Embed Size (px)
Citation preview
Liege Lourenço-Matharu Nov 2016
Managing the anxious child and sedation for dental paediatric patients
A
D A

Aims and objectives
An overview on management of anxious children receiving dental treatment with or without sedation





Different Child - Different Plan
Behaviour management
• Key factor in providing dental treatment • Based on empathy, child’s well being and best interest • Varied techniques - accepted legally in different
cultures and philosophies • Ongoing learning process throughout our professional
lives
The child and parents
• Attend equipped with learning set of behaviours to cope with situations
• These behaviours will be used in a dental setting
• Some will be helpful, some will make dental treatment difficult
• Parents unrealistic expectations
If only we were magicians or had crystal balls!!
Behaviour Management Techniques
Tell-show-do Modeling
Distraction Pain control
Parents in or out Empathy
Voice-control Stop sign
Positive reinforcement Time out
When all the above fails…
• Take in consideration treatment needed.
• Is it urgent or can it be stabilised?
• Can pain be managed so to give respite?
• Can treatment be attempted under IS?
• Can treatment be carried out under IV?
• Can treatment be carried out under IN?
• Can the treatment be carried out by OS?
• Should the treatment be carried out under GA?

Sedation
• Poswillo Report (1990) - recommendations to use sedation in preference to GA
• Historically, nitrous oxide has been the technique of choice in the UK
• Little advance in conscious sedation for children has happened since then
Systematic Review
• 65 studies included
• More than 19 agents and combinations
• 37% all studies used supplemental N2O/O2
• 48% studies used papoose-boards
• Modes: oral, sub-mucosal, intranasal, rectal, intravenous, intramuscular, inhalational
Systematic Review
• Over 8 groups of drugs used worldwide for conscious sedation in children
• N2O, benzodiazepines, antihistamines, propofol, opioids, alcohols, barbiturates and ketamine
• Multi-pharmacy increasing the risk of over-sedation or GA
Agents used for children
• Chloral hydrate and hydroxyzine
• Used in the majority of the studies in the USA alone or in combination plus other agents, including nitrous oxide and papoose-board

Agents used for children
Propofol (Anaesthetic induction)
• Needs operator/anaesthetist
• Continuous infusion or operator
controlled infusion and patient
controlled infusion
• Not licensed for use in children
Agents used for children Ketamine
• 10 studies: USA (4), South Africa (3), Norway (1), India (2): 7 oral, 2 rectal and 1 intranasal
• Analgesia, sedation and amnesia
• Side effects: nausea, vomiting, hypersalivation, and agitation/hallucinations (emergence phenomena) less commonly in children

