER/PR positive with one of the following features:tumor size >2 cm, age <35 years, or tumor grade 2 or 3.
Please see brief summary of full Prescribing Information, including Boxed WARNINGS and additional important safety information, on the following pages.
to drive outcomes in HER2+ adjuvant breast cancer
This is not an actual Herceptin patient.
S
E
H
E
E D
T
1
to drive outcomes in HER2+
TON_April2011_v7_TON 4/7/11 10:49 AM Page 24

A
©2010 Genentech USA, Inc. So. San Francisco, CA All rights reserved. 10606700 11/10
References: 1. Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353:1673-1684 and supplementary appendix. 2. Herceptin Prescribing Information. Genentech, Inc. October 29, 2010. 3. Data on fi le. Genentech, Inc. 4. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-1672.
T
Clinical Benefi t of 1 Year of Herceptin
Study Control Arm Herceptin Arm Reduction in Relative Risk of Recurrence†
Joint Analysisof NCCTG N9831and NSABP B-31
AC T(n=1880)
AC TH(n=1872) 52%
HR=0.48 (95% CI: 0.39-0.59), P≤0.0001
HERA‡ Observation only(n=1693)
Herceptin 1 year(n=1693) 46%
HR=0.54 (95% CI: 0.44-0.67), P≤0.0001
BCIRG 006 AC T(n=1073)
TCH(n=1075) 33%
HR=0.67 (95% CI: 0.54-0.84), P=0.0006
AC TH(n=1074) 40%
HR=0.60 (95% CI: 0.48-0.76), P≤0.0001
Boxed WARNINGS and Additional Important Safety Information Herceptin administration can result in sub-clinical and clinical cardiac failure. The incidence and
severity was highest in patients receiving Herceptin with anthracycline-containing chemotherapy regimens. In a pivotal adjuvant trial, one patient who developed CHF died of cardiomyopathy
Evaluate cardiac function prior to and during treatment. For adjuvant therapy, also evaluate cardiac function after completion of Herceptin. Discontinue Herceptin for cardiomyopathy
Herceptin can result in serious and fatal infusion reactions and pulmonary toxicity. Discontinue Herceptin for anaphylaxis, angioedema, interstitial pneumonitis, or acute respiratory distress syndrome
Exposure to Herceptin during pregnancy can result in oligohydramnios, in some cases complicated by pulmonary hypoplasia and neonatal death
Exacerbation of chemotherapy-induced neutropenia has also occurred Detection of HER2 protein overexpression is necessary for selection of patients appropriate for
Herceptin therapy The most common adverse reactions associated with Herceptin use were fever, nausea, vomiting,
infusion reactions, diarrhea, infections, increased cough, headache, fatigue, dyspnea, rash, neutropenia, anemia, and myalgia
1 year of Herceptin plus standard adjuvant therapy signifi cantly reduced the risk of disease recurrence1-4
Four pivotal trials involving more than 10,000 women demonstrated that 1 year of Herceptin therapy provided signifi cant clinical benefi t1-4
AC=anthracycline (doxorubicin) plus cyclophosphamide.T=Taxotere® (docetaxel) (in BCIRG 006) or paclitaxel (in the Joint Analysis).C=carboplatin (in the TCH regimen).H=Herceptin.Taxotere is a registered trademark of sanofi -aventis U.S. LLC.†Recurrence was defi ned as any clinical or radiologic evidence of tumor recurrence.‡ Patients were randomized upon completion of chemotherapy, surgery, and radiotherapy (if appropriate).
1-2 3 4:00 PM
TON_April2011_v7_TON 4/7/11 10:49 AM Page 25

HERCEPTIN® (trastuzumab)Brief Summary For full Prescribing Information, see package insert.
WARNING: CARDIOMYOPATHY, INFUSION REACTIONS, EMBRYO-FETAL TOXICITY, and PULMONARY TOXICITY Cardiomyopathy Herceptin administration can result in sub clinical and clinical cardiac failure. The incidence and severity was highest in patients receiving Herceptin with anthracycline containing chemotherapy regimens. Evaluate left ventricular function in all patients prior to and during treatment with Herceptin. Discontinue Herceptin treatment in patients receiving adjuvant therapy and withhold Herceptin in patients with metastatic disease for clinically significant decrease in left ventricular function. [see Warnings and Precautions and Dosage and Administration]Infusion Reactions; Pulmonary Toxicity Herceptin administration can result in serious and fatal infusion reactions and pulmonary toxicity. Symptoms usually occur during or within 24 hours of Herceptin administration. Interrupt Herceptin infusion for dyspnea or clinically significant hypotension. Monitor patients until symptoms completely resolve. Discontinue Herceptin for anaphylaxis, angioedema, interstitial pneumonitis, or acute respiratory distress syndrome. [see Warnings and Precautions] Embryo-Fetal Toxicity Exposure to Herceptin during pregnancy can result in oligohydramnios and oligohydramnios sequence manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. [see Warnings and Precautions, Use in Specific Populations]
INDICATIONS AND USAGE Adjuvant Breast Cancer Herceptin is indicated for adjuvant treatment of HER2 overexpressing node positive or node negative (ER/PR negative or with one high risk feature [see Clinical Studies] breast cancer • as part of a treatment regimen consisting of doxorubicin, cyclophosphamide, and either paclitaxel or docetaxel • with docetaxel and carboplatin • as a single agent following multi-modality anthracycline based therapy. Metastatic Breast Cancer Herceptin is indicated: • In combination with paclitaxel for first-line treatment of HER2-overexpressing metastatic breast cancer • As a single agent for treatment of HER2-overexpressing breast cancer in patients who have received one or more chemotherapy regimens for metastatic disease. Metastatic Gastric Cancer Herceptin is indicated, in combination with cisplatin and capecitabine or 5-fluorouracil, for the treatment of patients with HER2 overexpressing metastatic gastric or gastroesophageal junction adenocarcinoma, who have not received prior treatment for metastatic disease. CONTRAINDICATIONS None. WARNINGS AND PRECAUTIONS Cardiomyopathy Herceptin can cause left ventricular cardiac dysfunction, arrhythmias, hypertension, disabling cardiac failure, cardiomyopathy, and cardiac death [see Boxed Warning: Cardiomyopathy]. Herceptin can also cause asymptomatic decline in left ventricular ejection fraction (LVEF). There is a 4−6 fold increase in the incidence of symptomatic myocardial dysfunction among patients receiving Herceptin as a single agent or in combination therapy compared with those not receiving Herceptin. The highest absolute incidence occurs when Herceptin is administered with an anthracycline. Withhold Herceptin for 16% absolute decrease in LVEF from pre-treatment values or an LVEF value below institutional limits of normal and 10% absolute decrease in LVEF from pretreatment values [see Dosage and Administration]. The safety of continuation or resumption of Herceptin in patients with Herceptin-induced left ventricular cardiac dysfunction has not been studied. Cardiac Monitoring Conduct thorough cardiac assessment, including history, physical examination, and determination of LVEF by echocardiogram or MUGA scan. The following schedule is recommended: • Baseline LVEF measurement immediately prior to initiation of Herceptin • LVEF measurements every 3 months during and upon completion of Herceptin • Repeat LVEF measurement at 4 week intervals if Herceptin is withheld for significant left ventricular cardiac dysfunction [see Dosage and Administration] • LVEF measurements every 6 months for at least 2 years following completion of Herceptin as a component of adjuvant therapy. In Study 1, 16% (136/844) of patients discontinued Herceptin due to clinical evidence of myocardial dysfunction or significant decline in LVEF. In Study 3, the number of patients who discontinued Herceptin due to cardiac toxicity was 2.6% (44/1678). In Study 4, a total of 2.9% (31/1056) patients in the TCH arm (1.5% during the chemotherapy phase and 1.4% during the monotherapy phase) and 5.7% (61/1068) patients in the AC-TH arm (1.5% during the chemotherapy phase and 4.2% during the monotherapy phase) discontinued Herceptin due to cardiac toxicity. Among 32 patients receiving adjuvant chemotherapy (Studies 1 and 2) who developed congestive heart failure, one patient died of cardiomyopathy and all other patients were receiving cardiac medication at last follow-up. Approximately half of the surviving patients had recovery to a normal LVEF (defined as 50%) on continuing medical management at the time of last follow-up. Incidence of congestive heart failure is presented in Table 1. The safety of continuation or resumption of Herceptin in patients with Herceptin-induced left ventricular cardiac dysfunction has not been studied.Table 1 Incidence of Congestive Heart Failure in Adjuvant Breast Cancer Studies
Incidence of CHF Study Regimen Herceptin Control 1 & 2a ACb Paclitaxel+ Herceptin 2% (32/1677) 0.4% (7/1600) 3 Chemo Herceptin 2% (30/1678) 0.3% (5/1708) 4 ACb Docetaxel+ Herceptin 2% (20/1068) 0.3% (3/1050) 4 Docetaxel+Carbo+ Herceptin 0.4% (4/1056) 0.3% (3/1050)a Includes 1 patient with fatal cardiomyopathy.b Anthracycline (doxorubicin) and cyclophosphamide
Table 2 Incidence of Cardiac Dysfunctiona in Metastatic Breast Cancer Studies
Incidence NYHA I−IV NYHA III−IV Study Event Herceptin Control Herceptin Control 5 Cardiac (AC)b Dysfunction 28% 7% 19% 3% 5 Cardiac (paclitaxel) Dysfunction 11% 1% 4% 1% 6 Cardiac Dysfunctionc 7% N/A 5% N/Aa Congestive heart failure or significant asymptomatic
decrease in LVEF.b Anthracycline (doxorubicin or epirubicin) and
cyclophosphamide.c Includes 1 patient with fatal cardiomyopathy.In Study 4, the incidence of NCI-CTC Grade 3/4 cardiac ischemia/infarction was higher in the Herceptin containing regimens: (AC-TH: 0.3% (3/1068) and TCH 0.2% (2/1056)) as compared to none in AC-T. Infusion Reactions Infusion reactions consist of a symptom complex characterized by fever and chills, and on occasion included nausea, vomiting, pain (in some cases at tumor sites), headache, dizziness, dyspnea, hypotension, rash, and asthenia. [see Adverse Reactions] In postmarketing reports, serious and fatal infusion reactions have been reported. Severe reactions which include bronchospasm, anaphylaxis, angioedema, hypoxia, and severe hypotension, were usually reported during or immediately following the initial infusion. However, the onset and clinical course were variable including progressive worsening, initial improvement followed by clinical deterioration, or delayed post-infusion events with rapid clinical deterioration. For fatal events, death occurred within hours to days following a serious infusion reaction. Interrupt Herceptin infusion in all patients experiencing dyspnea, clinically significant hypotension, and intervention of medical therapy administered, which may include: epinephrine, corticosteroids, diphenhydramine, bronchodilators, and oxygen. Patients should be evaluated and carefully monitored until complete resolution of signs and symptoms. Permanent discontinuation should be strongly considered in all patients with severe infusion reactions. There are no data regarding the most appropriate method of identification of patients who may safely be retreated with Herceptin after experiencing a severe infusion reaction. Prior to resumption of Herceptin infusion, the majority of patients who experienced a severe infusion reaction were pre-medicated with antihistamines and/or corticosteroids. While some patients tolerated Herceptin infusions, others had recurrent severe infusion reactions despite pre-medications. Embryo-Fetal Toxicity Herceptin can cause fetal harm when administered to a pregnant woman. In post-marketing reports, use of Herceptin during pregnancy resulted in cases of oligohydramnios and oligohydramnios sequence manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. Advise women of the potential hazard to the fetus resulting from Herceptin exposure during pregnancy and provide contraception counseling to women of childbearing potential. [see Use in Specific Populations, Patient Counseling Information]. Pulmonary Toxicity Herceptin use can result in serious and fatal pulmonary toxicity. Pulmonary toxicity includes dyspnea, interstitial pneumonitis, pulmonary infiltrates, pleural effusions, non-cardiogenic pulmonary edema, pulmonary insufficiency and hypoxia, acute respiratory distress syndrome, and pulmonary fibrosis. Such events can occur as sequelae of infusion reactions [see Warnings and Precautions]. Patients with symptomatic intrinsic lung disease or with extensive tumor involvement of the lungs, resulting in dyspnea at rest, appear to have more severe toxicity. Exacerbation of Chemotherapy-Induced Neutropenia In randomized, controlled clinical trials the per-patient incidences of NCI CTC Grade 3−4 neutropenia and of febrile neutropenia were higher in patients receiving Herceptin in combination with myelosuppressive chemotherapy as compared to those who received chemotherapy alone. The incidence of septic death was similar among patients who received Herceptin and those who did not. [see Adverse Reactions] HER2 Testing Detection of HER2 protein overexpression is necessary for selection of patients appropriate for Herceptin therapy because these are the only patients studied and for whom benefit has been shown. Due to differences in tumor histopathology, use FDA-approved tests for the specific tumor type (breast or gastric/gastroesophageal adenocarcinoma) to assess HER2 protein overexpression and HER2 gene amplification. Tests should be performed by laboratories with demonstrated proficiency in the specific technology being utilized. Improper assay performance, including use of suboptimally fixed tissue, failure to utilize specified reagents, deviation from specific assay instructions, and failure to include appropriate controls for assay validation, can lead to unreliable results. Several FDA-approved commercial assays are available to aid in the selection of breast cancer and metastatic gastric cancer patients for Herceptin therapy. Users should refer to the package inserts of specific assay kits for information on the Intended Use, and the validation and performance of each assay. Limitations in assay precision make it inadvisable to rely on a single method to rule out potential Herceptin benefit. Treatment outcomes for adjuvant breast cancer (Studies 2 and 3) and for metastatic breast cancer (Study 5) as a function of IHC and FISH testing are provided in Tables 8 and 10. Assessment of HER2 protein overexpression and HER2 gene amplification in metastatic gastric cancer should be performed using FDA-approved tests specifically for gastric cancers due to differences in gastric vs. breast histopathology, including incomplete membrane staining and more frequent heterogeneous expression of HER2 seen in gastric cancers. Study 7 demonstrated that gene amplification and protein overexpression were not as well correlated as with breast cancer. Treatment outcomes for metastatic gastric cancer (Study 7), based on HER2 gene amplification (FISH) and HER2 protein overexpression (IHC) test results are provided in Table 12. ADVERSE REACTIONS The following adverse reactions are discussed in greater detail in other sections of the label: • Cardiomyopathy [see Warnings and Precautions] • Infusion reactions [see Warnings and
Precautions] • Embryo-fetal Toxicity [see Warnings and Precautions] • Pulmonary toxicity [see Warnings and Precautions] • Exacerbation of chemotherapy-induced neutropenia [see Warnings and Precautions] The most common adverse reactions in patients receiving Herceptin in the adjuvant and metastatic breast cancer setting are fever, nausea, vomiting, infusion reactions, diarrhea, infections, increased cough, headache, fatigue, dyspnea, rash, neutropenia, anemia, and myalgia. Adverse reactions requiring interruption or discontinuation of Herceptin treatment include CHF, significant decline in left ventricular cardiac function, severe infusion reactions, and pulmonary toxicity [see Dosage and Administration]. In the metastatic gastric cancer setting, the most common adverse reactions ( 10%) that were increased ( 5% difference) in the Herceptin arm as compared to the chemotherapy alone arm were neutropenia, diarrhea, fatigue, anemia, stomatitis, weight loss, upper respiratory tract infections, fever, thrombocytopenia, mucosal inflammation, nasopharyngitis, and dysgeusia. The most common adverse reactions which resulted in discontinuation of treatment on the Herceptin-containing arm in the absence of disease progression were infection, diarrhea, and febrile neutropenia. Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. Adjuvant Breast Cancer Studies The data below reflect exposure to Herceptin across three randomized, open-label studies, Studies 1, 2, and 3, with (n= 3355) or without (n= 3308) trastuzumab in the adjuvant treatment of breast cancer. The data summarized in Table 3 below, from Study 3, reflect exposure to Herceptin in 1678 patients; the median treatment duration was 51 weeks and median number of infusions was 18. Among the 3386 patients enrolled in Study 3, the median age was 49 years (range: 21 to 80 years), 83% of patients were Caucasian, and 13% were Asian.Table 3 Adverse Reactions for Study 3, All Gradesa:
1 Year Herceptin Observation Adverse Reaction (n= 1678) (n=1708)
CardiacHypertension 64 (4%) 35 (2%)Dizziness 60 (4%) 29 (2%)Ejection Fraction Decreased 58 (3.5%) 11 (0.6%)Palpitations 48 (3%) 12 (0.7%)Cardiac Arrhythmiasb 40 (3%) 17 (1%)Cardiac Failure Congestive 30 (2%) 5 (0.3%)Cardiac Failure 9 (0.5%) 4 (0.2%)Cardiac Disorder 5 (0.3%) 0 (0%)Ventricular Dysfunction 4 (0.2%) 0 (0%)Respiratory Thoracic Mediastinal DisordersCough 81 (5%) 34 (2%)Influenza 70 (4%) 9 (0.5%)Dyspnea 57 (3%) 26 (2%)URI 46 (3%) 20 (1%)Rhinitis 36 (2%) 6 (0.4%)Pharyngolaryngeal Pain 32 (2%) 8 (0.5%)Sinusitis 26 (2%) 5 (0.3%)Epistaxis 25 (2%) 1 (0.06%)Pulmonary Hypertension 4 (0.2%) 0 (0%)Interstitial Pneumonitis 4 (0.2%) 0 (0%)Gastrointestinal DisordersDiarrhea 123 (7%) 16 (1%)Nausea 108 (6%) 19 (1%)Vomiting 58 (3.5%) 10 (0.6%)Constipation 33 (2%) 17 (1%)Dyspepsia 30 (2%) 9 (0.5%)Upper Abdominal Pain 29 (2%) 15 (1%)Musculoskeletal & Connective Tissue DisordersArthralgia 137 (8%) 98 (6%)Back Pain 91 (5%) 58 (3%)Myalgia 63 (4%) 17 (1%)Bone Pain 49 (3%) 26 (2%)Muscle Spasm 46 (3%) 3 (0.2%)Nervous System DisordersHeadache 162 (10%) 49 (3%)Paraesthesia 29 (2%) 11 (0.6%)Skin & Subcutaneous Tissue DisordersRash 70 (4%) 10 (0.6%)Nail Disorders 43 (2%) 0 (0%)Pruritis 40 (2%) 10 (0.6%)General DisordersPyrexia 100 (6%) 6 (0.4%)Edema Peripheral 79 (5%) 37 (2%)Chills 85 (5%) 0 (0%)Aesthenia 75 (4.5%) 30 (2%)Influenza-like Illness 40 (2%) 3 (0.2%)Sudden Death 1 (0.06%) 0 (0%)InfectionsNasopharyngitis 135 (8%) 43 (3%)UTI 39 (3%) 13 (0.8%)Immune System DisordersHypersensitivity 10 (0.6%) 1 (0.06%)Autoimmune Thyroiditis 4 (0.3%) 0 (0%)
a The incidence of Grade 3/4 adverse reactions was <1% in both arms for each listed term.
b Higher level grouping term.The data from Studies 1 and 2 were obtained from 3206 patients, of whom 1635 received Herceptin; the median treatment duration was 50 weeks. The median age was 49 years (range: 24−80); 84% of patients were White, 7% Black, 4% Hispanic, and 4% Asian. In Study 1, only Grade 3−5 adverse events, treatment-related Grade 2 events, and Grade 2−5 dyspnea were collected during and for up to 3 months following protocol-specified treatment. The following non-cardiac adverse reactions of Grade 2−5 occurred at an incidence of at least 2% greater among patients randomized to Herceptin plus chemotherapy as compared to chemotherapy alone: arthralgia (31% vs. 28%), fatigue (28% vs. 22%), infection (22% vs. 14%), hot flashes (17% vs. 15%), anemia (13% vs. 7%), dyspnea (12% vs. 4%), rash/desquamation (11% vs. 7%), neutropenia (7% vs. 5%), headache (6% vs. 4%), and insomnia (3.7% vs. 1.5%). The majority of these events were Grade
2 in severity. In Study 2, data collection was limited to the following investigator-attributed treatment-related adverse reactions: NCI-CTC Grade 4 and 5 hematologic toxicities, Grade 3−5 non-hematologic toxicities, selected Grade 2−5 toxicities associated with taxanes (myalgia, arthralgias, nail changes, motor neuropathy, sensory neuropathy) and Grade 1−5 cardiac toxicities occurring during chemotherapy and/or Herceptin treatment. The following non-cardiac adverse reactions of Grade 2−5 occurred at an incidence of at least 2% greater among patients randomized to Herceptin plus chemotherapy as compared to chemotherapy alone: arthralgia (11% vs. 8.4%), myalgia (10% vs. 8%), nail changes (9% vs. 7%), and dyspnea (2.5% vs. 0.1%). The majority of these events were Grade 2 in severity. Safety data from Study 4 reflect exposure to Herceptin as part of an adjuvant treatment regimen from 2124 patients receiving at least one dose of study treatment [AC-TH: n = 1068; TCH: n = 1056]. The overall median treatment duration was 54 weeks in both the AC-TH and TCH arms. The median number of infusions was 26 in the AC-TH arm and 30 in the TCH arm, including weekly infusions during the chemotherapy phase and every three week dosing in the monotherapy period. Among these patients, the median age was 49 years (range 22 to 74 years). In Study 4, the toxicity profile was similar to that reported in Studies 1, 2, and 3 with the exception of a low incidence of CHF in the TCH arm. Metastatic Breast Cancer Studies The data below reflect exposure to Herceptin in one randomized, open-label study, Study 5, of chemotherapy with (n=235) or without (n=234) trastuzumab in patients with metastatic breast cancer, and one single-arm study (Study 6; n=222) in patients with metastatic breast cancer. Data in Table 4 are based on Studies 5 and 6. Among the 464 patients treated in Study 5, the median age was 52 years (range: 25−77 years). Eighty-nine percent were White, 5% Black, 1% Asian and 5% other racial/ethnic groups. All patients received 4 mg/kg initial dose of Herceptin followed by 2 mg/kg weekly. The percentages of patients who received Herceptin treatment for 6 months and 12 months were 58% and 9%, respectively. Among the 352 patients treated in single agent studies (213 patients from Study 6), the median age was 50 years (range 28−86 years), 86% were White, 3% were Black, 3% were Asian, and 8% in other racial/ethnic groups. Most of the patients received 4 mg/kg initial dose of Herceptin followed by 2 mg/kg weekly. The percentages of patients who received Herceptin treatment for 6 months and
12 months were 31% and 16%, respectively.Table 4 Per-Patient Incidence of Adverse Reactions Occurring in 5% of Patients in Uncontrolled Studies or at Increased Incidence in the Herceptin Arm (Studies 5 and 6)
Herceptin Single + Paclitaxel Herceptin ACb
Agenta Paclitaxel Alone + ACb Alone n = 352 n = 91 n = 95 n = 143 n = 135Body as a Whole Pain 47% 61% 62% 57% 42% Asthenia 42% 62% 57% 54% 55% Fever 36% 49% 23% 56% 34% Chills 32% 41% 4% 35% 11% Headache 26% 36% 28% 44% 31% Abdominal pain 22% 34% 22% 23% 18% Back pain 22% 34% 30% 27% 15% Infection 20% 47% 27% 47% 31% Flu syndrome 10% 12% 5% 12% 6% Accidental injury 6% 13% 3% 9% 4% Allergic reaction 3% 8% 2% 4% 2%Cardiovascular Tachycardia 5% 12% 4% 10% 5% Congestive 7% 11% 1% 28% 7% heart failureDigestive Nausea 33% 51% 9% 76% 77% Diarrhea 25% 45% 29% 45% 26% Vomiting 23% 37% 28% 53% 49% Nausea and vomiting 8% 14% 11% 18% 9% Anorexia 14% 24% 16% 31% 26% Heme & Lymphatic Anemia 4% 14% 9% 36% 26% Leukopenia 3% 24% 17% 52% 34%Metabolic Peripheral edema 10% 22% 20% 20% 17% Edema 8% 10% 8% 11% 5%Musculoskeletal Bone pain 7% 24% 18% 7% 7% Arthralgia 6% 37% 21% 8% 9%Nervous Insomnia 14% 25% 13% 29% 15% Dizziness 13% 22% 24% 24% 18% Paresthesia 9% 48% 39% 17% 11% Depression 6% 12% 13% 20% 12% Peripheral neuritis 2% 23% 16% 2% 2% Neuropathy 1% 13% 5% 4% 4%Respiratory Cough increased 26% 41% 22% 43% 29% Dyspnea 22% 27% 26% 42% 25% Rhinitis 14% 22% 5% 22% 16% Pharyngitis 12% 22% 14% 30% 18% Sinusitis 9% 21% 7% 13% 6%Skin Rash 18% 38% 18% 27% 17% Herpes simplex 2% 12% 3% 7% 9% Acne 2% 11% 3% 3% < 1%Urogenital Urinary tract infection 5% 18% 14% 13% 7%
a Data for Herceptin single agent were from 4 studies, including 213 patients from Study 6.
b Anthracycline (doxorubicin or epirubicin) and cyclophosphamide.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 26

