Embed Size (px)
Citation preview

20 JCN 2014, Vol 28, No 6
CONTINENCE
The International Continence Society (ICS) defines urinary incontinence simply as
‘the complaint of any involuntary leakage of urine’ (ICS, 2005). However, evidence suggests that it is a debilitating condition, which has a significant impact on the physical, emotional and social wellbeing of those affected (Howard and Steggall, 2010). Similarly, urinary incontinence is often under-reported and overshadowed by other conditions regarded as more prominent or urgent.
Moore and Fader (1999) found that although most nurses were aware of the negative impact of incontinence on patients’ quality of life, assessment and treatment was ‘less than optimum’. They suggested that reasons for this could include a lack of understanding about the causes of incontinence, as well as the benefits of even simple nursing interventions.
Managing urinary incontinence: guidelines for community nurses
Most community nurses will see patients with continence problems on a daily basis, even though this may not be the primary problem. For example, elderly patients and those with neurological conditions or diabetes are all at risk of developing bladder or bowel dysfunction.
The National Audit of Continence Care for Older People (Wagg et al, 2010) found that older people were more likely to receive an incontinence pad assessment rather than a detailed continence assessment. Although the provision of containment products may be an appropriate management option, it should not be the first step.
This article will outline basic bladder function, detail the causes and types of urinary incontinence, and explore the role of the community nurse in assessment and management.
BLADDER FUNCTION AND CAUSES OF INCONTINENCE
The urinary bladder is a hollow
muscular organ located in the pelvis. Its two major functions are the storage and emptying of urine. For continence to be maintained, there is a requirement for: Effective functioning of the
bladder sphincter mechanism and pelvic floor muscles
Effective functioning of the autonomic nervous system, micturition centres in the brain, and locomotor skills.
Janice Reid, continence services manager,Western Health and Social Care Trust, Londonderry
Increasing demographic changes in the type and age of patients as well as further government directives requiring more care at home, mean that there is a growing emphasis on primary care-led services. Large caseloads and patients with multiple and chronic health problems are stretching available community nursing resources. Against this background, continence promotion tends not to be a priority and at times it may seem easier and better to prescribe pads for patients with urinary incontinence. This article provides community nurses with guidance on the initial assessment and management options available for patients who present with urinary incontinence. Many patients will subsequently experience improvement in their symptoms (although not always complete resolution), with a corresponding improvement in overall quality of life.
KEYWORDS:Continence Assessment Urinary incontinence Management
Janice Reid
THE SCIENCE — CAUSES OF URINARY
INCONTINENCE
According to the NHS, the causes of urinary incontinence depend
on the type of incontinence experienced, for example: Stress incontinence: often
the result of a weakening or damage to the muscles that prevent urination, including pelvic floor muscles and the urethral sphincter
Urge incontinence: often caused by overactivity of the muscles that control the bladder (detrusor muscles)
Certain factors increase the chances of the development of urinary incontinence — pregnancy and vaginal birth; obesity; a family history of incontinence; and increasing age (although incontinence must not be regarded as an inevitable consequence of ageing).
Source: http://www.nhs.uk
Cre
dit:
Joe
Penn
a @
flick
r.com
http
s://c
reat
ivec
omm
ons.
org/
licen
ses/
by/2
.0/
Reid - continence - read by JBBBM.indd 2 04/12/2014 19:21
© 2014
Wou
nd C
are P
eople
Ltd

GREAT BEAR®
H E A LT H C A R E
JCNADVERTGBLSDEC14
New Product Sample Request
Name: ................................................................................
Address: ............................................................................
...........................................................................................
Phone Number: .................................................................
Email: ................................................................................
Please indicate sample required:
GB Libra Sheath Standard �Size: (24mm/28mm/31mm/35mm/40mm)
GB Libra Sheath Pop On �Size: (24mm/28mm/31mm/35mm/40mm)
GB Libra Sheath Wide Band �Size: (24mm/28mm/31mm/35mm/40mm)
GB Soft Skin Barrier Wipe �
Return to: Marketing Department, FREEPOST RRKC-BRRB-AZCG, Great Bear Healthcare,1 Lambourne Crescent, Cardiff Business Park, Llanishen, Cardiff, CF14 5GF
Available in 3 styles: Standard,Pop On and Wide Band in arange of sizes
Can be used with our GB Soft Skin Rangeof Adhesive Remover and Barrier Wipes
JCN Ad V2 12/14:Layout 1 3/12/14 15:13 Page 1
© 2014
Wou
nd C
are P
eople
Ltd

?? JCN 2014, Vol 28, No 5
CONTINENCE
22 JCN 2014, Vol 28, No 6
If any of the above requirements are compromised, there is a risk of urinary incontinence (Getliffe and Dolman 2007; Nazarko 2007). Therefore, factors that are likely to lead to incontinence include neurological conditions such as multiple sclerosis, spinal cord injury, Parkinson’s disease, and stroke or diabetic neuropathy, as well as so-called ‘mechanical’ problems including enlarged prostate gland, constipation, defective urethral sphincter or pelvic floor muscle weakness. Certain pharmacological therapies, such as sedatives and diuretics, can also result in urinary incontinence.
