Embed Size (px)
Citation preview

14.5.2020
Manuscript
Dynamic fluctuations of emotional states in adolescents with delayed sleep phase—a longitudinal
network modeling approach
Marko Elovainio, PhD 1,2
Liisa Kuula, PhD 1
Risto Halonen, MPsyc 1
Anu-Katriina Pesonen, PhD 1
1 SleepWell Research Program Unit, Department of Psychology and Logopedics, Faculty of
Medicine, University of Helsinki, Finland 2 National Institute for Health and Welfare, Finland
Correspondence: Marko Elovainio, University of Helsinki, P.O. Box 9, 00014, Helsinki, Finland
Phone: +358 50 3020621, email: [email protected]
Word count for abstract / main text: / 250 / 3531
Number of tables and figures: 1 Table / 3 figures
Funding: Academy of Finland

ABSTRACT
Background: Very late sleep rhythms are risks for social adjustment problems in adolescence.
Using ecological momentary assessment data, we quantified and visualized temporal and
contemporaneous within-persons dynamical relations of sleepiness and emotions in adolescents
with and without late sleep rhythms.
Methods: We analyzed a temporal network via multilevel vector autoregression (mlVAR)
modeling and a contemporaneous network through the partial associations between the residuals of
temporal and the between-subject multilevel models. We tested whether these networks were
different between those with a late circadian rhythm [concurrent delayed sleep phase (DSP) N =
172, 37% boys, 63% girls] and those without (N = 143, 22% boys, 78% girls).
Results: In adolescents without DSP, the temporal networks showed continuity only for low mood
from the previous to the following time point. In adolescents with DSP, there were more predictable
patterns of emotions. Feelings of depression led to a decrease of positive emotions and increase of
irritation and anxiety. The contemporaneous networks showed clusters of positive and negative
emotions in both groups and sleepiness decreased the experience of positive emotions concurrently.
Limitations: DSP in our current study was based only on one out of three diagnostic criteria of the
full disorder (DSM-5) and it was assessed only once.
Conclusions: These findings indicate that the dynamic organization of emotions and sleepiness is
different in adolescents with and without DSP. DSP adolescents have more predictable and
maladaptive emotional patterns during the day. Results provide new insight about why individuals
with DSP are at a heightened risk for decreased emotional adjustment.

INTRODUCTION
Globally, adolescents are sleeping fewer hours than they need (Owens, Adolescent Sleep Working
et al. 2014). This is followed by daytime sleepiness and symptoms of fatigue. Recent surveys
indicate a very high prevalence for hypersomnolence symptoms (>40% in U.S. youth), excessive
daytime sleepiness (>60% in Brazilian youth), or mild daytime sleepiness (>20% in Chinese youth)
during adolescence (Kolla, He et al. 2019, Meyer, Ferrari Junior et al. 2019, Wang, Liu et al. 2019).
Not surprisingly, daytime sleepiness has been associated with poorer sleep and a higher risk of
having mental health problems (Kolla, He et al. 2019).
To better understand adolescent development and the underlying processes, a closer
look at the dynamics of daytime sleepiness and emotional processes is needed. While a body of
evidence shows that quality of sleep and related alertness are associated with negative and positive
emotional states (Caldwell, Caldwell et al. 2004, Kahn-Greene, Killgore et al. 2007, Paterson,
Dorrian et al. 2011, Watling, Pawlik et al. 2017), little is known about their temporal dynamics.
Most of the studies have attempted to examine these associations independently (e.g., the effects of
sleepiness on emotions and the effects of emotions on sleepiness), but such separation does not
reflect the complexity of their mutual dependencies. Moreover, there appears to be a “vicious
cycle” as daytime sleepiness may compromise emotional regulation, which in many cases leads to
increased negative emotion that in turn disrupts sleep, leading to further impairments in alertness
and emotional wellbeing (Mauss, Troy et al. 2013). Understanding these dynamic and complex co-
occurring processes and their underlying mechanisms is of great importance to understand
developmental processes in adolescence, often driven by the common condition of chronically
insufficient sleep (Shochat, Cohen-Zion et al. 2014).
Regarding the dynamics between daytime sleepiness and mood in adolescence, one
group of adolescents is of specific interest: adolescents having a very late sleep rhythm, or delayed
sleep phase (DSP), which is a subclinical form of the delayed sleep phase disorder (DSPD). DSP is

