Embed Size (px)
DESCRIPTION
Beberapa profesional dental telah mempunyai perhatian terhadap penatalaksanaan pasien dengan seizure disorders. Peneliti berpendapat bahwa penambahan pengetahuan mengenai kejang dan bagaimana menanganinya sehingga pelayanan dental lebih nyaman. Artikel ini meninjau tipe-tipe kejang, mendiskusikan antikonvulsan yang biasa digunakan dan menguraikan beberapa perhatian khusus bagi dokter gigi yang memberikan pelayanan kepada pasien-pasien ini.
Citation preview

1995;126;1641-1647 J Am Dent Assoc
BJ Sanders, JA Weddell and NN Dodge disorders: dental and medical issues
Managing patients who have seizure
jada.ada.org ( this information is current as of June 6, 2009 ):The following resources related to this article are available online at
http://jada.ada.org/cgi/content/abstract/126/12/1641in the online version of this article at:
including high-resolution figures, can be foundUpdated information and services
http://jada.ada.org/cgi/collection/pharmacologyPharmacology http://jada.ada.org/cgi/collection/endodonticsEndodontics
: subject collectionsThis article appears in the following
http://www.ada.org/prof/resources/pubs/jada/permissions.aspthis article in whole or in part can be found at:
of this article or about permission to reproducereprintsInformation about obtaining
© 2009 American Dental Association. The sponsor and its products are not endorsed by the ADA.
on June 6, 2009 jada.ada.org
Dow
nloaded from
ARTICLE 2
Some dental professionals may
have concems about treating pa-
tients who have seizure disor-
ders. The authors contend that
Increased knowledge about
seizures and how to manage
them may make dental profes-
sionals more comfortable. This
article reviews the various
seizure types, discusses com-
monly used anticonvulsants and
their side effects and outlines
some special concerns dentists
may have In providing care to
these patients.
MANAGING PATIENTS VYHO HAVE SEIZUREDISORDERS: DENTAL AND MEDICAL ISSUESBRIAN J. SANDERS, D.D.S., M.S.; JAMES A. WEDDELL, D.D.S.,M.S.D.; NANCY N. DODGE, M.D.
Qetween 0.3 and 0.7 percent of the U.S. population have a seizuredisorder, and as many as 10 million people have been evaluated bya physician for this diagnosis.' The prevalence is highest in childrenbetween the ages of 2 and 5 years and at puberty, but the incidenceof first-time seizures increases significantly after the age of 50, sec-ondary to cerebrovascular disease.2A seizure is a temporary involuntary disturbance of brain func-
tion that may be manifested as impaired consciousness, abnormalmotor activity or behavior, sensory disturbances or autonomic dys-function. This is accompanied by abnormal electrical discharges inthe brain that usually, but not always, can be detected by electroen-cephalography.
Seizures are classified based on whether the abnormal electricalactivity begins in a localized area (partial seizures) or throughoutthe brain (generalized seizures). Partial seizures are further classi-fied according to whether or not consciousness is impaired, withsimple partial seizures showing a variety of motor, sensory, auto-nomic or psychic symptoms but no impairment of consciousness.Partial complex seizures are associated with impaired conscious-ness. Partial seizures with secondary generalization also occur, dur-ing which the seizure initially is localized to one area of the brainand then spreads to involve both hemispheres.3
Generalized seizures, which affect the entire brain at the sametime, may occur without warning. They are divided into severaltypes, including tonic-clonic, myoclonic, atonic and absence sei-zures. Tonic-clonic seizures result in the loss of consciousness, andthe incidence of injury caused by falling is great. The postictal peri-od, or the recovery period after the seizure, is long. During this pe-riod the person may be confused or sleepy or may complain of aheadache. Myoclonic seizures are brief muscle spasms that occur inclusters but usually do not result in a loss of consciousness. Atonicseizures are brief, involuntary losses of muscle tone that result in asignificant number of injuries from falls. A person experiencing anatonic seizure may or may not lose consciousness. Absence, or petitmal, seizures consist of multiple brief episodes during which con-
JADA, Vol. 126, December 1995 1641
.,il.
on June 6, 2009 jada.ada.org
Dow
nloaded from

-C[INICA[ PRACIICE
sciousness is lost, with few, ifany, motor manifestations.Simple absence seizures arebrief-lasting less than 10 sec-onds-with atypical absenceseizures lasting up to a minute.These seizures may be mistak-en for daydreaming.