In addition, there are a number of other issues that can impact on a person’s ability to respond to the urge to void the bladder. For example, impaired mobility and/or dexterity allied to cognitive problems can also increase the risk of incontinence, as can urinary tract infections or poor fluid intake (Nazarko, 2013).
Types of urinary incontinenceUrinary incontinence is normally classified on the basis of symptoms as outlined in Table 1, and includes stress, urge, mixed, functional and passive/reflex incontinence.
ASSESSMENT
The purpose of a continence assessment is to: Identify the nature and extent of
the continence problem Gather information that will aid
It is important for the assessing nurse to ensure questions are being asked in such a way that the patient will understand. This means avoiding jargon or unnecessarily complicated medical terminology.
However, as Getliffe and Dolman (2007) point out, such forms are only intended as guidance and a certain level of knowledge, skill and sensitivity is needed to ensure holistic assessment. Completed forms provide a data source for audit purposes, as well as allowing comparisons between baseline information obtained at the initial assessment and subsequent treatment outcomes (Getliffe and Dolman, 2007).
HistoryIt is important for the community nurse to allow the patient to describe the nature and extent of the continence problem, as well as the impact that it is having on his or her daily life. Discussion around medical and surgical history — including female obstetric history if relevant — may help to identify any predisposing factors that could contribute to urinary incontinence such as neurological conditions or previous pelvic surgery.
Urinary symptomsAlong with the information obtained from the history, asking trigger questions as detailed in Table 2 will assist the community nurse to make
accurate diagnosis and help plan treatment and care
Provide a baseline for monitoring progress
Identify factors that require the patient to be referred for additional investigation and treatment.
Several guidance documents have been produced over the years, most notably by the Department of Health (DH) and National Institute for Health and Care Excellence (NICE), detailing key points to be included in an initial continence assessment (DH, 2000; NICE, 2010; 2013). Most healthcare organisations will have developed local assessment forms for the community nurse to use based on this guidance, and examples of typical questions are listed in Table 2.
Table 1: Classification of types of incontinence
Symptoms Type of incontinence
Leakage with coughing, sneezing, physical exertion or exercise. Can be caused by weak pelvic floor muscles, which no longer support the bladder neck. Common during and after pregnancy. Less common in men — may occur after prostate surgery.
Stress (in the context of urinary incontinence the word stress is a mechanical term relating to pressure on the pelvic floor muscles, not emotional stress)
Leakage after sudden intense uncontrollable urge to pass urine. Feeling of needing to frequently void, day and night. Caused by bladder contractions during filling phase.
Urge
A combination of stress and urge symptoms. Mixed
Chronic urinary retention — likely to cause symptoms similar to stress and urge incontinence, plus may cause feeling of incomplete bladder emptying. Can be caused by faecal impaction, enlarged prostate gland in men, or a neurological condition.
Overflow
Environmental/mobility/dexterity factors can affect a person’s ability to reach toilet in time, resulting in leakage of urine.
Functional
Incontinence without warning day or night, or for no obvious reason.
Passive/reflex
Table 2: Examples of typical questions that could be asked in an initial continence assessment of a patient presenting with urinary incontinence1. Ask the patient to describe in his/her own words the bladder problems he/she is having.
2. Ask how long has this been a problem.
3. Ask if there are any other medical conditions? (Also ask about any surgical procedures and menstrual/obstetric history if relevant.)
4. Ask about urinary symptoms: Do you leak urine when you laugh, cough or sneeze? How long can you hold on when you get the desire to pass urine? How often do you need to pass urine? Do you have to get up during the night to go to the toilet? Do you ever leak urine before reaching the toilet? Do you know when you have leaked urine? Do you have any pain or discomfort when passing urine? Have you ever noticed any blood in
your urine?
