Embed Size (px)
Citation preview
ARTICLE IN PRESS
Travel Medicine and Infectious Disease (2006) 4, 275–280
KEYWORDMansonellaHypereosinMultiorganDiagnosticTherapy
1477-8939/$ - sdoi:10.1016/j.t
�Correspondifax: +41 61 284
E-mail addr
www.elsevierhealth.com/journals/tmid
Mansonella perstans causing symptomatichypereosinophilia in a missionary family
Christoph A. Fuxa, Bernard Chappuisb, Benedikt Holzerc,Christoph Aebia,d, Gerard Bordmanne, Hanspeter Martie,Christoph Hatze,�
aInstitute for Infectious Diseases, University of Bern, Friedbuhlstrasse 51, CH-3010 Bern, SwitzerlandbDepartment of Internal Medicine, University Hospital of Bern, Freiburgstrasse, CH-3010 Bern, SwitzerlandcGeneral Practitioner specialized in tropical diseases, Mittlere Strasse 3, CH-3600 Thun, SwitzerlanddDepartment of Pediatrics, University Hospital of Bern, CH-3010 Bern, SwitzerlandeMedical Department, Swiss Tropical Institute, Soc instr. s, CH-4002 Basel, Switzerland
Received 12 April 2005; accepted 28 July 2005Available online 25 October 2005
Sperstans;ophilia;disease;;
ee front matter & 2005maid.2005.07.001
ng author. Tel.: +41 6181 83.ess: christoph.hatz@un
Summary Mansonella perstans is rarely pathogenic. The rare reports of sympto-matic cases, however, include severe complications. Three cases of symptomatichypereosinophilia with multi-organ involvement are described in a missionary familyreturning from tropical Africa. Pathogenicity may be related to the induction ofhypereosinophilia rather than direct host-parasite interactions.& 2005 Elsevier Ltd. All rights reserved.
Introduction
Despite the wide distribution of Mansonella per-stans filaraemia across central and parts of north-ern Africa as well as northeastern South America,there are only few reports about symptomaticcarriers.1–9 M. perstans is, therefore, currentlyconsidered to be of little pathogenicity. However,this notion is largely based on the native populationand may not apply to temporary residents ofdifferent ethnic groups. The age at first exposure,
Elsevier Ltd. All rights reserv
284 82 55;
ibas.ch. (C. Hatz).
the immunological state and the number and timingof subsequent exposures to parasites have beenshown to influence the clinical presentation offilarial infections.10
Three cases of symptomatic hypereosinophiliaare described within a European family returningfrom the Central African Republic, where they hadlived for 12 years. M. perstans were the onlyparasites detected, and the symptoms were relatedto treatment in two cases. It is concluded that M.perstans can be pathogenic, at least for subjectswho are not native to endemic regions. The factthat all the observed symptoms can be explainedwith hypereosinophilia itself suggests that M.perstans might represent a trigger rather than a
ed.
ARTICLE IN PRESS
C.A. Fux et al.276
direct host pathogen and recalls the clinicalrelevance of severe hypereosinophilia.
Case histories
A 10 year-old Caucasian boy (case 1) consulted thefamily practitioner for fatigue and dyspnoe. In-vestigations revealed a severe mitral insufficiencywith consecutive pulmonary hypertension as well ashypereosinophilia of 7700� 109/l.
Further investigations of the family documentedeosinophilia in all members (Table 1). Preexistingallergies, atopy and a drug-induced hypersensitivitywere excluded anamnestically. There were neitherintestinal symptoms nor cutaneous pathologies.Filaraemia with M. perstans was detected in bothparents and the third son (Table 1). No otherparasites were found in any member of the family,neither in repeat blood samples nor in stoolsamples. A filarial ELISA test using Acanthocheilo-nema vitae antigens11 was positive in the threeindividuals with detected filaraemia and the young-est son. Unfortunately, this test does notdifferentiate between filarial species.12 Immuno-fluorescence tests directed against A. vitae-specificsurface antigens were negative in three andborderline in the fourth family member with apositive ELISA, arguing against the presence offilariae other than M. perstans. An ELISA foranisakis cross-reacted with all positive filarialserologies. All family members except the fatherexhibited antigen-specific IgG antibodies by anELISA with purified antigen from Strongyloidesratti. However, all the probes tested remainednegative for specific strongyloides IgE. Sampleswere similarly negative for circulating Wuchereriabancrofti-antigen in an immunochromatographictest and Gnathostoma spinigerum IgG antibodiesby western blotting.