often defined as having some of the three symptoms of the full disorder—most often the
persistently very late sleep rhythm. In population-based studies, this has been operationalized, for
example, as falling asleep after 1 a.m. at least 3 days per week (Danielsson, Markstrom et al. 2016).
DSP in adolescence is often followed by negative consequences in school performance (Gradisar
and Crowley 2013), and it has been associated with depression, anxiety, and symptoms of ADHD
(Sivertsen, Harvey et al. 2015). However, it is unclear how excessive daytime sleepiness and mood
are temporally organized. Tracking the daily fluctuations would give much needed understanding of
the topic.
However, feasible methods to measure and analyze complexity between sleepiness
and mood or other psychological processes have been scarce. To address the temporal dynamics, a
method called ecological momentary assessment (EMA), which uses repeated measurements of
multiple state-like factors with relatively short follow-up intervals, is needed. Regarding EMA and
sleep, previous studies have shown that experiences of fatigue in diseases such as multiple sclerosis
(Kratz, Murphy et al. 2017, Powell, Liossi et al. 2017) vary dynamically across the day, and
emotions are associated with these fluctuations (Powell, Liossi et al. 2017). Previous studies have
also shown that the experiences of psychological problems fluctuate over time, such as suicidal
ideation, even from hour to hour (Hallensleben, Spangenberg et al. 2017), and there are large
intrapersonal differences in these fluctuations.
Recently, a psychological network approach and related tools to analyze dynamic
relationships among multiple psychological variables have been developed (Epskamp, Cramer et al.
2012, Epskamp 2015). The basic idea behind the psychological network approach is that various
psychological states and problems develop as a result of the interaction among individual symptoms
or risk factors (Borsboom 2017). For example, troubles in sleeping may result in concentration
problems, which may lead to more rumination and daytime sleepiness, which in turn may lead to

negative emotional states. When the relations among these risk factors are sufficiently strong, they
can be self-sustained via a negative feedback loop.
Network analysis has so far mostly been applied to cross-sectional data but can also
be applied to EMA data using vector autoregression (VAR) techniques, in which a variable at a
certain time point (t1) is predicted by the same variable at the previous time point (t–1)
(autoregressive effects) and all other variables at t–1 (cross-lagged effects) (Epskamp, Waldorp et
al. 2018). These autoregressive and cross-lagged effects can be quantified and visualized in a
network. The network analyses with VAR techniques have extended more traditional multilevel
analysis by estimating and visualizing the co-occurrence of multiple variables, allowing generation
of hypotheses about the potential dynamic process among multiple variables. By allowing VAR
coefficients to differ across individuals via multilevel modeling, it is possible to model and
visualize temporal dynamics between sleepiness and mood at the group level. Thus, network
analyses could guide researchers and clinicians toward more complex and dynamic thinking about
psychological states (Fried, van Borkulo et al. 2017), such as sleepiness and emotional states. As far
as we know, there are no published studies focusing on the dynamics of emotional states using
longitudinal network approach, although some studies have modelled psychiatric problems,
including suicidality (Rath, de Beurs et al. 2019) and auditory verbal hallucinations (Jongeneel,
Aalbers et al. 2020).”
Network analysis extends standard time series analysis, such as hierarchal linear
modeling, by offering a visual representation of the relations among all assessed variables. In our
study, we applied the VAR method to examine the dynamic associations between daytime
sleepiness and emotional states, including being depressed, anxious, content, irritated, and happy.
To increase understanding of the effects of very late sleep rhythms on sleepiness and emotions, we
compared the sleepiness-emotion networks between those with a concurrent DSP and those without
classified based on actigraphy measurements.

METHODS
Sample and procedure
This research is part of the population-based cohort study SleepHelsinki!. Originally,
the Finnish Population Registry was utilized to identify all Finnish adolescents born between
January 1, 1999, and December 31, 2000 (n=10,476), who resided in Helsinki and whose native
language was registered as Finnish (72% of the total sample). The register thus included 7,539
adolescents (3,789 born in 1999 and 3,750 born in 2000), of whom 50% were boys. We sent
invitation letters to all registered adolescents to participate in the SleepHelsinki! study Phase 1,
which consisted of an online survey primarily targeting sleep, health, and behavior. The estimated
time for filling in the questionnaire was 30 minutes.
Altogether, 1,411 adolescents (19% of the initial cohort) responded to the online
survey, with valid responses from 1,374 (18%) participants. The age of the respondents did not
differ from the initial cohort mean age (p = 0.34), but the respondents were more often girls (66%, p
< 0.0001). All respondents signed an electronic consent form for Phase 1. Ethical permission was
obtained from The Hospital District of Helsinki and Uusimaa Ethics Committee for gynecology and
obstetrics, pediatrics, and psychiatry (Decision number 50/13/03/03/2016). The study is registered
under Clinical Trials (ID: 1287174).
The SleepHelsinki! study (total N = 552) focused on late sleep rhythms. Based by
online survey questionnaire two subsamples: (A) those without (N=188) and (B) those with late
sleep rhythms (N=364) were identified and invited to participate in the EMA phase. The criteria for
belonging to the late sleep phase group was reporting bedtime after 1 a.m. at least three times per
week. Out of these 552 adolescents, 353 agreed to participate and 24 dropped out before completing
the EMA phase, leaving us with a sample of 329 adolescents. The EMA period of the study was
conducted between November 2016 and December 2017. The data for this study were thus from

