Embed Size (px)
Citation preview

Prepared for the Auditor General for Scotland
Better equipped to care? Follow-up report on managing medical equipment
February 2004

Auditor General for ScotlandThe Auditor General for Scotland is the Parliament’s watchdog forensuring propriety and value for money in the spending of public funds.
He is responsible for investigating whether public spending bodiesachieve the best possible value for money and adhere to the higheststandards of financial management.
He is independent and not subject to the control of any member of theScottish Executive or the Parliament.
The Auditor General is responsible for securing the audit of the ScottishExecutive and most other public sector bodies except local authoritiesand fire and police boards.
The following bodies fall within the remit of the Auditor General:
• departments of the Scottish Executive eg the Health Department• executive agencies eg the Prison Service, Historic Scotland• NHS boards and trusts• further education colleges• Scottish Water• NDPBs and others eg Scottish Enterprise.
AcknowledgmentsAudit Scotland is grateful to those who acted as advisors to the study.We would like to thank the wide range of NHS Scotland staff whoparticipated in the audit.
The study team was Fiona Gailey, Catherine Vallely, Rhona Jack, andCraig McKinlay under the general direction of Barbara Hurst, Director ofPerformance Audit (Health & Community Care).
Audit Scotland is a statutory body set up in April 2000under the Public Finance and Accountability (Scotland) Act2000. It provides services to the Auditor General forScotland and the Accounts Commission. Together theyensure that the Scottish Executive and public sector bodiesin Scotland are held to account for the proper, efficient andeffective use of public funds.
Contents1
Main findingsPage 2
Part 1. IntroductionPage 4
Why medical equipment is importantPage 4
Our baseline studyPage 4
The follow-up auditPage 5
Part 2. Strategic management ofmedical equipmentPage 6
Main findingsPage 6
Why strategic input is neededPage 6
Strategic management at nationallevelPage 7
Strategic management at local levelPage 8
RecommendationsPage 10
Part 3. Risk managementPage 11
Main findingsPage 11
Good risk management processesare essential Page 11
Supporting risk management atnational levelPage 12
Risk management and risk exposureat local levelPage 13
RecommendationsPage 21
Part 4. Information to supportmanagementPage 22
Main findingsPage 22
Why management information isimportantPage 22
Sources of medical equipment dataPage 22
Quality of management informationPage 25
Using the management informationPage 26
RecommendationsPage 33
Appendix 1.Key points from Equipped to Careexecutive summaryPage 34
Appendix 2.Definition of medical equipment usedin this auditPage 35
Appendix 3.Membership of study advisory panelPage 38
Appendix 4.Trust operating income, 2001/02Page 39

2
Main findings
We did not follow up the more operational aspects of managing medical equipment, where our baseline work highlighted widespread good practice.
Main findings 3
Our follow-up audit of themanagement of medical equipmentinvolved all trusts
1, health boards
2and
the Scottish Executive HealthDepartment (SEHD). We havereviewed progress across Scotlandsince we published good practiceguidelines and recommendations inour 2001 report, Equipped to Care
3.
We did not follow-up the moreoperational aspects of managingmedical equipment, where ourbaseline work highlightedwidespread good practice. Wefocused on the main performanceissues arising from our baselinestudy, and found that:
• There are still significant risksfor patients where medical equipment is not managedwell, and there remainssubstantial room forimprovement across Scotland.
• There is limited strategic involvement in themanagement of medicalequipment at both national andlocal levels, so the SEHD andNHSScotland cannot be surethat any gaps between equipment needs andresources are being addressed.Trust boards need sufficient investment to replace medical equipment as it ages and to meet changes in services and technology.
• Progress is being made on riskmanagement at local level tosupport the delivery of highquality care. Overall, trustsfollow good practice for mostkey areas of medicalequipment policy. This includes
policies for acquiring and usingmedical equipment. But trustsneed to do more to show howthey are managing the risksassociated with operator errorand maintenance.
• Trusts lack the information tomanage their medicalequipment effectively. Thismeans that it is still notpossible to provide a clearpicture of key aspects of thecost, availability and use ofmedical equipment, andbenchmarking is impossible.
1 The term ‘trust’ includes island health boards throughout this report.2 During the course of this audit, the structure of NHSScotland began to evolve towards NHS boards with operating divisions. Our recommendations reflect these
new arrangements.3 Equipped to Care. Managing Medical Equipment in the NHS in Scotland. Audit Scotland, March 2001. Key points from the executive summary of this report are in
Appendix 1.

Part 1. Introduction
1.1 In this chapter we outline:
• the importance of managingmedical equipment
• our baseline audit
• the scope of our follow-up audit.
Why medical equipment is
important
1.2 Medical equipment is essential togood patient care. It is used in thecare of every patient and by mostfront-line staff. Some equipment isused for diagnosis, including X-rayand laboratory equipment. Otherequipment is used to treat patients,including radiotherapy machines,operating department andrehabilitation equipment. Theincreasing sophistication of medicalequipment can provide benefits topatients through better clinicaloutcomes and new, less invasivetechniques. There are also benefitsto the NHS, including shorter hospitalstays and the ability to treat morepatients.
1.3 Managing medical equipment iscomplex. Ensuring that the rightpiece of equipment is in the rightplace at the right time, together withtrained staff to use it, is a majorchallenge. The range of staff involvedin managing medical equipmentmeans that good coordination isrequired. Risks to patients and staffcan arise if medical equipment is notavailable when needed, not fullyfunctional and safe, or not usedproperly. Failure to manage theserisks can result in poor quality patientcare and lead to clinical negligenceclaims.
1.4 The investment in medicalequipment is substantial. Medicalequipment includes high cost, lowvolume items such as CT or MRIscanners
4and low cost, high volume
items such as blood pressuremonitors. Both types need to bemanaged well. Equipment can befinanced by capital procurement orlease for high cost items, andthrough revenue expenditure for lowcost items.
1.5 Management informationcontinues to be inadequate, so it isstill not possible to provide a clearpicture of key aspects of medicalequipment and assurances of valuefor money. We had to make specialarrangements to collect andcoordinate basic management data.Medical equipment purchased fromcapital in 2001/02 is estimated atover £60 million with a further £25 million purchased from revenuefunds. More than £44 million is spenton maintenance each year coveringequipment with an estimatedreplacement value of more than£630 million
5.
Our baseline study
1.6 Our baseline study was carriedout at local level on behalf of theAccounts Commission and so thenational position, including the SEHDrole, was outwith its scope. Althoughnot all trusts, health boards and theSEHD were included in this audit, ourkey findings and recommendationswere for all those with a role inensuring good planning andmanagement of NHSScotlandmedical equipment.
4 Descriptions of selected examples of equipment can be found in Appendix 2.5 See Exhibits 14 and 15 for expenditure details.
4

Part 1. Introduction 5
1.7 In Equipped to Care wehighlighted that trusts were good atmanaging many operational aspectsof medical equipment. For example,we found that finance departmentsensure compliance with EUprocurement legislation and standingfinancial instructions. And cliniciansreported satisfaction with responsetimes for equipment repairs.
1.8 But we also drew attention tothree key weaknesses where themanagement of medical equipmentcould be improved:
• lack of strategic involvement
• high exposure to risks
• lack of adequate information formanaging medical equipment.
The follow-up audit
1.9 We did not follow-up the moreoperational aspects of managingmedical equipment where ourbaseline work highlightedwidespread good practice. Instead,we focused on the main areas ofweakness highlighted above.
1.10 The follow-up audit was carriedout in trusts, health boards
6and the
SEHD. During the course of thisaudit, the structure of NHSScotlandbegan to evolve towards NHS boardswith operating divisions. Althoughour findings relate to the previousNHSScotland structure, ourrecommendations reflect these newarrangements.
1.11 Our audit approach wasdeveloped in consultation with astudy advisory panel (see Appendix 3for membership of the group).
1.12 In December 2002, we askedtrusts to complete a self-assessmentquestionnaire. This focused on themain areas where scope forimprovement was highlighted in ourbaseline report. External auditorsvalidated the completedquestionnaires.
1.13 External auditors also carried outa limited review at the 12 mainlandhealth boards about their strategicrole in relation to medical equipment.And we looked at the SEHD’sstrategic role in relation to medicalequipment.
1.14 The main messages arisingfrom our follow-up audit relate to:
• strategic management (Part 2)
• risk management (Part 3)
• management information (Part 4,and included in Parts 2 and 3).
1.15 Our key recommendations arehighlighted at the end of eachchapter and these supplement localactions plans.
6 Our follow-up audit did not include the special health boards.

6
Part 2. Strategic management of medicalequipment
Main findings
Strategic management of medicalequipment needs to be given ahigher priority at national and locallevels. Responsibility for medicalequipment is not always clear andpolicymakers still view medicalequipment only as an operationalissue.
We believe that there are somelimitations in the way the SEHDholds NHSScotland to account forplanning and providing medicalequipment to meet local needs inline with national strategies. Healthboards have not made clear whatinformation they require from trustsfor performance monitoring purposes.
Approximately two-thirds of trustboards cannot show that theirinvestment programmes arebased on realistic forward planningfor medical equipment or thatinvestment is sufficient to meetclinical governance requirementsor service priorities.
All trusts lack the information tomanage their medical equipmenteffectively. This means that it is
still not possible to provide a clearpicture of key aspects of the cost,availability and use of medicalequipment, and benchmarking isimpossible.
2.1 This chapter looks at strategicinvolvement in medical equipment atnational and local levels.
Why strategic input is needed
2.2 A strategic overview of medicalequipment is needed to make sure:
• the current level and condition ofmedical equipment is broadlyknown
• current and future needs formedical equipment are properlyassessed, so that the level andtype of medical equipment in useis in line with national and localhealthcare strategies, and supportsplanned service developments
• priorities for meeting equipmentneeds are agreed and resourced
• day-to-day management ofmedical equipment is carried outeffectively.
This will help ensure patient and staffsafety, support quality of care andachieve value for money.
2.3 Robust information is needed tosupport the planning and governanceof medical equipment at national andlocal level to show whether:
• levels of equipment are adequatefor identified healthcare needs
• rolling programmes of equipmentreplacement and additionalinvestment are adequate
• health & safety requirements aremet
• financial management is rigorousand is used to support effectivemanagement of equipment
• benchmarking is being used byNHSScotland organisations aspart of their performancemanagement processes
• value for money is beingachieved.

