Embed Size (px)
Citation preview
Manometric Asymmetry in the Anal Canal in Controls and Patients with Fecal Incontinence Nigel Williams, Ch.M., F.R.C.S., Josephine Barlow, M.Sc., Anthony Hobson, B.Sc., Nigel Scott, M.D., F.R.C.S., Miles Irving, M.D., F.R.C.S. From the Department of Surgery, University of Manchester, Hope Hospital, Salford, Manchester, United Kingdom
PURPOSE: This study was designed to ascertain the exis- tence of manometric asymmetry in the anal canal in con- trois and in patients with fecal incontinence. METHODS: A computerized manometric technique with an eight-channel perfusion catheter was used. Coefficient of variation (CV, a mathematical expression of the degree or magnitude of deviation of a set of data points from the mean) was devel- oped in this study as an index of anal canal manometric asymmetry. RESULTS: At 1 cm from the anal verge, mean CV was 9.3 and 8.7 percent in asymptomatic control males and females, respectively. During a maximum voluntary squeeze effort, mean CV in control males was 9.3 percent and was not significantly different (P = 0.28) from that in control females (7.8 percent). In 14 consecutive female patients with fecal incontinence, mean CV at rest (1 cm from the anal verge) was 21 percent and was significantly higher (P < 0.01) than in control females. Similarly, during a maximum voluntary squeeze effort, mean CV in patients with fecal incontinence was 20.5 percent and was signifi- cantly higher (P < 0.01) than in the female control group (7.8 percent). CONCLUSION: It is concluded that CV, a method of expressing anal sphincter manometric asymme- try, is a useful manometric parameter in the assessment of anorectal function. [Key words: Internal anal sphincter; External anal sphincter; Vector manometry; Radial asymme- try; Sphincter symmetry; Anal fissure; Fecal incontinence]
Williams N, Barlow J, Hobson A, Scott N, Irving M. Mano- metric asymmetry in the anal canal in controls and pa- tients with fecal incontinence. Dis Colon Rectum 1995;38: 1275-1280.
A nal m a n o m e t r y r emains one of the more com-
m o n inves t igat ions u s e d in assess ing anorec ta l
funct ion. i , 2 The mos t c o m m o n l y u s e d pa r ame te r s
f rom such a m a n o m e t r i c s tudy are the rest ing anal
canal p re s su re a n d the m a x i m u m anal canal p re s su re
fo l lowing a vo lun ta ry s q u e e z e effort. W h e r e micro-
ba l l oons are used , these p res su res c o m p r i s e the math-
emat ic c i rcumferent ia l m e a n of all p re s su res for that
surface area of the anal canal in direct contac t wi th the
ba l loon . Similarly, p e r f u s e d s ing le - lumen ca the ters
m e a s u r e anal canal p ressures at one loca t ion only.
Address reprint requests to Prof. Irving: Department of Surgery, University of Manchester, Hope Hospital, Salford, Manchester M6 8HD, United Kingdom.
Howeve r , these m e t h o d s are unab l e to de tec t m a n o -
metr ic radial a s y m m e t r y in the anal canal that m a y
occur in pat ients wi th fecal i ncon t inence resul t ing
f rom t raumat ic sph inc te r damage . 3-5 By contrast , mul-
t i lumen p e r f u s e d ca the ters assess anal canal p ressures
o n a c ross-sec t ional bas is at e ach r eco rd ing s tat ion
f rom the anal verge . It is, therefore , poss ib le , wi th
mul t i l umen catheters to e x a m i n e the p ressures in
each q u a d r a n t of the anal canal. 6
The ex i s tence of radial var ia t ion in anal canal pres-
sure has b e e n p rev ious ly d o c u m e n t e d b y the d e m o n -
s t rat ion of s ignif icant m a n o m e t r i c a s y m m e t r y in the
anal canal wi th anter ior quad ran t p ressures b e i n g
l o w e r than those lateral ly and p o s t e r i o r l y ] Several
m a n o m e t r i c terms have b e e n i n t roduc e d in an at-
t empt to quant i fy and express anal canal m a n o m e t r i c
asymmetry . These inc lude the "pressure vector , ''8
w h i c h desc r ibes the d i rec t ional s u m m a t i o n of four
q u a d r a n t p ressures in the anal canal and also the idea
of a m a n o m e t r i c "vector s y m m e t r y index. "4 In the
lat ter t echnique , a f lexible e igh t -channe l pe r fus ion
ca the te r is u s e d to ob ta in m a n o m e t r i c da ta that is
s to red on a pe r sona l c o m p u t e r and ana lyzed b y soft-
wa re d e v e l o p e d b y Perry. 4 The e ight channe l s of
m a n o m e t r i c data are r econs t ruc ted to gene ra t e a
t h r e e -d ime ns iona l wire f rame m o d e l of anal canal
pressures , and vec to r s y m m e t r y index rep resen t s 4
"the ratio of the smal les t to the largest sec tor v o l u m e s
of the p re s su re vec torgram." Using this index, uni ty
was t aken to r ep re sen t a per fec t ly symmet r i c sph inc-
ter (i.e., a per fec t circle) a n d in a ser ies of 21 a symp-
tomat ic female cont ro ls the m e a n vec to r s y m m e t r y
i n d e x (VSI) was 0.76.
