Embed Size (px)
Citation preview

Manual Coronary Endarterectomy with Saphenous Bypass: Experience with 263 Patients Eugene Wallsh, M.D., Andrew J. Franzone, M.D., Roy H. Clauss, M.D., Ciro Armellini, M.D., Felicien Steichen, M.D., and Simon H. Stertzer, M.D. I
ABSTRACT From January, 1972, until August, 1980, 271 manual coronary endarterectomies with bypass were performed in 263 patients. All patients underwent additional cardiac procedures simultane- ously. The group contained 254 distal right and 17 left endarterectomies (including 8 double endar- terectomies).
Clinical follow-up was 100°/~, operative mortality was 2.3% (6 out of 2631, and the rate of perioperative infarction was 4.9% (13 out of 263). Cineangiography was performed on 72 patients between 1 and 60 months after operation (mean, 15.4 months). Patency was 85% (61 out of 72).
Endarterectomy in a dominant right coronary ar- tery could be planned electively. Left coronary en- darterectomy was performed only when diffuse dis- ease prevented standard bypass.
Coronary endarterectomy may be used to extend operability with excellent clinical results, low perioperative mortality, and high late patency. Care- ful attention to technical aspects of core removal and myocardial protection are necessary for consistent results.
Manual coronary endarterectomy can be used to supplement standard bypass graft technique in coronary arteries with diffuse atherosclerosis. This report documents the cumulative experi- ence with this technique at Lenox Hill Hos- pital.
Materials and Methods From January, 1972, until August, 1980, 271 manual coronary endarterectomies with sa- phenous coronary- bypass were performed in
From the Departments of Surgery and Medicine, Lenox Hill Hospital, New York, NY. We thank Mr. Carl Manela for his technical assistance in the preparation of this manuscript. Presented at the Seventeenth Annual Meeting of The Soci- ety of Thoracic Surgeons, Jan 26-28,1981, Los Angeles, CA. Address reprint requests to Dr. Wallsh, 130 E 77th St, New York, NY 10021.
263 patients (238 men and 25 women). The age range was 35 to 74 years (mean, 58 years). There were 254 distal right and 17 left anterior descending coronary endarterectomies. Eight double endarterectomies were included. All patients simultaneously underwent additional cardiac procedures. Distal right coronary en- darterectomies were performed on angio- graphically dominant right coronary arteries with severe obstructive disease at the crux of the vessel. The disease process frequently ex- tended into the distal branches of the right coronary artery.
Techniques and results of coronary endar- terectomy with saphenous bypass have been described by several authors [l-91. Our own technique for manual endarterectomy with bypass has been modified since its original de- scription [lo]. When the right coronary artery was completely obstructed proximally, the dis- tal endarterectomy was performed on a nor- mothermic, beating heart. Cardiopulmonary bypass was carried out using arterial inflow to the ascending aorta, with a single cannula draining the right atrium. Ventricular venting was not used. Left atrial pressure was moni- tored continuously. The aVF lead was displayed on the electrocardiogram during the procedure. The acute margin of the heart was retracted ex- posing the crux of the right coronary vessel. A 1 cm incision was made about 1 cm from the bifurcation of the right coronary artery into its posterior descending coronary and atrio- ventricular groove branches. The incision was deepened to the atheromatous core. The outer linings of the coronary artery were teased from the core. Any circular muscle fibers ad- herent to the retained outer layers were scru- pulously removed to ensure a smooth lining. Interrupted sutures were placed circumferen- tially through the developed outer layers. Epicardium was included in each suture for maximum hemostasis.
