Embed Size (px)
Citation preview
Close-out report
CQI for Nutrition Assessment Counselling and Support program
March 2015
ACKNOWLEDGEMENTSThis training and mentorship report is made possible by the generous support of the American people through the U.S. Agency for International Development (USAID), through United States Government’s President’s Emergency Plan for AIDS Relief and FHI360. The contents and opinions expressed herein do not necessarily reflect the views of USAID or the United States Government.
Project contract number: 5586
Contents
1
CONTENTSINTRODUCTION ............................................................................................................................................2
QUALITY IMPROVEMENT TRAINING WORKSHOP .......................................................................................2
QUALITY IMPROVEMENT MENTORSHIP .....................................................................................................4
SOMKHELE CLINIC ....................................................................................................................................5
HLABISA GATEWAY CLINIC ...................................................................................................................... 11
KWAMSANE CLINIC ..................................................................................................................................17
HLABISA HOSPITAL ..................................................................................................................................21
INHLWATHI CLINIC ................................................................................................................................... 27
CONCLUSION ............................................................................................................................................ 31
CQI for Nutrition Assessment Counselling and Support program
2
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
INTRODUCTIONThe South Africa Nutrition Assessment, Counselling and Support Training Program is a USAID-funded program. The training and mentorship was provided by University Research Co., LLC (URC). The course is designed to assist the staff who work in the health sector to introduce
and improve Nutrition Assessment Counselling and Support (NACS) in South Africa, drawing on the science of Quality Improvement (QI) and how this approach may be used to make health care provision better. The course takes the participants through a simulation exercise of a NACS improvement journey during the workshop and the mentorship at facility level supports participants in applying the approach and using the tools in a real life situation in the field.
The initial 3-day course is followed by 6 months of coaching visits. Coaching is critical in providing practical support to help clinics:
» Form representative teams;
» Set aims and targets specific to their local needs, usually within larger national improvement aims;
» Develop measurement systems, including proper recording, data collection, aggregation and analysis;
» Facilitate discussions of the problems and possible solutions to test;
» Provide ongoing training and support for the improvement cycle (plan-do-study-act);
» Advocate for resolution of larger system issues such as supply chain, financial or policy problems;
» Integrate improvement into their ongoing work; and
» Synthesize learning.
QUALITY IMPROVEMENT TRAINING WORKSHOP
The Quality Improvement Training Workshop was conducted on 3 – 5 June 2014 at Hluhluwe Protea Hotel in uMkhanyakude District in KwaZulu-Natal Province.
The course was attended by 30 participants from the National Department of Health (NDoH), USAID, FHI360, the Provincial Department of Health (PDoH) of KwaZulu-Natal, and the uMkhanyakude district management and facility staff. Training was provided by two facilitators from URC/USAID’s Applying Science to Strengthen and Improve Systems (ASSIST) with support from two additional URC facilitators.
The training content drew on a comprehensive training manual titled ‘How to Improve
Health Care: Case Study for Nutrition Assessment Counselling and Support ’, which provided interactive content, presentations and practical applications of the theory being covered. The content addressed basic quality concepts, identified and explained the tools that can be used to identify quality gaps, understand systems and monitor performance, and shared QI models and strategies.
“[QI] breaks down a big problem into manageable chunks.” A. Bayai, NACS workshop participant
“QI requires teamwork.” M. Chapfunga, NACS workshop participant
3
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
The main findings from the three-day workshop, as observed and deduced by the consultants, included the following:
» There was a high level of active participation from all the participants and a keen interest in the content. The sessions commenced in a timely manner.
» The NDoH, PDoH, USAID and FHI staff provided valuable and extensive support during the training.
» Participants had only limited existing knowledge about improvement concepts and processes and how QI differs from Monitoring & Evaluation (M&E).
» None of the participants had been trained on NACS prior to the workshop. This required the facilitators to provide general information on NACS.
» There does not seem to be any specific focus on HIV or TB clients, and the NACS focus seems to be mostly on children.
» Mid-upper arm circumference (MUAC) and body mass index (BMI) measurements are conducted to a large extent, but there is little follow-up action in relation to the results.
» The participants were professionals who are keen to embrace new knowledge and expressed a strong commitment to implementing QI in relation to NACS work.
The workshop was highly interactive and included extensive group work. All participants engaged actively and positively and with a strong task-oriented focus. The following were the outputs from each day:
DAY 1 » Developed an improvement aim based on the case study
» Identified members of an improvement team based on the case study
» Developed a fishbone to analyze a problem based on their facility’s situation
» Developed a flowchart based on the case study or their current NACS process
DAY 2The participants were divided into 5 groups, with each group containing a member from a facility. The groups:
» Developed indicators to measure performance in NACS
» Plotted a time series chart based on case study data
» Developed a change package of improvement interventions
DAY 3 » Developed an improvement plan for NACS based on the facility’s existing
services and challenges
» Developed a process flowchart based on the improvement plan
“While you started work on improving one problem, you end up improving other problems which results in strengthening the whole system.” E. Gundani, NACS workshop participant
“It teaches you that accountability is essential. You have to take responsibility for your role in the QI team.” S. Barnardt, NACS workshop participant
“It helped staff to realize that the assumed problem was not the real problem and changed unrealistic expectations.” P. Baxen, NACS workshop participant
4
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
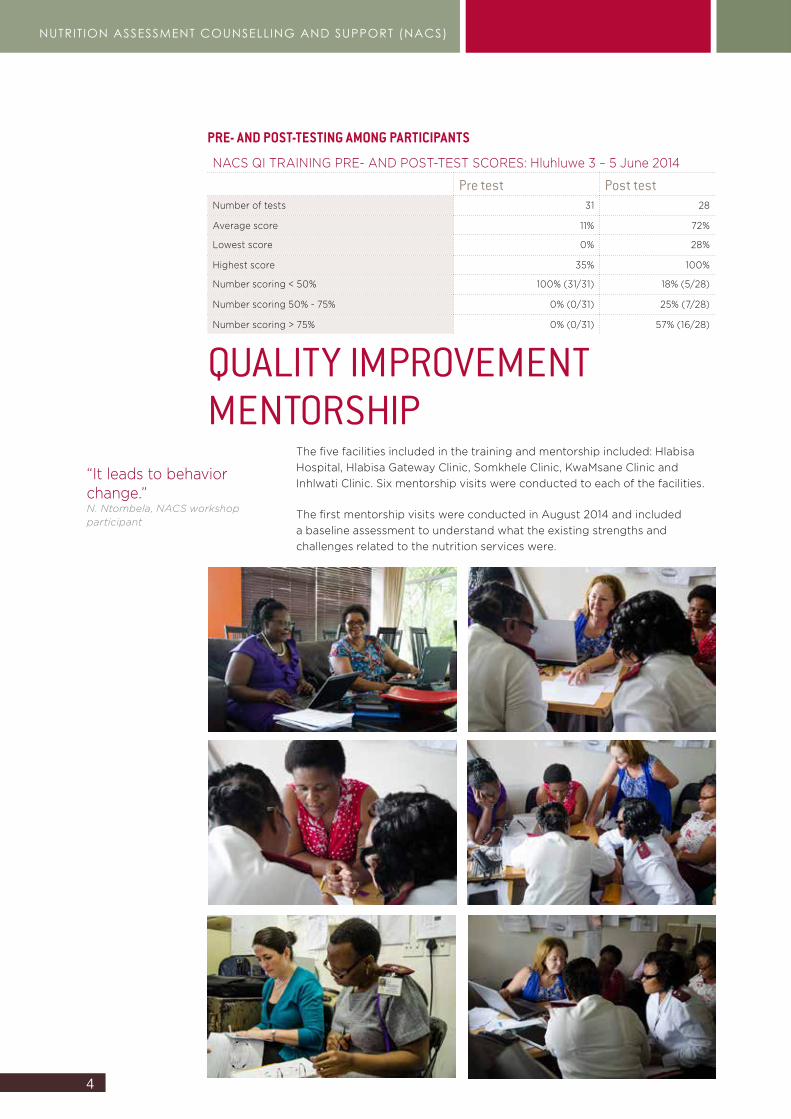
PRE- AND POST-TESTING AMONG PARTICIPANTS
NACS QI TRAINING PRE- AND POST-TEST SCORES: Hluhluwe 3 – 5 June 2014
Pre test Post testNumber of tests 31 28
Average score 11% 72%
Lowest score 0% 28%
Highest score 35% 100%
Number scoring < 50% 100% (31/31) 18% (5/28)
Number scoring 50% - 75% 0% (0/31) 25% (7/28)
Number scoring > 75% 0% (0/31) 57% (16/28)
QUALITY IMPROVEMENT MENTORSHIP
The five facilities included in the training and mentorship included: Hlabisa Hospital, Hlabisa Gateway Clinic, Somkhele Clinic, KwaMsane Clinic and Inhlwati Clinic. Six mentorship visits were conducted to each of the facilities.
The first mentorship visits were conducted in August 2014 and included a baseline assessment to understand what the existing strengths and challenges related to the nutrition services were.
“It leads to behavior change.” N. Ntombela, NACS workshop participant
5
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
Somkhele Clinic
SUMMARY OF QUALITY IMPROVEMENT PROJECTBackgroundQI training was conducted in June 2014. The training was attended by the operational manager, Sister Zungu, and the nutritional advisor, Thuthukani Nyawo. On 4 August 2014, the mentorship team conducted a baseline assessment at Somkhele Clinic on the quality of NACS services provided.
The baseline assessment revealed that there was no planning for the provision of NACS services. The facility had sufficient human resources. The facility had most of the guidelines related to nutrition – however, knowledge on the content of these guidelines was limited. Staff had to search for the guidelines and some were found in a box with other documents. There were no standard operating procedures for nutrition services. The nutrition advisor seemed to be the person leading the nutrition services. Nutrition supplies (supplementary nutrition products) and equipment (scales and measuring equipment) were available, except for equipment for the demonstration of preparing food safely. Storage was done correctly – however, the storage area was dirty.
In relation to nutrition services, clients were weighed but not measured, except when seen by the nutrition advisor. The Road to Health booklets for children aged less than 5 years were incomplete. The growth charts were not filled in and there was no interpretation of the results or recording of appropriate actions taken. Children that were malnourished were not identified and managed.
Health education was provided regularly by the nutrition advisor – however, there was poor recording of education topics and the number of clients that received education. There was poor linkage with community health workers and no guide for the referral of malnourished clients within the facility. There was no M&E of the nutrition services and no supervision or mentorship.
During July, the two staff members who attended the NACS QI training provided feedback to the rest of Somkhele staff on what was learned during the workshop. A quality improvement team was established and the team decided that due to the poor performance of the facility on the rate of exclusive breastfeeding (EBF) at 14 weeks, they wanted to improve the recording of EBF at 14 weeks.
“The NACS program has helped us to detect malnourished under-five children better and at an earlier stage – previously we struggled to detect these problems, and caught them much later. Early detection means we can intervene quicker and more effectively.” J.J. Zuma – Professional Nurse
6
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
Improvement aimInitial improvement aim: To improve the recording of EBF from 59% to 90% by December 2014. After testing the change, the team realized that the recording was incorrect and clients would not benefit from improved recording. The improvement aim was changed by the QI team to: To improve EBF rates at 14 weeks from 0% (accurate) to 90% at Somkhele Clinic by December 2014 through raising the use of 24 hour recall (question asked by staff to clients), training all nurses and community health workers on EBF and recording EBF.
Problem analysisThe QI team analyzed the problem of poor EBF rates at 14 weeks by using a cause and effect tool (fishbone) and developing a flowchart to identify problems in the process from registration to receiving nutrition assessment and support.