late adolescence (mean age 16.9 years, SD = 0.6) when the EMA measurements were done. A total
of 315 participants provided usable EMA data and formed the final analyses sample.
The participants underwent a minimum 7-day EMA assessment with three signal-
contingent assessments per day using the “Psymate” software, resulting in a maximum of 66
assessments per participant. The first EMA signal was scheduled in the morning (around 8–10
a.m.), the second in the afternoon (1–5 p.m.), and the final in the evening (around 8–10 p.m.).
Participants could postpone a prompt for 30 minutes if they were not able to answer the questions
immediately, and they had the possibility to reject a prompt. The data set consisted of 4,348
observations (315 persons).
Additionally, adolescents’ sleep timing was measured using accelerometers
(GeneActiv Original, Kimbolton, UK) to determine and confirm possible DSP tendencies. Mean
sleep duration in those with DSP was 7:23 hours (SD=1:01) and in those without 8:09 hours
(SD=0:43). The sleep mid-point in those with DSP was 5:31 (SD=1:05) and in those without 3:50
(SD=0:36).
Measures
During the EMA assessment, participants rated their momentary sleepiness-perceived
depressiveness, anxiousness, irritation, contentedness, and happiness by answering a structured 14-
item questionnaire. At each measurement point, participants reported how alert vs. sleepy they felt
during the last 10 minutes on a 9-point scale with 5 anchors (1 = very alert; 3 = alert; 5 = neither
alert nor sleepy; 7 = sleepy but no trouble staying awake; and 9 = very sleepy, fighting to stay
awake) (Karolinska Sleepiness Scale, KSS).
Additionally, participants reported how they felt using two positive effect and three
negative effect items using 7-point scales from 1 (not at all) to 7 (very much). These specific
emotions were chosen to include those most frequently appearing in several longer affect checklists
(Diener and Emmons 1984, Watson, Clark et al. 1988). The constructs represented were depression,

anxiety (worried), and hostility (irritated) on the negative affect side. Activation (energetic/
sleepiness) and positive feelings (happy, and content) were represented on the positive side. The list
was required to be short to facilitate its use over multiple daily assessments.
The actigraphy measurements covered a minimum of 3 nights (range 3–12 nights) and
yielded a binary classification of concurrent DSP tendency. This information was calculated based
on going to sleep after 1 a.m. at least three times per week. The classification was used to compare
the emotional responses of those with weaker circadian control to those without. Based on the
actigraphy measurements 172 participants were classified as having a late circadian rhythm and
having a concurrent delayed sleep phase (DSP) and 143 were classified as not having DSP (non-
delayed sleep phase / non-DSM) circadian rhythm. Of those with DSM 63% were girls and of those
with non-DSM 78% were girls (X2 = 8.22, df = 1, p-value = 0.004 for sex difference). Parental
education was used as a measure of parental socio-economic status (SES). Participants were asked
to report the highest educational attainment of their parents, and the highest report was selected as
the basis for classifying participants’ SES as (1) lower (2) middle, or, (3) upper. Lower SES
included minimum compulsory educational attainment. Education attained beyond this (i.e.
vocational school, technical college) was classified as middle level SES. SES was classified as
upper level if either parent had university level degree. Most of the parents of those in DSP (N=
119, 73%) and in those non-DSP (N = 105, 77%) belonged to the highest SES category. There were
no differences in parental socioeconomic status measured as education (lower / middle/ upper)
between the DSP and non -DSP group (2(2) = 0.83, p = 0.66).
Statistical analysis
To estimate the different network structures over all participants, we applied
multilevel vector autoregression (mlVAR) models on the data (Epskamp, Waldorp et al. 2018), as
implemented within the mlVAR package in R. In conducting the analyses and presenting the results

we mostly followed the procedure presented by Jongeneel and others (Jongeneel, Aalbers et al.
2020). Temporal dynamics within individuals are estimated by regressing scores of an emotion at
time t on a previous (i.e., lagged) value of itself at t-1. VAR modeling indicates that all variables at
time t are regressed on a t-1 version of themselves, resulting in a vector of lagged regression
coefficients (fixed effects). The multilevel modeling allows the VAR coefficients to differ between
individuals (random effects), and a temporal network was estimated. When visualizing the networks
in a two-dimensional graph, we used the Fruchterman-Reingold (FR) algorithm, which places nodes
that are highly connected in the center of the network. The estimates of between-subject effects, the
sample means within subjects, were used as predictors. The contemporaneous network was
estimated using the residuals of the multilevel model that were used to estimate the temporal and
between-subject effects (Epskamp, Waldorp et al. 2018).
In the graphical representation of the network, variables are presented as nodes. These
networks are called temporal networks because they can be indicative of potential causality given
that one variable preceded the other in time. Epskamp et al. (2018) introduced an additional
network for estimating EMA data (a contemporaneous network) that can be used in the partial
association between the residuals of the temporal network that are the result of associations between
the variables that are not explained by the current chosen time interval, the chosen lag, or anything
else that is not explicitly measured and modeled. In the contemporaneous network, the edges
between nodes represent the partial correlation obtained after controlling for both temporal effects
and all other variables in the same window of measurement (Epskamp, Waldorp, Mõttus, &
Borsboom, 2017; Fisher, Reeves, Lawyer, Medaglia, & Rubel, 2017). When data are collected from
multiple subjects, between-person networks using EMA data may also be estimated. Between-
subject predictors are calculated using the covariance structure of stationary means. In addition, we
calculated the centrality measures of each symptom in each network (strength centrality identifies
how well each emotion in a network is associated with the other emotions). We calculated the

