Embed Size (px)
Citation preview
MANAGEMENT OF VENTRICULAR TACHYARRYTHMIAS
Dr. Chetana Sen
Chairperson: Dr.B.P. Chatterjee

Definition• Ventricular tachyarrythmia defined as a
tachycardia (HR>100 bpm) in which the driving circuit or focus originates solely in ventricular tissue or Purkinje fibers.

Classification of Ventricular Arrhythmia by ECG (ACC)
• Ventricular Tachycardia: VT is a cardiac arrythmia of 3 or more consecutive complexes emanating from the ventricles at a rate > 100bpm (cycle length less than 600ms)
1. Sustained VT: VT greater than 30s in duration and or requiring termination for hemodynamic compromise in less than 30s.– Monomorphic- stable single QRS morphology– Polymorphic-changing or polymorphic QRS, cycle length
between 600 and 180ms
2. Nonsustained VT: VT terminating spontaneously within 30seconds.– Monomorphic– Polymorphic

Classification of Ventricular Arrhythmia by ECG (ACC)
• Bundle-branch re-entrant tachycardia
• Bidirectional VT
• Torsades de pointes
• Ventricular flutter
• Ventricular fibrillation

Initial Presentation
• Stable or Unstable
• History of CAD or previous MI
• History of syncope
• Depressed LV function
• Baseline ECG
Hemodynamically unstable:• chest pain
• shortness of breath• decreased level of
consciousness• Cardiogenic Shock
• pulmonary congestion,• congestive heart failure
• AMI• Wide complex or Narrow complex
• Regular or Irregular• Relation of P wave with
QRS• Diagnosis?

• 60 yr old, with ischemic heart disease and h/o MI 4 yrs ago presented with chest pain,drowsiness, BP 80/50,PR 150/min.
HemodynamicallyUnstable
Wide QRS > 120ms

ACLS protocol for Hemodynamic unstable Tachycardia with pulse



• VT or SVT with aberrancy???
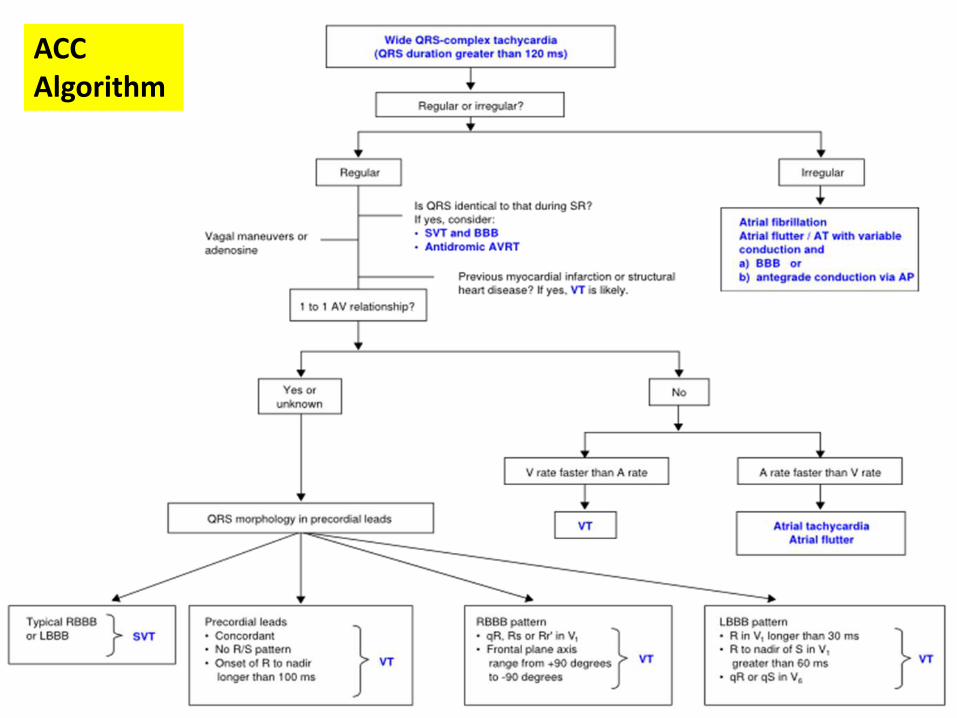
ACC Algorithm