The following contributing factors were identified:
Staff ClientsInadequate knowledge and skillsPoor recordingAttitude
Cultural beliefsMisconceptionsLong distance from clinicLimited EBF knowledgeTransport costsFinancial constraints
Resources ClinicLack of EBF counselling job aidLimited EBF guidelines
Weak referral systemLong queuesHigh catchment populationFlow of clients and where weight and length are measured
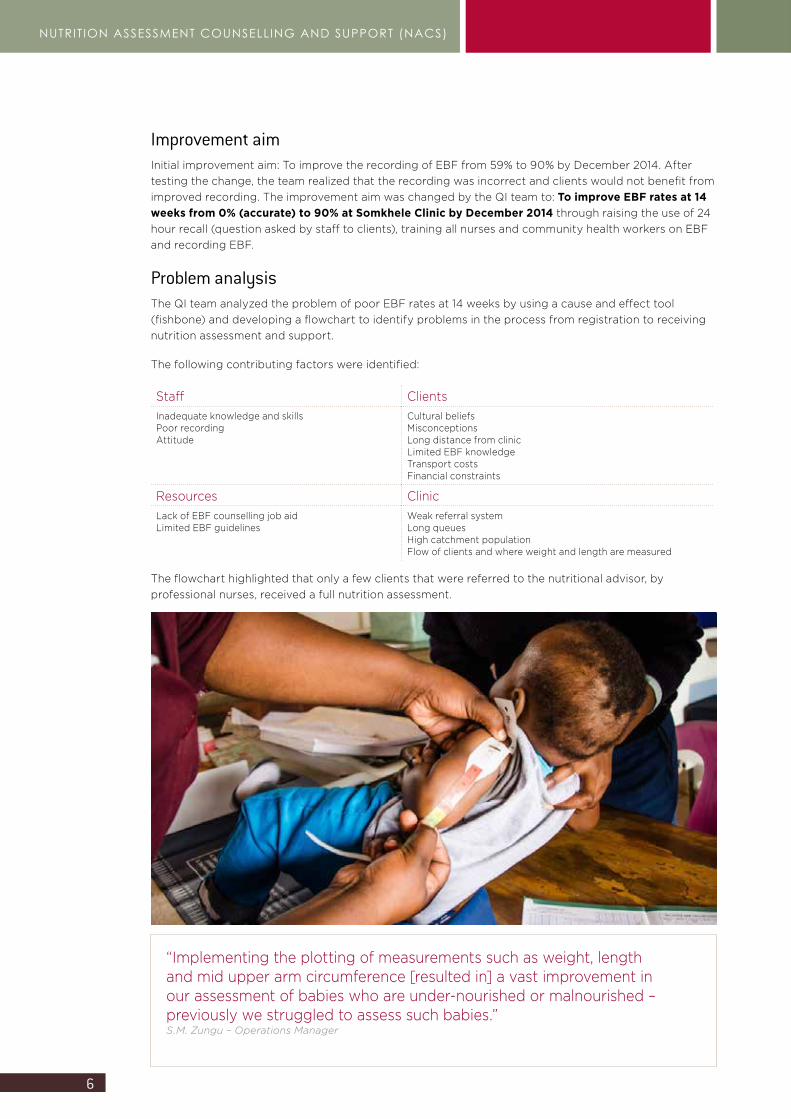
The flowchart highlighted that only a few clients that were referred to the nutritional advisor, by professional nurses, received a full nutrition assessment.
“Implementing the plotting of measurements such as weight, length and mid upper arm circumference [resulted in] a vast improvement in our assessment of babies who are under-nourished or malnourished – previously we struggled to assess such babies.” S.M. Zungu – Operations Manager
7
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
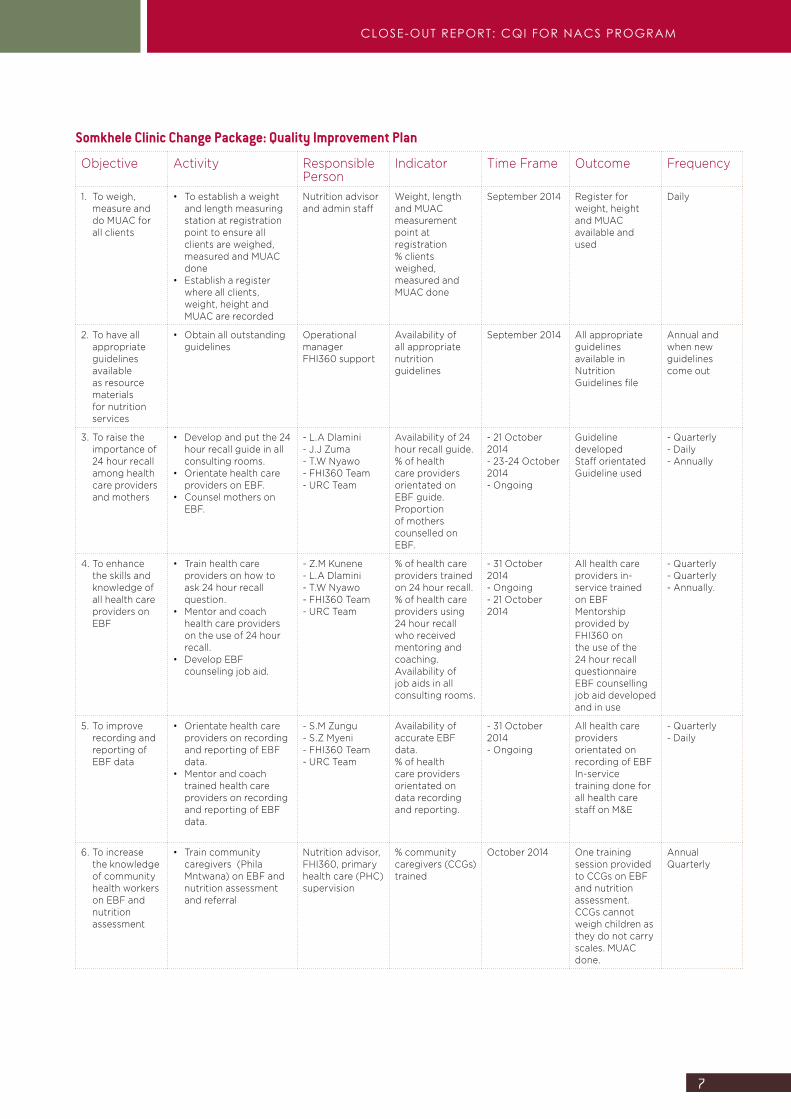
Somkhele Clinic Change Package: Quality Improvement Plan
Objective Activity Responsible Person
Indicator Time Frame Outcome Frequency
1. To weigh, measure and do MUAC for all clients
• To establish a weight and length measuring station at registration point to ensure all clients are weighed, measured and MUAC done
• Establish a register where all clients, weight, height and MUAC are recorded
Nutrition advisor and admin staff
Weight, length and MUAC measurement point at registration% clients weighed, measured and MUAC done
September 2014 Register for weight, height and MUAC available and used
Daily
2. To have all appropriate guidelines available as resource materials for nutrition services
• Obtain all outstanding guidelines
Operational managerFHI360 support
Availability of all appropriate nutrition guidelines
September 2014 All appropriate guidelines available in Nutrition Guidelines file
Annual and when new guidelines come out
3. To raise the importance of 24 hour recall among health care providers and mothers
• Develop and put the 24 hour recall guide in all consulting rooms.
• Orientate health care providers on EBF.
• Counsel mothers on EBF.
- L.A Dlamini- J.J Zuma- T.W Nyawo- FHI360 Team- URC Team
Availability of 24 hour recall guide.% of health care providers orientated on EBF guide.Proportion of mothers counselled on EBF.
- 21 October 2014- 23-24 October 2014 - Ongoing
Guideline developedStaff orientatedGuideline used
- Quarterly- Daily- Annually
4. To enhance the skills and knowledge of all health care providers on EBF
• Train health care providers on how to ask 24 hour recall question.
• Mentor and coach health care providers on the use of 24 hour recall.
• Develop EBF counseling job aid.
- Z.M Kunene- L.A Dlamini- T.W Nyawo- FHI360 Team- URC Team
% of health care providers trained on 24 hour recall.% of health care providers using 24 hour recall who received mentoring and coaching.Availability of job aids in all consulting rooms.
- 31 October 2014- Ongoing- 21 October 2014
All health care providers in-service trained on EBFMentorship provided by FHI360 on the use of the 24 hour recall questionnaireEBF counselling job aid developed and in use
- Quarterly- Quarterly- Annually.
5. To improve recording and reporting of EBF data
• Orientate health care providers on recording and reporting of EBF data.
• Mentor and coach trained health care providers on recording and reporting of EBF data.
- S.M Zungu- S.Z Myeni- FHI360 Team- URC Team
Availability of accurate EBF data.% of health care providers orientated on data recording and reporting.
- 31 October 2014- Ongoing
All health care providers orientated on recording of EBFIn-service training done for all health care staff on M&E
- Quarterly- Daily
6. To increase the knowledge of community health workers on EBF and nutrition assessment
• Train community caregivers (Phila Mntwana) on EBF and nutrition assessment and referral
Nutrition advisor, FHI360, primary health care (PHC) supervision
% community caregivers (CCGs) trained
October 2014 One training session provided to CCGs on EBF and nutrition assessment. CCGs cannot weigh children as they do not carry scales. MUAC done.
AnnualQuarterly
8
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
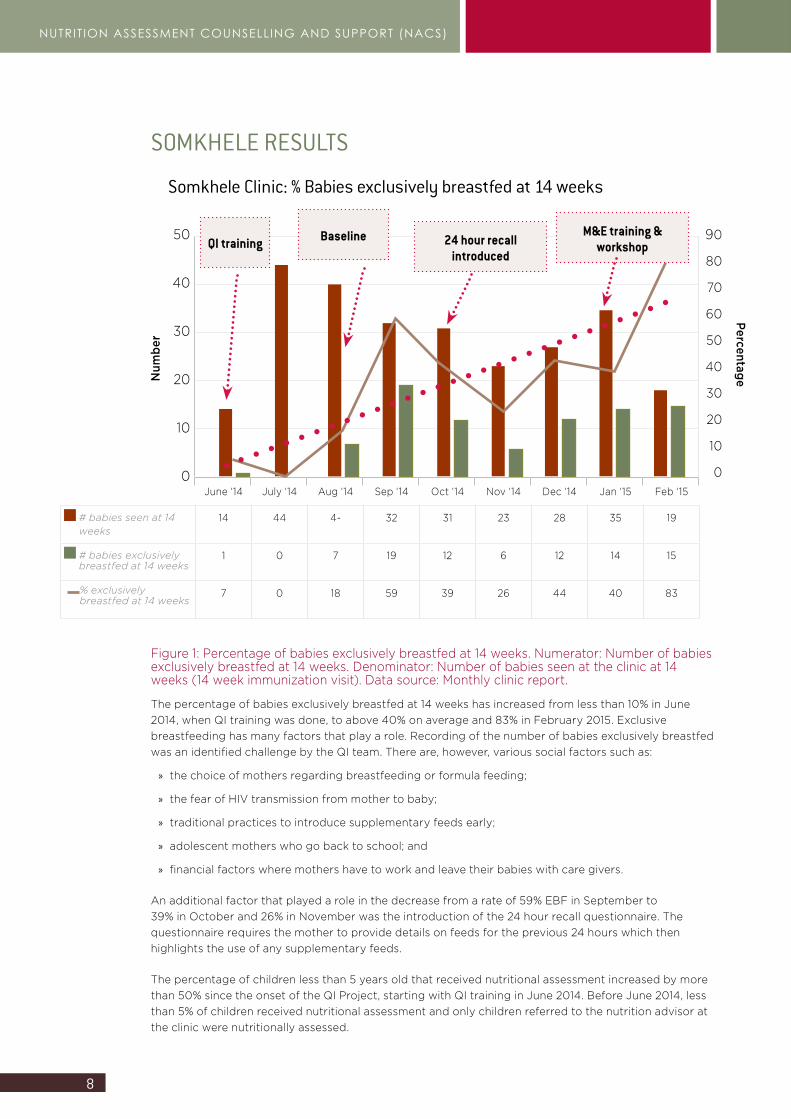
Somkhele Clinic: % Babies exclusively breastfed at 14 weeks
50
40
30
20
10
0
Num
ber
June ‘14 July ‘14 Aug ‘14 Sep ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
# babies seen at 14 weeks
14 44 4- 32 31 23 28 35 19
# babies exclusively breastfed at 14 weeks
1 0 7 19 12 6 12 14 15
% exclusively breastfed at 14 weeks
7 0 18 59 39 26 44 40 83
Baseline 24 hour recall introduced
M&E training & workshop
90
80
70
60
50
40
30
20
10
0
Percentage
QI training
Figure 1: Percentage of babies exclusively breastfed at 14 weeks. Numerator: Number of babies exclusively breastfed at 14 weeks. Denominator: Number of babies seen at the clinic at 14 weeks (14 week immunization visit). Data source: Monthly clinic report.