451 0003-4975/81/110451-07!$01.25 @ 1981 by The Society of Thoracic Surgeons

452 The Annals of Thoracic Surgery Vol 32 No 5 November 1981
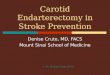
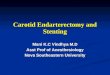
The atheromatous core was mobilized prox- imally first. The superficial coronary layers were progressively separated from the core by a combination of steady traction on the core and countertraction on the outer coats using a blunt instrument. After approximately 2 cm of core had been mobilized proximally, the speci- men was transected. The remaining proximal atheromatous material was permitted to retract. The distal specimen was then mobilized to the bifurcation of the posterior descending coro- nary and atrioventricular groove branches (Fig 1). The beating action of the heart against the steady traction on the core helped in separating the layers as distal dissection progressed. Each limb was removed separately. Excessive trac- tion could easily result in fracture of the spec- imen. Retained distal fragments or highly obstructive skip lesions could result in incom- plete endarterectomy, and could obstruct graft runoff and result in dissection with formation of a hematoma ad the endarterectomy site. Ex- amination of the extracted specimen usually confirmed complete removal of the core. The appearance of fine, translucent distal ends in&- cated core separation at a site of normal intima (Fig 2). However, if fracture of the endarterec- tomy specimen occurred or if atheromatous material could be palpated in the distal branches, an incision was made over the plaque. Then the residual material was mo- bilized and extracted from the branch vessel.
Fig I. Distal right coronary endarterectomy technique. The proximal core has been severed, and the distal specimen is being progressively extracted. Sutures are in place.
Fig 2 . Intact endarterectomy specimen demonstrating thin, tapering branch ends, which usually indicate cow- plete core extraction.

453 Wallsh et al: Manual Coronary Endarterectomy
The secondary arteriotomy was closed with fine interrupted sutures placed at the edges of the now widened arterial channel. A temporary Silastic shunt was used in the artery as a stent around which the sutures were placed [l l l . This shunt technique facilitated suture placement in the coronary vessel with the heart beating.
Retained plaque or skip lesions were re- moved prior to completion of the proximal bypass. This sequence usually avoided he- matoma formation. Should hematoma occur, it might extend along the distal coronary branches and make secondary core extraction extremely awkward.
Following endarterectomy, a reversed seg- ment of saphenous vein was sutured to the en- darterectomy site with the previously placed interrupted sutures. The proximal aorta- saphenous vein anastomosis was constructed with a continuous suture within a partially occluding vascular clamp on an appropriate portion of the ascending aorta.
If S-T segment changes occurred in lead aVF during extraction of the atheromatous core, moderate systemic hypothermia was begun. In several instances of persistent electrocardio- graphic changes following core extraction, de- spite intravenous administration of nitroglyc- erin and moderate systemic cooling, arterial blood was perfused into the endarterectomized channel using a soft T-shaped plastic cannula. The S-T segment changes were rapidly re- versed.
When the right coronary artery was not com- pletely obstructed, retraction of the edge of the heart for adequate exposure might occlude the intrinsic blood flow in the right coronary artery. Interruption of this flow in a dominant right coronary artery has resulted in profound elec- trocardiographic changes and rapid infarction. When there was incomplete coronary occlusion, the cardiopulmonary bypass technique was al- tered to include the use of hypothermic car- dioplegia. The endarterectomy technique was essentially the same.
Endarterectomy of the left anterior descend- ing coronary vessel was rarely a planned proce- dure. In diffusely diseased vessels, all attempts were directed at bypassing to an angiographi- cally patent portion of the vessel. However, two
situations necessitated endarterectomy. The first arose upon spontaneous separation of an atheromatous intima when wall integrity could not be reconstructed by appropriate suturing. The second involved a short area of total coro- nary obstruction interposed between two an- giographically patent segments. Endarterec- tomy of this short segment permitted runoff into a wide vascular bed with a single graft. Cardioplegia technique was usually employed during the performance of endarterectomy of the anterior descending coronary artery. A longer-than-normal arteriotomy was performed to facilitate manipulation of the atheromatous core. The appropriate plane for dissection was usually identified easily. Gentle traction on the core with countertraction on the outer layers with a blunt instrument served to deliver the core both proximally and distally. Spontaneous fracture of a short specimen at an appropriate site usually occurred. However, multiple ar- teriotomies along the anterior descending coro- nary artery have been necessary to ensure ade- quate core removal. Following delivery of the core, the vein bypass was constructed to the arteriotomy site by means of continuous suture technique. Antiplatelet drugs or anticoagulants were not used routinely in this series of pa- tients.