Manomet r i c a s y m m e t r y in the anal canal was inves-
t iga ted b y s tudying a s y m p t o m a t i c cont ro ls and pa-
t ients wi th fecal incon t inence . Coeff icient of var ia t ion
(CV), a ma thema t i c e xp re s s ion of the magn i tude o f
dev ia t ion of a set of da ta po in ts f rom the g r o u p mean ,
1275

1276
was developed as an indicator of manometric sphinc-
ter asymmetry.
MATERIALS A N D M E T H O D S
The study was approved by the Ethical Committee
of Salford Health Authority. All patients to be included
in the study gave informed consent.
Manometric procedures were performed in the left
lateral decubitus position. Bowel preparation was not
used before the manometr ic procedure. Manometry
was performed using an Amdorfer M3, eight-lumen
polyvinyl chloride catheter (Arndorfer Inc., Lec-
t romed UK Ltd, Letchworth, Herts, UK) connected to
a pneumohydraul ic capillary infusion system and per-
fused with sterile degassed water at 0.4 ml /min/chan-
nel using a perfusion pressure of 85 kPa. Perfusion
ports were located 3 cm from the catheter tip and
were arranged radially at 45 ~ intervals. The catheter
was graduated at 1-cm intervals, with larger gradua-
tions at 5-cm intervals. Channel 1 was identified by a
longitudinal line along the catheter. Each capillary
tube from the M3 eight-lumen catheter was connected
to a TNF-R disposable transducer (Viggo-Spectrum,
Swindon, Wiltshire, UK) and data transmitted to a PC Polygraf TM (PC Polygraf HR, Synectics Medical, En-
field, Middlesex, UK) with all eight channels set to
record manometric data. Data were then transmitted
to a personal computer on which the procedure was
monitored in real time and also stored directly on the
hard disk for subsequent review and analysis.
Before a manometr ic procedure the catheter-perfu-
sion system was calibrated to 50 m m H g using a meter
rule and then calibrated to the patient such that 0
m m H g was at the level of the anal verge. The catheter
was inserted into the anal canal to a distance of 6 cm
from the anal verge so channel 1 corresponded to
dorsal (as viewed in the lithotomy position) and left
until a steady manometric trace was obtained. Data
were collected using a station pull-through technique.
Once the patient was comfortable and the manomet-
ric trace had stabilized, recording was commenced at
6 cm from the anal verge. The station from the anal
verge was checked after each 1-cm withdrawal, and
radial orientation was maintained constant. Maximum voluntary squeeze effort was measured at the station of highest resting pressure. Each squeeze effort lasted be tween sLx and eight seconds, during which patients
were actively encouraged to maintain tonic activity,
and three such efforts were recorded.
WILLIAMS ETAL Dis Colon Rectum, December 1995
C o e f f i c i e n t o f Variation
CV was developed as a hypothetic value to de- scribe the magnitude or degree of deviation of all
eight individual data points from that which would
form a perfect circle, i.e., if all data points were equal,
then this would represent a perfect circle. Coefficient
of variation then represents the magnitude of devia-
tion away from a perfect circle as opposed to the
standard deviation of the eight manometric values, which, in the present context, represents the segment-
to-segment variability. Coefficient of variation was
calculated as follows:
Standard Deviation CV = X 100
Mean
where SD and mean are calculated from the eight
manometric values pertaining to that station.
Therefore, for each station recording eight channels of manometr ic data, the mean, standard deviation,
and CV were calculated and tabulated. The method of
calculating CV was identical for data obtained both at
rest and during max imum voluntary squeeze effort.
Statistical Analysis
Mean values represent the algebraic mean of all
eight values obtained at manometry and are followed
by standard error of the mean (SEM) in parentheses.
