Embed Size (px)
Citation preview
Oncology Nursing Society 43nd Annual CongressMay 17–20, 2018 • Washington, DC 1Preconference
Liz Stokes, JD, MA, RNDirectorAmerican Nurses Association Center for Ethics & Human [email protected]
Patricia Jakel, MN, RN, AOCNAdvanced Practice NurseUCLA Medical [email protected]
Key Session Takeaways1. Ethical dilemmas are often at the root of moral distress, and if left
unresolved, can lead to disengagement, strained relationships, burnout, and, inevitably, substandard patient care.
2. Early identification and intervention of ethical issues is key to managing moral distress, but it takes time, know-how, and in-vestment in resources to be successful.
3. The ability to build moral resilience exists within all of us but needs to be nurtured and refined to be effective. It is important that this occur at the individual, departmental, and organization-al levels in order to be truly robust.
Managing Moral Distress and Building ResiliencyWednesday, May 16 • 1–3 pm
Note one action you’ll take after attending this session: ____________________________________________________
________________________________________________________________________________
ONS 43rd Annual Congress
Preconference 1
Managing Moral Distress and Building Resiliency
Patricia Jakel, RN, MN, AOCNAdvance Practice Nurse, UCLA Santa Monica Medical Center
Associate Professor , UCLA SON
Liz Stokes, JD, MA, RNDirector
American Nurses Association Center for Ethics and Human Rights
Managing Moral Distress and Building Resiliency
Patricia Jakel, Rn, MN, AOCNAdvance Practice Nurse
UCLA Santa Monica Medical CenterAssociate Professor UCLA SON
ONS 43rd Annual Congress
Preconference 2
Disclosures
• No disclosures
Acknowledgments• Research participants in our previous and current research projects
- Clinical Nurses, Nurse Leaders, Physicians, Clinical Ethicists• Katherine Brown-Saltzman, MA, RN • Joan Henriksen, PhD, RN • Carol Pavlish, Ph.D., RN, FAAN • Ellen M. Robinson, Ph.D., RN• Research Assoicates
– Patricia Jakel, RN, MN, AOCN and Belinda Chen, MPH - statistician• ICU leadership, CNS’s, and ethics champions/coaches• Research assistants
- Christopher Farra, Jennifer Tamir, Julia Wong• Funding agency
- Impact Grant from American Association of Critical-Care Nurses
• Oncology Nursing Society
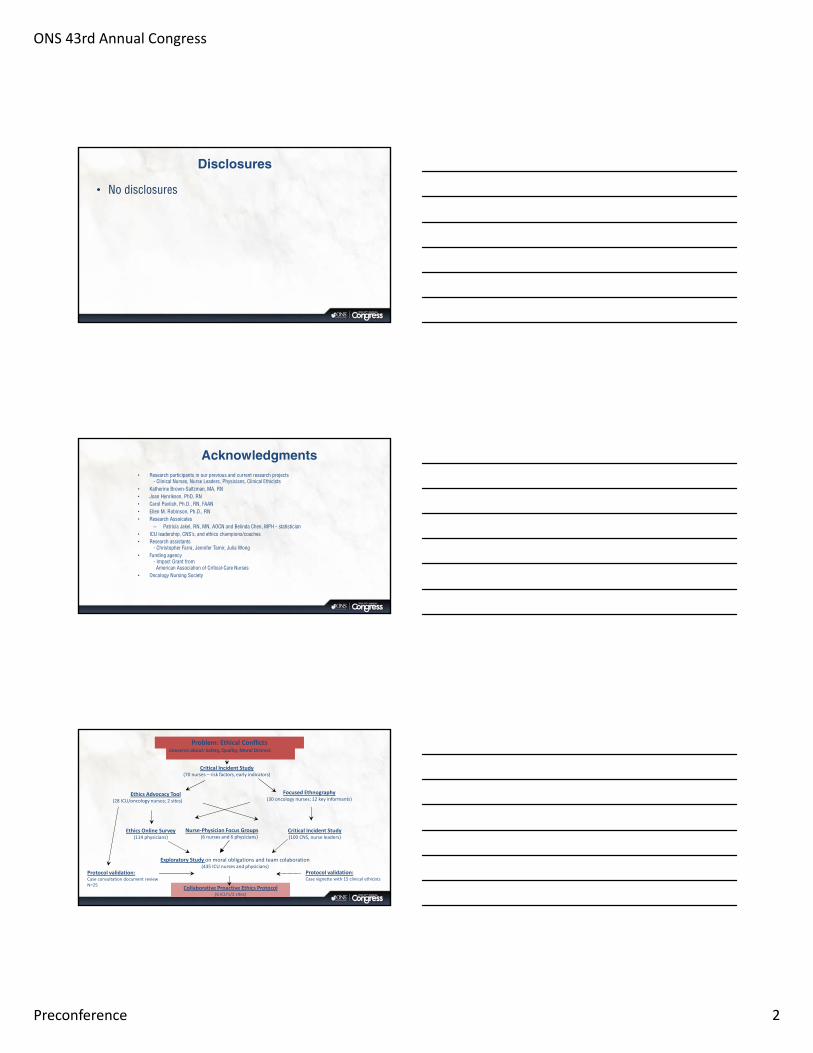
Problem: Ethical Conflicts
Critical Incident Study(70 nurses – risk factors, early indicators)
Ethics Advocacy Tool(28 ICU/oncology nurses; 2 sites)
Focused Ethnography (30 oncology nurses; 12 key informants)
Ethics Online Survey(114 physicians)
Critical Incident Study (100 CNS, nurse leaders)
Exploratory Study on moral obligations and team colaboration(435 ICU nurses and physicians)
Collaborative Proactive Ethics Protocol(6 ICU’s/3 sites)
Concerns about: Safety, Quality, Moral Distress
Protocol validation: Case vignette with 15 clinical ethicists
Protocol validation:Case consultation document reviewN=25
Nurse‐Physician Focus Groups(6 nurses and 6 physicians)
ONS 43rd Annual Congress
Preconference 3
Responding to the Aching Heart
Moral Distress - The Aching Heart
Experience of Moral Distress - “when one knows what to do but
institutional constraints make it nearly impossible to pursue right course of action” (Jameton, 1984)