Metastatic Gastric Cancer The data below are based on the exposure of 294 patients to Herceptin in combination with a fluoropyrimidine (capecitabine or 5-FU) and cisplatin (Study 7). In the Herceptin plus chemotherapy arm, the initial dose of Herceptin 8 mg/kg was administered on Day 1 (prior to chemotherapy) followed by 6 mg/kg every 21 days until disease progression. Cisplatin was administered at 80 mg/m2 on Day 1 and the fluoropyrimidine was administered as either capecitabine 1000 mg/m2 orally twice a day on Days 1-14 or 5-fluorouracil 800 mg/m2/day as a continuous intravenous infusion Days 1 through 5. Chemotherapy was administered for six 21-day cycles. Median duration of Herceptin treatment was 21 weeks; median number of Herceptin infusions administered was eight.Table 5 Study 7: Per Patient Incidence of Adverse Reactions of All Grades (Incidence 5% between Arms) or Grade 3 /4 (Incidence >1% between Arms) and Higher Incidence in Herceptin Arm
Herceptin +FC FC (N = 294) (N = 290) N (%) N (%)
Body System/ All Grades All GradesAdverse Event Grades 3 / 4 Grades 3/ 4
Investigations Neutropenia 230 (78) 101 (34) 212 (73) 83 (29) Hypokalemia 83 (28) 28 (10) 69 (24) 16 (6) Anemia 81 (28) 36 (12) 61 (21) 30 (10) Thrombocytopenia 47 (16) 14 (5) 33 (11) 8 (3)Blood And Lymphatic System Disorders Febrile Neutropenia _ 15 (5) _ 8 (3)Gastrointestinal Disorders Diarrhea 109 (37) 27 (9) 80 (28) 11 (4) Stomatitis 72 (24) 2 (1) 43 (15) 6 (2) Dysphagia 19 (6) 7 (2) 10 ( 3) 1 ( 1)Body as a Whole Fatigue 102 (35) 12 (4) 82 (28) 7 (2) Fever 54 (18) 3 (1) 36 (12) 0 (0) Mucosal Inflammation 37 (13) 6 (2) 18 (6) 2 (1) Chills 23 (8) 1 ( 1) 0 (0) 0 (0)Metabolism And Nutrition Disorders Weight Decrease 69 (23) 6 (2) 40 (14) 7 (2)Infections And Infestations Upper Respiratory Tract Infections 56 (19) 0 (0) 29 (10) 0 (0) Nasopharyngitis 37 (13) 0 (0) 17 (6) 0 (0)Renal And Urinary Disorders Renal Failure and Impairment 53 (18) 8 (3) 42 (15) 5 (2)Nervous System Disorders Dysgeusia 28 (10) 0 (0) 14 (5) 0 (0)
The following subsections provide additional detail regarding adverse reactions observed in clinical trials of adjuvant breast, metastatic breast cancer, metastatic gastric cancer, or post-marketing experience. Cardiomyopathy Serial measurement of cardiac function (LVEF) was obtained in clinical trials in the adjuvant treatment of breast cancer. In Study 3, the median duration of follow-up was 12.6 months (12.4 months in the observation arm; 12.6 months in the 1-year Herceptin arm); and in Studies 1 and 2, 23 months in the AC-T arm, 24 months in the AC-TH arm. In Studies 1 and 2, 6% of patients were not permitted to initiate Herceptin following completion of AC chemotherapy due to cardiac dysfunction (LVEF < 50% or
15 point decline in LVEF from baseline to end of AC). Following initiation of Herceptin therapy, the incidence of new-onset dose-limiting myocardial dysfunction was higher among patients receiving Herceptin and paclitaxel as compared to those receiving paclitaxel alone in Studies 1 and 2, and in patients receiving Herceptin monotherapy compared to observation in Study 3 (see Table 6, Figures 1 and 2).Table 6a Per-patient Incidence of New Onset Myocardial Dysfunction (by LVEF) Studies 1, 2, 3 and 4
LVEF <50% and Absolute Decrease Absolute from Baseline LVEF Decrease
LVEF 10% 16% <20% and <50% decrease decrease 10% 20%
Studies 1 & 2b AC TH 22.8% 18.3% 11.7% 33.4% 9.2% (n=1606) (366) (294) (188) (536) (148)
AC T 9.1% 5.4% 2.2% 18.3% 2.4% (n=1488) (136) (81) (33) (272) (36)
Study 3 Herceptin 8.6% 7.0% 3.8% 22.4% 3.5% (n=1678) (144) (118) (64) (376) (59)
Observation 2.7% 2.0% 1.2% 11.9% 1.2% (n=1708) (46) (35) (20) (204) (21)
Study 4c TCH 8.5% 5.9% 3.3% 34.5% 6.3% (n=1056) (90) (62) (35) (364) (67)
AC TH 17% 13.3% 9.8% 44.3% 13.2% (n=1068) (182) (142) (105) (473) (141)
AC T 9.5% 6.6% 3.3% 34% 5.5% (n=1050) (100) (69) (35) (357) (58)
a For Studies 1, 2 and 3, events are counted from the beginning of Herceptin treatment. For Study 4, events are counted from the date of randomization.
b Studies 1 and 2 regimens: doxorubicin and cyclo-phosphamide followed by paclitaxel (AC T) or paclitaxel plus Herceptin (AC TH).
c Study 4 regimens: doxorubicin and cyclophosphamide followed by docetaxel (AC T) or docetaxel plus Herceptin (AC TH); docetaxel and carboplatin plus Herceptin (TCH).
Figure 1 Studies 1 and 2: Cumulative Incidence of Time to First LVEF Decline of 10 Percentage Points from Baseline and to Below 50% with Death as a Competing Risk Event
Time 0 is initiation of paclitaxel or Herceptin + paclitaxel therapy.
Figure 2 Study 3: Cumulative Incidence of Time to First LVEF Decline of 10 Percentage Points from Baseline and to Below 50% with Death as a Competing Risk Event
Time 0 is the date of randomization.
Figure 3 Study 4: Cumulative Incidence of Time to First LVEF Decline of 10 Percentage Points from Baseline and to Below 50% with Death as a Competing Risk Event
Time 0 is the date of randomization.
The incidence of treatment emergent congestive heart failure among patients in the metastatic breast cancer trials was classified for severity using the New York Heart Association classification system (I−IV, where IV is the most severe level of cardiac failure) (see Table 2). In the metastatic breast cancer trials the probability of cardiac dysfunction was highest in patients who received Herceptin concurrently with anthracyclines. In Study 7, 5.0% of patients in the Herceptin plus chemotherapy arm compared to 1.1% of patients in the chemotherapy alone arm had LVEF value below 50% with a
10% absolute decrease in LVEF from pretreatment values. Infusion Reactions During the first infusion with Herceptin, the symptoms most commonly reported were chills and fever, occurring in approximately 40% of patients in clinical trials. Symptoms were treated with acetaminophen, diphenhydramine, and meperidine (with or without reduction in the rate of Herceptin infusion); permanent discontinuation of Herceptin for infusional toxicity was required in <1% of patients. Other signs and/or symptoms may include nausea, vomiting, pain (in some cases at tumor sites), rigors, headache, dizziness, dyspnea, hypotension, elevated blood pressure, rash, and asthenia. Infusional toxicity occurred in 21% and 35% of patients, and was severe in 1.4% and 9% of patients, on second or subsequent Herceptin infusions administered as monotherapy or in combination with chemotherapy, respectively. In the post-marketing setting, severe infusion reactions, including hypersensitivity, anaphylaxis, and angioedema have been reported. Anemia In randomized controlled clinical trials, the overall incidence of anemia (30% vs. 21% [Study 5]), of selected NCI-CTC Grade 2-5 anemia (12.5% vs. 6.6% [Study 1]), and of anemia requiring transfusions (0.1% vs. 0 patients [Study 2]) were increased in patients receiving Herceptin and chemotherapy compared with those receiving chemotherapy alone. Following the administration of Herceptin as a single agent (Study 6), the incidence of NCI-CTC Grade 3 anemia was < 1%. In Study 7 (metastatic gastric cancer) on the Herceptin containing arm as compared to the chemotherapy alone arm the overall incidence of anemia was 28% compared 21% and of NCI CTC Grade 3/4 anemia was 12.2% compared to 10.3%. Neutropenia In randomized controlled clinical trials in the adjuvant setting, the incidence of selected NCI-CTC Grade 4−5 neutropenia (2% vs. 0.7% [Study 2]) and of selected Grade 2−5 neutropenia (7.1% vs. 4.5% [Study 1]) were increased in patients receiving Herceptin and chemotherapy compared with those receiving chemotherapy alone. In a randomized, controlled trial in patients with metastatic breast cancer, the incidences of NCI-CTC Grade 3/4 neutropenia (32% vs. 22%) and of febrile neutropenia (23% vs. 17%) were also increased in patients randomized to Herceptin in combination with myelosuppressive chemotherapy as compared to chemotherapy alone. In Study 7 (metastatic gastric cancer) on the Herceptin containing arm as compared to the chemotherapy alone arm, the incidence of NCI CTC Grade 3/4 neutropenia was 36.8% compared to 28.9%; febrile neutropenia 5.1% compared to 2.8%. Infection The overall incidences of infection (46% vs. 30% [Study 5]), of selected NCI-CTC Grade 2−5 infection/febrile neutropenia
(22% vs. 14% [Study 1]) and of selected Grade 3−5 infection/febrile neutropenia (3.3% vs. 1.4%) [Study 2]), were higher in patients receiving Herceptin and chemotherapy compared with those receiving chemotherapy alone. The most common site of infections in the adjuvant setting involved the upper respiratory tract, skin, and urinary tract. In Study 4, the overall incidence of infection was higher with the addition of Herceptin to AC-T but not to TCH [44% (AC-TH), 37% (TCH), 38% (AC-T)]. The incidences of NCI-CTC Grade 3−4 infection were similar [25% (AC-TH), 21% (TCH), 23% (AC-T)] across the three arms. In a randomized, controlled trial in treatment of metastatic breast cancer, the reported incidence of febrile neutropenia was higher (23% vs. 17%) in patients receiving Herceptin in combination with myelo suppressive chemo-therapy as compared to chemo therapy alone. Pulmonary Toxicity Adjuvant Breast Cancer Among women receiving adjuvant therapy for breast cancer, the incidence of selected NCI-CTC Grade 2−5 pulmonary toxicity (14% vs. 5% [Study 1]) and of selected NCI-CTC Grade 3−5 pulmonary toxicity and spontaneous reported Grade 2 dyspnea (3.4% vs. 1% [Study 2]) was higher in patients receiving Herceptin and chemotherapy compared with chemotherapy alone. The most common pulmonary toxicity was dyspnea (NCI-CTC Grade 2−5: 12% vs. 4% [Study 1]; NCI-CTC Grade 2−5: 2.5% vs. 0.1% [Study 2]). Pneumonitis/pulmonary infiltrates occurred in 0.7% of patients receiving Herceptin compared with 0.3% of those receiving chemotherapy alone. Fatal respiratory failure occurred in 3 patients receiving Herceptin, one as a component of multi-organ system failure, as compared to 1 patient receiving chemotherapy alone. In Study 3, there were 4 cases of interstitial pneumonitis in Herceptin-treated patients compared to none in the control arm. Metastatic Breast Cancer Among women receiving Herceptin for treatment of metastatic breast cancer, the incidence of pulmonary toxicity was also increased. Pulmonary adverse events have been reported in the post-marketing experience as part of the symptom complex of infusion reactions. Pulmonary events include bronchospasm, hypoxia, dyspnea, pulmonary infiltrates, pleural effusions, non-cardiogenic pulmonary edema, and acute respiratory distress syndrome. For a detailed description, see Warnings and Precautions. Thrombosis/Embolism In 4 randomized, controlled clinical trials, the incidence of thrombotic adverse events was higher in patients receiving Herceptin and chemotherapy compared to chemotherapy alone in three studies (3.0% vs. 1.3% [Study 1], 2.5% and 3.7% vs. 2.2% [Study 4] and 2.1% vs. 0% [Study 5]). Diarrhea Among women receiving adjuvant therapy for breast cancer, the incidence of NCI-CTC Grade 2−5 diarrhea (6.2% vs. 4.8% [Study 1]) and of NCI-CTC Grade 3−5 diarrhea (1.6% vs. 0% [Study 2]), and of Grade 1−4 diarrhea (7% vs. 1% [Study 3]) were higher in patients receiving Herceptin as compared to controls. In Study 4, the incidence of Grade 3−4 diarrhea was higher [5.7% AC-TH, 5.5% TCH vs. 3.0% AC-T] and of Grade 1−4 was higher [51% AC-TH, 63% TCH vs. 43% AC-T] among women receiving Herceptin. Of patients receiving Herceptin as a single agent for the treatment of metastatic breast cancer, 25% experienced diarrhea. An increased incidence of diarrhea was observed in patients receiving Herceptin in combination with chemotherapy for treatment of metastatic breast cancer. Renal Toxicity In Study 7 (metastatic gastric cancer) on the Herceptin-containing arm as compared to the chemotherapy alone arm the incidence of renal impairment was 18% compared to 14.5%. Severe (Grade 3/4) renal failure was 2.7% on the Herceptin-containing arm compared to 1.7% on the chemotherapy only arm. Treatment discontinuation for renal insufficiency/failure was 2% on the Herceptin-containing arm and 0.3% on the chemotherapy only arm. In the postmarketing setting, rare cases of nephrotic syndrome with pathologic evidence of glomerulopathy have been reported. The time to onset ranged from 4 months to approximately 18 months from initiation of Herceptin therapy. Pathologic findings included membranous glomerulonephritis, focal glomerulosclerosis, and fibrillary glomerulonephritis. Complications included volume overload and congestive heart failure. Immunogenicity As with all therapeutic proteins, there is a potential for immunogenicity. Among 903 women with metastatic breast cancer, human anti-human antibody (HAHA) to Herceptin was detected in one patient using an enzyme-linked immunosorbent assay (ELISA). This patient did not experience an allergic reaction. Samples for assessment of HAHA were not collected in studies of adjuvant breast cancer. The incidence of antibody formation is highly dependent on the sensitivity and the specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to Herceptin with the incidence of antibodies to other products may be misleading. Post-Marketing Experience The following adverse reactions have been identified during post approval use of Herceptin. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. • Infusion reaction [see Warnings and Precautions] • Oligohydramnios or oligohydramnios sequence, including pulmonary hypoplasia, skeletal abnormalities, and neonatal death [see Warnings and Precautions] • Glomerulopathy [see Adverse Reactions] DRUG INTERACTIONS In Study 5, the mean serum trough concentration of trastuzumab was consistently elevated approximately 1.5-fold, when administered in combination with paclitaxel as compared to trough concentrations of trastuzumab when administered in combination with an anthracycline and cyclophosphamide. In other pharmacokinetic studies, where Herceptin was administered in combination with paclitaxel, docetaxel or doxorubicin, Herceptin did not alter the plasma concentrations of these chemotherapeutic agents, or the metabolites that were analyzed. In a drug interaction substudy conducted in patients in Study 7, the pharmacokinetics of cisplatin,
capecitabine and their metabolites were not altered when administered in combination with Herceptin. USE IN SPECIFIC POPULATIONS Pregnancy: Category D [see Warnings and Precautions, Nonclinical Toxicology] Herceptin can cause fetal harm when administered to a pregnant woman. In post-marketing reports use of Herceptin during pregnancy resulted in cases of oligohydramnios and of oligohydramnios sequence, manifesting as pulmonary hypoplasia, skeletal abnormalities, and neonatal death. These case reports described oligohydramnios in pregnant women who received Herceptin either alone or in combination with chemotherapy. In some case reports, amniotic fluid index increased after Herceptin was stopped. In one case, Herceptin therapy resumed after the amniotic fluid index improved, and oligohydramnios recurred. Monitor women exposed to Herceptin during pregnancy for oligohydramnios. If oligohydramnios occurs, perform fetal testing that is appropriate for gestational age and consistent with community standards of care. The efficacy of IV hydration in management of oligohydramnios due to Herceptin exposure is not known. Advise women of the potential hazard to the fetus resulting from Herceptin exposure during pregnancy. Encourage pregnant women with breast cancer who are using Herceptin to enroll in MotHER-the Herceptin Pregnancy Registry: phone 1-800-690-6720. [see Patient Counseling Information]. No teratogenic effects were observed in offspring from reproduction studies in cynomolgus monkeys at doses up to 25 times the recommended weekly human dose of 2 mg/kg trastuzumab. In mutant mice lacking HER2, embryos died in early gestation. Trastuzumab exposure was reported at delivery in offspring of cynomolgus monkeys treated during the early (Days 20-50 of gestation) or late (Days 120-150 of gestation) fetal development periods, at levels of 15 to 28% of the maternal blood levels. Nursing Mothers It is not known whether Herceptin is excreted in human milk, but human IgG is excreted in human milk. Published data suggest that breast milk antibodies do not enter the neonatal and infant circulation in substantial amounts. Trastuzumab was present in the breast milk of lactating cynomolgus monkeys given 12.5 times the recommended weekly human dose of 2 mg/kg of Herceptin. Infant monkeys with detectable serum levels of trastuzumab did not have any adverse effects on growth or development from birth to 3 months of age; however, trastuzumab levels in animal breast milk may not accurately reflect human breast milk levels. Because many drugs are secreted in human milk and because of the potential for serious adverse reactions in nursing infants from Herceptin, a decision should be made whether to discontinue nursing, or discontinue drug, taking into account the elimination half-life of trastuzumab and the importance of the drug to the mother. Pediatric Use The safety and effectiveness of Herceptin in pediatric patients has not been established. Geriatric Use Herceptin has been administered to 386 patients who were 65 years of age or over (253 in the adjuvant treatment and 133 in metastatic breast cancer treatment settings). The risk of cardiac dysfunction was increased in geriatric patients as compared to younger patients in both those receiving treatment for metastatic disease in Studies 5 and 6, or adjuvant therapy in Studies 1 and 2. Limitations in data collection and differences in study design of the 4 studies of Herceptin in adjuvant treatment of breast cancer preclude a determination of whether the toxicity profile of Herceptin in older patients is different from younger patients. The reported clinical experience is not adequate to determine whether the efficacy improvements (ORR, TTP, OS, DFS) of Herceptin treatment in older patients is different from that observed in patients <65 years of age for metastatic disease and adjuvant treatment. In Study 7 (metastatic gastric cancer), of the 294 patients treated with Herceptin 108 (37%) were 65 years of age or older, while 13 (4.4%) were 75 and over. No overall differences in safety or effectiveness were observed. OVERDOSAGE There is no experience with overdosage in human clinical trials. Single doses higher than 8 mg/kg have not been tested. PATIENT COUNSELING INFORMATION • Advise patients to contact a health care professional immediately for any of the following: new onset or worsening shortness of breath, cough, swelling of the ankles/legs, swelling of the face, palpitations, weight gain of more than 5 pounds in 24 hours, dizziness or loss of consciousness [see Boxed Warning Cardiomyopathy]. • Advise pregnant women and women of childbearing potential that Herceptin exposure can result in fetal harm [see Warnings and Precautions and Use in Specific Populations]. • Advise women of childbearing potential to use effective contraceptive methods during treatment and for a minimum of six months following Herceptin [see Warnings and Precautions]. • Advise nursing mothers treated with Herceptin to discontinue nursing or discontinue Herceptin, taking into account the importance of the drug to the mother [see Use in Specific Populations]. • Encourage women who are exposed to Herceptin during pregnancy to enroll in MotHER- the Herceptin Pregnancy Registry (1-800-690-6720) [see Warnings and Precautions and Use in Specific Populations].
HERCEPTIN® [trastuzumab]Manufactured by:Genentech, Inc.A Member of the Roche Group1 DNA WaySouth San Francisco, CA 94080-4990
Initial US Approval: September 1998Revision Date: October 29, 2010Herceptin® is a registered trademark of Genentech, Inc.HER0000111000©2010 Genentech, Inc.
4:00 PM
TON_April2011_v7_TON 4/7/11 10:49 AM Page 27

Extravasation is always a risk whenadministering medicines intra-venously. This is when the
infused drug infiltrates the tissue sur-rounding the injection site. The result-ing injury can range from mild to life-threatening, depending on whether thedrug involved is classified as an irritantor a vesicant. The Infusion Nurses Society (INS)
defines a vesicant as “an agent capableof causing injury when it escapes fromthe intended vascular pathway intothe surrounding tissue.”1Anthracyclines are vesicants com-
monly used to treat cancer. More than500,000 doses of anthracyclines areadministered intravenously in theUnited States each year,2 and an esti-mated 0.1% to 1.0% of doses involveextravasation.3 Although extravasa-
tion is rare, it is not always preventa-ble. This is partly because many pa -tients with cancer have thin, fragile,mobile veins, and multiple puncturesare required to administer intravenous(IV) chemotherapy.4 The literaturealso documents unexpected extravasa-tions via central venous catheters.5-8Anthracycline extravasation re -
quires immediate attention to miti-gate the risk of severe—even perma-nently disabling—tissue damage.9The potential consequences under-score the need for nurses to know andadhere to national evidence-basedpractice guidelines for managinganthracycline extravasation. Theyshould also use this knowledge tomake the case to their employer forfollowing best practices.
How Anthracycline ExtravasationAffects PatientsSymptoms of anthracycline extrava-
sation can be immediate or delayedand typically include swelling; red-ness; and pain, itchiness, or burning atthe site of infusion.9 As damage pro-gresses, skin discoloration, induration,and blistering are often observed. Sequelae of a minor extravasation
sometimes heal without involved care.More extensive cases of extravasationcan progress to ulcers, tissue necrosis,and infection. These patients mightrequire plastic surgery, skin grafting,physical therapy, and other interven-tions over several months that leavethem scarred or disfigured. In extreme
cases, they might be left with perma-nent physical impairment, such asnerve damage, partial loss of hand func-tion, or amputation.10Extravasation sometimes leads to
treatment delays, particularly forpatients who develop ulcers. Becausechemotherapy has a negative effecton fast-growing cells like thoseinvolved in healing, it might need tobe withheld until the ulcer resolves,even if surgical treatment is notrequired. Treatment interruptions canreduce the overall effectiveness ofanticancer therapy and contribute topoorer outcomes.9
Treatment Guidelines Improve Care The INS and the Oncology Nursing
Society (ONS) have issued guidelineson chemotherapy administration thataddress treatment extravasation.1,11Both sets of guidelines specify dexra-zoxane for injection (Totect) as theonly medical treatment approved bythe US Food and Drug Admin -istration to manage anthracyclineextravasation.1,11 TopoTarget USA,which manufactures dexrazoxane,packages the antidote as part of a sin-gle-patient emergency treatment kitcontaining 10 vials of dexrazoxaneand 10 vials of diluent.12If there are symptoms or other signs of
anthracycline extravasation (such asfluid leaking from the injection site orproblems with the rate of infusion),guidelines call for stopping treatment,assessing the site, and cooling it with anice pack for 15 to 20 minutes.1,11 The iceneeds to be removed from the site for atleast 15 minutes before administeringdexrazoxane, which INS guidelines sayshould be initiated within 6 hours ofextravasation.1 The drug is infused into alarge vein in the unaffected arm. The guidelines cite evidence from 2
prospective multicenter studies in sup-port of the dexrazoxane recommenda-tion. The studies showed that dexrazox-
ane prevented tissue necrosis requiringsurgical treatment in 98% of patients(Figure).13 The remaining 2% reflectsthe experience of 1 study participantwho had experienced massive anthracy-cline extravasation, encompassing anarea 253 cm2.13 Additionally, 74% ofpatients treated with dexrazoxane expe-rienced no delay in chemotherapy.13National treatment guidelines reflect
the best practices according to evidencein the medical literature and outcomesobserved in hospitals and in the com-munity. They are useful tools that aid indecision making on effective care andpromote patient safety. Guidelines also provide peace of mind
for the nursing professional. In additionto caring for the patient at the bedsideand responding to the patient’s needs,nurses usually bear the hefty responsibil-ity of placing an IV line or catheter,each time putting their career, license,and heart on the line. When extravasation occurs, a nurse’s
first impulse is to assume blame. Even ifthe pharmacy failed to place the anti-dote on the formulary or did not releasean adequate supply of antidote, thenurse might still feel responsible. I con-tinue to be haunted by a case of anthra-cycline extravasation that occurred inthe late 1980s, before an antidote exist-ed. The patient had a large doxorubicinextravasation through a vein in theupper arm that progressed to severe tis-sue necrosis and infection. Eventually,the patient’s arm was amputated. Fortunately, with national guidelines
now in place on the proper placement ofIV catheters and patency assessmentduring an infusion of vesicant therapy,extravasations are few and far between.When they do occur, the availability ofan antidote and guidelines on its admin-istration make severe extravasation-related complications such as amputa-tions far less likely.
Spending Money to Save MoneyAlthough evidence-based medicine
has gained widespread acceptance inmedical and nursing circles, the call isgrowing for all clinicians and hospitalsto adhere to national treatment guide-lines. With Donald Berwick as the new administrator of the Centers forMedicare & Medicaid Services (CMS),there will likely be even more emphasison patient-centered, evidence-basedapproaches to care. Berwick is the for-mer president and chief executive officerof the Institute for Healthcare Im -
28 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Supportive Care
Guidelines for Managing Anthracycline ExtravasationWhat Nurses Should KnowBy Marianne Bunce-Houston, RN, MS, AOCNS, CRNIOncology Clinical Nurse Specialist, Contra Costa Regional Medical Center, Martinez, California
Marianne Bunce-Houston, RN, MS, AOCNS, CRNI
Source: Reference 13.
100
90
80
70
60
50
40
30
20
10
Study 1 Study 2 Studies 1 and 2 combined
Patients, %
100% 19/19 97.4%
37/3898.2%
56/57
Figure. Proportion of patients in 2 prospective, multicenter trials of dexrazoxanewho did not require surgical intervention for anthracycline-induced necrosis.
I continue to be hauntedby a case of anthracyclineextravasation thatoccurred in the late 1980s, before an antidote existed.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 28

provement, a nonprofit organization thatworked to advance evidence-based med-icine throughout the world. Berwick isexpected to base CMS reimbursementand policy decisions partly on nationaltreatment guidelines; private insurers areexpected to follow the agency’s lead. Atsome point, reimbursement for treatingcomplications like extravasation mightdepend on being able to show evidenceof adherence to national guidelines.
Although hospitals are loath to admitit, economic considerations have thepotential to influence their degree ofadherence to national guidelines. Thecurrent economy has led hospitals tobecome increasingly cost conscious and
sometimes tempts even those committedto evidence-based practice to replace amore expensive proven treatment speci-fied by the guidelines with a less expen-sive unproven alternative.
In the case of dexrazoxane for injec-tion, some hospitals are pooling theirresources to reduce their costs. Eachemergency kit contains enough dexra-zoxane to satisfy the full 3-day regimenrequired to treat anthracycline extrava-
sation.12 Three hospitals, for example,will share the expense of a single kit,dividing the doses so that each hospitalhas a 1-day supply. Such resource sharing
is potentially problematic, eroding a hos-pital’s control over supplies. What if ahospital is unwilling to hand over its sup-
www.TheOncologyNurse.com March/april 2011 I VOl 4, NO 2 29
Supportive Care
Case Report:AnthracyclineExtravasation
Acall came from a nurseattending to 3 patients in theinfusion clinic. One patient
had received a full dose of doxoru-bicin (60 mg/m2) via the vein in thedorsum of her hand. Afterward, thenurse detected a trace of blood inthe infusion tube. While administer-ing post-dose hydration, she noticedthat the patient’s hand was com-pletely swollen.
I concluded that a possible anthra-cycline extravasation had occurred.Dispersion of a vesicant drug into sur-rounding cells can damage tissue andvital structures outside the discretearea of intravenous (IV) placement.To mitigate possible damage, weneeded to initiate the procedure foradministering the antidote for anthra-cycline extravasation.
I immediately went to the phar-macy department to request thedexrazoxane for injection (Totect)emergency kit used to treat anthra-cycline extravasation, which isstocked as part of our facility’s for-mulary. Over the course of 3 days,the patient received the full dose ofdexrazoxane for injection as indicat-ed. She did not experience anysequelae from the extravasation andwas able to maintain her treatmentschedule as planned.
Before the existence of an evi-dence-based treatment plan, thispatient might have developed ulcera-tion of the hand, wrist, and upperforearm. Timely administration of theantidote prevented these complica-tions. The patient later said, “I appre-ciate the nurse’s prompt response andthe careful handling of my feelings. Iwas just grateful my hand was savedand that the antidote was availablewithin minutes.”
Continued on page 30
Three hospitals, for example, will share the expenseof a single kit, dividing the doses so that eachhospital has a 1-day supply.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 29

www.TheOncologyNurse.com30 March/april 2011 I VOl 4, NO 2
Supportive Care
ply or is unable to do so within the 6-hour window for initiating dexrazoxaneafter suspected anthracycline extravasa-tion? What if a second patient needs theantidote before the supply is restocked?Another concern is that one hospitalmight be less diligent than another inmonitoring product expirations.
Hospitals need to recognize that nothaving dexrazoxane readily availableto treat a case of anthracycline extra -vasation will potentially be more cost-ly for the hospital, particularly if apatient develops necrosis and infec-tions (See Sidebar: Making the Casefor Dexra zoxane). Insurers might alsobalk at paying to treat conditions thatadherence to guidelines would likelyhave prevented.
Best Practices: In Everyone’s Best Interest
Nurses are often directly involvedwhen anthracycline extravasation oc -curs, underscoring their important rolein patient care. Evidence-based treat-ment guidelines are clear in recom-mending prompt administration ofdexrazoxane for injection as an antidoteto anthracycline extravasation; failure
to adhere to these guidelines putspatients at risk of significant morbidity.
A nurse who is aware of the avail-ability of an antidote to complicationsassociated with a specific causticagent but fails to use it is open topotential legal liability as a nameddefendant in a malpractice lawsuit.Lack of control over supplies or phar-macy cost-cutting does not alleviate anurse of this responsibility. A hospitaladministration that is familiar withthe ONS and/or INS guidelines butdoes not make the antidote availablefaces similar liability risks.
Nurses must therefore be more out-spoken when it comes to advocatingfor best practices. This requires stay-ing informed of available resources,which goes beyond specific medica-tions to include individuals withinthe system who can offer support and
cooperation. Pharmacists typicallyhold the purse strings on pharmaceu-ticals in hospital systems. On col -ogists might be supportive of nurses’requests but ultimately defer to thepharmacists. This makes it evenmore important for nurses to speakup and outline the case for adheringto best practices on anthracyclineextravasation. Begin by citing theemphasis of the national guidelineson timely and appropriate interven-tion as a means of providing quickresolution and preventing costly,debilitating complications. �
References1. Alexander M, Corrigan A, Gorski L, et al, eds.Infusion Nursing: An Evidence-Based Approach. 3rded. Norwood, MA: Infusion Nurses Society;2009:357-367.2. TopoTarget launches Totect in the US [pressrelease]. October 16, 2007. https://newsclient.omxgroup.com/cdsPublic/viewDisclosure.action?
disclosureId=240215&messageId=271989.Accessed April 1, 2010.3. Buter J. Savene (dexrazoxane): an effective non-surgical treatment for anthracycline extravasation.Hosp Pharm Eur. 2007;33:38-39.4. Rudolph R, Larson DL. Etiology and treatmentof chemotherapeutic agent extravasation injuries: areview. J Clin Oncol. 1987;5:1116-1126.5. Ener RA, Meglathery SB, Styler M. Ex -travasation of systemic hemato-oncological thera-pies. Ann Oncol. 2004;15:858-862.6. Langstein HN, Duman H, Seelig D, et al.Retrospective study of the management of chemo -therapeutic extravasation injury. Ann Plastic Surg.2002;49:369-374.7. Langer SW, Sehested M, Jensen PB, et al.Dexrazoxane in anthracycline extravasation. J ClinOncol. 2000;18:3064.8. Langer SW. Treatment of anthracycline extrava-sation from centrally inserted venous catheters.Oncol Rev. 2008;2:114-116.9. Langer SW. Extravasation of chemotherapy.Curr Oncol Rep. 2010;12:242-246.10. Jordan K, Behlendorf T, Mueller F, Schmoll HJ,et al. Anthracycline extravasation injuries: man-agement with dexrazoxane. Ther Clin Risk Manag.2009;5:361-366.11. Polovich M, Whitford JM, Olsen M, eds.Chemotherapy and Biotherapy Guidelines andRecommendations for Practice. 3rd ed. Pittsburgh, PA:Oncology Nursing Society Publications; 2009:ix, 108.12. Totect (dexrazoxane) for injection [packageinsert]. Rockaway, NJ: TopoTarget USA Inc.October 2007.13. Mouridsen HT, Langer SW, Buter J, et al.Treatment of anthracycline extravasation withSavene (dexrazoxane): results from two prospectiveclinical multicentre studies. Ann Oncol. 2007;18:546-550.
Contra Costa Regional Medical Center is apublic hospital with 167 beds. Despite ourhospital’s cost-conscious approach to formu-
lary management, it was one of the first in the areato add the dexrazoxane for injection (Totect) emer-gency treatment kit to its formulary. This additionpredated the On cology Nursing Society guidelineson managing anthracycline extravasation and fol-lowed a long process involving presentations to 4hospital committees.
In a presentation for pharmacy staff, I incorporatedseveral slides that graphically depicted the sequelaeof anthracycline extravasation, essentially telling myaudience, “This is what an extravasation looks like;this is what I’m afraid of.” Audience members were vis-ibly affected by the graphic images. After I completedall 4 presentations, the hospital approved my requestto add the dexrazoxane for injection emergency kit tothe hospital formulary for the treatment of anthracy-cline extravasation.
My experience exemplifies how incorporatingpatient stories and photos in your presentation canhelp decision makers realize that looking out for thepatients’ best interests is the fiscally responsible choice.Formulary managers, pharmacists, and other adminis-trators need to understand that sometimes a financialoutlay is needed if we are to adhere to best practicesdesigned to protect our patients from avoidable com-plications associated with tremendous emotional,physical, and monetary costs.
Making the Case for Dexrazoxane
Guidelines for Managing Anthracycline Extravasation... Continued from page 29
Day 1: redness and pain. Day 2: blistering. Day 12: induration, necrosis.
Nurses are often directly involved when anthracyclineextravasation occurs, underscoring their importantrole in patient care.
Figure. Sequelae of doxorubicin extravasation.
Photo Credits: Oncology Nursing Society. Reproduced with permission via Copyright Clearance Center; January 16, 2010.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 30