Part 2. Strategic management of medical equipment 7
Strategic management at national
level
Planning, needs assessment and
resource allocation
2.4 At a national level, the SEHD’sinvolvement is needed to ensure thatmedical equipment is available tosupport national strategies andclinical priorities.
2.5 Most responsibility for planning,needs assessment and resourceallocation is delegated to healthboards to allow them to decide localpriorities. The SEHD is generally onlydirectly involved in local plans toinvest in medical equipment when a business case needs to beapproved
10. Most funds are
distributed to health boards as part oftheir overall allocation
11.
2.6 However, the SEHD can getinvolved where national policy issuesimpact on medical equipmentrequirements, for example, for
cancer services (Exhibit 1). The aimof this approach is to ensure that theclinical and operational aspects ofdelivering care for cancer patientscan be delivered as a whole package.
Accountability at national level
2.7 The SEHD’s role is to ensure thathealth boards are discharging theirdelegated responsibilities effectively.As part of this, the SEHD has newlyintroduced a requirement to discloseforward capital investment in medicalequipment as part of the financialplanning regime that supports thelocal health plans.
2.8 There are also arrangements inplace for safety and clinicalgovernance issues to be consideredat national level. For example:
• The SEHD expects medicalequipment to be operated in linewith manufacturers’ instructionsas well as meeting any regulatoryrequirements such as the
radiological protection regulationscovering imaging devices.
• The SEHD has agreed to workwith the National Institute forClinical Excellence in England todevelop proposals to regulate theuse of new surgical instrumentsor existing instruments in newand innovative procedures.
• The Chief Medical Officer hasoverall responsibility for the safetyand efficacy of medicalequipment. The Medicines andHealthcare products RegulatoryAgency (MHRA) regulates this ona UK-wide basis.
• The SEHD has delegatedresponsibility for inspecting thequality of the healthcare systemto NHSQIS, and their standardsetting and review of a specificclinical area can involve medicalequipment.
7 A nuclear medicine imaging technique.8 Now part of NHSScotland Quality Improvement Scotland (NHSQIS).9 NSD is part of the NHSScotland Common Services Agency.10 NHS HDL (2002) 40, Capital Planning and Approval Processes.11 The allocation is made through the Arbuthnott formula, adjusted for cross-boundary flows and weighted to take account of regional specialist services.
1. Setting up a national group to look at Positron Emission Tomography (PET)7scanners in response to a report by
the Health Technology Board for Scotland (HTBS)8.
2. Commissioning a national programme for breast screening which is managed through the National ServicesDivision
9(NSD) and which has a rolling programme to replace mobile screening vans and associated
mammography equipment.
3. Spending about £1.4 million through NSD to introduce Liquid Based Cytology into the cervical screeningprogramme, which included equipment and training.
Exhibit 1Examples of SEHD input to the management of medical equipment for cancer care
Source: SEHD, 2003

8
2.9 The SEHD believes it dischargesits role in holding NHSScotland toaccount for its management ofmedical equipment by addressing itwithin policy areas such as cancer.The department’s aim is to ensurethat the clinical and operationalaspects of delivering care for cancerpatients can be delivered in a holisticway. In our view, the SEHD’sapproach has some limitations:
• It tends to focus on new and highcost items. But the level andstate of the existing stock ofmedical equipment including lowcost items also needs to beaddressed. The new requirementabout disclosing capitalinvestment will only give a partialview as it does not cover lowcost, high volume items.
• Items of medical equipment areoften used across policy areas; forexample, MRI scanners are usedto help diagnose a range ofconditions, not just cancer.
• It does not enable SEHD to holdNHS boards to account for theoverall planning and provision ofmedical equipment to meet localneeds in line with nationalstrategies. Medical equipment isnot directly covered by thePerformance AssessmentFramework (PAF) and is notroutinely covered in AccountabilityReviews.
The approach also contrasts with theDepartment of Health (DOH) inEngland which has introduced aspecific standard for managingmedical devices as part of its controlsassurance requirements for theNHS.
12
We recommend that the SEHDshould take a coordinated approachto the governance of medical
equipment and specify its reportingrequirements. This would enable thedepartment to routinely monitor themangement of all medicalequipment, not just items boughtfrom capital, in Accountability Reviewmeetings.
Strategic management at local
level
2.10 Health boards have a strategicrole in managing medical equipmentbut are not involved in day-to-dayoperational matters. They need to besure that their trusts have themedical equipment to deliverappropriate care for the localpopulation, in line with nationalpolicies and clinical priorities. Thismeans proper arrangements need tobe put in place to ensure clarity ofresponsibility, adequate needsassessment, appropriate prioritisationof expenditure, and performancemanagement and reporting.
Planning, needs assessment and
resource allocation
2.11 Health boards and over three-quarters of trust boards continue toview medical equipment only as anoperational issue. (Exhibit 2 highlightsthe six trust boards that were able todemonstrate important aspects ofstrategic involvement). Policymakers,overall, are not involved in medicalequipment needs assessments,performance monitoring andmanagement, and in ensuring accessto sufficient resources to meetpatient need. For example, onlyabout half of trust boards have needsassessment reports and medicalequipment investment programmeson their agendas. And approximatelytwo-thirds of trust boards cannotshow that their investmentprogrammes are based on realisticforward planning for medicalequipment or that investment issufficient to meet clinical governancerequirements or service priorities.
Accountability at local level
2.12 There is seldom an individual orgroup with overall responsibility formedical equipment throughout thehealth board area. But examples ofgood practice in accountabilityarrangements are beginning toemerge. For example, in Dumfries &Galloway, a member of the new NHS board has been given leadresponsibility for medical equipmentand it is developing an area-wide‘Equipped to Care Committee’.
2.13 In Equipped to Care werecommended that responsibility formedical equipment be delegated tosomeone on the trust boardsupported by a multidisciplinarygroup. At trust level, almost half stillhave no executive directorresponsible for medical equipment(Exhibit 2), and a third of trusts do nothave a broad-based committee (orarea-wide alternative) that deals withmore than equipment funding bids.A broad-based medical equipmentcommittee is one that is involved inplanning, needs assessment andother aspects of medical equipmentmanagement.
2.14 Performance monitoring ofmedical equipment is limited at locallevel. Neither health boards nor trustboards have made clear theirperformance reporting requirements.Three-quarters of trusts had notsubmitted any type of formal reportabout medical equipment to theirhealth board, and when they do,these tend to be about financialissues such as major capitalexpenditure or public privatepartnership projects. Also, trustreporting to trust boards tends tofocus on finance rather than qualityof care, (Exhibit 3 overleaf).
12 Medical Devices Management Standard, Department of Health, October 2001 (revised 2003).

Part 2. Strategic management of medical equipment 9
Trust & Island Health Boards
There is an
executive
director with
specific overall
responsibility
for medical
equipment
management.
There is a
broad-based
medical
equipment
committee
(trust or area).
There are
reporting
arrangements
and
accountabilities
for medical
equipment
which are
clear.
We have
received a
report(s) on
progress
towards
implementing
the good
practice
guidelines in
Equipped to
Care.
We can
demonstrate a
formal medical
equipment
investment
programme,
which enables
realistic
forward
planning.
Argyll & Clyde Acute Hospitals Trust ✓ ✓ ✓ ✗ ✗
Ayrshire & Arran Acute Hospitals Trust ✓ ✓ ✓ ✓ ✓
Ayrshire & Arran PCT ✓ ✓ ✓ ✓ ✓
Borders General Hospitals Trust ✓ ✓ ✗ ✓ ✗
Borders PCT ✗ ✗ ✗ ✗ ✗
Dumfries & Galloway Acute Hospitals Trust ✗ ✓ ✓ ✗ ✓
Dumfries & Galloway PCT ✗ ✓ ✓ ✗ ✓
Fife Acute Hospitals Trust ✓ ✓ ✓ ✗ ✗
Fife PCT ✓ ✓ ✓ ✓ ✗
Forth Valley Acute Hospitals Trust ✗ ✓ ✓ ✓ ✓
Forth Valley PCT ✗ ✗ ✗ ✗ ✗
Grampian PCT ✗ ✗ ✗ ✓ ✗
Grampian University Hospitals Trust ✓ ✓ ✓ ✓ ✓
Greater Glasgow PCT ✓ ✓ ✗ ✗ ✗
Highland Acute Hospitals Trust ✓ ✓ ✓ ✓ ✗
Highland PCT ✗ ✗ ✓ ✗ ✗
Lanarkshire Acute Hospitals Trust ✓ ✗ ✓ ✗ ✗
Lanarkshire PCT ✓ ✓ ✓ ✓ ✓
Lomond & Argyll PCT ✓ ✓ ✓ ✗ ✗
Lothian PCT ✗ ✓ ✗ ✗ ✓
Lothian University Hospitals Trust ✓ ✓ ✓ ✓ ✗
North Glasgow University Hospitals Trust ✗ ✓ ✗ ✓ ✓
Renfrewshire & Inverclyde PCT ✗ ✗ ✓ ✗ ✗
South Glasgow University Hospitals Trust ✗ ✓ ✓ ✓ ✓
Tayside PCT ✓ ✓ ✗ ✗ ✗
Tayside University Hospitals Trust ✓ ✓ ✓ ✓ ✓
Yorkhill Trust ✓ ✓ ✓ ✓ ✓
West Lothian Healthcare Trust ✗ ✗ ✓ ✗ ✗
Western Isles Health Board ✓ ✗ ✗ ✗ ✗
Shetland Health Board ✗ ✗ ✓ ✗ ✓
Orkney Health Board ✗ ✓ ✗ ✗ ✗
Source: Audit Scotland, 2003
Exhibit 2Important aspects of strategic involvement in medical equipment by trust boards
Only six trust boards were able to demonstrate these five important aspects of strategic involvement.