The percentage of babies exclusively breastfed at 14 weeks has increased from less than 10% in June 2014, when QI training was done, to above 40% on average and 83% in February 2015. Exclusive breastfeeding has many factors that play a role. Recording of the number of babies exclusively breastfed was an identified challenge by the QI team. There are, however, various social factors such as:
» the choice of mothers regarding breastfeeding or formula feeding;
» the fear of HIV transmission from mother to baby;
» traditional practices to introduce supplementary feeds early;
» adolescent mothers who go back to school; and
» financial factors where mothers have to work and leave their babies with care givers.
An additional factor that played a role in the decrease from a rate of 59% EBF in September to 39% in October and 26% in November was the introduction of the 24 hour recall questionnaire. The questionnaire requires the mother to provide details on feeds for the previous 24 hours which then highlights the use of any supplementary feeds.
The percentage of children less than 5 years old that received nutritional assessment increased by more than 50% since the onset of the QI Project, starting with QI training in June 2014. Before June 2014, less than 5% of children received nutritional assessment and only children referred to the nutrition advisor at the clinic were nutritionally assessed.
SOMKHELE RESULTS
9
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
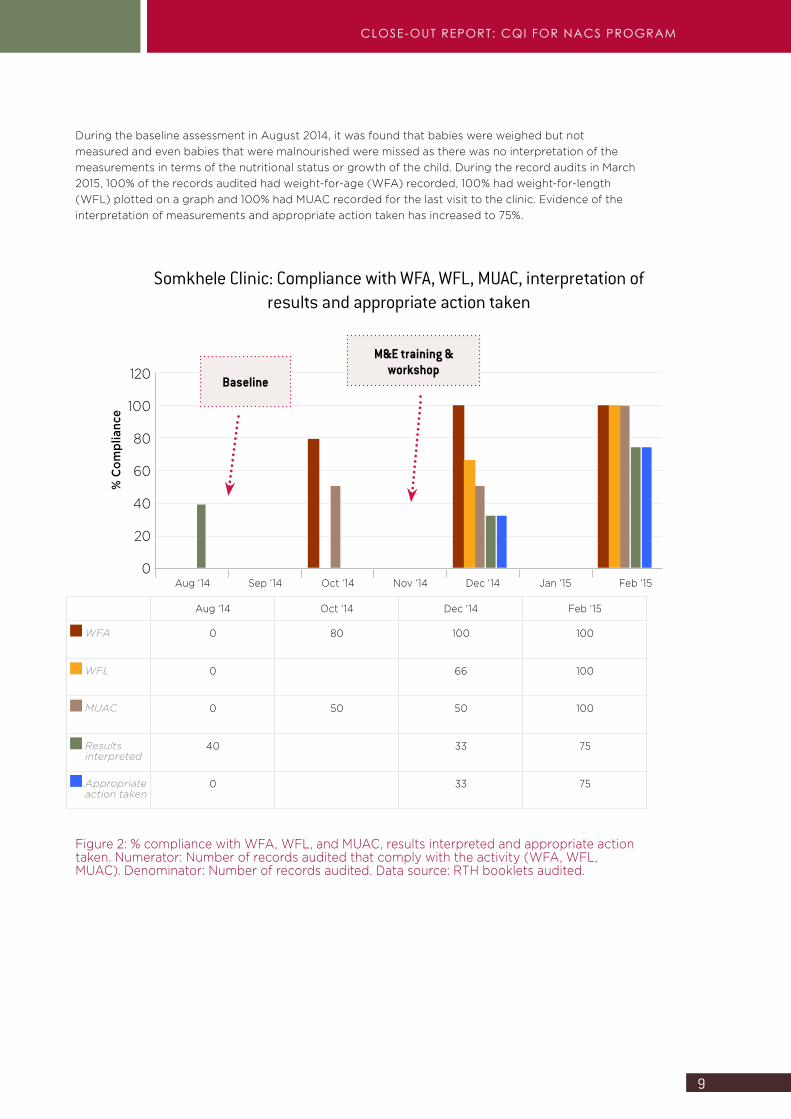
Somkhele Clinic: Compliance with WFA, WFL, MUAC, interpretation of results and appropriate action taken
120
100
80
60
40
20
0
% C
ompl
ianc
e
Aug ‘14 Sep ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
Baseline
M&E training & workshop
Aug ‘14 Oct ‘14 Dec ‘14 Feb ‘15
WFA 0 80 100 100
WFL 0 66 100
MUAC 0 50 50 100
Results interpreted
40 33 75
Appropriate action taken
0 33 75
Figure 2: % compliance with WFA, WFL, and MUAC, results interpreted and appropriate action taken. Numerator: Number of records audited that comply with the activity (WFA, WFL, MUAC). Denominator: Number of records audited. Data source: RTH booklets audited.
During the baseline assessment in August 2014, it was found that babies were weighed but not measured and even babies that were malnourished were missed as there was no interpretation of the measurements in terms of the nutritional status or growth of the child. During the record audits in March 2015, 100% of the records audited had weight-for-age (WFA) recorded, 100% had weight-for-length (WFL) plotted on a graph and 100% had MUAC recorded for the last visit to the clinic. Evidence of the interpretation of measurements and appropriate action taken has increased to 75%.
10
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
“We encourage mothers to exclusively breastfeed their babies up to 6 months, and to avoid mixed feeding for the first months, and we encourage them to bring their children to the clinic on a monthly basis to monitor their growth and development.” S.M. Zungu – Operations Manager
“We also try to encourage mothers to exclusively breastfeed until the baby is six months old, and we encourage the use of condoms until the baby is that age – continuing to have unprotected sex may render a baby HIV-positive who was born HIV-negative and to an HIV-negative mother.” T.P. Nkosi – Enrolled Nurse
“We have seen improvements in terms of weight gain where children and adults were previously suffering from malnutrition. But we have also seen people being able to bring uncontrolled diabetes and hypertension under control by changing their habits to include a more balanced diet.” T. Nyawo – Nutritional Advisor
Once we have detected a case of malnutrition, we start an intervention of supplementary feeding and education and information provision, and then monitor the child on a monthly basis. If the mother fails to bring the child in every month, we phone the mother and remind her to bring the child for monitoring. T. Nyawo – Nutritional Advisor
11
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
SUMMARY OF QUALITY IMPROVEMENT PROJECT BackgroundQI training was conducted in June 2014. The training was attended by a professional nurse and the nutritional advisor. On 5 August 2014, the mentorship team conducted a baseline assessment at Hlabisa Gateway Clinic on the quality of NACS services provided.
The baseline assessment revealed that there was no planning for nutrition services at the facility. The facility seemed to have limited human resources available. The clinic is situated close to the Hlabisa Hospital’s gate and provides all PHC services. The facility lacked many of the guidelines related to nutrition and knowledge on the content of guidelines was limited. There were no standard operating procedures for nutrition services. Nutrition supplies (supplementary nutrition products) and equipment (scales and measuring equipment) were available, except for equipment for the demonstration of preparing food safely. The scales were not calibrated and the measuring of babies was not accurately done. The storage area was clean and dry. The nutrition supplements were, however, stored directly against a wall and sunlight was shining directly on the supplements.
In relation to nutrition services, clients were weighed but not measured, except when seen by the nutrition advisor. Very few clients were referred to the nutrition advisor. The Road to Health booklets for children less than 5 years were incomplete. The growth charts were not plotted and there was no interpretation of results or recording of appropriate actions taken. Staff did not know what the role of the nutrition advisor was.
Health education was provided daily by the nutrition advisor as well as by professional nurses. Information and education communication (IEC) materials were available at the facility and nutrition related pamphlets were provided to clients. There was poor recording of the education topics covered and the number of clients that received education. There was poor linkage with the community and community services even though there were CCGs linked to the clinic. The operational manager was not sure about what they were doing in the community. There was no guide for the referral of malnourished clients within the facility and few clients were referred to the nutrition advisor. There was no M&E of the nutrition services and no supervision or mentorship. The priority problem identified was: Low rate of nutrition assessment and counselling for children less than 5 years of age.
Hlabisa Gateway Clinic
12
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
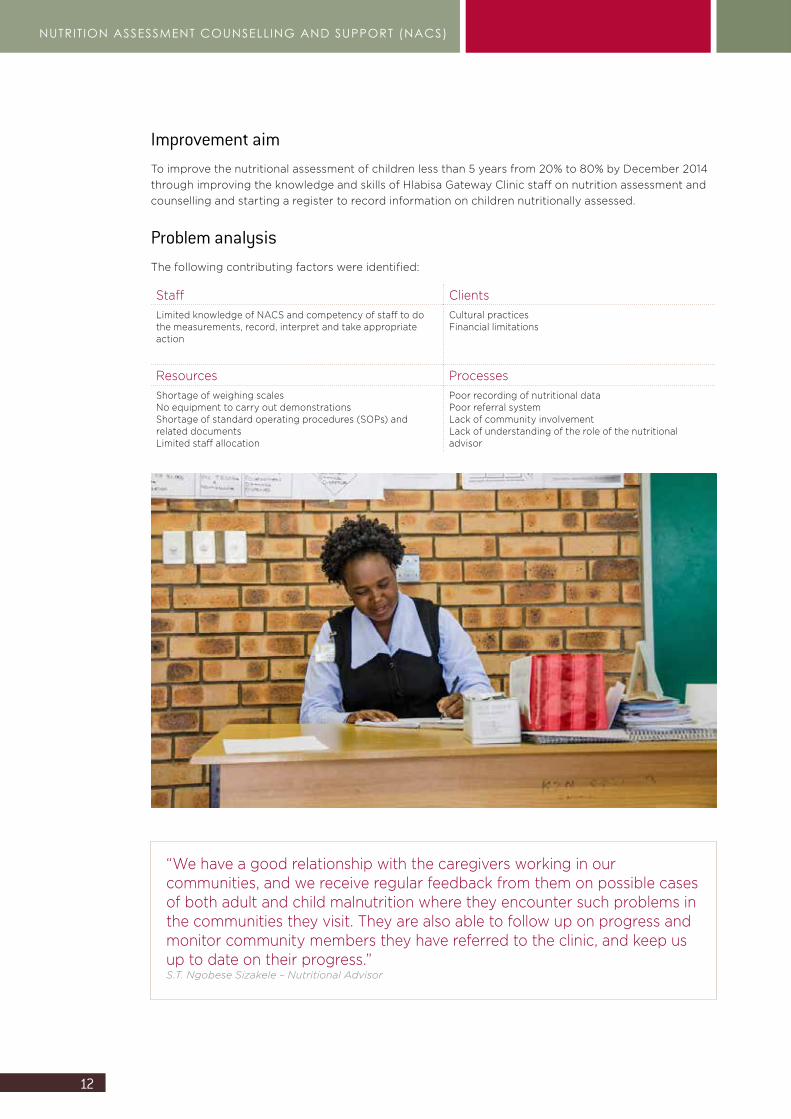
Improvement aimTo improve the nutritional assessment of children less than 5 years from 20% to 80% by December 2014 through improving the knowledge and skills of Hlabisa Gateway Clinic staff on nutrition assessment and counselling and starting a register to record information on children nutritionally assessed.