strength of the nodes for all networks, using the R package qgraph (Epskamp et al., 2012). In the
temporal network centrality indicates both how well each emotion is predicted by others (in-
strength) and how well it predicts others (out-strength).
Variables were standardized before estimation and scaled within persons via mlVAR.
Networks were presented using the graph package in R.
RESULTS
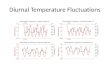
Means and standard deviations for all emotions and sleepiness in those with and
without DSP are presented in Table 1 and the distribution of the emotions in the high and low
sleepiness group in Figure 1. Those with DSP more often experienced anxiety, depression, and
irritation, and those without DSP more often were happy and content. There were no differences in
sleepiness reporting between the groups. Only small differences were found in distributions of
emotion reporting between those with and without DSP (Figure 1). Girls were slightly less happy
(mean 4.34 vrs. 4.81, p-value 0.006), less content (mean 4.46 vrs. 5.04, p-value 0.002), and more
anxious (mean 2.32 vrs. 1.88, p-value 0.025) than boys.
Temporal networks
The temporal network including the directed associations is based on time series EMA data that was
analyzed with timelags. All variables at a certain measurement point is predicted by the same
variable and all other variables at the previous measurement point providing information about the
temporal multivariate relations. All coefficients are allowed to differ across individuals by using
multilevel modeling, and thus time dynamics are possible to model and visualize at the group level.
The left top panel in Figure 2 shows how emotions predicted themselves (autoregressions) and each
other across time (adjusted predictions) in those without DSP and the left bottom panel in those
with DSP. Green lines represent positive and red lines (dotted) represent negative associations. The
thickness of the line corresponds to the strength of the association. The panels in the right-hand side
show the centrality measures.

In individuals without DSP, there were no significant patterns observable in the
fluctuation of emotions except a bidirectional loop between depression and irritation (0.12, p =
0.002/0.06, p = 0.17) and a continuous loop within depression and anxiety. In individuals with DSP,
there were several significant patterns in the temporal fluctuations of emotions. Feelings of
depression led to a decrease of positive emotions (depressed -> happy, -0.074, p = 0.032 and
depressed -> content -0.100, p = 0.004) and increase of irritation (0.09, p = 0.006) and anxiety
(0.08, p =0.005) in the next measurement point. Irritation led both to a more positive mood (irritated
-> happy, 0.088, p = 0.001, irritated -> content 0.057, p = 0.030) and less sleepiness (-0.080, p =
0.009) and also to a less anxious state of mind (-0.07, p = 0.003). None of the emotional states were
predicted by sleepiness (p-values of fixed effects coefficient from sleepiness to emotional states all
non-significant. Being anxious predicted sleepiness (0.08, p = 0.04) and happiness (-0.09, p =
0.005). Only depressiveness and anxiousness predicted themselves in the consecutive measurement
points.
In the temporal network, irritation had the highest on in-strength in those without DSP
and happiness in those with DSP, which shows that these emotions were most strongly predicted by
other emotions in these groups. In those without depressiveness and in those with DSP irritation and
depressiveness had high out-strength, meaning that their outgoing temporal associations were
relatively high (compared to other emotions in the network). However, considering the small
number of associations (edge weights) in those without DSP, it appears that none of the emotions
are strong predictors of other emotions.
Contemporaneous networks
The contemporaneous network, including all separate measurement points of each variable,
investigates concurrent relations between emotions. These relations are controlled for temporal
effects and all other emotions the same timepoint to compute a partial (independent of other
associations) correlations network and thus takes the temporal relationship into account. The

relationships within a measurement point can be separately analyzed from relationships between
timepoints in temporal models. In other words, it shows how emotions tend to co-occur at the same
moment, controlling for all other emotions at the same moment and for all temporal relations
among emotions.
Figure 3 shows the contemporaneous network between sleepiness and emotions in
individuals with and without DSP. The contemporaneous networks showed a clustering of positive
and negative emotions in both groups. Specifically, both sleepiness and irritation decreased the
experience of positive emotions concurrently. The contemporaneous networks were strikingly
similar in both groups. However, there were also subtle differences. In individuals with DSP,
sleepiness was associated only with decreased positive emotions, whereas in individuals without
DSP, sleepiness was in inverted association with irritation and in positive association with
depression. In both groups, positive emotions and depressiveness had the highest strength centrality.
Between subject network
Similarly, the between-individual networks (Figure 4) shows the pair-wise associations among the
mean levels of emotions over all measurement points, when adjusting for the mean levels of all
other emotions in the network. The between-subjects model is comparable to cross-sectional
analyses. In general, a positive connection between depressiveness, irritation and anxiety in this
analysis indicate that people with higher scores on depressiveness during a week tend to have
higher scores on anxiety/irritation during the same period and vice versa. In both DSP groups,
positive and negative emotions were again associated with each other and in that sense the results
presented in Figure 4 were relatively similar to those of the contemporaneous networks. In those
without DSP, happiness was negatively associated with irritation but in those with DSP, happiness
was negatively associated with depressiveness. Sleepiness was negatively associated sleepiness in
DSP whereas in non-DSP group sleepiness was associated with irritation. In those without DSP the
most central emotion was irritation, but in those with DSP it was happiness.