10
Exhibit 3Trust staff reporting to trust boards on medical equipment matters
2.15 But some health boards take amore active interest in medicalequipment managementperformance. For example, LothianHealth Board requires postimplementation reviews of specificprojects, and medical equipment ison the agenda for their trustaccountability reviews. Ayrshire &Arran, Dumfries & Galloway andGrampian Health Boards followed upthe recommendations from Equippedto Care with their local trusts toensure that medical equipment isbeing managed effectively. Andexamples of good practice inaccountability at trust level includefive trust boards having received thereports about medical equipmentclinical governance mattershighlighted in Exhibit 3: Ayrshire &Arran Acute Hospitals Trust, FifeAcute Hospitals Trust, GreaterGlasgow PCT, Lanarkshire AcuteHospitals Trust and Yorkhill Trust.
Recommendations
National1. The SEHD should consider
introducing a specific medicalequipment management standardto provide assurances that properstrategic and operational practicesare in place.
2. The SEHD should improvegovernance and accountability formedical equipment by usingperformance information toinform Accountability Reviews.This should include seekingassurances that any gapsbetween equipment needs andresources are being addressed.
Local3. NHS boards should assign
responsibility for all aspects ofmedical equipment in the area toan executive board member,supported by a multidisciplinarygroup. This would help ensurethat medical equipment isavailable to deliver care in linewith national strategies andclinical priorities.
4. NHS boards should ensure thattheir operating divisions haveprocesses in place to assess theirmedical equipment needs andagree priorities. They should alsoensure that medical equipmentinvestment programmes arebased on realistic forwardplanning.
5. NHS boards should specify theirreporting requirements formedical equipment and monitoroperating division performanceregularly.
6. Operating divisions should ensurethat responsibility for medicalequipment is clear throughouttheir organisations.
Overall, trust boards are better informed of medical equipment financial matters than they are of clinical
governance issues. Seven trust boards had not received any reporting at all for key clinical governance
issues.
Medical equipment matters Percentage
reporting
Clinical governance reporting • Risk analyses 58%to trust boards • Policies & procedures 55%
• Needs assessment 48%• Training 45%• Quality assurance, including accreditation 32%
Financial reporting to trust boards • Expenditure: capital 97%revenue 65%
• Funding bids 87%• Depreciation levels 71%• Medical equipment replacement programme 55%
Source: Audit Scotland, 2003
11
Part 3. Risk managementPart 3. Risk management
Main findings
The SEHD should do more to helpNHSScotland reduce riskexposure. The national riskmanagement scheme, CNORIS,has not brought about thereduction in risk expected whenwe published Equipped to Care.
The SEHD should make better useof information from existingnational information systems,including the Adverse Incidentreporting scheme, to identify risksand keep local health servicesinformed of them.
Some trusts are still relying heavilyon old equipment. Trust boardsneed sufficient investment toreplace medical equipment as itages and to meet changes inservices and technology.
Progress is being made on riskmanagement at local level.Overall, trusts follow good practicefor most key areas of medical
equipment policy, includingmanaging clinical incidentsinvolving medical equipment.
But trusts need to do more toshow how they are managingrisks associated with operatorerror and maintenance. Forexample, trusts must improve themanagement of staff training,such as systematically planningand recording the training receivedby healthcare staff for usingmedical equipment.
3.1 In this chapter, we review thenational arrangements to help riskmanagement of medical equipmentat local level. We then focus on thelocal level by examining riskmanagement arrangements andspecific medical equipment risks.
Good risk management processes
are essential
3.2 The aims of risk management areto avoid harming patients and staff,and to limit financial risk.
3.3 Using medical equipment carriesrisks:
• a patient, user, carer orprofessional can be injured as aresult of a medical device failureor its misuse
• a patient’s treatment can beinterrupted or compromised by amedical device failure
• a misdiagnosis can be made dueto medical device failure, resultingin inappropriate treatment
• a patient’s health can deterioratedue to a medical device failure
13.
Our baseline report included a seriesof recommendations and a goodpractice checklist to improve medicalequipment risk management inNHSScotland. This checklist is basedon guidance from the former MedicalDevices Agency
14.
13 Controls Assurance, Medical Devices Management Standard, Department of Health, 2003.14 Now, Medicines and Healthcare products Regulatory Agency (MHRA).

12
Supporting risk management at
national level
3.4 The SEHD has a supporting rolein managing risk at local level so thatcommon problems are identified andaction is taken to avoid recurrence. InEngland, the DOH has introduced aMedical Devices ManagementStandard as part of its controlsassurance system for the NHS. Thesystem provides the DOH withassurances that the risks associatedwith the acquisition and use ofmedical devices are minimised
15. The
outcomes of trust controls assuranceassessments are published on theDOH website. In addition, the DOHpublishes a summary of trustreported medical equipment risks.There is no equivalent in Scotland.
3.5 This section looks at the SEHDnational risk management scheme(CNORIS)
16, and the national Incident
Reporting and Investigation Centre.
The national risk management
scheme (CNORIS)
3.6 The national risk managementscheme for NHSScotland, CNORIS,is a compulsory insurance schemecovering clinical and non-clinical risks.Risks are assessed against an agreedset of standards. CNORIS operateson three levels (Exhibit 4). Levels twoand three can give real assurancesthat formal risk managementprocedures work, including those formedical equipment. AlthoughCNORIS does not have a specificstandard for medical equipment,aspects are included in somestandards. For example, the ClinicalIncident Reporting and ManagementStandards cover the use of medicalequipment
17.
3.7 By December 2002, only two-thirds of trusts and island healthboards had achieved the minimumstandard, CNORIS level one. Veryfew trusts had applied for level two,and no trust had achieved it.Therefore, trusts were not able to
use their CNORIS level rating todemonstrate that they had effectiverisk management processes in place.
3.8 The SEHD has decided to changethe national risk managementscheme from 1 April 2004
18. The
Healthcare Risk ManagementStandards established by CNORISare being merged with the NHSQISGeneric Clinical GovernanceStandards
19. Like CNORIS, NHSQIS
does not have a specific standard formedical equipment, but somestandards refer to it. There is now anopportunity for NHSScotland toconsider implementing a specificmedical devices managementstandard along the lines introducedby the DOH
20.
The national Incident Reporting and
Investigation Centre
3.9 The SEHD set up a nationalIncident Reporting and InvestigationCentre
21within Scottish Healthcare
Supplies (SHS)22. SHS investigates
adverse incidents that involve the
Exhibit 4Summary of CNORIS Healthcare Risk Management Standards
15 The standard includes 31 criteria of good practice for managing medical equipment. 16 Clinical Negligence and Other Risks (Non-clinical) Indemnity Scheme (CNORIS), NHS MEL(1999)86. 17 CNORIS Risk Management Standards, SEHD, July 2001.18 NHS HDL(2003)29. Clinical negligence and other risks indemnity scheme (CNORIS): integration of standards with NHSQIS generic clinical governance standards.
Standard Level Summary of CNORIS Healthcare Risk Management Standards
One Focuses on corporate ownership of risk through effective policies and procedures.
TwoSeeks evidence of implementation throughout the organisation and addresses operationalissues, in particular, challenging the organisation to strive for continual improvement.
Three
Necessitates a high degree of integration into culture and activities, and requires evidence thatthe organisation has dynamic risk management systems in operation, evidenced by continualimprovement.
Source: CNORIS Risk Management Standards, SEHD, July 2001

Part 3. Risk management 13
use of medical devices withinNHSScotland on behalf of the SEHD.Trusts must report on potential andactual problems covering, forexample: design and construction;user instructions, ease of operationand staff training; and technical oreconomic performance. SHS issuestop priority Hazard Notices (Exhibit 5)as well as standard Safety ActionNotices to help prevent problemsoccurring in the future. SHS alsoliaises with MHRA to keepNHSScotland up to date on problemsidentified elsewhere in the UK.
3.10 Currently, these adverseincident data are not centrallyanalysed or reviewed according totype of medical equipment incident,such as equipment failure or operatorerror. More use could be made ofthis management information toimprove the management of medicalequipment across NHSScotland. SHSis now looking at a system togenerate trend data of this type byApril 2004.
Risk management and risk
exposure at local level
3.11 NHS boards need to satisfythemselves that medical equipmentrisks are being managedappropriately. However, there are noformal reporting requirements onmedical equipment at local level, so itis not clear how boards know theextent of risk exposure. With theabolition of trusts, NHS boards havethe opportunity to ensure thatarrangements are consistent andcomprehensive across their areas. In this section, we examinearrangements for managing medicalequipment risks at local level, andspecific medical equipment risks.
Risk management arrangements
Risk management strategies3.12 Given the importance of medicalequipment in the provision of patientcare, local risk managementstrategies should include planningand using medical equipment. But42% of trust risk management
strategies included medicalequipment only in a partial way, and afurther 13% do not cover medicalequipment at all. The PCTs in ForthValley, Argyll & Clyde and Lothianparticularly need to develop their riskmanagement strategies to covermedical equipment.
Trust compliance with formal medical equipment policies3.13 Trusts have made progress inagreeing formal policies on acquiringand using medical equipment (Exhibit 6 overleaf). Theimplementation of these policieshelps to limit risk exposure. Forexample, a policy on commissioningnew equipment would set out whatneeds to be done when a device isfirst put into service: equipmentregisters need updating, staff mayneed training and a timetable ofplanned preventive maintenanceneeds to be established. Compliancewith the formal policy limits risk byhelping to ensure consistency inapproach and that all necessary tasks
Exhibit 5An example of Scottish Healthcare Supplies, Hazard Notice to NHSScotland
19 Formerly Clinical Standards Board for Scotland Generic Clinical Governance Standards. 20 Controls Assurance, Medical Devices Management Standard, Department of Health, England, October 2001 (revised 2003).21 NHS MEL(1995)74. Reporting of adverse incidents and defective equipment.22 Part of the Common Services Agency of NHSScotland.
Source: Scottish Healthcare Supplies, 2003
Risk of misconnection and over-compression
SHS recently issued a Hazard Notice where an incident had been reported in which a patient was injured as aresult of continuous high pressure being applied for some time to both legs by a sequential pressure device. The device is used to apply pressure to the lower limbs to help prevent deep vein thrombosis, for example, aftersurgery. The Notice advised that if a connection is damaged, the tubing set should be discarded.
Warning: Do not attempt to repair or replace broken tubing connectors as hazardous inflation of the sleeves may occur.

14
Exhibit 6Trust implementation of formal medical equipment policies
Trust staff mostly comply with formal policies for acquiring, commissioning and using medical equipment,
but there were four clear exceptions:
• Orkney Health Board could only demonstrate good practice for purchasing decisions, meeting health & safety requirements and reporting critical incidents
1.
• Lothian PCT could only demonstrate good practice for reporting critical incidents, meeting health & safetyrequirements, and using personal electronic equipment.
• Forth Valley Acute Hospitals Trust and Highland PCT could only demonstrate good practice for about half of thekey policy areas audited.
Medical equipment policies Percentage of
trusts
demonstrating
implementation
Acquiring medical equipment • Purchasing decisions 77%• Standardising on models of equipment 77%• Involving clinicians throughout the process 74%
Commissioning medical • Acceptance testing (eg, electrical testing) 90%equipment • Registering on inventories 87%
• Decommissioning of equipment 81%
Using medical equipment • Reporting critical incidents 100%• Health & safety requirements 97%• Personal electronic equipment
(eg, mobile phones) in clinical areas 87%• Maintenance and fault reporting 84%• Training 74%• Modified equipment 71%
Source: Audit Scotland, 2003
1 Critical incidents include clinical and non-clinical incidents where patient safety is at risk.