Problem analysisThe following contributing factors were identified:
Staff ClientsLimited knowledge of NACS and competency of staff to do the measurements, record, interpret and take appropriate action
Cultural practicesFinancial limitations
Resources ProcessesShortage of weighing scales No equipment to carry out demonstrations Shortage of standard operating procedures (SOPs) and related documentsLimited staff allocation
Poor recording of nutritional dataPoor referral system Lack of community involvementLack of understanding of the role of the nutritional advisor
“We have a good relationship with the caregivers working in our communities, and we receive regular feedback from them on possible cases of both adult and child malnutrition where they encounter such problems in the communities they visit. They are also able to follow up on progress and monitor community members they have referred to the clinic, and keep us up to date on their progress.” S.T. Ngobese Sizakele – Nutritional Advisor
13
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
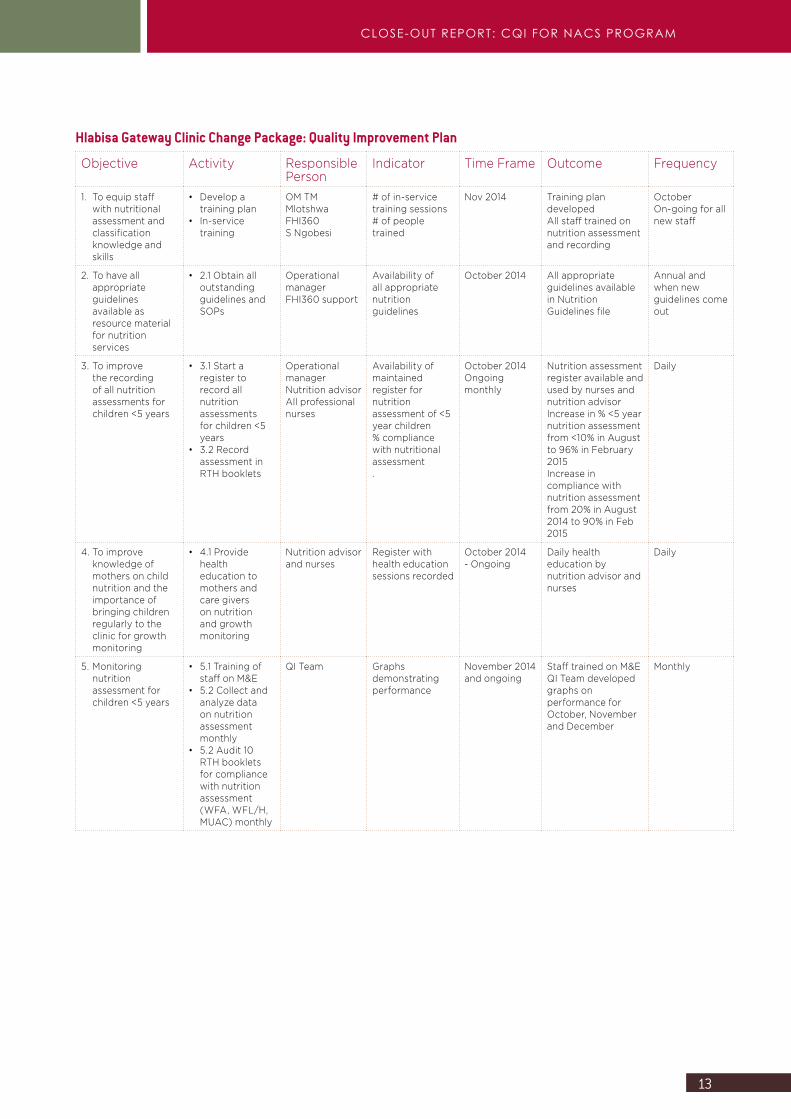
Hlabisa Gateway Clinic Change Package: Quality Improvement Plan
Objective Activity Responsible Person
Indicator Time Frame Outcome Frequency
1. To equip staff with nutritional assessment and classification knowledge and skills
• Develop a training plan
• In-service training
OM TM MlotshwaFHI360S Ngobesi
# of in-service training sessions# of people trained
Nov 2014 Training plan developedAll staff trained on nutrition assessment and recording
October On-going for all new staff
2. To have all appropriate guidelines available as resource material for nutrition services
• 2.1 Obtain all outstanding guidelines and SOPs
Operational managerFHI360 support
Availability of all appropriate nutrition guidelines
October 2014 All appropriate guidelines available in Nutrition Guidelines file
Annual and when new guidelines come out
3. To improve the recording of all nutrition assessments for children <5 years
• 3.1 Start a register to record all nutrition assessments for children <5 years
• 3.2 Record assessment in RTH booklets
Operational managerNutrition advisorAll professional nurses
Availability of maintained register for nutrition assessment of <5 year children% compliance with nutritional assessment.
October 2014Ongoingmonthly
Nutrition assessment register available and used by nurses and nutrition advisorIncrease in % <5 year nutrition assessment from <10% in August to 96% in February 2015Increase in compliance with nutrition assessment from 20% in August 2014 to 90% in Feb 2015
Daily
4. To improve knowledge of mothers on child nutrition and the importance of bringing children regularly to the clinic for growth monitoring
• 4.1 Provide health education to mothers and care givers on nutrition and growth monitoring
Nutrition advisor and nurses
Register with health education sessions recorded
October 2014- Ongoing
Daily health education by nutrition advisor and nurses
Daily
5. Monitoring nutrition assessment for children <5 years
• 5.1 Training of staff on M&E
• 5.2 Collect and analyze data on nutrition assessment monthly
• 5.2 Audit 10 RTH booklets for compliance with nutrition assessment (WFA, WFL/H, MUAC) monthly
QI Team Graphs demonstrating performance
November 2014 and ongoing
Staff trained on M&EQI Team developed graphs on performance for October, November and December
Monthly
14
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
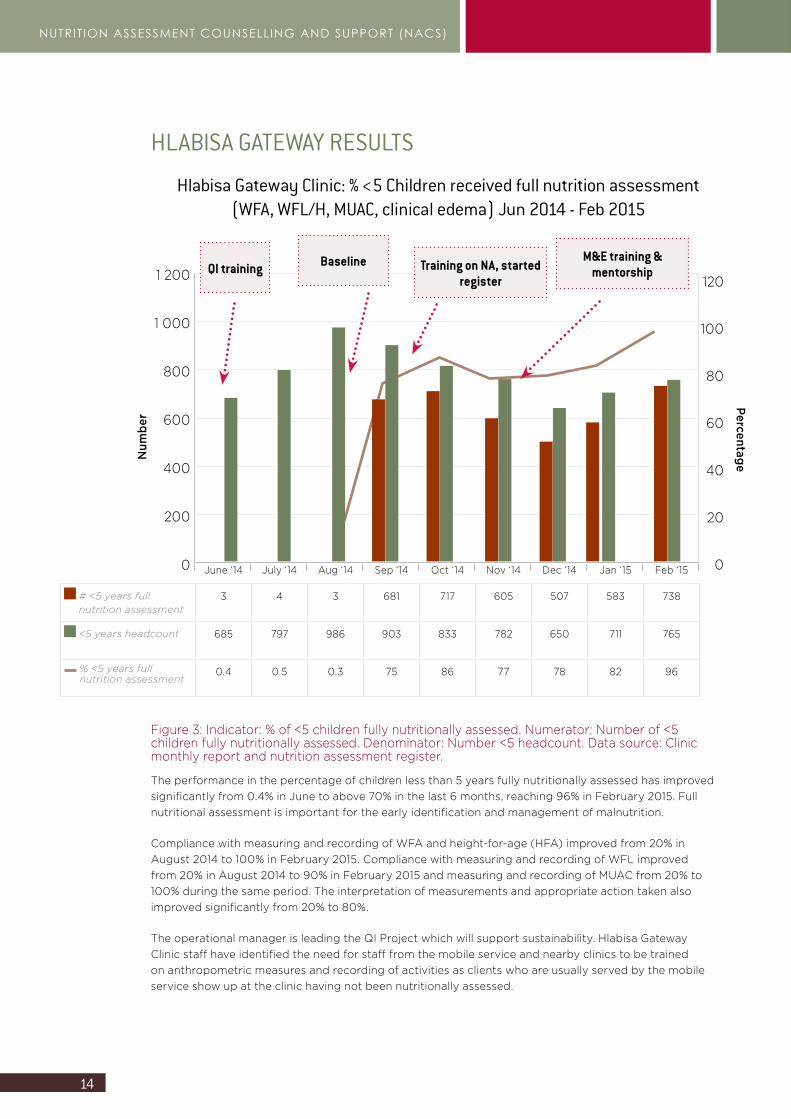
Hlabisa Gateway Clinic: % <5 Children received full nutrition assessment (WFA, WFL/H, MUAC, clinical edema) Jun 2014 - Feb 2015
1 200
1 000
800
600
400
200
0
Num
ber
June ‘14 July ‘14 Aug ‘14 Sep ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
# <5 years full nutrition assessment
3 4 3 681 717 605 507 583 738
<5 years headcount 685 797 986 903 833 782 650 711 765
% <5 years full nutrition assessment
0.4 0.5 0.3 75 86 77 78 82 96
Baseline Training on NA, started register
M&E training & mentorship
120
100
80
60
40
20
0
Percentage
QI training
Figure 3: Indicator: % of <5 children fully nutritionally assessed. Numerator: Number of <5 children fully nutritionally assessed. Denominator: Number <5 headcount. Data source: Clinic monthly report and nutrition assessment register.
The performance in the percentage of children less than 5 years fully nutritionally assessed has improved significantly from 0.4% in June to above 70% in the last 6 months, reaching 96% in February 2015. Full nutritional assessment is important for the early identification and management of malnutrition.
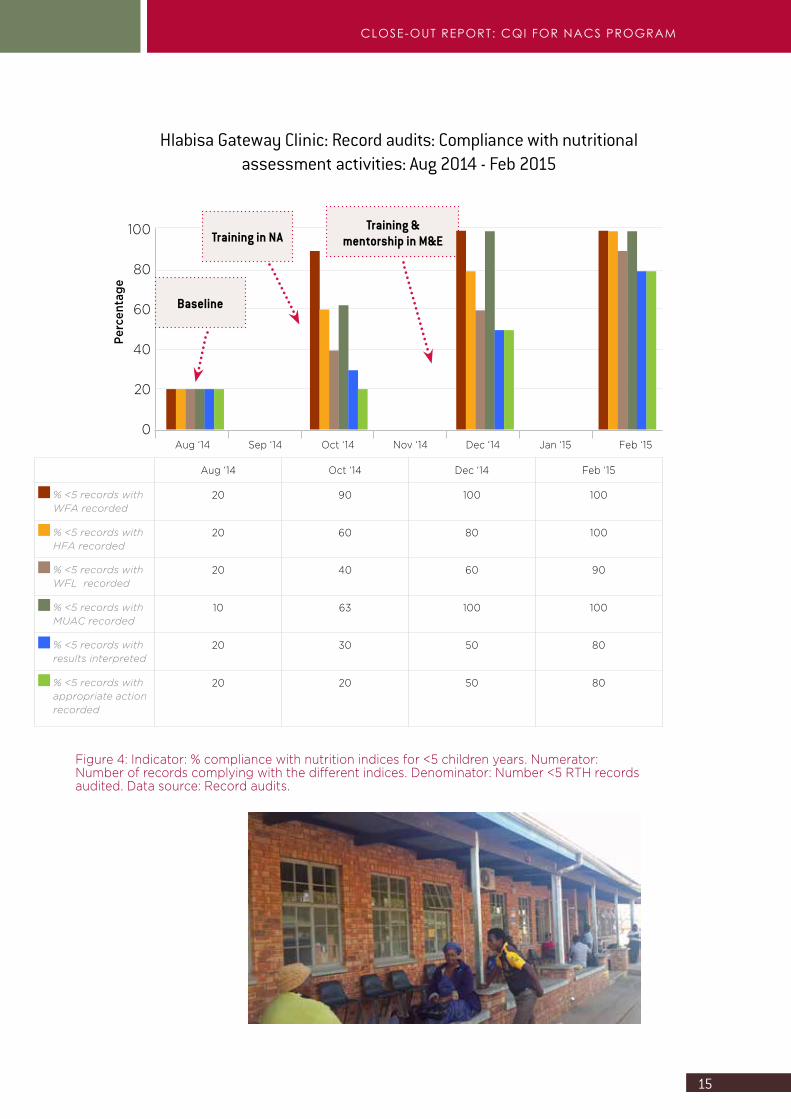
Compliance with measuring and recording of WFA and height-for-age (HFA) improved from 20% in August 2014 to 100% in February 2015. Compliance with measuring and recording of WFL improved from 20% in August 2014 to 90% in February 2015 and measuring and recording of MUAC from 20% to 100% during the same period. The interpretation of measurements and appropriate action taken also improved significantly from 20% to 80%.