DISCUSSION
Poor sleep patterns, sleepiness, and related emotional states form a complex network
of associations that fluctuate over time. As far we know, no studies thus far have focused on
delayed sleep phase and investigated how it affects everyday emotions. In our study, we applied
mlVAR models to analyze the temporal and contemporaneous associations between sleepiness and
multiple emotional states and analyzed whether these networks were different between those
suffering from very late sleep rhythm (DSP) and others. Previous research suggests that DSP is
associated with elevated anxiety and depression scores (Saxvig, Pallesen et al. 2012) and other
problems relating to emotion regulation as well as mental health problems (Sivertsen, Harvey et al.
2015). The causes behind DSP are multiple: biological mechanisms and those relating to
psychological wellbeing are prominent in delaying sleep phase, especially during adolescence
(Micic, Lovato et al. 2016). The same pathways that might lead to DSP are likely to result in poorer
emotional welfare because anxiety and rumination tend to result in later sleep onset times—these
phenomena may also occur reciprocally with late sleep timing (Hiller, Lovato et al. 2014, Stewart,
Gibb et al. 2018). On the other hand, a lack of self-regulating skills is likely to be associated with
later sleep timing or delayed sleep phase (Owens, Dearth-Wesley et al. 2016). These overall
associations have been reported in several studies (Gradisar and Crowley 2013). However, it is not
known how these general challenges are related to dynamic fluctuations of emotions during the day.
In our study, individuals with DSP reported higher average levels of irritation,
depressiveness, and anxiousness and lower levels of contentedness and happiness than those
without. This observation is in line with findings from a large American study investigating over
10,000 adolescents aged 13–18 years. They reported increased risks of mental problems, suicidality,
and mood disorders in relation to greater bedtime delay, and they also found that adolescent sleep
behavior deviated substantially from recommended optimal standards, which was also the case in
our current study (Zhang, Paksarian et al. 2017). We found that, specifically in individuals with

DSP, there were several significant patterns in the temporal fluctuations of emotions, whereas in
individuals without DSP, the only temporal associations were seen in the bidirectional loop between
depression and irritation and in the continuity of anxiety. In the DSP group, feeling depressed led
equally to irritation and anxiety but also to feeling less happy and content at the following
measurement point. Interestingly, in the DSP group, feelings of irritation seemed to be a driving
node that led to feeling less sleepy, happier, and more content and equally less anxious. While
depression preceded irritation, it could show how irritation may function as a catalyst emotion to
feel better.
Without negative feedback loops between emotions unbalanced states that are never
able to recover or reach any positive state of mind would result. Thus, at some point, there need to
be a recovery from negative emotion and in DSP adolescents, and feeling irritated was such as
node. Irritation is not only a negative emotion, but the arousal associated with this emotion may
also potentiate self-directed action to solve the situation causing irritation and then lead to recovery
of the emotion. For adolescents, the irritation maybe also a more frequent emotional response
compared to adults, and, according to the current findings, an important trigger to get out of the
negative emotion loop.
Unexpectedly, sleepiness was not a driving state of mind for specific emotions in the
next time point in either the DSP or non-DSP group; thus, none of the emotional states were
predicted by sleepiness in the previous time point. The DSP group did not report more daytime
sleepiness than the non-DSP group. In objective measurements, they had a later sleep rhythm of 1
hour and 40 minutes, but the difference in sleep duration was only 45 minutes. The mean sleep
duration in the DSP group was over 7 hours during the measurement period, suggesting a sub-
optimal but still reasonable amount of sleep. Previous studies have shown that partial daily sleep
restriction of 2–4 hours increases subjective sleepiness (Lo, Groeger et al. 2012, Slobodanka, Basta
et al. 2013). It was recently reported that restricting sleep for 1 hour over 6 days caused increased