Another type of seizure is thefebrile seizure. These usuallyare generalized tonic-clonicseizures with a postictal phasethat occur in children between6 months and 5 years of ageduring a febrile illness. Theepisode is not considered afebrile seizure if it accompaniesa traumatic injury or othermetabolic cause. Febrileseizures occur in 2 to 5 percentof the U.S. population, and 40percent of those affected havehad more than one episode.4There is usually no medicationunless the seizures occur re-peatedly. Children who havehad febrile seizures usuallyhave a normal EEG and normallab values within one week ofthe seizure.4
Status epilepticus is seizureactivity that occurs with suchfrequency that the seizures arealmost continuous with no timebetween for recovery. Statusepilepticus can be associatedwith any type of seizure, but itis most often a generalizedtonic-clonic seizure. The risks ofstatus epilepticus include air-way compromise, acidosis, hy-potension, hypertension, hyper-thermia, cerebral edema,hypoglycemia and possible dete-rioration of central nervous sys-tem functioning following theepisode.3'4
The correct diagnosis of theseizure is important so that theappropriate anti-epileptic medi-cation may be given. Becauseseveral drugs are equally effec-tive for controlling seizures, ad-
verse effects, age, gender andcost all become factors in medi-cation selection. Currently, phe-nobarbital and phenytoin(Dilantin, Parke-Davis) are themost commonly prescribedseizure medications, but carba-mazepine (Tegretol, BaselPharmaceuticals) and valproicacid (Depakene, Depakote,Abbott Laboratories) are beingprescribed more frequently forpatients with seizure disorders.5Patients who have seizurestypically take a single medica-
I Because several drugs areequally effectivefor con-trolling seizures, adverseeffects, age, gender andcost all becomefactors inmedication selection.
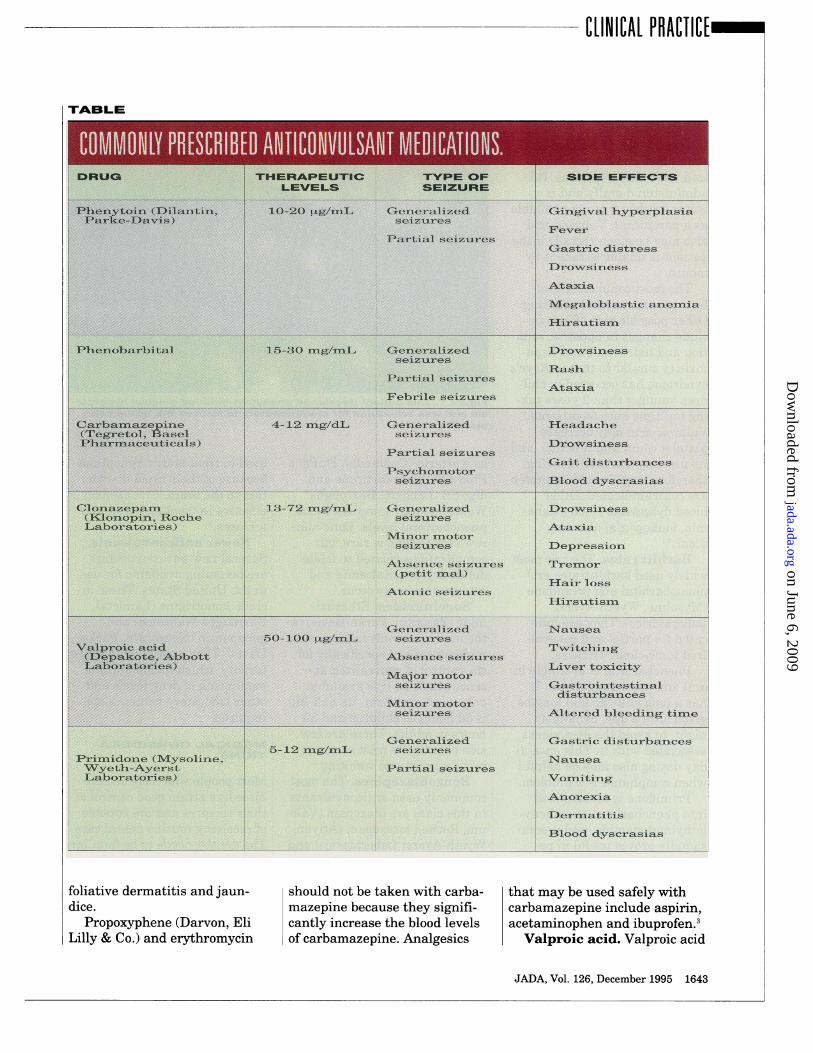
tion in dosages sufficient tomaintain therapeutic concen-trations. The table lists typicaltherapeutic levels, but the finaldetermination of dosage is indi-vidualized as some patients de-velop toxicity at lower concen-trations than others.
