Embed Size (px)
Citation preview
MANAGING MEDICAL PERFORMANCE
Mark Exworthy
21 May 2008
Outline
• Professional performance• Clinical performance• Disclosure of clinical performance data• Current ESRC project• St George’s Hospital • Theoretical perspectives
– Micro, meso and macro levels
Professional performance
• Professional resistance:– External accountability– Systemising work– Managerial control
• Minimalist strategy:– Notion of equality of competence– Only peer review permissible
• New frontiers of control?– From internal to external, implicit to explicit
• Performance = test of professional power
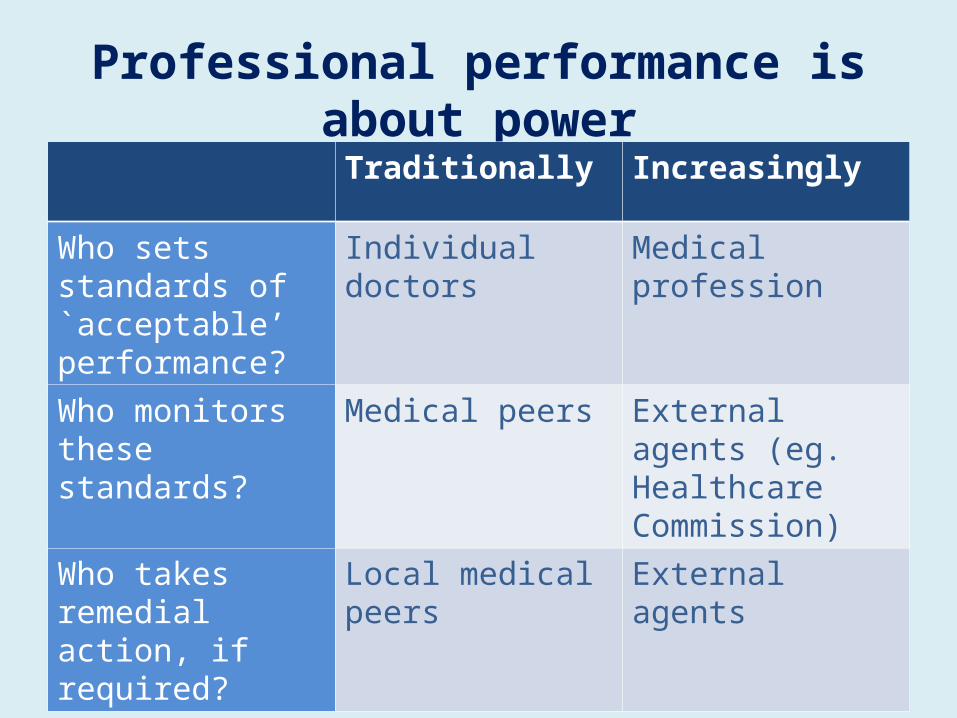
Professional performance is about powerTraditionally Increasingly
Who sets standards of `acceptable’ performance?
Individual doctors Medical profession
Who monitors these standards?
Medical peers External agents (eg. Healthcare Commission)
Who takes remedial action, if required?
Local medical peers External agents
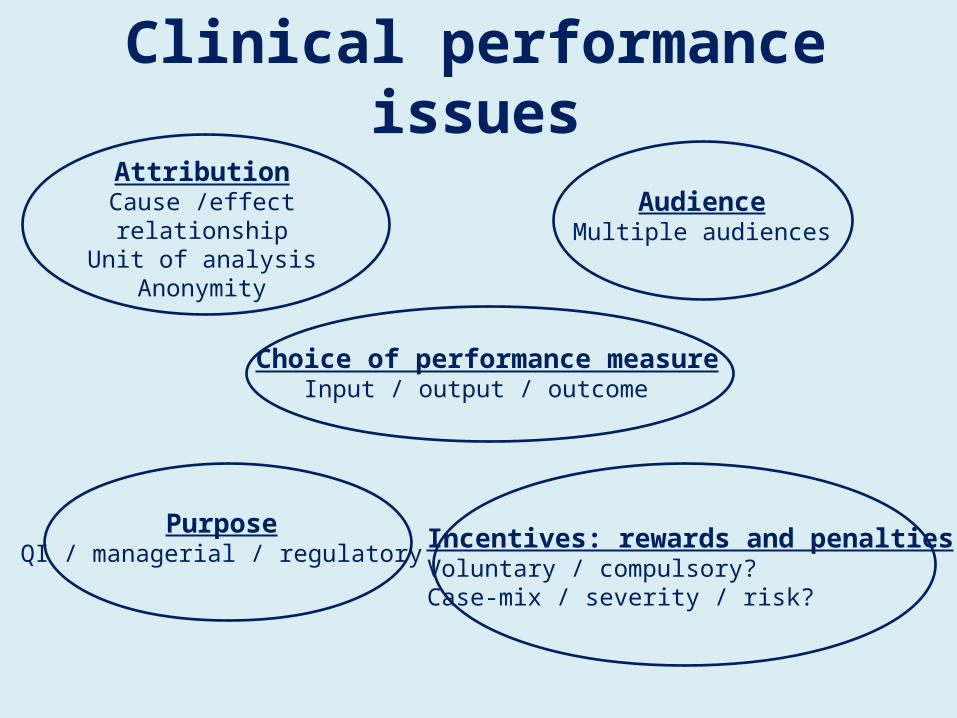
Clinical performance issuesAttribution
Cause /effect relationshipUnit of analysis
Anonymity
Choice of performance measureInput / output / outcome
AudienceMultiple audiences
PurposeQI / managerial / regulatory Incentives: rewards and penalties
Voluntary / compulsory?Case-mix / severity / risk?