Agents used for children
Sevoflurane – (2 studies)
• Pleasant to inhale, non-irritant
and non-pungent
• Non-polluting
• Needs a calibrated vaporiser
attached to the N2O machine
• Carried out by operator and anaesthetist
Agents used for children
Midazolam • More than 35 studies • Alone or in combination • Oral (13), IV (3), IN (9), IM (1), Submucosal (4) and
rectal (5) • Dosages ranging from 0.2 to 0.7 mg/kg
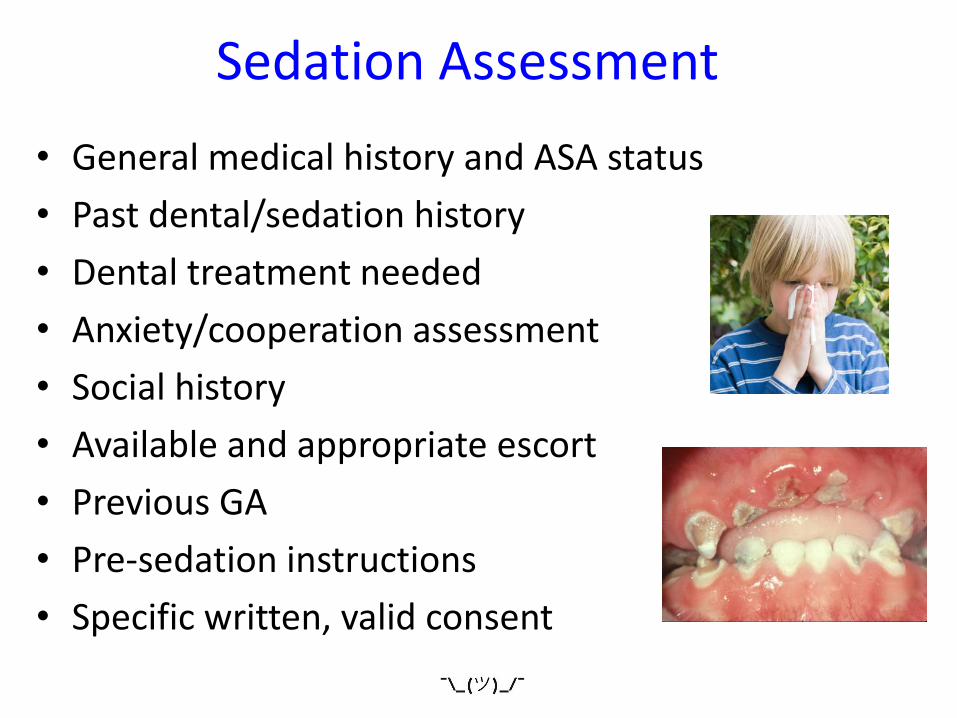
Which sedation? • General medical history and ASA status
• Past dental/sedation history
• Dental treatment needed
• Anxiety/cooperation assessment
• Social history
• Available and appropriate escort
• Previous GA
• Pre-sedation instructions
• Specific written, valid consent
Sedation Assessment

Inhalation Sedation
Nitrous Oxide
Indications for Inhalation Sedation
• Mildly anxious children
• Unpleasant procedure
• Medically compromised
• Needle phobia
• Gag reflex
• Other sedation methods contra-indicated
• Alternative to GA
Contra-indications to IS
• Relative contra-indications • Acute and chronic nasal obstruction • 1st trimester of pregnancy • Inability to co-operate or understand
• Absolute contra-indications • Inability to breathe nasally with open mouth • Very severe myasthenia gravis & MS • Very severe chronic obstructive airways
disease • Nasal or facial deformity • Psychiatric disorders & nasal hood phobia
Preparation for IS Sedation
• Parents may attend with other children
• Child must attend with a responsible adult
• Child should be fit and well on the day
• Child able to breath through the nose
• Light meal before appt
• Should take medication at usual time