ANTICONVULSANTMEDICATIONS
Phenytoin. Phenytoin wasfirst introduced in 1938 and iswidely used to treat partial andgeneralized tonic-clonicseizures. It has proven to be oneof the best tolerated anticonvul-sants and has an unusuallyhigh therapeutic index. Pheny-toin can be taken orally, in cap-sule form, or intravenously. It isnot indicated for intramuscularinjection because of poor ab-sorption and crystallization inthe muscle.
Alcohol use on a regularbasis may increase phenytoin
clearance, and blood level con-centrations should be carefullymonitored in patients known toconsume alcohol regularly.
Chronic effects associatedwith phenytoin include gingivalhyperplasia, hirsutism andcoarsening of the facial fea-tures. Phenytoin also can alterthe metabolism of vitamin D,which can result in bone disor-ders such as osteomalacia andhypocalcemia. Factors that in-crease the risk of osteomalaciaare a low dietary intake of vita-min D, minimal exposure tosunlight and concomitant thera-py with other anticonvulsantmedications or use of exogenousmale hormones. Blood dyscra-sias are unusual, but there havebeen documented cases ofleukopenia and bone marrowsuppression. Most analgesicscan be taken safely with pheny-toin. If well-monitored, patientsare capable of taking phenytoinfor many years with goodseizure control.34Carbamazepine. Carba-
mazepine is pharmacologicallyrelated to tricyclic antidepres-sants. It is useful in controllingpartial complex and generalizedtonic-clonic seizures. It is onlyavailable in an oral form. Car-bamazepine has a relativelyshort half-life that results indaily fluctuations and necessi-tates frequent daily dosing.Concomitant use with pheny-toin increases the clearancetime of carbamazepine signifi-cantly, resulting in higherdosage requirements.
Carbamazepine is equal tophenytoin in anti-epilepticproperties. It is widely pre-scribed by physicians because itdoes not cause gingival hyper-plasia or hirsutism. Adverse ef-fects include blood dyscrasias(including aplastic anemia), ex-
1642 JADA, Vol. 126, December 1995
on June 6, 2009 jada.ada.org
Dow
nloaded from
CLINICAL PRACTICE-'
TABLE
Phenytoin (Dilantine, 10-20ig/mL Generalized Gingival hyperplasiaParke-Davis) seizures
FeverPartial seizuires
PGastric distress
Drowsiness
Ataxia
Megaloblastic anemia
Hirsiitism
Phenobarbital 15-30 mg/mL. Generalized Drowsinessseizuires
RashPartial seizuires
AtaxiaFebrile seizures
Carbamazepine 4-12 mg/dL Geeneralized Headache(Tegretol, Basel seizuresPharmaceviticals) Drowsiness
Partial seizuresGait distuirbances
Psychomotorseizures Bo scrasias
Clonazepam 13-72 mg/mLI G-eneralized Drowsiness(Kloniopin, Roche seizuresLaboratories) Ataxia
Minor motorseizuires Depression
Absence seizures Tremor(petit mal)
Hair lossAtonic seizures
Hirstitism
Generalized Nausea50-100 Ztg/mL, seizuires
Valproic acid Twitching(Depakote, Abbott Absence seizuzresLaboratories) . miver toxicity
M\!ajor motorseizures Gastrointestinal
disturbancesMiinor motorseizuires Altered bleeding time
Generalized Gastric distuirbances5-12 mg/mL, seizLires
Primidone (Mysoline, NaiiseaWyeth-Ayerst Partial seizuresL.aboratories) Vomiting
AnorexiaDermatitis
Blood dyscrasias
foliative dermatitis and jaun-dice.
