Embed Size (px)
Citation preview
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Ida Sim, MD, PhD
March 11, 2003
Division of General Internal Medicine, and Program in Biological and Medical Informatics
UCSF
Clinical Research Informatics/Organizational Aspects of Health
Information Technology Use
Copyright Ida Sim, 2003. All federal and state rights reserved for all original material presented in this course through any medium, including lecture or print.
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Field Trip
• Palo Alto Medical Foundation- a state of the art EMR (EpicCare)– the promise and the reality
• Today Mar. 11– 1:30 to 3:30pm
• Directions sent out by e-mail
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Outline
• Clinical research informatics– infrastructure for clinical research– systems for supporting clinical research
• Organizational aspects of IT use– examples of IT failures– reasons
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Evidence Adaptive CDSSs
• CDSS recommendations should be evidence-based– should keep up-to-date with research findings– update mechanism should be semi-automatic
• Health care computing infrastructure should be integrated – for clinical care and decision support– for clinical research
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Need For Informatics Infrastructure • “A nationwide effort is needed to build a technology-
based information infrastructure that would lead to the elimination of most handwritten clinical data within the next 10 years, the committee said. ...Without a national pledge to create and fund such a technological framework, progress to enhance quality of care will be painfully slow.” (IOM, Crossing the Quality Chasm, Mar 2001)
• IOM reports asks Congress to spend $1 billion on health informatics
• How do needs of clinical research and clinical care dovetail?
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
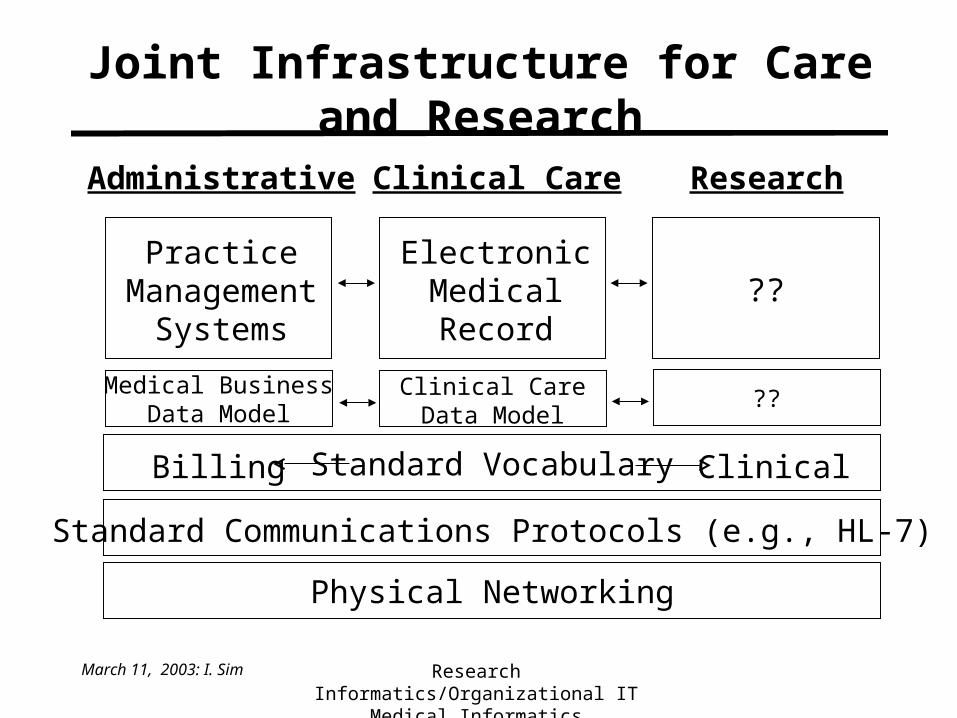
Joint Infrastructure for Care and Research
Administrative Clinical Care Research
ClinicalBilling
Physical Networking
Standard Communications Protocols (e.g., HL-7)
Standard Vocabulary
PracticeManagement
