Embed Size (px)
Citation preview

Manuscript: Explicit Constructivism: a missing link in ineffective lectures?Author: E.S.Prakash Supplement 1: Typical Lecture
This is an open access article distributed under the terms of the Creative Commons Attribution License http://creativecommons.org/licenses/by-nc-sa/3.0/
Note - Copyrighted images have been removed and replaced with a URL link to those images.

Chemical and neural regulation of respiration
E.S.Prakash, School of Medicine, AIMST University, Malaysia
E-mail: [email protected]

How much do we already know?
Just write the answers with the question number on a sheet of paper
1. At sea level, barometric pressure is: mmHg
2. Barometric pressure is the same as atmospheric pressure. T/F
3. In the upright position, ventilation-perfusion ratio is highest in the upper lung zones. T/F
4. The maximum volume of air that you can expel after a maximal inspiration is called:
5. The amount of air that remains in the lungs after a tidal expiration is called:

6. If you breathe 500 ml per breath 12 times a minute and your dead space is 150 ml, then, what is the amount of fresh gas supplied to your alveoli per minute?

Organization of content in these lectures: Neural control of breathing Neural control systems: functional organization Chemoreceptors: functional organization Classification of chemoreceptors Ventilatory responses:
to changes in acid-base balance To CO2 excess To oxygen lack Interaction of hypoxia and CO2

Content outline continued:
Nonchemical influences on respiration Responses mediated by airway receptors Responses mediated by receptors in the lung
parenchyma Coughing & sneezing
Regulation of respiration during sleep Abnormal respiratory patterns

Neural control of breathing
There are 2 systems: One for voluntary control One for spontaneous breathing

System for voluntary control of breathing:
Regulator neurons located in cerebral cortex When does this system work? When we control our breathing voluntarily Example: when you hold your breath Example: when you hyperventilate Pathway: From cerebral cortex to motor neurons
in the spinal cord which supply muscles of respiration (diaphragm & intercostal muscles)

System for spontaneous control of breathing:
Breathing is mostly spontaneous Breathing is rhythmic (rate as well as depth) We are not aware that we are breathing Location of respiratory center: medulla Please see schematic on next slide

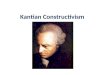
Mechanism of spontaneous breathing
Pons
Medulla
Pre-Botzinger complex; pre-BOTC (Pacemaker)
I neurons
Phrenic neuronsDiaphragm & intercostal muscles
Medullary chemoreceptors
Afferents from carotid bodies terminate here
Spinal cord

Component Details
Central chemoreceptor neurons (sensory)
Project to Pre-Botzinger complex of neurons
Pre-BOTC Discharge spontaneously; pacemaker neurons for breathing (like SA node in heart); entrained by input from chemoreceptors
I neurons Fire during inspiration; thus the name; project to lower motor neurons (e.g. phrenic n.) that drive muscles of inspiration

Feedback to the respiratory center from lungs: During inspiration,
lungs expand, and lung parenchyma is stretched; stretch receptors are present here; these are activated and convey information to the
brain via sensory branches of vagus nerve

Role of pons in respiration:
There is an area called pneumotaxic center in the pons;
If this area is damaged, then, depth of inspiration is increased (see next slide)
So, this center may serve to switch breathing from inspiration to expiration
This switch works to inhibit I neurons during expiration

Effect of vagotomy on breathing rate and depth; note the increase in depth
After vagotomy
Normal

Effect of damage to the pneumotaxic center in vagotomized animals:
apneusis
normal
After vagotomy

Functional organization of chemoreceptors:
A rise in PCO2, a fall in pH or PO2 of arterial blood increases respiratory neuron activity in the medulla.
Stimulus: a change in blood chemistry … Sensed by: receptors called chemoreceptors Response: change in minute ventilation

Functional organization of chemoreceptors (contd.)
Location of chemoreceptors: Central chemoreceptors (in
medulla); also called medullary chemoreceptors
Arterial chemoreceptors (in carotid & aortic bodies); sometimes called peripheral chemoreceptors

Functional organization of chemoreceptors (contd.) Innervation of peripheral (systemic arterial
chemoreceptors); Figure at Link: http://www.medicine.mcgill.ca/physio/resp-web/Figures/Figtt20.jpg
Note carotid body is supplied by branch of IX nerve and aortic bodies are supplied by branch of X nerve.