“being seriously compromised as a moral agent; relational experience shaped by workplace environment”
(Varcoe, Pauley, Webster, & Storch, 2012)
Definition
• From Latin ‘dis’ and ‘ad gratum’ which means ‘moving in different directions’
• Differences in conceptions of the good
• Different beliefs about moral obligations and who has a right to what
• From Latin ‘dis’ and ‘ad gratum’ which means ‘moving in different directions’
• Differences in conceptions of the good
• Different beliefs about moral obligations and who has a right to what
Moral Disagreement
(Expected in complex care)
• From Latin ‘confligere’ or ‘to strike together’
• Clashing of moral perspectives
• Evolve from moral disagreements that are ignored, poorly managed, intractable, authoritarian
• From Latin ‘confligere’ or ‘to strike together’
• Clashing of moral perspectives
• Evolve from moral disagreements that are ignored, poorly managed, intractable, authoritarian
Ethical Conflict
(Disruptive to complex care)
ONS 43rd Annual Congress
Preconference 4
Why We Think This is Important• Compromised communication and teamwork are linked to patient
mortality and morbidity.1,3,4,6,19
• Patient trust in HCPs erodes as conflict escalates.7,13,21
• Ethical conflicts are linked to system-level issues that are difficult to trace and correct.3,4,17,18,20,21
• Standardized interdisciplinary communication tools enhance care
quality and patient safety.5,12
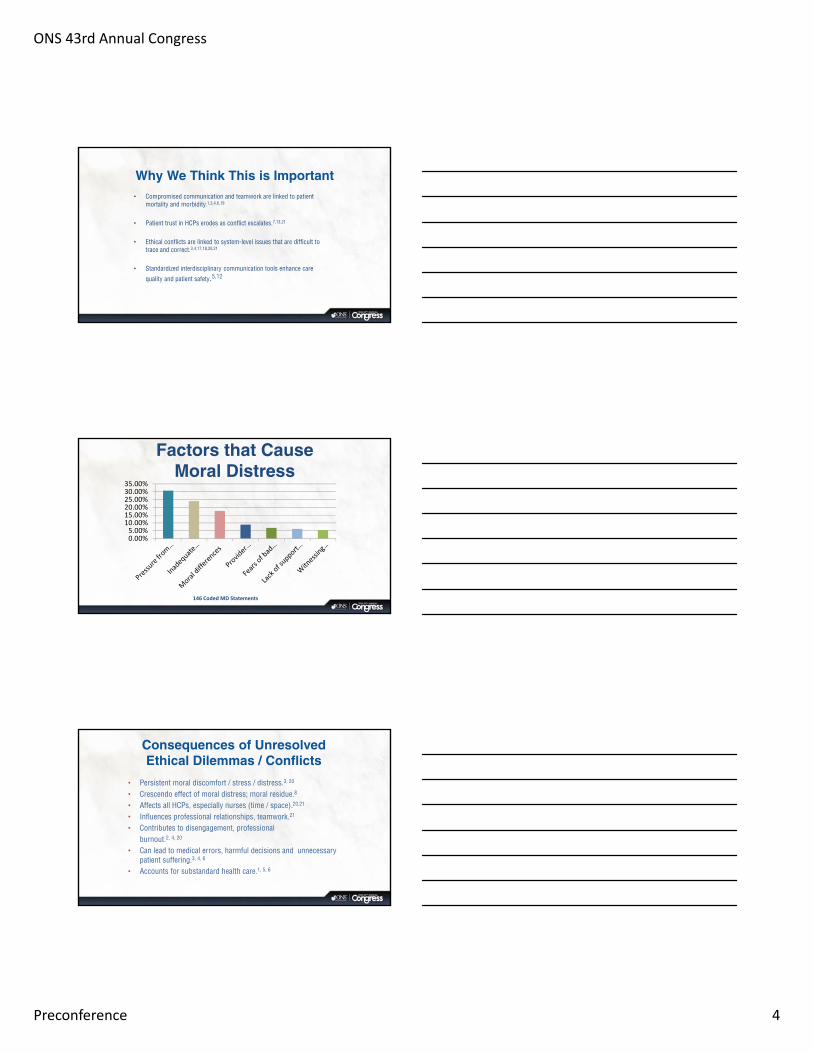
Factors that Cause Moral Distress
0.00%5.00%
10.00%15.00%20.00%25.00%30.00%35.00%
146 Coded MD Statements
Consequences of Unresolved Ethical Dilemmas / Conflicts
• Persistent moral discomfort / stress / distress.3, 20
• Crescendo effect of moral distress; moral residue.8
• Affects all HCPs, especially nurses (time / space).20,21
• Influences professional relationships, teamwork.21
• Contributes to disengagement, professional burnout.2, 4, 20
• Can lead to medical errors, harmful decisions and unnecessary patient suffering.3, 4, 6
• Accounts for substandard health care.1, 5, 6
ONS 43rd Annual Congress
Preconference 5
Accumulating Evidence of The Aching Heart
– “The distress was particularly high when we realized that every time we did something, she would bleed or something else would pop up.”
Evidence of the Aching Heart
• “… even though she was suffering a great deal – and they refused to allow anyone to give her morphine for pain.”
Evidence of the Aching Heart
• “He ended up passing away last year.”
ONS 43rd Annual Congress
Preconference 6
Evidence of the Aching Heart
“I think we do a great job of giving patients hope when we develop a plan for them, but then suddenly it doesn’t go well and then you ar left with all these decisions…we
don’t talk enough about what if treatment doesn’t work.”
The Aching Heart…
Aching
Heart
The Silent Ache
The Angry Ache
The Distancing
Ache
The Paralyzing
Ache
The Persistent
Ache
The Shared Ache
Pavlish & Brown‐Saltzman, 2016
Silent Ache
• “It’s what I was hoping to hear but it never happened.”
ONS 43rd Annual Congress
Preconference 7
The Distancing Ache
• “…the way you cope is to have good boundaries, just shut down.”
• “I just take myself out of the situation…”
The Distancing Ache
• “…way to survive is to be as closed as possible. The more open you are, it gets messy.”
The Angry Ache
• “Nothing we say matters.”