A 45 yr woman with palpitations
• Wide QRS complex• Irregularly irregular• LBBB pattern, no
secondary R wave in V1, no q in V6
Atrial fibrillation with LBBB

Brugada Criteria for SVT with aberrancy vs VT

Features favoring VT:
Taller left ‘rabbit ear’ in VT
N-W axis
Concordance
Reversible causes of VT
• Hypoxia• Hyperthyroidism• Catecholamines• Hypokalemia• Metabolic acidosis• Hypomagenesemia• Hypocalcemia• Drugs• Alcohol• Starvation

Principles of Management
1. Acute Management
2. Long term management for secondary prophylaxis of VT and prevention of Sudden Cardiac Death
3. Management of specific VT1. With structural heart disease/coronary artery
disease
2. Idiopathic VT
3. Inherited VT
Acute Management of Specific ArrhythmiasSustained Monomorphic VT
• Wide-QRS tachycardia should be presumed to be VT if diagnosis is unclear. (Class I)
• DC cardioversion in hemodynamic compromise.(Class I)• Iv procainamide for initial treatment of patients with
stable sustained monomorphic VT.(IIa)• Iv amiodarone if refractory. (IIa)• Iv lidocaine-initial management in MI.(IIb)• No response or frequently recurrent despite anti
arrythmics- transvenous catheter pacing. (IIa)• Calcium channel blockers should not be used in
patients to terminate wide-QRS-complex tachycardia of unknown origin, especially in patients with a history of myocardial dysfunction(III)

Acute Management of Specific Arrhythmias
Polymorphic VT
• Hemodynamic compromise-DC cardioversion (I)
• IV beta blockers are useful for patients with recurrent polymorphic VT, especially if ischemia is suspected or cannot be excluded. (I)
• IV loading with amiodarone in recurrent polymorphic VT in the absence of abnormal repolarization related to congenital or acquired LQTS. (I)
• Urgent angiography with a view to revascularization when myocardial ischemia cannot be excluded.(I)
• IV lidocaine in polymorphic VT specifically associated with acute myocardial ischemia or infarction. (IIb)
Principles of management:Long term management-Non sustained VT
• Goal of long-term therapy-prevent sudden cardiac death and recurrence of symptomatic VT,
• Asymptomatic nonsustained ventricular arrhythmias in low-risk populations -often need not be treated.
• Symptomatic non-sustained tachycardia-
– beta blockers
– Class IC agents, sotalol, or amiodarone can be effective.
– class IC agents should be avoided in patients with structural heart disease,especially CAD-Proarrythmic.

Principles of management:Long term management-Sustained VT
• Sustained VT or cardiac arrest in patients with structural heart disease
– Class III better than class I.
– empiric amiodarone-better survival than EP-guided antiarrhythmic drugs, and
– ICDs provide better survival than amiodarone.
• In patients who have survived cardiac arrest or who have sustained VT resulting in hemodynamic compromise and poor LV function (EF<0.35):
– ICD is the treatment of choice.
– In patients who refuse an ICD, empiric amiodarone.

• Anti-Tachycardia Pacing/Overdrive pacing• Rate Discrimination
• Rhythm Discrimination• Morphology Discrimination
Specific VT-VT in Ischemic cardiomyopathy
• Healed MI is the most frequent clinical setting for the development of sustained VT
• In the setting of a remote myocardial infarction:– the mechanism of VT is reentry
– Involves infarct scar and border zone
– VT in this setting typically monomorphic.
• Polymorphic VT or VF in the setting of ischemic heart disease usually occurs during active ischemia or infarction.

55 yr male, h/o MI 5 yrs ago, with chest pain and palpitations..
• Q waves (qR, QR or Qr) in related leads
• Notched or wide QRS complexes
• Low QRS voltage• A-V dissociation
• Paroxysmal sustained episodes
Sustained monomorphic VT in old MI

• Lateral wall- RBBB• Septal wall- LBBB
• QRS in Inferior leads:• Inferior wall- superior axis Epicardial site of exit• Anterior wall- superior or inferior axis
• QRS in precordial leads:• Basal- Positive concordance• Apical-Negative concordance

VT in Ischemic cardiomyopathy
Treatment:ICD therapy is indicated in1. patients resuscitated from VF when coronary revascularization is
not possible, and there is evidence of prior MI and significant LV dysfunction (class I)
2. patients with LV dysfunction due to MI who present with hemodynamically unstable VT (class I).
3. Primary prevention in patients with LV dysfunction due to prior MI who are at least 40 days post-MI and have an LVEF ≤30%-40% and NYHA class II or III (class I, level of evidence A).
4. Primary prevention in patients with LV dysfunction due to prior MI who are at least 40 days post-MI, and have an LVEF ≤30%-35% and NYHA class I (class Iia) patients with post-MI with normal LV function and recurrent VT (class IIa).