Some facts about systemic arterial chemoreceptors: There are 2 types of cells in the carotid body; Type I glomus cells contain oxygen sensitive K
channels (these are the chemoreceptors) Type II cells are supporting cells They have a very high blood flow In carotid bodies, blood flow rate: 2000 ml/100 g
tissue/min For example, the brain gets 50 ml/100 g/min

Stimuli that activate peripheral chemoreceptors: 1. Low PaO2 (hypoxemia)
2. Drop in arterial pH (acidosis)
3. Rise in PaCO2 (hypercapnia)
4. Low blood flow through the receptors; i.e., when cardiac output and BP are low
Note: these receptors are very sensitive to drop in PaO2 (hypoxemia) compared to rise in PaCO2 (hypercapnia)

So what are the normal values of each?
Arterial Blood Gases & pH Normal range
Arterial pH 7.35 – 7.45
Arterial PO2 81 – 100 mm Hg
Arterial PCO2 35 – 45 mm Hg

Central chemoreceptors(medullary chemoreceptors)
Location: brain stem, ventral surface of medullahttp://www.lib.mcg.edu/edu/eshuphysio/program/section4/4ch6/4ch6img/page21.jpg
They are located near I neurons They project to respiratory neurons Central chemoreceptors and respiratory neurons are
distinct They are mainly sensitive to changes in PaCO2
A rise in PaCO2 effectively stimulates central chemoreceptors

A rise in PaCO2 lowers CSF pH which is sensed by
medullary chemoreceptorsCO2 crosses the blood brain barrier (BBB)
CO2
brain ISF
CO2 + H2O H2CO3
Carbonic anhydrase
blood
H+ + HCO3
Drop in CSF pH

Central chemoreceptor neurons monitor the H+ ion concentration of brain ISF;
Greater the PaCO2, > the minute ventilation; If you lower PaCO2, minute ventilation is lowered

Effect of addition of metabolic acid (e.g., lactic acid, on ventilation) Example: lactic acidosis (metabolic acidosis) Arterial pH is low (< 7.35); Breathing is rapid and deep (Kussmaul’s
respiration) and CO2 is blown off This response is mediated by carotid bodies
(peripheral chemoreceptors) and is lost if they are removed.

Effect of a rise in blood pH on minute ventilation Example: metabolic alkalosis due to vomiting;
i.e., loss of HCl; Arterial pH is high (> 7.45) Respiration is slowed; i.e., decrease in minute
ventilation) As a result PaCO2 gradually rises

What happens if more CO2 is produced as a result of
metabolism?More CO2 in blood as a result of ↑metabolism
Transient rise in PaCO2
Fall in CSF pH
Respiration is stimulated effectively
Steady state PaCO2 is normal

Ventilatory response to CO2 lack or excess
Alveolar PCO2 (mm Hg)
Minute ventilation (l/min)
0
100
200
0 40 50 75 100

Ventilatory response to oxygen lack:
PO2 (mm Hg)
Minute ventilation (l/min)
0 25 50 75 100
0
100
200

Ventilatory response to hypoxia, hypercapnia, severe exercise and maximal voluntary
ventilation (MVV) compared
Alveolar PO2 or PCO2 (mm Hg)
Minute ventilation (l/min)
0
100
200
0 50 100
MVV: 125-175 l/min
Max. ventilation during exercise
Response to hypercapnia
Response to hypoxia

Comments:
Normally, minute ventilation is about 5 l/min MVV = 125-175 l/min (higher in males cf. females)
Thus, there is a great ventilatory reserve; But MVV can be sustained only for a short time Hypoxia and hypercapnia alone are not as potent
as severe exercise in stimulating ventilation So, other factors also drive ventilation during
exercise.

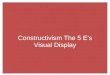
Interaction of ventilatory responses to CO2 and O2 (all partial
pressures in mm Hg)
40 50PACO2
Ventilation (l/min)
PAO2 = 40PAO2 = 55
PAO2 = 100
0
25
50
75
100

Conclusion: Conclusion: Hypoxia makes an individual more
sensitive to CO2 excess

Ventilation at high altitudes: Barometric (atmospheric) pressure is lower; When PaO2 is < 60 mm Hg, min. ventilation ↑ What happens to PaCO2? It is lowered as a result of hyperventilation What happens to pH of arterial blood? pH increases slightly say from 7.4 to 7.45 Arterial blood gases: Hypoxemia (low PaO2);
hypocapnia (PaCO2 < 35 mm Hg); respiratory alkalosis (pH > 7.45 because of hypocapnia)

Some working definitions for you:
Normocapnia: PaCO2 between 35 and 45 mm Hg Hypocapnia: PaCO2 < 35 mm Hg Hypercapnia: PaCO2 > 45 mm Hg Hypoxemia: PaO2 < 80 mm Hg Note: significant activation of carotid bodies
occurs only when PaO2 < 60 mm Hg

Effects of breath holding:
Respiration can be voluntarily inhibited for some time
Eventually, voluntary control is overridden (breaking point)
What is breaking due to? Rise in PaCO2 (acute hypercapnia) Fall in PaO2
Individuals can hold their breath longer after removal of carotid bodies;
Psychologic factors also contribute