ONS 43rd Annual Congress
Preconference 8
The Paralyzing Ache
• “. . . but wonders who will stand up for the patient.”
The Aftermath Ache
• “And we’re living with that tension now. We’re living with the fallout of that.”
• “We’ve fallen into the abyss and how are we going to climb out?”
The Persistent Ache
• “We just keep letting it pile up.”
ONS 43rd Annual Congress
Preconference 9
The Ache of Uncertainty
• “…and the family gets so confused. They hear so many different things from different people. And then we expect them to make decisions and they’ve never been in a situation like this.”
Top Three Indicators of High Risk for Ethical Conflicts22
Top 3 indicators in both settings pertained to:
Patient suffering Provider distress Family’s unrealistic expectations
Shared Suffering
The Shared Ache
• “This is awful. And it’s not awful because of you or you or you. It’s awful because of the situation. It’s a shared awful.”
ONS 43rd Annual Congress
Preconference 10
Recognizing the Aching Heart and Creating the Dialogue
• Physician: “These family meetings definitely get easier the more I do them but they’re still very, very heavy and I think whenever the family breaks down you realize how real the situation is, like this is not just a patient. This is somebody’s Mom. This is somebody’s husband. And generally, honestly, at that point I think silence works the best, and I give them time, you know, whether it’s to sob or you know…and the discussion ultimately goes well. I think family conferences make it very real that these are human beings and these decisions that we make as physicians and prognostications are going to have a big impact on somebody’s life. Also, I have to say that whenever I say that word [death or dying], it also comes in my mind that the person that I’m saying it to will probably remember those words that come out of my mouth for the rest of their lives. That’s kind of haunts me, you know? I will probably not remember that patient’s name a few months later, but they will probably always remember me and what I said. “
Responding to the Aching Heart: Collaborative Ethics Model
CO – community obligation to patients for safe, high quality, evidence and ethics‐based care
Activate ethics assessment
Deliberate responsibilities
Voice concerns
Open opportunities for dialogue
Collaborate across disciplines/views
Analyze differences
Transform into agreeable components
Evaluate processes and early actions
Ethics Skill‐
Building for HCPs
Becoming a Moral
Community
Current StudyCo‐Advocate: Proactive and Interdisciplinary Collaboration in
Ethically Difficult Situations
Multi‐site study in 2 ICUs in three settings: UCLA, Mayo Clinic and Massachusetts General Hospital
ICU nurses and physicians / PAs / NPs
Outcome Measures:
Clinical Outcomes: LOS, number / timing of family care conferences, code discussion, and ethics consultations
Clinician Outcomes: Moral distress, collaborative practice, ethics self‐efficacy
ONS 43rd Annual Congress
Preconference 11
that identifies the smoke . . .
before it becomes a raging fire.
The protocol allows for a view
Pilot Study on Ethics Assessment and Planning
“So I knew that there was something going on and this guy might code and we’re doing all these things to him and I already knew that this was going to end up being some sort of ethics thing, but the tool confirmed it. I think in a less obvious case where the son just wasn’t letting us do anything [for pain], the problems were not quite as clear and so checking off ‘Disagreements’ Yes. ‘Patient suffering.’ Oh my God, yes. ‘Moral distress.’ Of course. ‘Unrealistic’ I mean it was like yes, yes, yes. So it [tool] really puts words to the things that are ambiguous or the things that you can’t hone in on because you’re so busy delivering care, especially to critically ill patients.”
Four Components to the Intervention
• Interactive, case-based online orientation to theprotocol
• Ethics Early Action Protocol• Ethics assessment, analysis and plan
• Incorporated into existing systems of care• Daily rounds, SBAR reports, EMRs
• Ongoing support for clinicians• Ethics app: ethics terminology, communication
models, resilience strategies
ONS 43rd Annual Congress
Preconference 12
Ethics Early Action Protocol © 2015
Used by permissions from UCLA Ethics
Early Actions
#1 Orientation to Protocol
ONS 43rd Annual Congress
Preconference 13
Downloadable Ethics AppThree Components:
1. Ethics terminology
2. Actions to prevent, mitigate moral distress and burnout3. Communication guidelines such as ASCEND
Anticipate content and approach for family meeting,Summarize the situation, Capture patient/family concerns, Explore and explain Next stepsDocument conversation
App – “Healthcare Ethics” can be downloaded through iTunes or Google Play
The Ethics Intervention
1. Online Orientation to Ethics Protocol
2. Ongoing support for clinicians – Ethics App
3. Incorporated into existing systems of care –Ethics Early Action Protocol
Summary of Preliminary Findings
Patient Outcomes
• Length of ICU stay• Family Conferences
(frequency and timing)
• Code Conversations (frequency)
• Ethics Consultations (frequency, small N)
HypothesisResults
ONS 43rd Annual Congress
Preconference 14
Nurse Feedback
• Feeling more aware and empowered by the tool:It ‘validates’ their experience in the cases
• Gives them language skills
• Clinicians taking ownership of how the Protocol is usedExample: use of dotphrase in the EMR
Recognizing the Outcomes
• Family meetings now are routine: “It used to be like pulling teeth, reinserting them, and then pulling them out again.”
• ‘ABC-E’ - “E is for Ethics!”
• RN and MD presented collaboratively an ethics case at a conference
• Teaching Ethics – opportunity to learn in real time
Limitations & Opportunities
• Multi-site– Micro culture differences– Data collection difficulties
• Preliminary Interpretations• Acceptability of tool
• Refine protocol based on clinician suggestions
• Additional testing in different sites
• Adapt protocol for pediatrics• View data again from different
angles– Consider gender, ethnicity
ONS 43rd Annual Congress
Preconference 15
Summary of Preliminary Findings
Clinician Outcomes
• Decrease in clinician moral distress
• Increased perception of individual effectiveness in dealing with ethical issues
• Increase in perception of ethical climate of their work environment
HypothesisResult
Hospital Ethical Climate Survey
Ethics Self-Efficacy Survey• Measures level of confidence for a specific task or process (Bandura, 1997)• Perceptions are associated with:
– Likelihood of taking on challenging tasks (Mann et al., 2012)– Perseverance in the face of adversity / barriers (Rathert, May, & Chung, 2016)
• Can influence moral courage – overcoming personal fears and converting moral intentions to actions in spite of pressure to do otherwise (Rathert, May, & Chung, 2016)
• Ethics Self-Efficacy Scale was created by researchers using Bandura’s template– Fourteen questions with scale of 1-9
• Assessed for content relevance and clarity with nurses and physicians in all three sites and revised accordingly
ONS 43rd Annual Congress
Preconference 16
Ethics Self-Efficacy Scale
RESULTS: CLINICAL OUTCOMESCLINICIAN OUTCOMES
What Did We Find?