Manometric data were normally distributed, and as-
sessment was performed using parametric tests. Com-
parison of male and female controls and be tween patient groups was performed using unpaired t-test.
Data within individual groups were analyzed using
paired Student's t-test.
RESULTS
Patients
Nine male controls (median age, 62 (range, 28-83)
years) and 11 female controls (median age, 53 (range, 29-71) years) were studied. All patients had a normal
bowel habit. Two female controls were nulliparous, three were primiparous, and six were multiparous. All
primiparae and multiparae had delivered vaginally, with forceps-assisted delivery being necessary in one multiparous and one primiparous female.
Fourteen consecutive female patients (median age, 60 (range, 35-77) years) with fecal incontinence (FD were studied. Age distribution was not significantly different (t = 0.95; P = 0.35) be tween female controls and female patients with fecal incontinence. All pa-
Vol. 38, No. 12 ANAL CANAL MANOMETRIC ASYMMETRY
T a b l e 1. Comparison of Coefficient of Variation of Manometric Data During a Resting Pull-Through
1277
Coefficient of Variation Station from Anal Verge (cm)
6 5 4 3 2 1
Control males 48.4 25.7 23.7 21.0 11.2 9.3 Control females 41.4 33.6 28.6 22.8 13.2 8.7 Females-FI 36.9 37.9 39.6 29.0 28.2 21.0 t Value* 0.37 0.38 1.02 1.00 2.03 3.33 P Value 0.72 0.71 0.32 0.33 0.06 0.003
* Comparison of female controls (11) with females with fecal incontinence (FI; 14).
8o
oXg.
o 60 g
>
"6 40
13=d' o "'=9
~ 2o o
0 i i l l i i i
6 5 4 3 2 1 0
Station from the anal verge/cm
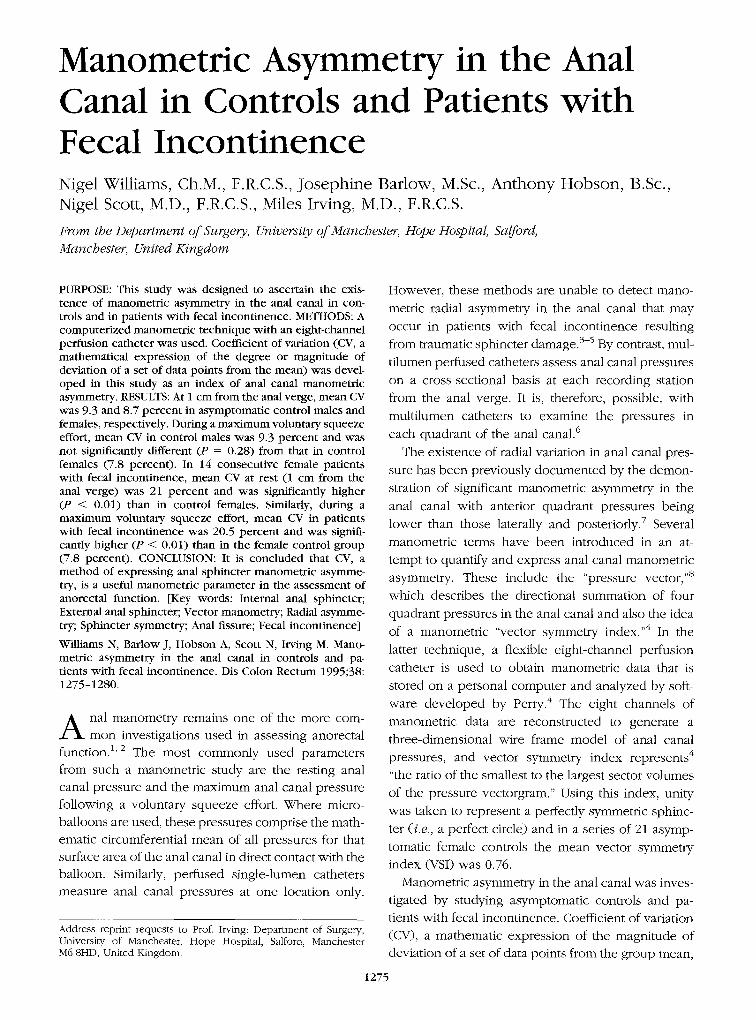
Figure 1. Coefficient of variation along the anal canal in controls (mean _+ SEM).
tients were parous. Two patients had delivered one
child, five had delivered two children, six had deliv-
ered three children, and one patient had delivered
four children. Traumatic delivery was reported by
three patients, two had had forceps-assisted delivery,
and two reported having had an episiotomy to facil-
itate childbirth.