Propoxyphene (Darvon, EliLilly & Co.) and erythromycin
should not be taken with carba- that may be used safely withmazepine because they signifi- carbamazepine include aspirin,cantly increase the blood levels acetaminophen and ibuprofen.3of carbamazepine. Analgesics Valproic acid. Valproic acid
JADA, Vol. 126, December 1995 1643
DRU43 YHERAPEUVIC IrYPE OF SIDE EFFECYSSEIZURELEVELS
on June 6, 2009 jada.ada.org
Dow
nloaded from
rnC[INICAI. PACIICL-
has a broad spectrum of anti-epileptic activity and is usefulin preventing generalized ab-sence, myodonic and general-ized tonic-clonic seizures. It isadministered orally and iswater soluble; it is not availableas a parenteral. Valproic acidalso may be given rectally if thepatient is unable to take it bymouth.
The most common side ef-fects are nausea and vomiting.Other possible side effects in-clude changes in appetite, seda-tion and hair loss. Fatal hepa-toxicity similar to that in Reye'ssyndrome has occurred in chil-dren younger than 2 years tak-ing multiple anticonvulsants.6Valproic acid may decreaseplatelet count and function, andits use may increase bleeding;therefore, aspirin and ibuprofenare contraindicated. Otherblood dyscrasias (such as ane-
mia, leukopenia) also mayoccur.3'4
Barbiturates. The two mostwidely used barbiturates are
phenobarbital and primidone(Mysoline, Wyeth-AyerstLaboratories). They are indi-cated for partial and general-ized tonic-clonic seizures.
Phenobarbital is available inoral and parenteral forms. Ithas a long half-life and may begiven once a day, usually atnight, to avoid the drowsinessassociated with it. This once-a-
day dosing also may be helpfulwhen compliance is a problem.
Primidone is metabolizedinto phenobarbital and pheny-lethylmalonamide, and it occa-sionally proves useful in pa-tients whose generalizedtonic-clonic seizures are notwell controlled with other anti-convulsants.
Drugs that increase the ac-
tivity of hepatic enzymes such
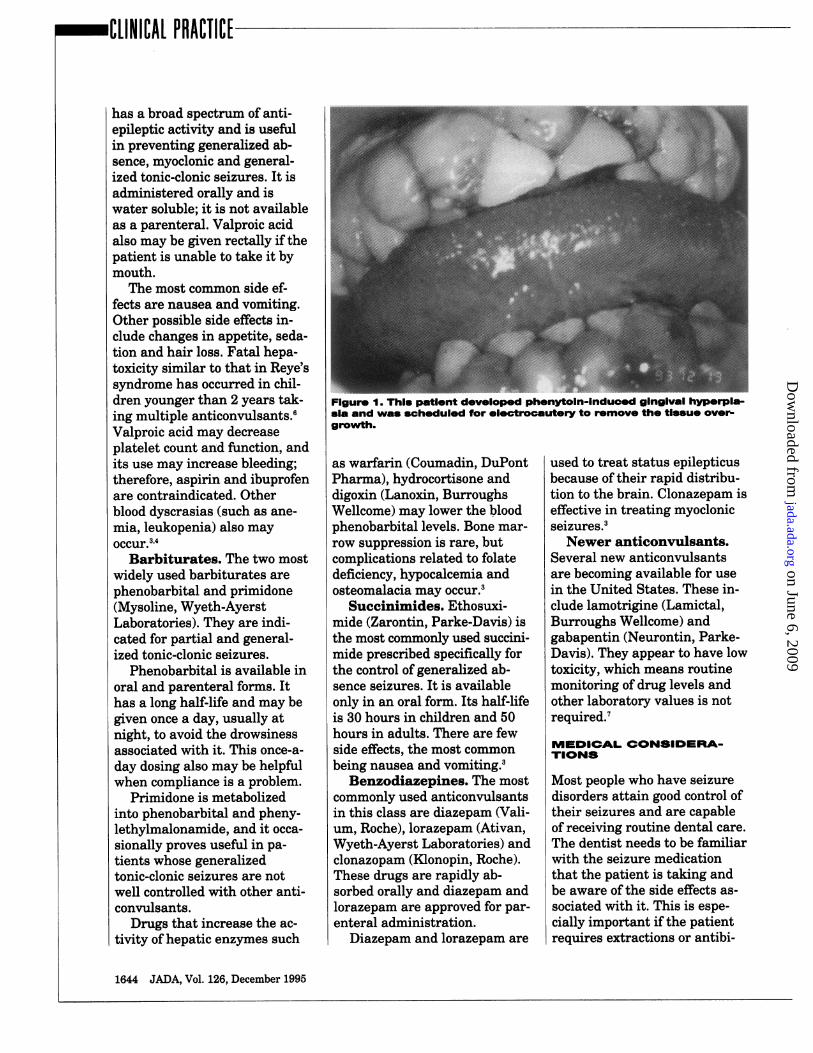