Part 3. Risk management 15
are completed. Overall, trusts couldshow that they generally follow goodpractice for most key areas ofmedical equipment policy. But therewere four clear exceptions: OrkneyHealth Board, Lothian PCT, ForthValley Acute Hospitals Trust andHighland PCT.
Specific medical equipment risks
3.14 The main risks to patient andstaff safety when using medicalequipment arise from inappropriatetraining and maintenance
23. Trusts
can reduce these risks bystandardising on makes and models.There are also other risks associatedwith the financial management ofequipment, including relying on olderequipment that may need to bereplaced at short notice and failing tomake adequate provision to replaceequipment.
Training3.15 According to the MDA
24,
operator error is the most commoncause of incidents involving medicalequipment. But only half of trustscould provide assurance that thoseoperating diagnostic or therapeuticequipment have a sufficientunderstanding of it to do so in a safeand efficient manner.
3.16 Training is a key element inreducing these risks. Training isprovided in a range of ways,including by equipmentmanufacturers and in-house trainers,all of which needs to be recordedand managed. But two-thirds oftrusts cannot identify theirinvestment in medical equipmenttraining. Therefore it is not clear howthese trust boards know how muchtraining is required and if they aremaking sufficient investment intraining. Also, Arygll & Clyde NHS,
Forth Valley Acute Hospitals Trust,Highland PCT, Lothian PCT, OrkneyHealth Board and Shetland HealthBoard could not demonstrate fromtheir training records that they adhereto medical equipment trainingpolicies. These training policiesgenerally state the requirement tomaintain records to demonstrate themedical equipment training receivedby healthcare professionals for usingspecific medical equipment.
Maintenance3.17 The other main risk to patientsafety is equipment problems as aresult of inadequate maintenance
25.
Trusts need to identify and plan forthe level of maintenance required formedical equipment and monitor itsdelivery. Equipment suppliers andmanufacturers, and NHS teams
26,
all provide trust equipmentmaintenance.
3.18 Four trusts could not identifytheir spend on maintenance and afurther 15 could only provide partialdata
27. No trust is involved in
maintenance benchmarking, so it isunclear how trusts could provideassurances that they are making bestuse of their maintenance resources.
3.19 While almost three-quarters ofthe trusts had undertaken a formalreview of medical equipment sincetrust reorganisation in 2001, almosthalf of trusts with in-housemaintenance did not include staffinglevels and skills as part of this review.Therefore, it is not clear how thesetrust boards know that theirinvestment in the in-housemaintenance team is appropriate.
3.20 External accreditation to arecognised quality standard for NHSmaintenance teams can provide
assurances of a quality service (Exhibit 7). But accreditation for in-house maintenance is notwidespread. Of the 23 trusts with in-house maintenance provision, only six are externally accredited,although some others have partialaccreditation. But Dumfries &Galloway Acute & MaternityHospitals Trust, Fife Acute HospitalsTrust, Forth Valley Acute HospitalsTrust, Highland Acute Hospitals Trust,Lothian University Hospitals Trust,Yorkhill Trust, plus the three islandhealth boards, all have in-housemaintenance with no externalaccreditation.
Standardisation3.21 As well as reducing safety risks,standardising equipment can helpreduce the cost of servicing andspares, and there may be benefitsfrom bulk purchasing. Exhibit 8demonstrates that there is stillconsiderable scope for furtherstandardisation across NHSScotland.Older models of equipment mayexplain this. But five trusts - FifeAcute Hospitals Trust, Forth ValleyAcute Hospitals Trust, Forth ValleyPCT, Renfrewshire & Inverclyde PCTand Tayside University HospitalsTrust – were not actively pursuing apolicy of standardisation for keyitems.
23 Medical device and equipment management for hospital and community based organisations, Medical Devices Agency (MDA) (now MHRA), 1998. 24 Now, MHRA. 25 The term maintenance is used in this report to cover all associated activities of repair, planned preventative maintenance, servicing, reconditioning, modification and
refurbishment, MHRA, 2000.26 For example, most acute trusts also provide maintenance services to other parts of the NHS.27 From the data available, about 38% of spend on medical equipment maintenance is for in-house maintenance.
Exhibit 7Medical devices and equipment management: repair and maintenance provision
Source: Medical Devices Agency (now MHRA), 2000
Quality Assurance Standards:
User organisations should only use a service provider who can demonstrate compliance with relevant qualitysystem standards, for example, BS EN 46002 or BS EN ISO 9002. Such systems provide a framework on whichservice providers can build the necessary structures to ensure their work is of the nature and quality intended.
16

Part 3. Risk management 17
Exhibit 8Number of different models for selected examples of medical equipment
Num
ber o
f tru
sts
Number of different models
0
2
4
6
8
10
12
14
1 - 3 4 - 6 7 - 9 10 - 12N
umbe
r of t
rust
s
Number of different models
0
2
4
6
8
10
12
1 - 3 4 - 6 7 - 9 10 - 12 13
Num
ber o
f tru
sts
Number of different models
0
1
2
3
4
5
6
1 - 3 4 - 6 7 - 9 10 - 12 13 - 16
7
8
Num
ber o
f tru
sts
Number of different models
0
1
2
3
4
5
6
1 - 3 4 - 6 7 - 9 10 - 12 21 - 3813 - 15 16 - 20
Num
ber o
f tru
sts
Number of different models
0
1
2
3
4
5
6
1 - 3 4 - 6 7
7
Source: Audit Scotland, 2003
Trusts are not always following good practice for standardising models of equipment.
Volumetric pumps Syringe pumps
Defibrillators ECG recorders
Dialysis machines

Perc
enta
ge ‘a
ge p
rofil
e’
0
20
40
60
80
100
Standard life of equipment
mostly 10 years 8 - 10 years 5 - 7 years
Within standard life
Reached standard life
Beyond standard life
Total number of items
Ang
iogr
aphi
c un
its
Volu
met
ric p
umps
Dia
lysi
s m
achi
nes
Gam
ma
Cam
eras
Den
tal X
-ray
units
Def
ibril
lato
rs
ECG
reco
rder
s
Fixe
d X-
ray
units
with
flur
osco
py
Gen
eral
pur
pose
X-ra
y un
its
Mob
ile X
-ray
units
CT
scan
ners
MR
I sca
nner
s
Syrin
ge p
umps
Dia
gnos
tic u
ltras
ound
sca
nner
s
Flex
ible
end
osco
pes
350 349 70 1202 1707 353 36 595 4612 34 6400 22 40 1245 543
18
Exhibit 9‘All Scotland’ age profiles for selected examples of medical equipment
Planning to replace ageing medicalequipment3.22 NHS boards need to ensure thatthey invest sufficiently in their medicalequipment replacement programmes.
3.23 Potentially, there are risks toquality of care and financial riskswhen medical equipment is olderthan its standard life. Equipmentbecomes obsolete in different ways,for example, when maintenancecosts become excessive, spares arenot available, equipment becomesunreliable and when new technologyoffers significant advantages.
Although the standard life varies withthe type of equipment, for manyitems it is between 7-10 years, basedon assumptions about levels ofusage, availability of spares, servicesupport and new equipmentimprovements
28. Twenty-five percent
of the medical equipment that welooked at is outwith its standard life,Exhibit 9.
3.24 Depreciation can be a usefulindicator to assess whether or notthe annual spend on medicalequipment is adequate because itshould reflect the standard life ofequipment. Equipment is typicallywritten down for financial purposes,over 5, 10 or 15 years throughdepreciation
29. In Equipped to Care,
we drew attention to a shortfallbetween depreciation and the capitalinvestment that had been made inmedical equipment. And weconcluded that trusts would faceincreasing problems due tosystematic underinvestment.
3.25 In 2001/02, capital expenditurein 42% of trusts fell short ofdepreciation levels, particularly inPCTs, indicating that their capitalinvestment is not keeping pace with estimated replacementrequirements. And for acute trustswhere there are larger numbers ofequipment on the fixed assetregister, on average 37%
30of
equipment still in use has no valueon the fixed asset register
31. NHS
boards need to be aware of thefinancial risks involved in placing somuch reliance on old equipment,which may need to be replaced atshort notice when it can no longer beadequately maintained
32.
Spending up at year end3.26 In Equipped to Care, we drewattention to the potential forinefficient spending on medicalequipment. This happens whentrusts, for example, ‘spend up’ foryear end cash managementpurposes rather than purchasing onthe basis of rational selection andprioritisation.
3.27 Fourteen trusts cannot provide aprofile of the timing of their revenueexpenditure. All trusts can, however,provide the profile for capitalexpenditure, demonstrating thatmost medical equipment capitalexpenditure continues to take place
28 Advice from Medical Equipment Managers, Study Advisory Panel, 2003. 29 The estimated value of the equipment used up in the year.30 The range was 11% - 62%.31 Note: Where equipment is working well, can be maintained and is still fit for purpose, there is no need to replace it.32 Part 4 provides trust-specific age profiles for selected equipment, and depreciation levels for 2001/02.
Source: Audit Scotland, 2003
Note: Includes trust data where complete age profiles were provided.
Approximately 25% of these items of medical equipment are older than the standard life.
'All
Sco
tland
' per
cent
age
quar
terly
spe
nd
Financial year 2001/02
0
30
40
50
60
70
80
Quarter 1 Quarter 2 Quarter 3 Quarter 4
20
10
March 2002 only
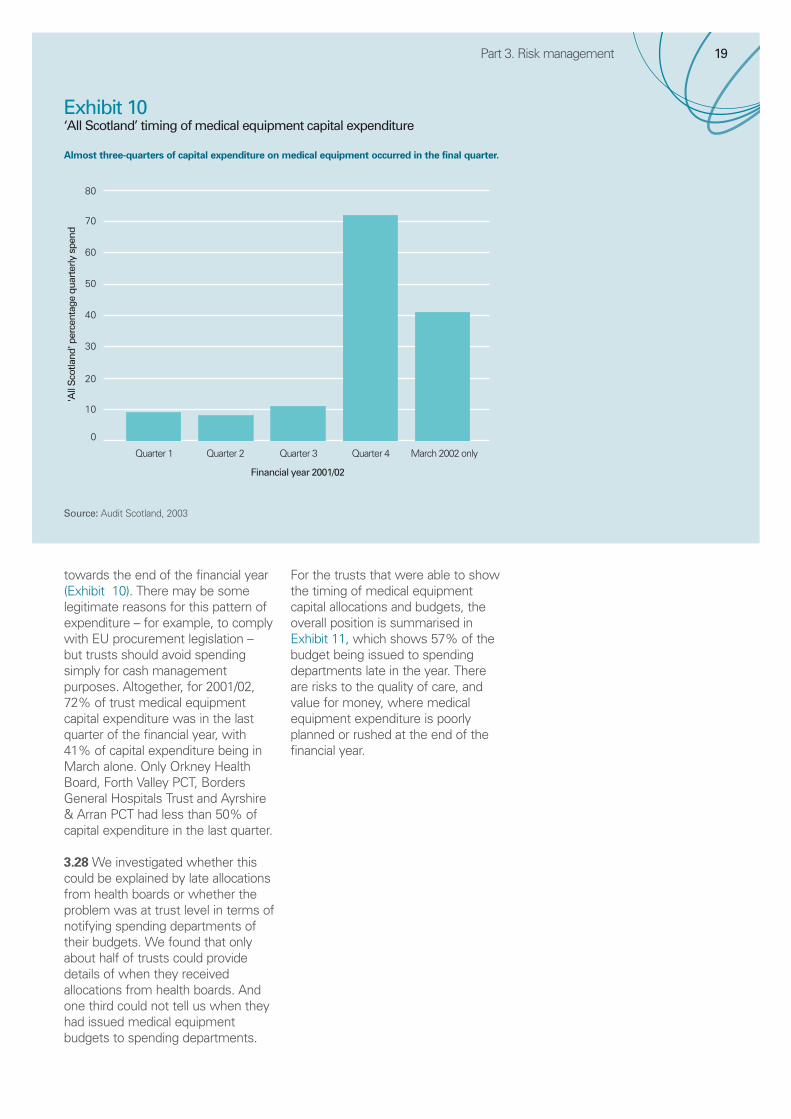
Exhibit 10‘All Scotland’ timing of medical equipment capital expenditure
Part 3. Risk management 19
towards the end of the financial year(Exhibit 10). There may be somelegitimate reasons for this pattern ofexpenditure – for example, to complywith EU procurement legislation –but trusts should avoid spendingsimply for cash managementpurposes. Altogether, for 2001/02,72% of trust medical equipmentcapital expenditure was in the lastquarter of the financial year, with41% of capital expenditure being inMarch alone. Only Orkney HealthBoard, Forth Valley PCT, BordersGeneral Hospitals Trust and Ayrshire& Arran PCT had less than 50% ofcapital expenditure in the last quarter.
3.28 We investigated whether thiscould be explained by late allocationsfrom health boards or whether theproblem was at trust level in terms ofnotifying spending departments oftheir budgets. We found that onlyabout half of trusts could providedetails of when they receivedallocations from health boards. Andone third could not tell us when theyhad issued medical equipmentbudgets to spending departments.
For the trusts that were able to showthe timing of medical equipmentcapital allocations and budgets, theoverall position is summarised inExhibit 11, which shows 57% of thebudget being issued to spendingdepartments late in the year. Thereare risks to the quality of care, andvalue for money, where medicalequipment expenditure is poorlyplanned or rushed at the end of thefinancial year.
Source: Audit Scotland, 2003
Almost three-quarters of capital expenditure on medical equipment occurred in the final quarter.