Resting: Male Controls
Mean resting pressure (MRP (SEM)) increased with
decreasing distance from the anal verge and was
highest at 1 cm from the anal verge (61.9 (4.77)
mmHg). CV was highest at 6 cm from the anal verge,
with a mean value of 48.4 percent for the nine male
controls (Table 1). There was a sharp decrease in CV
from 6 to 5 cm, but this failed to achieve statistical significance (t = 1.82; P = 0.11). The incremental
decrease in CV for each 1-cm interval from 5 to 3 cm
was not statistically significant (Fig. 1). Although the
decrease in mean CV from 3 (20 percent) to 2 cm (11.2 percent) appeared large, it was not significant (t =
1.73; P = 0.12). The mean CV then decreased further
to 9.3 percent at 1 cm.
Resting: Female Controls
MRP increased with decreasing distance from the
anal verge so it was highest at 1 cm (63.9 (5.43)
mmHg). Maximum CV was at 6 cm from the anal
verge (mean CV, 41.4 percent) in female controls.
This gradually decreased with decreasing distance
from the anal verge (Fig. 1; Table 1). Although there
was a sharp reduction in mean CV from 6 (41.4 per-
cent) to 5 cm (33.2 percent), this failed to achieve
statistical significance (t = 1.30; P = 0.22). The de-
crease in CV among 5, 4, 3, and 2 cm was not signif-
icant at any station. The lowest value for CV in the
anal canal (8.7 percent) was at 1 cm from the anal
verge and was significantly lower (t = 2.47; P = 0.03)
than that at 3 cm.
V o l u n t a r y S q u e e z e Effor t : C o n t r o l s
Maximum voluntary squeeze pressure (MSP) in
male controls was 188.8 (10.4) mmHg and in female
controls was 142.8 (7.38) mmHg (Table 2). Mean CV
of manometric data during MSP in men was 9.3 (1.27)
percent and in female controls was 7.8 (0.57) percent.
The difference in CV during MSP between male and
female controls was not significant (t = 1.11; P =
0.28).
Resting: Fecal Incontinence
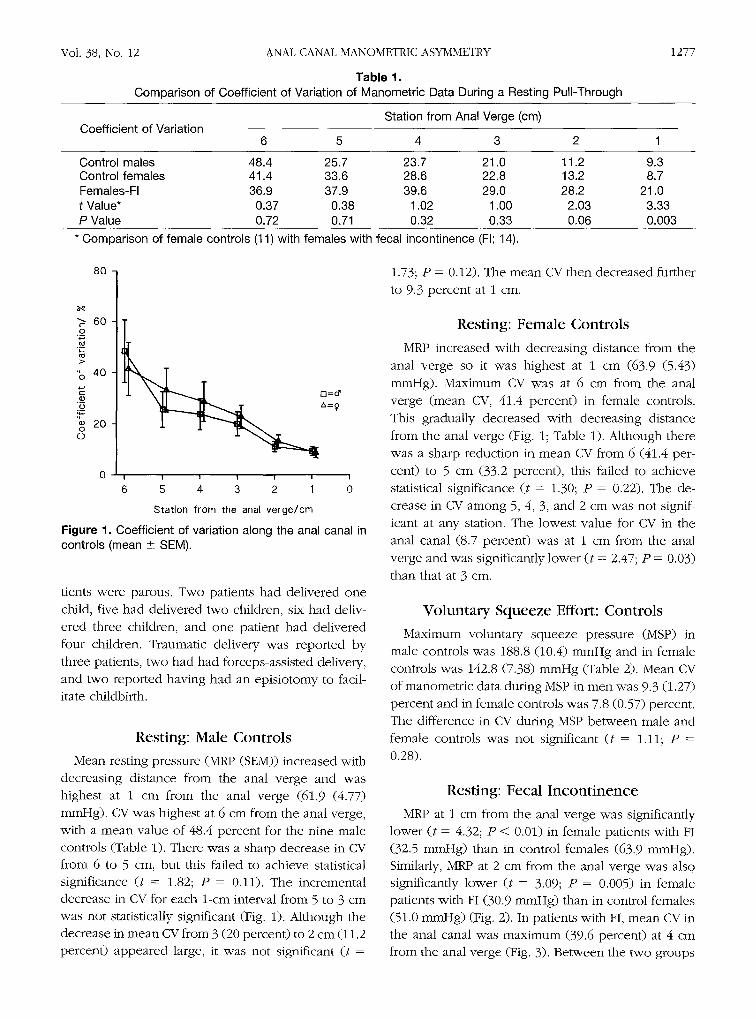