Moral Distress Scale - Revised
ONS 43rd Annual Congress
Preconference 17
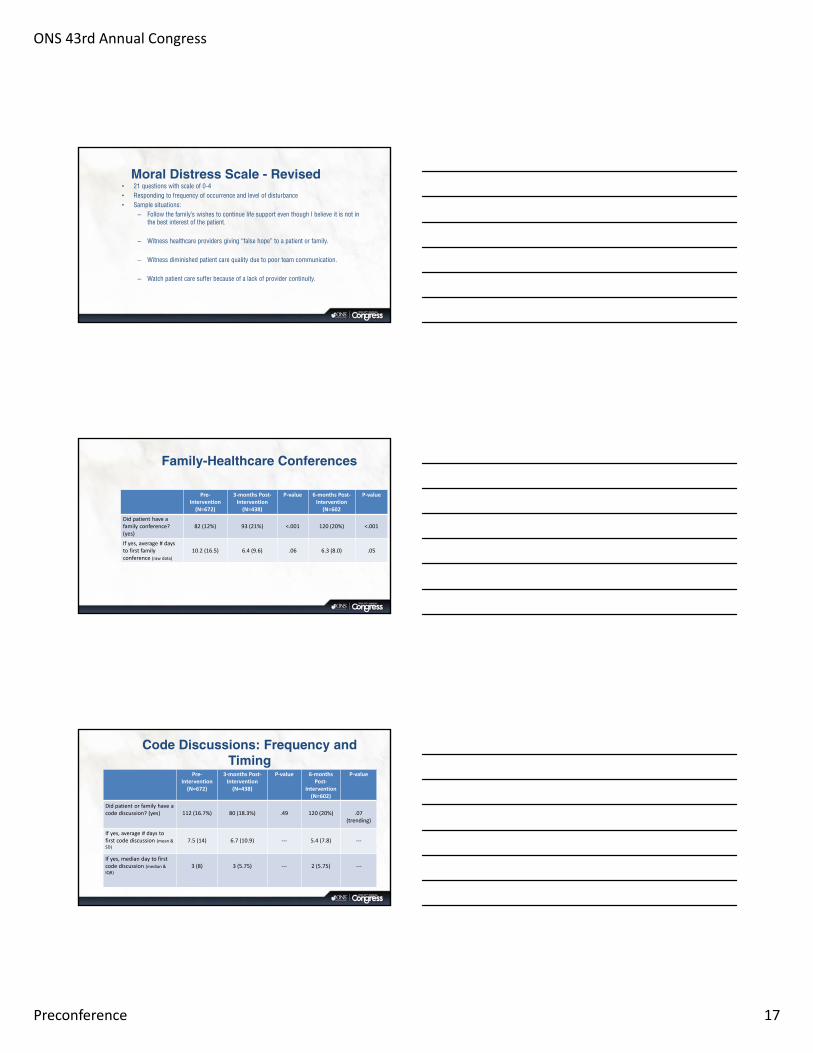
Moral Distress Scale - Revised• 21 questions with scale of 0-4• Responding to frequency of occurrence and level of disturbance• Sample situations:
– Follow the family’s wishes to continue life support even though I believe it is not in the best interest of the patient.
– Witness healthcare providers giving “false hope” to a patient or family.
– Witness diminished patient care quality due to poor team communication.
– Watch patient care suffer because of a lack of provider continuity.
Family-Healthcare Conferences
Pre‐Intervention(N=672)
3‐months Post‐Intervention(N=438)
P‐value 6‐months Post‐Intervention
(N=602
P‐value
Did patient have a family conference? (yes)
82 (12%) 93 (21%) <.001 120 (20%) <.001
If yes, average # days to first family conference (raw data)
10.2 (16.5) 6.4 (9.6) .06 6.3 (8.0) .05
Code Discussions: Frequency and Timing
Pre‐Intervention(N=672)
3‐months Post‐Intervention(N=438)
P‐value 6‐months Post‐
Intervention(N=602)
P‐value
Did patient or family have a code discussion? (yes) 112 (16.7%) 80 (18.3%) .49 120 (20%) .07
(trending)
If yes, average # days to first code discussion (mean &
SD)
7.5 (14) 6.7 (10.9) ‐‐‐ 5.4 (7.8) ‐‐‐
If yes, median day to first code discussion (median &
IQR)
3 (8) 3 (5.75) ‐‐‐ 2 (5.75) ‐‐‐