Quantiflex MDM
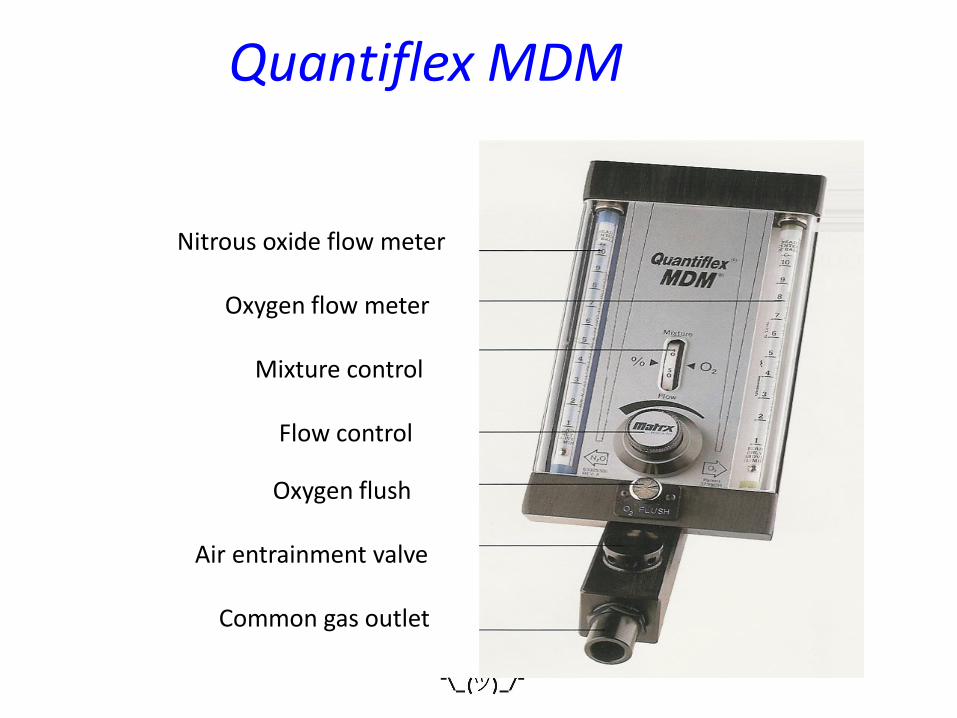
Quantiflex MDM
Nitrous oxide flow meter Oxygen flow meter Mixture control Flow control
Oxygen flush Air entrainment valve Common gas outlet
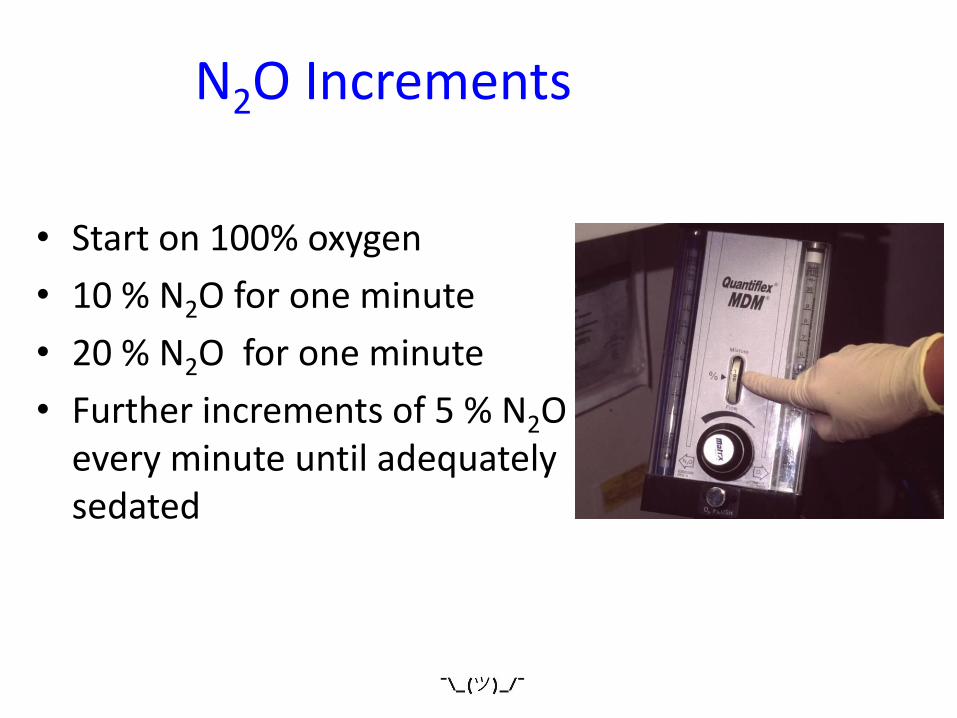
N2O Increments
• Start on 100% oxygen
• 10 % N2O for one minute
• 20 % N2O for one minute
• Further increments of 5 % N2O every minute until adequately sedated