Stephen F. Eckel, Pharm.D., M.H.A., BCPS
Melissa A. McDiarmid, MD, MPH, DABT
Kristie Howlett, RN, MS, CNS, AOCNS
National Safe Handling Awareness Day:
SAFE HANDLING BOOT CAMP
www.carmelpharmausa.com/aware5
Learning Objectives:At the completion of this activity, the participant will be able to:- Describe the evidence for the genotoxicity of anti-cancer chemotherapy in patients;- Relate the specific chromosomal targets that have been associated with various chemotherapy drug classes;- Discuss the sufficiency of current safe-handling policies in light of recent evidence of worker exposure;- Identify the concerns associated with handling hazardous medications;- Discuss pertinent aspects of the policy and procedure UNC Hospitals utilizes for handling hazardous medications;- Review future research opportunities around hazardous medications;- List ONS guidelines for safe handling;- Describe nursing basics for safe handling;- Describe proper donning of personal protective equipment (PPE).
STAT Educational Services, a division of National Pharmacy Technician Association Inc., is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
This knowledge-based program has been accredited for 1.0 contact hours of continuing education for pharmacists, pharmacy technicians, nurses, and risk managers.
Activity Type: KnowledgeTarget Audience: Pharmacists, Pharmacy Technicians, Nurses, & Risk ManagersUniversal Activity Number (UAN): 0384-9999-11-002-C05-P 0384-9999-11-002-C05-T
The University of Nebraska Medical Center College of Nursing Continuing Nursing Education is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Provided under Iowa Provider #78. Provider approved by the California Board of Registered Nursing, Provider #13699.
SA S
B B OOT BO T AF E H FE HA
BOOT CAMPSAFE HANDLING
BOOT CAMPSAFE HANDLING
anoitaN
e dnaHefSaSlla
erawAAwgnild
:yaDssene
ADM
TBA,.ssile MdimraiDcMAa
MtS e,HP, MDM
,.
CN SNCOOA,
,SNCr lwtsirK ttelwoHei
,, SMNR
plemrac.www
moc.asuamrah
5erawa/m
This knowledge-based program has been accredited for 1.0 contact hours of continuing education for pharmacists, pharmacy techni
dudeh ycamrahptacudETAATTTAS
This knowledge-based program has been accredited for 1.0 contact hours of continuing education for pharmacists, pharmacy techni
i .noittaa
cunoitaNfonoisivida,secivrrveSlanoi
This knowledge-based program has been accredited for 1.0 contact hours of continuing education for pharmacists, pharmacy techni
nInoitaicossAnaicinhceTTeycamrahPla
This knowledge-based program has been accredited for 1.0 contact hours of continuing education for pharmacists, pharmacy techni
noitatiderccAehtybdetiderccasi,.cn
cians, nurses, and risk managers.
A
This knowledge-based program has been accredited for 1.0 contact hours of continuing education for pharmacists, pharmacy techni
(noitacudEycamrahProflicnuoCn
cians, nurses, and risk managers.
gniunitnocforedivorpasa)EPCA
- Describe proper donning of personal protective equipment (PPE).
pecific chromo
- Describe nursing basics for safe handling;- List ONS guidelines for safe handling;- Review future research opportunities around hazardous medications;- Discuss pertinent aspects of the policy and procedure UNC Hospitals utilizes for handling hazardous medications;- Identify the concerns associated with handling hazardous medications;
ficiency of c - Discuss the suf fficiency of current safe-handling policies in light of recent evidence of worker exposure;- Relate the sp - Describe the e evidence for At the comple tion of this actLearning Obj ectives:
- Describe proper donning of personal protective equipment (PPE).
osomal targets that have been assoc
- Describe nursing basics for safe handling;- List ONS guidelines for safe handling;- Review future research opportunities around hazardous medications;- Discuss pertinent aspects of the policy and procedure UNC Hospitals utilizes for handling hazardous medications;- Identify the concerns associated with handling hazardous medications;
ficiency of current safe-handling policies in light of recent evidence of worker exposure; g
- Describe the evidence for the genotoxicity of anti-cancer chemotherapy in patients;, the participant will be able to:At the completion of this activity
- Describe proper donning of personal protective equipment (PPE).
ciated with various chemotherapy dr
- Review future research opportunities around hazardous medications;- Discuss pertinent aspects of the policy and procedure UNC Hospitals utilizes for handling hazardous medications;- Identify the concerns associated with handling hazardous medications;
ficiency of current safe-handling policies in light of recent evidence of worker exposure; py
- Describe the evidence for the genotoxicity of anti-cancer chemotherapy in patients;
- Discuss pertinent aspects of the policy and procedure UNC Hospitals utilizes for handling hazardous medications;
ug classes;ficiency of current safe-handling policies in light of recent evidence of worker exposure;
g
Registered Nursing, Provider #13699.
0384-9999-1
Provided under Iowa Provider #78. Provider approved by the California Board of
American Nurses Credentialing CenterEducation is accredited as a provider of continuing nursing education by the The University of Nebraska Medical Center College of Nursing Continuing Nursing
Universal Audience:arget TTarget
Activity T
Registered Nursing, Provider #13699.
1-002-C05-T
Provided under Iowa Provider #78. Provider approved by the California Board of
s Commission on ’American Nurses Credentialing CenterEducation is accredited as a provider of continuing nursing education by the The University of Nebraska Medical Center College of Nursing Continuing Nursing
0384-9999-1 0384-9999-1Activity Number (UAN):Universal
T Pharmacists, Pharmacy Audience: Knowledgeype: T Type:
Provided under Iowa Provider #78. Provider approved by the California Board of
1-002-C05-P
Accreditation. s Commission on Education is accredited as a provider of continuing nursing education by the The University of Nebraska Medical Center College of Nursing Continuing Nursing
Manage 0384-9999-1
echnicians, Nurses, & Risk ManagersTTechnicians, Nurses, & Risk Managers
Provided under Iowa Provider #78. Provider approved by the California Board of
The University of Nebraska Medical Center College of Nursing Continuing Nursing
echnicians, Nurses, & Risk Managers
TON_April2011_v7_TON 4/7/11 10:49 AM Page 31

Improved cure rates across multipletypes of cancer are spurring efforts toidentify optimal follow-up care for
cancer survivors. This is especiallyimportant for young cancer survivors,whose treatment-related adverse effectsmight not arise for years or even decades.Hodgkin lymphoma (HL) is a highly cur-able cancer that more commonly occursin young adults and children. The risk ofrecurrence varies among HL survivors,but many experience treatment-relatedtoxicity long after therapy completion1-7and have an elevated risk of othermedical problems, including secondmalignancies.1-4,6-9 Guidelines for fol-low-up care emphasize surveillance forrecurrent disease and second cancersand managing treatment-induced ad -verse effects.10-13Few studies have examined the qual-
ity of follow-up care HL survivorsreceive or considered the relationshipbetween follow-up care and out-comes.14,15 For example, it is uncertainwhether HL survivors with low likeli-hood of relapsing benefit from routinefollow-up computed tomography (CT)scanning. Growing concern about
exposure to diagnostic radiation16 sug-gests a need for studies to evaluate theextent to which routine CT scanningimproves patient outcomes.Previous studies have determined
that many cancer survivors—especiallysurvivors of childhood cancer—are notscreened for second cancers in accor-dance with current guidelines for fol-low-up care.17-19 Some studies havebeen limited by a reliance on patientreporting or a decision to restrict datato patients aged ≥65 years.17-19 Theobjective of the current study was toevaluate the follow-up care HLpatients receive and the degree towhich this care incorporates routineimaging, standard healthcare interven-tions, and guideline recommendationsfor cancer screening in HL survivors.
Study Population and ProtocolWe used the Ontario Cancer Registry
to identify all patients in Ontario givenan HL diagnosis from 1992 through 2000(N = 2900). Excluding patients with aprior malignancy or those who devel-oped a second malignancy within 12months of diagnosis, patients whorequired chemotherapy for >1 year afterdiagnosis, and patients who died duringthe first year of follow-up left a total of2071 HL survivors for study inclusion(median age, 35.4 years). To assess adher-ence to recommended routine and HL-specific cancer screening tests, we ana-lyzed billing records for physician visits,imaging tests, and cancer screening forfollow-up in years 2 through 15. Data forpatients who died or left the OntarioHealth Insurance Plan during the follow-up period were censored.
ResultsIn years 2 through 5 after diagnosis,
HL survivors averaged 4 visits annuallyto their primary care provider (PCP),with approximately 75% of patientsoverall making ≥1 PCP visit per year.During this same period, between 65%and 75% of patients each year made ≥1visit to a medical oncologist and between11% and 31% of patients each year saw aradiation oncologist at least once. Inyears 2 through 5, approximately 13% ofpatients visited a PCP but not an oncol-ogist. For years 6 through 9, cumulative-ly, 87.4% of patients made ≥1 visit totheir PCP. Although 86.7% of patientshad ≥1 appointment with the medicaloncologist during this 4-year interval, itis not clear whether the visits were forannual follow-up care or scheduled toaddress specific concerns.Overall, patients underwent a range
of imaging tests, including chest radi-
ography, CT scanning, gallium scan-ning, magnetic resonance imaging(MRI), and ultrasound. Imaging testscompleted >11 months after the previ-ous imaging procedure were catego-rized as “annual” screening. In the sec-ond year of follow-up, 87.8% ofpatients had ≥1 chest radiographs and66% had ≥1 CT scans. Rates steadilydeclined in each of the next few years;in year 5, 62.9% of patients had chestradiography and 31.8% received CTscanning. The rate for patients consid-ered to have undergone annual CTscanning during the 4-year period heldfairly constant at ~20% each year.During the first 4 years of follow-up, acumulative 5352 CT scans were per-formed, with 125 patients receivingchemotherapy within 6 months of CTscanning.Although most HL survivors visited
a PCP or an oncologist in the 14-year
www.TheOncologyNurse.com32 March/april 2011 I VOl 4, NO 2
CONTINUING EDUCATION
Follow-up Management of Hodgkin Lymphoma SurvivorsBy David C. Hodgson, MD, MPHAssociate Professor, Department of Radiation Oncology, University of Toronto
Staff Radiation Oncologist, Department of Radiation Oncology Princess Margaret Hospital/University Health Network, Toronto, Ontario, Canada
PROGRAM CE11 • RELEASE DATE: APRIL 15, 2011 • EXPIRATION DATE: APRIL 15, 2012
ESTIMATED TIME TO COMPLETE: 1.0 HOUR • COMPLETE THE POSTTEST AT WWW.THEONCOLOGYNURSE.COM
CONTINUING NURSING EDUCATIONACCREDITATION AND CONTACTHOURS STATEMENTScience Care is approved by the California Boardof Registered Nursing, Provider number 15559,for 1.0 Contact hour.
METHOD OF PARTICIPATION
1. Read the article in its entirety2. Go to www.TheOncologyNurse.com3. Select “Continuing Education”4. Click on this article’s title from the list shown5. Select “Click here to complete the posttest and obtain a CE certificate online”
6. Complete and submit the CE posttest and CE Activity Evaluation
7. Print your Certificate of Credit
This activity is provided free of charge to participants.
FACULTY DISCLOSURESAs a provider accredited by the California Board ofRegistered Nursing, Science Care must ensure bal-ance, independence, objectivity, and scientific rigorin all its activities. All course directors, faculty, plan-ners, and any other individual in a position to con-trol the content of this educational activity arerequired to disclose to the audience any relevantfinancial relationships with any commercial inter-est. Science Care must determine if the faculty’srelationships may influence the educational contentwith regard to exposition or conclusion and resolveany conflicts of interest prior to the commencementof the educational activity.
Disclosures are as follows:• David C. Hodgson, MD, MPH, has nothing to disclose.
• Dawn Lagrosa has nothing to disclose.• Chistina A. Liebertz, APN, RN, has nothing to disclose.
• Christin Melton has nothing to disclose. • Karen Rosenberg has nothing to disclose.
The staff of Science Care have nothing to disclose.
DISCLAIMERThe opinions and recommendations expressedby faculty, authors, and other experts whoseinput is included in this program are their ownand do not necessarily represent the viewpointof Science Care or Green Hill HealthcareCommunications, LLC.
COPYRIGHT STATEMENTCopyright © 2011 Science Care. All rights reserved.
EDITORIAL BOARDDavid C. Hodgson, MD, MPH
Princess Margaret Hospital/University Health Network610 University AvenueToronto, ON M5G 2M9Canada
Christina A. Liebertz, APN, RNUrology Outpatient CenterMemorial Sloan-Kettering Cancer Center1275 York AvenueNew York, NY 10065
STATEMENT OF NEEDHodgkin lymphoma is a highly curable cancer thatis most common in younger adults and children.Long after therapy completion, treatment-relatedtoxicities are often evident and second malignan-cies can arise. Follow-up care for patients inremission involves monitoring them for recurrentdisease and managing existing and emergenttreatment-induced adverse effects. Although cur-rent guidelines outline appropriate surveillancemeasures for detecting recurrence and secondmalignancies, limited data are available on thequality of follow-up care being provided to sur-vivors of Hodgkin lymphoma.
TARGET AUDIENCEAdvanced practice nurses, registered nurses, andother interested healthcare professionals, espe-cially those caring for cancer patients
LEARNING OBJECTIVESAfter completing this activity, the reader should beable to:• Recognize the need for long-term follow-up todetect and manage delayed effects of treatmentand second malignancies in patients withHodgkin lymphoma.
• Incorporate recommended interventions intopractice for screening Hodgkin lymphoma survivors for cancer.
Guidelines for follow-upcare emphasizesurveillance for recurrentdisease and secondcancers and managingtreatment-inducedadverse effects.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 32

maRch/apRil 2011 I vol 4, No 2 33www.TheoncologyNurse.com
follow-up period, 62.5% of survivorsaged 50 to 70 years never received stan-dard colorectal cancer screening as rec-ommended for this age demographic.Also in this period, 32.3% of womenaged 50 to 69 years never underwentmammography to screen for breast can-cer, and 19.9% of women aged 20 to 69years never received cervical cancerscreening. These screening rates weresimilar to rates of colorectal, breast, andcervical cancer screening among thegeneral population of Ontario.20Women aged 25 to 49 years who had
received an HL diagnosis ≥9 years earlierand underwent mediastinal radiotherapyas part of initial treatment (n = 526) wereconsidered eligible for early-onset breastcancer screening. Guidelines typicallyrecommend women treated with irradia-tion to the chest or axillary undergoannual mammography starting 8 to 10years after completion of therapy. During14 years of follow-up, only 22% of eligiblepatients underwent HL-specific breastcancer screening. Those women who sawonly their PCP and not an oncologistduring follow-up were significantly lesslikely to get HL-specific screening (oddsratio, 0.14; 95% confidence interval,0.03-0.64).
DiscussionWe believe our study is the first to
examine the provision of follow-up careto an unselected, population-basedcohort of HL survivors. Although mostpatients with HL are completely curedand never relapse, treatment-relatedadverse effects often persist or arise longafter treatment ends.Several studies have shown that
long-term survivors have an increasedrisk of heart disease,2,3,6,8 second malig-
nancy,4,7,9 thyroid dysfunction,1 andother medical problems resulting inpart from therapy. In particular, HL sur-vivors appear to have an increased riskof leukemia, non-Hodgkin lymphoma,and solid tumors of the breast, thyroid,colon, rectum, cervix, stomach, andlungs; the degree of increased riskvaries according to age at diagno sis,stage of disease, and treatment re -ceived.4,7,9 For example, radiation ther-apy that includes the mediastinum andaxillae is associated with an increasedrisk of breast cancer.21Oncology experts have developed
guidelines for follow-up care of HL sur-vivors (Table). These guidelines gener-ally emphasize detecting recurrence andmanaging residual and delayed effects oftreatment.10,13
Use of Computed TomographyScanningIt is standard to use imaging to con-
firm remission status in HL patientswho have completed therapy.Guidelines on the use of CT scanningfor follow-up care differ between theEuro pean Society of Medical Oncology(ESMO) and the National Com p re -hensive Cancer Network (NCCN).After confirming re mission, ESMO rec-ommends CT scanning only forpatients with suspicious clinical symp-toms.12 NCCN guidelines call for chestradiographs and CT scanning of thechest every 6 to 12 months during thefirst 2 to 5 years of follow-up and CTscanning of the abdominal/pelvic re -gion every 6 to 12 months for the first2 to 3 years of follow-up and thenannually for the next 2 years. After 5years, NCCN recommends annual radi-ographs or CT scans of the chest for
patients considered to have anincreased risk of lung cancer andoptionally for patients treatedwith a nonalkylating agent or whodid not receive chest radiotherapyand have no other risk factors forlung cancer.13 The NCCN guidelinesacknowledge that few data support theserecommendations but state that theyrepresent the “range of practice atNCCN institutions.”In follow-up years 2 through 5, HL
survivors in the study received a totalof 5352 CT scans—a rate more than 3times greater than the rate of CTscanning in the general population ofOntario.22 Only 125 patients initiatedchemotherapy within 6 months ofundergoing CT scanning, which sug-gests that routine scanning is not an effi-cient way to detect treatable diseaserecurrence. This is supported by previousstudies that found CT scanning to be no more effective than radiography atdetecting asymptomatic HL recurrence23and not cost-effective if it is assumed thatonly 8% of patients with recurrence areasymptomatic.24 Although use of CTscanning in this patient population wasconsistent with practices at NCCN insti-tutions, the low recurrence rate suggeststhat it was likely overused in follow-upcare. One limitation of this study was theinability to determine the reason forimaging tests using administrative data.
Screening for Second CancersSome HL survivors have a lifelong ele-
vated risk of second cancers9 and requirescreening for certain cancers earlier andmore frequently than the general popula-tion. A 2007 study concluded that therisk of colo rectal cancer for individualsaged 35 to 40 years who survived HL asan adolescent or young adult was compa-
rable to the risk seen in the general pop-ulation at age 50 to 54 years. The samestudy found that within 5 to 10 years ofan HL diagnosis, the risk of breast cancerfor young female survivors was similar tothat of a typical 50-year-old woman.9 Although patients in our study
made frequent visits to multiplephysicians, many did not undergocancer screening as advised by currentguidelines for the follow-up care forHL survivors. Of particular concern isthe large proportion of young womenwho received mediastinal radiothera-py for HL yet were never screened for
breast cancer.4,7,25 Guide lines typicallyrecommend that these survivors initi-ate breast cancer screening 8 to 10years posttherapy.10,13 Our findingsindicate that screening guidelines forHL survivors are not being incorpo-rated into clinical practice. Many HL survivors are also not receiv-
ing routine age-appropriate screening forbreast cancer, cervical cancer, and col-orectal cancer. Over the 14-year follow-up period in this study, nearly a majorityof eligible survivors did not appear toundergo colorectal cancer screening anda substantial proportion of patients didnot receive screening for cervical orbreast cancer. Despite their personal his-tory with cancer and frequent contactwith physicians, HL survivors were nomore likely than the general populationin Ontario to undergo routine screeningfor these 3 cancers.20
ConclusionOur study indicates that the rates of
cancer screening are too low for HL sur-vivors and the rate of CT scanning islikely too high, particularly in light ofemerging data on the contributing role ofradiation exposure during CT scanningto cancer development.16 To improve fol-low-up care, patients and clinicians needto be educated on the latent health risksfor HL survivors and their need for fol-low-up care.
Improving communication betweenoncologists and PCPs on issues facing HLsurvivors would also likely lead to bettercare.24,26-28 The cancer care team shouldeducate HL survivors on which symp-toms require prompt medical attentionfrom a physician, who will then deter-mine whether further evaluation is war-ranted. Efforts should also be made toboost rates of posttreatment screening forsecond cancers in HL survivors, particu-larly breast cancer screening in womenwho undergo mediastinal radiotherapy, tofacilitate earlier detection and treatment.
To Receive cRediT, compleTe The posTTesT aTTheOncologyNurse.com
Our study indicates that the rates of cancer screeningare too low for Hodgkin lymphoma survivors and therate of CT scanning is likely too high, particularly in lightof emerging data on the contributing role of radiationexposure during CT scanning to cancer development.
Continued on page 34
Table Summary of NCCN Guidelines on Follow-up Care for HL Survivors
When Frequency WhoPhysicalexam/blood test (with oncologist)
Years 1-2Years 3-5After year 5
Every 2-4 moEvery 3-6 moAnnually
All
Chest radiographor CT
Years 2-5After year 5
Every 6-12 moAnnually
AllPatients withincreased risk of lung cancera
Abdominal/pelvicCT (category 2B)b
Years 2-3 Every 6-12 mo All
Breast screeningb 8-10 years aftertherapy or age 40years (whichever is first)
Annually Women treatedwith chest/axillaryRT
aOptional after 5 years for patients treated with a nonalkylating agent, no chest RT, and no other risk factors.bCategory 2B recommendations are based on lower-level evidence and there is nonuniform consensus (but no major disagreement).cGuidelines note that the American Cancer Society recommends breast MRI and mammography in women whoreceived chest irradiation between 10 and 30 years of age.
HC Hodgkin Lymphoma; CT indicates computed tomography; MRI, magnetic resonance imaging; NCCN, NationalComprehensive Cancer Network; RT, radiotherapy.
Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology for Hodgkin’s LymphomasV.2.2010. ©2010 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines™ and all other NCCN content are trademarks owned by the National Comprehensive Cancer Network, Inc.
TON_April2011_v7_TON 4/7/11 10:49 AM Page 33

Some cancer centers in NorthAmerica have established structuredclinics in an attempt to provide thegrowing number of cancer survivorswith appropriate follow-up care. Thereis also growing emphasis on empower-ing survivors through education,encouraging them to take an activerole in their healthcare. Althoughthese are positive developments, evi-dence is lacking on how to structureeffective survivorship programs andadapt them to patients. In addition tostudying these issues, future researchshould determine the level of follow-up care from oncologists and PCPsneeded to improve the quality of careand/or outcomes for HL survivors. �
DisclosureFunding for the study was provided
by Cancer Care Ontario. The study wassupported by the Institute for ClinicalEvaluative Sciences, which is fundedby the Ontario Ministry of Health andLong-Term Care.
References1. Acharya S, Sarafoglou K, LaQuaglia M, et al.Thyroid neoplasms after therapeutic radiation formalignancies during childhood or adolescence. Cancer.2003;97:2397-2403.
2. Adams MJ, Lipsitz SR, Colan SD, et al. Cardio -vascular status in long-term survivors of Hodgkin’s dis-ease treated with chest radiotherapy. J Clin Oncol.2004;22:3139-3148.3. Aleman BM, van den Belt-Dusebout AW, De BruinML, et al. Late cardiotoxicity after treatment forHodgkin lymphoma. Blood. 2007;109:1878-1886.4. Bhatia S, Yasui Y, Robison LL, et al; for the LateEffects Study Group. High risk of subsequent neoplasmscontinues with extended follow-up of childhoodHodgkin’s disease: report from the Late Effects StudyGroup. J Clin Oncol. 2003;21:4386-4394.5. Mauch P, Ng A, Aleman B, et al. Report from theRockefeller Foundation Sponsored InternationalWorkshop on reducing mortality and improving quali-ty of life in long-term survivors of Hodgkin’s disease.Eur J Haematol Suppl. 2005;66:68-76.6. Swerdlow AJ, Higgins CD, Smith P, et al.Myocardial infarction mortality risk after treatment forHodgkin disease: a collaborative British cohort study. JNatl Cancer Inst. 2007;99:206-214.7. van Leeuwen FE, Klokman WJ, Hagenbeek A, et al.Second cancer risk following Hodgkin’s disease: a 20-year follow-up study. J Clin Oncol. 1994;12:312-325.8. Myrehaug S, Pintilie M, Tsang R, et al. Cardiacmorbidity following modern treatment for Hodgkinlymphoma: supra-additive cardiotoxicity of doxoru-bicin and radiation therapy. Leuk Lymphoma. 2008;49:1486-1493.9.Hodgson DC, Gilbert ES, Dores GM, et al. Long-termsolid cancer risk among 5-year survivors of Hodgkin’slymphoma. J Clin Oncol. 2007;25:1489-1497.10. Ralleigh G, Given-Wilson R. Breast cancer riskand possible screening strategies for young women fol-lowing supradiaphragmatic irradiation for Hodgkin’sdisease. Clin Radiol. 2004;59:647-650.11. Children’s Oncology Group Nursing DisciplineClinical Practice Subcommittee/Survivorship in col-laboration with the Late Effects Committee.Establishing and Enhancing Services for Childhood
Cancer Survivors: Long-Term Follow-UpProgram Resource Guide. 2007. www.survivorshipguidelines.org/pdf/LTFUResourceGuide.pdf.Accessed Dec ember 22, 2010.12. Engert E, Eichenauer DA, Dreyling M; ESMOGuidelines Working Group. Hodgkin’s lymphoma:ESMO clinical practice guidelines for diagnosis, treat-ment, and follow-up. Ann Oncol. 2010;21(suppl5):168-177. 13. NCCN Clinical Practice Guidelines in Oncology(NCCN Guidelines™) for Hodgkin Lymphoma.V.2.2010. ©2010 National Comprehensive CancerNetwork, Inc. All rights reserved. www.nccn.org/pro-fessionals/physician_gls/PDF/hodgkins.pdf. AccessedDecember 22, 2010.14. Ng AK, Li S, Recklitis C, et al. Health practice inlong-term survivors of Hodgkin’s lymphoma. Int JRadiat Oncol Biol Phys. 2008;71:468-476.15. Oeffinger KC, Ford JS, Moskowitz CS, et al.Breast cancer surveillance practices among womenpreviously treated with chest radiation for a child-hood cancer. JAMA. 2009;301:404-414.16. Brenner DJ, Hall EJ. Computed tomography—anincreasing source of radiation exposure. N Engl J Med.2007;357:2277-2284.17. Snyder CF, Earle CC, Herbert RJ, et al. Trends infollow-up and preventive care for colorectal cancersurvivors. J Gen Intern Med. 2008;23:254-259.18. Snyder CF, Frick KD, Kantsiper ME, et al. Pre -vention, screening, and surveillance care for breastcancer survivors compared with controls: changesfrom 1998 to 2002. J Clin Oncol. 2009;27:1054-1061.19. Nathan PC, Ness KK, Mahoney MC, et al.Screening and surveillance for second malignant neo-plasms in adult survivors of childhood cancer: a reportfrom the childhood cancer survivor study. Ann InternMed. 2010;153:442-451.20. Cancer Care Ontario. Cancer in Ontario:Overview, A Statistical Report. Toronto, Canada,2010. www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=81843. Accessed December 22, 2010.
21. Hodgson DC, Pintilie M, Yun L, et al.Cardiovascular morbidity following modern treat-ment for Hodgkin lymphoma: age- and sex-specificestimates of risk in the doxorubicin era. Int J RadiatOncol Biol Phys. 2008;72:S122-S123. 22. Laupacis A, Przybysz R, Keller MA. CT and MRIscanning. In: Access to Health Services in Ontario.ICES Atlas. 2nd ed. 2006:149-164.23. Dryver ET, Jernstrom H, Tompkins K, et al.Follow-up of patients with Hodgkin’s disease follow-ing curative treatment: the routine CT scan is of littlevalue. Br J Cancer. 2003;89:482-486.24. Guadagnolo BA, Punglia RS, Kuntz KM, et al.Cost-effectiveness analysis of computerized tomogra-phy in the routine follow-up of patients after primarytreatment for Hodgkin’s disease. J Clin Oncol.2006;24:4116-4122.25.Ng AK, Bernardo MV, Weller E, et al. Second malig-nancy after Hodgkin disease treated with radiation ther-apy with or without chemotherapy: long-term risks andrisk factors. Blood. 2002;100:1989-1996.26. Oeffinger KC, Wallace WH. Barriers to follow-upcare of survivors in the United States and the UnitedKingdom. Pediatr Blood Cancer. 2006;46:135-142.27.Oeffinger KC, McCabe MS. Models for deliveringsurvivorship care. J Clin Oncol. 2006;24:5117-5124.28.Oeffinger KC, Robison LL. Childhood cancer sur-vivors, late effects, and a new model for understand-ing survivorship. JAMA. 2007;297:2762-2764.
AcknowledgementJill Stein contributed to the preparation ofthis article.
www.TheoncologyNurse.com34 maRch/apRil 2011 I vol 4, No 2
CONTINUING EDUCATION
COMMENTARY
Importance of a Care Plan in the Follow-upManagement of Hodgkin Lymphoma SurvivorsBy Christina A. Liebertz, APN, RN Urology Outpatient Center, Memorial Sloan-Kettering Cancer CenterNew York, New York
This study found that computedtomography scans rarely led toactive therapy, despite the fact
that a high number of posttreatmentscans were performed. In addition, thestudy validated the ambiguous screen-ing value and cost-effectiveness of pro-cedures other than the history, physicalexamination and, possibly, chest x-ray.The lack of screening these patients
received posttreatment highlights theneed for standardized survivorshipcare guidelines and education of prac-titioners and patients. It is alarmingthat many high-risk patients did notreceive screening. How many of thesepatients could have found early,detectable, and treatable disease withsimple screening and follow-up? Oneof the limitations to this study is thatthese patients were diagnosed andtreated from 1992 to 2000, before thedevelopment and adoption of more
standardized guidelines for surveil-lance and follow-up for cancer sur-vivors. It would be interesting to see ifthese findings have changed and byhow much with the advent of moreeducational and formal survivorshipprograms. Also, because this study wasdone in Canada, it is difficult to knowhow these findings would compare if asimilar study were done within the UShealthcare system.This study clearly supports the need
for more research to establish evi-dence-based standards for follow-upand surveillance, along with methodsto decrease posttreatment toxicities,morbidity, and mortality. We alsoneed to evaluate the best, most effi-cient methods for providing this careand increasing patient adherence torecommendations. A limitation ofthis study is the lack of data aboutwhat other factors may have impacted
lack of screening. Besides practitionerrecommendation, other potential bar-riers to screening may have includedlack of insurance, decreased access tocare, and/or psychosocial issues suchas fear of recurrence.We have learned a lot about the
needs of Hodgkin lymphoma survivorsand survivorship care in general, butthere is still much to learn aboutimproving and providing that care.We need to develop methods to sup-port more consistent, effective, andthorough follow-up care and commu-nication. One method is developingposttreatment cancer care plans orsummaries that not only educate eachpatient about individualized follow-upcare, but also serve as a tool for all ofthat patient’s healthcare providers.Unfortunately, this is rarely provided. Regardless of the method used,
there should be open and ongoing
communication between the oncolo-gist and patient’s other healthcarepractitioners. Recommendations fromall of these providers should be consis-tent and based on best practices. Theyshould include assessments for treat-ment-related toxicities; education forgeneral health maintenance (eatinghabits, regular exercise, smoking ces-sation, vaccinations); appropriate fol-low-up and screening guidelines, espe-cially for high-risk conditions andcancers; and appropriate, efficient,and individualized surveillance guide-lines based on risks.Follow-up care should be clearly
defined, not random. We have mademany advances in survivorship care,but this study reinforces the need tocontinue to develop more efficientmethods to provide optimal posttreat-ment care and improve patient out-comes and quality of life. �
Continued from page 33
Follow-up Management of Hodgkin Lymphoma...
To Receive cRediT, compleTe The posTTesT aTTheOncologyNurse.com
TON_April2011_v7_TON 4/7/11 12:28 PM Page 34