ONS 43rd Annual Congress
Preconference 18
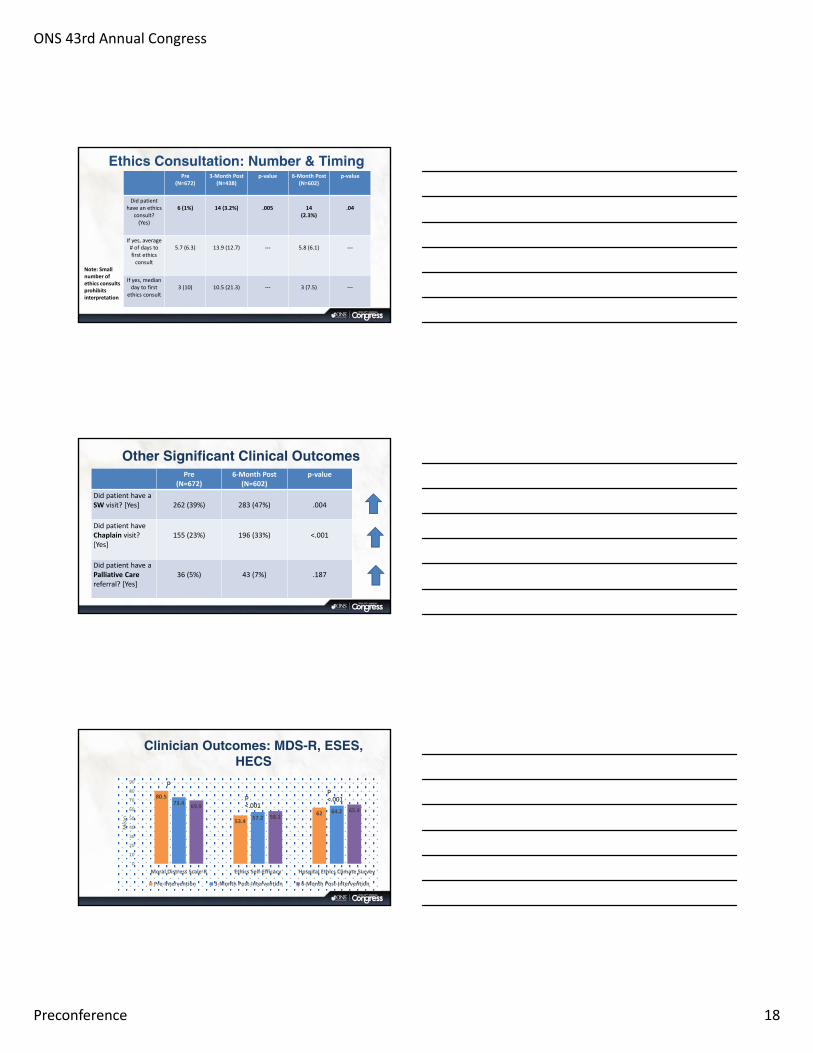
Ethics Consultation: Number & Timing Pre
(N=672)3‐Month Post
(N=438)p‐value 6‐Month Post
(N=602)p‐value
Did patient have an ethics
consult? (Yes)
6 (1%) 14 (3.2%) .005 14(2.3%)
.04
If yes, average # of days to first ethics consult
5.7 (6.3) 13.9 (12.7) ‐‐‐ 5.8 (6.1) ‐‐‐
If yes, median day to first
ethics consult3 (10) 10.5 (21.3) ‐‐‐ 3 (7.5) ‐‐‐
Note: Small number of ethics consults prohibits interpretation
Other Significant Clinical OutcomesPre
(N=672)6‐Month Post
(N=602)p‐value
Did patient have a SW visit? [Yes] 262 (39%) 283 (47%) .004
Did patient have Chaplain visit? [Yes]
155 (23%) 196 (33%) <.001
Did patient have a Palliative Care referral? [Yes]
36 (5%) 43 (7%) .187
Clinician Outcomes: MDS-R, ESES, HECS
80.5
53.4
62
73.4
57.264.2
69.9
58.165.4
0
10
20
30
40
50
60
70
80
90
Moral Distress Scale‐R Ethics Self‐Efficacy Hospital Ethics Climate Survey
Mean
Pre‐Intervention 3‐Month Post‐Intervention 6‐Month Post‐Intervention
p
p <.001
p <.001
ONS 43rd Annual Congress
Preconference 19
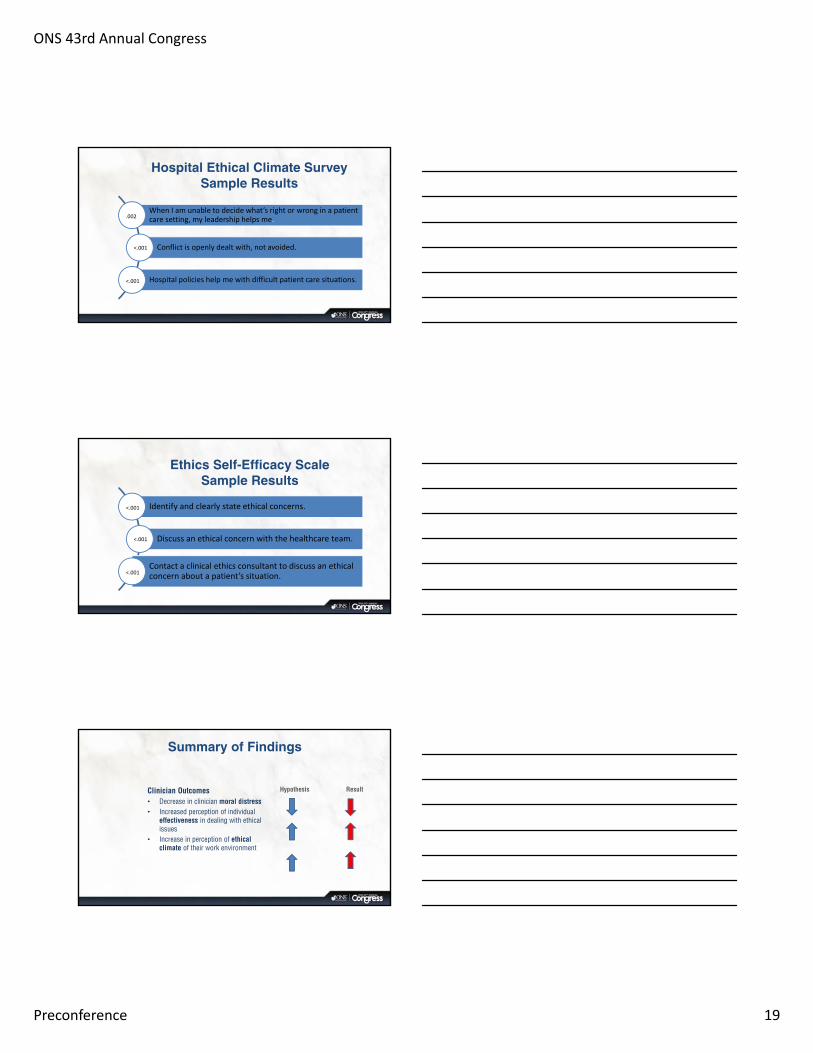
Hospital Ethical Climate SurveySample Results
When I am unable to decide what’s right or wrong in a patient care setting, my leadership helps me.
Conflict is openly dealt with, not avoided.
Hospital policies help me with difficult patient care situations.
