Embed Size (px)
Citation preview

Managing Dental Caries Risk Managing Dental Caries Risk in Young Children with HIV in Young Children with HIV
Infection: Infection:
The Rationale for Early Recognition and Prevention by
the Primary Care Team

Why Target Specific Populations?Why Target Specific Populations?
• Early Childhood Caries (ECC) is extraordinarily Early Childhood Caries (ECC) is extraordinarily predictable, based upon:predictable, based upon: RaceRace Socio-economic status (SES)Socio-economic status (SES) Feeding HabitsFeeding Habits Oral hygiene practicesOral hygiene practices
• ECC is easily diagnosed or is amenable to population ECC is easily diagnosed or is amenable to population screeningsscreenings
• ECC is easily preventedECC is easily prevented• ECC is easily treated in its early stages, andECC is easily treated in its early stages, and• ECC adversely impacts upon quality of life if left untreatedECC adversely impacts upon quality of life if left untreated

Why Target the Pediatric HIV Why Target the Pediatric HIV Population?Population?
• Survival rates of children with HIV infection continue to Survival rates of children with HIV infection continue to riserise
• The pediatric HIV population shares risk factors The pediatric HIV population shares risk factors observed in ECC populationsobserved in ECC populations 85% of HIV infected children are either African-American or85% of HIV infected children are either African-American or
HispanicHispanic Vertically transmitted HIV is a disease observed most Vertically transmitted HIV is a disease observed most
commonly in low SES populationscommonly in low SES populations HIV infected children have a higher decay rate than their HIV infected children have a higher decay rate than their
uninfected siblingsuninfected siblings HIV infected children carry a larger oral burden of lactobacilli HIV infected children carry a larger oral burden of lactobacilli
and and streptococcus mutansstreptococcus mutans Dental infections may be life threateningDental infections may be life threatening

Biology of Dental CariesBiology of Dental Caries

Etiology of Dental CariesEtiology of Dental Caries
Demineralization <------------ > Remineralization
•Frequent carbohydrate intake•Frequent exposure to acids•Plaque presence•Decreased salivary flow
•Exposure to fluoride•Removal of plaque•Balanced diet•Limited exposure to carbohydrates

What Factors Contribute to What Factors Contribute to Additional Risk in the Pediatric HIV Additional Risk in the Pediatric HIV
Population?Population?
• Increased caries susceptibilityIncreased caries susceptibility High carbohydrate diet supplementationHigh carbohydrate diet supplementation
• Effects on salivary pHEffects on salivary pH Frequent intake of sugar containing medicationsFrequent intake of sugar containing medications
• Effects on salivary function and oral floraEffects on salivary function and oral flora Compromised immunological statusCompromised immunological status
• Increased mutans streptococci and lactobacilli Increased mutans streptococci and lactobacilli levelslevels
• Increased systemic risk in face of infectionIncreased systemic risk in face of infection
• Compliance is poor among HIV infected Compliance is poor among HIV infected children with unmet dental needschildren with unmet dental needs

Untreated Dental CariesUntreated Dental Caries
• PainPain
• Eating difficultiesEating difficulties
• Sleep disturbanceSleep disturbance
• Growth and Growth and development affecteddevelopment affected
• Risk of systemic Risk of systemic infectioninfection
First Dental Visit - First Dental Visit - Anticipatory GuidanceAnticipatory Guidance
The American Academy of Pediatric The American Academy of Pediatric Dentistry recommends a dental Dentistry recommends a dental consultation shortly after the eruption consultation shortly after the eruption of the first primary tooth and no later of the first primary tooth and no later than 12 months of age.than 12 months of age.