sleepiness (Santisteban, Brown et al. 2019). In that study, however, a similar impact was observed
in the control group with a placebo treatment (sham restriction), which suggests subjective
sleepiness to be affected by the individual’s conception of obtained sleep. Accordingly, the DSP
group in our study may regard their conventional sleep amount sufficient.
Nevertheless, while sleepiness had no association with any of the emotions in
temporal networks, it was positioned as expected in the contemporaneous network. It showed how
feeling sleepy associated with being less happy and content; thus, sleepiness was associated with
reduced positive emotion. Only in the non-DSP group, sleepiness associated also with increased
depression. In both the DSP and non-DSP groups, the different negative and positive feelings
appeared as separate clusters that were inversely correlated.
Although a large body of evidence suggests that poor sleep increases the experience of
negative emotions, reduces the occurrence of positive emotions, and changes the ways in which
individuals experience, understand, express, and regulate these emotions (Walker and van der Helm
2009, Kahn, Sheppes et al. 2013), only a few studies have been able to model and analyze the
dynamic, ongoing process of emotion generation. The strength of the network analyses and
specifically the mlVAR models is the ability to model such complex and potentially causal
relationships. The finding that irritation, rather than depression or anxiety, is the key emotion in
long-term emotional generation and regulation is to be replicated in future studies. This result
would be in line with a body of research showing an association between sleep deprivation and
increased anger and aggression, which was found in men and women and across various age groups
(Saghir, Syeda et al. 2018).
Similar findings were obtained by the previous study using EMA in those with and
without psychiatric disorders. Cousins and co-workers (2011) found that although the relationships
between individual emotions and sleep duration were strongly dependent on present psychiatric
disorders, more time asleep was associated with more positive affect for all diagnostic groups the

following day. However, in adolescents with diagnosed depression disorders, positive emotions
were associated with longer sleep duration in the following night. Higher daytime positive affect in
those with anxiety disorders was associated with less time in bed (Cousins, Whalen et al. 2011).
The findings from the contemporaneous network models as compared to the ones
from the temporal network models suggest that the emotions that we normally think follow each
other, in fact, does that very rapidly or basically are present simultaneously. That means that
positive emotions co-occur with other positive emotions and negative with other negative emotions.
These rapid predictions or co-occurrences followed very similar patterns in both DSP groups.
Fluctuations from positive to negative and from negative to positive happens with a time lag and
that fluctuation seems to be more apparent in those with DSP.
Limitations
There are some limitations that need to be considered. First, the definition of DSP in
our current study was based only on one out of three diagnostic criteria of the full disorder (DSM-
5). The very late sleep rhythm was also assessed only once, without knowing whether it referred to
persistently late or transiently late sleep rhythm. False classifications are possible regarding
subclinical DSP. Nevertheless, the sleep rhythm was defined with actigraphy, which increases
reliability of the assessment. Although EMA has multiple strengths compared to surveys and other
measurement techniques, the intensive nature of EMA studies makes it very difficult to scale up the
number of participants. The participants also must be trained in the use of devices and programs.
However, the target population of this study was probably very familiar with both phones and the
types of devices used. Given the considerable respondent burden involved, there was a risk of
selective drop out (those with DSP sleepiness, depression, or anxiety would not respond). In our
study, the mean number of responses was larger in those with DSP than those without. However, in
general, it would have been preferable to be able to gather more observations per participant from
the mlVAR modeling. One clear advantage of the temporal network over conventional statistical