Exhibit 12Example of financial benefits gained by collaborating over medical equipment procurements
20
Exhibit 11‘All Scotland’ timing of medical equipment capital allocations and budgets
• North Glasgow University Hospitals Trust collaborated with Forth Valley and led the procurement of anaestheticmachines and ventilators. This saved Forth Valley an estimated £62,000.
• North Glasgow University Hospitals Trust led a collaboration with South Glasgow University Hospitals Trust andYorkhill Trust for the installation of a common platform for digital radiology systems, with an estimated saving of£235,000 for the trusts involved.
Source: Audit Scotland, 2003
Perc
enta
ge a
lloca
tion/
budg
ets
Capital allocation from health board/other to trusts
Capital budget from trusts to spending departments
Before 2001/02financial year
0April - June 2001 July- Sept 2001 Oct - Dec 2001 Jan - Mar 2002
10
20
30
40
50
60
Source: Audit Scotland, 2003
The timing of trust capital budgets to spending departments is especially late in the financial year.

21
Collaborating on procurement3.29 Reduced costs can also beachieved by collaborating with otherparts of NHSScotland to obtaindiscounts. And joint procurement toenhance spending efficiencies is anSEHD priority. Collaborating overprocurement also has other benefits,such as developing productexpertise.
3.30 Eighty-four percent of trustshave collaborated with ScottishHealthcare Supplies (SHS) whenprocuring medical equipment. Forexample, for the financial year endingMarch 2003, SHS purchasedequipment to the value of £16.6million on behalf of others throughspecial projects, including a CTscanner, diagnostic imagingequipment, and dental equipment.Trusts sometimes also collaboratewith each other and an example ofthe financial benefits realised is inExhibit 12. However, this kind ofprocurement arrangement is notcommon. And four trusts do notcollaborate with SHS or other trustson medical equipment procurement:Ayrshire & Arran PCT, Forth ValleyPCT, Renfrewshire & Inverclyde PCTand West Lothian Healthcare Trust.Our follow-up audit of managingsupplies in NHSScotland will reviewnew developments in NHSScotlandprocurement arrangements
33.
Recommendations
National7. The SEHD should ensure that the
new national risk managementscheme addresses the risksassociated with medicalequipment.
8. The SEHD should rationalise andmake use of the data fromexisting national systems thatcover medical equipment,including adverse incidents,clinical risk incidents andoccupational health & safety.
Local9. NHS board risk management
strategies should explicitly includemedical equipment.
10.NHS boards should discuss medical equipment risks andperformance information atperformance reviews withoperating divisions.
11.Operating divisions should ensurethat they manage risks,particularly in relation to:
• training, by ensuring that allstaff expected to useequipment are appropriatelytrained and that this is properlyrecorded
• maintenance, by ensuring thatthe split between differenttypes of service provider isevidence based and that in-house teams are adequatelyresourced
• forward investmentprogrammes, by ensuring thatthese are realistic in terms ofmeeting formally assessedmedical equipment needs.
12.Divisional management teamsshould ensure that they have theinformation needed to managemedical equipment effectivelyand to minimise risk.
33 In Good Supply? Managing Supplies in the NHS in Scotland, October 2001. A baseline audit report by Audit Scotland.
Part 3. Risk management

22
Part 4. Information to supportmanagement
Main findings
NHSScotland cannot demonstratethat it is making best use of itsmedical equipment resources forpatient care because of a lack ofinformation.
Where data do exist, their qualityis variable and they are not alwaysused to best effect.
From the data we were able toobtain, it is clear that substantialvariations remain among trusts forimportant aspects of medicalequipment.
4.1 This chapter looks at:
• why management information isimportant
• the main sources of medicalequipment data
• the quality of management data
• using the data.
Why management information is
important
4.2 Trusts need to know whatequipment they have and where thatequipment is for operationalpurposes to ensure that equipment isin the right place at the right time for patient care. Managementinformation is also required tosupport the planning, managementand governance of medicalequipment at local and nationallevels, as highlighted already in Parts2 and 3 of this report.
Sources of medical equipment
data
4.3 Good management informationrelies on the availability of robust,consistent data. Much of that data isneeded at trust level, to beaggregated, when required, for areaand national purposes. The mainsources for the data are trust medicalequipment maintenance registersand financial asset registers. Alltrusts maintain registers for financialand maintenance purposes, butwhere a device is (or should be) on
both registers, the data are notalways consistent. Exhibit 13 showsthe percentages of trusts whichcould readily identify key data forindividual items of equipment fromtheir registers. Overall, Forth ValleyPCT, Lothian PCT, Tayside PCT,Western Isles Health Board andOrkney Health Board had registerswith less complete data for individualitems of medical equipment.
4.4 Four trusts were not able todemonstrate readily from theirregisters, their complete inventory ofequipment – Western Isles HealthBoard, Orkney Health Board, LothianUniversity Hospitals Trust and LothianPCT. And Tayside UniversityHospitals Trust had particularproblems demonstrating fromregisters, the current location ofequipment.

23
Exhibit 13Ready access to key management information held on registers for individual items of medical equipment
Most trusts have ready access to key management information for individual items of medical equipment.
Part 4. Information to support management
Management information
held for individual medical
equipment items
Percentage of trusts able to
readily identify the information
Trusts not able to readily
identify the information
Current location of medicalequipment items, eg, by serialnumber
97% Tayside University
Model 100%
Make 100%
Supplier 100%
Purchase /Acquisition date 94% Lothian PCT and Tayside PCT
Purchase cost 87% Forth Valley PCT, Lothian PCT,Renfrewshire & Inverclyde PCT andWestern Isles Health Board
Expected /Standard life 90% Forth Valley PCT, Tayside PCT andWestern Isles Health Board
Annual depreciation 90% Forth Valley PCT, Tayside PCT andWestern Isles Health Board
Estimated replacement cost for items > £5,000
90% Forth Valley PCT, Lothian PCT andWestern Isles Health Board
Preventive maintenance and repairs 90% Tayside PCT, Western Isles HealthBoard and Orkney Health Board
Service histories 90% Tayside PCT, Western Isles HealthBoard and Orkney Health Board
Source: Audit Scotland, 2003

