-
Paediatric Respiratory Reviews xxx (2013) xxxxxx
G Model
YPRRV-903; No. of Pages 8
Mini-Symposium: Respiratory Emergencies in Children
Management of status asthmaticus in children
Muriel Koninckx 1,*, Corinne Buysse 2, Matthijs de Hoog 2
1 Paediatric Intensive Care, Middelheim Ziekenhuis, Lindendreef
1, Antwerp, Belgium2 Paediatric Intensive Care, Sophia Childrens
Hospital, Dr Molewaterplein 60 Rotterdam, The Netherlands
A R T I C L E I N F O
Keywords:
Paediatric status asthmaticus
Pathophysiology
Assessment
Treatment
S U M M A R Y
Recent literature on paediatric status asthmaticus (PSA)
confirms an increasing percentage of admissions
to paediatric intensive care units. PSA is a medical emergency
that can be fatal and needs careful and
prompt intervention. The severity of PSA is mainly determined by
clinical judgement of signs and
symptoms. Peak flow measurements and serial lung function
measurements are not reliable in PSA.
Validated clinically useful instruments are lacking. The three
main factors that are involved in the
pathophysiology of PSA, bronchoconstriction, mucus plugging and
airway inflammation need to be
addressed to optimise treatment. Initial therapies include
supplementation of oxygen, repetitive
administration of rapid acting b2-agonists, inhaled
anticholinergics in combination with systemicglucocorticosteroids
and intravenous magnesium sulphate. Additional treatment modalities
may include
methylxanthines, DNase, ketamine, sodium bicarbonate, heliox,
epinephrine, non-invasive respiratory
support, mechanical ventilation and inhalational
anaesthetics.
2013 Elsevier Ltd. All rights reserved.
EDUCATIONAL AIMS
The reader will be able to:
Understand the pathophysiology of paediatric status asthmaticus
Assess the severity of an asthma exacerbation, Implement different
treatment strategies for severe asthma.
Contents lists available at SciVerse ScienceDirect
Paediatric Respiratory Reviews
INTRODUCTION
Paediatric status asthmaticus (PSA) is a medical
emergencywarranting prompt recognition and intervention. A status
asth-maticus or severe asthma exacerbation is defined as an
acuteepisode that does not respond to standard treatment with
shortacting b2-agonists and corticosteroids, although a large
variationexists in this definition between authors.13 In other
definitions,need for hospitalisation, emergency room visit or
decline in peakexpiratory flow (PEF) is also taken into account.
PSA can result inrespiratory insufficiency as well as circulatory
failure and ispotentially life-threatening. The incidence of PSA
has to be viewedagainst the background of the total number of
asthmatic patients.4
In the United States, the number of patients with
asthmaincreased from 20.3 million to 25 million between 2009 and
2011.In 2009 the prevalence among children (less than 18 years old)
was
* Corresponding author. Tel.: +0032/496068751; fax:
+0032/2810292.
E-mail address: [email protected] (M. Koninckx).
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
1526-0542/$ see front matter 2013 Elsevier Ltd. All rights
reserved.http://dx.doi.org/10.1016/j.prrv.2013.03.003
9.6%. The prevalence in children is higher than in adults
(9.6%versus 7.7%). Mortality in children is lower compared to
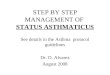
adults.Asthma was linked to 3,447 deaths including 5.4% children
(about9 per day) in 2007.5 The prevalence of asthma is
increasing,however, mortality is decreasing. This might, in part,
be due to acoding change from ICD-9 to ICD-10 (Fig. 1). In the
ICD-9classification asthma was subdivided in intrinsic, extrinsic
andchronic obstructive asthma. The ICD-10 classification uses
thedescriptors of mild, moderate and severe asthma.