Streptococcus mutansStreptococcus mutans Transmission Transmission
• ““Window of infectivity” -- transmission of cariogenic bacteria from Window of infectivity” -- transmission of cariogenic bacteria from caregiver to infant-- as early as 6 to 12 months caregiver to infant-- as early as 6 to 12 months
Karn T et al J Pub Health Dent 58:248-249, 1998Karn T et al J Pub Health Dent 58:248-249, 1998

Early Childhood Caries (ECC)Early Childhood Caries (ECC)
• Dental caries can occur at Dental caries can occur at any age after teeth eruptany age after teeth erupt
• ECC is particularly ECC is particularly damagingdamaging
• 25% of US children have 25% of US children have 80% of the dental caries80% of the dental caries

Objectives of Dental Screening Objectives of Dental Screening ExaminationExamination
• Identify abnormal Identify abnormal vsvs normal dental findings normal dental findings
• Perform visual dental exams in infants and Perform visual dental exams in infants and toddlerstoddlers Check for abnormalities of tooth eruption and Check for abnormalities of tooth eruption and
soft tissuessoft tissues Determine whether plaque is present on teethDetermine whether plaque is present on teeth Check teeth for “white spots” and cavitation Check teeth for “white spots” and cavitation
(cavities)(cavities)

Dental Screening Examination of Dental Screening Examination of Infants and ToddlersInfants and Toddlers
Knee to Knee Examination Position
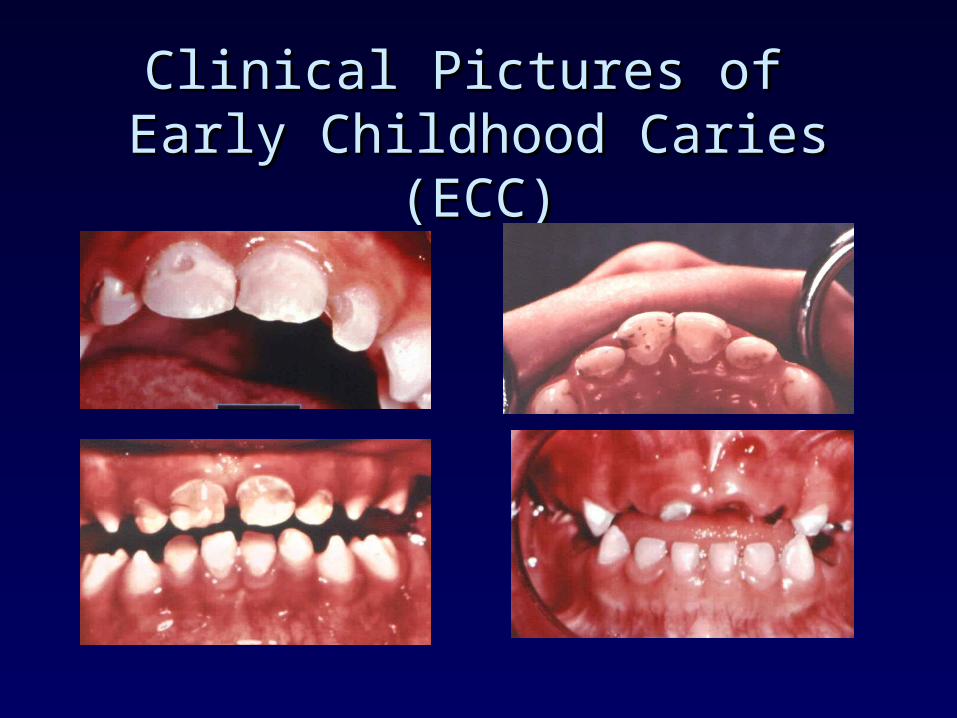
Clinical Pictures of Clinical Pictures of Early Childhood Caries (ECC)Early Childhood Caries (ECC)

ECC Distinguishing FeaturesECC Distinguishing Features
• Associated with prolonged bottle-feeding and Associated with prolonged bottle-feeding and breastfeeding*breastfeeding*
• Develops rapidly--progressing from white spot Develops rapidly--progressing from white spot lesions (subsurface decalcification) to frank lesions (subsurface decalcification) to frank cavitationcavitation
• Affects the upper incisor primary teeth firstAffects the upper incisor primary teeth first
• Primary molars are secondarily affectedPrimary molars are secondarily affected
• Mandibular incisors affected when disease has Mandibular incisors affected when disease has become very severebecome very severe
*Breastfeeding is contraindicated in HIV infected children

Dental Screening Examination Dental Screening Examination FindingsFindings
• Pointing out plaque to child’s caretakerPointing out plaque to child’s caretaker

Dental Screening Examination Dental Screening Examination FindingsFindings
• Decalcification and early cavitationDecalcification and early cavitation
DecalcificationCavitation

