Embed Size (px)
Citation preview

1
Managing Blood Pressure in 2019: Achieving New Goals
Daniel Blanchard, MDProfessor of Medicine
UC San Diego Cardiovascular CenterLa Jolla, California

The SPRINT StudyA Randomized Trial of Intensive Versus Standard Blood-Pressure
Control
NEJM 2015;373:2103-16
2

SPRINTStudy Overview
• 9361 patients, >50 yrs (mean age 68 years, 28% >75 yrs), with SBP >130 and <180 mmHg & at increased CV risk but no DM.
• Pts were assigned to intensive treatment with a target of SBP<120 mm Hg or standard treatment with a target of SBP<140 mm Hg.

SPRINT Study
Primary end point : Composite of cardiac events including MI, HF or CV mortality.
After a median of 3.3 years, the Data Safety Monitoring Committee ended the study early.
4

The SPRINT Research Group. N Engl J Med 2015. DOI: 10.1056/NEJMoa1511939
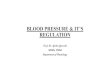
Systolic Blood Pressure in the Two Treatment Groups over the Course of the Trial
Mean # of BP medications 2.8 vs.1.8Mean SBP at 1 year 136 vs.121 mmHg

The SPRINT Research Group. N Engl J Med 2015. DOI: 10.1056/NEJMoa1511939
Primary Outcome and Death from Any Cause.
CV DeathACSHF

SPRINT Primary Outcome and its Components
Event Rates and Hazard Ratios Intensive Standard
No. of Events Rate, %/year No. of Events Rate, %/year HR (95% CI) P value
Primary Outcome
243 1.65 319 2.19 0.75 (0.64, 0.89)
<0.001
All MI 97 0.65 116 0.78 0.83 (0.64, 1.09)
0.19
Non-MI ACS 40 0.27 40 0.27 1.00 (0.64, 1.55)
0.99
All Stroke 62 0.41 70 0.47 0.89 (0.63, 1.25)
0.50
All HF 62 0.41 100 0.67 0.62 (0.45, 0.84)
0.002
CVD Death 37 0.25 65 0.43 0.57 (0.38, 0.85)
0.005

SPRINT Study
The benefit was greatest in the SENIOR group (>75 yrs):
33% v. 25%: primary endpoint (CV death, ACS, heart failure)
34% v 27%: mortality.
37% reduction in acute HF: NNT 28--(HF increased mortality rate 27-fold)--NNT to prevent a death: 41
8

SPRINT Study:Serious adverse events
Intensive treatment
Standard treatment
Hazard ratio P value
> 30% reduction in GFR
1.2 %/y 0.35 %/y 3.49 <0.001
Hypotension 2.4 % 1.4 % 1.67 0.001
Electrolyte abnormalities
3.1 % 2.3 % 1.35 0.02
AKI 4.1 % 2.5 % 1.66 <0.001
Orthostatic hypotension
16.6 % 18.3 % 0.88 <0.001
Important?

Conclusions
• Among non diabetic patients at high CV risk (especially in the elderly), SBP goal of <120 mmHg resulted in lower rates of major CV events and death from any cause compared with goal of <140 mmHg,

Conclusions
• But, aggressive treatment was associated with higher rates of adverse events, including renal dysfunction, hypotension, and electrolyte abnormalities.

N Engl J MedVolume 362(17):1575-1585
April 29, 2010
The ACCORD Study Group
Effects of Intensive BP control in Type 2 DM

Study Overview
• 4733 patients, mean age 62 yrs with type 2 DM, with high CV risk received treatment aimed at a target systolic BP of <120 mm Hg or <140 mm Hg.
• Primary end point: nonfatal MI, nonfatal stroke, or CV death.
•• Mean follow-up of 4.7 years.

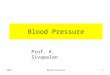
Mean Systolic Blood-Pressure Levels
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585
At 1 y mean SBP 133 v 119 mmHg
Baseline SBP 139/76 for both groups
Number of meds: 3.4 vs. 2.1

Kaplan-Meier Analyses
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585
Annual rate1.9% v 2.1%l
Event rate in the standard therapy: 50% less than expected

Primary and Secondary Outcomes
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585
Number of patients treated for 5 yrs. to prevent 1 stroke = 89