Hypereosinophilia returned to normal valuesafter the boy (case 1) was treated with a singledose of ivermectin (200 mg/kg body weight) andalbendazole 200mg bid for 5 days. He subsequentlyunderwent mitral valve replacement. Histologyshowed myxoid degeneration without eosinophilicinfiltrations. Two cycles of prednisolone wereadministered to suppress recurrent hypereosino-philia, fatigue, transient cough and dyspnoe. Thelatter correlated with pulmonary infiltrations(Fig. 1a and b). The boy was readmitted fourmonths after valve replacement with hypereosino-philia, cardiac failure and fever. Echocardiographydocumented thrombosis of the mechanical valvedespite therapeutic anticoagulation necessitating
replacement of the valve prosthesis (Fig. 1c).13
Eosinophil counts finally returned to normal valuesafter therapy with steroids, diethylcarbamazine(DEC) and ivermectin (Table 1). The boy remainedasymptomatic over more than one year with three-monthly suppressive ivermectin medication.
At her first consultation, the eosinophilic granu-locytes of the asymptomatic mother (case 2)totaled 6100� 109/l. A diagnostic 50mg single-dose of DEC (Mazotti-test) provided no clinical orlaboratory signs of parasite decay. The skin-snipwas negative for O. volvulus and M. streptocercamicrofilariae. Treatment for M. perstans, consistingof a single dose of ivermectin (200 mg/kg) followedby albendazole 200mg bid was started. Transientswelling of the lips and the feet, pricklingparaesthesia, blurred vision and dyspnoe occurreda few days later. The medication was stopped after12 days and she was admitted to hospital with ageneralized maculo-papular exanthema and sinustachycardia. A cardiopathy was documented bynegative inferior ST-segments as well as elevatedserum troponin I (36.1 mg/l; norm o0.6) andcreatinin-kinase (725U/l; norm o167). Blood pres-sure and echocardiography were normal. Theeosinophilic count mounted to 19,900� 109/l,equaling 55% of total granulocytes. CRP was16mg/l (norm o5). Antinuclear antibodies, anti-neutrophil cytoplasmic antibodies and the rheuma-toid factor were negative. Several hours afteradmission, agitation, disorientation, choreaatheto-tic movements and hyperreflexia of the extremitieswere noted. No inflammatory cells were present inthe CSF, but magnetic resonance imaging documen-ted disseminated cerebral diffusion defects. Allclinical and laboratory abnormalities returned tonormal values within days after administering125mg of methylprednisolone per day. Both cor-onary angiography and myocardial biopsy per-formed 24 h after the onset of steroid therapywere normal. Without any further treatment, thepatient has remained asymptomatic and withnormal eosinophilic granulocyte counts for morethan 12 months.
The treatment for asymptomatic filaraemiaof the 14 year-old third son (case 3) had to bestopped after 11 days because of subfebriletemperatures, urticaria and a sharp rise in eosino-philic count (43,900� 109/l). He had been treatedwith a single dose of ivermectin (200 mg/kg) andalbendazole 200mg bid. All pathologic findingsnormalized after the addition of prednisolone withan initial dose of 30mg bid, tapered over 2 weeks.Echocardiography was normal and no pathologicalfindings have been observed during repeatedfollow-up visits.