• Drugs:1. Amiodarone or sotalol, in combination with beta-blockers if
possible, as an adjunctive therapy to reduce symptoms in patients with prior MI, LV dysfunction, and VT unresponsive to beta-blockers alone/ frequent ICD shocks/ non candidates for ICD
2. Prophylactic antiarrhythmic drug therapy is not indicated to reduce mortality, but only to reduce symptoms in patients fulfilling the characteristics above mentioned. (III)
3. Class IC antiarrhythmic drugs in patients with a past history of MI should not be used. (III)
• Ablation reserved for refractory VT or very well tolerated VT. • Surgical endocardial resection of the scarred area in refractory VT
caused by previous infarction. • For recurrent VT or VT storm refractory to medications or ablation,
cardiac sympathetic denervation has been effective in limited studies.

VT in Dilated Cardiomyopathy(non-ischemic)
• ventricular arrhythmias and sudden death
• Incidence of VT –50-60% DCM, resp for 8-50% deaths
• Macro reentry -dominant mechanism
• Bundle branch reentry ventricular tachycardia (BBRVT) is the most characteristic
• BBRVT Responsible for VT in up to 41% of DCM

VT in Dilated Cardiomyopathy(non-ischemic)
• EP testing-– to diagnose bundle-branch reentrant tachycardia and to guide ablation.– diagnostic evaluation in sustained palpitations, wide-QRS-complex
tachycardia, presyncope, or syncope (I)
• ICD –(receiving chronic optimal medical therapy, and who have reasonable expectation of survival with a good functional status for more than 1 year.)
1. significant LV dysfunction who have sustained VT or VF (I)2. for primary prevention to reduce total mortality by a reduction in SCD
who have an LVEF less than or equal to 30% to 35%, are NYHA functional class II or III. (I); or even in NYHA class I (IIb)
3. unexplained syncope, significant LV dysfunction4. termination of sustained VT in patients with normal or near normal
ventricular function
• Amiodarone for sustained VT/VF (IIb)

Bundle Branch Reentrant VT
• Commonly in disease with severe LV dysfunction like DCM & conduction abnormalities in the HPS
• BBR VT may also be seen in:– Myotonic dystrophy
– Hypertrophic cardiomyopathy
– Ebstein anomaly
– Following valvular surgery
– Proarrhythmia due to Na channel blockers
• Presyncope, syncope or sudden death - VT with fast rates > 200 bpm

ECG in sinus rhythm - non-specific or
typical BBB patterns with prolonged QRS
duration
• EPS:His electrogramsprecede each V
• HV interval during tachycardia > HV in
baseline• Changes in V–V interval
follow the changes in H–H
Bundle Branch Reentrant VT
• High recurrence rate after drugs
• RFA - first line therapy; ablation of the RB
• A PPI should be implanted if the post-ablation HV interval is 100 ms or longer
• ICD implant should be considered if myocardial VT occur spontaneously or are inducible or if EF < 35%

VT in Hypertrophic Cardiomyopathy
• SCD in adults with asymptomatic HCM- 1%, NSVT – 8%
• On 24-hr Holter -90% have ventricular arrhythmias
• Long term prophylactic pharmacologic therapy now not recommended in high-risk population
• Risk Factors for SCD??
1. Family history of premature HCM-related death2. Unexplained syncope, particularly in young patients, or if
demonstrated to be arrhythmia-based3. Frequent, multiple, or prolonged episodes of NSVT4. Hypotensive or attenuated BP response to exercise
5. Extreme LVH with maximum wall thickness ≥ 30 mm

VT in Hypertrophic Cardiomyopathy
• ICD (receiving chronic OMT with reasonable expectation of survival with a good functional status for more than 1 year)– sustained VT and/or VF.(I)
– primary prophylaxis against SCD.(IIa) • Amiodarone therapy can be effective for treatment in
patients with HCM with a history of sustained VT and/or VF, or for prophylaxis of SCD when an ICD is not feasible.(IIa,IIB)
• EP testing may be considered for risk assessment for SCD in patients with HCM.(IIb)