Systems
ElectronicMedicalRecord
??
Medical BusinessData Model
Clinical CareData Model
??
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
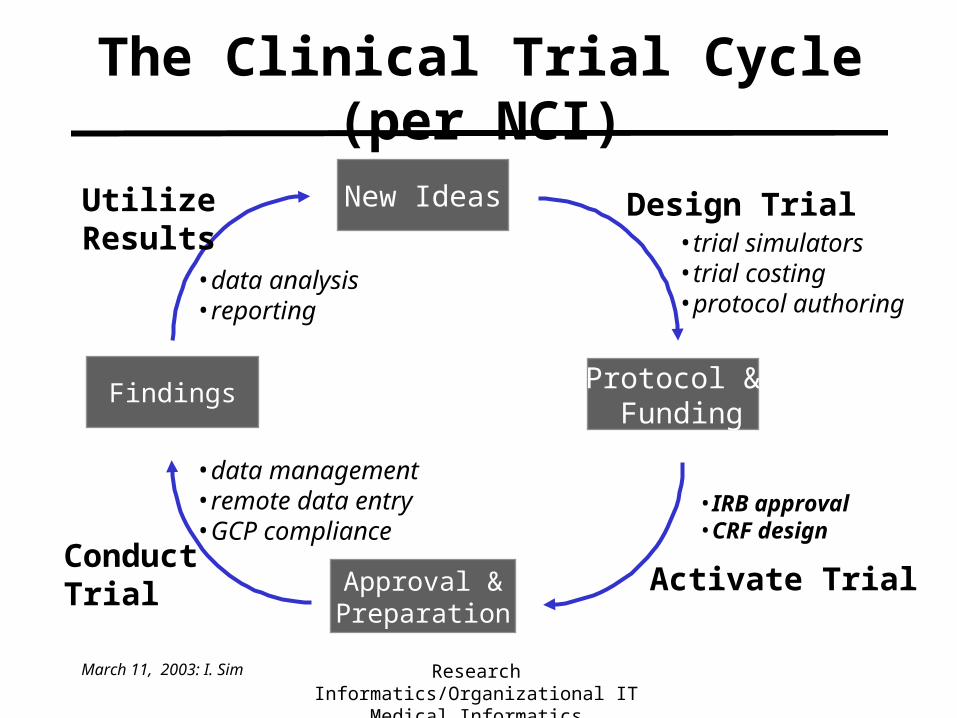
The Clinical Trial Cycle (per NCI)
New Ideas
Protocol & Funding
Findings
Approval &Preparation
Design Trial
Activate TrialConductTrial
UtilizeResults •trial simulators
•trial costing•protocol authoring
•IRB approval•CRF design
•data management•remote data entry•GCP compliance
•data analysis•reporting
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
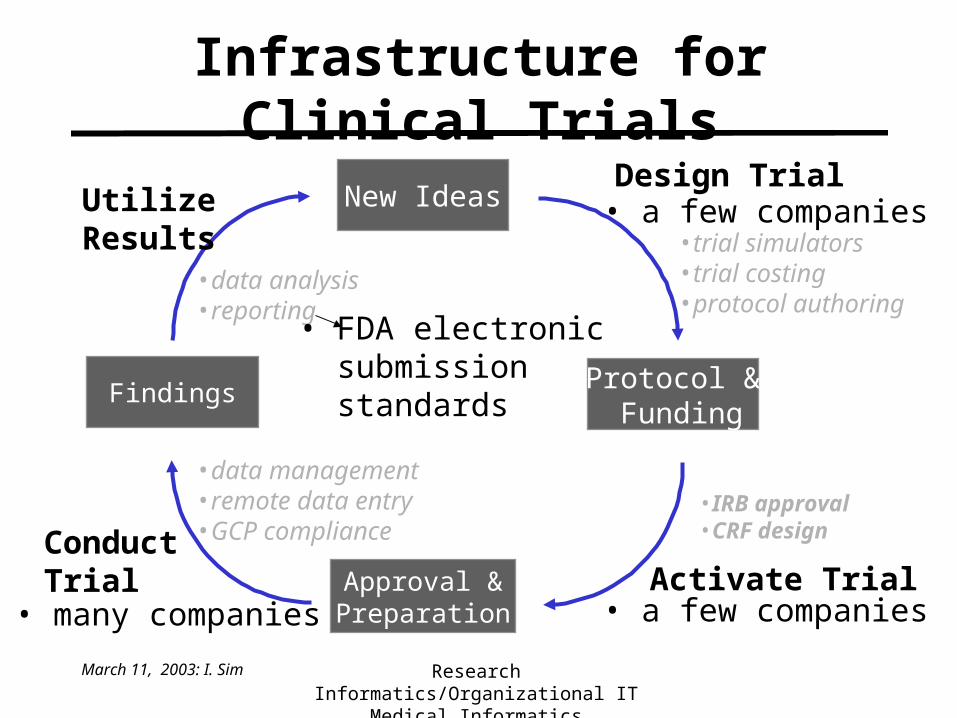
Infrastructure for Clinical Trials
New Ideas
Protocol & Funding
Findings
Approval &Preparation
Design Trial
Activate TrialConductTrial
UtilizeResults •trial simulators
•trial costing•protocol authoring
•IRB approval•CRF design
•data management•remote data entry•GCP compliance
•data analysis•reporting
• a few companies• many companies
• FDA electronic submission standards
• a few companies
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
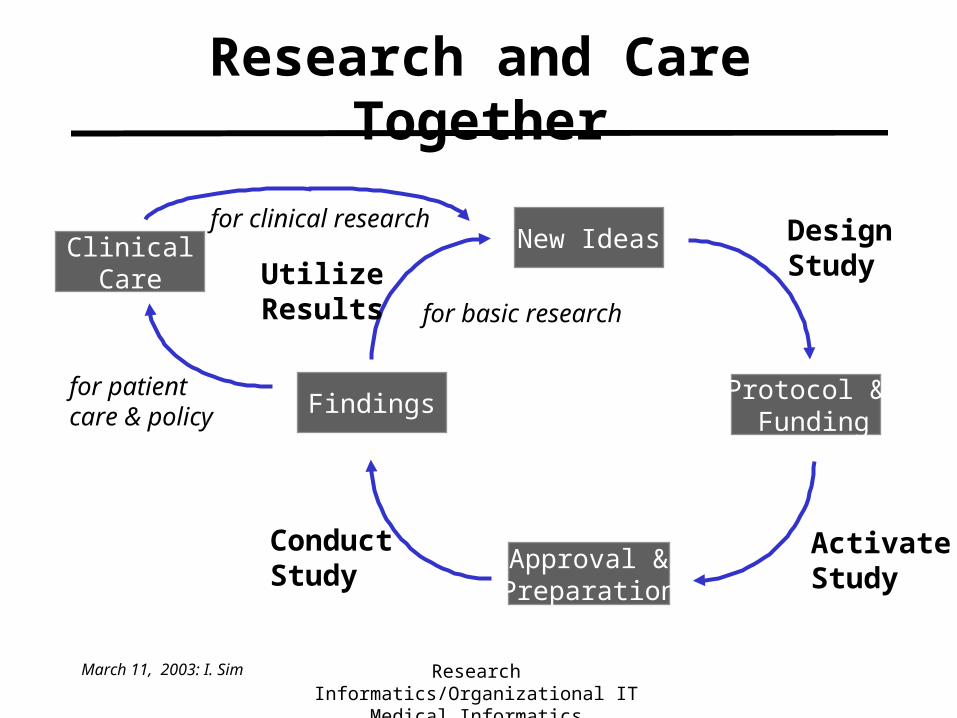
Research and Care Together
for patientcare & policy
ClinicalCare
for clinical researchNew Ideas
Protocol & Funding
Findings
Approval &Preparation
DesignStudy
ActivateStudy
ConductStudy
UtilizeResults for basic research
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
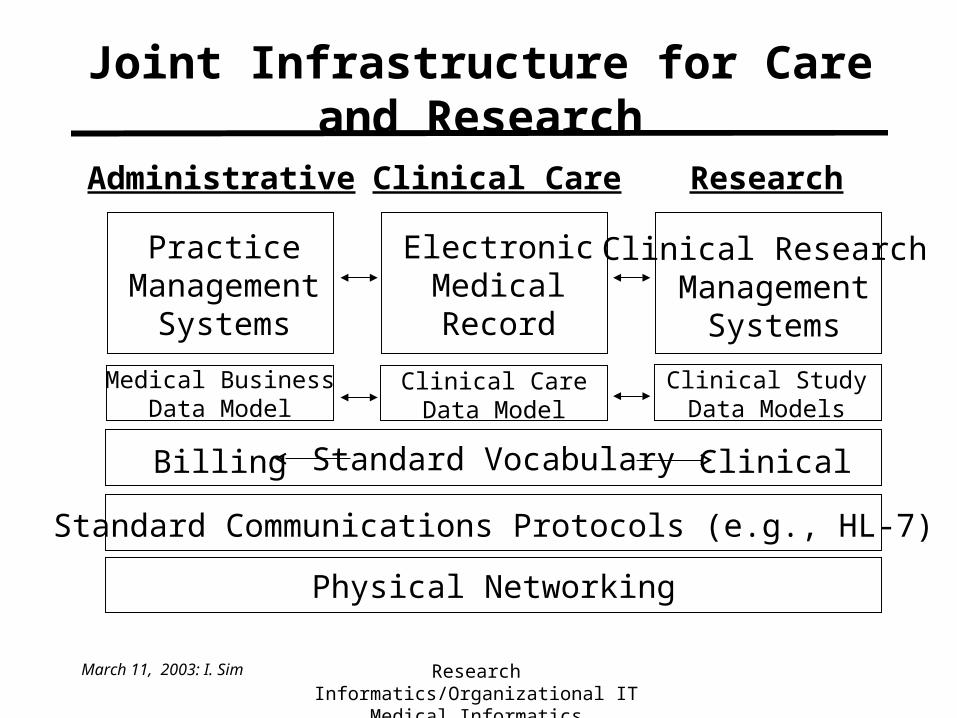
Joint Infrastructure for Care and Research
Administrative Clinical Care Research
ClinicalBilling
Physical Networking
Standard Communications Protocols (e.g., HL-7)
Standard Vocabulary
PracticeManagement
Systems
ElectronicMedicalRecord
Clinical Research Management
Systems
Medical BusinessData Model
Clinical CareData Model
Clinical StudyData Models
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Case: Clinical Research Informatics• You are planning a study on infant jaundice...• What relevant studies have been completed on this
topic?• What ongoing studies should you know about?• You’re interested in running your study over the
web as much as possible.– what types of study activities can be done over the
web?– how good is the technology for these activities?