ARTICLE IN PRESS
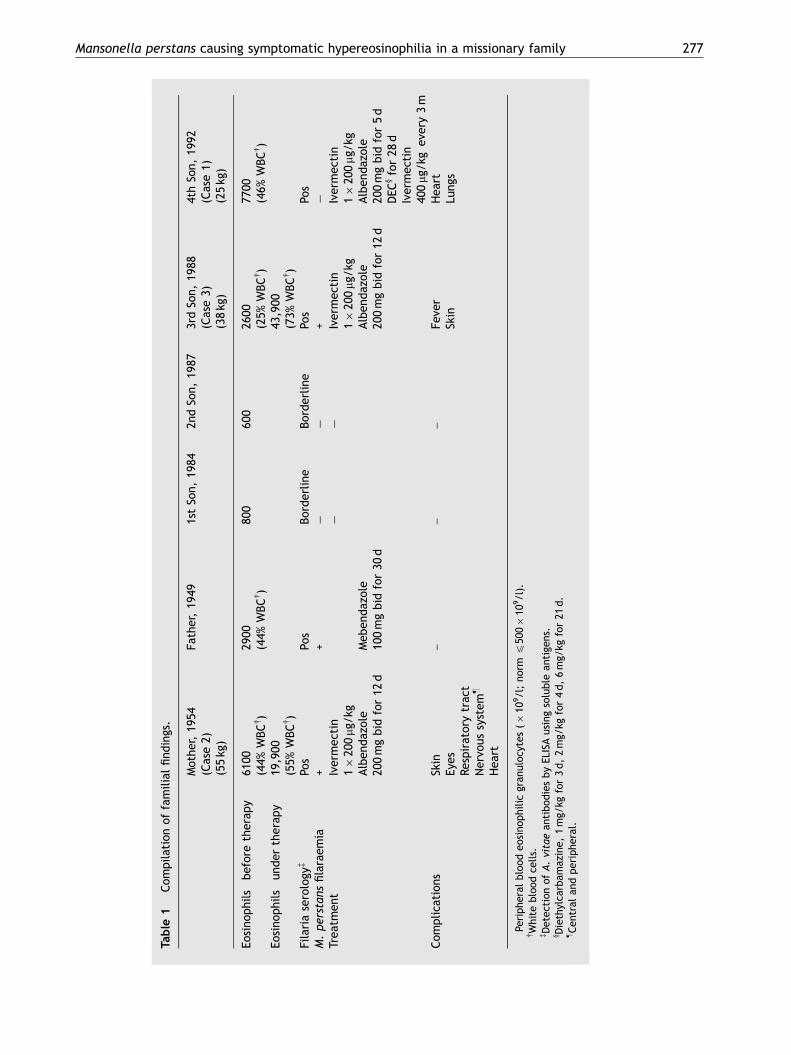
Table
1Com
pilationof
familialfind
ings.
Mothe
r,19
54Fa
ther,19
491stSo
n,19
842n
dSo
n,19
873rdSo
n,19
884thSo
n,19
92(Case2)
(Case3)
(Case1)
(55kg
)(38kg
)(25kg
)
Eosino
phils�beforetherap
y61
0029
0080
060
026
0077
00(44%
WBCy)
(44%
WBCy)
(25%
WBCy)
(46%
WBCy)
Eosino
phils�un
der
therap
y19
,900
43,900
(55%
WBCy)
(73%
WBCy)
Filariaserologyz
Pos
Pos
Borderline
Borderline
Pos
Pos
M.pe
rstans
filaraem
ia+
+�
�+
�
Trea
tmen
tIvermec
tin
��
Ivermec
tin
Ivermec
tin
1�20
0mg
/kg
1�20
0mg
/kg
1�20
0mg
/kg
Alben
dazole
Meb
endazole
Alben
dazole
Alben
dazole
200mgbid
for12
d10
0mgbid
for30
d20
0mgbid
for12
d20
0mgbid
for5d
DEC
yfor28
dIvermec
tin
400mg
/kg
every3m
Com
plica
tion
sSkin
––
–Fe
ver
Hea
rtEy
esSkin
Lung
sRe
spiratorytrac
tNervo
ussystem
z
Hea
rt
�Pe
riphe
ralblood
eosino
philicgran
uloc
ytes
(�10
9/l;no
rmp50
0�10
9/l).
yWhite
blood
cells.
zDetec
tion
ofA.vitaean
tibod
iesbyEL
ISAusingsolublean
tige
ns.
y Diethylca
rbam
azine,
1mg/
kgfor3d,2mg/
kgfor4d,6mg/
kgfor21
d.
zCen
tral
andperiphe
ral.