24
Exhibit 14Summary of important medical equipment management information
Source: Audit Scotland, 2003
Note: To be interpreted in conjunction with Exhibit 16 which highlights data quality information.* A third of capital expenditure was for Lothian University Hospital Trust 2001/02.
Type of information Summary for data provided Trusts not able to
demonstrate information
Financial information For financial year 2001/02
Total expenditure
Capital expenditure*Revenue expenditureLease expenditure
£71,480,000
£60,801,000£3,811,000£6,868,000
7 PCTs, 5 acute trusts and 1 other body1 acute and 2 other bodies/not relevant for 13 trusts
Total replacement value
(excluding replacement value for
leased equipment)
Medical equipment replacementvalues for items on the fixed assetregisterThe estimated replacement value ofthe medical equipment which is>£500 & <£5,000 including VAT
£483,731,000
£377,745,000
£105,986,000
5 PCTs, 2 acute trusts and 1 other body3 provided partial data
1 PCT, 1 acute trust and 2 otherbodies
Net Book Value £190,635,000 1 other body
The level of depreciation held onfixed asset registers
£32,311,000
Maintenance expenditure
Commercial third partyIn-house departmentOther NHS
£23,150,000
£13,955,000£8,730,000£465,000
3 PCTs and 1 other body
15 provided partial data
Investment in training 32% of Trusts can identify theirinvestment in training for the use ofmedical equipment
10 PCTs, 6 acute trusts and 5 otherbodies
Leasing agreements 18 trusts have leasing agreements£34,435,000 is the estimated value ofequipment leased across trusts
Not relevant for 13 trusts
Other management information
Monitoring usage of major items of equipment
18 trusts have systems in place tomonitor major items of medicalequipment
Not relevant for some PCTs
Performance indicators 32% of trusts have formally specifieda range of medical equipmentperformance indicators (PIs) that theykeep under review
10 PCTs, 6 acute trusts and 5 otherbodies
Benchmarking initiatives 36% of trusts are actively engaged in formal medical equipmentbenchmarking initiatives with similarorganisations
7 acute trusts, 9 PCTs and 4 otherbodies

Part 4. Information to support management
Exhibit 15Gaps in basic financial management data and estimated ‘All Scotland’ position
25
Quality of management
information
4.5 Given the importance of medicalequipment, it is vital that decisionsare made based on soundinformation. But we found both gapsand quality issues in the supportingdata.
Gaps in the data
4.6 It is still not possible to provide aclear picture of key aspects ofmedical equipment held inNHSScotland (Exhibit 14 opposite).Overall, Lomond & Argyll PCT,Dumfries & Galloway PCT, HighlandPCT, Tayside University HospitalsTrust and Western Isles Health Boardhad poorer access to summarymanagement information for theirholdings of medical equipment. AndRenfrewshire & Inverclyde PCT haddifficulty in providing collatedmanagement information for our2002 trust questionnaire.
4.7 For example, there were gaps inbasic financial management data,2001/02 (Exhibit 14). The main gapsin financial data are:
• 42% of trusts were not able toprovide total figures for theirrevenue expenditure on medicalequipment. So the figure of £11 million (including leaseexpenditure), which wasidentified through the audit,significantly understates the ‘AllScotland’ position, which weestimate at £25 million (Exhibit 15).
• Trusts should be aware ofreplacement values for medicalequipment so that they can makerealistic provision for it in theirinvestment programmes. Buteight trusts could not providetheir estimated replacement valuefor medical equipment purchasedfrom capital and four trusts could
not give it for equipment boughtfrom revenue. So the £378 millionand £106 million reported bytrusts, significantly understate the‘All Scotland’ position which weestimate at £630 million. Trustsalso lease medical equipmentwith a replacement valueestimated at £34.5 million.
• It is important to ensure thatthere is sufficient investment inmaintenance for medicalequipment because this, alongwith training, has the greatestimpact on device safety. But fourtrusts could not provide theirmaintenance figures, and 15trusts could only provide partialdata, so the £23 million reportedby trusts understates the ‘AllScotland’ position which weestimate at over £44 million
38.
34 These estimates are extrapolated from the trusts that did provide the required information on the basis that the rest would have a similar profile. 35 Trusts also estimated the replacement value of leased equipment at £34.5 million, 2001/02.36 This covers items held on the fixed asset register.37 This covers items with a purchase value of >£500 and < £5,000, including VAT.38 Estimated at 7% of the ‘grossed up’ replacement value, as advised by the Medical Equipment Managers on our Study Advisory Panel (Exhibit 15).
Source: Exhibit 14
Financial management
data
Data provided by
trusts for financial
year 2001/02
£million
Trusts not able to
provide information
Estimated ‘All Scotland’
position34
£million
Revenue expenditure £11 7 PCTs; 5 acute; 1 other body
£25
Replacement values35
• Capital36
• Revenue37
£378
£106
5 PCTs; 2 acute; 1 other body
1 PCT; 1 acute; 2 other bodies
£510
£120
Maintenance expenditure £23 3 PCTs; 1 other; 15 partial data
£44

26
Reliability of the data
4.8 External auditors assessed thequality of data that were provided bytrusts and we found that datareliability varied among trusts andamong data types. For the majority ofdata categories reviewed, trustswere able to demonstrate, overall,that they had robust data (Exhibit 16).In particular, financial managementdata, where available, were mostlyreliable. Trusts with more reliablemanagement data, overall formedical equipment are: Argyll &Clyde Acute Hospitals Trust, Ayrshire& Arran Acute Hospitals Trust,Yorkhill Trust, West LothianHealthcare Trust, Shetland HealthBoard and Lanarkshire AcuteHospitals Trust. But several trustscould only provide estimates thatcould not be substantiated for somekey data. There is room forimprovement, in particular, in thereliability of medical equipmentmanagement data for: GreaterGlasgow PCT, Lothian PCT, ForthValley PCT, Fife PCT and OrkneyHealth Board.
Using the management
information
4.9 Management information onlyadds value if it is reported and used.Agreed PIs can be a useful tool tosupport benchmarking andperformance management. But theSEHD and health boards do not usemedical equipment PIs for thispurpose. Ten trusts make use of PIsfor medical equipment, but these aremostly limited to operational aspectsof medical physics teams. Forexample, North Glasgow UniversityHospitals Trust uses some medicalequipment PIs of this type, which arereviewed at their ISO-accreditedbioengineering meetings. Theseinclude statistics on utilisation forequipment in imaging, radiotherapyand laboratories; and equipmentinstallations with more than fourservice calls in six months.
4.10 Some informal comparisons aremade at the Scottish MedicalEquipment Manager meetings.However, without agreed PIs,benchmarking initiatives betweensimilar organisations are impossible.The lack of an agreed minimum dataset to provide managementinformation for medical equipmentmeans that it is difficult forNHSScotland to demonstrate that itis using its resources well. We had tomake special arrangements to collectand coordinate basic managementdata. From the data we did obtain,we have provided some provisionalbenchmarking data (Exhibits 17 - 21following). And these highlightcontinued unexplained variationsamong trusts.
4.11 Exhibits 17 - 21 provideexamples of PIs that would be usefulfor managing medical equipment. Asa minimum, we would expect truststo benchmark medical equipment interms of: age profile; investing inmedical equipment to maintain andimprove levels of equipment; thelevel of equipment available; and,spend on maintaining the equipment.
4.12 The substantial variations shownin the Exhibits need to be explainedby trusts. Some variation will beexplained by the use of estimatesand incomplete (partial) data, or bydifferences in accounting proceduresas discussed in the explanatory notesto Exhibits. Once data issues of thiskind have been identified andaddressed, the remaining variationswould reflect real differencesbetween trusts. Meanwhile, theExhibits should be interpreted withcare. It is important to resolve thedata issues as quickly as possible sothat real differences between trustscan be shown and the benchmarkingresults can then be used to informthe development of good practice.
Age profiles (Exhibit 17)4.13 The age of key items ofequipment varies substantiallybetween trusts and some trusts arerelying heavily on equipment that isbeyond its standard life.

Part 4. Information to support management 27
Exhibit 16Auditor data quality ratings for validated trust medical equipment management data
The quality of some medical equipment management data needs to improve.
Quality rating descriptions
Reliable: Where auditors found responses to be reliable, ie, based on actuals or generally reliable with some basedon estimates.
Estimated: Responses based on estimates.
No clear audit trail for the data.
Data Overall quality rating No clear audit trail for the data
Net Book Value Reliable Greater Glasgow PCT
Depreciation Reliable
*Replacement value on fixed asset register
Mostly reliable and 1 estimated
Replacement value for items >£500and <£5,000
Mixture of reliable and estimated Orkney Health Board
Leasing data Mixture of reliable and estimated
*Timing of medical equipmentallocations
Mixture of reliable and estimated Fife PCT, Forth Valley PCT,Lanarkshire PCT and Lothian PCT
*Timing of medical equipmentexpenditure
Mostly reliable and 1 estimated Fife PCT, Forth Valley PCT, LothianUniversity, Lothian PCT and WesternIsles Health Board
*Maintenance expenditure Mixture of reliable and estimated Ayrshire & Arran PCT, Dumfries &Galloway Acute, Fife PCT, ForthValley PCT, Greater Glasgow PCT andOrkney Health Board
Financial benefits for collaboratingover procurement
Mixture of reliable and estimated Lomond & Argyll PCT, GreaterGlasgow PCT, Highland Acute andOrkney Health Board
Investment in training Mixture of reliable and estimated Grampian PCT and South GlasgowUniversity
*Age profiles of equipment Mixture of reliable and estimated Orkney Health Board
Standardisation Mostly reliable and 1 estimated Greater Glasgow PCT
Systems for monitoring usage ofmajor items of equipment
Mixture of reliable and estimated Highland Acute and Lothian PCT
Source: Audit Scotland, 2003
Note: To be interpreted in conjunction with Exhibit 14, which highlights where management data were/not available.* Where partial data was provided by some trusts.