Results Clinical follow-up of the 263 patients was 100% either by office interview or letter to the patient or attending physician. Follow-up ranged from 5 to 96 months (mean, 54 months). The opera- tive mortality was 2.3% (6 out of 263). Low cardiac output and myocardial infarction ac- counted for the deaths. Immediate graft fail- ure with hematoma was evident in 1 patient. Perioperative myocardial infarction as indi- cated by new electrocardiographic Q waves or positive isoenzyme changes occurred in 4.9% (13 out of 263). Nine of these intraoperative in- farctions occurred in the first 29 patients oper- ated on in this series. During this period, elec- tive electrical fibrillation was used during operation. The occurrence of a small Q wave in lead aVF during the procedure was not consis- tently associated d i th technical failure of the graft. Four of the patients who had new Q

454 The Annals of Thoracic Surgery Vol 32 No 5 November 1981
waves were restudied and found to have patent grafts. In 2 of 11 patients in whom hematomas developed at the site of saphenous bypass en- darterectomy, electrocardiographic changes de- veloped consistent with myocardial damage. With modification of the endarterectomy tech- nique as described, the incidence of local hematoma and regional electrocardiographic changes has markedly decreased. Hematomas have not occurred in the group of 17 patients undergoing endarterectomy of the anterior de- scending coronary artery.
Late presumed coronary deaths occurred in 1.9% (5 out of 263). Two late noncoronary deaths also occurred: one from sepsis and the other from hepatitis.
Postoperative catheterization for cineangiog- raphy was performed on 27% (72 out of 263) of patients between 1 and 60 months (mean, 15.4 months) after operation. This group consisted of 1 anterior descending and 71 right coronary artery endarterectomies. The overall patency was 85% (61 out of 72). The graft to the anterior descending coronary artery was closed.
Comment Endarterectomy with saphenous bypass is a useful adjunct in the treatment of diffuse coro- nary artery disease. Technically inoperable ves- sels or vessels with limited operability by an- giographic appearance can be salvaged by this technique. Late patency may be enhanced by anastomosis to an atherosclerosis-free, grossly smooth vessel when compared with bypasses constructed in heavily diseased segments. More complete revascularization is possible with en- darterectomy by wider distribution of the graft flow.
Elective coronary endarterectomy and sa- phenous coronary graft can usually be planned in the right coronary artery when an angio- graphically dominant vessel is completely obstructed proximally and shows retrograde filling of the distal branches through collateral circulation. Endarterectomy of the left anterior descending coronary artery is nonelective. The results are less predictable than in the right coronary artery. However, in some situations its use is unavoidable. Endarterectomies of diagonal and marginal branches were initially
evaluated and discontinued because of incon- sistent core extraction.
The segmental wall motion of the inferior surface of the left ventricle demonstrated by contrast ventriculography is not an absolute determinant of the feasibility or the success of distal right coronary endarterectomy with bypass. This finding is in contrast to another report [7]. Despite fibrosis in the inferior wall, restoration of blood flow in the distal branches of the right coronary artery may represent the source of major collaterals to the remaining cir- culation in patients with diffuse coronary artery disease.
Complete core removal is essential for success of the endarterectomy. Confirmation of com- plete extraction by examination of the distal branches of the atheromatous specimen can be deceiving. In the right coronary artery, palpa- tion of the distal vessels is especially important in disclosing either retained specimens or skip areas of plaque. Removal of these distal ob- structions is essential for consistent success of the procedure.
In a dominant, small right coronary artery, less than 2 to 3 mm in diameter, pliable walls of the core may not separate easily. Attempting extraction can leave a thin, porous wall result- ing in diffuse hematoma formation at the anastomosis and along the coronary branches. This can cause immediate failure of the endar- terectomy and bypass graft, with regional in- farction. In this series, hematoma formation oc- curred in 11 of 263 patients (4.2%) with severe diffuse atherosclerosis.
Local dissection of an atherosclerotic plaque at the site of saphenous coronary bypass in ves- sels in which endarterectomy has not been performed has been demonstrated to be one of the causes of graft failure [12]. Endarterectomy with bypass to vessels with heavily athero- sclerotic walls seems to be a reasonable surgi- cal alternative to simple bypass.