Figure 1. Thil paVont developed pnenytomn-mnduoo gingva. nyperp-ssa and was scheduled for elotrobautery to romove the tlsue over-
growth.
as warfarin (Coumadin, DuPontPharma), hydrocortisone anddigoxin (Lanoxin, BurroughsWellcome) may lower the bloodphenobarbital levels. Bone mar-
row suppression is rare, butcomplications related to folatedeficiency, hypocalcemia andosteomalacia may occur.3
Succinimides. Ethosuxi-mide (Zarontin, Parke-Davis) isthe most commonly used succim-mide prescribed specifically forthe control of generalized ab-sence seizures. It is availableonly in an oral form. Its half-lifeis 30 hours in children and 50hours in adults. There are fewside effects, the most commonbeing nausea and vomiting.3
Benzodiazepines. The mostcommonly used anticonvulsantsin this class are diazepam (Vali-um, Roche), lorazepam (Ativan,Wyeth-Ayerst Laboratories) andclonazopam (Kionopin, Roche).These drugs are rapidly ab-sorbed orally and diazepam andlorazepam are approved for par-enteral administration.
Diazepam and lorazepam are
used to treat status epilepticusbecause of their rapid distribu-tion to the brain. Clonazepam iseffective in treating myoclonicseizures.3Newer anticonvulsants.
Several new anticonvulsantsare becoming available for usein the United States. These in-clude lamotrigine (Lamictal,Burroughs Wellcome) andgabapentin (Neurontin, Parke-Davis). They appear to have lowtoxicity, which means routinemonitoring of drug levels andother laboratory values is notrequired.7
MEDICAL CONSIDERA-TIONS
Most people who have seizuredisorders attain good control oftheir seizures and are capableof receiving routine dental care.
The dentist needs to be familiarwith the seizure medicationthat the patient is taking andbe aware of the side effects as-
sociated with it. This is espe-cially important if the patientrequires extractions or antibi-
1644 JADA, Vol. 126, December 1995
on June 6, 2009 jada.ada.org
Dow
nloaded from

CLINICAL PRACTICE
Figure 2. The same patlent as In Flgure 1 Immediately after the gin-givectomy.