The operational manager is leading the QI Project which will support sustainability. Hlabisa Gateway Clinic staff have identified the need for staff from the mobile service and nearby clinics to be trained on anthropometric measures and recording of activities as clients who are usually served by the mobile service show up at the clinic having not been nutritionally assessed.
HLABISA GATEWAY RESULTS
15
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
Hlabisa Gateway Clinic: Record audits: Compliance with nutritional assessment activities: Aug 2014 - Feb 2015
100
80
60
40
20
0
Perc
enta
ge
Aug ‘14 Sep ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
Baseline
Training in NATraining &
mentorship in M&E
Aug ‘14 Oct ‘14 Dec ‘14 Feb ‘15
% <5 records with WFA recorded
20 90 100 100
% <5 records with HFA recorded
20 60 80 100
% <5 records with WFL recorded
20 40 60 90
% <5 records with MUAC recorded
10 63 100 100
% <5 records with results interpreted
20 30 50 80
% <5 records with appropriate action recorded
20 20 50 80
Figure 4: Indicator: % compliance with nutrition indices for <5 children years. Numerator: Number of records complying with the different indices. Denominator: Number <5 RTH records audited. Data source: Record audits.
16
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
“We try to encourage mothers-to-be to start visiting the clinic from early on, while they are still pregnant, so that we can educate them both on how to look after their babies’ nutritional needs once they are born, but also to be able to look after both mother and baby already during their pregnancy. We have found our twice-weekly group education sessions to be well attended and to give mothers a head start in knowing how to feed and care for their babies.” S.T. Ngobese Sizakele – Nutritional Advisor
17
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
KwaMsane Clinic
SUMMARY OF QUALITY IMPROVEMENT PROJECTBackgroundQI training was conducted in June 2014. The training was attended by a professional nurse and the nutritional advisor. On 6 August 2014, the mentorship team conducted a baseline assessment at KwaMsane clinic on the quality of NACS services provided.
The baseline assessment revealed that there was no planning for the provision of NACS services. The facility had sufficient human resources. The facility had most of the guidelines related to nutrition – however, knowledge on the content of the guidelines was limited. There were no standard operating procedures for nutrition services. Nutrition supplies (supplementary nutrition products) and equipment (scales and measuring equipment) were available, except for equipment for the demonstration of preparing food safely. The storage area was clean and dry – however, nutrition supplements were stored directly on the floor and against a wall.
In relation to nutrition services, clients were weighed but not measured, except when seen by the nutrition advisor. The Road to Health booklets for children less than 5 years were incomplete. The growth charts were not filled in and there was no interpretation of results or recording of appropriate actions taken. Children that were malnourished were not identified and managed. The majority of children that were admitted to Hlabisa Hospital with malnutrition, came from KwaMsane.
Health education was provided daily by the nutrition advisor as well as professional nurses. IEC materials were available at the facility. There was poor recording of the education topics covered and the number of clients that received education. There was linkage with the community through the clinic committee and community health workers. There was no guide for the referral of malnourished clients within the facility. There was no M&E of the nutrition services and no supervision or mentorship.
After the NACS QI training in June, the two staff members who attended the training provided feedback to the rest of KwaMsane staff on what was learned during the workshop. A QI Team was established and the team started doing MUAC for children and BMI for adults. The KwaMsane staff identified the low percentage of children less than 5 years that received nutrition assessment at the facility as the priority problem for improvement.
“This QI has changed our work forever. It opened our eyes and has not only improved the nutrition services, but all our programs and, most of all, our morale and attitudes.” Sr Ndaba
18
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
Improvement aimTo increase the percentage of children less than 5 years who are nutritionally assessed (measuring weight, height, MUAC, and edema) and classified from 0% to 90% in KwaMsane clinic, by the end of January 2015.
The % of children less than 5 years nutritionally assessed was, however, not monitored as only children assessed by the nutrition advisor and one professional nurse (integrated management of childhood illness – IMCI) were monitored. The % compliance with nutrition assessment for children was monitored through bi-monthly record audits of Road to Health booklets.
Problem analysisThe following contributing factors were identified:
Staff Clients
Inadequate knowledge and skillsPoor recordingAttitudePoor compliance with nutrition assessmentHigh staff turnover of IMCI trained nurses
Attitude towards clinic services
Resources Processes
Staff allocation not adequate for 24 hour service Clients from feeder clinics not assessedHigh patient loadNutrition assessment done only by IMCI nurse, when not available – not done
“NACS has been useful for monitoring the progress of babies and children - we can track if they’ve gained weight and if they are the correct weight and height for their age group. If they are below weight we give the mother nutritional advice according to Road to Health guidelines for the child’s age group.” T. Gumede – Professional Nurse
19
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
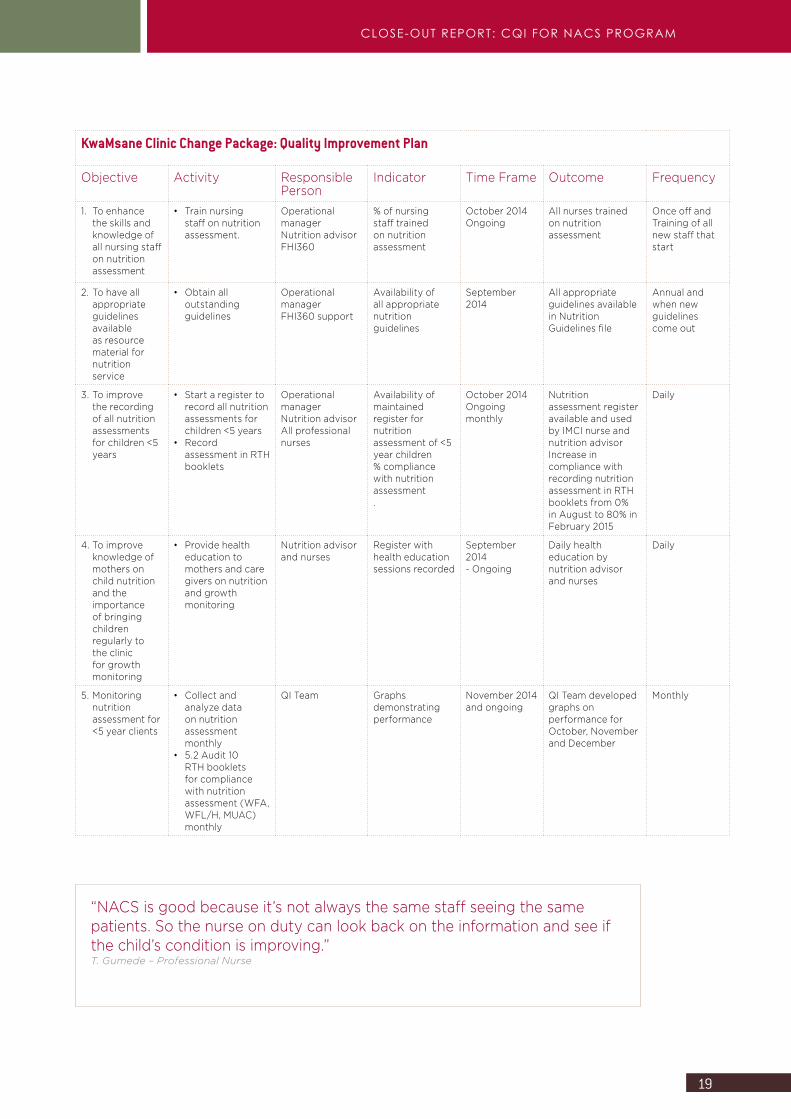
KwaMsane Clinic Change Package: Quality Improvement Plan
Objective Activity Responsible Person
Indicator Time Frame Outcome Frequency
1. To enhance the skills and knowledge of all nursing staff on nutrition assessment
• Train nursing staff on nutrition assessment.
Operational managerNutrition advisorFHI360
% of nursing staff trained on nutrition assessment
October 2014Ongoing
All nurses trained on nutrition assessment
Once off andTraining of all new staff that start
2. To have all appropriate guidelines available as resource material for nutrition service
• Obtain all outstanding guidelines
Operational managerFHI360 support
Availability of all appropriate nutrition guidelines
September 2014
All appropriate guidelines available in Nutrition Guidelines file
Annual and when new guidelines come out
3. To improve the recording of all nutrition assessments for children <5 years
• Start a register to record all nutrition assessments for children <5 years
• Record assessment in RTH booklets
Operational managerNutrition advisorAll professional nurses
Availability of maintained register for nutrition assessment of <5 year children% compliance with nutrition assessment.
October 2014Ongoingmonthly
Nutrition assessment register available and used by IMCI nurse and nutrition advisorIncrease in compliance with recording nutrition assessment in RTH booklets from 0% in August to 80% in February 2015
Daily
4. To improve knowledge of mothers on child nutrition and the importance of bringing children regularly to the clinic for growth monitoring
• Provide health education to mothers and care givers on nutrition and growth monitoring
Nutrition advisor and nurses
Register with health education sessions recorded
September 2014- Ongoing
Daily health education by nutrition advisor and nurses
Daily
5. Monitoring nutrition assessment for <5 year clients
• Collect and analyze data on nutrition assessment monthly
• 5.2 Audit 10 RTH booklets for compliance with nutrition assessment (WFA, WFL/H, MUAC) monthly
QI Team Graphs demonstrating performance
November 2014 and ongoing
QI Team developed graphs on performance for October, November and December
Monthly
“NACS is good because it’s not always the same staff seeing the same patients. So the nurse on duty can look back on the information and see if the child’s condition is improving.” T. Gumede – Professional Nurse
20
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
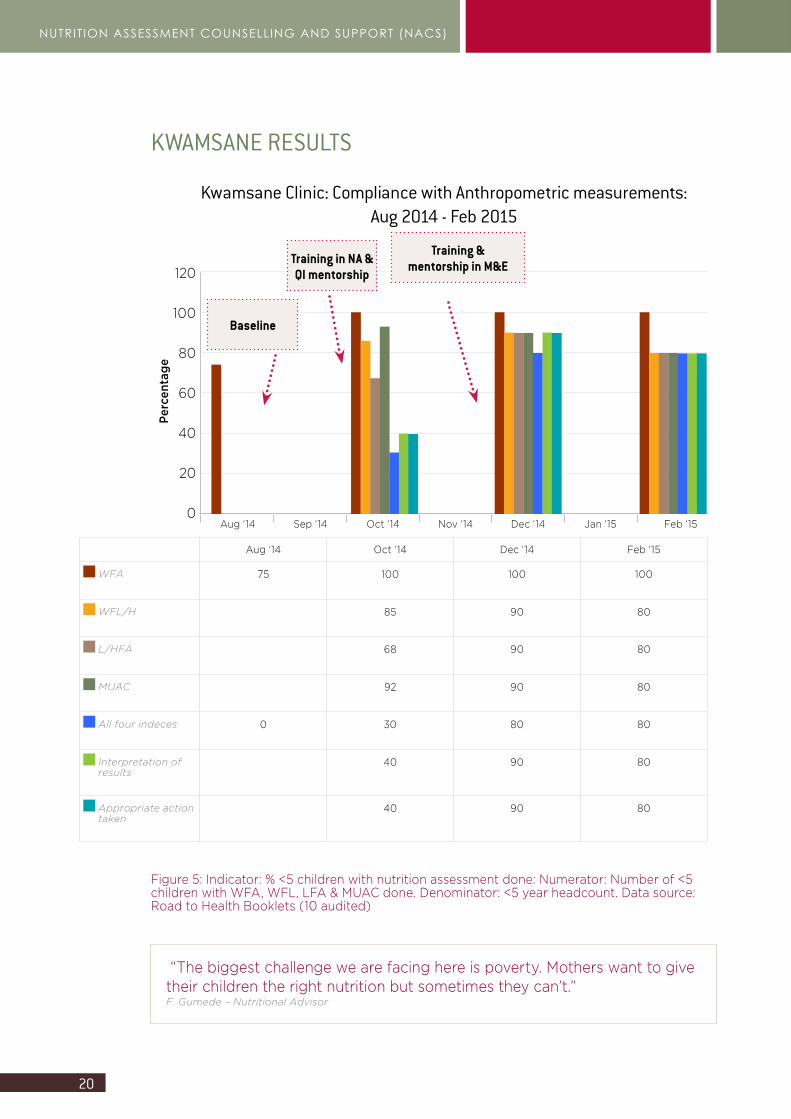
Kwamsane Clinic: Compliance with Anthropometric measurements: Aug 2014 - Feb 2015
120
100
80
60
40
20
0
Perc
enta
ge
Aug ‘14 Sep ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
Baseline
Training in NA & QI mentorship
Training & mentorship in M&E
Aug ‘14 Oct ‘14 Dec ‘14 Feb ‘15
WFA 75 100 100 100
WFL/H 85 90 80
L/HFA 68 90 80
MUAC 92 90 80
All four indeces 0 30 80 80
Interpretation of results
40 90 80
Appropriate action taken
40 90 80
Figure 5: Indicator: % <5 children with nutrition assessment done: Numerator: Number of <5 children with WFA, WFL, LFA & MUAC done. Denominator: <5 year headcount. Data source: Road to Health Booklets (10 audited)
KWAMSANE RESULTS
“The biggest challenge we are facing here is poverty. Mothers want to give their children the right nutrition but sometimes they can’t.” F. Gumede – Nutritional Advisor
21
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
Hlabisa Hospital
SUMMARY OF QUALITY IMPROVEMENT PROJECTBackgroundQI training was conducted in June 2014. The training was attended by two nurses from the facility. On return from the training, the staff members provided feedback on what was learned to other facility staff. In the OPD, the trained staff members established a QI Team and started a register to record nutrition assessments conducted. Weight, height and MUAC (for children older than 6 months) were introduced and BMI and MUAC for adults. On 6 August 2014, the mentorship team conducted a baseline assessment at Hlabisa Hospital on the quality of NACS services provided.