MRP at 1 cm from the anal verge was significantly
lower (t = 4.32; P < 0.01) in female patients with FI
(32.5 mmHg) than in control females (63.9 mmHg). Similarly, MRP at 2 cm from the anal verge was also
significantly lower (t = 3.09; P = 0.005) in female patients with FI (30.9 mmHg) than in control females
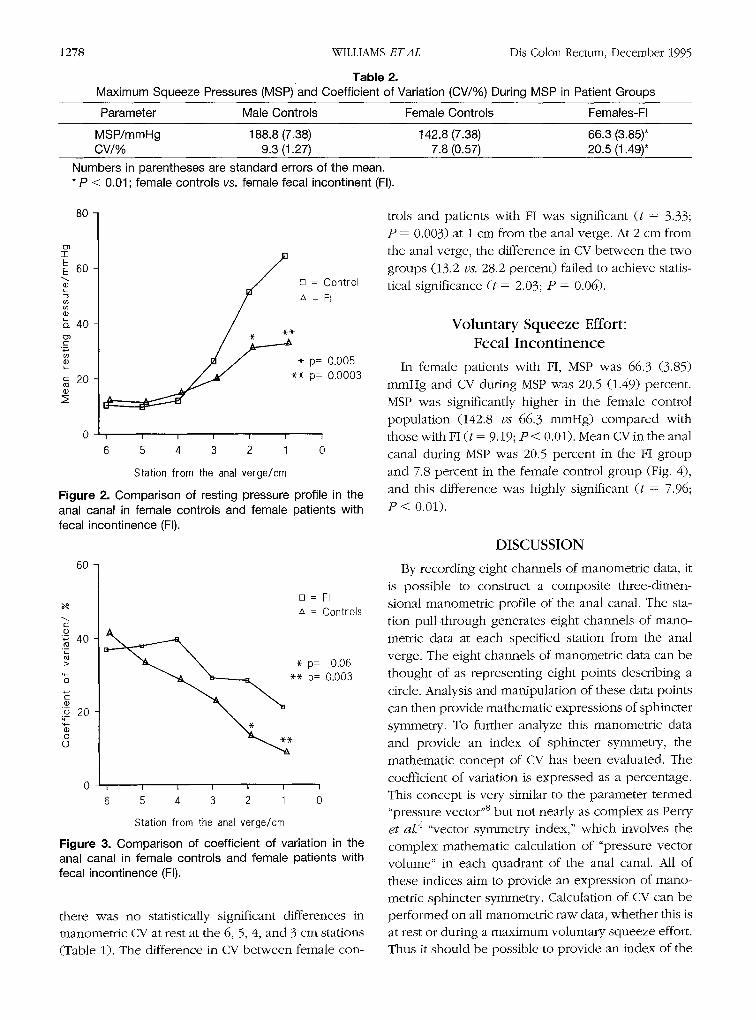
(51.0 mmHg) (Fig. 2). In patients with FI, mean CV in
the anal canal was maximum (39.6 percent) at 4 cm from the anal verge (Fig. 3). Between the two groups
1278 WILLIAMS E T A L Dis Colon Rectum, December 1995
Table 2. Maximum Squeeze Pressures (MSP) and Coefficient of Variation (CV/%) During MSP in Patient Groups
Parameter Male Controls Female Controls Females-FI
MSP/mmHg 188.8 (7.38) 142.8 (7.38) 66.3 (3.85)* CV/% 9.3 (1.27) 7.8 (0.57) 20.5 (1.49)*
Numbers in parentheses are standard errors of the mean. * P < 0.01; female controls vs. female fecal incontinent (FI).
80
(3) T
E E 60
L
e)
b. 40
c
L
c 20 oo �9
~ = Control = FI
* * ~ p= 0.005
*
* p= 0.0003
I I I I I t I
6 5 4 3 2 1 0
Station from the anal verge/cm
Figure 2. Comparison of resting pressure profile in the anal canal in female controls and female patients with fecal incontinence (FI).
60
[] = FI A = Controls
�9 .~ 4o
> * p= 0.06 "6 ~-* p= 0.003
E ._ o 20 �9 0
0 I I I I I I I
6 5 4 3 2 1 0
Station from the anal verge/cm
Figure 3. Comparison of coefficient of variation in the anal canal in female controls and female patients with fecal incontinence (FI).
there was no statistically significant differences in manometric CV at rest at the 6, 5, 4, and 3 cm stations (Table 1). The difference in CV between female con-
trois and patients with FI was significant (t = 3.33; P = 0.003) at 1 cm from the anal verge. At 2 cm from
the anal verge, the difference in CV between the two groups (13.2 vs. 28.2 percent) failed to achieve statis-
tical significance (t = 2.03; P = 0.06).