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Relevant Trials: Completed
• Medline• Cochrane Controlled Trials Register
– ~328,000 records of controlled trials– manual logging of CCTs by hand searching journals– accessible from UCSF machines (IP address) only
• can set up proxy access
• metaRegister of Controlled Trials– 11,000 commercial and ongoing trials
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Relevant Trials: Ongoing
• Non-profit/government– www.clinicaltrials.gov
• 5700 trials, ~3000 open• NIH-supported and some commercial cancer and AIDS trials
– cancertrials.nci.nih.gov– www.actis.org
• AIDS Clinical Trials Information Service – www.trialscentral.org (from Cochrane people)
• pointers to hundreds of clinical trial registries, by disease
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Relevant Trials: Ongoing
• Commercial: mostly for patient recruitment– www.centerwatch.com– www.ClinicalTrialFinder.com– www.controlled-trials.com– www.clinicaltrials.com– etc., etc., etc.
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Case: Clinical Research Informatics• You are planning on a study on infant jaundice...• What relevant studies have been completed on this
topic?• What ongoing studies should you know about?• You’re interested in running your study over the
web as much as possible.– what types of study activities can be done over the
web?– how good is the technology for these activities?
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Clinical Study Tasks
• Project website• Subject recruitment• Eligibility determination• Protocol and forms distribution• Randomization• Data collection
– adverse events tracking
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Industry is the Innovator
• RCTs now a $3.6 billion business (C. Scott, 7/00)
– in 1988, 95% of RCTs conducted by academics– now, over 80% conducted by industry
• Ergo, much of the technology innovation in clinical research execution is going on in industry– Applied Clinical Trials software directory
• http://www.actmagazine.com/appliedclinicaltrials/data/articlestandard/appliedclinicaltrials/452002/37090/article.pdf
• What’s the global picture for research informatics technologies?