The baseline assessment revealed that there was no planning for nutrition services at the facility. The OPD seemed to have limited human resources available and no nutrition advisor. The facility lacked many of the guidelines related to nutrition and knowledge on the content of guidelines was limited. There were no standard operating procedures for the nutrition services. Nutrition supplies (supplementary nutrition products) were available and were issued by the hospital dietician. Nutrition supplements were stored correctly. Weight and length measuring equipment was available. There was, however, only one baby scale and measuring device for OPD, while there are several consulting rooms.
In relation to nutrition services, clients were weighed but not measured. Since the training in June, the staff started doing MUAC for children older than 6 months and BMI for adults. Road to Health booklets for children less than 5 years were incomplete. Clients that attend OPD were, however, not regular clients and receive PHC care from the referring clinics.
Health education was provided daily by nursing staff, but on various topics and little evidence of nutrition education existed. IEC materials were available at the nutrition unit, away from OPD. Clients were only referred to the dietician by doctors. There was poor linkage with the PHC services. There was no M&E of the nutrition services and no supervision or mentorship. Knowledge and skills on nutrition assessment was limited. Nutrition assessment in tuberculosis (TB), antiretroviral therapy (ART) and ante natal units was also poor.
The priority problem identified by the OPD staff was: Low rate of nutrition assessment and counselling for children less than 5 years of age.
22
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
Improvement aimTo improve nutritional assessment of children less than 5 years from 20% to 80% by December 2014 through improving knowledge and skills of Hlabisa Hospital OPD staff on nutrition assessment and counselling and starting a register to record information on children nutritionally assessed.
Problem analysis
The following contributing factors were identified:
Staff ClientsLimited knowledge of NACS and competency of staff to do the measurements, record, interpret and take appropriate actionStaff attitudeStaff rotation
High patient load
Resources ProcessesShortage of scales, length mat and MUAC tapes Shortage of SOPs and related documentsLimited staff allocation Limited space
Poor recording of nutritional dataPoor referral system Limited availability of policies and guidelines related to nutritionPoor communication
“I need the clinic staff’s help and healthcare advice to make sure my baby is ok as he grows up. For example, they weigh and measure my baby and take his temperature – things I can’t do at home myself.” S. Mnguni – client of nutrition program at OPD
23
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
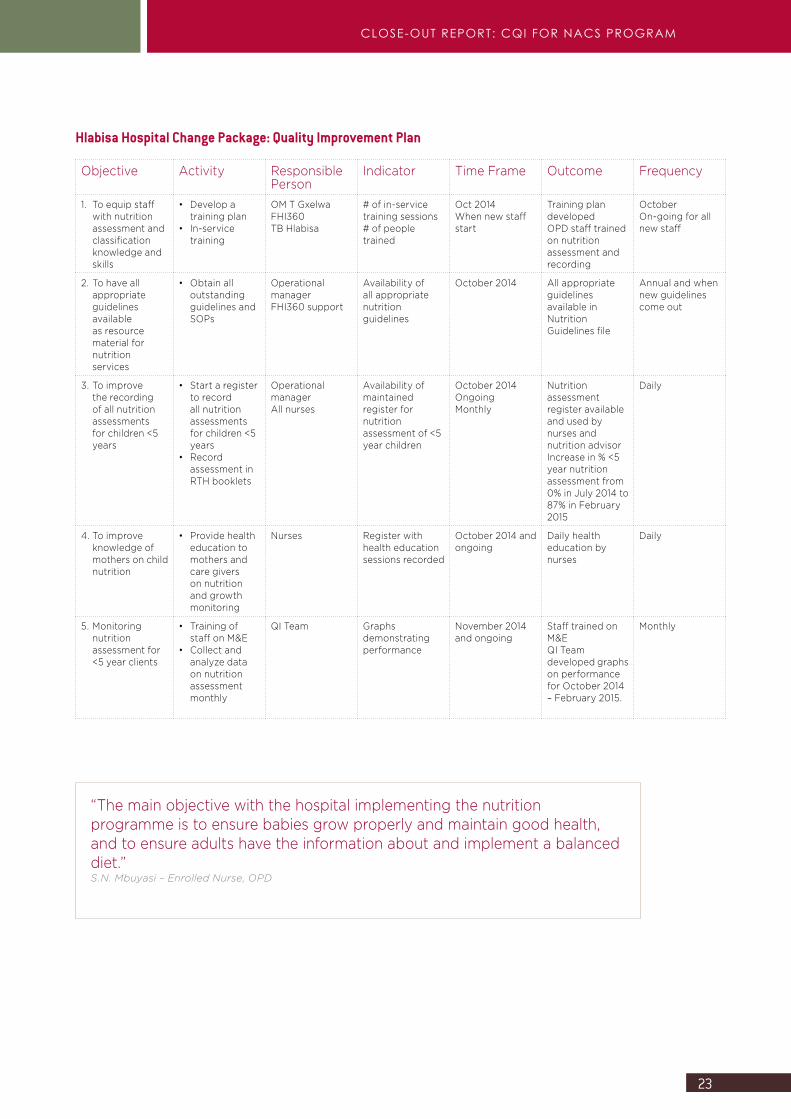
Hlabisa Hospital Change Package: Quality Improvement Plan
Objective Activity Responsible Person
Indicator Time Frame Outcome Frequency
1. To equip staff with nutrition assessment and classification knowledge and skills
• Develop a training plan
• In-service training
OM T GxelwaFHI360TB Hlabisa
# of in-service training sessions# of people trained
Oct 2014When new staff start
Training plan developedOPD staff trained on nutrition assessment and recording
October On-going for all new staff
2. To have all appropriate guidelines available as resource material for nutrition services
• Obtain all outstanding guidelines and SOPs
Operational managerFHI360 support
Availability of all appropriate nutrition guidelines
October 2014 All appropriate guidelines available in Nutrition Guidelines file
Annual and when new guidelines come out
3. To improve the recording of all nutrition assessments for children <5 years
• Start a register to record all nutrition assessments for children <5 years
• Record assessment in RTH booklets
Operational managerAll nurses
Availability of maintained register for nutrition assessment of <5 year children
October 2014OngoingMonthly
Nutrition assessment register available and used by nurses and nutrition advisorIncrease in % <5 year nutrition assessment from 0% in July 2014 to 87% in February 2015
Daily
4. To improve knowledge of mothers on child nutrition
• Provide health education to mothers and care givers on nutrition and growth monitoring
Nurses Register with health education sessions recorded
October 2014 and ongoing
Daily health education by nurses
Daily
5. Monitoring nutrition assessment for <5 year clients
• Training of staff on M&E
• Collect and analyze data on nutrition assessment monthly
QI Team Graphs demonstrating performance
November 2014 and ongoing
Staff trained on M&EQI Team developed graphs on performance for October 2014 – February 2015.
Monthly
“The main objective with the hospital implementing the nutrition programme is to ensure babies grow properly and maintain good health, and to ensure adults have the information about and implement a balanced diet.” S.N. Mbuyasi – Enrolled Nurse, OPD
24
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
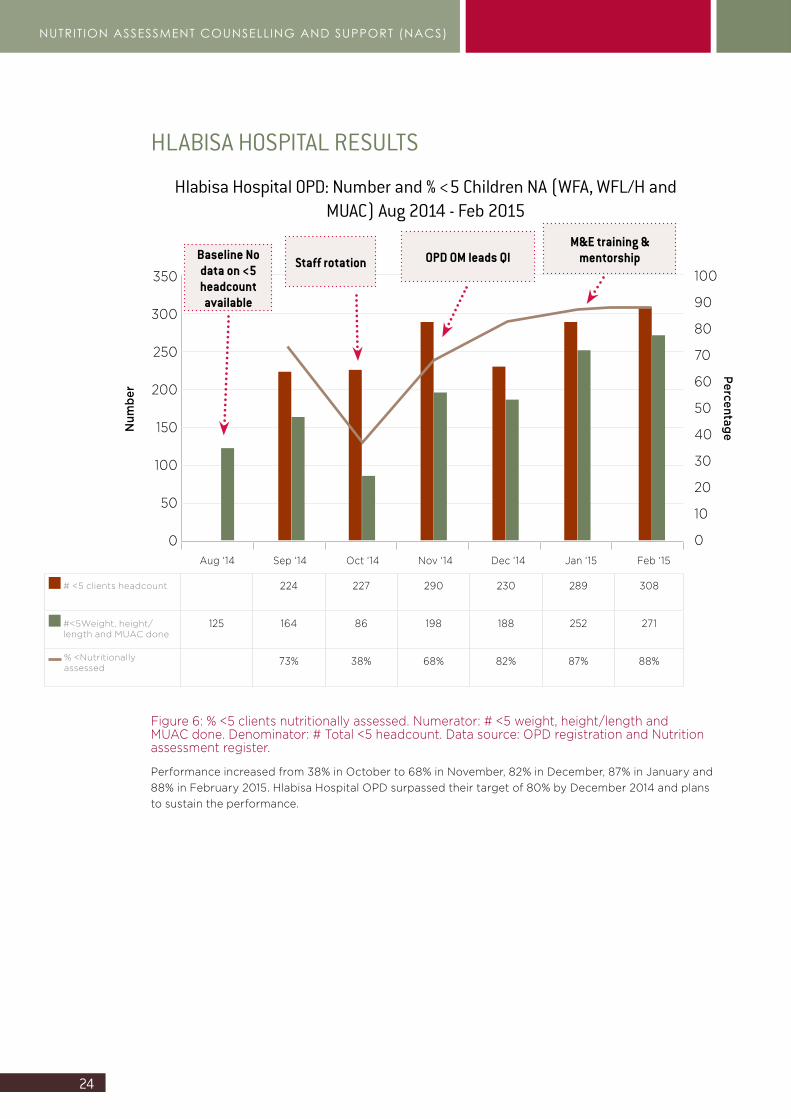
HLABISA HOSPITAL RESULTS
Figure 6: % <5 clients nutritionally assessed. Numerator: # <5 weight, height/length and MUAC done. Denominator: # Total <5 headcount. Data source: OPD registration and Nutrition assessment register.