Mansonella perstans causing symptomatic hypereosinophilia in a missionary family 277
ARTICLE IN PRESS
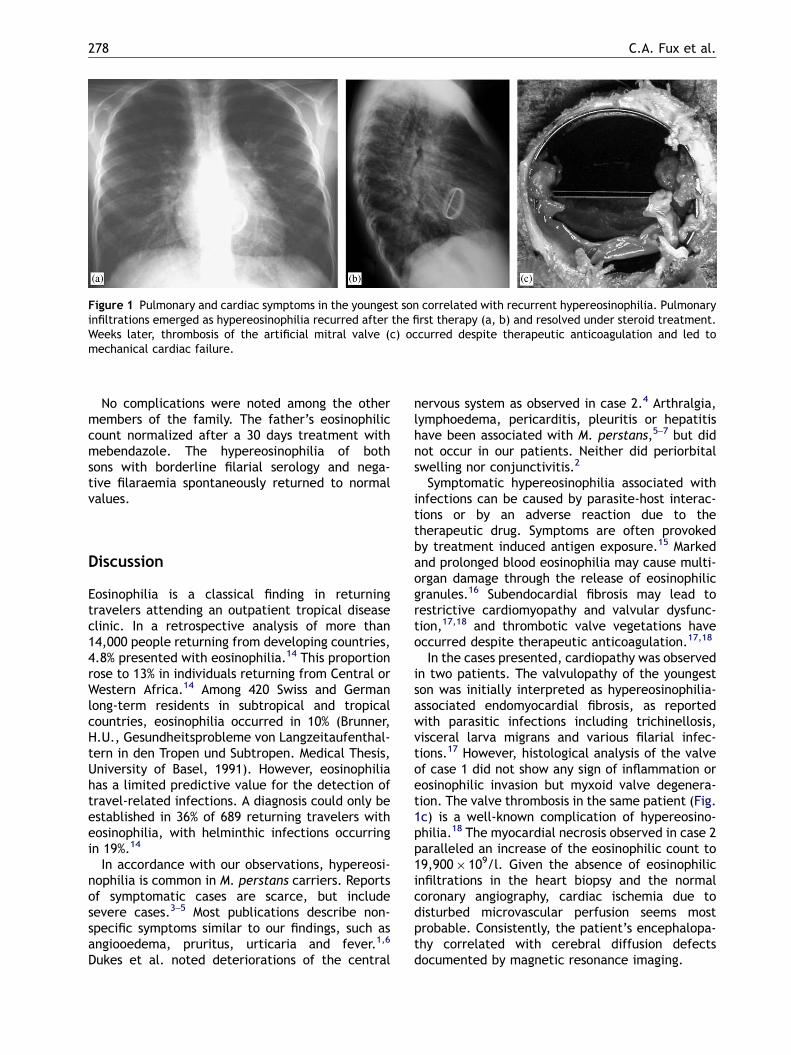
Figure 1 Pulmonary and cardiac symptoms in the youngest son correlated with recurrent hypereosinophilia. Pulmonaryinfiltrations emerged as hypereosinophilia recurred after the first therapy (a, b) and resolved under steroid treatment.Weeks later, thrombosis of the artificial mitral valve (c) occurred despite therapeutic anticoagulation and led tomechanical cardiac failure.
C.A. Fux et al.278
No complications were noted among the othermembers of the family. The father’s eosinophiliccount normalized after a 30 days treatment withmebendazole. The hypereosinophilia of bothsons with borderline filarial serology and nega-tive filaraemia spontaneously returned to normalvalues.
Discussion
Eosinophilia is a classical finding in returningtravelers attending an outpatient tropical diseaseclinic. In a retrospective analysis of more than14,000 people returning from developing countries,4.8% presented with eosinophilia.14 This proportionrose to 13% in individuals returning from Central orWestern Africa.14 Among 420 Swiss and Germanlong-term residents in subtropical and tropicalcountries, eosinophilia occurred in 10% (Brunner,H.U., Gesundheitsprobleme von Langzeitaufenthal-tern in den Tropen und Subtropen. Medical Thesis,University of Basel, 1991). However, eosinophiliahas a limited predictive value for the detection oftravel-related infections. A diagnosis could only beestablished in 36% of 689 returning travelers witheosinophilia, with helminthic infections occurringin 19%.14
In accordance with our observations, hypereosi-nophilia is common in M. perstans carriers. Reportsof symptomatic cases are scarce, but includesevere cases.3–5 Most publications describe non-specific symptoms similar to our findings, such asangiooedema, pruritus, urticaria and fever.1,6
Dukes et al. noted deteriorations of the central
nervous system as observed in case 2.4 Arthralgia,lymphoedema, pericarditis, pleuritis or hepatitishave been associated with M. perstans,5–7 but didnot occur in our patients. Neither did periorbitalswelling nor conjunctivitis.2
Symptomatic hypereosinophilia associated withinfections can be caused by parasite-host interac-tions or by an adverse reaction due to thetherapeutic drug. Symptoms are often provokedby treatment induced antigen exposure.15 Markedand prolonged blood eosinophilia may cause multi-organ damage through the release of eosinophilicgranules.16 Subendocardial fibrosis may lead torestrictive cardiomyopathy and valvular dysfunc-tion,17,18 and thrombotic valve vegetations haveoccurred despite therapeutic anticoagulation.17,18
In the cases presented, cardiopathy was observedin two patients. The valvulopathy of the youngestson was initially interpreted as hypereosinophilia-associated endomyocardial fibrosis, as reportedwith parasitic infections including trichinellosis,visceral larva migrans and various filarial infec-tions.17 However, histological analysis of the valveof case 1 did not show any sign of inflammation oreosinophilic invasion but myxoid valve degenera-tion. The valve thrombosis in the same patient (Fig.1c) is a well-known complication of hypereosino-philia.18 The myocardial necrosis observed in case 2paralleled an increase of the eosinophilic count to19,900� 109/l. Given the absence of eosinophilicinfiltrations in the heart biopsy and the normalcoronary angiography, cardiac ischemia due todisturbed microvascular perfusion seems mostprobable. Consistently, the patient’s encephalopa-thy correlated with cerebral diffusion defectsdocumented by magnetic resonance imaging.