Perc
enta
ge ‘a
ge p
rofil
es’
0
20
40
60
80
1005 6 11
General purpose X -rays units
Total number of items
Equipment age
3 3 37 2 3 124 8 43 14 19 1913 12 67 35 16 24524
Lana
rksh
ire P
CT
Gre
ater
Gla
sgow
PC
T
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Forth
Val
ley
Acu
te
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Loth
ian
PCT
Fife
Acu
te
Gra
mpi
an P
CT
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
vers
ity
Ren
frew
shire
& In
verc
lyde
PC
T
Lom
ond
& A
rgyl
l PC
T
Shet
land
Hea
lth B
oard
Lana
rksh
ire A
cute
Bor
ders
Gen
eral
Hos
pita
ls
Fife
PC
T
Ork
ney
Hea
lth B
oard
>0 - 3 years
>3 - 5 years
>5 - 7 years
>7 - 10 years
>10 - 15 years
>15 years
Perc
enta
ge ‘a
ge p
rofil
es’
0
20
40
60
80
10011 24 95 72 74 40 83 84 84 39 90 32 31 19 13 54 67 7244 12013 10213 1428632
Defibrillators
Total number of items
Equipment age
Lana
rksh
ire P
CT
Gre
ater
Gla
sgow
PC
T
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Forth
Val
ley
PCT
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Loth
ian
PCT
Fife
Acu
te
Gra
mpi
an P
CT
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
vers
ity
Ren
frew
shire
& In
verc
lyde
PC
T
Lom
ond
& A
rgyl
l PC
T
Shet
land
Hea
lth B
oard
Lana
rksh
ire A
cute
Bor
ders
PC
T
Forth
Val
ley
Acu
te
Ork
ney
Hea
lth B
oard
Bor
ders
Gen
eral
Hos
pita
ls
Hig
hlan
d PC
T
>0 - 3 years
>3 - 5 years
>5 - 7 years
>7 - 10 years
>10 - 15 years
>15 years
28
Exhibit 17Age profiles for selected examples of medical equipment by trust

Perc
enta
ge ‘a
ge p
rofil
es’
0
20
40
60
80
1004 2 47 6 6 21 5 85 189 123 21 58 38 105 128 60 82 23 102 2 6 132
Flexible endoscopes
Total number of items
Equipment age
>0 - 3 years
>3 - 5 years
>5 - 7 years
>7 - 10 years
>10 - 15 years
>15 years
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Loth
ian
PCT
Fife
Acu
te
Gra
mpi
an P
CT
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
vers
ity
Lom
ond
& A
rgyl
l PC
T
Shet
land
Hea
lth B
oard
Lana
rksh
ire A
cute
Forth
Val
ley
Acu
te
Ork
ney
Hea
lth B
oard
Bor
ders
Gen
eral
Hos
pita
ls
Dum
fries
& G
allo
way
PC
T
Perc
enta
ge ‘a
ge p
rofil
es’
0
20
40
60
80
1004 26 79 148 149 383 175 17 922 253 596 81628 14 12 17 32 16139 213 262 201 110
Volumetric pumps
Total number of items
Equipment age
>0 - 3 years
>3 - 5 years
>5 - 7 years
>7 - 10 years
>10 - 15 years
>15 years
Lana
rksh
ire P
CT
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Forth
Val
ley
PCT
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Tays
ide
PCT
Fife
Acu
te
Gra
mpi
an P
CT
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
vers
ity
Lom
ond
& A
rgyl
l PC
T
Shet
land
Hea
lth B
oard
Bor
ders
PC
T
Bor
ders
Gen
eral
Hos
pita
ls
Forth
Val
ley
Acu
te
Hig
hlan
d PC
T
Part 4. Information to support management 29
Source: Audit Scotland, 2003
Note: Only includes trust data where complete ages profiles were provided. Certain items of equipment were not relevant for some trusts.

£000
Depreciation
Lothian Universitydepreciation £4.7mcapital expenditure £21m
Capital expenditure
Dum
fries
& G
allo
way
Acu
te
Fife
Acu
te
Bor
ders
Gen
eral
Hos
pita
ls
Tays
ide
Uni
vers
ity
Forth
Val
ley
Acu
te
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Lana
rksh
ire A
cute
Hig
hlan
d A
cute
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Acute trusts
£000
Depreciation
Capital expenditure
Shetland Health Board
Mixed/Other bodies
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Orkney Health Board Western Isles HealthBoard
West Lothian Healthcare Yorkhill
30
Exhibit 18Capital expenditure and depreciation of medical equipment by trust
In 2001/02, capital expenditure for medical equipment did not always match depreciation
£000
Depreciation
Capital expenditure
Forth
Val
ley
PCT
Gre
ater
Gla
sgow
PC
T
Hig
hlan
d PC
T
Ayr
shire
& A
rran
PCT
Dum
fries
& G
allo
way
PC
T
Lom
ond
& A
rgyl
l PC
T
Lana
rksh
ire P
CT
Bor
ders
PC
T
Primary Care Trusts (PCTs)
Loth
ian
PCT
Gra
mpi
an P
CT
Ren
frew
shire
& In
verc
lyde
PC
T
Tays
ide
PCT
0
100
200
300
400
500
600
Fife
PC
T
Source: Audit Scotland, 2003
Note: These graphs show a one-year snapshot of expenditure and depreciation. Financial year 2001/02.

Part 4. Information to support managementPe
rcen
tage
Financial year 2001/02
Lana
rksh
ire P
CT
Gre
ater
Gla
sgow
PC
T
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Forth
Val
ley
Acu
te
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Loth
ian
PCT
Fife
Acu
te
Gra
mpi
an P
CT
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
vers
ity
Ren
frew
shire
& In
verc
lyde
PC
T
Lom
ond
& A
rgyl
l PC
T
Shet
land
Hea
lth B
oard
Lana
rksh
ire A
cute
Bor
ders
Gen
eral
Hos
pita
ls
Fife
PC
T
Ork
ney
Hea
lth B
oard
0
2
4
6
8
10
12
14
Tays
ide
PCT
Dum
fries
& G
allo
way
PC
T
Hig
hlan
d PC
T
Bor
ders
PC
T
Forth
Val
ley
PCT
Acute trusts Primary Care Trusts (PCTs) Mixed/Other bodies
Exhibit 19Total Net Book Value of medical equipment held by trusts as a percentage of trust operating income
31
Investing to maintain and improvelevels of equipment (Exhibit 18)
Capital4.14 Depreciation information helpsto assess whether or not theexpenditure on equipment purchasedfrom capital is sufficient at least tocover ‘replacement’ equipment
39. It
needs to be presented as trend dataso that fluctuations in investment areseen in context. We have onlyprovided a one-year snapshotbecause trend data are not routinelyavailable. If 2001/02 reflects thetrend, then investment in at least42% of trusts is insufficient toreplace equipment and maintainexisting levels of equipment, far lessimprove them. While Exhibit 18shows that acute trusts appear to beperforming better than PCTs, this hasto be seen in the context that, onaverage, 37% of equipment still inuse has no value on their fixed assetregister.
Revenue4.15 Annual expenditure on medicalequipment funded from revenue alsoneeds to be shown as trend data toensure that investment in low cost/high volume items is adequate tomeet service requirements.
Net Book Value40
(Exhibit 19)4.16 Net Book Value as a percentageof trust operating income is ameasure that can be used to indicatetrust levels of medical equipmentprovision. For example, Exhibit 19shows that there is a three-folddifference between acute trusts, butsome of this might be explained bydifferences in the way trustsdepreciate their medical equipmentand record equipment on fixed assetregisters.
Replacement value41
(Exhibit 20)4.17 Replacement value as apercentage of trust operating incomeis another way of measuring trust
levels of medical equipmentprovision. Exhibit 20 showsreplacement value of medicalequipment as a percentage ofoperating income, for capital andrevenue. Again, this highlights thedegree of variation between truststhat were able to providereplacement values. There are manygaps in the data and some figuresare based on estimates.
Maintenance spend (Exhibit 21)4.18 We would expect maintenancespend to be related to trustreplacement values and these dataare shown in Exhibit 21. This showsthat there are still substantialvariations in how much trusts spendon the maintenance of their medicalequipment. However, somereplacement values are estimated, asdescribed previously, and themajority of trusts could only giveincomplete data on maintenanceexpenditure (Exhibit 14).
39 It is not always possible or meaningful to separate expenditure between ‘replacement’ equipment and ‘new’ equipment purchased to, for example, provide anincreased level of service.
40 The estimated value of the equipment after depreciation has been taken into account.41 The estimated investment the organisation would require to replace the equipment.
Source: Audit Scotland, 2003
Note: Net Book Value of medical equipment on fixed asset register. To be interpreted in conjunction with explanatory notes below.For operating income, see Appendix 4.

Exhibit 21Maintenance expenditure as a percentage of total replacement value by trust
Financial year 2001/02
Perc
enta
ge
0
5
10
15
20
25
Medical equipment items costing>£5,000
Medical equipment items costing<£5,000 and >£500
Lana
rksh
ire P
CT
Gre
ater
Gla
sgow
PC
T
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Forth
Val
ley
Acu
te
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Loth
ian
PCT
Fife
Acu
te
Gra
mpi
an P
CT
Sout
h G
lasg
ow U
nive
rsity
Arg
yll &
Cly
de A
cute
Loth
ian
Uni
vers
ity
Ren
frew
shire
& In
verc
lyde
PC
T
Lom
ond
& A
rgyl
l PC
T
Shet
land
Hea
lth B
oard
Lana
rksh
ire A
cute
Bor
ders
Gen
eral
Hos
pita
ls
Fife
PC
T
Ork
ney
Hea
lth B
oard
Tays
ide
PCT
Hig
hlan
d PC
T
Bor
ders
PC
T
Dum
fries
& G
allo
way
PC
T
Forth
Val
ley
PCT
Acute trusts Primary Care Trusts (PCTs) Mixed/Other bodies
Perc
enta
ge
Lana
rksh
ire P
CT
Wes
t Lot
hian
Hea
lthca
re
York
hill
Dum
fries
& G
allo
way
Acu
te
Ayr
shire
& A
rran
PCT
Tays
ide
Uni
vers
ity
Forth
Val
ley
Acu
te
Nor
th G
lasg
ow U
nive
rsity
Ayr
shire
& A
rran
Acu
te
Gra
mpi
an U
nive
rsity
Hig
hlan
d A
cute
Fife
Acu
te
Gra
mpi
an P
CT
Shet
land
Hea
lth B
oard
Lana
rksh
ire A
cute
Bor
ders
Gen
eral
Hos
pita
ls
0
2
4
6
8
10
12
14
Tays
ide
PCT
Bor
ders
PC
T
Acute trusts Primary Care Trusts (PCTs) Mixed/Other bodies
32
Exhibit 20Replacement value for *capital and **revenue medical equipment items as a percentage of trust operating income
Source: Audit Scotland, 2003*Medical equipment items originally costing ≥£5,000.**Medical equipment items originally costing <£5,000 and >£500.
Note: Eight trusts did not provide replacement value for capital items and four trusts did not provide estimated replacement value for revenue items. To beinterpreted in conjunction with explanatory notes on previous page.For operating income, see Appendix 4.
Source: Audit Scotland, 2003
Note: Only includes trusts that gave maintenance expenditure and replacement values, many of which are estimated. Some data are partial. Tobe interpreted in conjunction with explanatory notes previous page.