5. Ask about the patient’s normal bowel habit.
6. Ask about any medication the patient may be taking — both prescribed and purchased.
Reid - continence - read by JBBBM.indd 4 04/12/2014 19:21
© 2014
Wou
nd C
are P
eople
Ltd

General Enquiries & Student SupportCall: +44 (0)1926 493313Email: [email protected]
© 2014
Wou
nd C
are P
eople
Ltd

CONTINENCE
24 JCN 2014, Vol 28, No 6
Answer the following questions about this topic, either to test the
new knowledge you have gained or to form part of your ongoing practice
development portfolio.
1 – What are the common symptoms of urinary incontinence?
2 – Can you name some of the main differences between stress and urge incontinence?
3 – Can you name five important questions to ask as part of a urinary continence assessment?
4 – What is the importance of cognitive awareness in urinary incontinence?
5 – Can you explain the relevance of urinary tract infection when assessing urinary incontinence?
Five-minute test
a comprehensive assessment of the person’s urinary symptoms and allow a provisional diagnosis to be made (see Table 1 for classification of symptoms).
Normal bowel habitBowel habits vary between individuals (Kyle and Prynn, 2007) and, therefore, it is important for nurses to ascertain what patients consider to be normal for them in order to assess if they are at risk of constipation and subsequent urinary symptoms. For example, a rectum loaded with impacted faeces can disrupt the flow of urine from the bladder, resulting in incomplete emptying and possible overflow incontinence (Getliffe and Dolman, 2007).
MedicationIt is important for the community nurse to be aware that many common medications can increase the risk of bladder problems and/or urinary incontinence. As Nazarko (2008) points out, the use of sedatives can affect patients’ cognitive awareness and their ability to recognise the need to pass urine. Similarly, the anticholinergic (a substance that inhibits parasympathetic nerve
existing toilets are safe and accessible to use. For example, reduced or poor mobility can affect timely access to the toilet; similarly, problems with dexterity can affect the person’s ability to perform intermittent self-catheterisation, or adjust zips and buttons on clothing, which can delay their access to a toilet.
Quality of life An important part of the assessment is to determine what impact any urinary incontinence has had on the person’s quality of life. There are many quality of life measuring tools in the literature but, as Getliffe and Dolman (2007) point out, where such a tool is to be used on a regular basis, it is sensible to choose one which is straightforward and quick to use. For example, a simple question could be, ‘How bothersome are your urinary symptoms on a scale of 1–5, where 1 equals “not very” or “not at all” and 5 equals “intolerable”?’
A simple question like this can be repeated at subsequent reviews to monitor progress and establish a baseline measurement of any continence issues.
Urinary tract infection A urinary tract infection can precipitate or exacerbate urinary incontinence and, therefore, it is important that the initial assessment of any patient presenting with urinary incontinence should include a reagent strip urinalysis to test for
impulses) effects of antidepressants can cause voiding problems, leading to urinary retention with overflow incontinence and the risk of urinary tract infections (British Medical Association [BMA]and the Royal Pharmaceutical Society of Great Britain [RPS], 2014). In addition, constipation can be caused by the use of some analgesics (Kyle and Prynn, 2007).
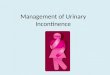
Other factors to considerAny answers to the questions contained in Table 2 should enable the nurse to begin formulating a provisional diagnosis of the type of incontinence the patient may have. However, there are several other factors that need to be considered to complete the assessment and decide on appropriate treatment options. Figure 1 illustrates these factors, which will be discussed below in more detail.
Cognitive awareness Impaired cognitive awareness can affect a person’s ability to remain continent. For example, as Kennedy (2007) points out, the patient may be unable to locate the toilet or identify what it is for; or may come away from the toilet before finishing due to a limited concentration span.
Mobility and dexterityQualified community nurses are often highly skilled in assessing the mobility, dexterity and environment of patients in their care to ensure that
Environmental assessment
Visual examination of skin/perineum
Urinalysis
Cognitive awareness
Quality of life assessment
Onward referral if required
Mobility and dexterity
Assessment of bladder diary
FACTORS TO CONSIDER
AS PART OF CONTINENCE ASSESSMENT
Figure 1.Elements that community nurses should consider as part of a continence assessment.
Reid - continence - read by JBBBM.indd 6 04/12/2014 19:21
© 2014
Wou
nd C
are P
eople
Ltd

JCN 2014, Vol 28, No 6 25
CONTINENCE
leucocytes and nitrites. The presence of leucocytes and nitrites in a patient also experiencing symptoms including dysuria, urgency and frequency is likely to indicate a urinary tract infection. This should be confirmed by laboratory testing to determine the most suitable antibiotic treatment (Moore and Fader, 1999). A result positive for leucocytes and nitrites in the absence of the symptoms mentioned above should not normally be treated with antibiotics (DiVito, 2014).