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Project Website
• Project website– GISSI website GISSI-x summaries, references
• http://wwwcardio.marionegri.it/trials.htm
– HERS main results revised tables from JAMA report• http://www.keeptrack.ucsf.edu/hers2/HERSfindat.htm
• Requirements– web server computer
• use a web hosting service (see http://www.cnet.com)• or have a web server program (e.g., Apache)
– pages of material• produce these using Word (save as HTML file)• or use a web editor (FrontPage, Dreamweaver)
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
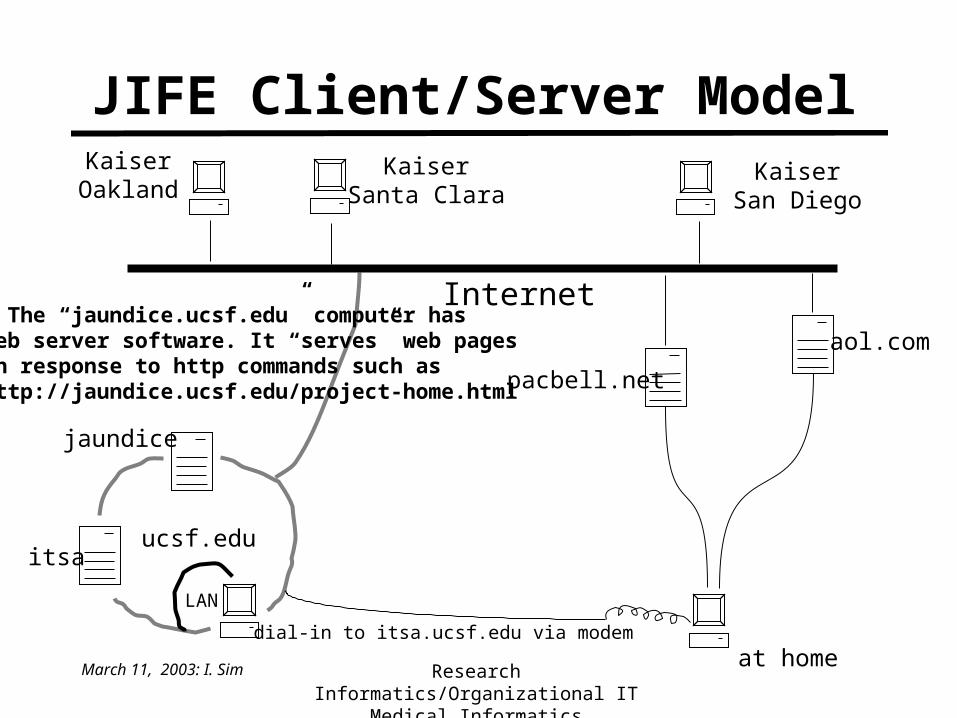
JIFE Client/Server Model
itsa
jaundice
ucsf.edu
KaiserOakland
KaiserSanta Clara
Internet
at homedial-in to itsa.ucsf.edu via modem
pacbell.net
aol.com
LAN
KaiserSan Diego
• The “jaundice.ucsf.edu” computer hasweb server software. It “serves” web pagesin response to http commands such ashttp://jaundice.ucsf.edu/project-home.html
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Project Website (cont.)
• Personnel– webmaster: handles the machine stuff– web designer: produces text & graphical content– database administrator/programmer: many databases
(e.g., FilemakerPro, Access, SQL) can now be exported to the web, but usually this involves moderate programming
• Status: easily doable today
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
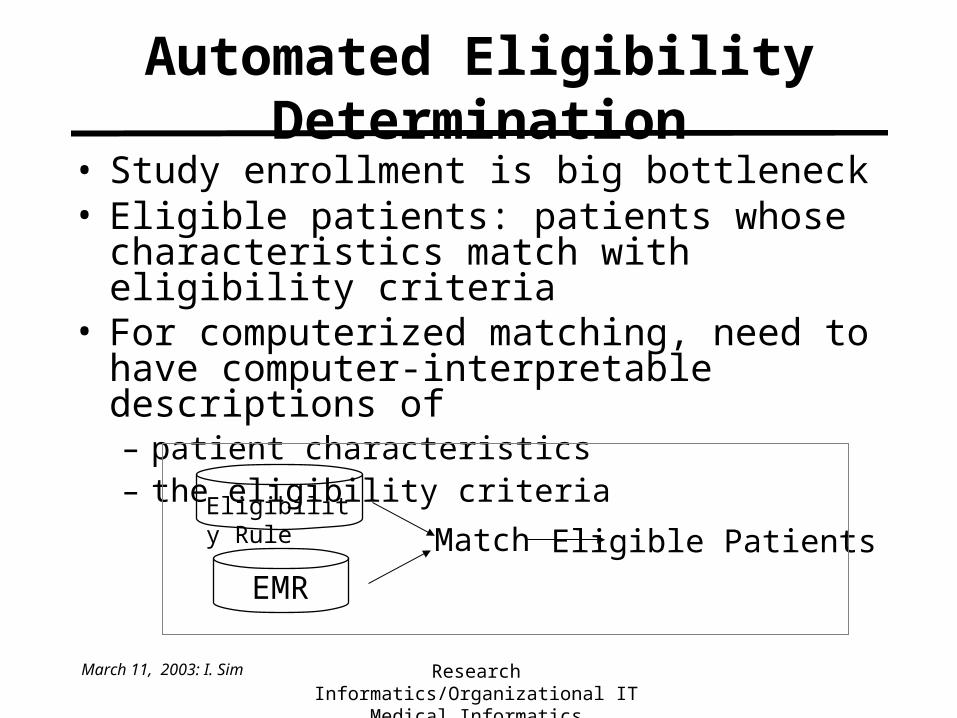
Automated Eligibility Determination
• Study enrollment is big bottleneck• Eligible patients: patients whose characteristics
match with eligibility criteria• For computerized matching, need to have computer-
interpretable descriptions of– patient characteristics– the eligibility criteria
Match Eligible Patients
EMR
Eligibility Rule
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
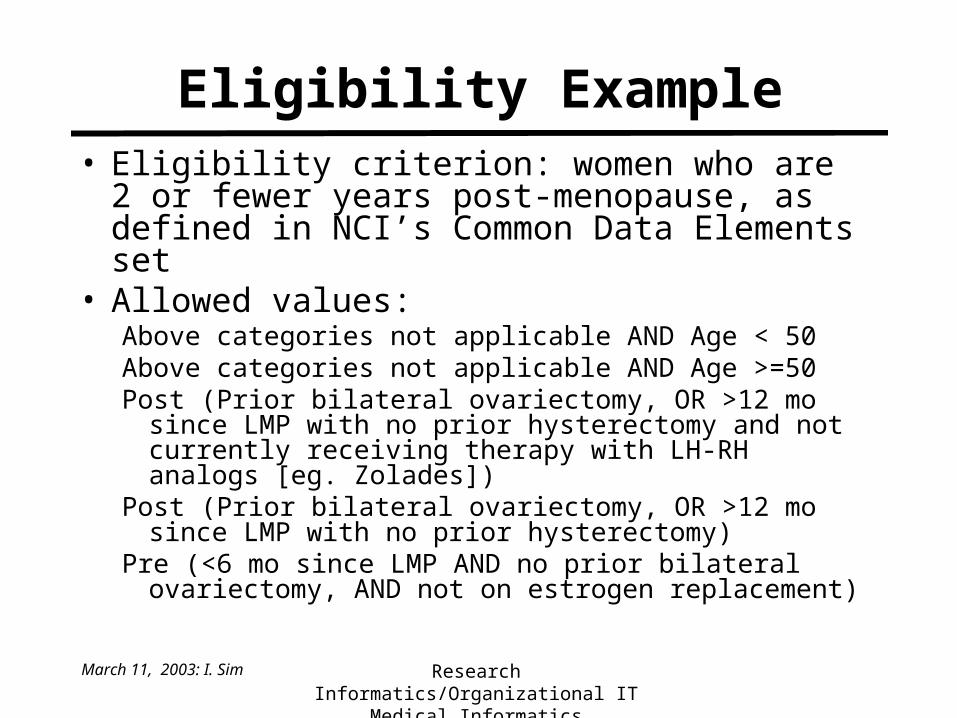
Eligibility Example• Eligibility criterion: women who are 2 or fewer
years post-menopause, as defined in NCI’s Common Data Elements set
• Allowed values:Above categories not applicable AND Age < 50Above categories not applicable AND Age >=50Post (Prior bilateral ovariectomy, OR >12 mo since LMP with