The incidence of perioperative infarction of 4.9% (13 out of 263) primarily reflects the nine instances that occurred within the first 29 pa- tients undergoing operation in this series [lo]. Elective ventricular fibrillation was used with these patients. Subsequently, this technique has been discarded.

455 Wallsh et al: Manual Coronary Endarterectomy
The operative mortality of 2.3% in these pa- tients with severe diffuse coronary artery dis- ease, as well as the late patency rate of 85% (61 out of 72) in the follow-up period, indicate an expanding role for coronary endarterectomy in the operative treatment of extensive coronary disease. Myocardial protection and careful at- tention to the technical aspects of core removal are essential.
Improvement in the operative status of the atherosclerotic vessel wall as well as the possi- bility of vein grafting to angiographically inop- erable vessels has been a consistent observa- tion in manual coronary endarterectomy with bypass.
References 1.
2.
3.
4.
5.
6.
7.
8 .
9.
10.
Robinson G , Kaplitt MJ, Philips P, Pate1 8: Com- plete surgical correction of the totally occluded and diffusely diseased right coronary artery. J Thorac Cardiovasc Surg 60:504, 1970 Absolon KB, Lewis EH, Bashour F: Simultaneous peripheral coronary endarterectomy and bypass graft in coronary artery obstruction. Surg Gyne- col Obstet 132:1083, 1971 Urschel HC Jr, Razzuk MA: Reconstruction of the left anterior descending coronary artery: prox- imal vein bypass and distal gas endarterectomy. JAMA 16:141, 1971 Urschel HC Jr, Razzuk MA, Wood RE, Paulson DL: Distal COz coronary artery endarterectomy and proximal vein bypass graft. Ann Thorac Surg 14:10, 1972 Dumanian AV, Giragos HG, Hadidian HA, et al: Endarterectomy of the branches of the left coro- nary artery in combination with an aorta-to- coronary artery reversed saphenous vein graft. Ann Thorac Surg 14:609, 1972 Groves LK, Loop FD, Silver GM: Endarterectomy as a supplement to coronary artery-saphenous vein bypass surgery. J Thorac Cardiovasc Surg 64:514, 1972 Cheanvechai C, Groves LK, Reyes EA, et al: Manual coronary endarterectomy: clinical ex- perience in 315 patients. J Thorac Cardiovasc Surg 70:524, 1975 - Hochberg MS, Merrill WH, Michaelis LL, McIn- tosh CL: Results of combined coronary endar- terectomy and coronary bypass for diffuse coro- nary artery disease. J Thorac Cardiovasc Surg 75:38, 1978 Morton BC, Beanlands DS, Chambers RS, et al: Fate of the graft and native vessel following en- darterectomy of the left anterior descending coronary artery. Can J Surg 22:142, 1979 Wallsh E, Weinstein G, Franzone AJ, Stertzer
SH: The use of distal right coronary endarterec- tomy and saphenous coronary bypass to decrease total grafts and extend operability in patients with coronary artery disease. In Norman JC (ed): Coronary Artery Medicine and Surgery: Con- cepts and Controversies. New York, Appleton- Century-Crofts, 1975, chap 68
11. Franzone AJ, Wallsh E, Stertzer SH, et al: Re- duced incidence of intraoperative myocardial infarction during coronary bypass surgery with use of intracoronary shunt technique. Am J Car- diol 39:1017, 1977
12. Griffith LSC, Bulkley BH, Hutchins GM, Brawley RK: Occlusive changes at the coronary artery- bypass graft anastomosis: morphologic study of 95 grafts. J Thorac Cardiovasc Surg 73:668, 1977
Discussion DR. HAROLD c. URSCHEL, JR. (Dallas, TX): I congratu- late Dr. Wallsh on his presentation. These good re- sults with the mechanical endarterectomy are limited to the right coronary artery primarily. Although a few of his patients were restudied in five years, the average was 15 months. I think we still have to con- sider this short-term follow-up, but the close to 90% patency is certainly in line with other series that have been presented, including ours. I do not believe that it is better to do an endarterectomy on a beating heart, and prefer a quiet, still heart on which to per- form the endarterectomy and the subsequent vein graft.