Clinical Technique
• Calming mono-tonal voice
• Imagery/visualisation
• Muscle relaxation techniques
• Semi-hypnotic suggestion
• Music
• Ceiling pictures/artwork
• Dimmed lights
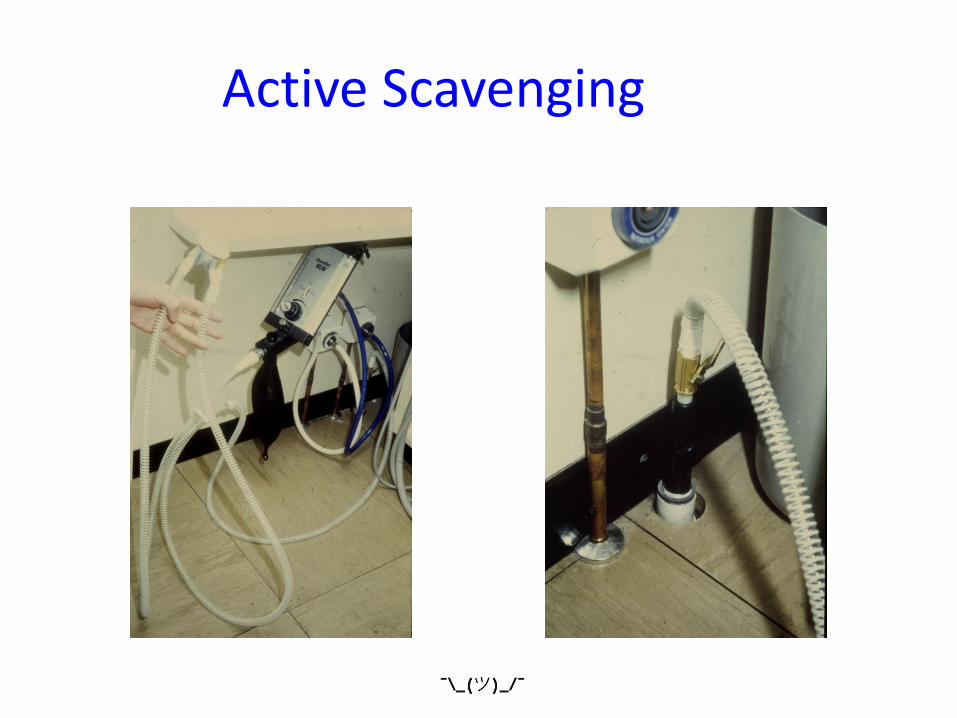
Active Scavenging
Midazolam: IV, IN and OS
• Calms the patient, relaxes skeletal muscles, produces anxiolytic and sedative-hypnotic effects
• Anterograde amnesia
• It is also an anticonvulsant
• In children these effects are similar to those seen in adults
Midazolam: undesirable
• Respiratory depression: muscle relaxant and reduced sensitivity of CNS chemoreceptors
• CV effects: small fall in arterial BP compensated by baroreceptor reflex: (increase pulse rate) - no clinical significance
• It may paradoxically show increased aggression, irritability and anxiety
Midazolam: Indications
• Moderate to severe anxiety
• A movement disorder or a physical,
mental or learning disability
• An increase gag reflex
• An unpleasant or complicated procedure
Midazolam: Contraindications
Relative:
• High BP (very rare in children)
• Alcohol or narcotics dependency
• Recreational drug use
• Impairment of renal or hepatic function
• No escort/or with other children
Midazolam: Contraindications
Absolute:
• Allergy to benzodiazepines
• Pregnancy and breast feeding
• Untreated severe psychiatric disease
• ASA IV and V