no prior hysterectomy and not currently receiving therapy with LH-RH analogs [eg. Zolades])
Post (Prior bilateral ovariectomy, OR >12 mo since LMP with no prior hysterectomy)
Pre (<6 mo since LMP AND no prior bilateral ovariectomy, AND not on estrogen replacement)
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
EMR Data Needed
• Gender• Age• Time since LMP, whether
– 6 or fewer months, or 12 or more months
• Past surgical history– bilateral ovariectomy and/or hysterectomy
• Therapy– LH-RH analogs, or– estrogen replacement
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Computer-Interpretable Eligibility Rule
• NCI working on common model for representing eligibility rules
• Logical rules– (Prior bilateral ovariectomy) OR (>12 mo since LMP AND no prior hysterectomy)– first order logic is the best representation model for this
• Temporal constraints – greater than 12 months since LMP...– representing time requires second-order logic
• Can do simple cases with database rules and triggers
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Promising, but...
• Richly detailed EMR not widely available or well integrated
• Coding of eligibility rules is difficult• At present, can only expect computer to suggest
potential subjects. EMR can– prompt MD in real-time to refer patient to study, or– periodically batch notify MD of eligible patients, or– send letter of solicitation to patients
• Similar problems bedevil automated identification of guideline eligibility
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Protocol and Forms Distribution• Allows for centralized forms management and storage
through a project website• If expecting users to download, print, fill out and fax form
back– need protocol and forms in electronic format (e.g.,Word or PDF)
• scan it using a scanner ($100-$4000)– makes an image of the page (e.g., .gif or .jpeg)
• optical character recognition (OCR) scanning– convert scanned text into an editable document (e.g., Word)
• Status: easily doable today
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
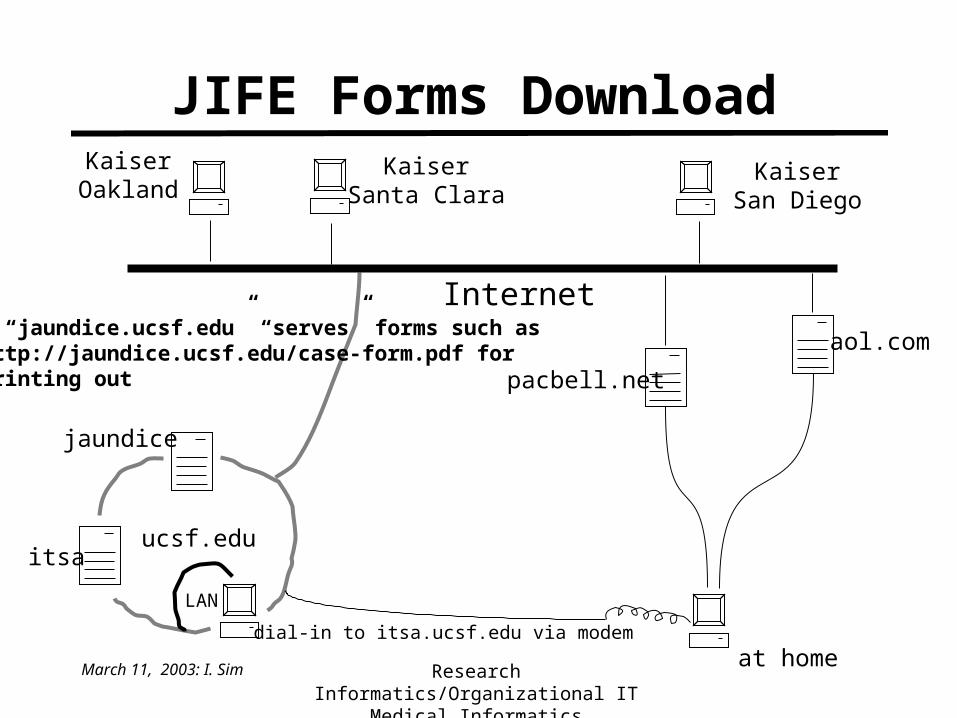
JIFE Forms Download
itsa
jaundice
ucsf.edu
KaiserOakland
KaiserSanta Clara
Internet
at homedial-in to itsa.ucsf.edu via modem