.002
<.001
<.001
Ethics Self-Efficacy Scale Sample Results
Identify and clearly state ethical concerns.
Discuss an ethical concern with the healthcare team.
Contact a clinical ethics consultant to discuss an ethical concern about a patient’s situation.
<.001
<.001
<.001
Summary of Findings
Clinician Outcomes• Decrease in clinician moral distress• Increased perception of individual
effectiveness in dealing with ethical issues
• Increase in perception of ethical climate of their work environment
Hypothesis Result
ONS 43rd Annual Congress
Preconference 20
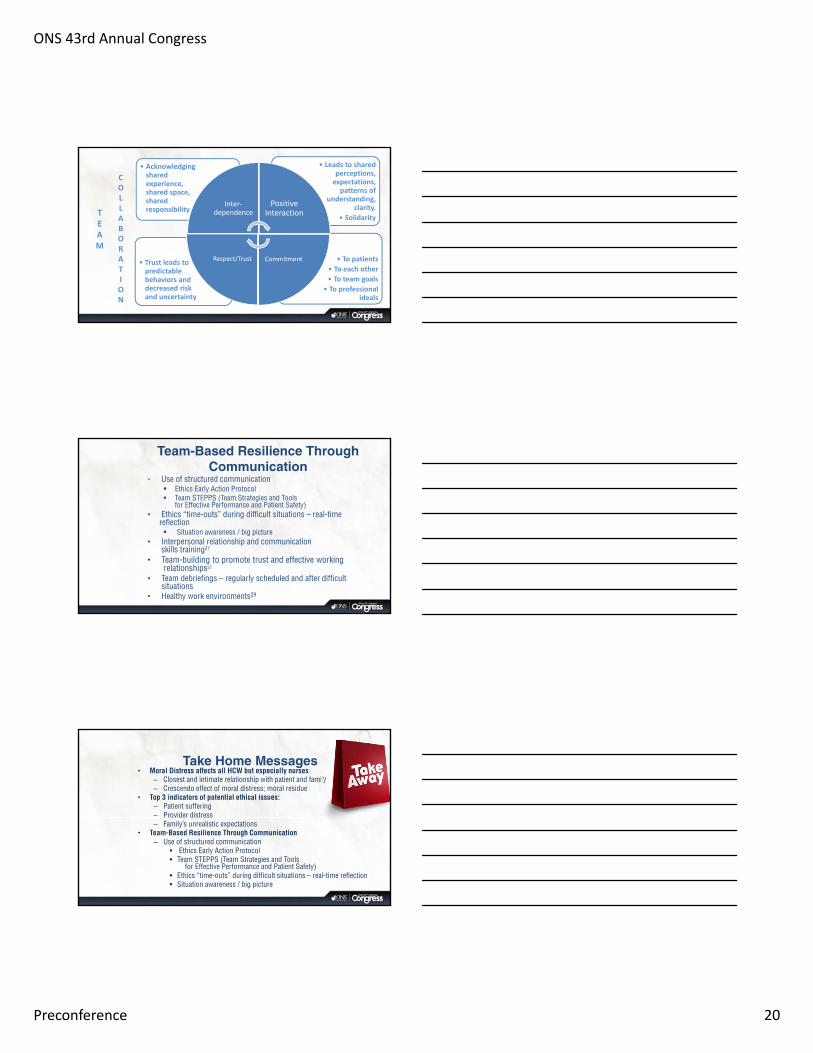
• To patients
• To each other
• To team goals
• To professional ideals
• Trust leads to predictable behaviors and decreased risk and uncertainty
• Leads to shared perceptions, expectations, patterns of
understanding, clarity.
• Solidarity
• Acknowledging shared experience, shared space, shared responsibility
Inter‐dependence
Positive Interaction
Commitment Respect/Trust
TEAM
COLLABORATION
Team-Based Resilience Through Communication
• Use of structured communication Ethics Early Action Protocol Team STEPPS (Team Strategies and Tools
for Effective Performance and Patient Safety)• Ethics “time-outs” during difficult situations – real-time
reflection Situation awareness / big picture
• Interpersonal relationship and communication skills training27
• Team-building to promote trust and effective workingrelationships27
• Team debriefings – regularly scheduled and after difficultsituations
• Healthy work environments29
Take Home Messages• Moral Distress affects all HCW but especially nurses
– Closest and intimate relationship with patient and family– Crescendo effect of moral distress; moral residue
• Top 3 indicators of potential ethical issues:– Patient suffering– Provider distress– Family’s unrealistic expectations
• Team-Based Resilience Through Communication – Use of structured communication
Ethics Early Action Protocol Team STEPPS (Team Strategies and Tools
for Effective Performance and Patient Safety) Ethics “time-outs” during difficult situations – real-time reflection Situation awareness / big picture
ONS 43rd Annual Congress
Preconference 21
Responding to the Aching Heart
“It takes onlyone
listening earto aid the
aching heart.”CV Mankin
References1. Aiken, L., Clarke, S., Sloane, D., Lake, E., & Cheney, T. (2008). Effects of hospital care environment on patient mortality and nurse
outcomes. Journal of Nursing Administration, 38(5), 223‐229
2. American Credentialing Center (2008). Overview of ANCC Magnet Recognition Program. Retrieved from http://www.nursecredentialing.org/Magnet/ResourceCenters/MagnetResearch/Magnet‐Overview‐Brochure.pdf
3. Austin, W. (2012). Moral distress and the contemporary plight of health professionals. HEC Forum, 24, 27‐38.
4. Balvere, P., Cassells, J., & Buzaianu, E. (2012). Professional nursing burnout and irrational thinking. Journal for Nurses in Staff Development, 28(1), 2‐8
5. Boyle, D. K., Miller, P., & Forbes‐Thompson, S. (2005). Communication and end‐of‐life care in the intensive care unit: Patient, family, and clinician outcomes. Critical Care Nursing Quarterly, 28(4), 302‐316.
6. Cimiotti J., Aiken, L., Sloane, D., & Wu, E. (2012). Nurse staffing, burnout, and healthcare‐associated infections. American Journal of Infection Control, 40, 486‐490.