Performance increased from 38% in October to 68% in November, 82% in December, 87% in January and 88% in February 2015. Hlabisa Hospital OPD surpassed their target of 80% by December 2014 and plans to sustain the performance.
Hlabisa Hospital OPD: Number and % <5 Children NA (WFA, WFL/H and MUAC) Aug 2014 - Feb 2015
350
300
250
200
150
100
50
0
Num
ber
# <5 clients headcount 224 227 290 230 289 308
#<5Weight, height/length and MUAC done
125 164 86 198 188 252 271
% <Nutritionally assessed
73% 38% 68% 82% 87% 88%
Staff rotation OPD OM leads QIM&E training &
mentorship100
90
80
70
60
50
40
30
20
10
0
Percentage
Baseline No data on <5 headcount available
Aug ‘14 Sep ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
25
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
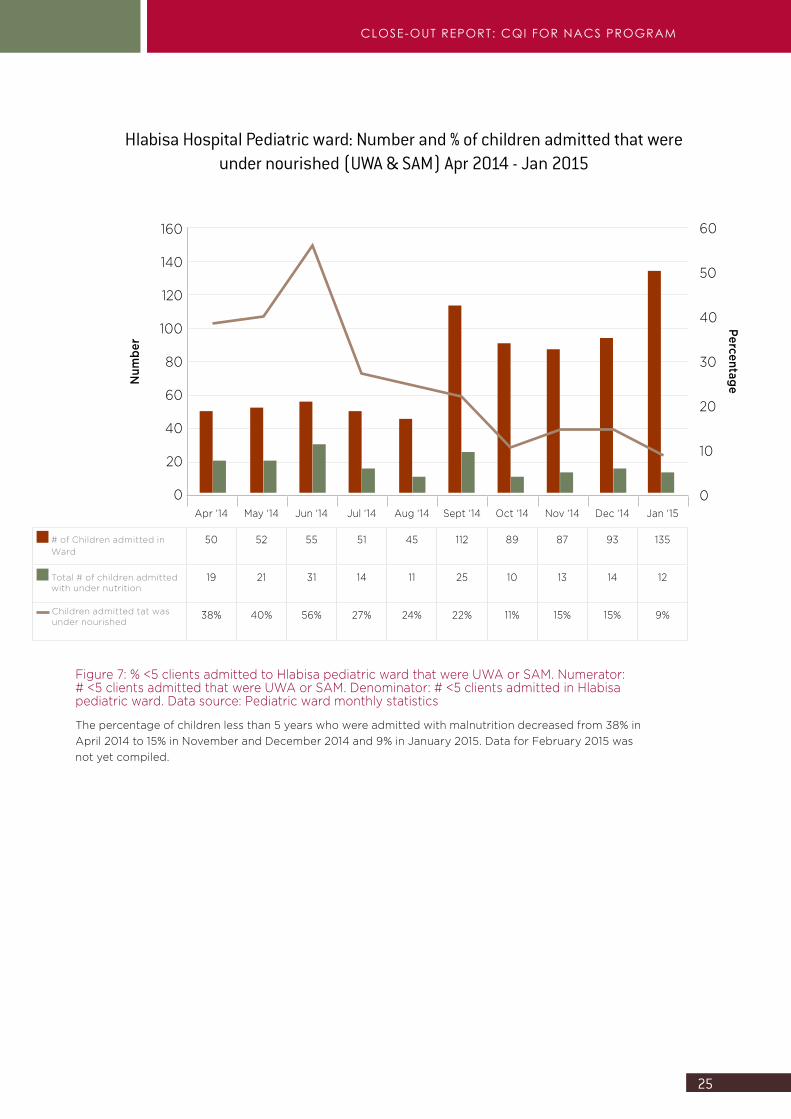
Figure 7: % <5 clients admitted to Hlabisa pediatric ward that were UWA or SAM. Numerator: # <5 clients admitted that were UWA or SAM. Denominator: # <5 clients admitted in Hlabisa pediatric ward. Data source: Pediatric ward monthly statistics
The percentage of children less than 5 years who were admitted with malnutrition decreased from 38% in April 2014 to 15% in November and December 2014 and 9% in January 2015. Data for February 2015 was not yet compiled.
Hlabisa Hospital Pediatric ward: Number and % of children admitted that were under nourished (UWA & SAM) Apr 2014 - Jan 2015
160
140
120
100
80
60
40
20
0
Num
ber
Apr ‘14 May ‘14 Jun ‘14 Jul ‘14 Aug ‘14 Sept ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15
# of Children admitted in Ward
50 52 55 51 45 112 89 87 93 135
Total # of children admitted with under nutrition
19 21 31 14 11 25 10 13 14 12
Children admitted tat was under nourished
38% 40% 56% 27% 24% 22% 11% 15% 15% 9%
60
50
40
30
20
10
0
Percentage
26
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
“Most mothers who are able to bring their babies to the clinic for regular checks and follow our advice on a six-month exclusive breastfeeding regime or alternative feeding options should breastfeeding prove to be impossible have reported that their babies are growing well and thriving.” M.K. Hudla – Operations Manager
“To ensure our nutrition program is an ongoing process of educating, monitoring and supporting communities around nutritional health issues, Inhlwati Clinic has regular nutrition awareness campaigns. The most recent campaign was held in August 2014 and certainly contributed to people having more knowledge and being more aware of how they can look after their health through improving their eating habits where they can.” T.S. Ngubane – Nutritional Advisor
27
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
INHLWATHI CLINIC
SUMMARY OF QUALITY IMPROVEMENT PROJECTBackgroundQI training was conducted in June 2014. The training was attended by a professional nurse and the nutritional advisor. On 5 August 2014, the mentorship team conducted a baseline assessment at Inhlwati Clinic on the quality of NACS services provided.
The baseline assessment revealed that a draft QI plan was developed by the facility staff after the QI training in June. The facility seemed to have limited human resources available. The clinic is situated in a rural area and provides all PHC services, including obstetric care. The facility lacked most of the guidelines related to nutrition and knowledge on the content of guidelines was limited. There were no standard operating procedures for nutrition services. Nutrition supplies (supplementary nutrition products) and equipment (scales and measuring equipment) were available, except for equipment for the demonstration of preparing food safely. The scales were not calibrated and a measuring mat was available but not used. The storage area was clean and dry and nutrition supplements were stored correctly.
In relation to nutrition services, clients were weighed but not measured, except when seen by the nutrition advisor. The Road to Health booklets for children less than 5 years were incomplete. The growth charts were not plotted and there was no interpretation of results or recording of appropriate actions taken.
Health education was provided daily by the nutrition advisor as well as professional nurses. IEC materials were available at the facility and nutrition related pamphlets were provided to clients. There was poor recording of the education topics covered and the number of clients that received education. There was linkage with the community through the clinic committee and community health workers. There was no guide for the referral of malnourished clients within the facility and clients were only referred verbally. There was no M&E of the nutrition services and no supervision or mentorship.
After the NACS QI training in June, the two staff members who attended the training provided feedback to the rest of Inhlwati staff on what was learned
“The nutrition program is of great benefit to the clinic staff, as we are able to identify malnourished babies more directly by using MUAC and weight and height indicators. It also benefits our diagnosis and treatment of adult malnutrition through the use of body mass index indicators and providing advice on proper diet.” M.K. Hudla – Operations Manager
28
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
during the workshop. A QI Team was established and the team started doing MUAC for children and BMI for adults. The problem identified as the priority problem: Lack of identification and classification of children under 2 years who are undernourished by using the MUAC, height and weight for age.
Improvement aimThe initial improvement aim was: To improve the nutrition assessment and classification of children under 2 years from 0 to 90% by June 2015 through measuring weight/length for age and MUAC. When the team reached the point where monitoring and evaluation of the improvement package started, they experienced a challenge to collect the data to monitor the performance. No headcount was recorded for children less than 2 and many hours were spent trying to collect the appropriate data. When the team realized that it was not sustainable to monitor the specific target group, the improvement aim and indicators were changed to target children less than 5. The headcount for this target group was routinely collected.
The adjusted improvement aim: To increase the percentage of children less than five years nutritionally assessed (measuring weight, height, MUAC, and edema) and classified from 0% to 90% in Inhlwati Clinic by the end of June 2015.