pacbell.net
aol.com
LAN
KaiserSan Diego
• “jaundice.ucsf.edu” “serves” forms such ashttp://jaundice.ucsf.edu/case-form.pdf for printing out
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Protocol and Forms Distribution
• If expecting users to enter data online over the web– need someone to design the forms and build them to be
served over the web• e.g., using Access Visual Basic
– need security mechanisms (e.g., user login)– need data validation checks built into forms entry– data forms must send data to a database
• Status: doable with some programming
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
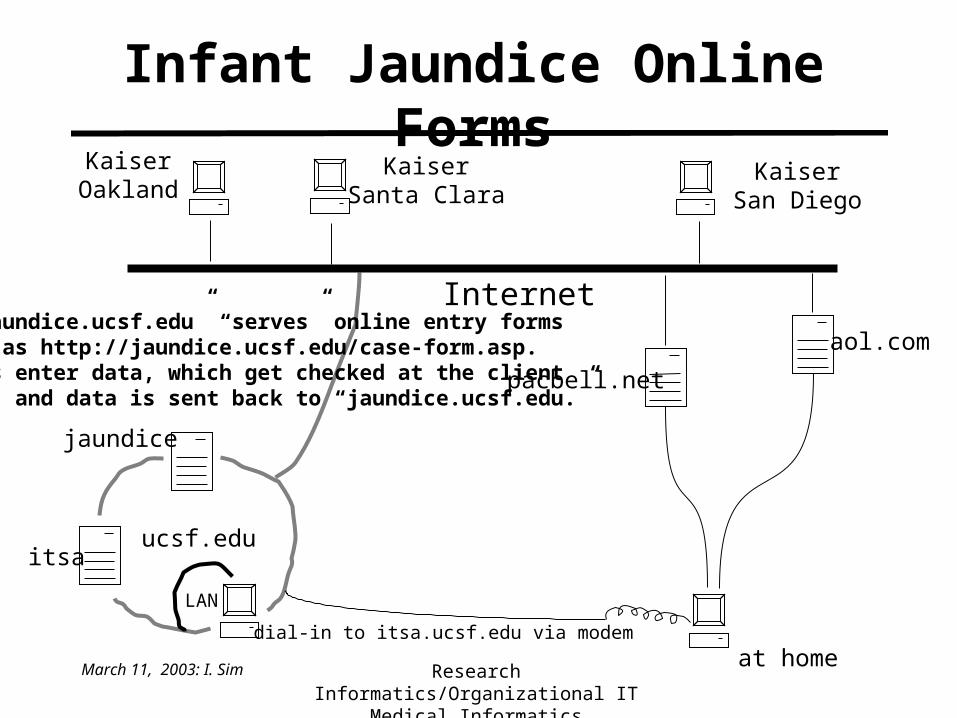
Infant Jaundice Online Forms
itsa
jaundice
ucsf.edu
KaiserOakland
KaiserSanta Clara
Internet
at homedial-in to itsa.ucsf.edu via modem
pacbell.net
aol.com
LAN
KaiserSan Diego
• “jaundice.ucsf.edu” “serves” online entry formssuch as http://jaundice.ucsf.edu/case-form.asp.Users enter data, which get checked at the clientside, and data is sent back to “jaundice.ucsf.edu.”
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
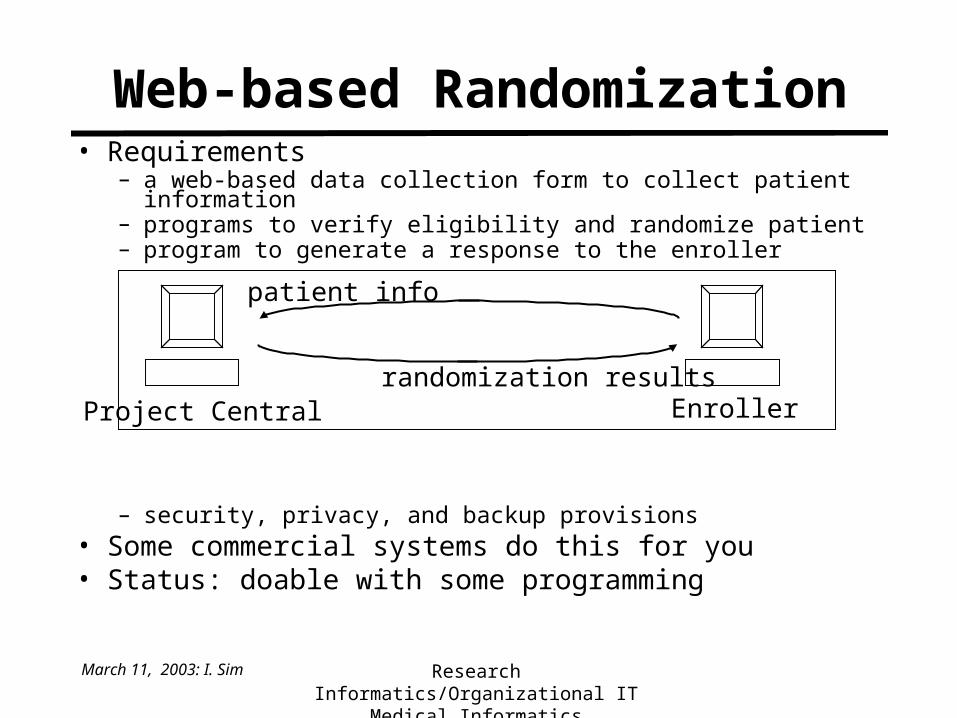
• Requirements– a web-based data collection form to collect patient information– programs to verify eligibility and randomize patient– program to generate a response to the enroller
– security, privacy, and backup provisions• Some commercial systems do this for you• Status: doable with some programming
Web-based Randomization
Project Central Enroller
patient info
randomization results
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Electronic Data Capture• Fax• Voice
– most systems about 95-99% accurate for restricted domains
– can speak normally, but may need to train computer to your voice
• Handheld Electronic– your favorite PDA and docking station for downloading
to a database (over the web)– wireless PDAs can’t be far from a receiver node
• radiofrequency: slow, prone to interference• infrared: requires line of sight between PDA and node
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Issues in Remote Data Capture
• Managing copies (local and central copies?)• Concurrent updates
– what if 2 people want to update same record?