7. Edelstein, L., DeRenzo, E., Waetzig, E., Zelizer, C., & Mokwunye, N. (2009). Communication and conflict management training for clinical bioethics committees. HEC Forum, 21(4), 341‐349.
8. Epstein, E., & Hamric, A. (2009). Moral distress, moral residue, and the crescendo effect. The Journal of Clinical Ethics, 20(4), 330‐342.
9. Garon, M. (2012). Speaking up, being heard: Registered nurses’ perceptions of workplace communication. Journal of Nursing Management, 20, 361‐371.
10. Institute of Medicine. (2010). The future of nursing: Leading change, transforming health.
11. Joint Commission. (2009). Leadership in healthcare organizations: A guide to Joint Commission leadership standards. http://www.jointcommission.org/assets/1/18/WP_leadership_standards.pdf
References12. Leonard, M., Graham, S., & Bonacum, D. (2004). The human factor: The critical importance of effective teamwork and
communication in providing safe care. Quality and Safety in Health Care, 13(Suppl 1), i85‐i90. doi: 10.1136/qshc.2004.010033
13. McCullough, L. (2012). An ethical framework for the responsible leadership of accountable care organizations. American Journal of Medical Quality, 27, 189‐194.
14. Pavlish, C., Brown‐Saltzman, K., Hersh, M., Shirk, M., & Nudelman, O. (2011a). Early Indicators and Risk Factors for Ethical Issues in Clinical Practice. Journal of Nursing Scholarship, 43 (1),13‐21.
15. Pavlish, C., Brown‐Saltzman, K., Hersh, M., Shirk, M., Rounkle, AM. (2011b) Nursing priorities, actions, and regrets for ethical situations in clinical practice. Journal of Nursing Scholarship. 43(4):385‐95.
16. Pavlish, C., Brown‐Saltzman, K., Jakel, P., & Rounkle, A. (2012). Nurses’ responses to ethical challenges in oncology: An ethnographic study. Clinical Journal of Oncology Nursing.
17. Pavlish, C., Brown‐Saltzman, K., Fine, A., & Jakel, P. (In press.). Making the call: A proactive ethics framework.” HEC Forum.
18. Pendry, P. (2007). Moral distress: recognizing it to retain nurses. Nursing Economics, 25(4), 217‐221.
19. Rosenstein, A., & O’Daniel, M. (2005). Disruptive behavior and clinical outcomes: Perceptions of nurses and physicians. American Journal of Nursing, 105(1), 54‐64.
20. Ulrich, C., Hamric, A., & Grady, C. (2010). Moral distress: A growing problem in the health professions? Hastings Center Report, 40(1), 20‐22.
21. Van Soeren, M., & Miles, A. (2003). The role of teams in resolving moral distress in intensive care unit decision‐making. Critical Care, 7, 217‐218. doi:10.1186/cc2168
ONS 43rd Annual Congress
Preconference 22
References22. Pavlish, C., Henriksen Hellyer, J., Brown‐Saltzman, K. et al. (2015). Screening situations for risk of ethical conflicts: A pilot study. American Journal of
Critical Care, 24, 248‐256.
23. Pavlish, C., Brown‐Satlzman, K., So, L. et al. (2015). Avenues of action in ethically complex situations. JONA, 45(6), 311‐8.
24. Pavlish, C., Brown‐Saltzman, K., Fine, A., & Jakel, P. (2014). Making the call: A proactive ethics framework. HEC Forum.
25. Pavlish, C., Brown‐Saltzman, K., Jakel, P. et al. (2013) The nature of ethical conflicts and the meaning of moral community in oncology practice. Oncology
Nursing Forum.
26. Pavlish, C., Brown‐Saltzman, K, et al. (2016). SUPPORT: An evidence‐based model for leaders addressing moral distress. JONA, 46(6), 313‐320.
27. Moss, M., Good, V., Gozal, D., Kleinpell, R., & Sessler, C. (2016). An official Critical Care Societies Collaborative Statement: Burnout syndrome in critical
care healthcare professionals: A call for action. Critical Care Medicine, 44, 1414‐1421.
28. Rushton, C., Batcheller, J., Schroeder, K., & Donohue, P. (2015). Burnout and resilience among nurses practicing in high‐intensity settings. American
Journal of Critical Care, 24(5), 412‐420.
29. American Association of Critical‐Care Nurses. (2016). Healthy Work Environments.
30. Neville, T., Wiley, J., Yamamoto, M., Flitcraft, M., Anderson, B., Curtis, R., & Wenger, N. (2016). Concordance of nurses and physicians on whether critical
care patients are receiving futile treatment. American Journal of Critical Care, 24, 403‐410.
Managing Moral Distress and Building Resiliency
Liz Stokes, JD, MA, RNDirector
American Nurses Association Center for Ethics and Human Rights
@ANAEthics
Disclosures
• No Disclosures
ONS 43rd Annual Congress
Preconference 23
Moral Resilience• Concept is in it’s infancy; evolving understanding• “The capacity of an individual to sustain or restore
their integrity in response to moral complexity, confusion, distress, or setbacks” (Rushton, 2016, p. 112a).
• “The ability and willingness to speak and take right and good action in the face of an adversity that is moral/ethical in nature” (Lachman, 2016, p. 122).
Moral Resilience• Moral resilience, like other forms
of resilience, is built in response to adversity
• All health care professionals have innate and learned capacities that can be leveraged toward and strengthened to address distress
Individual Moral Resilience• Cultivating moral resilience may be necessary
to respond to the aspects of the clinical environment that are not easily modifiable, such as caring for patients with complex, often life-limiting conditions, and witnessing suffering, death, disability, and social injustices.
ONS 43rd Annual Congress
Preconference 24
Promising Areas for Individual Moral Resilience
• ethical competence• ethics in education• self-regulation and mindfulness• self-care
Ethical Competence• The possession of ethical
knowledge next to the ability to ‘‘see’’ what a situation presents (ethical perception); to reflect critically about what nurses know, are, and do (ethical reflection); to bring out the ethical practice (ethical behavior); and to ‘‘be’’ ethical (Gallagher, 2006).