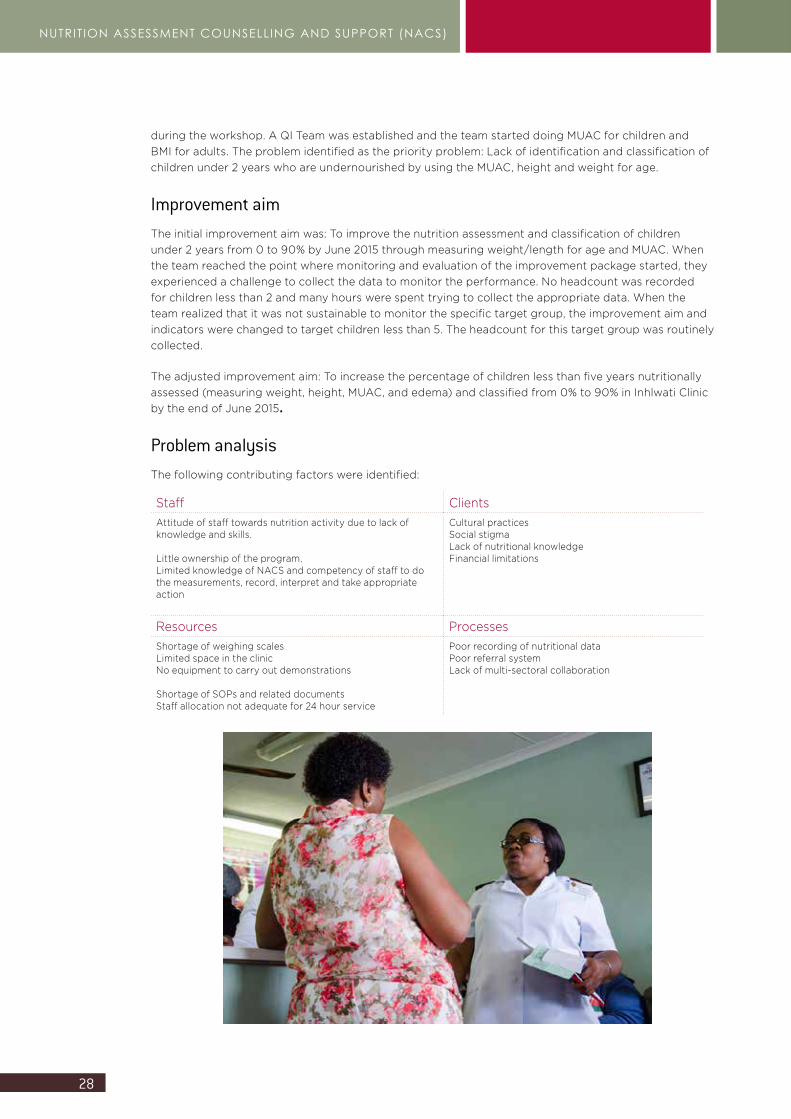
Problem analysisThe following contributing factors were identified:
Staff ClientsAttitude of staff towards nutrition activity due to lack of knowledge and skills. Little ownership of the program.Limited knowledge of NACS and competency of staff to do the measurements, record, interpret and take appropriate action
Cultural practicesSocial stigma Lack of nutritional knowledge Financial limitations
Resources ProcessesShortage of weighing scales Limited space in the clinic No equipment to carry out demonstrations Shortage of SOPs and related documentsStaff allocation not adequate for 24 hour service
Poor recording of nutritional dataPoor referral system Lack of multi-sectoral collaboration
29
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
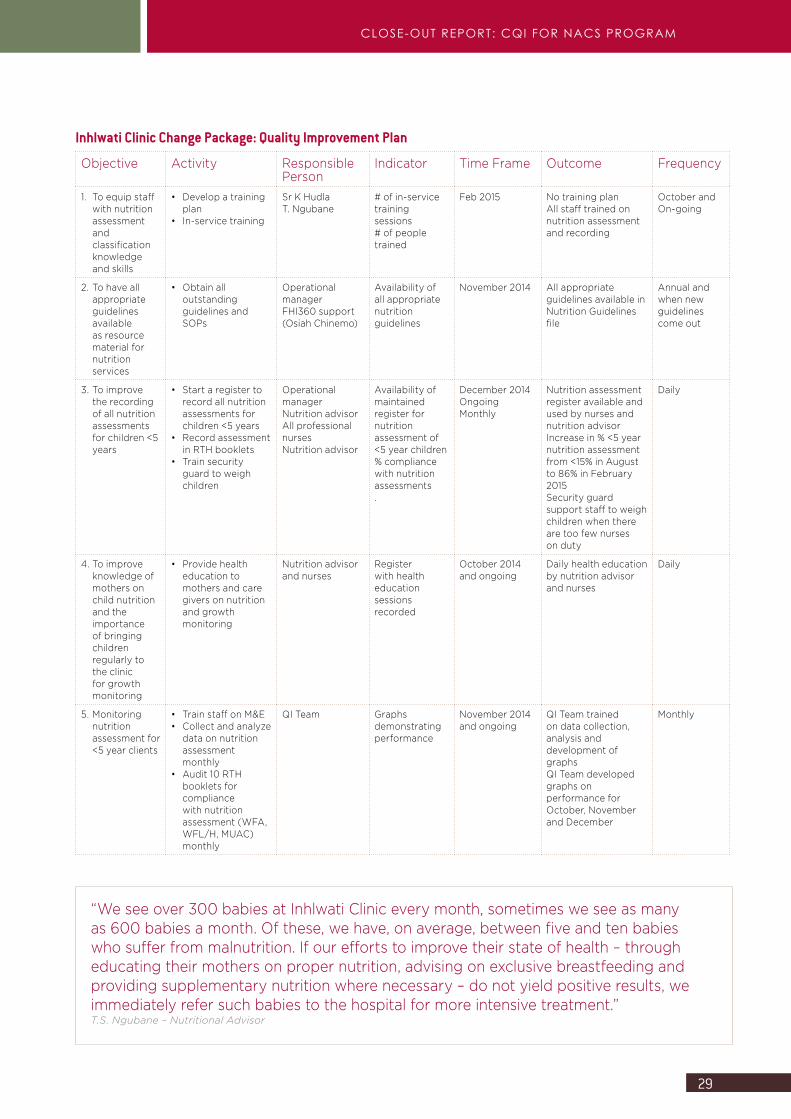
Inhlwati Clinic Change Package: Quality Improvement Plan
Objective Activity Responsible Person
Indicator Time Frame Outcome Frequency
1. To equip staff with nutrition assessment and classification knowledge and skills
• Develop a training plan
• In-service training
Sr K Hudla T. Ngubane
# of in-service training sessions# of people trained
Feb 2015 No training planAll staff trained on nutrition assessment and recording
October andOn-going
2. To have all appropriate guidelines available as resource material for nutrition services
• Obtain all outstanding guidelines and SOPs
Operational managerFHI360 support (Osiah Chinemo)
Availability of all appropriate nutrition guidelines
November 2014 All appropriate guidelines available in Nutrition Guidelines file
Annual and when new guidelines come out
3. To improve the recording of all nutrition assessments for children <5 years
• Start a register to record all nutrition assessments for children <5 years
• Record assessment in RTH booklets
• Train security guard to weigh children
Operational managerNutrition advisorAll professional nursesNutrition advisor
Availability of maintained register for nutrition assessment of <5 year children% compliance with nutrition assessments.
December 2014OngoingMonthly
Nutrition assessment register available and used by nurses and nutrition advisorIncrease in % <5 year nutrition assessment from <15% in August to 86% in February 2015Security guard support staff to weigh children when there are too few nurses on duty
Daily
4. To improve knowledge of mothers on child nutrition and the importance of bringing children regularly to the clinic for growth monitoring
• Provide health education to mothers and care givers on nutrition and growth monitoring
Nutrition advisor and nurses
Register with health education sessions recorded
October 2014 and ongoing
Daily health education by nutrition advisor and nurses
Daily
5. Monitoring nutrition assessment for <5 year clients
• Train staff on M&E• Collect and analyze
data on nutrition assessment monthly
• Audit 10 RTH booklets for compliance with nutrition assessment (WFA, WFL/H, MUAC) monthly
QI Team Graphs demonstrating performance
November 2014 and ongoing
QI Team trained on data collection, analysis and development of graphsQI Team developed graphs on performance for October, November and December
Monthly
“We see over 300 babies at Inhlwati Clinic every month, sometimes we see as many as 600 babies a month. Of these, we have, on average, between five and ten babies who suffer from malnutrition. If our efforts to improve their state of health – through educating their mothers on proper nutrition, advising on exclusive breastfeeding and providing supplementary nutrition where necessary – do not yield positive results, we immediately refer such babies to the hospital for more intensive treatment.” T.S. Ngubane – Nutritional Advisor
30
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)
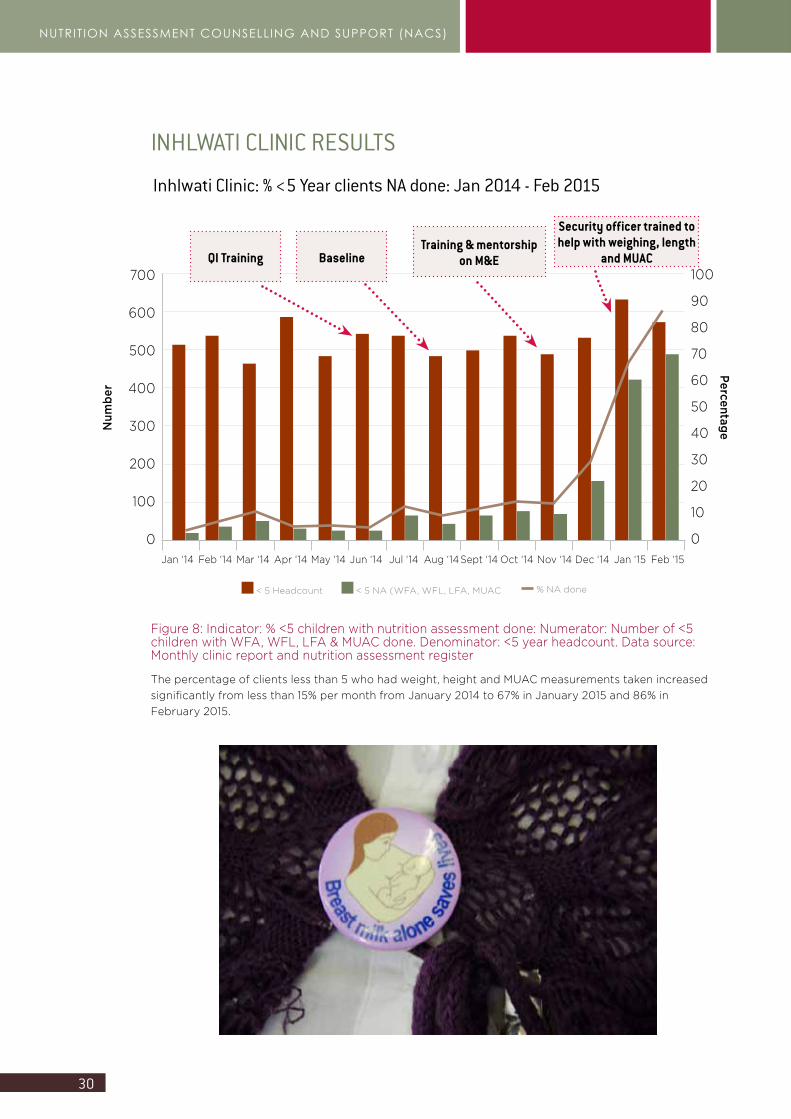
INHLWATI CLINIC RESULTS
Inhlwati Clinic: % <5 Year clients NA done: Jan 2014 - Feb 2015
700
600
500
400
300
200
100
0
Num
ber
Jan ‘14 Feb ‘14 Mar ‘14 Apr ‘14 May ‘14 Jun ‘14 Jul ‘14 Aug ‘14Sept ‘14 Oct ‘14 Nov ‘14 Dec ‘14 Jan ‘15 Feb ‘15
100
90
80
70
60
50
40
30
20
10
0
Percentage
BaselineTraining & mentorship
on M&E
Security officer trained to help with weighing, length
and MUACQI Training
< 5 Headcount < 5 NA (WFA, WFL, LFA, MUAC % NA done
Figure 8: Indicator: % <5 children with nutrition assessment done: Numerator: Number of <5 children with WFA, WFL, LFA & MUAC done. Denominator: <5 year headcount. Data source: Monthly clinic report and nutrition assessment register
The percentage of clients less than 5 who had weight, height and MUAC measurements taken increased significantly from less than 15% per month from January 2014 to 67% in January 2015 and 86% in February 2015.

31
CLOSE-OUT REPORT: CQI FOR NACS PROGRAM
URC staff trained all FHI360 staff members and two staff members from each of the five pilot facilities on basic QI principles and technology during the training workshop in June 2014. Mentorship was provided during six mentorship visits to each of the five facilities. During the mentorship visits, FHI360 staff participated fully in the process and supported the facilities with some of the improvement activities such as training of staff in nutrition assessment. Each facility worked through the quality improvement steps. Baseline assessments were conducted at the facilities to identify quality gaps and strengths in the nutrition services. Each facility established a QI Team and identified a priority problem to focus on for quality improvement in the nutrition services. Each facility analyzed the problem using a process analysis and a fishbone. Improvement aims were developed for each project. Change packages were developed, tested and implemented. Not all interventions were successful and some changes were adapted or discarded. Indicators were identified to monitor the progress of the QI projects. Each of the five facilities received mentorship on data collection, data analysis and interpretation and on the development of graphs to demonstrate the data and progress. Staff from each facility developed graphs from their project’s data. Quality improvement activities were documented in the NACS QI file. Every facility synthesized their QI project and created a storyboard with information on: QI team members, how the priority problem was identified, quality improvement aim, changes tested and implemented, results achieved, lessons learned and what they see as the next step. All the FHI360 staff demonstrated the knowledge and skills to apply QI principles and technology and to provide mentorship to facility staff on QI. FHI staff also demonstrated skills on data collection, analysis, interpretation and documentation of QI projects.
URC recommends that the pilot facilities receive support to sustain the QI work and participate in scaling NACS QI up to mobile services and nearby facilities that were not part of the pilot project. Additional support for strengthening of monitoring and evaluation systems is also recommended. Supervision of the nutrition services also still needs strengthening.
URC recognizes all the facility staff that participated in the QI work. The staff participated in spite of heavy workloads and disappointment when anticipated results were not achieved. They were willing to try doing things differently and were proud of their achievements.
URC also recognizes the support from uMkhanyakude district management for supporting the QI project. Ruth Maoela has accompanied the mentorship teams on most of the visits. DoH involvement is essential for ownership, sustainability and scaling up of the QI work.
Conclusion
32
NUTRIT ION ASSESSMENT COUNSELLING AND SUPPORT (NACS)

CLOSE-OUT REPORT: CQI FOR NACS PROGRAM






