Dental Screening Examination Dental Screening Examination FindingsFindings
• Decalcification and cavitationDecalcification and cavitation

Dental Screening Examination Dental Screening Examination FindingsFindings
• Hypoplastic enamel (no decay)Hypoplastic enamel (no decay)

Early Diagnosed Dental CariesEarly Diagnosed Dental Caries
• May be managed easily and painlessly May be managed easily and painlessly with preventive and restorative therapywith preventive and restorative therapy

Objectives of Assessment of Objectives of Assessment of Caries RiskCaries Risk
• Provide preventive recommendations Provide preventive recommendations to parentto parent
• Provide preventive treatmentProvide preventive treatment
• Refer to dentist for necessary Refer to dentist for necessary preventive and restorative treatmentpreventive and restorative treatment

Dietary Risks for ECCDietary Risks for ECC
• Bottle-feeding after 12 monthsBottle-feeding after 12 months
• Sleeping with the bottleSleeping with the bottle
• Bottle-feeding sugar-containing Bottle-feeding sugar-containing substancessubstances
• Breastfeeding ad lib*Breastfeeding ad lib*
• Using pacifiers dipped in sweetenersUsing pacifiers dipped in sweeteners
• Snacking > 3 times per daySnacking > 3 times per day
• Snacking on cariogenic foods and Snacking on cariogenic foods and drinksdrinks
Milgrom and Weinstein, 1999
*Breastfeeding is contraindicated for HIV infected children and HIV infected mothers.
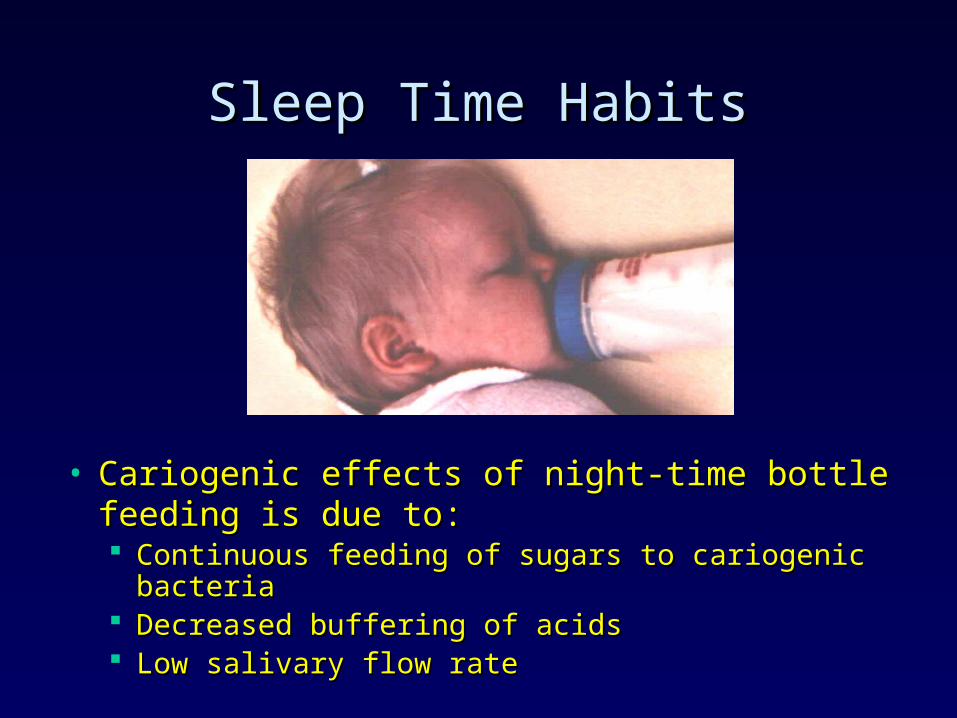
Sleep Time HabitsSleep Time Habits
• Cariogenic effects of night-time bottle feeding is Cariogenic effects of night-time bottle feeding is due to:due to: Continuous feeding of sugars to cariogenic bacteriaContinuous feeding of sugars to cariogenic bacteria Decreased buffering of acidsDecreased buffering of acids Low salivary flow rateLow salivary flow rate

MedicationsMedications
• Be aware of sucrose Be aware of sucrose contentcontent
• Evaluate medications Evaluate medications taken for chronic taken for chronic conditionsconditions