“ To never have to face cancer again.”
THE PROMISE OF 1000 ORIGAMI CRANES
The ancient Japanese tradition of senbazuru promises
that anyone who folds 1000 origami cranes will be
granted a wish, such as long life or recovery from illness
— at Millennium, our wish is to cure cancer.
We’re committed to patients and strive to make a
difference in their lives. 1000 Cranes of Hope is an online
monument that contains the collective wishes of patients,
caregivers, healthcare providers and our employees who
all stand together in the fight against cancer.
Add your wish to create a new crane — and make
a difference. For each crane created, Millennium will
make a donation to benefit professional and charitable
cancer organizations.
Kathy GramMillennium Employee & Cancer Survivor
Visit 1000cranesofhope.com to add your wish to the flock.
Sponsored by Millennium: The Takeda Oncology Company ©2011 Millennium Pharmaceuticals, Inc. All rights reserved. CCO205
TON_April2011_v7_TON 4/7/11 10:50 AM Page 35

www.TheOncologyNurse.com36 March/april 2011 I VOl 4, NO 2
Patient-Centered Outcomes Research
As nations around the globe strug-gle to afford the growing cost ofcare for their citizens, more peo-
ple are asking ‘how much is too much?’when it comes to cancer. Although theJohn G. Kuhn Keynote Lecture deliveredat the annual meeting of the Hematology/Oncology Pharmacy Association wastitled “The Cost of Cancer Therapy,”speaker Tito Fojo, MD, PhD, with themedical oncology branch of the NationalCancer Institute (NCI), says cost is notthe real issue. “If you frame the argumentin terms of cost, you’re going to lose it,”he told the audience of pharmacists. Fojosaid the real issues are “how effectivedrugs are and how toxic drugs are.”Fojo offered examples of drugs used in
clinical practice that he believes notonly fail to improve survival but actuallyharm patients, including cetuximab(Erbitux) in metastatic colorectal cancer(mCRC) and bevacizumab (Avastin) in breast cancer. He noted that contro-versy surrounds these examples and noteveryone shares his views—includingGiuseppe Giaccone, his supervisor at theNCI and a member of the AmericanSociety of Clinical Oncology (ASCO)
panel responsible for adding the combi-nation of cetuximab and paclitaxel tothe ASCO guidelines for first-line therapyof mCRC. The examples Fojo cites are alsofound in the National ComprehensiveCancer Network (NCCN) treatmentguidelines.
Even if one disagrees with Fojo’s con-clusions, his review of the pivotal trialsused to support approval of cetuximab inmCRC and bevacizumab in breast can-cer underscores important considerationsfor stakeholders when deciding how
anticancer drugs should be developed,evaluated, and used. “Our drug develop-ment, drug approval, and drug consump-tion strategies need better focus,” saidFojo, who lamented that despite thedecade that has elapsed since imatinib(Gleevec) ushered in the “targeted ther-apy revolution,” too many treatments arestill used indiscriminately in broadpatient populations. Fojo sees room for improvement at all
levels: academia, the pharmaceuticalindustry, government agencies like theUS Food and Drug Administration(FDA), and clinicians caring for patientswith cancer. All are responsible for “ourfailure to deliver on the promise of per-sonalized medicine.” The experience with cetuximab in
mCRC supports Fojo’s contention thatresearchers need to analyze drugsprospectively, identifying predictivemarkers before initiating trials. Fouryears after cetuximab’s 2004 approval,investigators reported in the NewEngland Journal of Medicine that it wasineffective in patients with mutatedKRAS. In 2009 ASCO issued itsProvisional Clinical Opinion recom-mending KRAS testing before prescrib-ing cetuximab but called compliancewith the opinion voluntary. Fojo said a prospective investigation
might have uncovered the KRAS issuebefore trials were initiated. Cetuximabinhibits epidermal growth factor receptor(EGFR), and Fojo said, “As early as1990, Bert Vogelstein at Hopkins hadreported that as many as 50% of colorec-tal patients harbored KRAS.” In 1998,KRAS was reported to be in the EGFRsignaling pathway. “Despite this, wewent ahead and conducted studies with-out looking at this prospectively.” Continued investigation into the
causes of poor response to cetuximabamong some patients with wild-typeKRAS will likely whittle the viablepatient population down even further.“Eventually, we’ll be able to identify the80% of patients that do not benefit andgive it only to the 20% who benefit sub-stantially, and a drug that was marginalto begin with will become highly effec-tive,” explained Fojo.Fojo said he is concerned that “in -
creasingly, therapies that demonstrate atbest marginal improvement are beingused in the treatment of cancer.” Withbreast cancer, we might even be goingbackwards he said, pointing to the con-troversy over bevacizumab. He empha-sized that his views did not representthose of the NCI or anyone else. Fojo faulted the decision to approve
bevacizumab based on data from the
Eastern Cooperative Oncology Group(ECOG) 2100 study, which suggestedadding it to paclitaxel significantly pro-longed progression-free survival (PFS)but not overall survival (OS). Althoughthe study showed nonsignificant im -provement in OS favoring bevacizumab,Fojo said, “Nonsignificant improvementis no improvement.” He added that itwas unusual for a study to reflect majordiscordance between PFS and OS. Fojo and other researchers published a
report in Lancet Oncology last year thatreviewed major studies published since1996 with a statistically significant PFSor OS and found “tight correlationbetween the two.” He therefore believesECOG 2100 is an outlier.Even if bevacizumab does improve PFS,
in Fojo’s opinion, PFS on its own is not animportant end point. “Delaying symptomsis a worthwhile goal, but delaying PFS doesnot equal delaying symptoms,” he said.Studies need to focus more on
whether the regimens used are harmingpatients. Fojo noted that in ECOG 2100,patients treated with bevacizumab expe-rienced more than twice as many adverseevents as the control group. Given itsfailure to improve OS and its cost, Fojosaid the toxicity is unacceptable, but heacknowledged that many breast cancerspecialists disagree. The FLEX trial,investigating cetuximab in mCRC, alsofound high rates of serious grade 3 and 4toxicities related to cetuximab, particu-larly skin reactions that are sometimesdisfiguring. With the growing use of oral treat-
ments, Fojo said it is important that studiesnot overlook the grade 1 and 2 toxicities.“The scale was developed for chemothera-py, but when you are taking a drug everyday for months on end, a grade 1 or 2 eventcan be very difficult.”While cost is relevant for drugs that
cause serious adverse effects but demon-strate minimal efficacy, Fojo said it comesdown to the notion that you do not harmpatients for little improvement in survival.Various attempts to combine therapieshave hurt patients without helping them,and Fojo called for an end to this “incre-mental approach” to treatment.Finding better treatments requires
determining the settings in which thedrugs work best but also the ones inwhich they do not work. Fojo said thiswould require major journals to givegreater weight to negative studies, whichare often relegated to second- and third-tier journals. It also requires expandingincentives for pharmaceutical companiesto take a more personalized approach todrug development, where rewards arelikely to be less lucrative. �
Making Cancer Drugs Worth the Cost By Christin Melton
“Delaying symptoms is aworthwhile goal, butdelaying PFS does not equal delayingsymptoms.”
—Tito Fojo, MD, PhD
How Costly Is Cancer Care in theUnited States?
The National Cancer Institute set out to answer this question last year andpublished results of their investigation in the January 2011 issue of the
Journal of the National Cancer Institute. The study’s authors point to flaws in previ-ous cancer cost estimates, many of which did little more than take figures from15 years ago and adjust them for inflation. When one considers the major transformations in cancer care in just the past
decade, it is not hard to see why these earlier estimates are unreliable. Using theSurveillence, Epidemiology, and End Results database to obtain incidence ratesand Medicare records for medical expenses, Mariotto and colleagues estimatedthe following:
US Cancer Care Costs in 2010: $124.57 billion
Projected US Cancer Costs in 2020:$157.77 billion-$207 billion**Lowest figure assumes constant incidence, survival, and cost; highest figure assumes increase for greater use of targeted therapies.
Most expensive cancers in 2010 (in billions):Breast: $16.50 Colorectal: $14.14 Lymphoma: $12.14 Lung: $12.12 Prostate: $11.85
For men and women whose deaths were caused by cancer in 2010, costs werehighest in the first 12 months after diagnosis and the last 12 months of life acrossall malignancies. The greatest increase in cost from the first year to the last yearwas for melanoma. For example, a woman aged <65 years accumulated $6057 inmedical costs in the year of diagnosis and $85,175 in the final year of life.
Source: Mariotto AB, et al. Projectons of the cost of cancer care in the United States: 2010-2020. J Natl CancerInst. 2011;103(2):117-128.
TON_April2011_v7_TON 4/7/11 10:50 AM Page 36

YOU INFUSE ANTHRACYCLINES,BUT ARE YOU PREPAREDFOR AN EXTRAVASATION?
TWO PRICE OPTIONS AVAILABLE
For more information, call 866-478-8274 or visit our website at www.totect.comTo order Totect®, contact one of our authorized distributors.
ASD Healthcare(800) 746-6273
Cardinal Specialty(866) 677-4844
McKesson/OTN(800) 482-6700
Oncology Supply(800) 633-7555
US Oncology(888) 987-6679
1 Mouridsen HT et al. Treatment of anthracycline extravasation with savene (dexrazoxane).Results from two prospective clinical multicentre studies. Ann Oncol 2007; 18:546-550.2 Totect® package insert. 3 Polovich M, White JM, Olsen, M (eds.). Chemotherapy and Biotherapy Guidelines and Recommendations for Practice (ed 3). Pittsburgh, PA, Oncology Nursing Society, 2009.4 Alexander M, Corrigan A, Gorski L, Hankins J, Perucca R. (eds). Infusion Nurses Society Infusion Nursing an Evidence-Based Approach (ed 3). Boston, MA, Infusion Nurses Society, 2009.5 Jacobsen J., et al. American Society of Clinical Oncology/Oncology Nursing Society Chemotherapy Administration Safety Standards. Oncology Nursing Forum, 2009; 36:651-658.© 2010 Topotarget USA. All rights reserved. TOT0112/7-10Totect and its logo mark are registered trademarks of Topotarget A/S
First and only FDA approved treatment for anthracycline extravasation.
Supplied as a convenient and accessible complete three day treatment kit for single patient use, which should be proactively stocked on-site and infused as soon as possible andwithin 6 hours of an anthracycline extravasation.
Demonstrates 98% overall e�cacy based on two biopsy-con�rmed clinical trials1,2 inreducing or avoiding surgical intervention (i.e., surgical debridement, plastic surgery and their related costs), thereby reducing postponement of a patient’s chemotherapy treatments and the avoidance of long-term consequences.
Cited in nursing guidelines.3,4 Extravasation management is now a chemotherapy administration safety standard.5
Totect® Kit (dexrazoxane) for injection is for intravenous infusion only. Totect is indicated for the treatment of extravasation resulting from intravenous anthracycline chemotherapy.
10:55:02 AM
TON_April2011_v7_TON 4/7/11 10:50 AM Page 37

Rx onlyTotect® is a registered trademark of Topotarget A/SUS Patent No. 6,727,253B2NDC 38423-110-01
Manufactured by:Ben Venue Laboratories, Inc.Bedford, OH 44146
Hameln Pharmaceuticals GmbH31789 HamelnGermany
Manufactured for:Topotarget A/SFruebjergvej 3DK-2100 CopenhagenDenmark
TOT0112/7-10© 2010 Topotarget USA
www.totect.com
Totect® – Brief prescribing information Please refer to the package insert for full prescribing information. Each Totect carton contains 10 vials of Totect® (dexrazoxane for injection) 500 mg and 10 vials of 50 mL diluent. Indication: Treatment of extravasation resulting from IV anthracycline chemotherapy. Dosage and administration: Totect is a cytotoxic drug. Vial contents must be mixed and diluted before use. Totect should not be mixed or administered with any other drug during the infusion. Administration of Totect should begin as soon as possible and within 6 hours following the anthracycline extravasa-tion. Totect should be given as an intravenous (IV) infusion once daily for 3 consecutive days. The dose of Totect is based on the patient’s body surface area: day one, 1000 mg/m2; day two, 1000 mg/m2; day three, 500 mg/m2. For patients with a body surface area of > 2 m2, a dose of 2000 mg should be given on days 1 and 2, and a dose of 1000 mg should be given on day 3. Treatment on Day 2 and Day 3 should start at the same hour (+/- 3 hours) as on the �rst day. The Totect dose should be reduced 50% for patients with creati-nine clearance values of <40 mL/minute. Cooling procedures such as ice packs should be removed from the a�ected area at least 15 minutes prior to Totect administration. Totect (dexrazoxane for injection) must be reconstituted with diluent supplied in the carton. The patient’s Totect dose is diluted in 0.9% 1000 mL NaCl prior to administration. Procedures for proper handling and disposal of anticancer drugs should be considered. Several guide-lines on this subject have been published.3-5 Direct contact of Totect® with the skin or mucous membranes prior to and following reconstitution should be avoided. If contact occurs, wash immediately and thoroughly with water. Contraindications: None.Warnings and Precautions: Myelosuppression: treatment with Totect is asso-ciated with leukopenia, neutropenia, and thrombocytopenia. Hematological monitoring should be performed. Use in Pregnancy: Pregnancy Category D. Totect can cause fetal harm when administered to a pregnant woman. There is no adequate information about the use of Totect in pregnant women. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. Adverse reactions: The most common adverse reactions (≥ 16%) are nausea, pyrexia, injection site pain and vomiting.
Drug Interactions: No drug interactions have been identi�ed. Based on anecdotal reports concurrent use of topical dimethyl sulfoxide (DMSO) at the site of tissue injury may reduce the benefit of Totect. Additionally, nonclinical studies using a mouse model that simulates extravasation of anthracyclines has shown that concomitant treat-ment with topical DMSO decreases the efficacy of systemic dexrazoxane. Use in Speci�c Populations: Nursing Mothers: Discontinue drug or nursing, taking into consideration the importance of drug to the mother. Renal Impairment: Reduce the Totect dose by 50% In patients with creatinine clearance values <40 mL/min. Pediatric Use: The safety and e�ectiveness of Totect in pediatric patients have not been established. Geriatric Use: This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Be-cause elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function. Overdosage: There are no data on overdosage. There is no known antidote for dexrazoxane. Carcinogenesis, Mutagenesis, Impairment of Fertility: The carcinogenic potential of dexrazoxane has not been investigated. Nevertheless, a study by the National Cancer Institute has reported that long term dosing with razoxane (the racemic mixture of dexrazoxane, ICRF-187, and its enantiomer ICRF-186) is associated with the development of malignancies in rats and possibly in mice. Dexrazoxane was not mutagenic to bacteria in vitro (Ames assay), but caused signi�cant chromosomal aberrations in mammalian cells in vitro. It also increased the formation of micronucleated polychromatic erythrocytes in mice. Thus, dexrazoxane is mutagenic and clastogenic. The possible adverse effects of Totect on the fertility of humans and experimental animals, male or female, have not been adequately studied. Testicular atrophy was seen with dexrazoxane administration at doses as low as 30 mg/kg weekly for 6 weeks in rats (about 1/5 the human dose on a mg/m2 basis) and as low as 20 mg/kg weekly for 13 weeks in dogs (about half the human dose on a mg/m2 basis).
TON_April2011_v7_TON 4/7/11 10:50 AM Page 38

March/april 2011 I VOl 4, NO 2 39www.TheOncologyNurse.com
Guidelines
diately applicable to clinical practicefor patients with breast cancer,announced Robert W. Carlson, MD,Stanford Comp rehensive CancerCenter, Palo Alto, California, whoserved as chair of the breast cancerpanel. Some of the leading cancerinstitutions that inform the NCCNguidelines have already implementedmany of these recommendations.
Despite the recent controversy regard-ing decision by the US Food and DrugAdministration (FDA) to rescind theindication for bevacizumab (Avastin) inpatients with metastatic breast cancer(MBC), the NCCN reaffirmed its sup-port for using a doublet of bevacizumaband paclitaxel for this population.
Carlson said the panel decided to keepthe combination of bevacizumab andpaclitaxel in the guidelines as a treat-ment option based on the fact that thedata had not changed. “If the data werecompelling 2 years ago, [they are] com-pelling enough today,” he said. Thepanel added a footnote acknowledgingthat the use of this regimen does notimprove overall survival (OS) and only“modestly improves time to progressionand response rates.” Carlson said panelmembers were less confident of the dataon combining bevacizumab with otherapproved chemotherapy agents.
The updated guidelines also reflectrecent FDA approvals of eribulin(Halaven) monotherapy for womenwith MBC who have received at least2 prior chemotherapy regimens, in -cluding a taxane and an anthracycline,and denosumab (Xgeva) to help pre-vent skeletal-related events in patientswith solid tumors that have metasta-sized to the bone.
Eribulin, a cytotoxic agent, became a“preferred” agent in MBC based on finaldata from the EMBRACE study, inwhich 762 patients were randomized toeribulin or treatment of physician’schoice (TPC). Median OS was 13.1months in the eribulin arm versus 10.6months in the TPC arm, representing a19% reduction in risk with the newagent (P = .041). The rate of 1-year OSwas 53.9% in the eribulin arm comparedwith 43.7% for the TPC arm. Sig -nificantly more patients in the eribulinarm experienced grade 3/4 neutropenia,leukopenia, and peripheral neuropathy,but study investigators de scribed adverseevents as manageable.
The inclusion of denosumab wasbased on its approval following phase3 trial data showing that patients ran-domized to denosumab experienced23% fewer skeletal-related events(SREs) than patients given zoledronicacid (Zometa; P = .001). Denosumabalso delayed the time to first onstudySRE by 18% versus zoledronic acid
(P = .001). Rates of OS and disease-free survival (DFS) were similar in thestudy arms.
Translational FindingsThe panel recommended that any
work-ups for metastatic lesions seek todetermine the hormonal and HER2 sta-tus of the metastases “if unknown, orig-inally negative, or not over-expressed.”This was based on a growing body ofdata showing discordance between hor-monal status of the primary tumor andmetastases. For example, a study pre-sented at the American Society ofClinical Oncology annual meeting in2010 identified several cases in whichthe hormonal status of the patient’s livermetastases did not match the hormonalstatus of her primary tumor. The findingsresulted in treatment changes for >12%of patients. “This recommendation islikely to get stronger as these data are for-mally published,” Carlson said.
Representing a significant change incurrent clinical practice, the NCCNguidelines now advise against completeaxillary lymph node dissection forwomen with clinically node-negativeT1-T2 breast tumors and fewer than 3involved sentinel lymph nodes whoundergo surgery and radiation therapy.Carlson said the recommendation isbased on data from a single randomizedtrial, the landmark ACOSOG Z0011study. Investigators found no differencein rates of locoregional recurrence,DFS, and OS between patients whounderwent complete axillary lymphnode dissection and those who had sen-tinel lymph node dissection. The rec-ommendation applies only to patientswho match the well-defined character-istics observed in the subset of patientswho formed the study population.
The panel considered whether to rec-ommend clinicians test patients for theCYP2D6 polymorphism prior to pre-scribing tamoxifen but decided against it.Panel members noted significant discrep-ancies between major studies investigat-ing whether this mutation is associatedwith tamoxifen resistance. “The currentNCCN guidelines are silent on this
issue. Oncologists should interpret thisas a recommendation not to performCYP2D6 testing at this time,” saidCarlson.
Prostate CancerIn updating guidelines for prostate
cancer, the panel reportedly spent con-siderable time weighing whether thedata favor active surveillance or immedi-ate treatment for certain patient popula-tions. James L. Mohler, MD, RoswellPark Cancer Institute, Buffalo, NewYork, discussed the NCCN’s recommen-dation to monitor more rigorously menwho opt for active surveillance. “TheNCCN remains concerned about over-diagnosis and overtreatment of prostatecancer, as growing evidence suggests thatovertreatment commits too many mento side effects that outweigh a very smallrisk of prostate cancer death,” he said. Healso reviewed new treatment options foradvanced prostate cancer.
Active Surveillance OK—for SomeActive surveillance, also termed
watchful waiting, is a viable option forpatients whose risk of progression is lowto very low. The “very low risk” categoryis reserved for men with clinically signif-icant prostate cancer, and the 2010guidelines incorporated strict criteria fordetermining which patients meet thisdesignation. Per 2010 guidelines, activesurveillance was considered suitable formen identified as “very low risk” andmen considered “low risk” who have alife expectancy <10 years.
The 2011 updates to the guidelinesincrease the level of monitoring recom-mended for men in the “very low risk”category whose life expectancy is <20years. Men who elect this approachshould receive the following:
• Prostate-specific antigen (PSA)tests every 6 months
• A digital rectal examination at leastevery 12 months
• Repeat biopsies as often as every 12 months.
Mohler outlined challenges in deter-mining whether some men with prostatecancer should get active surveillancerather than treatment. Large clinicalstudies examining this question haveapplied different criteria for active sur-veillance and disease progression, mak-ing it difficult to reconcile findingsbetween series. Concerns also remainabout overtreatment rates and the clini-cal risks associated with biopsies.
“Ultimately, this decision must bebased on careful, individualized weight- ing of a number of factors and is anoption that needs to be thoroughly dis-cussed,” he said. Mohler added thatmore clinical research is required toanswer this question definitively.
New Therapeutic Options:Sipuleucel-T, Cabazitaxel,Denosumab
For men with advanced metastaticcastration-resistant prostate cancer(CRPC), the panel voted to add sip-uleucel-T (Provenge) and cabazitaxel(Jevtana) as new therapeutic options.The FDA approved both treatments in 2010, after studies showed theyimproved OS.
Sipuleucel-T, an autologous cellularimmunotherapy, is classified as a cate-gory 1 recommendation, which meansthe evidence is strong and panel mem-bers concurred on including the drug.“It is appropriate as salvage treatmentfor patients with CRPC who haveminimally symptomatic disease, a per-formance status of 0 or 1, and a lifeexpectancy of at least 6 months,”Mohler said. The relative risk for deathwith sipuleucel-T was 22%, accordingto a study by Kantoff and colleaguespublished in the New England Journalof Medicine last year (P = .03). It didnot improve disease progression. Ser -ious adverse effects were minimal, butmany patients had immune-modulatedreactions.
Cabazitaxel, a taxane, was approvedin conjunction with prednisone as a sec-ond-line option for men with meta -static CRPC that recurred followingtherapy with a docetaxel (Taxotere)-based chemo therapy regimen. In theTROPIC study, men who receivedcabazitaxel plus prednisone saw a 2.4-month improvement in OS comparedwith men treated with mitoxantrone(P <.001).
As was the case with the breast can-cer guidelines, the NCCN added deno-sumab as an alternative to zoledronicacid for the prevention of SREs inpatients with bone metastases. Mohlersaid selecting an agent for bone protec-tion depends on whether the patienthas underlying comorbidities or hasreceived zoledronic acid previously.Denosumab did not improve OS in menwith prostate cancer but did demon-strate superiority to zoledronic acid on
NCCN Updates Treatment Guidelines... Continued from cover
Continued on page 40
Robert W. Carlson, MD
James L. Mohler, MD
TON_April2011_v7_TON 4/7/11 10:50 AM Page 39