Voluntary Squeeze Effort: Fecal Incont inence
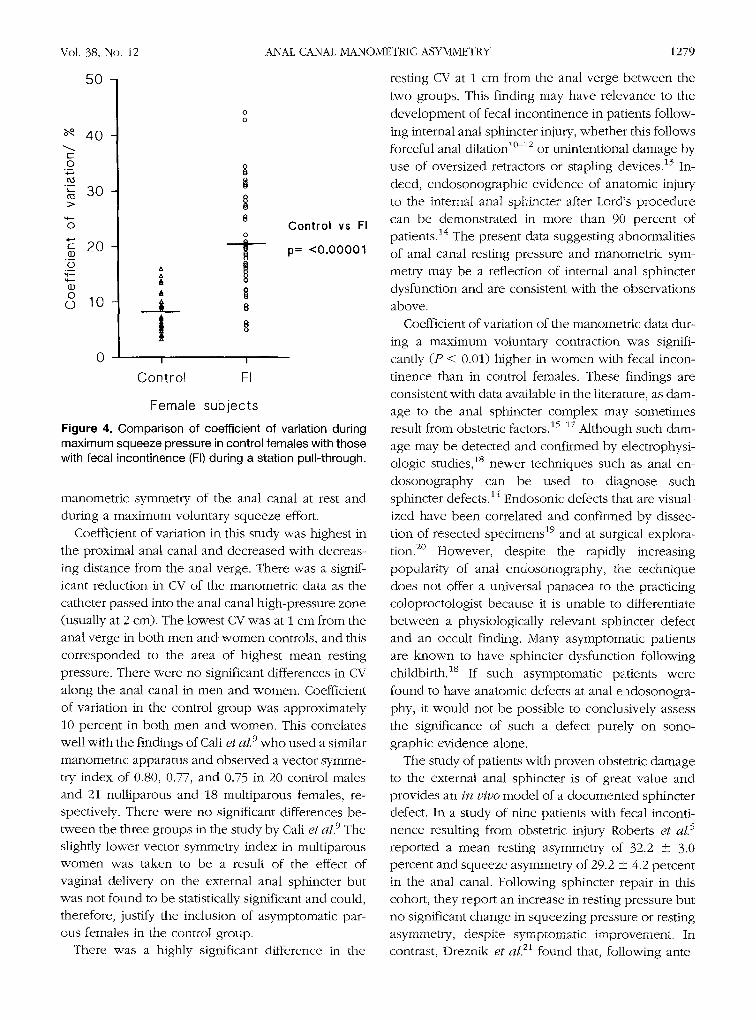
In female patients with FI, MSP was 66.3 (3.85) m m H g and CV during MSP was 20.5 (1.49) percent.
MSP was significantly higher in the female control population (142.8 vs 66.3 mmHg) compared with
those with FI (t = 9.19; P < 0.01). Mean CV in the anal canal during MSP was 20.5 percent in the FI group
and 7.8 percent in the female control group (Fig. 4),
and this difference was highly significant (t = 7.96;
P < 0.01).
DISCUSSION
By recording eight channels of manometric data, it is possible to construct a composite three-dimen-
sional manometric profile of the anal canal. The sta- tion pull-through generates eight channels of mano-
metric data at each specified station from the anal verge. The eight channels of manometric data can be
thought of as representing eight points describing a
circle. Analysis and manipulation of these data points can then provide mathematic expressions of sphincter
symmetry. To further analyze this manometric data and provide an index of sphincter symmetry, the
mathematic concept of CV has been evaluated. The
coefficient of variation is expressed as a percentage. This concept is very similar to the parameter termed "pressure vector ''8 but not nearly as complex as Perry et al. 4 "vector symmetry index," which involves the complex mathematic calculation of "pressure vector volume" in each quadrant of the anal canal. All of
these indices aim to provide an expression of mano- metric sphincter symmetry. Calculation of CV can be performed on all manometric raw data, whether this is at rest or during a maximum voluntary squeeze effort. Thus it should be possible to provide an index of the
Vol. 38, No. 12
5 0
40 c- O
' - 30
0
E 20 �9
O ,+.-
0 �9 10
0
A It A
I I
Cont ro l FI
ANAL CANAL MANOMETRIC ASYMMETRY 1279
resting CV at 1 cm from the anal verge be tween the
two groups. This finding may have relevance to the
development of fecal incontinence in patients follow-
ing internal anal sphincter injury, whether this follows forceful anal dilation 1~>/2 or unintentional damage by
use of oversized retractors or stapling devices. 13 In-
deed, endosonographic evidence of anatomic injury to the internal anal sphincter after Lord's procedure
can be demonstrated in more than 90 percent of Control vs FI patients. 14 The present data suggesting abnormalities
p= <0.00001 of anal canal resting pressure and manometric sym-
metry may be a reflection of internal anal sphincter
dysfunction and are consistent with the observations
above.