Midazolam: Reversal
Flumazenil:
• Benzodiazepine
• Antagonist at the receptors
• Greater affinity for the BDZ receptor displaces MDZ
Sedation clinic
Methods for IV
• IV Information leaflet is given
• Emla/Ametop tube and patches are given to patient to place1 hr before appointment
• Consent is taken and appointment arranged
Preparation for IV Sedation
• Parents must not attend with other children
• Child must attend with a responsible adult • Child should be fit and well on the day • Light meal before appt • Should take medication at usual time • Not use public transport to go home
Methods
• Pulse oximeter and clinical monitoring throughout treatment and recovery
Methods
• Baseline, intra-operative, post-operative and discharge BP are recorded
IV
Methods
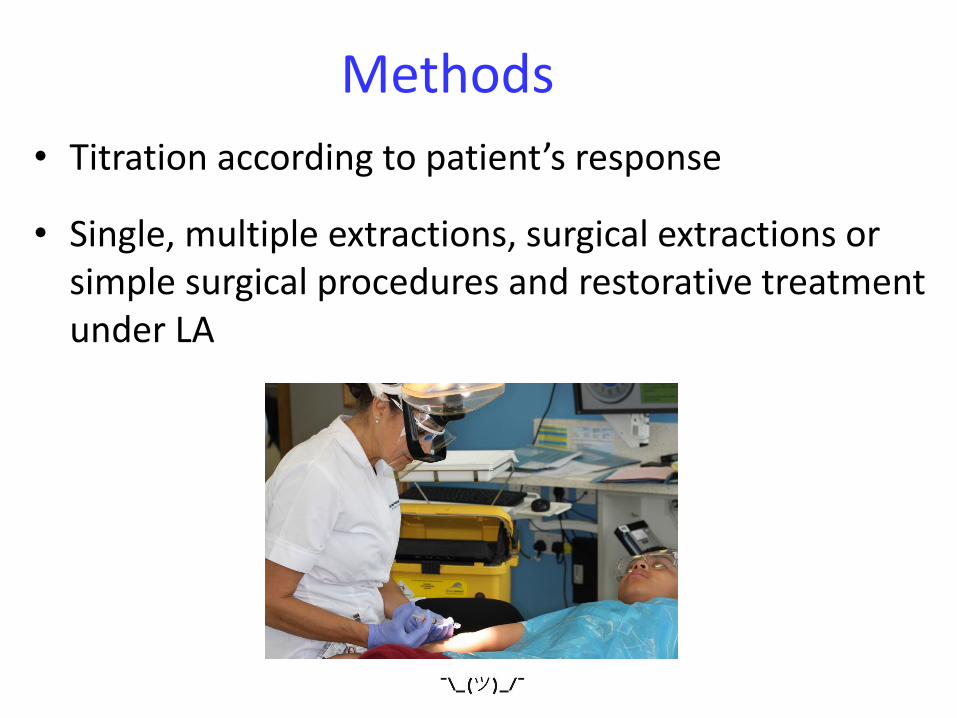
• Titration according to patient’s response
• Single, multiple extractions, surgical extractions or simple surgical procedures and restorative treatment under LA
Preparation for Oral Sedation
• Parents must not attend with other children • Child must attend with a responsible adult • Child should be fit and well on the day • Light meal 4 to 6 hours before appt • Should take medication at usual time
• Not use public transport to go home
Oral Sedation
• MDZ is given as a flavoured syrup after weight of the child is taken
• Child is encouraged to go to the toilet
• Child is taken to a play area under supervision
• After 10 to 15 minutes parents bring the child to the dental chair
Oral midazolam
Weight - less than 30 kg - max 10mg
Midazolam 0.5 mg/kg is given orally
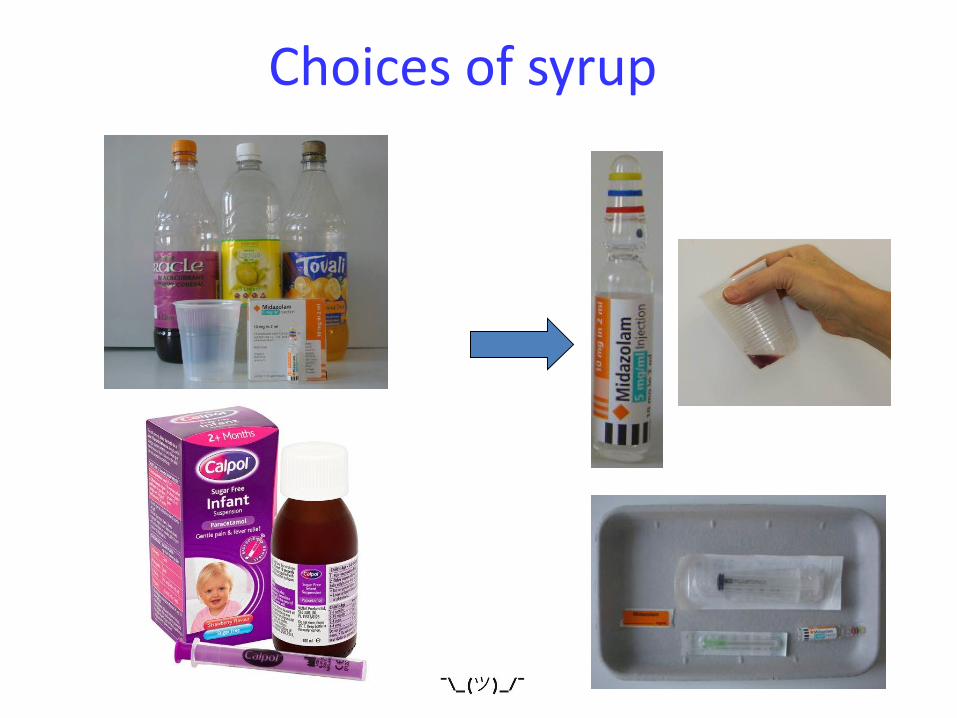
Choices of syrup