Historically, endarterectomy was used to attack coronary artery disease before the vein graft, and most of the early procedures were just endarterec- tomies alone with closure of the arteriotomy. Because we had a very high occlusion rate in the late 1960s, we changed our technique by closing the arteriotomy with a high-flow vein graft and combining the me- chanical endarterectomy with administration of car- bon dioxide so we could get a more complete distal endarterectomy, particularly in the left anterior de- scending coronary artery.
We now have done about 223 endarterectomies, the majority in the left anterior descending coronary artery, and the early patency has been around 90%. We do not know what the late patency will be. How- ever, in general, when occlusion occurs in the en- darterectomized vessel on restudy, there is usually much better collateral filling into this area than be- fore the operation. This knowledge plus the fact that these vessels would not be revascularized with- out endarterectomy probably make endarterectomy worth doing in certain instances. It may be the only way to help improve ventricular function in patients with severe diabetes or abnormal blood lipids,
The authors’ poor early results show improvement with experience. Catastrophe occurs, however, when we open a diseased vessel, separate the intima, and

456 The Annals of Thoracic Surgery Vol 32 No 5 November 1981
do an incomplete endarterectomy. Therefore, re- gardless of our philosophy of elective endarterec- tomy, whether we do it frequently or infrequently, I think we should all be proficient with this technique and be able to perform a complete, expeditious en- darterectomy if we damage a vessel we intended to graft initially.
DR. PABLO PEDRAZA (Milwaukee, WI): I congratulate Dr. Wallsh on his presentation of an excellent paper. We have performed coronary endarterectomy with increasing frequency over the past ten years. My associate, Dr. Johnson, and I have done single and multiple endarterectomies in about 30% of patients operated on in the last few years. Coronary endar- terectomy is our treatment of choice for severe, ad- vanced coronary disease. In most cases, it is the only practical method of revascularizing the septum.
In the past, we have demonstrated normal flow re- sponse of endarterectomized vessels with xenon washout studies. I will review our short-term pa- tency. From March, 1978, through July, 1980, 507 of 984 (52%) patients underwent recatheterization be- fore discharge; 167 of 507 (33%) had at least one coronary endarterectomy. Overall patency of grafts to endarterectomized arteries was 217 of 242 (89.7%) compared with 429 of 476 (90.1%) for conventional saphenous vein grafts in the same patients. Patency was essentially the same regardless of which major coronary system was endarterectomized.
For myocardial protection we rely on intermittent ischemic arrest at 30 to 34°C systemic. Rates of perioperative infarction and mortality have been similar to those reported today. We believe that coronary endarterectomy is here to stay.
DR. FRED E. VERMEULEN (Utrecht, The Netherlands): I also compliment the authors for their fine study and especially for their excellent results. Some years ago we did an analysis of 240 patients with 264 endar- terectomies. The data that came out of that study were somewhat at variance with those shown today.
Our rate of infarction after operation was higher, being 11% if we include hospital mortality or 8% if we consider only the survivors, and it appeared to be related to the preoperative status of the vessels. In 116 occluded vessels, eight infarctions occurred (7%), half of them not related to the area of the endarterec- tomy. However, for the endarterectomies done on 137 stenotic vessels, the infarction rate was much higher-15°/o-with 16 of the 20 infarctions related to the area of the endarterectomy. Could the low postoperative infarction rate in the authors' series be related to the fact that they mainly performed endar- terectomies in totally occluded vessels?
Regarding the patency rate, we noted that there was no relationship in our series with the preopera- tive status of the vessel. That means that endarterec-
tomies were followed by a 25% graft occlusion rate both in those that were done for occluded vessels and in those for stenotic vessels. However, in contradic- tion to what the authors showed, we noticed an in- creased occlusion rate from 19% overall to 35% if the endarterectomy was done in an area where there was already an infarction. So we disagree with the au- thors on this paint, as they did not detect any influ- ence of the local status of the ventricle on the graft patency.