Bladder diaryAnother valuable element of the continence assessment is the completion of a three-day bladder diary or frequency/volume chart (NICE, 2013). A typical diary will record the frequency, volume and times of urine passed, along with the type, amount and times of fluids consumed over each 24-hour period. Episodes of urinary leakage can also be recorded.
Information contained in the diary will help community nurses form a diagnosis, as well as detailing the patient’s voiding patterns, amount and timing of incontinent episodes, fluid intake and output volumes, and the types of fluid being consumed. This information can then be used as part of the patient’s treatment plan, which might include, for instance, bladder re-training in those with urge incontinence — the aim being to increase the length of time between micturition (by training the individual to ‘hold on’).
The nurse should explain the importance of the bladder diary to the patient and give advice and support where necessary on how to complete it correctly.
With the consent of the patient, the community nurse can also perform a visual assessment of the skin integrity in the perineal and rectal areas to check for evidence of excoriation, dry fragile tissues or vaginal prolapse in females, which would require specialist onward referral. In some cases, digital rectal examination may be appropriate if there are concerns that constipation is contributing to the person’s
incontinence issues (Royal College of Nursing [RCN], 2012).
MANAGEMENT
Once completed, the information gained from a thorough continence assessment will assist the community nurse in identifying the problems causing urinary incontinence, whether they are a result of bladder dysfunction, or other associated problems (Nazarko, 2008).
Management options can then be considered and discussed with the patient. Treating reversible causes such as urinary tract infections can improve symptoms relatively quickly (Leaver, 2011). Also, implementing lifestyle changes, including adjusting fluid intake and avoiding ‘just-in-case’ toilet visits to treat urge incontinence can be beneficial. This is because voiding simply as a precaution means the bladder becomes used to holding less urine and increases its sensitivity, leading to urinary frequency.
Likewise, functional incontinence can be effectively managed by improving toilet access, for instance.
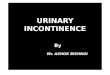
Figure 2 provides an algorithm of non-containment treatment options for the types of urinary incontinence commonly seen by community nurses — these involve looking at other options for management apart from containment with pads, pants or sheaths.
If patients do not improve or are assessed as requiring a more complex level of treatment, the community nurse should refer on to the continence nurse specialist for further investigation and management.
As Nazarko (2013) correctly points out, it is not possible for continence to be promoted successfully in every patient and, therefore, the outcome of the assessment may be to prescribe absorbent containment products. However, the latest NICE guidance on management of urinary
Figure 2.Algorithm of non-containment treatment options.
Stress urinary incontinence• Lifestyle advice, e.g. smoking
cessation, weight loss advice, fluid management
• Pelvic floor exercises leaflet
• Onward referral to continence advisory service/physiotherapy
Urge incontinence • Exclude treatable causes
• Lifestyle advice
• Leaflet on bladder retrainingand pelvic floor exercises
• Onward referral to continence advisory service
Overflow incontinence
• Determine cause and treat if appropriate, e.g. constipation
• Advice on voiding technique
• Refer to continence advisory service for bladder scan and further management
Functional incontinence
• Provision of aids/equipment, e.g. bedside commodes, urinals, night lights
• Adaptive clothing
• Occupational therapy referral if appropriate
Mixed incontinenceTreat the most bothersome
symptom first
URINARY INCONTINENCE Non-containment treatment/management algorithm
for community nurses
Reid - continence - read by JBBBM.indd 7 04/12/2014 19:21
© 2014
Wou
nd C
are P
eople
Ltd

26 JCN 2014, Vol 28, No 6
CONTINENCE
incontinence in women states that ‘absorbent products, hand-held urinals and toileting aids should not be considered as treatments for urinary incontinence’. The guidance further states that these should be used only as (NICE, 2013): A ‘stop-gap’ strategy while the
patient awaits definitive treatment An addition to other
ongoing therapy For the long-term management
of urinary incontinence only after other treatment options have been explored and excluded. Any community nurse should
have access to local guidance on the range of absorbent products available (or can consult a continence specialist nurse), but as Cottenden et al (2005) highlight, it is important to consider several key elements as part of product selection. Generally speaking, the frequency, volume and flow rate of the person’s urinary incontinence influences product choice and it is sensible to try a smaller, more discreet product in the first instance.