models is that associations are bidirectional meaning that all variables are simultaneously predictors
and outcomes which provides information about the temporal multivariate relations in the data.
There were more girls than boys in our sample but larger share of boys belonged to
the DSP group. Thus, although the potential effects of gender differences on the association
between emotions is probably small, that needs to be confirmed in the future studies. Our data were
mostly collected during the school year, and data collection was paused for the summer holidays.
The actigraphy measurement period was aimed to represent typical sleep behavior, and we found no
differences between DSP groups across the representativeness of all seven weekdays. We can’t rule
out bias due to residual confounding as this was an observational study. One factor potentially
causing such bias, is socioeconomic status of the family, that may associate with both DSP and
emotions. However, there were no differences in parental socioeconomic status between DSP and
non-DSP groups in our sample and thus that could have technically not been a confounder in the
models.
Conclusions
A delayed sleep phase is extremely common in adolescents but rarely studied beyond
sleep behavior or sporadic health effects. Our study explores practical implications that emerge in
everyday life. The findings in our study highlight that DSP is related to higher levels of irritation,
depressiveness, and anxiousness and lower levels of contentedness and happiness than those with
earlier sleep phases. This suggests that DSP may play a part in every reaction and every emotion a
teenager experiences and thus further emphasizes the need for support for those with DSP.
REFERENCES
Borsboom, D. (2017). "A network theory of mental disorders." World Psychiatry 16: 5-13. Caldwell, J. A., J. L. Caldwell, J. K. Smith and D. L. Brown (2004). "Modafinil's effects on simulator performance and mood in pilots during 37 h without sleep." Aviat Space Environ Med 75(9): 777-784. Cousins, J. C., D. J. Whalen, R. E. Dahl, E. E. Forbes, T. M. Olino, N. D. Ryan and J. S. Silk (2011). "The bidirectional association between daytime affect and nighttime sleep in youth with anxiety and depression." J Pediatr Psychol 36(9): 969-979. Danielsson, K., A. Markstrom, J. E. Broman, L. von Knorring and M. Jansson-Frojmark (2016). "Delayed sleep phase disorder in a Swedish cohort of adolescents and young adults: Prevalence and associated factors." Chronobiol Int 33(10): 1331-1339. Diener, E. and R. A. Emmons (1984). "The independence of positive and negative affect." Journal of Personality and Social Psychology 47: 1105-1117. Epskamp, S. (2015). "bootnet: Bootstrap methods for various network estimation routines." R-package. Epskamp, S., A. O. Cramer, L. J. Waldorp and e. al. (2012). "qgraph: network visualizations of relationships in psychometric data. ." J Stat Softw 12: 1-18. Epskamp, S., L. J. Waldorp, R. Mottus and D. Borsboom (2018). "The Gaussian Graphical Model in Cross-Sectional and Time-Series Data." Multivariate Behav Res: 1-28. Fried, E. I., C. D. van Borkulo, A. O. Cramer, L. Boschloo, R. A. Schoevers and D. Borsboom (2017). "Mental disorders as networks of problems: a review of recent insights." Soc Psychiatry Psychiatr Epidemiol 52(1): 1-10. Gradisar, M. and S. J. Crowley (2013). "Delayed sleep phase disorder in youth." Curr Opin Psychiatry 26(6): 580-585. Hallensleben, N., L. Spangenberg, T. Forkmann, D. Rath, U. Hegerl, A. Kersting, T. W. Kallert and H. Glaesmer (2017). "Temporal Dynamics of Suicide Thoughts. First Results of an Ecological Momentary Assessment Study in Inpatients with depressive Disorders." Zeitschrift Fur Psychosomatische Medizin Und Psychotherapie 63(1): 60-61. Hiller, R. M., N. Lovato, M. Gradisar, M. Oliver and A. Slater (2014). "Trying to fall asleep while catastrophising: what sleep-disordered adolescents think and feel." Sleep Med 15(1): 96-103. Jongeneel, A., G. Aalbers, I. Bell, E. I. Fried, P. Delespaul, H. Riper, M. van der Gaag and D. van den Berg (2020). "A time-series network approach to auditory verbal hallucinations: Examining dynamic interactions using experience sampling methodology." Schizophr Res 215: 148-156. Kahn, M., G. Sheppes and A. Sadeh (2013). "Sleep and emotions: bidirectional links and underlying mechanisms." Int J Psychophysiol 89(2): 218-228. Kahn-Greene, E. T., D. B. Killgore, G. H. Kamimori, T. J. Balkin and W. D. Killgore (2007). "The effects of sleep deprivation on symptoms of psychopathology in healthy adults." Sleep Med 8(3): 215-221. Kolla, B. P., J. P. He, M. P. Mansukhani, S. Kotagal, M. A. Frye and K. R. Merikangas (2019). "Prevalence and Correlates of Hypersomnolence Symptoms in US Teens." J Am Acad Child Adolesc Psychiatry 58(7): 712-720. Kratz, A. L., S. L. Murphy and T. J. Braley (2017). "Ecological Momentary Assessment of Pain, Fatigue, Depressive, and Cognitive Symptoms Reveals Significant Daily Variability in Multiple Sclerosis." Arch Phys Med Rehabil 98(11): 2142-2150.