• Merging data• Security and privacy• System downtime• System response time• Workflow issues
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Adverse Events (AE) Monitoring
• Dedicated systems for capturing this data for FDA requirements– built in checks for adhering to GCP (Good Clinical
Practice)
• Standard electronic data model for adverse events pending– will simplify adverse events data exchange
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Clinical Research Informatics Summary
• Project website– easily doable today
• Protocol and forms distribution– easily doable today
• Randomization– doable with some programming
• Data collection– fax– voice– electronic handheld– remote physiologic monitors
• Adverse events monitoring
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Teaching Points
• Clinical care informatics infrastructure should be integrated with clinical research infrastructure
• Many aspects of clinical research can be done electronically, but in fragmented fashion
• Industry very active in clinical research– business imperatives dominate infrastructure design

March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Outline
• Clinical research informatics– infrastructure for clinical research– systems for supporting clinical research
• Organizational aspects of IT use– examples of IT failures– reasons
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Learning Goals
• Develop a conceptual approach to analyzing and preventing IT implementation failures
• Appreciate importance of user-centered design, at all phases of an IT project
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Failures: U Virginia
• 700-bed hospital, 200 staff, 1200 resident MDs, 3600 RNs• 1981: consultants recommended financial and clinical medical
information system (MIS)– projected savings $26.3 million over 5 years– payback time less than 2 years
• 1985: accounting, then AdmissionDischargeTransfer – accounts receivable decreased from 100 to 60 days
• 88-91: clinical functions added sequentially– dietary and radiology orders; lab orders, results retrieval; pharmacy
pathways;
• 92: full deployment in and outpatient– all orders, all lab results, xray reports in MIS
(Acad Med 68:20-25)
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Failures: U Virginia (cont)
• Pros– pharmacy more efficient, fewer errors
• Cons– residents unplugged computers, refused to enter orders– 3 years behind schedule– 3x original cost estimate– Generated no reduction in staffing
• Governance– originally entirely by the Computing Services Group– final transition required special committee including of
Chairs of Medicine, Surgery, Peds
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Failures: HP, MGH, etc. etc
• Hewlett-Packard EMR at Palo Alto VA– clinicians did not use the system
• display would log off after only a few minutes• huge monitors placed between doctor and patient
• MGH – results reporting system in 1970s led to resistance in
early 1990s to new systems
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Classes of Failures• Total failure
– system never implemented or immediately abandoned
• Partial failure– major goals unattained, or significant undesirables
• Sustainability failure– lab ordering reduction systems
• Replication failure– “Bayesian” abdominal pain diagnosis system (DeDombal,
‘72)
• 8 study centers: diagnosis improved from 46% to 65% • laparotomy rate and appendiceal perforations fell 50%• not replicated elsewhere
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Why Health IT (HIT) Fails
• Is it a shortcoming of technology?– didn’t capture the health problem correctly? – didn’t have enough info or was too slow?– used the wrong reasoning method? – insufficient diagnostic/modeling/ etc. performance?
• Was it poor interface design?• Was it lack of user training?• If a system fails, what can be learned to prevent
another failure?
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
General IT Management Challenges
• HIT failures are instances of general IT failures– California DMV spent $45m from 87-93 on aborted
electronic license system– IRS, INS, FDA, …$165m on CONFIRM car rental
and hotel reservation system (AA, Marriott, Budget, Hilton
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
What’s Common to IT Projects?
• Technology driven– a hammer looking for a problem
• e.g. “Wow I have a Palm Pilot! What can I do with this?”
• Problem driven– a problem looking for a solution
Initial ProblematicState of the World
ImprovedState of the World
Solution involving IT
InaccurateHeart Attack Dx
ImprovedHeart Attack Dx
Baxt’s Neural Network
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
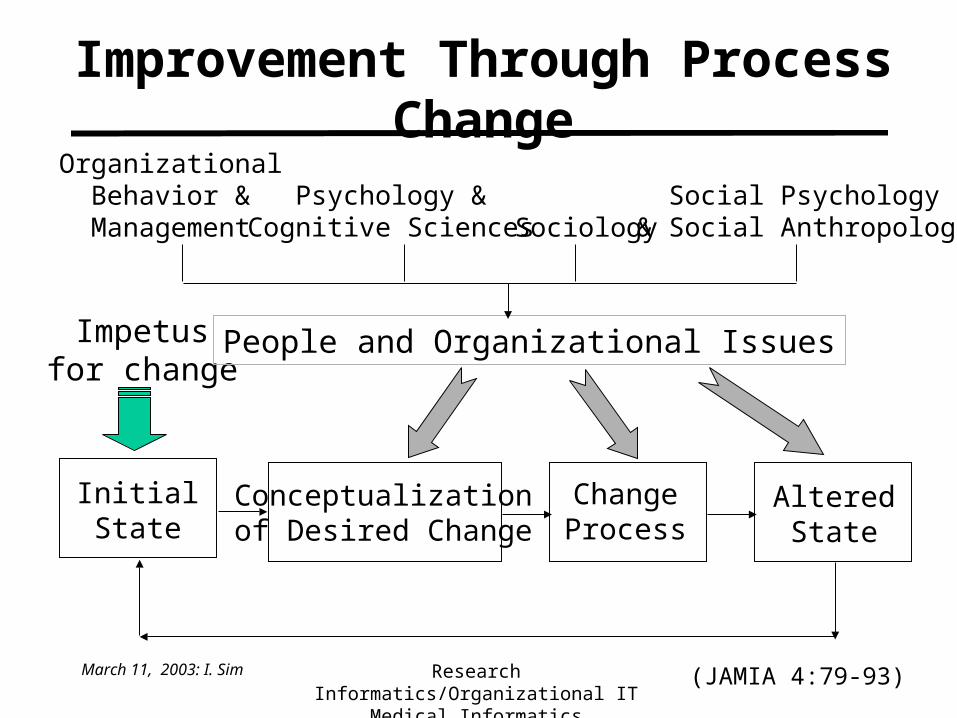
Improvement Through Process Change
InitialState
Conceptualizationof Desired Change
ChangeProcess
AlteredState
Impetusfor change
(JAMIA 4:79-93)
OrganizationalBehavior &
ManagementPsychology &
Cognitive Sciences SociologySocial Psychology
& Social Anthropology
People and Organizational Issues
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Conception–Reality Gaps• Conception–reality gaps often arise from mismatches
between formal and behavorial reality– formal: what’s official– behavorial: the real skinny
• Types of Gaps– technical, managerial, medical
• Dimensions of Gaps– Information– Technology– Processes– Objectives and Values– Staffing and Skills– Management and Structures– Other resources: money and time
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Technical Rationality Gaps• aka the Org Chart Illusion• U Virginia order entry system allowed only MDs
to write electronic orders – subinterns (4th year med students) could not enter
orders for later co-signing– in non-computer version, subI writes orders and
resident later co-signs it • care is delivered, subI learns autonomy and decision-making• saves time for resident• returns time saved in the form of teaching (usually)
• Similar gaps for nursing care plans, worker time sheets, etc.