40 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Guidelines
multiple end points, including delayingtime to first onstudy SRE.
Non–Small Cell Lung CancerThe guideline updates provide recom-
mendations on the need to determinethe histologic subtype of non–small-celllung cancer (NSCLC) tumors and con-duct genetic tests in some patients beforeselecting a therapeutic regimen. David S. Ettinger, MD, Sidney Kimmel Com -p rehensive Cancer Center at JohnsHopkins School of Medicine, Baltimore,Maryland, de scribed the changes as piv-otal. “We are heading toward the era ofmutation driving the therapy, and it’sextremely important for our patients,”said Ettinger. In 2011, he added,“Histology matters and NOS [not other-wise specified] is unacceptable.” When evaluating patients with recur-
rent or metastatic NSCLC for systemictherapy, the molecular diagnostics sec-tion of the 2011 guidelines recommendsestablishing the histologic subtypebefore testing for genetic mutations(Figure). Ettinger said all patients withadenocarcinoma should undergo molec-ular testing. Testing for epithelial growth factor
receptor (EGFR) is a category 1 recom-mendation for patients with adenocarci-noma or tumors of large cell histologyand patients with NSCLC NOS. EGFRtesting is not recommended in cases ofsquamous cell carcinoma.In addition to updating information
on EGFR and KRAS gene status, theguidelines discuss the EML4-ALK genetranslocation. It is estimated that aber-rations of EGFR, KRAS, and ALK drive>60,000 new cases of NSCLC in theUnited States each year, and each is animportant predictor of response to vari-ous targeted therapies. Crizotinib, a novel agent that targets
EML4-ALK, has been submitted to theFDA for approval. It has the potentialto improve prognosis for the 5% to 10%of patients positive for the EML4-ALKtranslocation. A recent phase 2 clinicaltrial of EML4-ALK–positive patientswith adenocarcinoma found robust,durable responses to crizotinib, andEttinger said updated findings from thisstudy will be important. No standardmethod exists to detect the EML4-ALKtranslocation, but he said studies arelooking at polymerase chain reaction,immunohistochem istry, and fluorescencein situ hybridization.For patients with adenocarcinoma
who progress or are resistant to first-linetherapy with erlotinib (Tarceva), theguidelines have added bevacizumab(Avastin) plus a platinum doublet as atreatment option. Ettinger said combin-ing bevacizumab with paclitaxel and car-boplatin might be effective for patients
with tumors of nonsquamous histologybut should not be used for squamous cellcarcinoma. He noted that bevacizumabis changing the landscape of treatmentfor stage IV NSCLC.
Non-Hodgkin LymphomaA new guideline on diagnosing and
treating posttransplant lymphoprolifera-tive disease (PTLD) and the reclassifi-cation of 2 therapies as category 1 rec-ommendations in follicular lymphoma(FL) are central to the guideline updatesfor non-Hodgkin lymphoma (NHL).Andrew D. Zelenetz, MD, PhD,Memorial Sloan-Kettering CancerCenter, New York, chaired the NHLpanel and discussed the revisions.
New Guidelines for TransplantComplication“PTLD has emerged as a significant
complication of solid organ and allo-geneic bone marrow transplantation,”said Zelenetz. Advances in our under-standing of the pathogenesis of PTLDand improvements in detection strate-gies are allowing clinicians to identifypatients at high risk of the disease earli-er. “The single biggest risk factor forPTLD is the presence of an Epstein-Barrvirus [EBV] mismatch between therecipient and the donor,” he said. “Thetime from organ transplant is criticallyimportant, with most of these lesionsdeveloping within the first year.”The NCCN guidelines specify tests
for PTLD and designate them as“essential” or “useful in selected cases.”Essential tests include histopathology,immuno phenotyping, and the EBV-encoded RNA in situ hybridizationassay. EBV viral load is deemed “usefulin selected cases.”
Depending on PTLD subtype, recom-mended treatment options includereducing immunosuppression, which iseffective in 23% to 64% of patients; sin-gle-agent rituximab (Rituxan), associat-ed with a response rate as high as 90% inpatients with early and polymorphiclesions; and gancyclovir or anotherantiviral prophylaxis for EBV-positivepatients. Although chemoimmunothera-py is also an option, Zelenetz said, “Iwould reserve chemoimmunotherapy forpatients in whom other, simpler maneu-vers have failed.”
Stronger Evidence for FollicularLymphoma RegimensIn the FL section of the guidelines,
the combination of bendamustine(Treanda) and rituximab (B-R) wasupgraded to a category 1 recommenda-tion for first-line treatment. A pivotaltrial compared B-R with standard ther-apy using cyclophosphamide, doxoru-bicin, vincristine, prednisone, and ri -tux imab (CHOP-R). B-R was as sociatedwith significant improvement in pro-gression-free survival (PFS) and the rateof complete response versus CHOP-R;OS was similar in both trial arms.Consolidation with 90Y ibritumo -
mab tiuxetan (Zevalin), a radiotherapyagent, followed by rituximab mainte-nance therapy was also reclassified as acategory 1 recommendation for treat-ment after first remission. Patients onthis regimen had prolonged PFS but noimprovement in OS.Because “no maintenance strategy in
FL has yet demonstrated a benefit inOS,” Zelenetz said observation remainsan appropriate option in the NCCNalgorithm for initial treatment of thedisease. He emphasized the importance
of individualized treatment planning forpatients with FL.
Chronic Myelogenous LeukemiaTwo newer tyrosine kinase inhibitors
(TKIs) received new indications asfirst-line treatment options for chronicmyelogenous leukemia (CML) in thepast year. Susan O’Brien, MD, theUniversity of Texas M. D. AndersonCancer Center, Houston, said theNCCN panel updated guidelines toinclude nilotinib (Tasigna) and dasa-tinib (Sprycel) as options for patientswith newly diagnosed Philadelphiachromosome–positive CML. Studiesshow dasatinib and nilotinib are asso-ciated with significantly higherresponse rates than imatinib (Gleevec)at 12 months and fewer patients treat-ed with these agents progressed toaccelerated phase or blast crisis. Data from the ENESTnd study,
reported at the 2010 annual meeting ofthe American Society of Hematology,showed that >60% of patients withnewly diagnosed CML had achievedmajor molecular response at 24months with nilotinib compared with37% of patients treated with imatinib.Less than 2% of nilotinib-treatedpatients progressed to acceleratedphase or blast crisis, experienced by4% to 6% of patients in the imatinibarm. “This is the most clinically rele-vant data in the short-term, becausetransformation heralds a very poorprognosis,” said O’Brien. The phase 3 DASISION study com-
pared dasatinib, an SRC inhibitor,with imatinib in patients with newlydiagnosed CML in the chronic phase.At a median of 12 months’ follow-up,patients in the dasatinib arm weremore likely to have experienced majormolecular response and complete cyto-genetic response than patients treatedwith imatinib. O’Brien said trials indicate these
newer agents offer nearly identicalimprovements in short-term end points,although their ultimate effect on PFSand OS has not been determined.Adverse effects with both agents are con-sidered manageable. With 3 approvedfirst-line agents, oncologists have theoption of starting patients on one of thenewer drugs at diagnosis or initiatingtreatment with imatinib and switchingto nilotinib or dasatinib in the second-line. Both have proven highly effectivein patients resistant to or intolerant ofimatinib who do not have the T315Imutation, which renders patients resis t-ant to all available TKIs. �
These and other guidelines are availablefree of charge to registered users of theNCCN Website at www.nccn.org.
NCCN Updates Treatment Guidelines... Continued from page 39
Unknown, 42%
KRAS, 30%
EGFR, 15%
EML4-ALK, 5%
MEK, 1%PIK3CA, 1%FGFR4, 2%BRAF, 2%
HER2, 2%
Figure. Frequency of Oncogene Mutations in Non–Small Cell Lung Cancer
TON_April2011_v7_TON 4/7/11 10:50 AM Page 40

Medication Access Support.A cancer diagnosis presents many challenges for your patients— and for those who love and care for them. That’s why PatientOne offers reimbursement support and financial assistance for eligible patients who are prescribed Lilly Oncology products. It’s the kind of support that can make access to medication easier—and make a difference in the lives of your patients.
To learn more, visit www.LillyPatientOne.com or call 1-866-4PatOne (1-866-472-8663).
Your goal is to give him a cancer treatment that’s right for him.
When you choose a Lilly Oncology product, our goal is to make sure he has access to it.
Patient Assistance I Insurance Expertise I Claims AppealsMG69852 02/11PRINTED IN USA © 2011, Lilly USA, LLC. ALL RIGHTS RESERVED.
TON_April2011_v7_TON 4/7/11 2:03 PM Page 41

www.TheOncologyNurse.com42 March/april 2011 I VOl 4, NO 2
The Whole Patient
Managing Elderly Patients Who Have Comorbidities
Cancer treatment–induced diar-rhea (CTID) occurs in 50% to80% of patients receiving
chemo therapy and 50% of patientsundergoing radiotherapy. Older patients,women, patients on an irinotecan-con-taining regimen, and patients treated inthe adjuvant setting are at higher risk ofCTID, reported Kelly Markey, PharmD,BCOP. Markey is a clinical pharmacistwith the gastrointestinal tumor programat Moffitt Cancer Center in Tampa,Florida, and discussed CTID at the annu-al meeting of the Hematology/OncologyPharmacy Association.
“There are many different sourcesfor diarrhea in this patient popula-tion,” she said. It can be caused by sur-gery, nosocomial infection, treatment,graft-versus-host disease, and thepatient’s malignancy.
A diagnostic work-up for diarrhearequires obtaining a clinical history and adescription of the stool. “Stool descrip-tion is especially important, includingnot only the number of stools but thecomposition,” said Markey. “Are theywatery or bloody? Did they occur noctur-nally?” Patients should be checked forfever and asked if they have experienceddizziness, cramping, pain, or weakness.
“Sometimes fever can indicate infectionor even bowel obstruction,” she noted.Current medications or diet might alsocontribute to diarrhea.
Persistent diarrhea requires a stoolwork-up, complete blood count, andassessment of electrolyte levels. Markeysaid an abdominal examination is alsonecessary, as is an endoscopy in somecases, to check for Clostridium difficile orinflammatory bowel disease. “Noso -comial infections are most often associ-ated with C difficile,” she said. Otherculprits include Salmonella, Shigella,Campylobacter, and Escherichia coli. Fordiarrhea lasting >7 days, “You need tostart thinking about your protozoa.”
Patients meeting National CancerInstitute criteria for grade 1/2 persistentdiarrhea but who do not have fever,dehydration, neutropenia, or blood intheir stool can be seen at the office.Patients with grade 3/4 diarrhea requirehospital admittance, even if they haveno other symptoms. Markey said probi-otics, which contain live bacteria oryeast, secrete acids that lower the pHlevel in the gastrointestinal (GI) tract,which thwarts the growth of pathogenicbacteria. “They also secrete toxins tothese bacteria, such as hydrogen perox-
ide, and they inhibit the binding of thesebacteria to the GI tract,” she explained.Caution is recommended when usingprobiotics in patients who are immuno-compromised or have central venousdevices. Probiotics should not be used inpatients on an antifungal agent. A con-cern with probiotics is that they are notquality controlled by the US Food andDrug Administration.
Several antimotility agents are used inthe initial treatment of CTID. “Manytimes I find my patients haven’t maxi-mized use of their first-line agents, suchas loperamide, and we prematurely movethem to a second-line agent,” saidMarkey. “You want to make sure you’remaximizing your dosing.”
For patients with persistent diarrhea,long-acting and short-acting octreotideare available. “Long-acting wouldn’t beused in the refractory-treatment popula-tion, but it is being investigated as a pro-phylactic, particularly in the radiation-induced population,” she said. One studyfound continuous octreotide infusioneffective in patients with colorectal can-cer who were receiving 5-fluorouracil.Diphenoxylate, opium tincture, budes-onide, and cholestyramine resin areother options for CTID.
If C difficile is the culprit, metronida-zole or vancomycin are standard first-lineoptions. “The problem with these agentsis they can be efficacious up front, but20% to 30% of patients are going torecur within 60 days...the majority recurwithin 2 weeks,” said Markey. Severalnew drugs for C difficile are on the mar-ket. In 2010, a small study by Basu andcolleagues reported that 73% of pa -tients who were refractory to metronida-zole responded to rifamycin (Xifaxan). A2011 study by Louie and associates deter-mined that fidaxomicin (not yet ap -proved) was noninferior to vancomycinas initial therapy for C difficile; it wasassociated with a lower rate of recur-rence. Nitazoxanide (Alinia) is usedagainst protozoa with similar effective-ness to vancomycin. It is also activeagainst norovirus and rotavirus.
Persistent diarrhea can be a life-threatening complication of anticancertherapy. Even low-grade persistent diar-rhea has a negative effect on quality oflife. Persistent diarrhea requires promptinvestigation, particularly when accom-panied by fever. It is important to letpatients with cancer know when diar-rhea warrants calling their healthcareprovider or seeking hospitalization. �
Considerations for Cancer Treatment–Induced DiarrheaBy Christin Melton
The median age for someone toreceive a cancer diagnosis is 67years according to the Sur -
veillance, Epidemiology, and End Resultsdatabase and even higher for certainmalignancies. For example, many gas-trointestinal cancers are diagnosed inseptuagenarians. With the advancing ageand expanding waistlines of the US pop-ulation, the number of patients seen atoncology clinics who have multiplechronic conditions is also expanding.Said Rowena Schwartz, PharmD,BCOP, director of oncology pharmacyat Johns Hopkins Hospital in Balti -more, Maryland, and president of theHematology/Oncology Pharmacy As -sociation, “We know that as patientsage, there are more comorbidities; andas patients age, the instance of cancerincreases, so it makes sense that thosego together.”
Schwartz said elderly patients withcomorbidities often have worse out-comes with anticancer therapies and saidno one is certain why. “Is it because theyhave high comorbidities and they don’ttolerate treatments, or is it because wedose-modify to deal with the comorbidi-ties? Is it because they don’t present untiltheir disease is advanced because their
cancer symptoms are confused with thecomorbidities?” she asked. “We don’tknow why. The data in comorbiditiesand the data in geriatrics are not reallyplentiful,” explained Schwartz.
The COPIT (Cancer in the Oldest:Prevalence, Related-Illnesses, and Treat -ment Modalities) study looked at recordsfor 194,797 US military veterans aged>70 years with cancer (99.6% were men)to assess the rates of various comorbidi-ties in this aged population. Theresearchers found that 70% had hyper-tension, >50% had hyperlipidemia, 40%had heart disease, 25% had diabetes,21% had osteoarthritis, 17% were med-ically frail, 10% had depression, and 6%had dementia. Some patients fell intomore than 1 of these categories.
A single-institution study byWedding and colleagues found a highrate of comorbidity in adult patients with
cancer in all age demographics. Com -orbidities were severe in approximatelythree-quarters of the elderly patientscompared with half of the youngerpatients. The rate of severe comorbidi-ties was similar in the cohort of elderlypatients without cancer (79%).
Schwartz said a 2010 literature re viewby Lee and associates looked at 34 stud-ies and concluded that clinicians usedchemotherapy less often or at lower dosesfor patients who had comorbidities,regardless of the type or stage of cancer.More than two-thirds (69%) of the 29studies to report on overall survivalfound it was diminished in patients withcancer who had comorbidities. Theprevalence, range of comorbid condi-tions, and their effects on treatment andoutcomes point to the need for cliniciansto consider comorbidities when caringfor patients with cancer. Schwartz
believes this is something that must bedone on an individual basis, but also atthe clinical trial level.
“There are no clinical trials that lookat comorbidities and look at treatment inindividual populations,” Schwartz said.“We may need to look at specific comor-bidities in specific populations with spe-cific types of disease.”
Monitoring patients with comor-bidities involves more than askingquestions at a follow-up visit. Schwartzprefers to telephone patients, particu-larly when prescribing anticoagulationtherapies. “I like to do phone follow-ups because you can do it every dayand get a better picture.” That dailyinteraction is important for some ofthe highest risk patients because “peo-ple’s memories just don’t jive withwhat actually happens,” she said. Thisis especially true for elderly patients,who, weeks later, might not rememberto tell their clinician about a symptomthat seemed important at the time.Schwartz said monitoring an elderlypatient with comorbidities also re -quires engaging the people in theirlives who provide support. “Figure outwhere they live and who provides thatoverview of care.” —CM �
“I like to do phone follow-upsbecause you can do it every dayand get a better picture.”
—Rowena Schwartz, PharmD, BCOP
TON_April2011_v7_TON 4/7/11 2:03 PM Page 42

VELCADE and Millennium are registered trademarks of Millennium Pharmaceuticals, Inc. Other trademarks are property of their respective owners.
Millennium Pharmaceuticals, Inc., Cambridge, MA 02139
Copyright © 2010, Millennium Pharmaceuticals, Inc. All rights reserved. Printed in USA V-10-0196 11/10
TON_April2011_v7_TON 4/7/11 10:50 AM Page 43

care and, at the same time, remainsilent about a major health risk,” shesaid. Studies show intervention from aclinician nearly doubles the chances ofa patient succeeding in his or herattempt to quit smoking compared withpharmacologic interventions alone orself-help materials. Although medical oncologists often
tell smokers they should quit, Pruemersaid they do not always explain why.“Patients may think, ‘I’ve already gotcancer, what’s the reason to quit?’” Sherattled off several: Smoking and nico-tine exposure decrease the effectivenessof certain anticancer therapies, particu-larly erlotinib (Erbitux); tobacco useimpairs wound healing after surgery andincreases the risk of infection; and forpatients receiving radiotherapy, smokingis associated with greater epithelial dam-age in irradiated tissue and a higher inci-dence of mucositis. Perhaps the mostimportant reason to quit is that patientswho continue smoking have a higherrisk of second cancers, shorter survival,and worse quality of life.
The first step in getting a patient toquit is finding out how much theysmoke, which is not always easy. “Doyou know that 1 in 6 smokers reallydoesn’t tell the truth about how muchthey smoke?” Pruemer asked. Health -care providers need to be understand-ing when patients seem reluctant todiscuss their tobacco use. Pruemer rec-ommended highlighting the linkbetween smoking and their cancer tomotivate them to take the next steps.“If you don’t have a [tobacco cessation]program, refer them to one you knowabout. They are out there.”A successful program addresses the
physiological and behavioral aspects ofdependence. “These two have to worktogether. ...We can’t just hand thepatient a box of patches and expectthem to be able to quit,” said Pruemer. People highly dependent on ciga-
rettes find it harder to quit. Thisincludes someone who smokes >1 pack aday or who lights up within 30 minutesof waking. People with psychiatric disor-ders or a history of chemical dependencyalso struggle. Some patients are con-vinced that cigarettes have positiveeffects, like keeping them calm or pre-venting weight gain. Pruemer said clini-
cians must dispel these myths anddescribe how cigarettes operate on themphysiologically. Another component ofbehavioral modification is identifyingtheir smoking triggers. “Make sure theyunderstand the difference between aphysical craving and habit.”
Before selecting a pharmacologic aid,Pruemer recommended working withthe patient to establish their goals, suchas relieving withdrawal symptoms, con-trolling urges, and abstinence. Mostpatients have tried quitting before, soshe recommended finding out what
worked and what did not work in thoseattempts. The pharmacologic optionsare essentially equal in effectiveness,and which one to use is primarily a mat-ter of preference. Nicotine replacement therapy (NRT)
comes in various forms and is a popular
MC49941 06-10
www.TheOncologyNurse.com44 March/april 2011 I VOl 4, NO 2
The Whole Patient
Are You Talking to Patients About Smoking Cessation? Continued from cover
Health care providers needto be understanding whenpatients seem reluctant todiscuss their tobacco use.
TON_April2011_v7_TON 4/7/11 10:50 AM Page 44

option, but it should be used with cautionin patients with underlying cardiovascu-lar disease. Pruemer said the standarddose might not work for heavier smokers.“I have a lot of patients that come in andthey smoke 3 or 4 packs a day—I had alady who smoked 5 packs a day. If yougive them the equivalent of 1 pack ofnicotine, they’re not going to quit,” she
explained. A Mayo Clinic study in 1995demonstrated higher quit rates at endpoints of 8 weeks, 6 months, and 1 year inpatients using a 44-mg patch comparedwith the 11-mg or 22-mg patches.Although researchers have not found anincrease in adverse effects when using thedose equivalent of 2 patches, Pruemersaid, “I would not do this unless patients
are under the guidance of a physicianthat you’re working with.”
Prescription options consist of bupro-pion SR (Zyban) and varenicline.“Bupropion works by increasing thecentral nervous system levels ofdopamine, which makes patients feelbetter.” The drug is started 1 week priorto the scheduled quit date. Patients take
150 mg once daily for 3 days and thenincrease to twice-daily dosing for theremaining 7 to 10 weeks of therapy. Thedrug increases the risk of seizures, andPruemer advised extreme caution forpatients with a history of brain surgery ortrauma, patients taking medications thatincrease seizure risk, and patients withsevere cirrhosis. Bupropion is contraindi-cated in patients with bulimia, anorexianervosa, or seizure disorders, and in thosewho are abruptly quitting alcohol orsedatives.
Varenicline binds to nicotine recep-tors, blocking the usual dopaminergicboost patients get from smoking. It alsohelps alleviate withdrawal symptoms. Aswith bupropion, patients should start thedrug 1 week prior to their quit date; itshould be taken with food. The dose istitrated to 1 mg twice daily by the start ofthe second week. This dosing is contin-ued for 10 weeks. Pruemer cautionedthat varenicline increases the risk ofdepression.
Patients unable to quit on a single-agent option might be candidates fortherapy that combines NRT agents oruses an NRT agent with bupropion.Varenicline should not be used as part ofa combination regimen. Another optionis to continue on pharmacologic therapybeyond the standard treatment period.
During the question and answer ses-sion, Pruemer was asked whether pa -tients with rapidly progressive disease orin palliative care should quit. “Eventhose patients are going to have a higherrisk of pneumonia and more complica-tions at the end of life, and their qualityof life is going to be poorer. There’s plen-ty of data that still recommends theyshould be quitting,” she responded.
The benefits of smoking cessation areimmediate and long-term for patientswith cancer, and Pruemer said, “It canbe one of the single most effectivestrategies to improve outcomes for ourpatients.” Individuals who work atplaces that do not offer smoking cessa-tion programs can still help theirpatients who smoke by initiating theconversation and then referring them toan established program. �
March/april 2011 I VOl 4, NO 2 45www.TheOncologyNurse.com
The Whole Patient
Patients unable to quit ona single-agent optionmight be candidates fortherapy that combinesNRT agents or uses anNRT agent with bupropion.
ADVERTISEMENT
* Crawford J, et al. J Natl Compr Canc Netw. 2008. Nationwide, prospective registry study conducted in 115 community-based, randomly selected, IRB-approved sites, evaluating the incidence and timing of neutropenia and neutropenic events in the first cycle and in cycles 2–3 across major tumor types.
References: 1. Crawford J, et al. J Natl Compr Canc Netw. 2008;6:109-118. 2. Kuderer N, et al. Cancer. 2006;106:2258-2266. 3. Lyman G, et al. J Clin Oncol. 2003;21:4524-4531. 4. Lyman G, et al. J Clin Oncol. 2004;22:4302-4311. 5. Lyman G, et al. J Natl Compr Canc Netw. 2009;7:99-108. 6. Link B, et al. Cancer. 2001;92:1354-1367. 7. Picozzi V, et al. Oncology. 2001;15:1295-1306.8. Bonadonna G, et al. N Engl J Med. 1995;332:901-906. 9. Bonadonna G, et al. BMJ. 2005;330:217-222. 10. Chirivella I, et al. Breast Cancer Res Treat. 2009;114:479-484. 11. Kwak L, et al. J Clin Oncol. 1990;8:963-977. 12. Bosly A, et al. Ann Hematol. 2008;87:277-283.
What happens to the patient caught in the complications of chemotherapy-induced neutropenia?
Figure. Overall survival by average relative dose intensity (ARDI)
0.0
0.4
0.6
0.7
0.8
Years post-chemotherapy
0.3
0.5
0.9
1.0
ARDI: ≤ 85%
ARDI: 86% to ≤ 90%
ARDI: > 90%
0 1 2 3 4 5 6 7 8
Esti
mat
ed s
urv
ival
Retrospective chart data of overall survival in 210 patients treated with CHOP-21 according to average relative dose intensity (ARDI). CHOP = cyclophosphamide, doxorubicin, vincristine, and prednisone.
Adapted from Bosly A, et al. Ann Hematol. 2008.
For patients with NHL, age > 60 years, advanced disease stage and poor performance status were associated with relative dose intensity < 85%.4
You can intervene for your next patient A comprehensive risk assessment protocol is critical to helping you identify patients at risk for clinically significant febrile neutropenia.
C onsider the risk of the chemotherapy regimenie, chemotherapeutics administered, alone or in combination
A ssess patient risk factorseg, age ≥ 65 years, poor performance status
R isk increases with more comorbiditieseg, COPD, cardiovascular disease, diabetes mellitus
Evaluate each patient prior to every cycle
To request a febrile neutropenia Risk Assessment Checklist, email: [email protected].
Assess the risk.
Consider your last patient with neutropeniaDid your patient experience any consequences from severe or febrile neutropenia? According to a prospective registry study of 2,692 patients encompassing major tumor types, 29.3% overall were impacted by severe or febrile neutropenia in the first 3 cycles of chemotherapy, leaving a large opportunity for risk assessment intervention. This study also showed that the risk of severe or febrile neutropenia was greatest in the first cycle. That risk continued in subsequent cycles.*1
Febrile neutropenia–related hospitalization can lead to mortalityIn a retrospective database analysis (N = 41,779), the inpatient mortality rate for febrile neutropenia–related hospitalization was 9.5%. This inpatient mortality rate was directly related to the number of major comorbidities present at the time of admission. Major comorbidities were defined as any major organ dysfunction requiring diagnostic or therapeutic intervention. Inpatient mortality ranged from 2.6% (556/21,386) for patients with no comorbidities to over 50% (181/358) for those with 4 or more.2
Optimal chemotherapy delivery was shown to improve survival in some tumor typesRetrospective studies have shown that dose delays and reductions due to severe or febrile neutropenia may impact treatment plans and result in unfavorable outcomes for some diagnoses.3-7
While there are inherent risks associated with chemotherapy treatment, landmark studies in both non-Hodgkin’s lymphoma (NHL) and early-stage breast cancer have shown that closer adherence to standard doses is one factor that was associated with increased survival rates.8-11
A retrospective analysis demonstrated significantly longer median survival (7.08 years) for patients with NHL who received > 90% average relative dose intensity of CHOP-21 compared with those who received ≤ 90% (N = 210; P = 0.002) (see Figure).12
Multivariate analyses have identified several independent risk factors for reduced relative dose intensity. The risk factors for relative dose intensity < 85% among early-stage breast cancer patients included age, weight, and three-drug regimens (CAF or CMF).3
© 2010 Amgen. All rights reserved. MC49941 06-10
TON_April2011_v7_TON 4/7/11 10:50 AM Page 45

Geriatric case management shouldalways begin with a Comp -rehensive Geriatric As sessment,
said Demetra Antimisiaris, PharmD,GCP, FASCP, assistant professor withthe Department of Family Medicine &Geriatrics and director of GeriatricPharmacotherapy at the University ofLouisville School of Medicine inKentucky. In a presentation at the 2011annual meeting of the Hematology/Oncology Pharmacy As sociation, Anti -misiaris said many criteria must be con-sidered when assessing a patient’s func-tionality: nutritional status, activitylevels, medical and psychological states,environment, and gait and balance.Obtaining this baseline measure is criti-cal because commonly prescribed andover-the-counter medications often haveunanticipated effects on an elder’sbehavior or function.
Antimisiaris said medications—evenrun-of-the-mill drugs like ibuprofen—were never tested in this demographicprior to approval. “Older adults areunderrepresented in clinical trials,” shesaid, adding that exclusions for comor-bidities prevent many elderly patientsfrom participating. “Data is especiallysparse for individuals 75 and older.”
Antimisiaris cited an Alzheimer’sdrug trial as an example of how drugswind up being used in patients for whomthey were never tested. This particulartrial limited enrollment to individualswith Alzheimer’s and “no other neurode-generative disease,” she said. Because anAlzheimer’s diagnosis is typically onlyconfirmed at autopsy, Antimisiaris saidthe drug is likely going to be used inpatients with other types of dementia,causing unexpected toxicities.
Even if more drug trials included theoldest patients, applying the resultswould be challenging. “We becomemore diverse as we age,” she said,explaining that “a pediatric kidney is apediatric kidney, but a 65-year-old’skidney might be different from another65-year-old’s kidney depending on howthey lived their life as they aged.”
Complicating the ability to recog-nize when an elderly patient is havinga negative response to a drug or combi-nation of drugs is the range of nonspe-cific signs and symptoms they exhibit.“Elderly people don’t present with theclassic symptoms you might expect,”said Antimisiaris. One reason is that,as people age, protein levels diminishand the blood-brain barrier becomesincreasingly porous. As a result, manypatients will exhibit psychologicalchanges, like “agitation, manic behav-ior, change in effect, confusion, noteating, or not sleeping.”
Guidelines in hand, a physicianmight respond to a complaint ofinsomnia with a prescription for zolpi-dem (Ambien), when replacing or dis-continuing a drug in the patient’s cur-rent regimen could have resolved theproblem. “Being strong in geriatric med-ication management requires knowinghow unnecessary medication use hap-pens and how to recognize when amedication is causing problems,” saidAntimisiaris. “We’re so guidance driv-en [that] we’ve kind of lost the partabout being able to see toxicities whenthey’re right in front of us.” Shedescribed a huge gap between “thebench science and the bedside” andsaid providers must exercise clinicaljudgment when caring for elders.
“Polypharmacy is prevalent amongelderly patients,” Antimisiaris said,noting that guidelines often fail toaddress how drugs interact. Studiesshow total drug burden is important forthis patient population, and she point-ed to a 2007 study by Garfinkle andcolleagues. They found that cuttingthe number of drugs given to a group ofgeriatric patients in palliative care byan average of 2.8 improved outcomescompared with a control group ofpatients whose drug regimens stayedthe same. The 1-year mortality ratewas 21% in the study group versus 45%in the control arm, and only 11.8% ofpatients in the study group neededreferrals to acute care each year com-pared with 30% of patients in the con-trol group. Drug burden affects qualityof life, Antimisiaris said, with eachadditional unit negatively affectingphysical function and cognitive taskperformance. “Keep what you need,lose what you want. … Keep the war-farin, lose the Ambien.”
Antimisiaris outlined important con-siderations when medicating elderlypatients:
• Elders have decreased total bodywater, so use “baby doses” of water-soluble drugs to prevent excessivedrug concentrations.
• Elders typically have more body fat
and thus an increased risk of toxi- city when using fat-soluble orlipophilic drugs (psychotropics,vitamins A and E, some statins),which are slow to activate andaccumulate.
• Elders have decreased serum pro-tein levels and consequently a high-er rate of free drug, so treat to effi-cacy and not to levels.
• Almost 50% of elders are slowmetabolizers, associated with anincreased risk of adverse effectsand toxicity; don’t just assume thedrug is not working and thenincrease the dose.
• Watch for drug–drug interactionsand toxicities in patients treatedwith 1 or more drugs metabolizedalong the CYP3A4 pathway.
• Elders, especially those aged >85years, frequently have impairedkidney and renal function, so eval-uate total drug burden.
• Try to elicit from the patient infor-mation about changes in behavioror mood by asking questions like“Are you sleeping?” or “Are youstill doing [a favorite activity]?”;responses might indicate anadverse drug reaction.
Prescribing the right drugs is onlyone component of drug managementfor geriatric patients; adherence isanother. With the typical physician’soffice visit lasting only 7 minutes,Antimisiaris said, “nobody is testing[elderly patients’] literacy or cognitivefunction” to assess whether they arecapable of managing their drug regi-men. “Have the patient draw a clock,”she suggested. “That will tell youwhether they can handle taking anaspirin a day,” she said.
Antimisiaris warned that the comingyears are likely to bring an influx of eld-erly patients to oncology clinics. “Theelders are coming…they’re sicker, morefrail, and harder to manage,” she said.Before that happens, we must do moreto learn about needs specific to elderlypatients and to educate care teams onwhat we already know. �
www.TheOncologyNurse.com46 March/april 2011 I VOl 4, NO 2
The Whole Patient
BalloonKyphoplastyReduces Painfrom VertebralCompressionFractures
Managing Geriatric PatientsBy Christin Melton
In a randomized trial of patients withcancer who were suffering from verte-bral compression fractures (VCFs),
balloon kyphoplasty was associated withgreater pain relief and better quality oflife than nonsurgical care. According tothe authors, patients who receivedkyphoplasty relied significantly less onpain medication, bed rest, and walkingassistance 1 month after undergoing theprocedure.
James Berenson, MD, founder andpresident of the Institute for Myelomaand Bone Cancer Research in WestHollywood, California, led the multi- national Cancer Patient FractureEvaluation (CAFE) study, and resultswere published online in LancetOncology. In an interview with TheOncology Nurse-APN/PA, Berenson said,“Any cancer patient with a vertebralcompression, whether the cancer in -volves the vertebral body or not, wouldbe a candidate for this procedure.” Hesaid balloon kyphoplasty should be per-formed “without delay” as soon as asymptomatic VCF is diagnosed. Balloonkyphoplasty might be contraindicated,however, in patients with advanced dis-ease who are not expected to survivelong or those who are considered poorsurgical risks.
The study enrolled 134 adults withcancer, each of whom had suffered 1 to3 VCFs. More than half the patients(60%) had a diagnosis of multiplemyeloma or breast cancer, both ofwhich are associated with bone com-plications. Investigators randomized 70patients to undergo the balloon kypho-plasty procedure, along with the optionto use nonsurgical care for pain asneeded. The remaining 64 patientsmade up the control group, and thesepatients could only use nonsurgicalmethods of relieving pain. All patientswere allowed to continue their cancertreatments as prescribed.
To measure improvement in back-specific functionality, the researchteam administered the Roland-Disability Questionnaire (RDQ) atbaseline and repeated it at a 1-monthfollow-up appointment. Using the RDQscale, 0 indicates no disability and 24indicates a maximum level of disability.At baseline, the mean RDQ score forpatients in the kyphoplasty group was17.6 compared with 18.2 for the control
“Being strong in geriatric medication managementrequires knowing how unnecessary medication usehappens and how to recognize when a medication iscausing problems.”
—Demetra Antimisiaris, PharmD, GCP, FASCP
TON_April2011_v7_TON 4/7/11 10:50 AM Page 46