Coefficient of variation of the manometric data dur-
ing a maximum voluntary contraction was signifi-
cantly (P < 0.01) higher in w o m e n with fecal incon-
tinence than in control females. These findings a r e
consistent with data available in the literature, as dam-
age to the anal sphincter complex may sometimes result from obstetric factors. 15 17 Although such dam-
age may be detected and confirmed by electrophysi- ologic studies, 18 newer techniques such as anal en-
dosonography can be used to diagnose such sphincter defects. 14 Endosonic defects that are visual-
ized have been correlated and confirmed by dissec-
tion of resected specimens 19 and at surgical explora-
tion. 2~ However, despite the rapidly increasing
popularity of anal endosonography, the technique
does not offer a universal panacea to the practicing coloproctologist because it is unable to differentiate
be tween a physiologically relevant sphincter defect and an occult finding. Many asymptomatic patients
are known to have sphincter dysfunction following childbirth, is If such asymptomatic patients were
found to have anatomic defects at anal endosonogra-
phy, it would not be possible to conclusively assess
the significance of such a defect purely on sono- graphic evidence alone.
The study of patients with proven obstetric damage to the external anal sphincter is of great value and
provides an in v ivo model of a documented sphincter defect. In a study of nine patients with fecal inconti- nence resulting from obstetric injury Roberts et aL 5
reported a mean resting asymmetry of 32.2 -+ 3.0 percent and squeeze asymmetry of 29.2 + 4.2 percent in the anal canal. Following sphincter repair in this cohort, they report an increase in resting pressure but no significant change in squeezing pressure or resting
asymmetry, despite symptomatic improvement. In contrast, Dreznik et al. 21 found that, following ante-
Female subjects
Figure 4. Comparison of coefficient of variation during maximum squeeze pressure in control females with those with fecal incontinence (FI) during a station pull-through.
manometric symmetry of the anal canal at rest and
during a maximum voluntary squeeze effort.
Coefficient of variation in this study was highest in
the proximal anal canal and decreased with decreas-
ing distance from the anal verge. There was a signif- icant reduction in CV of the manometr ic data as the catheter passed into the anal canal high-pressure zone
(usually at 2 cm). The lowest CV was at 1 cm from the anal verge in both men and w o m e n controls, and this
corresponded to the area of highest mean resting
pressure. There were no significant differences in CV
along the anal canal in men and women. Coefficient
of variation in the control group was approximately
10 percent in both men and women. This correlates well with the findings of Call e t aL 9 who used a similar
manometr ic apparatus and observed a vector symme- try index of 0.80, 0.77, and 0.75 in 20 control males and 21 nulliparous and 18 multiparous females, re -
s p e c t i v e l y . There were no significant differences be- tween the three groups in the study by Cali et al. 9 The slightly lower vector symmetry index in multiparous
w o m e n was taken to be a result of the effect of vaginal delivery on the external anal sphincter but was not found to be statistically significant and could, therefore, justify the inclusion of asymptomatic par- ous females in the control group.
There was a highly significant difference in the
1280
rior sphincter reconstruction in 28 patients with ob-
stetric injury, there was an increase in both resting and squeezing pressures "in all quadrants. ''21 They
concluded that "squeeze pressure may not be the
most important determinant of success" and qualified
this with "sphincter profile may also influence out- come to a lesser extent." Similarly, Blatchford et aL 22
performed sphincteroplasty in nine women with doc-
umented obstetric injury to the anal sphincter. Fol-
lowing sphincteroplasty all patients had significant
improvement in continence. More startling, however,
was the change in vector symmetry index before
(VSI = 0.42) and after (VSI = 0.67) sphincteroplasty
(P < 0.005), despite no significant change in resting
or squeezing pressures. The authors concluded that
"sphincter symmetry is an important factor in the
continence mechanism independent of anal canal
pressure."