Administration
Monitoring

Recovery Play Area
• Patient is taken to recovery • Monitored by one member of
the team • Post-op/sed information given • Patient is discharged when alert
and responsive
Preparation for IN Sedation
• Parents must not attend with other children
• Child must attend with a responsible adult
• Child should be well and have unblocked nose
• Light meal 4 to 6 hours before appt
• Should take medication at usual time
• Not use public transport to go home
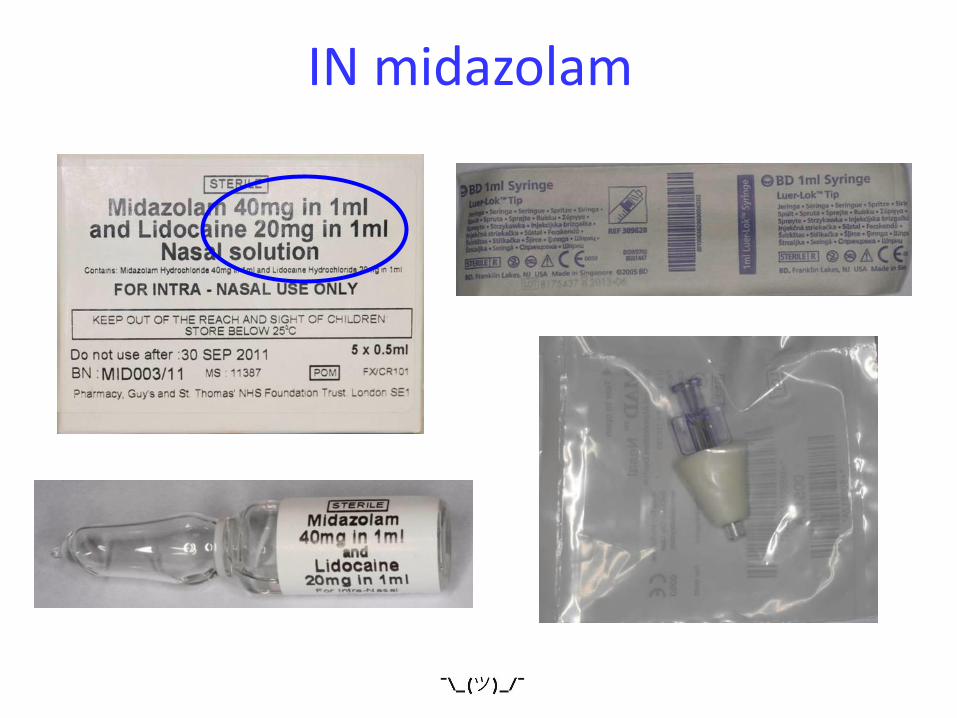
IN midazolam
IN - Weight
Midazolam 0.2 mg/kg, intranasally

IN - Administration
IN
Side-effects
• Diplopia
• Hiccups
• Vomiting
• Crying in recovery
• Agitated in recovery
• Lip biting
• Passing water

Recommendations to practice
• The report from the standing committee for sedation classified midazolam sedation for subjects under 12 years as an ‘alternative technique’
• A total of 100 cases of IV or IS sedation over the previous two years are recommended
• Training must be supported by four years of post-registration experience as a dental practitioner in the UK
Follow guidelines
• BSPD: “A Policy Document on Sedation for Paediatric Dentistry”, 1996
• A Conscious Decision: A review of the use of GA and conscious sedation in primary dental care, 2000
• National Clinical Guidelines in Paediatric Sedation, 2002
• Recent Advances in Conscious Sedation, 2003