Arrythmogenic Right Ventricular Dysplasia
• Ventricular arrhythmias are usually exercise-related
• Sensitive to catecholamines
• Most Common- LBBB morphology VT
• RBBB VT - LV involvement or a left septalbreakthrough site
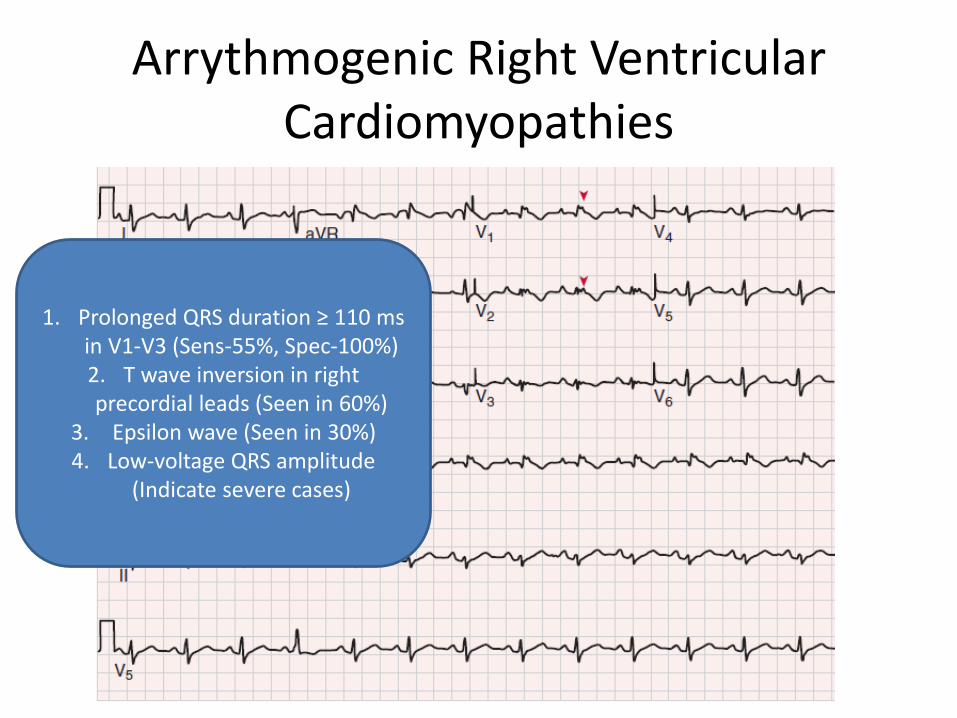
Arrythmogenic Right Ventricular Cardiomyopathies
1. Prolonged QRS duration ≥ 110 msin V1-V3 (Sens-55%, Spec-100%)2. T wave inversion in right precordial leads (Seen in 60%)
3. Epsilon wave (Seen in 30%)4. Low-voltage QRS amplitude
(Indicate severe cases)

Arrythmogenic Right Ventricular Cardiomyopathies
• Documented VT/VF on chronic OMT, have reasonable expectation of survival- ICD to prevent SCD
• Severe disease LV inv, FH of SCD, undiagnosed syncope, on chronic OMT-ICD
• Amiodarone or sotalol effective , when ICD not feasible
• Ablation can be adjunctive
• EP testing might be useful for risk assessment

Bidirectional VT
• Bidirectional ventricular tachycardia (BVT) is a rare ventricular dysrhythmia characterised by a beat-to-beat alternation of the frontal QRS axis.
Causes
• most commonly associated with severe digoxin toxicity.
• familial catecholaminergic polymorphic ventricular tachycardia (CPVT).
• herbal aconite poisoning.