Factors prompting disclosure of clinical performance
1. Patient `revolt’– Consumerism in health-care; `expert patient’
2. Media reporting of scandals– Bristol RI, Shipman, Neale, Ledward, Alder Hey etc
3. Freedom of information– 2000 Act applicable in UK since 2005
4. Modernisation of welfare– Challenge to established professions
5. Changing professionalism– Evidence-based medicine– Professional re-stratification– Re-professionalisation
6. International policy networks– Policy transfer
History of attempts to publish surgical outcome data in England
Health Secretary promises to publish hospital death rates for individual cardiac surgeons by 2004. Deadline missed.
Guardian newspaper uses Freedom of Information Act to gain and publish results – data variable and sometimes raw
Healthcare Commission requires all hospitals doing heart surgery to publish risk adjusted data on death rates for individual surgeons.
17 units provide data on individual surgeons – 13 units only provide aggregate data – 3 fail to provide any data by deadline.
Healthcare Commission website publishes results for units Rate of survival said to be well above expected range – overall survival 96.6% - expected range 93.7% to 94.5%
2002
2006
2007
NHS surgery success rates to be made publicJohn Carvel, Guardian
Tuesday 28 August 2007
A radical overhaul of NHS strategy which will give patients a right to know the success rates of every specialist unit in every hospital is being planned by leading surgeons and government officials.
For the first time, patients will be allowed to compare the quality of the clinical care provided in each NHS department. People with a particular medical condition will be able to assess the quality of the relevant specialist teams at rival NHS hospitals before choosing where to go for treatment. In some specialties, results for individual surgeons may be available.

Mortality at St George'shttp://www.stgeorges.nhs.uk/mortalityindex.asp
“At the time of writing we are the first hospital in the UK to publish inpatient death rates by clinical specialty.
This means that if you are a patient, relative, or member of the public, you can see how we have been performing in different clinical areas. Included is a careful explanation of how the graphs are worked out, how we adjust for risk-factors, and important caveats about what this information should not be used for.
As a leading centre in cardiac surgery, we also collect and analyse very detailed information about our performance in this area.
This section of the site contains 'raw' and risk adjusted mortality rates for individual surgeons, as well as information about post-operative quality.”