Reducing Risk of ECCReducing Risk of ECC
• Motivate parents to change specific parenting Motivate parents to change specific parenting practicespractices Modifying faulty feeding practices Modifying faulty feeding practices
• Be sensitive to cultural influenceBe sensitive to cultural influence
• No night-time bottle use and ad-lib bottle No night-time bottle use and ad-lib bottle
• No juice or soda in bottleNo juice or soda in bottle
• Encourage parent to use cup at an early ageEncourage parent to use cup at an early age
• Recommend reducing number (frequency) of sweet Recommend reducing number (frequency) of sweet snacks or drinkssnacks or drinks
• Limit sweets to mealtimesLimit sweets to mealtimes

Inadequate Oral Hygiene as Risk Inadequate Oral Hygiene as Risk for ECCfor ECC
• Parents not brushing their children’s teethParents not brushing their children’s teeth• Quality of cleaning is more important than Quality of cleaning is more important than
frequencyfrequency
Plaque on labial surfaces of incisors - best predictor of future development of ECC
(Alaluusua, et al , 1994)

Reducing Risk of ECCReducing Risk of ECC
• Motivate parents to change specific parenting Motivate parents to change specific parenting practicespractices Teeth cleaning Teeth cleaning
• Be flexible and give simple instructionsBe flexible and give simple instructions
• Recommend toothpaste - demonstrate amountRecommend toothpaste - demonstrate amount
• Fluoride supplementsFluoride supplements
• Professional fluoride treatmentsProfessional fluoride treatments Fluoride varnish applicationFluoride varnish application

Tooth-brushing a Young ChildTooth-brushing a Young Child
• Should begin with the Should begin with the eruption of the first tootheruption of the first tooth
• Should be supervised Should be supervised until age 7until age 7
• Only pea-sized amount Only pea-sized amount of toothpaste is neededof toothpaste is needed

ADA Recommended Supplemental ADA Recommended Supplemental Fluoride Dosage ScheduleFluoride Dosage Schedule

Fluoride VarnishFluoride Varnish
• Developed in the late 1960s and Developed in the late 1960s and early 1970s early 1970s
• By 1980s were widely used in By 1980s were widely used in European countriesEuropean countries
• In US, FDA approved as cavity In US, FDA approved as cavity liners and for treatment of liners and for treatment of hypersensitivityhypersensitivity
• Effective in reducing caries in Effective in reducing caries in permanent dentition but few permanent dentition but few studies have been done on the studies have been done on the primary dentition.primary dentition.
Which Child under Three is at High Which Child under Three is at High Risk for ECC?Risk for ECC?
• Does the child sleep with a bottle, or has the child Does the child sleep with a bottle, or has the child slept with a bottle after 12 months of age?slept with a bottle after 12 months of age?
• Does the child have frequent (3 or more/day) Does the child have frequent (3 or more/day) cariogenic snacks?cariogenic snacks?
• Does the child have visible plaque on upper Does the child have visible plaque on upper incisors? Do parents neglect to brush?incisors? Do parents neglect to brush?
• Does the family, especially older siblings, have Does the family, especially older siblings, have dental caries?dental caries?
• Does the child drink water with less than optimal Does the child drink water with less than optimal fluoride content?fluoride content?
The more “yes” answers, the greater the risk for ECC.
Milgrom and Weinstein, 1999

Oral Health Recommendations for Oral Health Recommendations for the Child with HIV Infectionthe Child with HIV Infection
• Primary dental and oral care of children with HIV Primary dental and oral care of children with HIV infection should include a careful oral examination at infection should include a careful oral examination at regular intervals, with an emphasis on oral health regular intervals, with an emphasis on oral health promotion, prevention and early intervention.promotion, prevention and early intervention.
• Dental evaluations should begin shortly after Dental evaluations should begin shortly after emergence of the first of the primary teethemergence of the first of the primary teeth
• Pediatricians, nurse practitioners, physician Pediatricians, nurse practitioners, physician assistants, dentists or hygienists may be directly assistants, dentists or hygienists may be directly involved in the early screening of patients for involved in the early screening of patients for identification of risk factorsidentification of risk factors





