group. At 1-month follow-up, RDQscores for the kyphoplasty group declinedby a mean of 8.3 points to 9.1 (P <.0001). In contrast, RDQ scores onlydeclined a mean of 0.1 points for thecontrol arm, falling to 18.0 (P <.0001).
Other standardized tests were used tomeasure pain, physical and mentalhealth, and performance status. The 10-point pain scale reflected a significantdrop of 3.8 points in pain levels for thekyphoplasty group at 7 days postproce-dure; this compared with a 0.3-pointdrop in pain levels for the control arm (P <.0001). At 1 month, end points con-tinued to favor balloon kyphoplasty.
At 1 year, pain assessments for thegroups began to converge, and no sig-nificant difference in pain levels wasobserved between the 2 arms. Berensonsaid data at the end of the trial werebiased because “only a small minorityof patients made it to that time point.”He noted that those patients in thestudy who were alive at 1-year follow-up likely had better quality of life ingeneral, particularly regarding painlevels, compared with the study popu-lation as a whole.
Berenson and colleagues notedthat 94% of patients treated withkyphoplasty had been taking painmedications prior to the procedure.At a follow-up assessment 1 monthafter undergoing the procedure, in -vestigators found the proportion ofpatients using pain medication haddeclined to 52%. In the control arm,however, the use of pain medicationremained consistent.
After 1 month, patients initially ran-domized to the control group were per-mitted to cross over into the kyphoplastygroup, and 38 patients decided to do so.This subgroup of 38 patients experiencedimprovement in pain and function atsimilar rates and levels to the patientsassigned to the original kyphoplastygroup. One-year assessments of patientsin the initial kyphoplasty group andpatients in the kyphoplasty crossovergroup showed that they had maintainedtheir 1-month improvements in painand function.
The authors hypothesized that theimproved function afforded by balloonkyphoplasty might contribute to a reduc-tion in the risk of events such as decubi-tus ulcers and pneumonia, which are not
uncommon in patients who have cancer.“A procedure that effectively treatsVCFs for patients with cancer mightconfer clinical and quality-of-life bene-fits beyond treatment of the fractureitself,” they wrote.
Balloon kyphoplasty is associatedwith few adverse effects. Berenson said,“Very rarely, there can be significantextravasation of the cement outside ofthe cavity in which it is intended.”
The study was limited by its shortduration and its open-label design. In anaccompanying editorial, David Schiff,MD, and Mary E. Jensen, MD, Uni -versity of Virginia, Charlottesville, saidbecause of the study design, a placeboeffect could not be ruled out. They saidadditional trials should be conductedbefore adopting the costly surgical proce-dure as standard practice.
Medtronic, which makes the Kyphon
balloon kyphoplasty device used in thestudy, provided funding. Berenson and other authors have
received consulting fees, honoraria, andresearch funding from Medtronic. Severalauthors were Medtronic employees, andone disclosed relationships with Synthes,Orthofix, and Alphtec. Schiff has receivedconsulting fees from Genentech, andJensen acknowledged consulting fees fromKuros Biosurgery.—CM �
March/april 2011 I VOl 4, NO 2 47www.TheOncologyNurse.com
The Whole Patient
How do you manage this common condition when cancer patients may not mention it?
You talk about it. If left untreated, Dry Mouth
can lead to some fairly serious dental problems, in
addition to the day-to-day discomfort. But with all
your cancer patients are going through, they may
think that their dry mouth discomfort is not worth
mentioning. It’s important to ask them specifi cally
about dry mouth symptoms.
Some patients fi nd relief by constantly sipping
water. But the relief doesn’t last, because water just
wets the mouth rather than lubricates it the way
saliva does. With its proteins and enzymes, saliva
is essential for protecting the mouth and teeth. So
when dry mouth symptoms are present, it’s essential
to identify them.
Then you can do something about it. Biotène,
with its patented LP3-system, helps to soothe dry
mouth discomfort and supplement some of saliva’s
natural defenses. And only Biotène offers products
in the 3 areas necessary to manage your patients’
dry mouth symptoms:
1. Soothe & Moisturize2. Daily Cleaning3. Saliva stimulation
Plus, Biotène can be used alongside your patients’
medications. Get them talking about their dry mouth
symptoms. And recommend Biotène to help make
their days a little more tolerable.
© 2011 GlaxoSmithKline Consumer Healthcare
Soothe & Moisturize Daily Cleaning(gel, spray, liquid) (toothpaste, mouthwash)
Saliva Stimulation(chewing gum)
www.biotene.com
How do you manage this common condition when How do you manage this common condition when DRY MOUTH
#1 FOR DRY MOUTH MANAGEMENT
Balloon kyphoplasty isassociated with fewadverse effects.
TON_April2011_v7_TON 4/7/11 10:50 AM Page 47

www.TheOncologyNurse.com48 March/april 2011 I VOl 4, NO 2
News in Review
Researchers from the NationalCancer Institute report that radi-ation therapy for a first cancer is
unlikely to lead to a second cancer diag-nosis later in life. Berrington de Gonzalezand associates conducted a retrospectivereview of data from the Surveillance,Epidemiology, and End Results cancer reg-istry for nearly 650,000 adults whoreceived a cancer diagnosis between 1973and 2002 and survived at least 5 years.Approximately 50% of patients receivedradiation, and only 8% of these (n = 3266)developed a second malignancy consideredattributable to the therapy (95% confi-dence interval [CI], 7%-9%).Almost all 650,000 patients were at
least 20 years of age at diagnosis and had1 of 15 tumor types commonly treatedwith radiation: rectal, lung, breast,prostate, cervical, testicular, endometri-al, brain, central nervous system, ocularand orbital, laryngeal, salivary gland,oropharyngeal, and soft tissue tumors.An estimated 60,000 patients, including42,000 given radiotherapy, developed asecond primary cancer, suggesting thatthe overall rate of second primary can-cers is low. The authors said at 15 years’ follow-
up, 5 excess cancers occurred per every
1000 patients whose initial cancers weretreated with radiotherapy (median fol-low-up, 12 years).Among patients who received radia-
tion, secondary cancer risk variedaccording to the initial type of cancer.The relative risk was lowest for womentreated for breast cancer, at 1.10 (95%CI, 1.07-1.13). Men treated for testicularcancer had the highest relative risk, at1.43 (95% CI, 1.13-1.84). Factors associ-ated with increased risk of a second can-cer included younger age at diagnosis ofthe first cancer and greater radiationexposure (>5 Gy) during therapy. Therisk increased as the patients aged.The authors ruled out second cancers
that occurred within 5 years of radiationtherapy as being treatment related. Theynoted that patients often have more fol-
low-up care in the first 5 years after treat-ment and were concerned that includingcancers diagnosed during this time framemight bias results.The investigators did not assess
whether the patients had other knownrisk factors for cancer, such as smokinghistory, hormonal therapy, obesity, andexposure to carcinogenic chemotherapydrugs. They did a subanalysis of patientswho did not receive chemotherapy, how-ever, and found consistent results. Mostpatients in the study received radiother-apy prior to widespread use of intensity-modulated radiotherapy, but the authorsbelieve studies will continue to showthat the benefits of radiotherapy out-weigh the risk of second cancers. Thestudy was published online in Lancet Oncology in March. �
Radiation Therapy for Initial Cancer CausesRelatively Few Second Cancers By Christin Melton
Factors associated with increased risk of a secondcancer included a younger age at diagnosis of thefirst cancer and greater radiation exposure (>5 Gy)during therapy.
APP Pharmaceuticals hasissued a voluntary recall of 5 lots of irinotecan hydro -
chloride injection (Camptosar) as aprecautionary measure. No adverseevents related to the recalled prod-ucts have been reported. The follow-ing lots have been recalled:• 870DE00301• 870CZ00301• 870DE00101• 870DE00201• 870DE00401APP issued the recall after receiv-
ing customer complaints associatedwith lot 870DE00301, in which par-ticulates were observed in the prod-uct solution. An investigation of thevials returned to the manufacturerestablished that the particulate mat-ter was a fungal microbial contami-nant. After consulting with the USFood and Drug Administration, andas a precautionary measure, all lotsproduced immediately before andafter lot 870DE00301 are beingrecalled. For complete details, visitwww.apppharma.com. �
Voluntary Recallof IrinotecanAnnouncedBy Dawn Lagrosa
Variation in Prescribing Instructions Confuses Patients on Multidrug Regimens
Every physician has a preferred wayof writing prescription instruc-tions, and pharmacists differ in
how they translate those instructions tothe pill bottle. A study published in theAnnals of Internal Medicine by Wolf andassociates found that the lack of a uni-versal medication schedule (UMS) tostandardize how prescriptions are writ-ten and filled contributes to poorpatient adherence and increases safetyconcerns. Elderly patients or thosewith low health literacy are moreprone to confusion when trying to fol-low a multidrug regimen.In a 2008 report, “Standardizing
Medication Labels,” the Institute ofMedicine (IOM) recommended imple-menting a UMS to reduce misunder-standings related to medication use.Noting that 90% of prescriptions requireno more than 4 daily doses, the IOMcalled for delineating 4 standard dosagetimes—morning, noon, evening, andbedtime—to help patients taking multi-ple drugs to consolidate doses. Reception
to the proposal was mixed, with calls formore research.To determine whether a UMS was
needed, investigators assessed the abilityof 464 patients aged 55 to 74 years toadhere to a hypothetical 7-drug prescrip-tion regimen. The patients were part of abroader study that incorporated a 2-hourinterview to evaluate their adeptness atperforming everyday health tasks. Most(84%) had at least 1 chronic health con-dition; approximately 61% were collegeeducated and an equal proportion hadhousehold incomes >$50,000.Researchers gave every patient pre-
scription bottles containing fake pillsand mock labels for 7 retired drugs; dos-ing instructions varied between thedrugs. Patients also received a pill boxwith 24 slots marked with consecutive 1-hour intervals, going from 12:00 AM to11:00 PM. Each patient was verballyinstructed to “imagine that your doctorhas prescribed you these medications. Iwould like you to please show me whenyou would take these medicines over the
course of 1 day,” and offered additionalinstruction as needed.Although the drugs could be neatly
consolidated into 4 dosing intervals,participants sorted them into an aver-age of 6 slots. Some consolidated theregimen into as few as 3 dosing periods,whereas others used as many as 14slots. One-third of patients indicated 7intervals each day for taking drugs;14.9% indicated 4 times or fewer.Labels for 3 drugs had identical dosing
instructions and could therefore havebeen taken simultaneously, yet one-thirdof patients failed to do so. Another 2drugs required thrice-daily dosing, with 1stipulating to take it with food and water.Only 50.5% of participants scheduledthem to be taken together. Another 2drugs needed to be taken twice a day; thelabel for one said “twice daily” and theother said “every 12 hours.” In all, 79%of patients failed to consolidate theminto concurrent dosing intervals.For drugs calling for twice-daily dos-
ing, an average of 10.3 hours elapsed
between doses (range, 1 hour to 18hours). For thrice-daily dosing, a mean of5.4 hours elapsed between the first andsecond doses and 6.5 hours between thesecond and third doses.Low health literacy—ascribed to
20.7% of patients—was the only factorthat independently predicted a greaterlikelihood of taking medications morethan 7 times per day. Patients with lowhealth literacy and no chronic condi-tions had the worst rate of efficient consolidation.The authors said strategies are need-
ed to help patients understand how totake prescriptions and how to consoli-date multiple prescriptions. They saidadopting a UMS could “unite medicaland pharmacological practice” andsuggested that an electronic healthrecords system could be used to facili-tate standardization in prescribing.They also recommended educatingproviders on how to identify patientslikely to have trouble adhering to acomplicated regimen.—CM �
TON_April2011_v7_TON 4/7/11 10:50 AM Page 48

TON_April2011_v7_TON 4/7/11 10:51 AM Page 49

Data published in the Lancet inMarch support the effective-ness of eribulin mesylate
(Halaven)—a microtubule inhibitor—in women with advanced breast cancerthat has progressed after several treat-ments. The US Food and DrugAdministration approved eribulin inNovember 2010 for metastatic breastcancer patients treated with at least 2chemotherapy regimens (an anthracy-cline and a taxane). As EMBRACEinvestigator Chris Twelves, MD, said lastyear at the American Society of ClinicalOncology annual meeting, this is the firstevidence that a chemotherapeutic agentcan improve overall survival (OS) in aheavily pretreated population.
The primary end point of EMBRACEwas a significant increase in OS, andthis was met, with eribulin improvingsurvival by 2.5 months. Median OS was13.1 months in the eribulin arm versus10.6 months in the treatment of physi-cian’s choice (TPC) group (hazard ratio[HR], 0.81; 95% confidence interval[CI], 0.66-0.99; P = .041). Following eribulin’s demonstrated
activity against breast cancer in phase1 and phase 2 studies, investigatorsenrolled 762 women from 19 coun-tries for this phase 3 trial. All partici-pants had locally advanced or recur-rent metastatic breast cancer and hadcompleted 2 to 5 chemotherapy regi-mens. In the study, 16% of womenwere HER2-positive and 19% hadtriple-negative disease, but resultswere not stratified according to can-cer subtype.Investigators randomized patients at
a 2:1 ratio to eribulin (n = 508; 1.4mg/m2 intravenously on days 1 and 8 ofa 21-day cycle) or TPC (n = 254).Median duration of treatment was 3.9months in the eribulin group, with59% of patients receiving at least 5cycles. Most (96%) patients in the
TPC arm received chemotherapy andcontinued treatment for a median of2.1 months; 9 patients took hormonalagents for a median of 1.0 month.
During the study, fewer deathsoccurred in the eribulin arm than inthe TPC group (54% vs 58%, respec-tively), and more patients in the
eribulin arm than in the TPC arm sur-vived 1 year (53.9% vs 43.7%, respec-tively). Independent review foundprogression-free survival (PFS) slight-
www.TheOncologyNurse.com50 March/april 2011 I VOl 4, NO 2
News in Review
Experts from various disciplines will be featured in blog segmentsover the course of theyear, allowing members to interact with their colleagues on multiplesubject areas.
Informational/educational resources to help you and your patients navigatetheir cancer treatmentand improve their qualityof life.
Members receive subscriptions to theJournal of Oncology Navigation & Survivorshipand The Oncology Nurse-APN/PA(a more than $190 value).
RESOURCES
BLOGS
JOIN THE LARGESTNurse & Patient Navigator Association
The addition of new biomarkers forestablishing a prognosis for pa -tients with breast cancer has beenrecommended in the 2010 edition of theAmerican Joint Committee of Cancer’sCancer Staging Handbook.1 Human epider-mal growth factor receptor type 2(HER2) status and multigene signature“scores” have been added to estrogenreceptor (ER) and progesterone receptor(PR) determinations.1 So, where are weregarding multigene signature scores? Atthis time, two tests are commercially
available in the United States: OncotypeDX (Genomic Health) and MammaPrint(Agendia).
21-gene recurrence score assayAvailable since 2004, Oncotype DXuses a process called reverse-transcriptasepolymerase chain reaction (RT-PCR) tolook at 21 genes: 16 are linked to breastcancer and five are reference genes usedfor normalizing the expression of the can-cer-related genes. The chosen genes have
DECEMBER 2010www.TheOncologyNurse.com
VOL 3, NO 8
Journal ofOncology Navigation &Survivorship™
between pages 34 and 35
Journal of Oncology
™
The Official Journal of the Academy of Oncology Nurse Navigators
NAVIGATION & SURVIVORSHIP®
DECEMBER 2010www.AONNonline.org
VOL 1, NO 7
Lillie Shockney, RN, BS, MASJohns Hopkins Breast CenterJohns Hopkins UniversitySchool of MedicineBaltimore, MarylandSharon Gentry, RN, MSN, AOCN,CBCNDerrick L. Davis ForsythRegional Cancer CenterWinston-Salem, North Carolina
Nicole Messier, RNVermont Cancer CenterBurlington, VermontPamela Matten, RN, BSN, OCNSt. Joseph HospitalOrange, California
Elaine Sein, RN, BSN, OCN, CBCNFox Chase Cancer Center PartnersRockledge, PennsylvaniaTricia Strusowski, MS, RNHelen F. Graham Cancer CenterChristiana Care Health SystemNewark, Delaware
Linda Fleisher, MPH, PhD(c)Fox Chase Cancer CenterCheltenham, PennsylvaniaSusan M. Gardner, RN, CBEC, CBCNValley Medical CenterRenton, Washington
Jay R. Swanson, RN, BSN, OCNSaint Elizabeth Cancer InstituteLincoln, NebraskaCarol Lewis, RN, BSN, OCN, CRNIMemorial HermannThe Woodlands, Texas
Sean T. WalshExecutive [email protected]
Leadership Council
©2010 Green Hill Healthcare Communications, LLC
AONN Staff
www.AONNonline.org
GUIDE OUR PATHStart a Local, State, or Regional Affiliate,Join a Committee
The George Washington CancerInstitute (GWCI) recently re -ceived a $2.4 million grant fromthe DC Cancer Consortium to estab-lish and coordinate a City-wide PatientNavi gation Network (CPNN) inWash ington, DC. The CPNN will create a seamless,cohesive framework for coordination ofcancer care throughout the city to ensurethat all city residents get appropriate can-cer screening and treatment regardless oftheir ability to pay. The network will alsohelp patients identify support servicesthroughout the cancer continuum, in -cluding posttreatment survivorship. Twenty-five separate institutions,including hospitals, cancer centers, andcommunity organizations in theWashington, DC, area are members of
the network, and patient navigators areembedded at every site, said StevenPatierno, PhD, executive director ofthe GWCI.
The program, he explained, providestraining once a month to every navigatorand every navigator’s supervisor. It alsoprovides a central communications portal
and a secure Internet-based data collec-tion process, which allows the navigatorsto upload their navigation logs and theirpatient interactions in real time.
He gave an example of how coordina-tion of care works. “If a patient is seen ata community advocacy group that doesContinued on page 2
CARE COORDINATIONCity-wide Patient Navigation NetworkCoordinates Washington, DC, Cancer CareBy Karen Rosenberg
The Center for the Advancementof Cancer Survivorship, Navi -gation, and Policy (caSNP), acollaboration of the George Wash ingtonCancer Institute (GWCI) and the uni-versity’s School of Public Health andHealth Services Department of HealthPolicy, was established in 2009 with support from Pfizer and the PfizerFoundation. The center’s goals are toadvance patient navigation and cancersurvivorship efforts both locally andnationally through training, research,
policy analysis, and education. caSNP grew out of the understandingthat there is “overlap between patientnavigation, survivorship, and policy andboth of these intersect with local andnational healthcare policy,” explainedSteven Patierno, PhD, executive directorof the GWCI. “We wanted to create aplatform to talk about navigation and sur-vivorship in the context of policy in aunited program.” The center offers training programs atthree levels:
• Navigation training is designed fornavigators, including nurses, socialworkers, and lay persons. Traineesfrom institutions across the coun-try learn about barriers that affecttheir patients, are trained tolaunch or improve programs, andgain tools for implementing insti-tutional change.• Executive level training is de signedfor chief executive officers, chieffinancial officers, hospital adminis-
NAVIGATION TRAININGCenter Provides Platform for Discussion ofCancer Survivorship, Navigation, and Policy By Karen Rosenberg
Continued on page 2
“The CPNN will create a seamless,cohesive framework for coordination ofcancer care throughout the city. ” —Steven Patierno, PhD
GENETIC TESTINGMultigene Signature Scores andBreast Cancer 2010By Deena Damsky Dell, MSN, RN-BC, AOCN Clinical Nurse Specialist, Fox Chase Cancer Center,Philadelphia
©2010 Green Hill Healthcare Communications, LLC
Continued on page 12
Mammography technologist Jessica Davis, RT(R) (M), is part of a multi-disciplinary breast cancer care team working to improve access toscreening, treatment, and research.
Geisinger Medical Center’sCancer Institute Joins theNCCCPBy Dawn Lagrosa
This past April, Geisinger Medical Center’s (GMC) Cancer In -stitute became one of 14 sites added to the National CancerInstitute Community Cancer Centers Program (NCCCP). Joining
this national network of community cancer centers offers GMC theopportunity to expand its state-of-the-art cancer care and research innortheast Pennsylvania.GMC is a part of Geisinger Health System (Geisinger), which servesa mostly rural population and has cancer centers in Danville, Wilkes-Barre, State College, and Hazleton. Geisinger takes pride in its innova-tive approach to healthcare delivery to this population, which alsoincludes many elderly patients. In addition, a significant portion isunderserved because of socioeconomic status and transportationproblems. Thanjavur Ravikumar, MD, FACS, director of the Center forSurgical Innovation, and co-chair of the oncology service line at
CANCER CENTER PROFILE
Continued on page 18
CONFERENCE NEWSOncology Nursing Society’s 11th AnnualAdvanced Practice Nursing Conference/Institutes of LearningOrlando, Florida, November 11-14, 2010.See who was there: page 8.
Kimberly Gessner, Holly Gentry, and Marlene Ferguson display copies of The Council of
Dads, a book by keynote speaker Bruce Feiler.
Fostering a Dialogue to Improve Patient Care & Outcomes
Submit your cases online today at www.myelomacases.com
InsideLung CancerStereotactic Radiation for Non–small-cell Lung CancersPage 20
Fast Neutron RadiotherapyPage 25
Continuing Education Maintenance "erapy in Patients withAdvanced Non–small-cell Lung CancerPage 30
Breast CancerProlonging Chemotherapy in MetastaticBreast Cancer Improves SurvivalPage 44
www.AONNonline.org/join
������� �� ����� ����������������������������������������������
Member Benefits* Include:•Best Practices
•Continuing Education
•Networking
•Expert Opinion Blogs
•Community Resources
•Publications
AONNKsize2711lt
Journal of Oncology
™
The Official Journal of the Academy of Oncology Nurse Navigators
NAVIGATION & SURVIVORSHIP®
OCTOBER 2010
www.AONNonline.org
VOL 1, NO 5
Lung Cancer Navigator of the Year—
Laura Hunnibell, RN, MSN, ARNP,
AOCN, of the Veteran
s Affairs (VA)
Connecticut Healthcar
e System West
Haven Campus works t
o develop and
implement the naviga
tor role, and
assists her facility in
improving the
stage at diagnosis for
patients with
lung cancer. She speaks
nationally and
leads an advisory grou
p to develop a standar
d position
description for cancer
care coordinators/navi
gators in the
VA Healthcare System.
Gastrointestinal Cancer Navigator of
the Year—Julie Pope, RN, BSN
, of
the Derrick L. Davis Fo
rsyth Regional
Cancer Center, Winston
-Salem, North
Carolina, empowers pati
ents and their
families with knowled
ge about their
care and resources. In
addition, she
supports them through
her caring and
compassion.
Breast Cancer Navigator of the
Year—Susan Bowman, RN, OCN,
MSW, of Wellspan He
alth at York
Cancer Center, York,
Pennsylvania,
has been a nurse navig
ator for nearly
10 years. She offers info
rmation, sup-
port, and clinical coord
ination for her
patients. She has also
ex tended her
role into survivorship
care by devel-
oping a curriculum to s
upport survivors with t
heir lifelong
recovery process.
Lillie Shockney, RN, B
S, MAS
Johns Hopkins Breast C
enter
Johns Hopkins Universi
ty
School of Medicine
Baltimore, Maryland
Sharon Gentry, RN, MSN, AOCN
,
CBCNDerrick L. D
avis Forsyth
Regional Cancer Center
Winston-Salem, North
Carolina
Nicole Messier, RN
Vermont Cancer Center
Burlington, Vermont
Pamela Matten, RN, BSN, OCN
St. Joseph Hospital
Orange, California
Elaine Sein, RN, BSN
, OCN, CBCN
Fox Chase Cancer Cente
r Partners
Rockledge, Pennsylvani
a
Tricia Strusowski, MS, RN
Helen F. Graham Cance
r Center
Christiana Care Health S
ystem
Newark, Delaware
Linda Fleisher, MPH, PhD(c
)
Fox Chase Cancer Cente
r
Cheltenham, Pennsylvan
ia
Susan M. Gardner, RN, CBEC
, CBCN
Valley Medical Center
Renton, Washington
Jay R. Swanson, RN,
BSN, OCN
Saint Elizabeth Cancer
Institute
Lincoln, Nebraska
Carol Lewis, RN, BSN
, OCN, CRNI
Memorial Hermann
The Woodlands, Texas
Sean T. Walsh
Executive Director
Leadership Council
©2010 Green Hill Healthcare Communications, LLC
Continued on page 2
AONN Staff
CONFERENCE NEWS
First Annual
Conference
Honors Excellence
in Navigation
www.AONNonline.org
GUIDE OUR PATH
Start a Local, State, or R
egional Affiliate,
Join a Committee
As a key part of the inaugural conference, the Academy present-
ed the Excellence in Navigation & Survivorship Awards.
Re cognizing excellence in patient navigation and survivorship
care, six recipients were selected from more than 50 nominations.
GETTING STARTED
Launching the
Navigation Program t
hat
Is Best for You. Part
2:
Justifying Your Progr
am
By Dawn Lagrosa
Your cancer
center offers patient na
vigation. You are
guiding patients through
the healthcare system, o
ver-
coming barriers as they p
resent themselves. Rega
rdless
of the navigation model
you are using, you will n
eed to track
and report clinical outc
omes and the financial
impact of
patient navigation. You
will have to show a retur
n on invest-
ment, as well as sustaina
bility and patient satisfac
tion. Most
important—you will nee
d to show that navigatio
n is making
an impact on the bottom
line.
Strategies to justify a na
vigation program were p
resented
by a panel of nurses and
administrators at the th
ird annual
Oncology Update of th
e American College of
Oncology
Administrators. Because
each presenter’s navigat
ion program
was designed for its comm
unity’s specific needs, th
e outcomes
measures tracked and th
e methods of doing so va
ry.
FINANCIAL CHALLENGES
Oncology Social
Workers Can Help
Patients with Financi
al
Challenges of Treatme
nt
By Karen Rosenberg
Financial challenges are a
key issue for patients wi
th can-
cer and can interfere w
ith treatment protocol
s and
patient adherence. Acco
rding to a study presented
at the
2010 annual meeting o
f the American Society
of Clinical
Oncology, however, only
about one third of patie
nts turn to
oncology social workers t
o help them overcome th
ese barriers.
In a collaborative project
by Kelton Research, Los
Angeles,
and the Association of O
ncology Social Workers
(AOSW),
Martin Eichholz and his
associates surveyed newl
y diagnosed
cancer patients, caregive
rs, and AOSW members
about the
financial impact of canc
er treatment. Surveys we
re completed
Continued on page 2
Continued on page 2
Navigator of the Year
PUBLICATIONS
Eribulin Improves Overall Survival in Women with HeavilyPretreated Metastatic Breast CancerBy Christin Melton
Chris Twelves, MD
©A
SC
O/T
odd
Bu
cha
na
n 2
01
0
TON_April2011_v7_TON 4/7/11 10:51 AM Page 50

ly better with eribulin, at a median of 3.7months versus 2.2 months when takingTPC (HR, 0.87; 95% CI, 0.71-1.05; P = .137) in the intent-to-treat (ITT)population. Investigator assessmentfound significantly improved PFS for theeribulin arm of the ITT population (HR,0.76; 95% CI, 0.64-0.90; P = .002).
In this heavily pretreated population,12% of patients given eribulin demon-
strated objective response comparedwith only 5% of patients receivingTPC (P = .002). The median durationof response was shorter with eribulinthan with TPC (4.2 vs 6.7 months,respectively; P = .159), but the clinicalbenefit rate for the eribulin arm washigher than for the TPC arm due toeribulin’s improvements in OS andresponse (23% vs 17%, respectively).
Most patients experienced 1 ormore adverse events, most of whichwere grade 1/2. In the eribulin arm,
99% (503) of patients suffered anadverse event, which was serious inone-quarter of patients. In the TPCarm, 93% (230) of patients had anadverse event, with 26% experiencinga serious adverse event.
Compared with the TPC group, theeribulin arm had higher rates of grade 3/4neutropenia (21% vs 45%, respectively),leukopenia (6% vs 14%, respectively),and peripheral neuropathy (2% vs ~9%,respectively). Patients taking eribulinwho had grade 1/2 neuropathy at thestart of the study were no more likelyto develop grade 3/4 neutropenia thanpatients starting the study with no signsof neuropathy. Hyper sensitivity reactionswere uncommon, reported in only 1% ofpatients taking eribulin.
In each study arm, 1% of patientssuffered fatal adverse events due totreatment. The 5 eribulin-relateddeaths were attributed to febrile neu-tropenia, lung infection, broncho-pneumonia, and dyspnea (2 cases).Treat ment-related deaths in the TPCarm consisted of 1 case of febrile neu-tropenia and 1 case of aspergillosis.
After the study’s conclusion, arequested updated analysis of OS ratesfound that 76% of patients in theeribulin arm had died compared with80% of patients in the TPC group(HR, 0.81; 95% CI, 0.67-0.96; P = .014). Investigators said thisshowed eribulin’s survival advantagepersisted over time. An ongoing studyis comparing eribulin with cap -ecitabine in women with previouslytreated metastatic breast cancer in aneffort to assess quality of life.
Although the authors concede thatthe range of agents used in the TPCgroup could be considered a limita-tion of the study, they counter thattheir protocol better reflects “real-lifechoices made by oncologists and theirpatients.” They recommend thateribulin be considered a new standardof treatment for heavily pretreatedwomen with metastatic breast cancer.The authors disclosed that the study wasfunded by Eisai and Eisai employees tookpart in analyzing the data. �
March/april 2011 I VOl 4, NO 2 51www.TheOncologyNurse.com
News in Review
� � � � � � � � � �
In this heavily pretreated population, 12% of patientsgiven eribulin demonstrated objective responsecompared with only 5% of patients receiving TPC.
Questions orcomments about
this issue?
Conference Overview
All clinical and nonclinical professionals involved or interestedin patient navigation and survivorship. This conference will enhance the skills and knowledge of:• Oncology Nurse Navigators• Patient Navigators • Oncology Nurses & Nurse Practitioners
• Administrators • Oncology Social Workers • Case Managers • Practice Managers
Who Should Attend
• Navigation and Survivorship Program Planning and Implementation
• Best Practices• Collaborative Navigation• Psychosocial Care and Distress Management• Compassion Fatigue• Tumor-site Focused Breakouts/Workshops
Topics Include
Register Online atwww.AONNonline.org/conference
NAVIGATING PATIENTS ACROSS THECONTINUUM OFCANCERCARETM
AONN’s second annual conference will further advance nav-igation and survivorship in cancer care through the addition ofa variety of sessions, topics, and networking events. Attendeeswill receive a thorough understanding of the state of navigationand survivorship in today’s evolving healthcare system.
CURRENT MEMBERS - $295(Save $200 off full registration of $495.)
NEW MEMBERS - $335(Registration includes member dues.)
NONMEMBERS - $495
CONFERENCE LOCATIONSan Antonio Marriott Rivercenter Hotel
101 Bowie StreetSan Antonio, TX 78205-3901
Phone: 210.223.1000
Second Annual Navigation and Survivorship Conference
September 16-18, 2011 - San Antonio, Texas
Second Annual Navigation and Survivorship Conference
September 16-18, 2011 - San Antonio, Texas
AONNKsize2711rt
©iS
tock
pho
to.c
om/Y
inYa
ng
E-mail us at [email protected].
TON_April2011_v7_TON 4/7/11 12:30 PM Page 51