otic therapy. There is no one
theory for the pathogenesis ofseizures; they can be triggeredby many things such as anxiety,illness, fatigue, metabolicchanges and hyperventilation.When obtaining the patient's
medical history, it is importantto find out the seizure frequen-cy, how long the seizures last,whether the patient loses con-
sciousness or stops breathing,when the last seizure occurredand how the seizures usuallyare controlled. It is also impor-tant to find out the patient'stypical condition after a seizure(for example, is he or she con-
fused or sleepy, or does he or
she have headaches?).The office staff must be sen-
sitive to the embarrassmentthat many individuals feelafter a seizure, and they mustmake every effort to make thepatient comfortable. Many pa-tients will suffer a partial lossofmemory near the time of theincident, and some patients be-come incontinent during a
seizure, further elevating their
self-consciousness.Do not be alarmed if the pa-
tient is initially hard to arouse,as people often fall into a deepsleep after a seizure. It is usual-ly best to defer dental treat-ment when a patient has had amoderate to severe seizure, buta mild seizure may go unnoticedand usually will not interferewith treatment if the patientwishes to continue.
Patients who have grand-mal, tonic-clonic seizures maybe able to describe a sensationor aura before losing conscious-ness. The patient then experi-ences a brief period of musclerigidity (10 to 20 seconds). Thisis followed by generalized mus-
culoskeletal contractions andrelaxations that last from twoto five minutes. During thepostictal phase, which can lastfrom 10 to 30 minutes, themuscles relax and the respira-tory and cardiovascular sys-tems are depressed. Full recov-ery may take up to three hours.A seizure that stops and re-turns before the patient re-
gains consciousness is signifi-cantly more serious and maybe an indication of statusepilepticus.4'8
The first step in managing aseizure in the dental office is toprotect the patient from furtherinjury. The dental chair shouldbe placed in the supine positionand as close to the floor as pos-sible. Do not place anything inthe patient's mouth to prop itopen, such as mouth props or atongue blade, as this may causefurther injury.
Be sure to open the airway toallow adequate exchange of oxy-gen. This is best accomplishedby positioning the head so thatit is flexed and the neck ex-tended. It may help to place arolled towel under the patient'sshoulders. Suction the orophar-ynx for any excessive secretionsthat could obstruct the airway.Obtain vital signs such as heartrate and blood pressure and besure to contact the emergencymedical service as soon as theseizure begins to ensure promptmedical attention and follow-up.8,9As stated previously, recur-
rent seizures can be life-threat-ening. These must be treatedpromptly to avoid neuronaldamage, altered cerebralmetabolism, acidosis and hy-poxia.'0
Patients with recurrentseizures usually are stabilizedwith anticonvulsant medica-tions given intravenously.Unless your office staff istrained in the pharmacologicalmanagement of seizures, thisshould be managed by the EMSpersonnel. The current drug ofchoice to control recurrentseizures is lorazopam given at adose of 0.05 to 0.1 milli-gram/kilogram. Diazepam alsomay be given at doses of 0.2 to
JADA, Vol. 126, December 1995 1645
on June 6, 2009 jada.ada.org
Dow
nloaded from

-CLINICAL PRACIICE-
0.5 mg/kg, but lorazepam hasbeen found to have a longerhalf-life and is less likely tocause respiratory depressionand hypotension.
DENTAL CONSIDERA-TIONS
The presence of a seizure disor-der can influence some treat-ment decisions. For example,decisions regarding prostheticscan be affected by the, likelihoodof seizures. As a general rule, itis better to place a fixed pros-thesis than a removable appli-ance because the removableprosthesis can dislodge during aseizure. Also, placement of com-plete metal units should be con-sidered as they can minimizethe chance of a fracture.Likewise, use of acrylic facingson anterior crowns can facilitaterepair should a fractureoccur."'12
The most significant oralcomplication related to seizuremedication is gingival hyperpla-sia secondary to phenytoin ther-apy. About half the patientsplaced on phenytoin will showevidence of gingival enlarge-ment, usually within two to 18months after initiation of themedication. The etiology is stillunknown, but there appears tobe an increase in the number offibroblasts in the connective tis-sues.'3
Gingival hyperplasia mayoccur at any age, but it seems toaffect younger patients to agreater degree than adults. Menand women are equally affected.There does not appear to be acorrelation between dosage andthe incidence of gingival hyper-plasia. There is strong clinicalevidence of a correlation be-tween poor oral hygiene and theamount of tissue overgrowth.'4"15The gingival areas affected, in
order of severity, are- facial surfaces of the maxil-lary anteriors;- facial surfaces of themandibular anteriors;- buccal surfaces of the maxil-lary posteriors;- buccal surfaces of themandibular posteriors.