Bidirectional VT
• QRS axis shifts 180 degrees from left to right with each
alternate beat.• Another possible pattern is
alternating left and right bundle-branch block

Idiopathic VT-RVOT/LVOT
• Only 10% of cases of VT occur in the absence of structural heart disease, termed idiopathic VT.
• The majority of idiopathic VTs (75-90%) arise from the right ventricle — e.g right ventricular outflow tract tachycardia(RVOT).
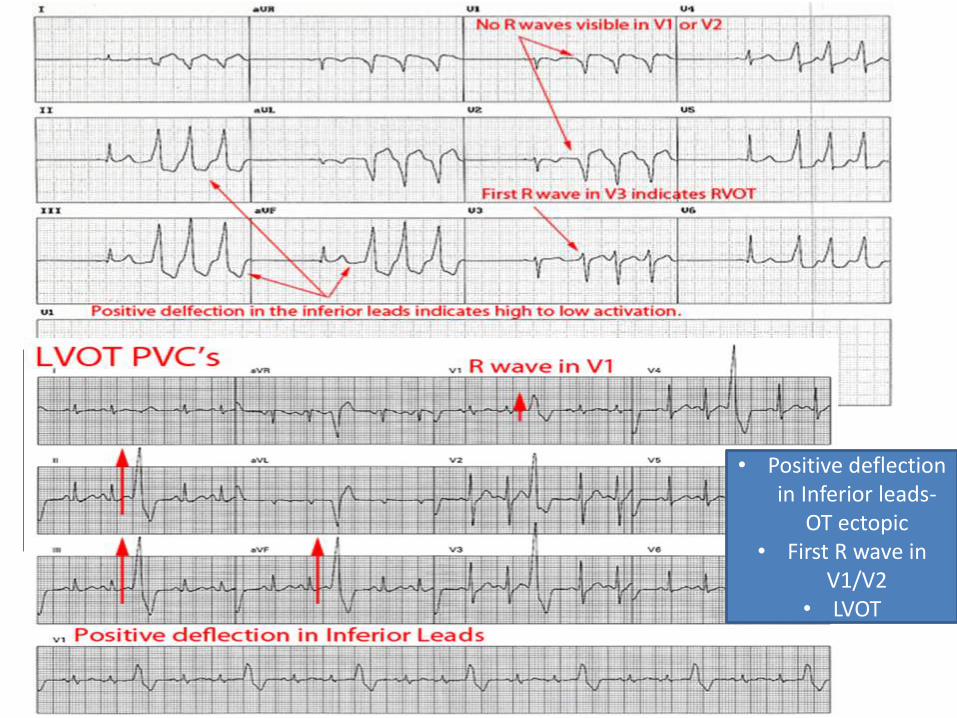
• Positive deflection in inferior leads-Outflow tract ectopic• First R wave in V3
• RVOT• Positive deflection
in Inferior leads-OT ectopic
• First R wave in V1/V2
• LVOT

Fascicular VT• Most common idiopathic VT of the left ventricle.• It is a re-entrant tachycardia, typically seen in young patients
without structural heart disease.• Diagnosis can be difficult and this rhythm is often
misdiagnosed as SVT with RBBB• Verapamil is the first line treatment.Causes• Young healthy patients (15-40 years of age; 60-80% male).• Most episodes occur at rest but may be triggered by exercise,
stress and beta agonists.• A similar ECG pattern of fascicular VT may occur with
digoxin toxicity, but here the mechanism is enhanced automaticity in the region of the fascicles.
• Digoxin-induced fascicular VT is responsive to Digoxin Immune Fab.
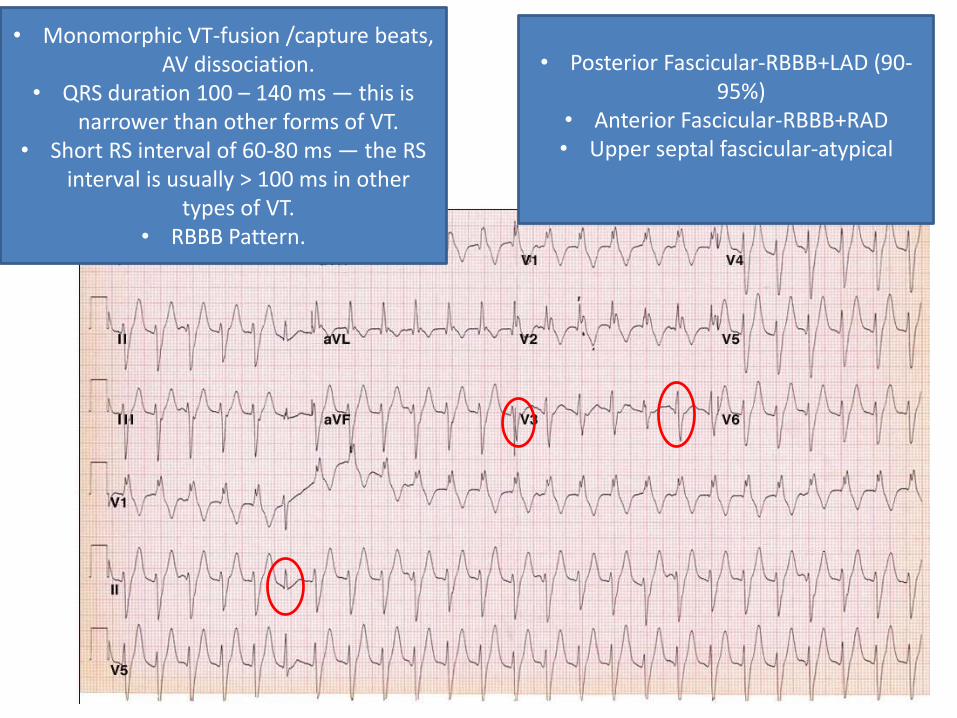
• Monomorphic VT-fusion /capture beats, AV dissociation.
• QRS duration 100 – 140 ms — this is narrower than other forms of VT.
• Short RS interval of 60-80 ms — the RS interval is usually > 100 ms in other
types of VT.• RBBB Pattern.
• Posterior Fascicular-RBBB+LAD (90-95%)
• Anterior Fascicular-RBBB+RAD• Upper septal fascicular-atypical