Part 4. Information to support management 33
Recommendations
(Also, see recommendations in Parts2 and 3.)
National13.The SEHD should ensure that a
minimum data set for managingmedical equipment is agreed andimplemented.
14.The SEHD should make use ofthis performance information toinform Accountability Reviewsand other performancemonitoring processes.
Local15.Operating divisions should ensure
that the information held onmedical equipment registersmeets agreed minimum data setrequirements, is up to date,accurate and easily accessible.Regular reviews of the availability,reliability and consistency of datashould be undertaken byoperating divisions.
16.NHS boards should ensure thismedical equipment performanceinformation is used to assesswhether the local area is makingbest use of its medical equipmentresources for patient care.

34
Equipped to Care:
Managing Medical Equipment in
the NHS in Scotland, 2001
Key points and conclusion from theexecutive summary of this report.
Key points
Trusts are responsible for managing asignificant investment in medicalequipment. In 1997/98:
• the total value of medicalequipment was in the region of£170 million
• expenditure on new andreplacement equipment was £25 million
• expenditure on maintenance wasaround £20 million.
Despite its financial significance, andthe important implications for clinicalgovernance if medical equipment isnot managed well, few trust boardstake an active role in:
• determining priorities for theacquisition of medical equipment
• examining trust procurementpractices
• monitoring training, usage andmaintenance issues.
There continues to be scope forimprovements in the combinedpurchasing of medical equipment:
• we were unable to obtaininformation from trusts on theuptake of national contracts
• a substantial amount ofequipment is purchased at a locallevel without consideration givento the potential benefits ofaggregating purchases.
Trusts are managing many of theoperational medical equipmentissues well …
• finance departments are ensuringcompliance with EU procurementlegislation and Standing FinancialInstructions
• multidisciplinary involvement inprocurement is commonplace
• clinicians reported satisfactionwith response times forequipment failure, so interruptionsto services are rare.
… but some trusts are exposingthemselves to unnecessary risks:
• data on total expenditure (capitaland revenue) are not availablefrom national financial returns
• Audit Scotland had to obtaininformation by surveying trustsdirect
• not all trusts could easily providebasic information on expenditureand usage.
… although our snapshot dataindicated that:
• there are variations in trustexpenditure on medicalequipment, and the level ofequipment available, not fullyexplained by differences in typeof trusts
• expenditure on new andreplacement equipment is failingto match depreciation.
Conclusion
There is room for improvement inthe management of medicalequipment. A common themethroughout the study was inadequatemanagement information andreporting systems. In particular, givenits strategic importance and clinicalgovernance considerations, it isdisappointing that, at many trusts,board members do not have accessto robust information which wouldhelp them set priorities and managethe risks associated with medicalequipment. For example, they needto ensure that they are aware of andunderstand the implications of anyshortfall between depreciation andthe combined capital and revenuepurchases. Board members shouldensure that responsibility for medicalequipment is delegated to someoneon the trust board. In turn, theyshould ensure that good practiceguidelines (outlined in the mainbaseline report) are implemented andmonitored.
Appendix 1

Appendix 2 35
Appendix 2
Definition of medical equipment
used in this audit
Medical devices are all instruments,apparatus, appliances, materials orother articles, used for the purposesof diagnosis, prevention, monitoring,treatment or alleviation of disease orinjury or handicap. Medical devicesdo not include estates relatedequipment such as catering andlaundry equipment. Medical devicesdo not include hospital computingequipment unless the IT equipmentis linked to patient connectedmedical equipment, or laboratoryequipment or is part of a PictureArchiving Communication System.
Medical equipment is a subset ofmedical devices. We have definedmedical equipment as all devicesthat are connected to the patientas part of their treatment and carein hospitals and health centres,and devices used for diagnostic,therapeutic and laboratorypurposes.
Medical equipment does not includeconsumable medical devices such assyringes and dressings.
Medical equipment excluded fromthis audit were: equipment locatedwithin Sterile Supply Units (ie, inTheatre Sterile Supplies Unit (TSSU)or Central Sterile SupplyDepartments (CSSDs)); plant,including operating lights, piped gassystems; small operating instrumentsprocessed through TSSU; implanteddevices (eg, pacemakers); “normal”beds, trolleys, chairs, wheelchairs,and low cost rehabilitation equipment(eg, crutches).
Examples of medical equipmentincluded in this audit are describedoverleaf:

36
Groups of Equipment Description
Imaging Equipment
Equipment that gives a picture of physiological structures, eg, X-ray, Ultrasound, MRI, CT, Gamma Cameras. Seebelow. Some of these items represent high cost items, for example, CT and MRI. Imaging equipment includes:
CT Scanners Computerised Tomography Scanner. Uses a thin beam of X-raysrotated around the body to computer generate an image of a ‘slice’through the body. Found in X-ray Departments. Costs around£600,000.
Diagnostic Ultrasound Scanners Uses high frequency sound waves ‘bounced’ off body structures toproduce images of organs. Found in X-ray Departments, Cardiology,Obstetrics, Urology Departments / Units. Costs from £15,000 to£150,000.
MRI Scanner Magnetic Resonance Imaging Scanner. Using magnetic fields, thehydrogen nucleus within the body are caused to spin, giving awaytheir location to the scanner. The scanner builds up an image of thedensity of the spinning nucleus. Shows detailed images of forexample, sections of the brain. Found in X-ray Departments. Costaround £1,000,000.
Gamma Cameras Gamma cameras detect and build up a picture of gamma radiationemanating from the patient. The patient is usually injected with aradioactive gamma emitter that concentrates in parts of the patient’sbody that are growing actively such as tumours. This gives an imagebased on the biological activity rather than structure. These will befound in Radiology or Medical Physics Departments and will costabout £300,000.
Other X-ray Equipment
Angiographic Units Uses X-rays and opaque dyes to produce moving images of bloodflow. This finds blockages and abnormalities in blood vessels. Thesecan be treated with tools passed through the veins and the radiologist/ cardiologist can treat the problem while observing the screen. Foundin X-ray Departments. Cost around £800,000.
Dental Units Used to take X-rays of the teeth. Found in most dental clinics. Costaround £5,000. More complex dental units can cost £30,000.
General Purpose X-ray Units This is the basic kit of an X-ray Department. Takes images of mostparts of the body. Costs from £40,000.
Fixed Units with Fluoroscopy These take moving images for barium swallows and enemas. Found inmany X-ray Departments. Cost around £330,000.
Mobile Units Basic X-ray machines on wheels – goes to wards, theatres, A&E etc.Costs around £30,000.

Appendix 2 37
IV Systems
Intra-venous systems are used for accurately controlling the injection of drugs into the patient. They are usuallysyringe drivers or infusion pumps. Some may be specially designed for a particular purpose – anaesthetic agents,epidurals etc. IV Systems include:
Syringe Pumps (routine) Syringe pumps are normally used to deliver small quantities of drugwith a high degree of accuracy. The drug is contained in a syringe.These will be found in most wards, theatres and intensive care. Costswill be between £1,000 and £2,000.
Volumetric Pumps (routine) Volumetric pumps control the delivery of larger quantities of drugs orfluids. They can also pump at greater rates than a syringe driver. Thesewill also be found in most wards and departments. Cost is upwards of£2,000.
Other Medical Equipment
Defibrillators Delivers an electric shock to a fibrillating heart to restore normalbeating. This is emergency equipment found in most hospital wardsand departments. Also carried by ambulances. Costs between £1,500and £9,000.
Dialysis Machines (haemodialysis) This is an artificial kidney. Patients will be connected to these threetimes a week for about 6 hours at a time to ‘clean’ the blood. Found inRenal Units. Cost around £14,000.
ECG Recorders Produces a trace of the electrical activity of the heart. The trace can beused to diagnose heart disease. Found in ECG Departments, somewards and A&E. Costs from £2,000 to £8,000.
Flexible Endoscopes Used to look inside the body. Modern equipment has a video cameraat the tip; older equipment uses a fibre optic bundle to take the picturefrom the tip to a microscope at the eyepiece. The tips can be steeredby the operator and tools can be passed through to take biopsies, stopbleeding etc. Small instruments can look into the bladder, sinuses,airway and lungs. Larger instruments are passed into the stomach andinto the colon. Individual instruments cost between £8,000 and£28,000. A complete set-up including video monitor, light source, videoprocessor and some flexible endoscopes would cost about £150,000.
Source: MHRA; and Medical Equipment Managers on our Study Advisory Panel, 2003.
38
Appendix 3
Study Advisory Panel
Mike Nieman Trust Medical Equipment Manager on baseline study advisory panel, Aberdeen Royal Infirmary, Grampian and Scottish Medical Equipment Manager Group nominee
Mike Sik Scottish Medical Equipment Manager Group nomineeCrosshouse Hospital, Ayrshire & Arran
Robin Pollock Scottish Medical Equipment Manager Group nomineeRaigmore Hospital, Highland
Michael Baxter SEHD nominee, finance specialistHead of Private Finance and Capital Unit, SEHD
Brian Howarth Senior Audit Manager, involved in baseline auditAudit Scotland
Miles Moorhouse On baseline study advisory panel, supplies specialistDirector, Scottish Healthcare Supplies, CSA
Charles Swainson Medical Director on baseline study advisory panel, and Trust ChiefLothian University Hospitals Trust Executive nominee

Appendix 4 39
Appendix 4
Source: Audit Scotland Trust Survey, 2002
Trust Operating Income 2001/02
Acute Trusts £000
Argyll & Clyde 171,220
Ayrshire & Arran 163,866
Borders General Hospitals 44,074
Dumfries & Galloway 60,000
Fife 112,441
Forth Valley 111,000
Grampian University 236,705
Highland 87,768
Lanarkshire 232,726
Lothian University 381,792
North Glasgow University 438,582
South Glasgow University 202,051
Tayside University 233,000
Primary Care Trusts (PCT)
Ayrshire & Arran 196,538
Borders 65,000
Dumfries & Galloway 93,676
Fife 194,304
Forth Valley 163,096
Grampian 305,000
Greater Glasgow 470,000
Highland 139,347
Lanarkshire 297,000
Lomond & Argyll 94,583
Lothian 344,177
Renfrewshire & Inverclyde 165,472
Tayside 251,000
Mixed/Other Bodies
Yorkhill 86,815
Orkney Health Board 24,577
Shetland Health Board 30,000
Western Isles Health Board 44,517
West Lothian Healthcare 142,492


Better equipped to care? Follow-up report on managing medical equipment
Audit Scotland110 George StreetEdinburgh EH2 4LH
Telephone0131 477 1234Fax0131 477 4567
www.audit-scotland.gov.uk ISBN 1 904651 31 3 AGS/2004/2