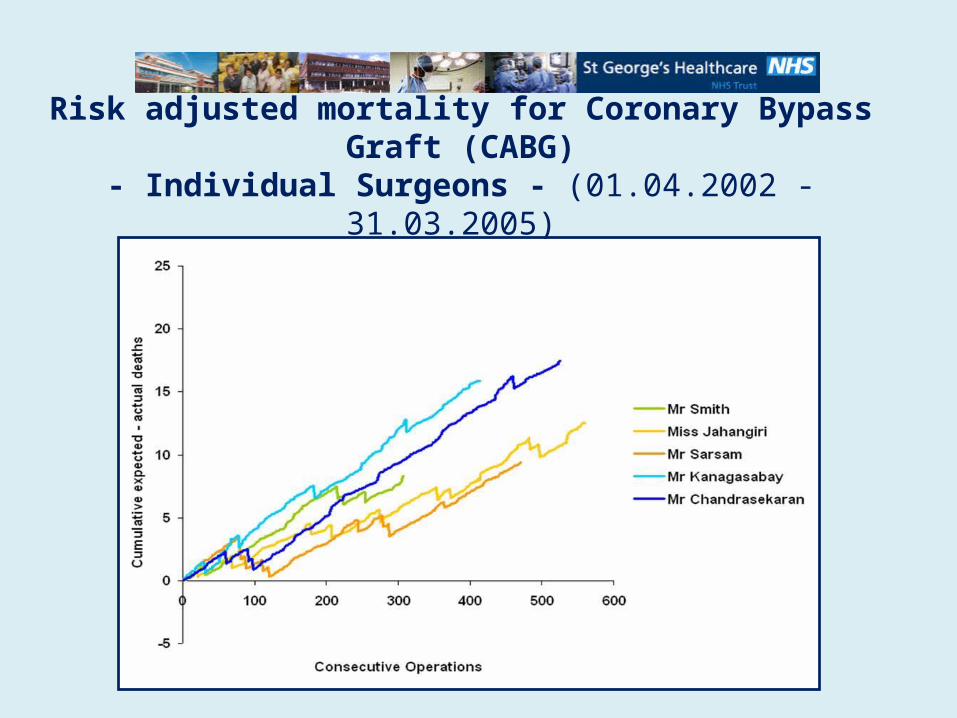
Risk adjusted mortality for Coronary Bypass Graft (CABG)- Individual Surgeons - (01.04.2002 - 31.03.2005)
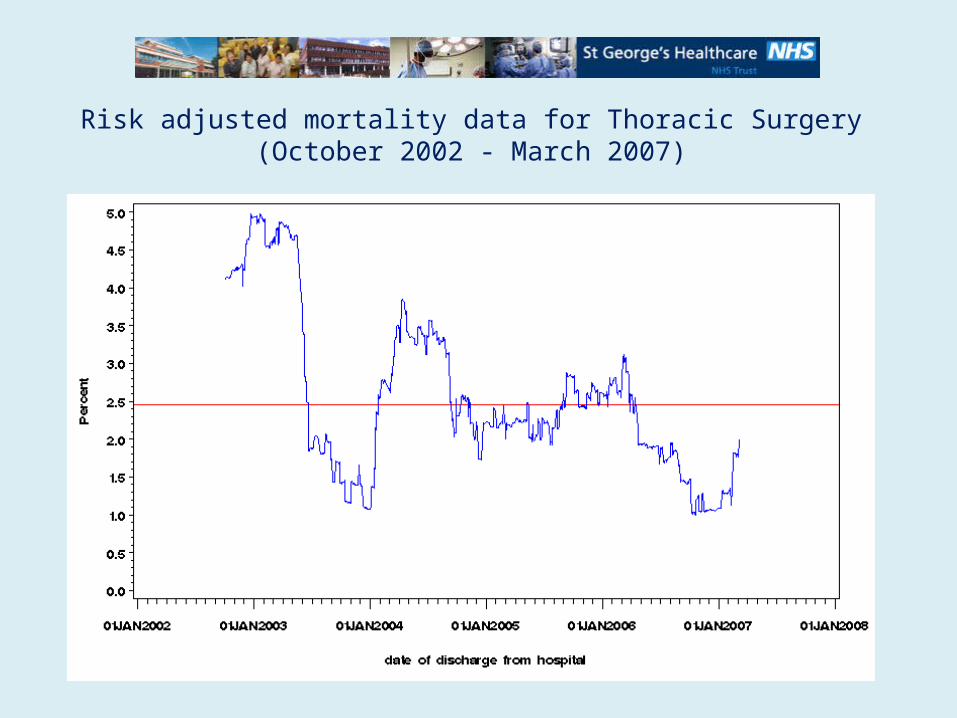
Risk adjusted mortality data for Thoracic Surgery(October 2002 - March 2007)
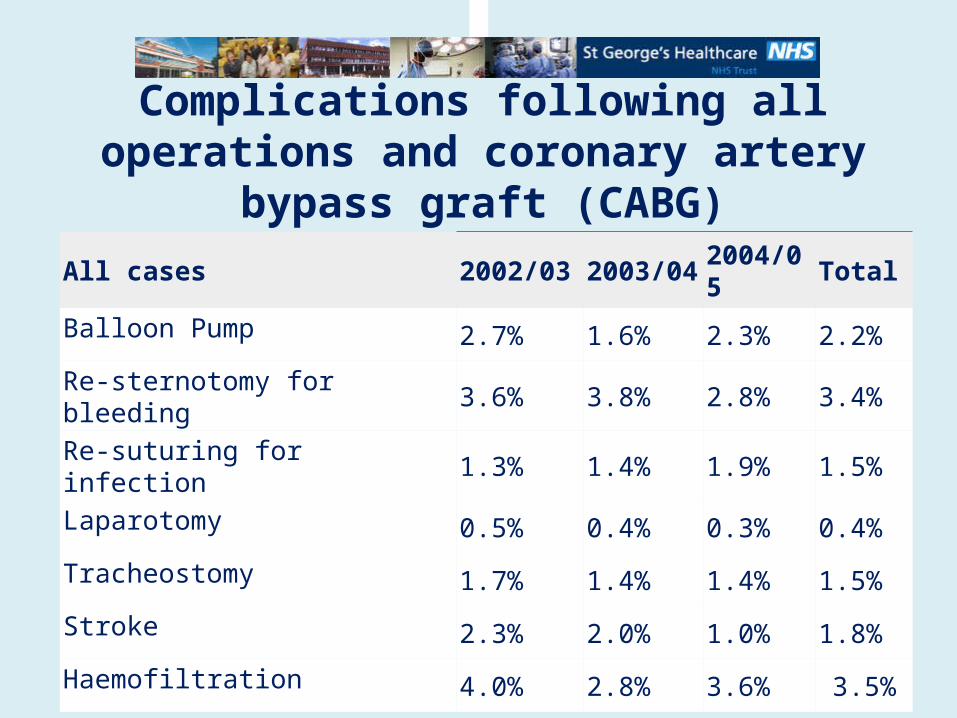
Complications following all operations and coronary artery bypass graft (CABG)
All cases 2002/03 2003/04 2004/05 Total
Balloon Pump 2.7% 1.6% 2.3% 2.2%
Re-sternotomy for bleeding 3.6% 3.8% 2.8% 3.4%
Re-suturing for infection 1.3% 1.4% 1.9% 1.5%
Laparotomy 0.5% 0.4% 0.3% 0.4%
Tracheostomy 1.7% 1.4% 1.4% 1.5%
Stroke 2.3% 2.0% 1.0% 1.8%
Haemofiltration 4.0% 2.8% 3.6% 3.5%

International experience• Sweden
– National quality registries, mainly since 2000
• Australia– Public hospital report, announced 2008
• Germany– Hospital reports, since 2005
• USA– Report scorecards. Eg. New York from `89
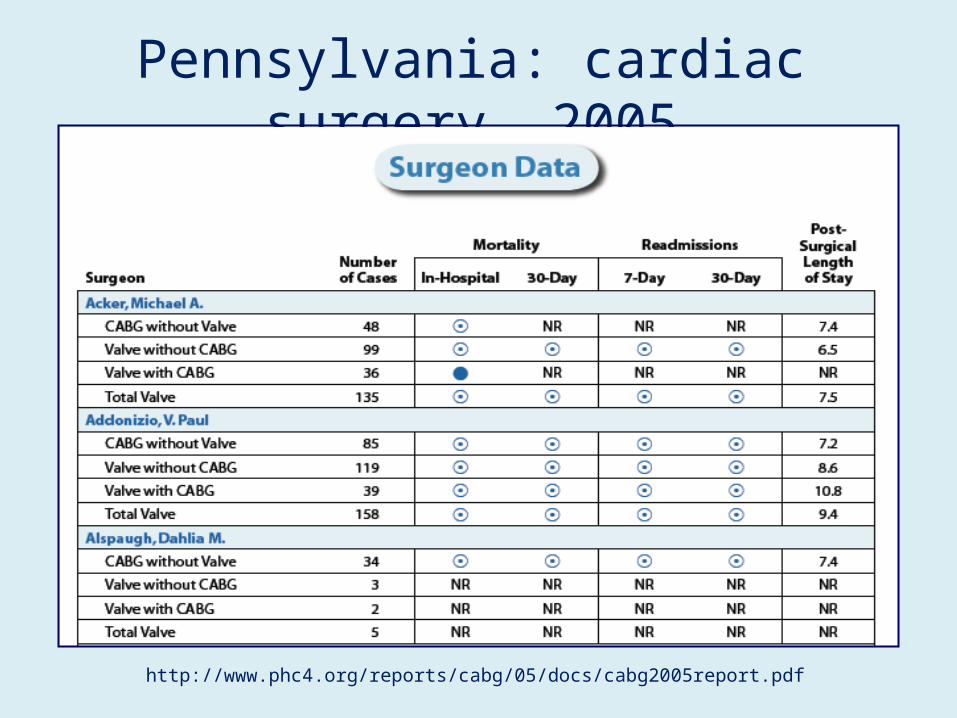
Pennsylvania: cardiac surgery, 2005
http://www.phc4.org/reports/cabg/05/docs/cabg2005report.pdf
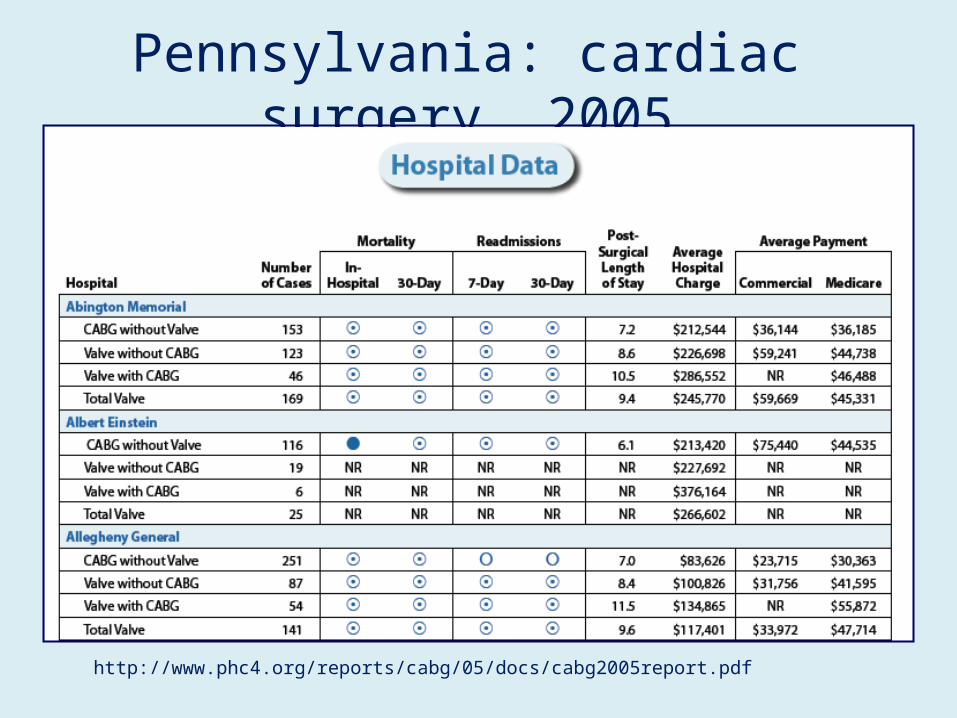
Pennsylvania: cardiac surgery, 2005
http://www.phc4.org/reports/cabg/05/docs/cabg2005report.pdf
Disclosure of clinical performance data