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Managerial Rationality Gap• Managerial perspective
– increases in pharmacy expenses are the biggest component of escalating health care costs
– reduce drug costs (eg proton pump inhibitors) by negotiating specific price reductions (e.g., for lansoprazole)
– switch all patients to cheapest drug of class unless physician objects (from omep- to lanzoprazole)
• MD perspective– MD knows dosing, typical response, side effect profile of
omeprazole; managers provide no support for process change
• Patient perspective– patient is used to omeprazole, it works fine without side
effects, he doesn’t want to deal with a new medication
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
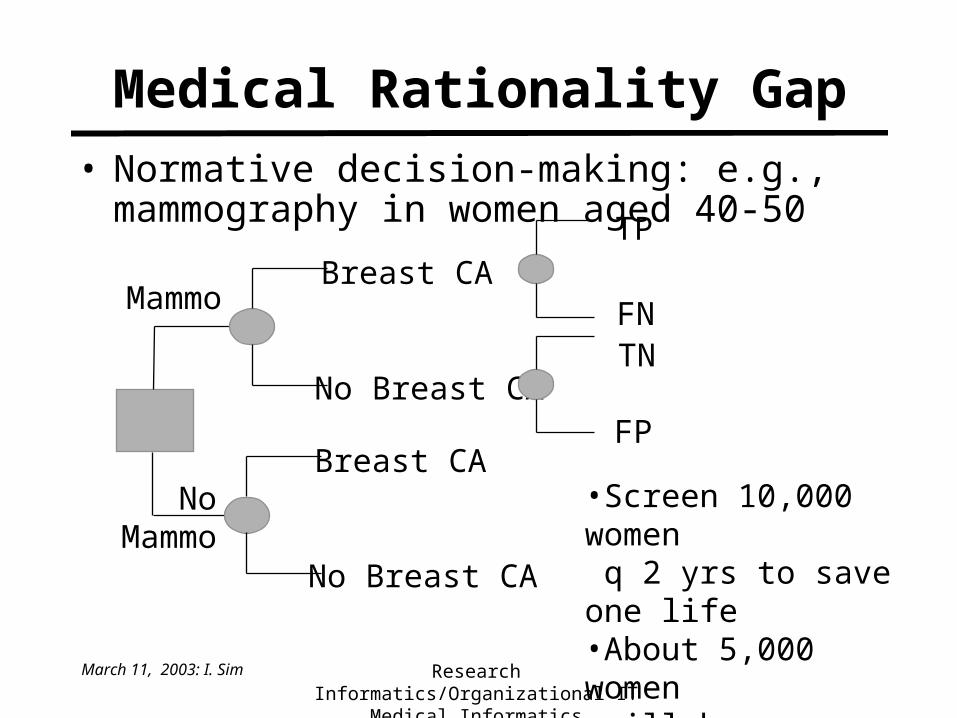
Medical Rationality Gap• Normative decision-making: e.g., mammography
in women aged 40-50
NoMammo
MammoBreast CA
No Breast CA
Breast CA
No Breast CA
FP
TNFN
TP
•Screen 10,000 women q 2 yrs to save one life•About 5,000 women will have a false positive
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Conception–Reality Gaps• Conception–reality gaps often arise from mismatches
between formal and behavorial reality– formal: what’s official– behavorial: the real skinny
• Types of Gaps– technical, managerial, medical
• Dimensions of Gaps– Information– Technology– Processes– Objectives and Values– Staffing and Skills– Management and Structures– Other resources: money and time
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Example CDSS• Diabetic retinopathy leads to many cases of
preventable blindness• Referral and followup rates for diab. ret. low• Tele-opthalmology for routine opthal screening
– primary care doctors have tele-eye stations (EyePACS) in their offices
– take digital images of patient retina– transmit images to opthalmologist for decision
on need for referral
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
ITP...
• Information – is system satisfying a true need of intended users?
• are retinal diseases not picked up? preventable blindness?
• Technology– is technical infrastructure available and realistic?
• broadband access to physician offices for teleopthalmology?
• Process– is new workflow significantly different from old?
• how to integrate into primary care visit workflow?
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
...OSMO
• Objectives and values– is it role/responsibility of internist to screen for eye
diseases?
• Staffing and skills– internist office personnel will run the tele-eye station?
• Management and structure– who owns the tele-eye station? who owns the retinal
images?
• Other resources– opthalmologists lose the business of routine eye exams
March 11, 2003: I. Sim Research Informatics/Organizational ITMedical Informatics
Summary of Org Change
• IT projects often fail (spectacularly)• Important source of failure is “people and
organizational issues”• Technology is a just a tool for process change
– can be positive and/or negative
• Better to consider people and organizational pitfalls during design and implementation– be careful if your research protocol involves new IT