20yr female, went swimming, following which she had a syncope. Her ECG.
• Markedly prolonged QT (QTc~700 ms)
• Wide and ample T waves in V2-V4, deep T wave inversion
in the inferior leads• T wave alternans
T wave alternans may be seen in a subgroup of patients with prolonged QT and implies a very heterogeneous repolarization and a more imminent risk of TdP. More typically seen in congenital long QT syndrome

Long QT syndrome
QT interval : total duration of ventricular activity.
• Need for QTc Interval :The QT interval varies with RR interval. False high values may be noted in Bradycardias.
• BAZETT’s Formula : QTc = QT ∕√ (RR) (RR in seconds)• A useful rule of thumb is that, with a normal heart rate ( 60 - 100
bpm), the QT interval SHOULD NOT exceed half the RR interval.
• D/D for long QT:• Electrolytes ( low K, low Mg, low Ca) (+other: hypothyroidism)• Drugs (antiarrhythmics class I, III; macrolide or quinolone antibiotics;
antipsychotics…)• Ischemia• Congenital long QT syndrome (LQT 1,2,3)

Congenital Long QT syndromeLQT1 Gene
• Most common type; 80% have first presentation < 20 yrs
• T wave is broad and occupies majority QT interval
• Most common triggers: exercise, emotional stress; Respond to beta-blockers
• Jervell Lange syndrome and Romano Ward syndrome are severe forms.
LQT2 Gene
• T wave tends to be bifid and notched
• Additional Trigger factors are sleep, auditory stimulation
• Respond to B-Blockers
LQT3 Gene
• Poorest prognosis amongst all
• T wave is asymmetrical or Late biphasic
• Trigger factor : Bradycardia ( sleep )
• B-Blockers Contraindicated; Exercise is not Restricted
Implantation of an ICD along with use of beta blockers is recommended for LQTS patients with previous cardiac arrest or syncope or VT.

Pt goes into this rhythm
Torsades de pointe (polymorphic VT with changing QRS polarity, with a long baseline QTc)
VF (disorganized and chaotic rhythm, QRS almost vanishes every now and then) Defibrillation
sinus

Torsades de Pointes
• 3 therapies:1-Defibrillation2-Magnesium 2 g IV (regardless of Mg level) + start correcting K3-Temporary pacing after the run of TdP has resolved. Temporary pacing prevents TdP from recurring:
Usually, TdP occurs in a pt with prolonged QT who is also bradycardic. Bradycardia further prolongs QT and furthers disperses repolarizationdelays across the myocardium. Bradycardia is a major trigger of TdP, particularly TdP in patients with acquired long QT. Pacing to a rate of 80-100 bpm will prevent TdP recurrence.
Pacing does not apply to our pt here because he is tachycardic. Congenital long QT, as opposed to acquired long QT, is often triggered by catecholamine surge and may be associated with tachycardia
No Amiodarone. Amiodarone prolongs QT

27 yr male, with syncope, family h/o SCD.
RBBB pattern ST elevation in leads
V1 through V3. Type 2 Brugada pattern with a “saddleback” ST-segment
elevation greater than 1 mm and a biphasic T wave in V1
(positive in V2-V3).
Aftera procainamide challenge, the prototypic changes on the ECG
are exaggerated, with an increase in ST elevation, ECG shows a type 1 pattern with a
downward-slopingcoved ST elevation and negative
T waves in V1-V3.