The lingual surfaces are af-fected to a lesser degree.
The tissue overgrowth maylead to delayed eruption of theteeth, misalignment, retention
As a general rule, it isbetter to place afixedprosthesis than a remov-able appliance because theremovable prosthesis candislodge during a seiure.
of food and debris, halitosis andan unsightly gingival appear-ance (Figure 1). Gingival over-growth resolves itself in one tosix months after withdrawal ofthe phenytoin16; with severecases, it may be beneficial toconsult with the patient's physi-cian about alternative seizuremedications to avoid some ofthese problems.
If the hyperplasia interfereswith oral function or esthetics,gingivectomy should be per-formed. The procedure can beperformed by electrocautery orlaser or with surgical instru-ments. If a full-mouth gingivec-tomy is performed in the oper-ating room, electrocautery orlaser is preferred because thereis less bleeding, and it is usu-ally not necessary to place asurgical dressing (Figures 1 and2).'7 Because the incidence of re-currence is higher with poor
oral hygiene, the patient shouldbe encouraged to maintain astringent hygiene routine.A positive-pressure appliance
may be used to prevent futuregrowth of the gingiva. The ap-pliance should be placed imme-diately after surgery and shouldbe worn at night and usuallythree hours during the day.Pressure appliances also can re-tard the growth of the hyper-plastic tissue in instanceswhere surgery is contraindi-cated.
Place patients who havegingival hyperplasia on a three-month recall. This will helpensure immaculate oral hy-giene. One study also suggeststhat a topical application ofstannous fluoride as part of thepatient's oral hygiene routinewill help control the gingivalovergrowth.'8CONCLUSION
Patients with seizure disordersmay be treated in the privatedental setting. A thorough med-ical history should tell you- what type of seizures the pa-tient has;- how well the seizures arecontrolled;- the frequency and duration ofseizures;- what might trigger a seizure;- what to expect when the pa-tient has a seizure.
Familiarize yourself with thepatient's seizure medicationsand the side effects associatedwith them. The information youobtain and document from thepatient will make you and yourstaff more comfortable. Themedical information also willenable you to be prepared for aseizure, possibly prevent onefrom occurring and provide bet-ter service to the patient over-all. .
1646 JADA, Vol. 126, December 1995
on June 6, 2009 jada.ada.org
Dow
nloaded from

CLINICAL PRACTIICE
Dr. Sanders is an assistant professor,Department of Pediatric Dentistry, IndianaUniversity, and an assistant professor, JamesWhitcomb Riley Hospital for Children,Indianapolis. Address reprint requests to Dr.Sanders, James Whitcomb Riley Hospital forChildren, 702 Barnhill Drive, Room 1110,Indiana University Medical Center,Indianapolis, Ind. 46202-5200.
Dr. Weddell is an associate professor,Department of Pediatric Dentistry, IndianaUniversity, and dental director, JamesWhitcomb Riley Hospital for Children,Indianapolis.
Dr. Dodge is an associate professor,Department of Pediatric Dentistry, IndianaUniversity, and an associate professor, JamesWhitcomb Riley Hospital for Children,Indianapolis.
1. Little JW, Falace DA. Dental manage-ment of the medically compromised patient.3rd ed. Chicago: Mosby-Yearbook; 1988:279-90.
2. Treiman DM. Current treatment strate-gies on selected situations in epilepsy.Epilepsia 1993;34(Supplement 65):517-23.
3. Cohen DW, ed. A symposium: the oral
manifestations of gingival hyperplasia.Compendium Contin Educ Dent1990;Supplement 14:S490-S514.