Ethical Competence• the ability to identify large-scale and everyday ethical issues
inherent in complex health care environments
• the ability to critically reflect and apply ethical theories in a dialectical decision-making process in which moral actions are justifiable, and
• resources assisting health care professionals to develop individualized resilient protective factors, including social skills, social support, goal efficacy, and problems-solving
ONS 43rd Annual Congress
Preconference 25
Ethics in Education• Ethics education has a positive
impact on ethical decision-making and moral action in nurses (Grady et al., 2008).
• Ethics education should occur continuously in safe environments that encourage understanding rather than judgment, engage discussion, and guide root cause understanding.
Self- Regulation• Self-regulation is the ability to mindfully
recognize what is happening in the moment and to monitor, evaluate, reinforce, or adapt one’s responses to changing conditions or adversity (Holtz, Heinze, & Rushton, 2017; Masten, 2014).
Mindfulness• Mindfulness is moment-to-
moment awareness, which is cultivated by intentionally focusing attention; noticing and releasing sensations, emotions, and thoughts that are distracting or depleting; promoting relaxation; and having personal insight (Kabat-Zinn, 2005).
ONS 43rd Annual Congress
Preconference 26
Mindfulness
Self Care• Provision 5 of the Code of Ethics for Nurses with
Interpretive Statements holds that “the nurse owes the same duties to self as to others, including the responsibility to promote health and safety, preserve wholeness of character and integrity, maintain competence, and continue personal and professional growth” (ANA, 2015).
ONS 43rd Annual Congress
Preconference 27
Develop Personal Plan• Assess you emotional and
physical wellbeing• Take note of your strengths• Take note of your weaknesses• Write it down/Own it• Start small and be patient
Moral Support System• Ensure that every individual nurse has access to
resources to mitigate moral distress and cultivate moral resilience.
Organizational Responsibility• Organizations have a vested interest in
recognizing that moral distress can negatively impact the retention of health care professionals in the field, and should consider implementing strategies that promote moral resilience among their workforce.
ONS 43rd Annual Congress
Preconference 28
Organizational Responsibility• Understanding the responses to ethical challenges
can be facilitated through: – incentives, – regulations, and – professional requirements such as attention to building
integrity, ethical competence, self-stewardship, and self-regulation, and recognizing the signals of moral distress and other forms of moral suffering.
Organization Actions• Assess, & if appropriate, implement
standards for a healthy work environment (AACN, 2016; Agency for Healthcare Research and Quality, 2013).
• Assess & adopt action steps outlined in the CCSC Statement on Burnout Syndrome (Moss et al., 2016).
• Programs aimed at developing capacities and skills in moral resilience.
Organization Actions• Raise awareness of moral distress, burnout, & compassion
fatigue• Provide nurses with tools for self-calibration (Shanafelt &
Noseworthy, 2017). • Promote strategies to support nurses’ moral resilience• Ensure core competencies in ethics for all levels of nursing
students, faculty, employees and other professionals. • Develop innovative technologies for nursing students &
staff to develop moral resilience strategies & self-care.
ONS 43rd Annual Congress
Preconference 29
Organization Actions• Document & study the impact of
individual interventions on nurses • Conduct intervention studies for root
causes of moral distress • Fund, develop, & evaluate innovative
individual & organizational models. • Collaborate with interprofessional
ethics organizations & medical societies to raise awareness.
Take Aways• Self aware• Ethical competent• Self regulation• Self care• Identify values• Develop personal plan
Take Aways• Assess and implement healthy work
environment• Raise awareness of moral distress,
burnout, & compassion fatigue• Provide nurses with tools for ethical
competence, self-calibration, and moral resilience
• Study the impact of interventions

ONS 43rd Annual Congress
Preconference 30
http://nursingworld.org/ExploringMoralResilience
A Call to Action: Exploring Moral Resilience Toward a Culture of Ethical Practice
References• Agency for Healthcare Research and Quality. (2013). Health Assessments in Primary Care. Retrieved from http://www.ahrq.gov/
professionals/prevention-chronic-care/improve/ system/health-assessments/index.html• American Association of Critical-Care Nurses. (2016). AACN healthy work environment assessment. American Association of CriticalCare Nurses website.
Retrieved from http://www. aacn.org/wd/hwe/content/aboutassessment. content?menu=hwe&lastmenu=divheader_web_ assessment_tool• American Nurses Association. (2015). Code of ethics for nurses with interpretive statements. Silver Spring, MD: ANA. Retrieved from www.
nursingworld.org/Code-of-Ethics • American Nurses Association. (2017). Call to action: Exploring moral resilience toward a culture of ethical practice. Retrieved from
http://nursingworld.org/ExploringMoralResilience• Gallagher, A. (2006). The teaching of nursing ethics: content and method. In A. J. Davis, V. Tschudin, L. de Raeve (Eds.), Essentials of teaching and
learning in nursing ethics: Perspectives and methods (pp. 223-239). London, UK: Churchill Livingstone.• Grady, C., Danis, M., Soeken, K. L., O’Donnell, P., Taylor, C., Farrar, A., & Ulrich, C. M. (2008). Does ethics education influence the moral action of
practicing nurses and social workers? The American Journal of Bioethics, 8(4), 4-11.• Holtz, H., Heinze, K., & Rushton, C. (2017). Inter‐professionals’ definitions of moral resilience. Journal of Clinical Nursing. doi:10.1111/ jocn.13989• Kabat-Zinn, J. (2005). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain and illness. New York: Delacourt Press• Lachman, V. D. (2016). Moral resilience: managing and preventing moral distress and moral residue. MedSurg Nursing, 25(2), 121-125.• Moss, M., Good, V. S., Gozal, D., Kleinpell, R., & Sessler, C. N. (2016). A Critical Care Societies collaborative statement: burnout syndrome in critical care
health-care professionals. A call for action. American Journal of Respiratory and Critical Care Medicine, 194(1), 106-113.• Rushton, C. H. (2016a). Moral resilience: a capacity for navigating moral distress in critical care. AACN Advanced Critical Care, 27(1), 111-119• Shanafelt, T. D., & Noseworthy, J. H. (2017). Executive leadership and physician well-being: nine organizational strategies to promote engagement and
reduce burnout. Mayo Clinic Proceedings, 92(1) 129-146.





