We studied 105 patients by postoperative angiog- raphy, and compared the patency in grafts leading to endarterectomized vessels versus grafts leading to nonendarterectcimized vessels in the same patients (acting as their own control) and analyzed the quality of the runoff. We subdivided them into three groups: early controls (18 endarterectomies and 25 controls), an intermediate group after a mean of 7 months (64 endarterectomies and 49 controls), and a long-term group with a rnean of 21 months (62 endarterec- tomies and 75 controls). We found that the overall patency rate, even after almost two years, is still ac- ceptable: 74% after endarterectomy versus 81% in the control grafts. However, it was striking to us that at any time, about half of the patent grafts to endar- terectomized vessels did show a clearly residual or recurrent stenosis that, in our definition, was in ex- cess of 50% of the lumen. I wonder if the authors analyzed the quality of the runoff in their post- operative angiography series.
DR. GEORGE E. REED (Valhalla, NY): Dr. Wallsh very kindly asked me to review his manuscript, and I was delighted to have this preview. This beautifully pre- sented paper is a landmark, which I think should lay to rest any question about the appropriateness of right coronary endarterectomy or the effectiveness of manual endarterectomy. The 85% patency rate found in a group of patients who were restudied primarily because of chest complaints shows that this proce- dure can be the equal of the conventional bypass operation.
When one considers that the group who had repeat angiography was at a higher risk initially for graft closure and additionally that all had chest com- plaints, it suggests that the results are probably even more laudatory than we realize.
I was, however, disappointed to find that only 1 of the 17 left coronary endarterectomies was restudied and that this graft was closed. It is upon these left- sided procedures that I would like to elaborate.
During the past year, encouraged by having seen several late studies on patients who had right coro- nary endarterectomy and comforted by the safety af- forded by cardioplegia, and then confronted by an inoperable left anterior descending coronary artery in a very young man, we began doing left-sided en- darterectomies at the Westchester Medical Center. A

457 Wallsh et al: Manual Coronary Endarterectomy
total of 175 endarterectomies were performed in the last year in 132 patients. Of these, 63 were of the left anterior descending coronary or circumflex coronary artery. Our early clinical results corroborate the safety of this procedure as described by Dr. Wallsh. The only death in this group resulted from myocar- dial infarction, which occurred during repeat coro- nary angiography two weeks after operation in a pa- tient in whom all vessels were patent.
This is not a new operation. It has been well de- scribed, with minor variations, by many authors during the past ten years. What makes it more at- tractive now is the safety and precision that cardio- plegia provides. The salient features should be re- emphasized. It is imperative that the distal vessel be meticulously cleared of the disease and that we realize that multiple, long arteriotomies are fre- quently necessary.
DR. WALLSH: I thank the discussants and am gratified to see the renewed interest in a very useful tech- nique. I will attempt to answer some of the ques- tions brought up by Dr. Vermeulen, but have to base my answer partially on the fact that I did not hear any description of the surgical technique. I cannot explain why the rates of postoperative infarction and patency were different from our re- sults.
However, I will comment on the angiographic ap- pearance. Among the 72 patients studied, 8 were followed with multiple recatheterizations, not in- cluded as separate studies within the group. Some endarterectomies that we restudied were irregular in appearance, but during the period of restudy, they stayed open. I cannot explain this. Perhaps it is re- lated to nonatherosclerotic narrowing that may not change with time.
Notice from the American Board of Thoracic Surgery
The American Board of Thoracic Surgery now requires that candidates pass both the written and oral portions of the certifying examination.
In 1980 and thereafter, a written examination will be given prior to the oral examination. It will be necessary to pass the written examina- tion before the oral examination can be taken. The closing date for registration for 1983 is Au- gust 1,1982. The exact times and places of these examinations will be announced later.
A candidate applying for admission to the 1983 certifying examination must fulfil1 all the requirements for the Board in force at the time the application is received.
Please address all communications to the American Board of Thoracic Surgery, 14640 E Seven Mile Road, Detroit, MI 48205.