More guidelines
• Advanced Conscious Sedation Techniques for Paediatric Patients Training Syllabus
• Guidance for Commissioning – NHS England Dental Sedation Services – A Framework Tool
• A Guide to Maintaining Professional Standards in Conscious Sedation for Dentistry
• Safe Practice Scheme: Conscious Sedation Evaluation for Dentistry in the UK
• Conscious Sedation A Referral Guide for Dental Practitioners (in conjunction with DSTG)
And more guidelines… • RCS/RCA - Standing Committee for Sedation, 2007 • The NICE guidelines on sedating children, 2010 • Advanced Sedation, Training syllabus - DSTG, 2011
• IACSD – Intercollegiate Advisory Committee for Sedation in Dentistry guideline, 2015
Information Leaflets
• Create pictorial info for OS, IN, IV and IS patients • IV and IS forms must be given to 12-16 yr olds
• Age appropriate information
Information leaflets
• Need to mention ‘unpredictability’ of MDZ in pt info sheet
• Written info should be in line with NHS guidance reflecting the needs of different group with learning disabilities / where English is not the first language
• Alternatives to sedation
Information leaflets
Indications for sedation must be added:
• Anxiety – need anxiety scale measured
• Traumatic procedure
• Level of coop – need Frankl scale measured
• Nature of clinical procedure
Clinicians providing sedation
• Sedationist's training must be both from accredited courses and supervised practice
• CPD – must have 12 hours every 5 years including for IS
• Competence: minimal 20 IV, 10 OS/IN and 10 IS sedations a year
• If ‘irregular’ sedationist – mentoring and retraining needed
Clinicians providing sedation
• PILS for IS, IV, IN and OS • Nurse must be NEBDN / or equivalent
including for IS • Must know how to deal with respiratory
depression and collapsed airway
• Staff training and scenarios – new staff
Log book for all sedations
• Patients details
• Baseline vital signs
• Sedation agent
• Route
• Dose
• Reversal
• Untoward incidents
Regular scenario team training
• Respiratory depression • Airway support • Unconscious pt
• Obstruction • Vomiting • Failure of sedation • Idiosyncratic response • Delayed recovery • +ve pressure • Ventilation, airway adjuncts

Monitoring
• Level of consciousness
• Depth of sedation
• Airway patency
• Heart Rate and depth, skin colour, cap refill, pulse rate: rhythm vol
• SpO2 reading needed and BP for IV:
1. Pre-op
2. Intra-op
3. Post-op
4. Before discharge

Recovery
Must be supervised and monitored Discharge criteria: • Pt must be orientated in time, place and person • Vital signs stable • no pain / discomfort • HA • Cannula removed • Escort present • Analgesia given post-op • Post-op and post-sed instructions given

Miscellaneous
• Immediate treatment only if in best interest of the child
• Children under 16 must have an escort for IS
• OS and IN - sedation not pre-med, hence cannulation is necessary
Clinical Governance
• Critical incidents must be reported
• Assessment of outcomes will be undertaken through audit and reflection
• Records of equipment maintenance must be retained for inspection
Audits
• Midazolam over sedation
• Untoward events/complaints
• Monitor Sp02
Never events which must be reported centrally
IV for young patients: It works for some… not for all!!

IN: has its downs and ups!!

OS: not for all… but for some!!
The truth, the whole truth and nothing but the truth
Sedating children is very difficult:
• They have parents • They have no experience with cannulation • They have no experience of being “tipsy” • They have no experience of numbness • They “pretend” to be calm and then panic • They have abundant hormones • They can scream very loud!!! …What really helps is the amnesia…
So…
Recognise limitations
Know when not to start
Learn when to stop
Accept defeat
Refer!!










![Conscious Sedation In The Provision of Dental Care · patients requiring dental care and Conscious Sedation is a fundamental component of this. [2] q Competently provided Conscious](https://img.pdfslide.us/doc/110x75/5e80f906b673072b2a542a7a/conscious-sedation-in-the-provision-of-dental-care-patients-requiring-dental-care.jpg)