Effects of hyperventilation:
Overbreathing to exhaustion; Eventually there is a “breaking point” Note a period of apnea following
hyperventilation; What is breaking here due to? CO2 lack
Overbreathing
apnea

Effects of chronic hypercapnia: When does chronic hypercapnia occur?
What is the basic cause of chronic hypercapnia? Failure to eliminate CO2; (respiratory failure) Reason: reduction in alveolar ventilation Note:
acute hypercapnia stimulates breathing chronic hypercapnia depresses the respiratory center

Nonchemical influences on respiration:Stimulus Response Name of
reflexReceptor
Excessive lung inflation
Inhibition of inflation; lung
deflation
Hering Breuer
inflation reflex
Vagal afferents
from airways
Excessive lung deflation
Inhibition of deflation; lung
inflation
Hering Breuer
deflation reflex
Vagal afferents
from airways
Lung inflation
Further inflation
Head’s paradoxical
reflex
?

Nonchemical influences on respiration (contd.):Stimulus Response Name of
reflexReceptor
Lung hyperinflation;
increase in pulmonary
interstitial fluid pressure; or intravenous injection of capsaicin
Apnea followed by tachypnea;
bradycardia; hypotension; skeletal
muscle weakness
J reflex Juxtacapillary receptors (C vagal fiber endings)
Injection of histamine
Cough, bronchoconstriction,
mucus secretion
Cough reflex
Irritant receptor;
among airway epithelial cells

Mechanism and significance of cough:
Deep inspiration
Forced expiration against a closed glottis
Intrathoracic pressure increases to 100 mm Hg or more
Glottis opened by explosive outflow of air
Airways are cleared of irritants

Ondine’s curse:
Spontaneous control of breathing is disrupted; Voluntary control is intact; One could stay alive only by remembering to
breathe; Clinical analog:
bulbar poliomyelitis affecting respiratory neurons in the brain stem;
disease processes compressing the medulla

Regulation of respiration during sleep:
Respiration is less rigorously controlled during sleep;
Brief periods of apnea occur even in normal people;
Ventilatory response to hypoxia varies; Sensitivity of brain stem mechanisms reduced?

Abnormal breathing patterns:
Periodic breathing(Cheyne-Stokes respiration)
Normal

Cheyne-Stokes respiration: Periods of apnea punctuated by periods of
hyperpnea It occurs in:
congestive heart failure brain stem disease affecting respiratory centers
Mechanisms postulated to explain this:
1. Prolonged lung-to-brain circulation time
2. Changes in sensitivity of medullary respiratory neurons

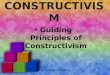
Activity: Hyperventilate to exhaustion Then, note your pattern of breathing Explain your observations
Periodic breathing
normal
hyperventilation
Following hyperventilation

Outline of the explanation: Hyperventilation eliminates CO2; Apnea is due to lack of CO2
During apnea, PaO2 falls & stimulates breathing Few breaths eliminate hypoxia Now there is no stimulus for breathing So there is apnea again Normal breathing resumes only when PaCO2 is
40 mm Hg Conclusion: normal breathing pattern is entrained
by PaCO2 not PaO2

Some items for self-study:
How is breathing regulated during exercise? What is the mechanism of hiccups? What is the mechanism of yawning? What is the mechanism of sneezing? What happens when you sigh?

POST-TEST

You should also be able to answer these questions:
1. Describe with the help of schematic diagram, the neural mechanism of spontaneous breathing
2. Describe with the help of schematic diagram, the neural mechanism of voluntary control of respiration
3. Describe with the help of schematic diagram, the role of systemic arterial chemoreceptors in the regulation of alveolar ventilation

4. Describe with the help of schematic diagrams the functional organization and functions of medullary chemoreceptors.
5. How does CO2 stimulate breathing?
6. What is the relationship between PaCO2 and minute ventilation?
7. Describe the mechanism responsible for periodic breathing following voluntary hyperventilation

8. Explain the factors that affect breath holding time.
9. Briefly explain the effect of damage to the pneumotaxic center on the pattern of breathing
10. Briefly explain the effect of vagotomy on the pattern of breathing in experimental animals.

11. What is the difference between the effect of acute hypercapnia and chronic hypercapnia on minute ventilation?
12. What is Kussmaul’s respiration? When does it occur? What is the mechanism involved?
13. What is periodic breathing? When does it occur? What is Cheyne-Stokes respiration?
14. What are the Hering Breuer reflexes?
15. What is Head’s paradoxical reflex?

Required Reading:
Chapter 36. Regulation of respiration. Ganong WF. Review of Medical Physiology, Mc Graw Hill Co, 2005