The increasing prevalence of asthma is seen mainly indeveloped
countries. Environmental factors play an importantrole in this
disease, next to genetic predisposition.6 Data on theincidence or
prevalence of PSA are scarce. In a New Jersey cohort,admission for
status asthmaticus between 1992 and 2006approximately halved from
1.92 to 0.93 per 1000 children. Incontrast, ICU care related to
asthma increased from 0.09 to 0.31 per1000 patients. A much higher
percentage of children admittedto hospital for status asthmaticus
received ICU care, but the rateof children needing mechanical
ventilation was the same
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003mailto:[email protected]://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003http://www.sciencedirect.com/science/journal/15260542http://dx.doi.org/10.1016/j.prrv.2013.03.003
-
Figure 1. Number and rate* of asthma deaths, by year and
International Classificationof Diseasesy (ICD) United States,
1980-2004.
M. Koninckx et al. / Paediatric Respiratory Reviews xxx (2013)
xxxxxx2
G Model
YPRRV-903; No. of Pages 8
(0.02/1000).7 In Finland about 1% of the hospital admissions
forasthma need intensive care, but numbers vary between 1 to
15%.Since indications for PICU admission vary between countries
thesenumbers are hard to compare.8 The number of children that
needmechanical ventilation is decreasing and varies between 8 and
33%of the PSA related PICU admissions.9 This may be due to
theincreasing use of non-invasive respiratory support for
severeasthma. It can be concluded that more children with PSA
areadmitted to the ICU but the need for invasive
mechanicalventilation seems to have decreased, although this is
influencedby admission criteria. Mechanical ventilation in PSA is a
risk factorfor mortality in the 10 years after discharge and close
follow up issuggested.8,9
PATHOPHYSIOLOGY OF STATUS ASTHMATICUS
The three main factors that are involved in the
pathophysiologyof asthma are bronchoconstriction, mucus plugging
and airwayinflammation, with the exacerbation usually induced by a
viralinfection.10 The relative contribution of these factors
determinesthe targets for optimal therapy. Some patients
underestimate theseverity of airway obstruction: they have a
reduced sensation ofdyspnoea while breathing with increased airway
resistance andhave decreased hypoxic ventilatory drive, resulting
in little reserveat presentation.11 These are patients that are
predisposed to nearfatal asthma.
In fatal and near fatal asthma we can distinguish two
differentclasses: type I or slow onset fatal asthma and type II or
rapid onsetfatal asthma.12 Predisposing factors in type I are
inadequatetherapy, inadequate compliance, inappropriate control and
psy-chological factors. Type II can occur epidemically (soybean,
castorbean or unknown) or sporadically (NSAID, allergen, sulphites,
foodor unknown).13
Type I is a progressive obstruction of the airways in
patientsalready constantly using bronchodilators. These patients
areusually undertreated with inhaled corticosteroids.
Bronchodilatingmedications cause a maximal smooth muscle
relaxation. Mean-while, the process of inflammation and oedema
continues due toinadequate treatment. Only a small increase in
oedema orinflammation can be fatal. Given the state of maximal
broncho-dilation, further use of short acting b2-agonists will not
have muchadditive effect and cannot reverse the bronchial
obstruction. Thesepatients are at risk for severe therapy resistant
PSA. Airwayplugging is demonstrated and secretions are
characterised byeosinophils in pathological examinations.14 In a
prospective study
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
of the characteristics of (near) fatal asthma, about 80% belong
totype I.15 These exacerbations are preventable with
extensiveasthma control and administration of adequate doses of
inhaledcorticosteroids.
Type II is a rapid onset type, also called sudden
asphyxialasthma. It is an acute and sudden onset form where death
canfollow in only a few hours after start of the clinical
symptoms.Severe bronchospasm occurs with little or no mucus
plugging andairway inflammation.3,12 In contrast, Type I cases
demonstratemainly neutrophilic inflammation. In this type there is
a higherincidence of respiratory arrest, impaired consciousness
level, alower pH and a silent chest reported. Clinical improvement
isdirectly related to improvement of bronchoconstriction.
Thesepatients can deteriorate very rapidly, but with
appropriateinterventions recovery can be accomplished swiftly, as
demon-strated by a shorter length of hospital stay and fewer hours
ofmechanical ventilation.15
The previously described mechanisms cause an occlusion of
theairway lumen with reduced ventilation leading to low
ventilation/perfusion(V/Q) ratios and gas exchange abnormalities.
Thedistribution of areas with reduced ventilation and
hypoxicvasoconstriction is widespread through the bronchial tree
andinterspersed with areas of better V/Q.