Lo, J. C., J. A. Groeger, N. Santhi, E. L. Arbon, A. S. Lazar, S. Hasan, M. von Schantz, S. N. Archer and D. J. Dijk (2012). "Effects of partial and acute total sleep deprivation on performance across cognitive domains, individuals and circadian phase." PLoS One 7(9): e45987. Mauss, I. B., A. S. Troy and M. K. LeBourgeois (2013). "Poorer sleep quality is associated with lower emotion-regulation ability in a laboratory paradigm." Cogn Emot 27(3): 567-576. Meyer, C., G. J. Ferrari Junior, R. D. Andrade, D. G. Barbosa, R. C. da Silva, A. Pelegrini and E. P. Gomes Felden (2019). "Factors associated with excessive daytime sleepiness among Brazilian adolescents." Chronobiol Int 36(9): 1240-1248. Micic, G., N. Lovato, M. Gradisar, S. A. Ferguson, H. J. Burgess and L. C. Lack (2016). "The etiology of delayed sleep phase disorder." Sleep Med Rev 27: 29-38. Owens, J., G. Adolescent Sleep Working and A. Committee on (2014). "Insufficient sleep in adolescents and young adults: an update on causes and consequences." Pediatrics 134(3): e921-932. Owens, J. A., T. Dearth-Wesley, D. Lewin, G. Gioia and R. C. Whitaker (2016). "Self-Regulation and Sleep Duration, Sleepiness, and Chronotype in Adolescents." Pediatrics 138(6). Paterson, J. L., J. Dorrian, S. A. Ferguson, S. M. Jay, N. Lamond, P. J. Murphy, S. S. Campbell and D. Dawson (2011). "Changes in structural aspects of mood during 39-66 h of sleep loss using matched controls." Appl Ergon 42(2): 196-201. Powell, D. J. H., C. Liossi, W. Schlotz and R. Moss-Morris (2017). "Tracking daily fatigue fluctuations in multiple sclerosis: ecological momentary assessment provides unique insights." J Behav Med 40(5): 772-783. Rath, D., D. de Beurs, N. Hallensleben, L. Spangenberg, H. Glaesmer and T. Forkmann (2019). "Modelling suicide ideation from beep to beep: Application of network analysis to ecological momentary assessment data." Internet Interv 18: 100292. Saghir, Z., J. N. Syeda, A. S. Muhammad and T. H. Balla Abdalla (2018). "The Amygdala, Sleep Debt, Sleep Deprivation, and the Emotion of Anger: A Possible Connection?" Cureus 10(7): e2912. Santisteban, J. A., T. G. Brown, M. C. Ouimet and R. Gruber (2019). "Cumulative mild partial sleep deprivation negatively impacts working memory capacity but not sustained attention, response inhibition, or decision making: a randomized controlled trial." Sleep Health 5(1): 101-108. Saxvig, I. W., S. Pallesen, A. Wilhelmsen-Langeland, H. Molde and B. Bjorvatn (2012). "Prevalence and correlates of delayed sleep phase in high school students." Sleep Med 13(2): 193-199. Shochat, T., M. Cohen-Zion and O. Tzischinsky (2014). "Functional consequences of inadequate sleep in adolescents: a systematic review." Sleep Med Rev 18(1): 75-87. Sivertsen, B., A. G. Harvey, S. Pallesen and M. Hysing (2015). "Mental health problems in adolescents with delayed sleep phase: results from a large population-based study in Norway." J Sleep Res 24(1): 11-18. Slobodanka, P., M. Basta, A. Vgontzas, I. Kritikou, M. Shaffer, M. Tsaoussoglou, D. Stiffler, Z. Stefanakis, E. Bixler and G. P. Chrousos (2013). "Effects of recovery sleep after one work week of mild sleep restriction on interleukin-6 and cortisol secretion and daytime sleepiness and performance." Am J Physiol Endocrinol Metab( 305): E890–E896,. Stewart, E., B. Gibb, G. Strauss and M. Coles (2018). "Disruptions in the Amount and Timing of Sleep and Repetitive Negative Thinking in Adolescents." Behav Sleep Med: 1-9. Walker, M. P. and E. van der Helm (2009). "Overnight therapy? The role of sleep in emotional brain processing." Psychol Bull 135(5): 731-748. Wang, Z. Y., Z. Z. Liu, C. X. Jia and X. Liu (2019). "Age at menarche, menstrual problems, and daytime sleepiness in Chinese adolescent girls." Sleep 42(6).

Watling, J., B. Pawlik, K. Scott, S. Booth and M. A. Short (2017). "Sleep Loss and Affective Functioning: More Than Just Mood." Behav Sleep Med 15(5): 394-409. Watson, D., L. A. Clark and A. Tellegen (1988). "Development and validation of brief measures of positive and negative affect: The PANAS scales." Journal of Personality and Social Psychology 54: 1063-1070. Zhang, J., D. Paksarian, F. Lamers, I. B. Hickie, J. He and K. R. Merikangas (2017). "Sleep Patterns and Mental Health Correlates in US Adolescents." J Pediatr 182: 137-143.

Figure 1. The distributions of sleepiness and emotional states in those with and without DSP
Figure 2. Temporal networks of sleepiness and emotional states according to DSP status. The green
lines represent positive and red negative partial correlations. Strength centrality represent the extent
how well a node is connected to other nodes. A high in-strength means the node is strongly
predicted by other nodes and high out-strength means that the node is a strong predictor of other
nodes.
Figure 3. Contemporaneous networks of sleepiness and emotional states according to DSP status.
The green lines represent positive and red negative partial correlations. Strength centrality represent
the extent how well a node is connected to other nodes.
Figure 4. Between – subject networks of sleepiness and emotional states according to DSP
status. The green lines represent positive and red negative partial correlations. Strength centrality
represent the extent how well a node is connected to other nodes.
Table 1. Emotional states and number of measurements by groups of DSP
Means and (SD)
No
N=1,833
Yes
N=2,293 p-value
Sleepiness during the day (range 1–8) 4.52 (1.99) 4.56 (1.91) 0.505
Feeling happy (range 1–7) 4.59 (1.37) 4.43 (1.42) 0.001
Feeling content (range 1–7) 4.62 (1.48) 4.40 (1.48) <0.001
Feeling depressed (range 1–7) 1.92 (1.29) 2.19 (1.56) <0.001
Feeling irritated (range 1–7) 2.29 (1.56) 2.42 (1.59) 0.012
Feeling anxious (range 1–7) 2.19 (1.52) 2.39 (1.70) <0.001
Number of measurement times 11.3 (9.55) 11.9 (10.0) 0.030