Anew study shows that tamox-ifen protects high-risk womenagainst breast cancer for as
long as a decade after treatment ends.Joyce Noah-Vanhoucke, PhD, Arch -imedes Inc, San Francisco, Cali fornia,and colleagues conducted the meta-analysis and found that using tamox-ifen to prevent breast cancer in post-menopausal women aged <55 years wascost-effective and saved lives.The researchers created a virtual clin-
ical trial filled with simulated patientsbased on breast cancer incidence andsurvival rates from the Surveillance,Epidemiology, and End Results registry.Treatment in the mathematical modelfollowed protocols used in 4 randomized,placebo-controlled trials that evaluatedthe effectiveness of 5 years of tamoxifenat preventing breast cancer.
All women in the simulation wereaged <55 years when treatment startedand postmenopausal, and all had a Gailrisk score of 1.66% or greater, indicatinga high risk for breast cancer. The studypopulation was restricted to women aged<55 years to allow a more accurateassessment of tamoxifen’s contributionto reducing breast cancer risk or increas-ing the risk of events such as endometri-al cancer and blood clots, which aremore common in older women.
In the article, published in Cancer,the authors said previous studies that
found tamoxifen was not cost-effectivedue to its side effects profile had basedtheir calculations on the assumption thattamoxifen’s prophylactic benefit endedwhen the drug was stopped. The studiesselected for the meta-analysis hadextended follow-up that showed benefitsdid not end with treatment but persistedfor another 10 years.
For every 1000 women treated withtamoxifen in the original trials, 36 life-years were saved or 29 quality-adjustedlife-years (QALYs), at a cost of $11,530per QALY. In evaluating results for thesubpopulation of women aged <55 yearsused in the model, the authors said,“Tamoxifen use in this population is fore-cast to save 85 QALYs per 1000 post-menopausal women age <55 with costsavings of $47,580 compared with notreatment over lifetime follow-up.” Atotal of 69 life-years were also saved.Stratifying women according to riskscores showed that as breast cancer riskincreased, years saved and QALYsincreased while the cost per QALYdecreased.
Tamoxifen’s use as a chemopreven-tive has been limited because of sideeffects. The authors said the studyshowed that the benefits of tamoxifenprophylaxis in this patient populationcompensated for the risks and costs ofmanaging adverse events, even thoughsome were serious.—CM �
Data published in the Journal of theAmerican Medical As sociation inMarch indicate that for 20% of
women with early-stage breast cancer,removing malignant lymph nodes fromthe armpit does not improve survival orprevent recurrence. Women in the phase3 trial who underwent complete axillarylymph node dissection (ALND) hadhigher rates of lymphedema than thosewho had sentinel lymph node dissection(SLND) alone (P <.001). They also hadhigher rates of wound infection, axillaryseromas, and paresthesias (70% vs 25%,respectively; P <.001).The study, known as the American
College of Surgeons Oncology GroupZ0011 trial, was conducted at 115 sitesfrom May 1999 to December 2004 toassess whether SLND was noninferiorto ALND. In total, 891 women withsimilar clinical and disease characteris-tics were randomized to ALND orSLND and followed for a median of
6.3 years with regular physical exami-nations and annual mammograms.All women enrolled in the study had
stage T1-T2 noninvasive tumors (5 cmor less), with no more than 2 positivesentinel lymph nodes at biopsy, no pal-pable axillary nodes, and no metastaticspread. Initial treatment consisted oflumpectomy, and 605 underwent whole-breast radiation; women who hadreceived neoadjuvant hormonal therapyor chemotherapy were ineligible. Fol -lowing surgery, 403 women in theALND group and 423 in the SLND-onlyarm received adjuvant systemic therapy,with the types of therapy given fairly wellbalanced between the study arms.Women in the ALND group had anaverage of 17 nodes removed comparedwith 2 in the SLND arm.At a median of 6.3 years after enroll-
ment, 52 women in the ALND grouphad died compared with 42 in the SLNDgroup, for an unadjusted hazard ratio of
0.79 (90% confidence interval, 0.56-1.10), which the authors said demon-strated the noninferiority of SLND alone(P = .008). The 5-year overall survivalrates were also similar between thegroups, at 92.5% in the SLND-only armand 91.8% in the ALND group. No sta-tistically significant difference in survivalrates was observed when stratifying thepatients according to estrogen- or proges-terone-receptor status.In the SLND-only arm, 83.9% of
women had no recurrence at 5 yearscompared with 82.2% of women in theALND group (P = .14). The 5-year rateof local recurrence was 1.6% in theSLND-only arm versus 3.1% in theALND group, supporting the conclusionthat ALND does not prevent recurrence.
The authors concluded that “the onlyrationale for ALND in these patientswould be if the finding of additionalnodal metastases would result in changesin systemic therapy.” Because current
treatment guidelines generally call forthe same adjuvant therapy regimenregardless of nodal status, the authorssaid “ALND does not appear to be war-ranted in this patient population.” For women with early-stage breast
cancer similar to the women in thisstudy, foregoing ALND offers the poten-tial to improve quality of life significant-ly. Armando E. Giuliano, MD, chief ofsurgical oncology at the John WayneCancer Institute at St. John’s HealthCenter, Santa Monica, Cali fornia, waslead author of the study. He presentedpreliminary findings last year at theannual meeting of the American Societyof Clinical Oncology and noted thenthat it might be hard for some physiciansto abandon ALND, which has beenstandard practice for at least a century.Additional studies will need to deter-
mine whether women with more than 2positive sentinel nodes or matted nodescan safely forego ALND. �
Axillary Lymph Node Dissection Unnecessary for SomeEarly-Stage Patients with Breast CancerBy Christin Melton
www.TheOncologyNurse.com52 March/april 2011 I VOl 4, NO 2
News in Review
Tamoxifen Protective 10 YearsAfter Treatment Marijuana Ingredient Improves
Eating and Sleeping
Asmall Canadian study foundthat patients who took delta-9-tetrahydrocannabinol (THC),
the psychoactive ingredient in mari- juana, slept better and derived moreenjoyment from eating than patientsgiven a placebo. The University ofAlberta investigators, led by associateprofessor Wendy Wismer, recruited ter-minal patients with advanced cancerwho were randomly assigned to take 2.5mg of dronabinol (a pill form ofTHC) or placebo twice daily for 18days. Afterward, the participantscompleted questionnaires to assesswhether their quality of life improvedduring the study.Chemotherapy, along with certain
types of cancer, often affects the sens-es of smell and taste and leads toanorexia in some patients. Helpingpatients maintain a healthy weightand nutritional status is challenging,which was the impetus for the study.All the participants underwentchemotherapy prior to enrollment,and approximately two-thirds report-ed mild to moderate changes in theirsense of taste.Although 73% of the THC group
found food more appealing and 55%said food tasted better while taking the
drug, overall calorie intake was similarbetween the 2 groups. Patients in theTHC group did increase their con-sumption of meat, a food that com-monly induces nausea during chemo -therapy and tends to be avoided.
The investigators said patients tak-ing THC reported improvement intheir sleeping habits. A 2009 study byPalesh and associates appearing in theJournal of Oncology observed that morethan three-quarters of patients withcancer experience sleep disorders dur-ing chemotherapy, and 43% meet thecriteria for a diagnosis of insomnia.Palesh and colleagues found a correla-tion between sleep disorders anddepression, and the authors of thisCanadian study speculated that THCmight help alleviate sleep disorders anddepression. They said it might alsoreduce pain, inflammation, and anxi-ety. The THC and control arms hadsimilar rates of adverse events, whichwere minimal overall.
The study by Wismer and associ-ates is limited by its small study sizeand did not analyze the effects ofsmoking marijuana for medicinal pur-poses. The complete findings areavailable in the March issue of theAnnals of Oncology.—CM �
TON_April2011_v7_TON 4/7/11 12:30 PM Page 52

�������������������
���������������� ��������������������� �� ���� ������ ���������� ���������������������������
To use 2D barcodes, download the ScanLife app:• Text “scan” to 43588• Go to www.getscanlife.com
on your smartphone’s web browser, and select “Download”
• Visit the app store for your smartphone
Scan Here to Register.
������������������������������
���������� ����������������� �����������������
��� �������
�� ��� ����� ���
�������������
���������
���������������
����
�������
�������
������� �
�� ��� ���� ������
�������������������
������������ �����
�� �����������������������
Current activities atwww.COEXM.com include:
Pushing Your Limits
COEKsize2711CE©iStockphoto.com/altaykaya
� �� �� � �� �TON_April2011_v7_TON 4/7/11 10:53 AM Page 53

www.TheOncologyNurse.com54 March/april 2011 I VOl 4, NO 2
News in Review
The US Food and Drug Ad min -istration (FDA) held a publicmeeting in February to assess
whether stricter criteria are needed whenconsidering oncology drugs for accelerat-ed approval. Measures enacted in 1992allow the FDA to grant acceleratedapproval for drugs targeted at unmetneeds in cancer based solely on data fromsingle-arm studies and relying on endpoints other than the standard metric ofoverall survival. At the meeting, expertswith the FDA’s Oncologic DrugsAdvisory Committee (ODAC) criticizedthe FDA, with Silvana Martino, DO,who directs the Breast Cancer Programat the Angeles Clinic and ResearchInstitute in Santa Monica, California,calling its actions “ignorant.”Gary Lyman, MD, MPH, professor of
medicine and director of comparativeeffectiveness and outcomes research atDuke University School of Medicineand the Duke Comprehensive CancerCenter in Durham, North Carolina, saton the ODAC panel and discussed thehearing with The Oncology Nurse-APN/PA. “The major concern of theODAC is that accelerated approval hasbeen granted on the basis of a single-armstudy in more than half of instances,
which limits a full comparative look atefficacy and safety,” he explained.Lyman said relying on such limited
evidence might be appropriate in excep-tional cases, such as for drugs to treat raretumors or when a drug has very strong,observable treatment effects, but “thedefault recommendation is that this con-ditional approval be based on at least onewell-designed randomized, controlledtrial [RCT] reporting significant im -provement in an outcome measurementlikely to convey clinically meaningfulbenefit.” In every case, approval shouldbe “based on the robustness of the resultsin terms of a strong treatment effect anda very favorable risk-to-benefit ratio,”said Lyman.On the rare occasions when acceler-
ated approval is granted without datafrom an RCT, Lyman said ODAC rec-ommends that the FDA require thedrug’s maker to have an RCT under wayor imminent. The FDA should reviewplans for the trial to ensure that its designallows for reliable results, suitable to sup-port licensing approval.The review of the accelerated
approval process was prompted by theFDA’s controversial decision inDecember to withdraw approval of
bevacizumab (Avastin) in breast cancer,which Lyman said was the first time theagency had rescinded an approved indi-cation of a drug brought to market underthis mechanism. “There are a number ofothers—including 6 that we reviewedyesterday—that have not fulfilled theirpostmarketing requirements and may bevulnerable,” he added. The drugs inquestion include Erbitux by Eli Lilly,Bexxar and Arranon by GlaxoSmith -Kline, Clolar by Genzyme, Vectibix byAmgen, and Gleevec by Novartis forits indication in gastrointestinal stro-mal tumors.At the meeting, the panel ques-
tioned manufacturers about their fail-ure to submit requisite follow-up datafor these 6 drugs, but the FDA gave noindication that their approval status isin jeopardy. Most of the manufacturerscited difficulty recruiting enoughpatients for clinical trials to producemeaningful results as the primary rea-son for the delays. Amgen’s representa-tive told the committee the companywas confident it had complied with theFDA requirements.Whereas most companies that
receive accelerated approval for a drugshow due diligence in complying with
follow-up requirements, Lyman said afew have taken a decade or longer to sub-mit the requested data. “The ODACmembers [believe] that plans for morefrequent updates—perhaps annually—ofstudies with outstanding validation orpostmarketing requirements would helpshorten the time interval to completionand consideration for full approval.”Members of the ODAC panel also
voiced concern that the FDA hadoccasionally granted full approval to acancer drug without requiring soliddata from an RCT. “The ODACbelieves that, with few exceptions,such approval should be based on atleast 2 well-done RCTs with consistentor robust results,” said Lyman.Lyman acknowledged that patients
with cancer and advocacy groups havecomplained in the past that strictstandards delay access to lifesavingmedications. “It will be importantthat no unnecessary delays occur,” hesaid. If drug companies are pushed tofulfill their postmarketing require-ments more promptly, Lyman said heexpects it to shorten the time to fullapproval and decrease how long anineffective or unsafe drug remains onthe market. �
FDA Panel Recommends Stricter Process forAccelerated Approval of Cancer DrugsBy Christin Melton
Patients with inoperable metastat-ic melanoma now have anothertreatment option as ipilimumab
becomes the second immunotherapydrug approved by the US Food andDrug Administration (FDA) for thetreatment of cancer. Fortunately forclinicians, ipilimumab also has a new,easier-to-pronounce name—Yervoy.Specifically, Yervoy is indicated forpatients with unresectable metastaticmelanoma that is newly diagnosed orprogresses despite prior therapy.Ipilimumab is a recombinant, human
monoclonal antibody. It works by in -hibiting cytotoxic T-lymphocyte anti -gen-4 (CTLA-4), a protein that isinvolved in downregulating T-cells, tokeep the immune system from attackinghealthy tissue. Ipilimumab blocksCTLA-4 so that the T-cells remainactive and the patient’s immune systemcontinues to fight the cancer as long ashe or she is receiving treatment.Data from a pivotal phase 3 trial of
ipilimumab, which were published in
the New England Journal of Medicine in2010, show that patients who receivedipilimumab alone or in combinationwith gp100 had better survival out-comes than patients treated only withgp100. Median overall survival (OS)for patients in the ipilimumab trialarms reached 10 months comparedwith 6 months for patients in thegp100 monotherapy arm.The rate of 1-year survival was
46% for patients treated with ipili-mumab versus 25% for patients ongp100 monotherapy. Investigatorsestimated the 2-year survival rate at24% for the ipilimumab group and14% for the gp100 arm. Ipilimumabwas associated with a 34% reductionin risk of death (hazard ratio, 0.66; P = .0026).The overall response rate (ORR)
was only 10.9% for patients receivingipilimumab, but this was significantlyhigher than the ORR seen in the com-bination arm and the gp100 monother-apy group (5.7% vs 1.5%, respective-
ly). The authors reported that themean duration of response was 11.5months for the group that receivedipilimumab and gp100 combined buthad not been reached in the othergroups because >50% of patients whoexperienced complete or partialresponses had not relapsed.Approximately 10% of patients dis-
continued ipilimumab because of treat-ment-related adverse events. Amongpatients receiving ipilimumab alone, themost common adverse events (allgrades) were fatigue (41%), diarrhea(32%), pruritus (31%), rash (29%), andcolitis (8%). Some patients treatedwith ipilimumab did have severe orfatal immune-mediated adverse reac-tions, including enterocolitis (7%),endocrinopathy (4%), dermatitis (2),hepatitis (1%), neuropathy (1%),nephritis (1%), and eosinophilia (1%).Some of these can be treated with corti-costeroids, according to researchers prac-ticing at one of the institutions that con-ducted phase 3 ipilimumab trials.
In a review article on the drug, pub-lished in Seminars in Oncology in 2010,Boasberg and colleagues warn that“colonic perforation can occur” andcall for patients who develop diarrheato be monitored carefully, “with strictadherence to treatment algorithms.”The researchers note that if adverseeffects are caught promptly and man-aged properly, “Ipilimumab is anextremely safe drug to administer.”Bristol-Myers Squibb, which manu-
factures the drug, has worked with theFDA to develop a Risk Evaluation andMitigation Strategy for ipilimu mab inan effort to help clinicians manage orprevent the most serious treatment-related adverse events. The companyannounced that it has launched acopayment program to assist “eligible,commercially insured patients whohave been prescribed ipilimumab” inline with its FDA-approved indication. Information on ipilimumab and
the REMS program is available atwww.yervoy.com. —CM �
Ipilimumab (Yervoy) Is First Melanoma Drug Approved in a Decade
TON_April2011_v7_TON 4/7/11 12:33 PM Page 54

TON_April2011_v7_TON 4/7/11 10:53 AM Page 55

www.TheOncologyNurse.com56 March/april 2011 I VOl 4, NO 2
News in Review
Recruiting adults with cancer totake part in clinical trials is anongoing challenge in the United
States, but the growing number of stud-ies for targeted therapeutics and thepositive news emerging from these stud-ies might help turn that around. Trialsof targeted agents depend heavily onpharmacokinetic and pharmacodynam-ic testing to assess outcomes, promptinga team of researchers to investigate howwilling patients are to undergo varioustesting procedures in the trial setting.
Raoul Tibes, MD, PhD, associatedirector of the Acute and ChronicLeukemia Program at the Mayo Clinicin Scottsdale, Arizona, led the collabo-rative study, which he describes as thefirst of its kind. “This has never beenasked in a prospective and such a sys-tematic way,” he said in an interview.Tibes and his colleagues from Scotts -dale Healthcare and the TranslationalGenomics Research Institute believethat the results will be useful in plan-ning future clinical trials, particularly ofmolecular-targeted therapies. “Lookingat data in detail, it may inform whatspecific tests are easier tolerated bypatients and those can be incorporatedpreferentially in trials over others,”explained Tibes.
The researchers analyzed the willing-ness of 61 patients with advanced cancer to submit to various pharma-co dynamic and pharmacokinetic tests,including imaging, while participatingin a clinical trial. Perhaps not unex-pectedly, the patients were more willingto undergo noninvasive tests, such as
urine and blood testing, than they wereto submit to invasive procedures liketumor and skin biopsies. When it cameto imaging, patients were more recep-tive to getting ultrasounds, radiographs,echocardiograms, computed tomogra-phy scans, and positron-emission tom -ography scans than they were to under-going magnetic resonance imaging.
Although the study found that somepatients were less willing to have abiopsy during a trial than some of theother tests, “Skin biopsies did not posegreat burden on patients,” Tibes noted.More reluctance was observed when itcame to tumor biopsies, but nearly allthe patients consented to at least 1tumor biopsy and several agreed torepeat the procedure. Patients whofound an invasive test inconvenient orhad negative feelings about the experi-ence were somewhat less willing torepeat the test. Tibes said, “This tells usthat researchers can ask for tumor biop-sies but need to be mindful of the num-ber to ask for.”
The study included 39 men and 22women, but the data show “gender wasnot a major determining factor” of apatient’s willingness to undergo testing.“Demographics, overall, had littleinfluence,” said Tibes. The investiga-tors did find that “college graduates andpatients with higher income had ahigher positive association with will-ingness to undergo most tests.” Patientswith insurance coverage were also morelikely to agree to requested procedures.
Tibes said the study “supports clini-cal trials that have frequent biomarkercollection and imaging studies andgives clinical researchers the data onhand to support this.” He said this isimportant in an era where many of thenewer drugs are targeted therapies,requiring complex analyses of molecu-lar factors to assess matters like cancerorigin, disease progression, and treat-ment response.
Having information about how adrug is expected to work for a particularpatient provides that patient withgreater reassurance about participatingin a trial for a novel drug. “The morescientifically rational and the moredata, including molecular data—evendata that is still experimental—themore support it lends to participate in aparticular study,” said Tibes.
In most trials involving a novel drug,a lot of unknowns remain, but Tibesbelieves this does not deter mostpatients. “New agents and drugs canwork even without us understandingwhy and still offer great clinical bene-
fit,” he pointed out. “Patients that havefew treatment options left are willing totry these options.”
Although the study did not attemptto measure whether explaining a testhelped elicit the patient’s cooperation,Tibes said his involvement conductingtrials indicates, “If tests and proce-dures are explained to a patient, mostpatients are willing and agreeable tohave these performed.” He added thatpatients in phase 1 trials are generallymore willing to undergo proceduresthan suggested by experts and others
who have never been directly in -volved in early oncology trials beyondtalking about how much is reasonableto ask of patients.
“In my experience, patients in a phase1 setting understand the limitations ofclinical research, but it still gives patientsand their loved ones hope that some-thing can be done!” said Tibes, who thenadded, “Hope dies last.”
The study by Tibes and associatesappears online in the journal Cancerand is scheduled for inclusion in theJuly 15, 2011, print edition. �
Study Shows Patients in Clinical Trials Receptive to Most TestingBy Christin Melton
“If tests and proceduresare explained to a patient,most patients are willingand agreeable to havethese performed.”
—Raoul Tibes, MD, PhD
Medicare Plans to CoverProvenge
The Centers for Medicare &Medi caid Services (CMS) hasre leased a proposed decision
memo that suggests it will cover thecost of sipuleucel-T (Provenge), theimmunotherapy vaccine approved inApril 2010 for men with asympto-matic or mildly symptomatic meta -static castrate-resistant prostate can-cer, for on-label use. CMS contractorswill have discretion as to whetherthey will cover it for off-label use.To date, no studies have been pub-
lished that support off-label use ofsipuleucel-T, but CMS decided toleave the coverage question open sothat patients in clinical trials investi-gating off-label indications mighthave access to the drug. The agencynoted that it does not expect clini-cians to prescribe sipuleucel-T forindications unsupported by evidence,but if this occurs regularly, CMS saidit would reconsider the ruling.When sipuleucel-T was first
approved, CMS took the unusualstep having the Medicare EvidenceDevelopment and Coverage Ad -visory Committee (MEDCAC) re -view the clinical trial data beforeagreeing to cover the drug’s estimat-ed $93,000 cost. The committeecompleted its review in November2010, and panel members rated the
drug an average of 3.6 for effective-ness despite concerns about flaws inthe trials’ protocols and analyses.CMS also asked the Blue Cross &
Blue Shield Technology EvaluationCenter to conduct an independentinvestigation of the evidence for itseffectiveness. The center concludedit had “moderate” efficacy.During an initial 30-day public
comment period, 620 (94.4%) of the657 comments received by CMSexpressed support for covering sipuleucel-T. CMS also reviewednational guidelines and met withofficials from Dendreon to discussthe trials.In issuing its proposed coverage
decision, CMS noted the underrepre-sentation of non-white men in thetrials and “encourage[d] researchersto take appropriate steps to assurethat clinical trials enroll subject pop-ulations that reflect the distributionof pa tients affected by the disease.”Black men are more than twice aslikely to die from prostate cancer aswhite men.CMS has initiated another call for
public comments on its proposeddetermination. The agency says itwill review these comments andissue its final ruling by June 30,2011.—CM �
“New agents and drugs can work even without usunderstanding why and still offer great clinical benefit.”
—Raoul Tibes, MD, PhD
TON_April2011_v7_TON 4/7/11 10:53 AM Page 56