ARTICLE IN PRESS
Mansonella perstans causing symptomatic hypereosinophilia in a missionary family 279
With the development of pneumopathy (Fig. 1aand b) in the absence of microfilaraemia, thedifferential diagnosis in case 1 included tropicalpulmonary eosinophilia (TPE). TPE is induced mostfrequently by undetected W. bancrofti19 and occursin nonimmune individuals rather than endemicpopulations. It is characterized by hypereosinophi-lia, asthma-like symptoms and non-specific pul-monary infiltrations in combination with generalmalaise. In our patient, pulmonary symptoms werepreceded by rising eosinophilic counts and respon-sive to steroid treatment. No signs pointed towardsa cardiac etiology of the pulmonary findings at thattime point. The recurrence of symptomatic hyper-eosinophilia after treatment with ivermectin andthe negative immunochromatographic test for W.bancrofti, however, argue against TPE in thispatient.
The development of classical allergy symptomsand rising eosinophilic counts after the onset oftherapy in two patients may have been stimulatedby a massive release of antigen of decayingparasites. Based on the current literature, thesymptoms observed are not directly associated witheither ivermectin or mebendazole. For M. perstans,a temporary rise in circulating immune complexesunder treatment has been observed. Yet, we areaware of only one report of clinical deteriorationunder therapy. Focal peritonitis in patients receiv-ing DEC for onchocerciasis was attributed todecaying adult M. perstans.20 Rare cases ofencephalopathy under treatment with ivermectinhave been observed in patients with high Loa loafilaraemia.15 Although higher concomitant M. per-stans microfilaraemia has been detected in thesepatients, no causative role could be established forthis parasite. Contrary to these cases, symptoms inour patient arose later than 5 days after the onsetof treatment. Furthermore, no parasites or inflam-matory signs were found in the CSF.
The treatment of M. perstans, although rarelyindicated, is not satisfactory. Multiple courses areoften necessary to eradicate the parasites. Currentstrategies include mebendazole 100mg bid for 30days, or albendazole 400mg bid for 10 days,although there are contradictory reports aboutthe efficacy of the latter.21,22 A 600 mg/kg singledose of ivermectin has been ineffective,23 and thetherapeutic success of repeated doses depended onthe cumulative dose.24 We combined ivermectinand albendazole in three of our patients in theattempt to treat M. perstans as well as undetected,possibly pathogenetic parasites. Although there islittle evidence for the efficacy of DEC against M.perstans, we prescribed it for the youngest son,because eosinophilia had recurred after a combined
treatment with ivermectin and albendazole andbecause the boy met inclusion criteria for TPE.
References
1. Adolph PE, McQuay RM. Diagnosis and treatment ofAcanthochilonema perstans filariasis. Am J Trop Med Hyg1962;11:76.
2. Baird JK, Neafie RC, Connor DH. Nodules in the conjunctiva,bung-eye, and bulge-eye in Africa caused by Mansonellaperstans. Am J Trop Med Hyg 1988;38:553–7.
3. Bourguignon G. Fatal acute hepatitis with massive localisa-tion of microfilaria perstans in the liver: Case. Ann Soc Belg1937;17:1.
4. Dukes DC, Gelfand M, Gadd KG, Clarke VD, Goldsmid JM.Cerebral filariasis caused by Acanthocheilonema perstans.Cent Afr J Med 1968;14:21–7.