The ACCORD Study: Signals of adverse effects
Intensive Therapy Standard Therapy
Elevation in Scr > 1.5Scr > 1.3
13 %11 %
8 % (p<0.001)7 % (P<0.001)
Potassium <3.2 2.1% 1.1%(P=0.01)
eGFR < 30 ml/min 4.2% 2.2% (<0.001)
Higher incidence of hypotension (0.7% vs. 0.04%, P<0.001)

• In patients with type 2 DM with high CV risk, targeting a systolic BP of <120 mm Hg as compared with <140 mm Hg did not reduce major CV events, but increased the likelihood of hypotension & adverse renal outcome.
ACCORD - Conclusions

• Bummer of a result.
• 2/3 of diabetic patients have HTN
• Are there newer treatments for pts with diabetes and HTN?
• .
ACCORD - Conclusions

Sodium-Glucose Contransporter 2 (SGLT2) Inhibitors
New agents that improve diabetic control and
decrease weight.
Recent small studies of effect on blood pressure:

Sodium-Glucose Contransporter 2 (SGLT2) Inhibitors
12-week effect on BP in
T2DM pts with nocturnal
hypertension
Kario, et al. Circulation 2019;139:2089

Sodium-Glucose Contransporter 2 (SGLT2) Inhibitors
24-week effect on BP in African-American pts with T2DM & HTN
Ferdinand, et al. Circulation 2019;139:2098

How do we apply the results of SPRINT to real world practice?
BP was measured with patients seated for 5 min
in a quiet room without talking, as an average of
3 measurements with an automated device and
with the observer outside the room.
Is your practice setting like this??

How do we apply the results of SPRINT to real world practice?
BP readings were probably ~10 mmHg
lower than typical practice readings,
suggesting a <130 mmHg rather than <120
mmHg target for systolic BP.

SPRINT vs. the real world
The excess of hypotension, syncope, AKI,
and electrolyte disturbances in the intensive
arm suggests caution in targeting systolic BP
levels <120 mmHg in usual clinical practice.

New Guidelines, Nov. 2017
Normal systolic BP remains below 120 mmHg
Decrease in target BP from 140/90 to maximum of 130/80 mmHg
Goal of <120 mmHg is most useful in clinics that use the SPRINT method to measure BP.
In those that don’t (the majority), 130/80 or less may be a better goal

New Guidelines
Hypertension has been split into stage 1 (130/80 to 139/89 mm Hg) and stage 2 (140/90 mm Hg and higher)
Goals for BP lowering in stage 1 are primarily non-pharmacologic, unless ACC/AHA ASCVD 10-year risk calculation is >10%
Recommendations include: Weight loss, DASH diet, Alcohol moderation, Physical activity

“ASCVD Risk Estimator Plus” Free App from American College of Cardiology
Risk based on
– Age & Sex
– Racial background
– Blood pressure
– Total cholesterol & HDL
– History of diabetes
– History of smoking
– Use of antihypertensives, statins, & aspirin
This is a novel concept in guiding HTN treatment

New Guidelines Stage 1 Hypertension with low 10-yr CV risk
(<10%): institute lifestyle changes, f/u in 3-6 mo.
Stage 1 HTN with elevated CV risk: lifestyle changes and one antihypertensive medication, follow-up in a month.
Stage 2 HTN: lifestyle changes and TWO anti-hypertensive medications, follow-up in less than a month.

New Guidelines Before beginning antihypertensive meds, it is
reasonable to first measure home and ambulatory blood pressures
Patients with resistant HTN, sudden onset HTN, young age at onset, etc., should be screened for secondary HTN.
Almost all patients over 75 have >10% 10-year ASCVD risk

Benefit vs. Harm
But all quartiles had lower event rates with intensive treatment

New Guidelines
Prevalence of HTN in Americans will increase from ~32% to ~40% of adults.
Focus on home and ambulatory BP measurement to identify white-coat & masked HTN.
NHLBI sponsored, with many organizations signed on—but not the ADA, ACP, and ACFP

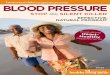
Sim J, et al. JACC 2014;64:588-97.
400,000 Kaiser Patients on Medications for Hypertension

Sim J, et al. JACC 2014;64:588-97.

35
Always room for improvement…

36

SPRINT vs. ACCORD:Why the Difference?
ACCORD SPRINT
Population 4733 9361
Diabetes? Yes No
Mean age 62 68
Primary outcome 9 vs 10% 5 vs 7%
Major CV event 10.6 vs 11.4% 2.9 vs 3.3%
37
Three times the CV event rate in ACCORD vs. SPRINT:Could this overwhelm the benefit from BP lowering?