However, the person’s daily activities may influence the choice of product, for instance, a person who enjoys sport may require a different product to a person who is largely sedentary. It may also be appropriate to provide different absorbencies for daytime and overnight use, for example, a high-absorbency pad can be left in place overnight to facilitate undisturbed sleep. It is also important to consider the person’s level of mobility and dexterity and whether carer assistance is required to change a product.
Reusable or washable products may also be an option, but the nurse must consider if the person responsible for doing the laundry has the ability and facilities to cope.
Other containment options include the use of urinary sheaths for male patients. There are a wide range of sizes and lengths now available and it is important that the patient is measured and sized accurately and that this device is fitted correctly.
Indwelling urinary catheters may also have a place in the management of intractable incontinence, particularly where there is damage to the skin. This should always be discussed with the continence specialist nurse.
CONCLUSION
With increased demographic changes meaning that patients are living longer, coupled with government directives shifting the emphasis of healthcare provision to primary care services, the role of the community nurse has changed significantly in recent years (Oldman, 2014). Large caseloads and patients with multiple chronic health problems are combining to stretch nursing resources and, unfortunately, continence promotion tends not to be a priority. As Nazarko (2013) points out, it is often easier for clinicians to prescribe pads for patients with urinary incontinence.
However, continence remains a crucial area of expertise for community nurses. This article provides guidance on the initial assessment and management options for patients who present with urinary incontinence. With appropriate assessment and management from community nurses, many patients will experience improvement — if not always resolution — of their symptoms, with a corresponding improvement in overall quality of life. JCN
REFERENCES
BMA/RPS (2014) British National Formulary. BMA/RPS, London
Cottenden A, Bliss D, Fader M, et al (2005) Management with continence products. In: Abrams P, Cardozo L, Khoury S, Wein A (eds). Incontinence. Health Publications, Paris: pp149–253
DH (2000) Good Practice in Continence Services. NHS Executive, London
DiVito M (2014) Management of urinary
tract infection (UTI) in the community. J Comm Nurs 28(3): 18–26
Getliffe K, Dolman M (2007) Assessing bladder function. In: Getliffe K, Dolman M (eds). Promoting Continence – A Clinical and Research Resource. 3rd edition. Elsevier, Edinburgh
Howard F, Steggall M (2010) Urinary incontinence in women: quality of life and help-seeking. Br J Nurs 19(12): 742–49
ICS (2005) Evaluation and Treatment of Urinary Incontinence, Pelvic Organ Prolapse and Faecal Incontinence. Available at: www.ics.org/Publications/ICI_3/v2.pdf/summary.pdf (accessed 11 November, 2014)
Kennedy M (2007) Vulnerable groups – mental health needs. In: Getliffe K, Dolman M (eds). Promoting Continence – A Clinical and Research Resource. 3rd edition. Elsevier, Edinburgh
Kyle G, Prynn P (2007) Bowel care. In: Getliffe K, Dolman M (eds). Promoting Continence – A Clinical and Research Resource. 3rd edition. Elselvier, Edinburgh
Leaver RB (2011) Essential guide to urinary incontinence Pract Nurs 41(8): 33–6
Moore K, Fader M (1999) Promoting continence in the community. Br J Comm Nurs 4(1): 36–43
Nazarko L (2007) Continence problems following stroke. Nurs Res Care 9(4): 152–5
Nazarko L (2008) A guide to continence assessment for community nurses. Br J Comm Nurs 13(5): 219–26
Nazarko L (2013) Continence series 4: the importance of assessment. Br J Healthcare Assistants 7(3): 118–24
NICE (2010) Lower Urinary Tract Symptoms: the management of lower urinary tract symptoms in men. Available at: www.nice.org.uk/guidance/cg97 (accessed 11 November, 2014)
NICE (2013) Urinary Incontinence: the management of urinary incontinence in women. Available at: www.nice.org.uk/guidance/cg171 (accessed 11 November, 2014)
Oldman C (2014) Game plan. Primary Health Care 24(6): 13
RCN (2012) Management of Lower Bowel Dysfunction Including DRE and DRF. Available at: www.rcn.org.uk/__data/assets/pdf_file/0007/157363/003226.pdf (accessed 11 November, 2014)
Wagg A, Harari D, Husk J, et al (2010) National Audit of Continence Care for Older People. Available at: www.rcplondon.ac.uk/projects/national-continence-audit-reports (accessed 11 November, 2014)
Red Flag Absorbent pads
Be wary of overusing absorbent products like incontinence pads — these should only be regarded as a ‘stop-gap’ strategy while the patient awaits definitive treatment options.
Reid - continence - read by JBBBM.indd 10 04/12/2014 19:22
© 2014
Wou
nd C
are P
eople
Ltd