Brugada Syndrome
• RBBB and ST-segment elevation in the anterior precordial leads, without any evidence of structural heart disease
• Type 1, type 2, or type 3 patterns on ECG • Brugada syndrome should be suspected in :
– type 1 ECG pattern in >1 right precordial lead (V1 to V3) if there is documented VF, polymorphic VT, family history of SCD, Brugada-pattern ECG in other family members, or syncope.
– Type 2 and type 3 findings on the ECG are not diagnostic of Brugada syndrome.
– If type 2 or type 3 ECG patterns (in more than one right precordial lead) convert to a type 1 pattern after Procainamide challenge + at least one clinical criterion (listed above) is also present=consider the diagnosis of Brugada syndrome
• Mutations in genes for the sodium channel (SCN5A) and calcium channel have been identified in many families

Brugada Syndrome
• ICD for prevention of SCD
• Isoproterenol for VT storm; also Quinidine.
• EP study for risk stratification in asymptomatic Brugada Syndr.

Premature Ventricular Contraction

Accelerated Idioventricular Rhythm
• AIVR results when the rate of an ectopic ventricular pacemaker exceeds that of the sinus node.
• AIVR is classically seen in the reperfusion phase of an acute STEMI, e.g. post thrombolysis.
• Usually a well-tolerated, benign, self-limiting arrhythmia.
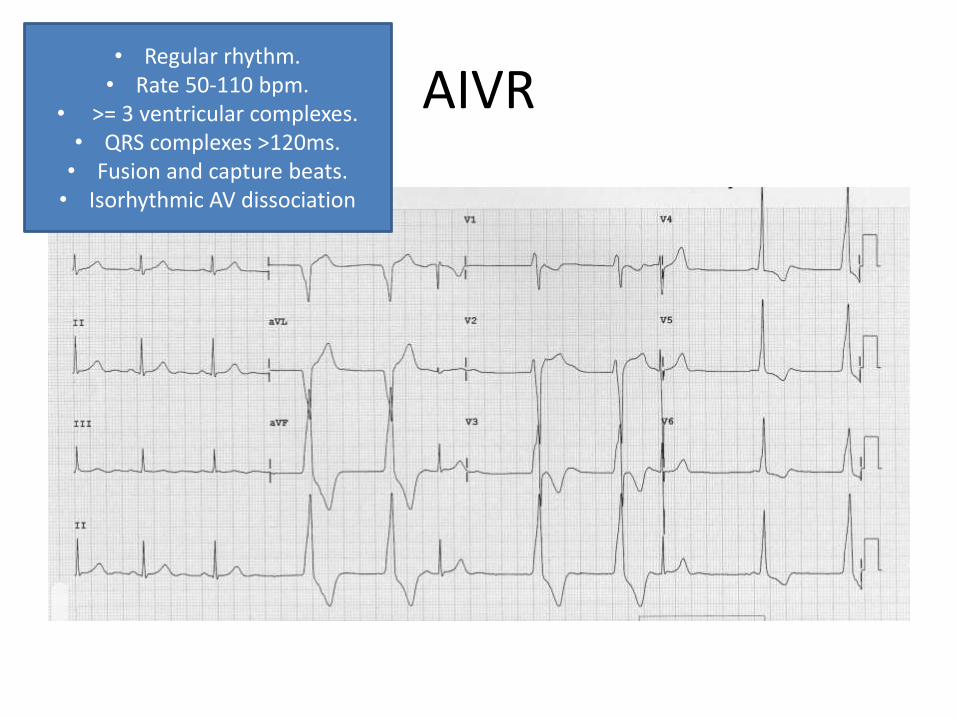
AIVR• Regular rhythm.• Rate 50-110 bpm.
• >= 3 ventricular complexes.• QRS complexes >120ms.• Fusion and capture beats.• Isorhythmic AV dissociation

Ventricular Flutter/Fibrillation
V. flutter
V. Fibrillation

Thank You





