C O N C L U S I O N S
The discovery of significant anal sphincter mano-
metric asymmetry at rest and during a maximum vol-
untary squeeze effort in patients with fecal inconti-
nence, in this study, represents an important and
interesting finding and adds further credence to the
findings of others that anal sphincter manometric
asymmetry is an important parameter in the assess-
ment of anorectal function. Indeed, the concept of
sphincter symmetry appears to be pivotal in our un-
derstanding of the mechanisms of continence, and
assessment of such a manometric index could prove
to be of benefit in patient management in the future.
REFERENCES
1. Parks TG. The usefulness of tests in anorectal disease. World J Surg 1992;16:804-10.
2. Read NXV, Bannister JJ. Anorectal manometry: tech- niques in health and anorectal disease. In: Henry MM, Swash M, eds: Coloproctology and the pelvic floor. London: Butterworths, 1985:65-87.
3. Coller JA. Clinical application of anorectal manometry. Gastroenterol Clin North Am 1987;16:17-33.
4. Perry RE, Blatchford GJ, Christensen MA, Thorson AG, Attwood SE. Manometric diagnosis of anal sphincter injuries. Am J Surg 1990;159:112-7.
5. Roberts PL, Coller JA, Schoetz DJ Jr, Veidenheimer MC. Manometric assessment of patients with obstetric inju- ries and fecal incontinence. Dis Colon Rectum 1990;33: 16-20.
WILLIAMS E T A L Dis Colon Rectum, December 1995
6. McHugh SM, Diamant NE. Anal canal pressure profile; a reappraisal as determined by rapid pullthrough tech- nique. Gut 1987;28:1234-41.
7. Taylor BM, Beart Jr RW, Phillips SF. Longitudinal and radial variations of pressure in the human anal sphinc- ter. Gastroenterology 1984;86:693-7.
8. Sakaniwa M, Sawaguchi S, Okhawa H, Ikebukuro K. Computerised analysis of anorectal manometry. Prog Pediatr Surg 1989;24:21-32.
9. Cali RL, Blatchford GJ, Perry RE, Pitsch RM, Thorson AG, Christensen MA. Normal variation in anorectal ma- nometry. Dis Colon Rectum 1992;35:1161-4.
10. Lord PH. A new regime for the treatment of haemor- rhoids. J R Soc Med 1968;61:935-6.
11. Hancock BD. Lord's procedure for haemorrhoids; a prospective anal pressure study. Br J Surg 1981;68: 729-30.
12. Snooks SJ, Henry MM, Swash M. Fecal incontinence after anal dilatation. Br J Surg 1984;71:617-8.
13. Molloy RG, Moran KT, Coulter J, Waldron R, Kirwan WO. Mechanism of sphincter impairment following low anterior resection. Dis Colon Rectum 1992;35:462-4.
14. Speakman CT, Burnett SJ, Kamm MA, Bartram CI. Sphincter injury after anal dilatation demonstrated by anal endosonography. Br J Surg 1991;78:1429-30.
15. Deen K1, Kumar D, Williams JG, OlliffJ, Keighley MR. The prevalence of anal sphincter defects in fecal incon- tinence; a prospective endosonic study. Gut 1993;34: 685-8.
16. Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum 1993;36:77-97.
17. Sfrensen M, Tetzschner T, Rasmussen OO, Bjarnesen J, Christiansen J. Sphincter rupture in childbirth. Br J Surg 1993;80:392-4.
18. Snooks SJ, Setchell M, Swash M, Henry MM. Injury to innervation of pelvic floor sphincter musculature in childbirth. Lancet 1984;2:546-50.
19. Sultan AH, Nicholls RJ, Kamm MA, Hudson CN, Beynon J, Bartram CI. Anal endosonography and correlation with in-vitro and in-vivo anatomy. Br J Surg 1993;80: 508-11.
20. Deen KI, Kumar D, Williams JG, Olliff J, Keighley MR. Anal sphincter defects: correlation between endoanal ultrasound and surgery. Ann Surg 1993;218:201-5.
21, Dreznik Z, FleshmanJW, Kodner 1J, Fry RD. Restoration of squeeze pressure with sphincter repair to achieve continence [meeting abstract]. Dis Colon Rectum 1990; 33:P22.
22. Blatchford GJ, Perry RE, Christensen MA, Thorson AG. The effect of sphincteroplasty on manometric vector symmetry [meeting abstract]. Dis Colon Rectum 1990; 33:P22.





