5. Foster D. Filariasis: A rare cause of pericarditis. J Trop MedHyg 1956;59:212.
6. Holmes GK, Gelfand M, Boyt W, Mackenzie P. A study toinvestigate the pathogenicity of a parasite resemblingAcanthocheilonema perstans. Trans R Soc Trop Med Hyg1969;63:479–84.
7. Kahn JB. Pleural effusion associated with Dipetalonemaperstans (Acanthocheilonema perstans). J Infect Dis 1983;147:166.
8. Sasa M. Filariasis. A global survey of epidemiology andcontrol. Baltimore: University Park Press; 1976.
9. Wanji S, Tendongfor N, Esum M, Ndindeng S, Enyong P.Epidemiology of concomitant infections due to Loa loa,Mansonella perstans, and Onchocerca volvulus in rain forestvillages of Cameroon. Med Microbiol Immunol (Berl)2003;192:15–21.
10. Klion AD, Massougbodji A, Sadeler BC, Ottesen EA, NutmanTB. Loiasis in endemic and nonendemic populations:immunologically mediated differences in clinical presenta-tion. J Infect Dis 1991;163:1318–25.
11. Speiser F. Application of a multi-antigen enzyme-linkedimmunosorbent assay (ELISA). Ann Soc Belge Med trop1982;62:103–20.
12. Rocha A, Dreyer G, Poindexter RW, Ottesen EA. Syndromeresembling tropical pulmonary eosinophilia but of non-filarial aetiology: serological findings with filarial antigens.Trans R Soc Trop Med Hyg 1995;89:573–5.
13. Pavlovic M, Berdat P, Holzer B, Aebi C, Carrel T, PfammatterJP. Severe mitral valve involvement in a child withhypereosinophilia secondary to parasitic infection. J HeartValve Dis 2003;12:649–51.
14. Schulte C, Krebs B, Jelinek T, Nothdurft HD, von SonnenburgF, Loscher T. Diagnostic significance of blood eosinophilia inreturning travelers. Clin Infect Dis 2002;34:407–11.
15. Gardon J, Gardon-Wendel N, Demanga N, Kamgno J,Chippaux JP, Boussinesq M. Serious reactions after masstreatment of onchocerciasis with ivermectin in an areaendemic for Loa loa infection. Lancet 1997;350:18–22.
16. Cooper PJ, Awadzi K, Ottesen EA, Remick D, Nutman TB.Eosinophil sequestration and activation are associated withthe onset and severity of systemic adverse reactionsfollowing the treatment of onchocerciasis with ivermectin.J Infect Dis 1999;179:738–42.
17. Boustany Jr CW, Murphy GW, Hicks Jr GL. Mitral valvereplacement in idiopathic hypereosinophilic syndrome. AnnThorac Surg 1991;51:1007–9.

ARTICLE IN PRESS
C.A. Fux et al.280
18. Watanabe K, Tournilhac O, Camilleri LF. Recurrent throm-bosis of prosthetic mitral valve in idiopathic hypereosino-philic syndrome. J Heart Valve Dis 2002;11:447–9.
19. Ong RK, Doyle RL. Tropical pulmonary eosinophilia. Chest1998;113:1673–9.
20. Baird JK. Mansonella perstans infection (Mansonelliasis). In:Connor DH, Chandler FW, Schwartz DA, Manz HJ, Lack EE,editors. Pathology of infectious diseases. Stamford, Con-necticut: Appleton & Lange; 1997. p. 1487–91.
21. Duong TH, Kombila M, Ferrer A, Nguiri C, Richard-Lenoble D.Decrease in Mansonella perstans microfilaraemia after alben-dazole treatment. Trans R Soc Trop Med Hyg 1998;92:459.
22. Van den Enden E, Van Gompel A, Vervoort T, Van der Stuyft P,Van den Ende J. Mansonella perstans filariasis: failure ofalbendazole treatment. Ann Soc Belg Med Trop 1992;72:215–8.
23. Van den Enden E, Van Gompel A, Van der Stuyft P, Vervoort T,Van den Ende J. Treatment failure of a single high dose ofivermectin for Mansonella perstans filariasis. Trans R SocTrop Med Hyg 1993;87:90.
24. Fischer P, Kilian AH, Bamuhiiga J, Kipp W, Buttner DW.Prevalence of Mansonella perstans in western Uganda andits detection using the QBC-fluorescence method. ApplParasitol 1996;37:32–7.