4. Hirtz DG, Nelson KB. The naturalhisotry of febrile seizures. Ann Rev Med1983;34:453-71.
5. Millikan CH, ed. Seizure disorders: clini-cal management. Part II. Detroit: Parke-Davis; 1976:6-23.
6. Konig SA. Severe hepatotoxicity duringvalproate therapy: an update and report oneight new fatalities. Epilepsia1994;35(5):1005-15.
7. Harden CL. New antiepileptic drugs.Neurology 1994;44(5):787-95.
8. Malamed SF. Managing medical emer-gencies. JADA 1993;124(8):40-51.
9. Selbst SM. Office management of statusepilepticus. Pediatr Emerg Care1991;7(2):106-9.
10. Pellock JM. Status epilepticus in chil-dren: update and review. J Child Neurol1994;9(Supplement 2):S27-35.
11. Rucker LM. Prosthetic treatment for thepatient with uncontrolled grand mal epilepticseizures. Spec Care Dentist 1985;5(5):206-7.
12. Braham RL, Casamassimo PS, NowakAJ, Posnick WR, Steinberg AD. The dentalimplications of epilepsy. Rockville, Md.: U.S.Department of Health Education and
Welfare, 1977; DHEW publication no. HSA78-5217.
13. Stinnett E, Rodu B, Grizzle WE. Newdevelopment in understanding phenytoin-in-duced gingival hyperplasia. JADA1987;114:814-6.
14. Thomason JM, Seymour RA, RawlinsMD. Incidence and severity of phenytoin in-duced gingival overgrowth in epileptic pa-tients in general medical practice.Community Dent Oral Epidemiol1992;20:288-91.
15. Modeer T, Dahllof G. Development ofphenytoin-induced gingival overgrowth innon-institutionalized epileptic children sub-jected to different plaque control programs.ACTA Odontol Scand 1987;45(2):81-5.
16. Dahllof G, Axio E, Modeer T. Regressionof phenytoin-induced gingival overgrowthafter withdrawal of medication. Swed Dent J1991;15(3):139-43.
17. Jones JE, Weddell JA, McKown CG.Incidence and indications for surgical man-agement of phenytoin-induced gingival over-growth in a cerebral palsy population. J OralMaxillofac Surg 1988;46:385-90.
18. Steinberg AD. Clinical management ofphenytoin-induced gingival overgrowth inhandicapped children. Pediatr Dent1981;3(Special Issue):130-6.
JADA, Vol. 126, December 1995 1647
Your Two Partners for Cost -Effective, Quality Lab Work !NSK's Highly Acclaimed, Best- Selling Electric and Air Turbine Handpieces .
VOLVERE GX - 35,000rpm PRESTO - 320,000rpm @35psi
"urers HIGHERK UORQUthtan most other engines * LONG BEAK1NGiL1{E:in the industry. NSKs DUST-SEAL prevents invasion of debris
* GXs high- torque coreless micranotor promises into handpiece nose and ball bearings.less burnout, more power. *NO LUBRICATION to the handpiece required.
*Gentle Start and Quick Stop. 0C(HIP AIR from handpiece nose blows chips away* Easy chuck change and cleaning. from the work area for clearer vision.* Lever type or Ring type heavy-duty handpiece. *TIME SAVING:*FEED BACK CONTROL assures smooth rotation CHIP AIR also maintains the work metal coolunder increased load at slow speeds. to enable you to hold it from beginning to finish.
*OVER-LOAD PREVENTION system for safety. *EASY BUR CHANGE. NO HOSE DRAG.*COMPACT,LIGHT WEIGHT handpiece.
For more information, call or write your NSK America authorized distributor.p * VNSK AMERICA CORPORATION
700B Cooper Court, Schaumburg, IL 60173Phone (708)843-7664 Fax (708)843-7622 Manufacturedby NakanishiDentalMfg. Co.,Ltd.
YYVe4YVTIT'% FIMA-1,T%r%T TV' -1- --- --I- -.--
on June 6, 2009 jada.ada.org
Dow
nloaded from