Timing of HormonalReplacement Therapy AffectsBreast Cancer Risk LONDON—New data by a group fromOxford University in England show thatwomen who wait ≥5 years aftermenopause to start hormone replace-ment therapy (HRT) are less likely to getbreast cancer than women who initiateHRT almost as soon as they experiencemenopause. The authors note that mul-tiple studies have demonstrated anincreased risk of breast cancer for womentaking HRT after menopause, but theysaid few have considered whether theinterval between onset of menopauseand start of HRT influences risk. In conducting the retrospective
analysis, Valerie Beral, FRS, and associ-ates relied on data for 1.13 millionpostmenopausal women (median age,56.6 years) recruited in 1996-2001 toparticipate in the United Kingdom’sMillion Women Study. Investigatorsestimated the adjusted relative risk(RR) of breast cancer for current HRTusers (n = 394,697), past users (n =221,056), and never-users (n =513,272). Women in the HRT groupwere further stratified according totime elapsed between menopause andinitiation of HRT, type of hormoneused, and duration of HRT.A total of 15,759 cases of breast
cancer were reported, with 9632(61%) incidents in women currentlyor previously on HRT. RR was signifi-cantly greater in women who startedHRT before or within 5 years ofmenopause (RR, 1.43; 95% confi-dence interval [CI], 1.35-1.51; P <.001) than for women who waitedat least 5 years after menopause tobegin HRT (RR, 1.05; 95% CI, 0.89-1.24; P = .6). Women who did notbegin HRT until ≥5 years aftermenopause had nearly the same risk ofbreast cancer as women who neverused HRT. The breast cancer risk waslower for women who waited ≥5 yearsafter menopause to begin HRT regard-less of type or duration of HRT andbody mass index. Complete findingswere published in the Journal of theNational Cancer Institute.
What Women Need to KnowAbout MammographyLONDON—False-positive mammogra-phy results increase anxiety anddecrease quality of life (QOL) for somewomen, negative effects that persist for1 year or longer. Lideke van der Steeg,
PhD, and colleagues from St. ElisabethHospital in Tilburg, the Netherlands,say their findings suggest that clini-cians need to do a better job of inform-ing women before breast cancerscreening about the pros and cons ofthe procedure. Over a 5-year period, women who
received abnormal mammographyresults at 1 of 3 Dutch hospitals wereinvited to enroll in the study. In -vestigators administered questionnairesthat assessed QOL in various areas. Ofthe 385 women who completed the sur-veys, 152 had a breast cancer diagnosisand 233 received a false-positive resultfollowing mammography.Medical records showed that women
in the false-positive group often under-went more tests to rule out a breast can-cer diagnosis than women confirmed tohave breast cancer. Only 14% ofwomen with confirmed breast cancerhad ≥4 diagnostic procedures comparedwith 32% of women eventually foundnot to have breast cancer. More thanhalf (54.9%) of women in the false-pos-itive group had to go back to the out-patient clinic for additional work-upwithin the first year of initial screening,with some women returning as many as8 times.
The researchers believe the multiplescreenings and procedures to rule outbreast cancer, which included biopsiesin some cases, gave rise to the women’sanxiety and negatively affected theirQOL. For some women, particularlythose prone to anxiety, the reduction inQOL was significant.
“Cancer screening is intuitivelyappealing, and common sense dictatesthat early detection is good and with-out risk,” van der Steeg and her teamwrote in the article appearing in theBritish Journal of Surgery, noting thatmost breast cancer screening programshave been shown to reduce breast can-cer–related deaths. Many women, how-ever, overestimate their odds of breastcancer and the benefits of mammogra-phy, and they are unaware of the false-positive risk. This rate is typically said tohover around 6% in the United States,but varies according to region, clinicianexperience, and patient characteristics;the risk of a false positive increases withsuccessive mammograms. The authors add that women are also
not aware of potential dangers of receiv-ing a false-positive mammography re -sult, such as the need for additional testsand the associated increase in anxietyand diminished QOL. This informationis not touted in campaigns promotingroutine mammography screening, andvan der Steeg and colleagues urge clini-cians to provide women with balancedinformation about breast cancer screen-ing, addressing the benefits and risks ofthe procedure.
Prevalence of Depression inBreast Cancer PatientsOverestimatedLONDON—A British study publishedin Lancet Oncology undermines thewidely held belief that depression isendemic in patients with cancer.Investigators for the meta-analysisfound that 30% to 40% of patients seenin oncologic, hematologic, and pallia-tive-care settings suffered from a com-bination of mood disorders. As a result,“Clinicians should remain vigilant formood complications, not just depres-sion,” said the authors of the study, ledby Alex J. Mitchell, MRCPsych,Department of Cancer Studies andMolecular Med icine, Leicester RoyalInfirmary, Leicestershire PartnershipTrust, United Kingdom. The research team looked at data from
94 studies encompassing 14,078 adultsin 14 countries who were screened fordepression, anxiety, and adjustment dis-orders in the first 5 years after cancerdiagnosis. The prevalence of mood dis-orders, including depression, wasassessed using criteria from theDiagnostic and Statistical Manual ofMental Disorders or InternationalClassification of Diseases.
Overall, 29.0% of patients in pallia-tive-care settings (n = 4007) and38.2% of patients in oncologic andhematologic settings (38.2%) experi-enced mood disorders. Rates of depres-sion were similar between patients inpalliative-care settings and those inoncologic and hematologic settings(16.5% vs 16.3%, respectively). Com -pared with patients in the palliative-care setting, patients in the oncologicand hematologic setting were slightlymore likely to have an adjustment dis-order (15.4% vs 19.4%, respectively)and clinically significant anxiety (9.8%vs 10.3%, respectively).Mitchell and associates emphasized
that although patients with cancerexperience depression less often thancommonly thought, it “remains animportant and overlooked complicationof cancer.” According to the authors,studies suggest patients with depressionare less likely to remain active in theirmedical care, have longer hospital stays,and have significantly worse quality oflife and survival outcomes. The authors added that their study
highlights the need for clinicians toremain vigilant for signs of a number ofmood disorders in patients. They recom-mended using simple screening tools toevaluate patients for distress, declines inquality of life, unmet needs, and a desirefor help.Although the rates of mood disor-
ders and depression remained fairlyconsistent when stratifying data byage, sex, and clinical setting, theinvestigators said the studies did notprovide sufficient information forthem to assess results by cancer type orduration of illness. �
March/april 2011 I VOl 4, NO 2 57www.TheOncologyNurse.com
International News
Reports from the Netherlands and the United KingdomBy Jill Stein
Clinicians need to do abetter job of informingwomen before breastcancer screening aboutthe pros and cons of theprocedure.
Clinicians need to toremain vigilant for signs of a number of mood disorders in patients.
©C
op
yrig
ht
Big
sto
ck.c
om
/mo
nke
ybu
sin
essim
age
s
©C
op
yrig
ht
Big
sto
ck.c
om
/Sa
vo
l_6
7
TON_April2011_v7_TON 4/7/11 10:54 AM Page 57

www.TheOncologyNurse.com58 March/april 2011 I VOl 4, NO 2
For the up to two-thirds of men withazoospermia after chemotherapy,microdissection testicular sperm
extraction (TESE) and intracytoplasmicsperm injection (ICSI) can salvage fer-tility, according to the largest reportedseries of postchemotherapy microdis-section TESE-ICI to date. Althoughprechemotherapy sperm banking re -mains a recommended part of any treat-ment plan, researchers from WeillCornell Medical College in New YorkCity demonstrated that assisted repro-ductive techniques should be offered topatients who did not preserve sperm.Hsiao and colleagues analyzed 84
TESE procedures performed in 73patients with persistent postchemothera-py azoospermia (mean time since treat-ment, 18.6 years). Of the 61 patientswho underwent testicular biopsy, 90.2%showed a Seroli-cell–only pattern and9.8% showed hypospermatogenesis.Surgeons retrieved sperm from 37%
of patients, which equated to 42.9% ofprocedures. From these sperm, a 57.1%fertilization rate per injected oocytewas achieved, resulting in a 50% clini-cal pregnancy rate (confirmed by fetal
heartbeat 32 days postprocedure) and a42% live birth rate. Sperm retrieval rates differed by dis-
ease site, with the highest rate (85%)seen in men who were treated for testic-ular cancer and the lowest rate (14%) inmen treated for sarcoma. The researchersspeculated that these rates correlate not
with the cancer site but with the therapycommonly used for these cancers, that is, low gonadotoxic platinum-basedchemo therapy and high rates of expo-sure and higher doses of alkylatingagents, respectively. Retrieval success was found to associ-
ate with exposure to an alkylating agent,
with exposure associated with less suc-cess than no exposure (21.4% vs 45.7%,respectively). On multivariate analysis,however, this association did not reachsignificance. Testicular histopathologypattern correlated with retrieval rates aswell. Hypospermatogenesis was uniform-ly associated with successful spermretrieval (100%), whereas a Seroli-cell–only pattern correlated with a lower rateof success (38.2%). Some factors did not affect retrieval
rates. Testicular volume, follicle-stimu-lating hormone, time since chemothera-py, age at TESE, and luteinizing hor-mone use were not found to correlatewith TESE outcome. The researchers noted that because
this was not a retrospective trial, it isdifficult to determine the impact of asingle agent when analyzed as part of achemotherapy regimen. In addition,the small study did not accrue enoughpatients who received gonadal radia-tion treatment for the researchers toanalyze the data. The complete study is published
online in the Journal of ClinicalOncology (March 14, 2011). �
Imbalanced investment and relationalamelioration emerged as areas of carethat were viewed differently by navi-
gators and their patients in an analysisof perspectives from each group.Researchers from the University ofRochester interviewed 18 pairs ofpatients and navigators as part of a larg-er randomized controlled trial. In doingso, Yosha and colleagues identifiedstruggles the navigators, in this studywell-trained lay community healthworkers supervised by social workers,were experiencing but to which thepatients were unaware. Most noticeably, navigators expressed
tension from their dual responsibilities ofadvocacy for their patients’ autonomy indecision making and their desire to pro-mote decisions consistent with guide-line-concordant care. Patients not onlyexpressed comfort with their decisionsbut also, when asked, noted that theywere unaware of the navigators’ struggleregarding this issue.Another significant struggle for nav-
igators was improving, and not worsen-
ing, any relationship difficulties betweena patient and other members of thehealthcare team. Navigators ex presseddiscomfort in having to support a patientwithout passing judgment on medicalproviders when there was an adversarialrelationship between that patient andprovider. Navigators noted that notmaking the situation worse was animportant goal in these situations.
There was consensus on patient needsidentified. Emotional support, informa-tional support, and accompanimentemerged as important for both groups.These needs, however, were viewed dif-ferently by navigators and patients.Navigators often saw emotional support
as a main part of their job function.Patients generally did not expect emo-tional support but found it beneficial astime progressed. Most patients expressedappreciation for their navigators in theinterviews conducted after acute treat-ment. They appreciated not only thehelp they received but the help theirfamily members received from the navi-gation intervention.
The researchers concluded that aspatient navigation programs continue toevolve, instruction on the imbalancedinvestment in the relationship betweenpatient and navigator can be used toimprove navigator training. Trainingprograms should educate navigators to
anticipate these struggles and offer navi-gators methods to help manage them.“This study clearly identifies some of
the unique issues that navigators dealwith every day, especially in the 3complex ‘struggles’ explained in thefindings. These issues can be verytime-consuming in a patient–naviga-tor meeting,” noted Frank delaRama,RN, MS, AOCNS, a practicing navi-gator and clinical nurse specialist atthe Palo Alto Medical FoundationCancer Care Clinic. “Healthcare thesedays often seems to be occupied withpatient satisfaction, dashboard meas-ures, and other stats. Provider perspec-tives could easily identify an area ofneed, or even validate aspects of cur-rent practice, as well as help supportthe amount of time/resources allocatedto navigator services.”Published study results are available
in: Yosha AM, Carroll JK, Hendren S, etal. Patient navigation from the pairedperspectives of cancer patients and nav-igators: a qualitative analysis. PatientEduc Couns. 2001;82:396-401. �
Navigators’ and Patients’ Perspectives on theNavigation Experience
Azoospermic Survivors Not Necessarily Sterile
Navigation & Survivorship Brought to you by
www.AONNonline.org
Most noticeably, navigators expressed tension fromtheir dual responsibilities of advocacy for theirpatients’ autonomy in decision making and theirdesire to promote decisions consistent withguideline-concordant care.
TON_April2011_v7_TON 4/7/11 10:54 AM Page 58

��� �� ��� ���Editor in ChiefSagar Lonial, MDAssociate Professor of Hematology and Oncology Emory University School of Medicine
Editor in ChiefStephanie A. Gregory, MDThe Elodia Kehm Chair of Hematology Professor of MedicineDirector, Section of HematologyRush University Medical Center/Rush University
Topics include:• Newly Diagnosed Patients• Maintenance Therapy• Transplant-Eligible Patients• Retreatment• Transplant-Ineligible Patients• Cytogenetics• Side-Effect Management• Bone Health
Newsletter Series
���������������� ���������������� �� ���
������ ��������� ���
Topics include:• Hodgkin Lymphoma• Follicular Lymphoma• Mantle Cell Lymphoma• Waldenstrom’s Macroglobulinemia• Diffuse Large B-Cell Lymphoma• T-Cell Lymphoma
���������������� ������������������
������ ��������������
Target AudienceThese activities were developed for physicians, nurses, and pharmacists.
AccreditationThis activity has been approved for 1.0 AMA PRA Category 1 Credit™ (a total of 14.0 credit hours will be issued for completion of all activities). Nursing and Pharmacy credit hours will also be provided.For complete learning objectives and accreditation information, please refer to each activity.
This activity is jointly sponsored by Global Education Groupand Medical Learning Institute, Inc.
Coordination for this activity provided by Center of Excellence Media, LLC.
������� �������� ����������� ����� ������������
YOUR QUESTIONS ANSWERED
COEKsize40611MM
For information about the physician accreditation of this activity, please contact Global at 303-395-1782 or [email protected].
This activity is supported by educational grant from Cephalon Oncology,Millennium Pharmaceuticals, Inc., and Seattle Genetics, Inc.
This activity is supported by an educational grant from Millennium Pharmaceuticals, Inc.
� �� �� � �� �TON_April2011_v7_TON 4/7/11 10:54 AM Page 59

www.TheOncologyNurse.com60 March/april 2011 I VOl 4, NO 2
Nursing Life
Can Alternative Medicine Prevent Burnout?
Burnout is a common problemamong nurses. A 2008 study in theOnline Journal of Issues in Nursing
reported that 44% of nurses aged <30years and 38% of nurses aged ≥30 yearsexperience “acute” burnout. In thehopes of reducing job-related stress,Kent State University’s College ofNursing has joined forces with theUrban Zen Foundation, run by fash-ion designer Donna Karan, to imple-ment a program that teaches nurses tocare for themselves using principles ofalternative medicine.
Karan’s foundation operates theUrban Zen Integrative Therapy(UZIT) program, which integrates var-ious holistic practices designed to help
heal the mind and body. UZIT incor-porates yoga, essential oil therapy,Reiki, nutrition, and contemplativecaregiving.
The College of Nursing launched theUZIT “Care for the Caregiver” class as apilot program in September 2010,enrolling 30 advanced nursing students.The class met monthly in person andthen provided weekly online Webinars.Students were required to documenttheir progress with the Eastern tech-niques in a journal.
Kent State University College ofNursing is one of the largest nursingschools in the country. Laura Dzure c,dean of the college, believes these effortsto teach nursing students how to managework-related stress and head off burnoutcould have a lasting effect on the profes-sion and ultimately lead to better patientcare. The college is offering the class
again this semester and eventually hopesto make it available to all its nursing stu-dents. You can learn more about UZIT atwww.urbanzen.org.—CM �
When it comes to socialmedia, some studiesindicate that nurses
have bounded ahead of otherhealthcare professionals in embrac-ing the digital platform. A 2010 sur-vey of 292 nurses by NicholsonKovac Inc found that 65% said they“would engage in social media forreasons of professional develop-ment.” Slightly more than three-quarters (77%) acknowledged visit-ing Facebook and 11% said they useTwitter. More than 80% of nursesresponded that they access Websitesto find healthcare information, and41% said they visit Websites of man-ufacturers to learn more about prod-ucts and services.
Now a new book, The Nurse’sSocial Media Advantage by RobertFraser, BScN, RN (Sigma Theta TauInternational), instructs nursing pro-fessionals on how to harness socialmedia to improve their nursing prac-tice. The book addresses variousissues in a Q&A format and reviewsa range of topics the author believesare important for social media usersworking in healthcare, includinghow to assess your legal risks.
Fraser is a nurse in Canada anddescribes himself as being passionateabout “how technology can changethe way we share information.” Heencourages nurses to be at the fore-front of technology and become partof a global nursing network. Thebook costs $24.95 and is availablethrough www.nursingknowledge.orgor at www.amazon.com. �
Do YouTweet?
Nursing by the Numbers
Every year, the demand for health-care services grows in the UnitedStates and more responsibilities
for providing that care are shifted to nurses. While NursingSchool.orgreports that the country has at least 5.5million nurses and nursing aides, thisnumber is not nearly high enough tokeep pace with the rising number ofpatients. The resulting shortage leavesmany nurses feeling overworked andunderpaid.
Nurses’ wages vary according to cer-tification and region (Figure). Themost qualified nurses make goodmoney—the average annual salary fora certified registered nurse anesthetistis $129,530. But is this enough whenyou consider that 2.5 million regis-
tered nurses plus the 2.3 million nurs-ing aides and 750 thousand licensedpractical nurses spend a cumulative 11billion hours working each year?
And the job is not always pleasant.Nurses get yelled at (and not just bypatients!) and come into close con-tact with the full spectrum of bodily
fluids on a regular basis. Nursing alsohas its dangers. A nurse suffers moreinjuries than a construction workerand is more likely to be physicallyassaulted than your average prisonguard. Is it any surprise that 1 out of5 emergency department nursesmeets the criteria for posttraumatic
stress disorder?After reading these statistics, you
might wonder why those who go intonursing stick with the job. A 2010survey of 1399 registered nurses byAMN Healthcare suggests at leastone-third say they might not! Thesurvey found 29% of nurses overallplan to reduce their role in nursing orleave nursing and 6% of hospitalnurses plan to retire in the next 1 to3 years.
The survey also found that mostnurses are satisfied with theircareers and that 59% of nurseswould select nursing again if they hadto do it all over and 64% wouldadvise young people to consider nurs-ing as a career.
Most nurses say they are in the jobbecause they like helping people andbeing in a position to make a valuablecontribution to society. In the end,nurses save lives, and that is some-thing you can’t put a price tag on. �
Figure. Median Hourly Wage for LPNs and RNs (May 2009)
45.00
40.00
35.00
30.00
25.00
20.00
15.00
10.00
5.00
0.00USA AL AZ CA CT FL IN MS MT NY TX
RN
LPN
Source: United States Department of Labor, Bureau of Labor Statistics.
A nurse suffers more injuries than a constructionworker and is more likely to be physically assaultedthan your average prison guard.
If you are attending the 2011 OncologyNursing Society Annual Con gress inBoston, we would like to hear from you. E-mail [email protected] and shareyour experiences at the conference in 500words or fewer. We will select the best e-mails to published in an up coming issue ofThe Oncology Nurse-APN/PA and on ourWebsite.
Going to theONS Meeting?
Hourly W
age, $
Region
©C
opyright
Big
sto
ck.c
om
/NejroN
TON_April2011_v7_TON 4/7/11 1:17 PM Page 60

THANK YOU FORMAKING US#1*Source: © Kantar Media, custom study of Oncology Nursing publications among The Oncology Nurse-APN/PA circulation (December 2010).
����������������� ����
���������������������� �������The Oncology Nurse-APN/PA����������� ���������
The #1 Read
Oncology Nursing
Tabloid Publication*
In a recent survey, oncology nurse parctitioners (NPs)ranked The Oncology Nurse-APN/PA their favoritetabloid publication in the oncology nursing market.
� � � �� �� � �� �TON_April2011_v7_TON 4/7/11 2:09 PM Page 61

62 March/april 2011 I VOl 4, NO 2 www.TheOncologyNurse.com
Meetings
PROVENGE® (sipuleucel-T)Suspension for Intravenous Infusion Rx Only
BRIEF SUMMARY — See full Prescribing Information for complete product information
INDICATIONS AND USAGE: PROVENGE® (sipuleucel-T) is an autologous cellular immunotherapy indicated for the treatment of asymptomatic or minimally symptomatic metastatic castrate resistant (hormone refractory) prostate cancer.
DOSAGE AND ADMINISTRATION For Autologous Use Only.
given at approximately 2-week intervals.
as diphenhydramine.
on the infusion bag.Do Not Initiate Infusion of Expired Product.
Do Not Use a Cell Filter.
on the severity of the reaction.
(See Dosage and Administration [2] of full Prescribing Information.)
CONTRAINDICATIONS: None.
WARNINGS AND PRECAUTIONS
PROVENGE is intended solely for autologous use.
Acute infusion reactions
an acute infusion reaction.
patients in the PROVENGE group.
should be administered as needed.
Handling Precautions for Control of Infectious Disease. PROVENGE is notleukapheresis material and PROVENGE may carry the risk of transmitting infectious diseases to health care professionals handling the product. Universal precautions should be followed.
Concomitant Chemotherapy or Immunosuppressive Therapy. Use of either chemotherapy or immunosuppressive agents (such as systemic corticosteroids) given concurrently with the leukapheresis procedure or PROVENGE has not been
appropriate to reduce or discontinue immunosuppressive agents prior to treatment with PROVENGE.
Product Safety Testing. PROVENGE is released for infusion based on the microbial and sterility results from several tests: microbial contamination
-
results become positive for microbial contamination after PROVENGE has been
-
to determine the source of contamination.
(See Warnings and Precautions [5] of full Prescribing Information.)
ADVERSE REACTIONS
rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
PROVENGE group who underwent at least 1 leukapheresis procedure in four
peripheral blood mononuclear cells.
group included acute infusion reactions (see Warnings and Precautions) -
were Caucasian.
5-7 BRUSSELS, BELGIUMIMPAKT Breast Cancer Conferencewww.esmo.org
8-12 LONDON, UNITED KINGDOMEuropean Society for TherapeuticRadiation and Oncology InternationalOncology Forumwww.estro-events.org
3-7 CHICAGO, ILAmerican Society of Clinical OncologyAnnual Meetingwww.asco.org
23-25 ATHENS, GREECEMultinational Association of SupportiveCare in Cancer/International Society of Oral Oncology InternationalSymposiumwww.mascc2011.org
MAY 2011
©C
op
yrig
ht
Big
sto
ck.c
om
/Jo
ris&
Ba
rba
ra©
Co
pyrig
ht
Big
sto
ck.c
om
/ma
rty
©C
op
yrig
ht
Big
sto
ck.c
om
/Stu
art
B
21-24 CARLSBAD, CA12th International Lung CancerCongresswww.cancerlearning.com
15-17 LAS VEGAS, NVInternational Conference andExhibition on Cancer Science &Therapyhttp://omicsonline.org/cancerscience2011/
8-10 SAN FRANCISCO, CABreast Cancer Symposiumwww.breastcasymposium.org
JULY 2011 AUGUST 2011
©C
opyright
Big
sto
ck.c
om
/tu
ckerb
34
JUNE 2011
SEPTEMBER 2011
TON_April2011_v7_TON 4/7/11 10:54 AM Page 62

March/april 2011 I VOl 4, NO 2 63www.TheOncologyNurse.com
Meetings
Cerebrovascular Events.
(See Adverse Reactions [6] of full Prescribing Information.)
To report SUSPECTED ADVERSE REACTIONS, contact Dendreon Corporation at 1-877-336-3736 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Table 1 Incidence of Adverse Events Occurring in ≥5% of Patients Randomized to PROVENGE
Any Adverse EventChillsFatigueFever
NauseaJoint acheHeadacheCitrate toxicityParesthesiaVomiting
ConstipationPainParesthesia oralPain in extremity
Edema peripheralHot flushHematuria
Hypertension
Upper respiratory tract infection
chest painCoughNeck painWeight decreasedUrinary tract infectionRash
Tremor
591 (98.3)
186 (30.9)
291 (96.0)
97 (32.0)
All Gradesn (%)
All Gradesn (%)
Grade 3-5n (%)
Grade 3-5n (%)
PROVENGE (N = 601) Control* (N = 303)
*Control was non-activated autologous peripheral blood mononuclear cells.
P-A-11.10-073.00
Dendreon Corporation 3005 First Avenue Seattle, Washington 98121
23-27 STOCKHOLM, SWEDENEuropean Society for MedicalOncology European MultidisciplinaryCancer Congresswww.esmo.org
16-18 SAN ANTONIO, TXAcademy of Oncology NurseNavigators Second Annual Navigationand Survivorship Conferencewww.aonnonline.org
6-11 SAN ANTONIO, TX34th Annual San Antonio BreastCancer Symposiumwww.sabcs.org
10-13 SAN DIEGO, CAAmerican Society of HematologyAnnual Meeting and Expositionwww.hematology.org
SEPTEMBER 2011 DECEMBER 2011
TON_April2011_v7_TON 4/7/11 10:54 AM Page 63

Now, they are focused on it.
Before, Frank's immune cells could barely recognize a prostate cancer cell.
INDICATION: PROVENGE® (sipuleucel-T) is an autologous cellular immunotherapy indicated for the treatment of asymptomatic or minimally symptomatic metastatic castrate resistant (hormone refractory) prostate cancer. IMPORTANT SAFETY INFORMATION: PROVENGE is intended solely for autologous use and is not routinely tested for transmissible infectious diseases.In controlled clinical trials, serious adverse events reported in the PROVENGE group include acute infusion reactions (occurring within 1 day of infusion) and cerebrovascular events. Severe (Grade 3) acute infusion reactions were reported in 3.5% of patients in the PROVENGE group. Reactions included chills, fever, fatigue, asthenia, dyspnea, hypoxia, bronchospasm, dizziness, headache, hypertension, muscle ache, nausea, and vomiting. No Grade 4 or 5 acute infusion reactions were reported in patients in the PROVENGE group.The most common adverse events (incidence ≥15%) reported in the PROVENGE group are chills, fatigue, fever, back pain, nausea, joint ache, and headache.Please see Brief Summary of full Prescribing Information on the adjacent page.
www.PROVENGE.com
©2011 Dendreon Corporation. All rights reserved. February 2011. Printed in the U.S.A. Dendreon, the Dendreon logo, and PROVENGE are registered trademarks of Dendreon Corporation.P-A-02.11-007.00
In asymptomatic or minimally symptomatic metastatic castrate resistant prostate cancer
Stimulate a Response
*Control was nonactivated, autologous, peripheral blood mononuclear cells. †The dosing interval ranged from 1 to 15 weeks in controlled clinical trials.
Extends median survival beyond 2 years—25.8 months compared with 21.7 months for patients in the control* group (P=.032)
Reduction in risk of death—22.5% (HR=0.775, 95% CI: 0.614, 0.979)
Therapy completed in 3 cycles—3 infusions, at approximately 2-week intervals†
Most common adverse events are primarily mild or moderate— chills, fatigue, fever, back pain, nausea, joint ache, and headache
PROVENGE is the first in a new class of therapy that is designed to activate a patient’s own antigen-presenting cells
to stimulate an immune response against prostate cancer.
In asymptomatic or minimally symptomatic metastatic castr
In asymptomatic or minimally symptomatic metastatic castr
In asymptomatic or minimally symptomatic metastatic castr
In asymptomatic or minimally symptomatic metastatic castr
esistant prate rIn asymptomatic or minimally symptomatic metastatic castr
ostate canceresistant pr
In asymptomatic or minimally symptomatic metastatic castr
In asymptomatic or minimally symptomatic metastatic castr
In asymptomatic or minimally symptomatic metastatic castr
In asymptomatic or minimally symptomatic metastatic castr
esistant prate rIn asymptomatic or minimally symptomatic metastatic castr
ostate canceresistant pr
that is designed to activate a patientPROVENGE is the first in a new class of therapy
that is designed to activate a patientPROVENGE is the first in a new class of therapy
’that is designed to activate a patient
PROVENGE is the first in a new class of therapy
esenting cells s own antigen-pr
PROVENGE is the first in a new class of therapy
esenting cells
PROVENGE is the first in a new class of therapy
Reduction in risk of death—22.5%
with 21.7 months for patients in the contrExtends median survival beyond 2 years—
to stimulate an immune rthat is designed to activate a patient
Reduction in risk of death—22.5%
with 21.7 months for patients in the contrExtends median survival beyond 2 years—
to stimulate an immune rthat is designed to activate a patient
(HR=0.775, 95% CI: 0.614, 0.979)Reduction in risk of death—22.5%
oup (ol* grwith 21.7 months for patients in the contr25.8 months comparExtends median survival beyond 2 years—
esponse against pto stimulate an immune rs own antigen-pr’that is designed to activate a patient
(HR=0.775, 95% CI: 0.614, 0.979)
=.032)Poup (ed 25.8 months compar
recnacetatsoresponse against pesenting cells s own antigen-pr
(HR=0.775, 95% CI: 0.614, 0.979)
.resenting cells
IND
VENGE® (sipuleucel- PRO:ONITAATCIIND
chills, fatigue, feverMost common adverse events ar
Therapy completed in 3 cycles—
The dosing interval ranged fr†
ol was nonactivated, autologousContr*
T) is an autologous cellular immunotherVENGE® (sipuleucel-
, back pain ue, fever r, back pain, nausea, joint ache, and headache Most common adverse events ar
Therapy completed in 3 cycles—
om 1 to 15 weeks in contrThe dosing interval ranged fr, peripheral blood mononuclear cells.ol was nonactivated, autologous
T) is an autologous cellular immunother
, back pain, nausea, joint ache, and headache e primarily mild or moderate—Most common adverse events ar
3 infusions, at apprTherapy completed in 3 cycles—
olled clinical trials. om 1 to 15 weeks in contr, peripheral blood mononuclear cells.
apy indicated for the trT) is an autologous cellular immunother
, back pain, nausea, joint ache, and headache e primarily mild or moderate—
oximately 2-week intervals3 infusions, at appr
atment ofeapy indicated for the tr
†oximately 2-week intervals
eported in 3.5% ofr(occurring In trIMPORasymptomatic or minimally symptomatic metastatic castrIND
patients in the PROeported in 3.5% ofwithin 1 day of(occurring
trials,clinical olled contrIn infectious disesible ansmistr
INF SAFETY Y INFORMAANTT SAFETYTTANTIMPORasymptomatic or minimally symptomatic metastatic castr
VENGE® (sipuleucel- PRO:ONITAATCIIND
oupVENGE gr patients in the PROebr infusion) and cerwithin 1 day of
events adverse serious trials,ases.infectious dise
VENGE is intended solely for autologous use and is not r PROON:IT FORMA ATasymptomatic or minimally symptomatic metastatic castr
T) is an autologous cellular immunotherVENGE® (sipuleucel-
actions included chills,e R.oup Severovascular events.ebr
VENGE PROthe in eported revents
VENGE is intended solely for autologous use and is not resistant (hormone rate rasymptomatic or minimally symptomatic metastatic castr
T) is an autologous cellular immunother
asthenia, fatigue,, feveractions included chills,ade 3) acute infusion re (Gr Sever
acute include oup grVENGE
VENGE is intended solely for autologous use and is not rostate canceractory) prefresistant (hormone r
apy indicated for the trT) is an autologous cellular immunother
xia, hypoa, dyspne asthenia,eactions wereade 3) acute infusion r
actionserinfusion acute
outinely tested forVENGE is intended solely for autologous use and is not r.ostate cancer
atment ofeapy indicated for the tr
PnauseTer
br
Summary ofase see BriefleP and heache, joint a,nauseadverse most common he
eported in patients in the PROe ractions weres, dizzinesonchospasm,br
patients in the PROeported in 3.5% of
escribing Information on the adjacent page.rP full Summary ofadache. and he
(incidence ≥15%) events adverse VENGE greported in patients in the PRO
hypertension,adache, hes,VENGE gr
escribing Information on the adjacent page.
VENGE PROthe in eported r(incidence ≥15%) .oupVENGE gr
and vomiting.a, nause muscle ache, hypertension,oup
escribing Information on the adjacent page.
fatigue,chills,e oup argrVENGE
ade 4 or 5 acute infusion No Gr and vomiting. fatigue,
pain, back ,fever fatigue,
ade 4 or 5 acute infusion hypo dyspne
P-A-02.11-007.00ademarktr
eon,DendrAll rights r©2011 Dendr
P-A-02.11-007.00ation.orporeon C Dendrs of
egistere rVENGE ar and PRO,eon logo the Dendreon,.S.A.rinted in the U Pebruary 2011. Feserved.
ation.orporeon C©2011 Dendr
ed egister
www
.comPROVENGE.www
Stimulate a Response
Stimulate a Response
Stimulate a Response
TON_April2011_v7_TON 4/7/11 10:54 AM Page Cov4