Extant evidence suggests...• Limited use of published performance data• Data are often crude, ambiguous, difficult to
interpret• Published data are available to managers /
external agents previously• Reasons for disclosure are complex and overlap:
– Perception of transparency• Avoids potential intrusive surveillance later
– Reputation (Patient Choice policy)
Project: Managing Medical Performance: a pilot study to investigate the impact of surgical performance upon clinicians and managersTeam:
Dr. Mark Exworthy (PI; RHUL)Prof. Jon Gabe (RHUL)Prof. Ian Rees Jones (Bangor University)Dr. Glenn Smith (RHUL, from 1 July 2008)
Time: 1 year, 2008-2009
Funding: ESRC Public Services Programme (3rd call)www.publicservices.ac.uk
Managing medical performanceResearch questions
1. To investigate the inter-connections between theoretical perspectives in terms of the motives, meanings and impacts of competing notions of performance upon cardiac surgeons, other clinicians, hospital managers, regulators and policy-makers.
2. To conduct an empirical investigation of the motives, meanings and impacts of (published) performance data upon cardiac surgeons, other clinicians, institutional managers and external regulators and policy-makers, so as to inform a wider study of medical performance and governance.
Managing medical performance: multi-level analysis
• Micro-level:– Inter-professional relations– Socialisation of surgeons
• Meso-level:– Use of data by managers– Impact on organisational culture
• Macro-level:– Impact of / on regulatory regime of performance
disclosure
Theoretical perspectivesMicro-level
• Soft governance– Complete control impossible– Rigid exterior with loosely coupled practices– Senior professionals
• Key organisational role but possess weak external powers• Senior professionals play role in legitimation
• Re-stratification– Not de-professionalisation but re-professionalisation– Disclosure promotes admin elite interest vis-a-vis
rank-and-file professional
Theoretical perspectivesMeso-level
• Panoptic surveillance– External gaze at internal practices– `Calculating selves’– Control at a distance
• Structural interests– Do managers challenge or collude with
professionals?– Is there a challenge to medical power (eg.
questioning merits of surgery)?
Theoretical perspectivesMacro-level
• Regulation – Self-regulation under threat?
– Role of the GMC and Healthcare Commission
• State-profession `contract’ – Re-alignment between state and profession relationship
– How far is the profession itself changing?• Role of Royal Colleges & professional bodies