An important complication of PSA is airleak which may
manifestwith pneumothorax, pneumomediastinum, subcutaneous
emphy-sema and pneumopericardium due to increased
intrathoracicpressure.4 This is mainly seen in PSA patients
ventilated with highpeak pressures and is one of the drivers for
the increasing use of non-invasive ventilation in the acute
setting.4 Myocardial infarction,hardly seen in children, is
possible due to hypotension and elevatedinthrathoracic pressures.
This increases left ventricular afterloadwhich can in turn decrease
coronary blood flow. Mucus plugging canprovoke atelectasis.
Electrolyte disturbances including hypokalemiacaused by salbutamol
are possible. Myopathy and rhabdomyolysisare described when giving
steroids in combination with neuromus-cular blockers.16 Lactic
acidosis and anoxic brain injury have alsobeen described.17 These
problems warrant close monitoring andspeedy intervention in a
PICU.
DETERMINATION OF ASTHMA SEVERITY
A gold standard for the assessment of the severity of an
asthmaexacerbation does not exist. Similar to adults, there is a
lack ofvalidated instruments to determine asthma severity in
children.The primary importance of defining severity is to
determinefurther patient management. Depending on severity patients
canbe divided into life threatening asthma, necessitating
immediatetherapy and PICU admission, slow responding forms that
needhospital admission and patients that can be discharged
directlyfrom the emergency department. Second, a tool for
definingseverity of PSA can be used to assess the effect of
therapeuticinterventions. Peak flow measurements, serial lung
functionmeasurements, pulse oximetry and clinical examination
andasthma scoring systems are tools that can be potentially
helpful.
Peak flow measurements and serial lung function measurements
Peak expiratory flow rates (PEFR) or forced exipiratory volumein
one second (FEV1) are difficult to reliably perform in childrenwith
acute asthma, especially in those under 5 years of age. Inchildren
aged between 6 and 18 years, only 64% were able toperform PEFR
adequately.18 Stable peak flow records can bepresent despite severe
bronchial hyperresponsiveness resulting infatal asthma.19 Thus, it
is not recommended to rely on peak flowmeasurements for assessing
severity.
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003
-
M. Koninckx et al. / Paediatric Respiratory Reviews xxx (2013)
xxxxxx 3
G Model
YPRRV-903; No. of Pages 8
Pulse oximetry
Measuring SaO2 is an important tool to determine asthmaseverity,
but always in combination with other parameters. InitialSaO2 95%
91-95%
PaCO2 < 5.6 kPa < 5.6 kPa
PaO2 Normal > 8 kPa
C.A. Camargo, G. Rachelefsky, M. Schatz. Managing asthma
exacerbations in the emergen
expert panel report 3 guidelines for the management of asthma
exacerbations. Proc Am
The presence of several parameters, not necessarily all, gives
an indication of the seve
Many of these parameters have not been studied systematically,
they only serve as gu
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
are wheezing, work of breathing and prolongation of
expiration.This score might have limited clinical use, since these
three itemsdo not easily detect subtle changes in the clinical
situation.
For clinical purposes, at this point in time, treatment will
bemainly driven by clinical signs and symptoms rather than
resultsfrom lung function testing.
PICU admission is necessary in a minority of PSA
patients.Several predicting factors defining the need for intensive
care havebeen identified. A history of three or more emergency
presenta-tions in the previous year, an elevated serum IgE level,
oxygensaturations of 91% or less on presentation or a longer
duration ofasthma can predict the need for intensive care
admission.24
Next to these factors, PICU admission in PSA patients
wasrecently related to allergies, active or passive smoking,
earlierhospitalization for asthma and non-sanitized homes.25
THERAPY
Choices in treatment of PSA are made taking the
underlyingpathophysiology into account. Treatment is directed at
reversal ofinflammation and bronchoconstriction, and in a later
phase also ofrelieving mucus plugging if necessary. The initial
goal is correctionof significant hypoxaemia and reversal of the
airflow obstruction assoon as possible. Initial therapies for PSA
are supplementation ofoxygen, repetitive administration of
rapid-acting b2-agonists (e.g.salbutamol), inhaled
anti-cholinergics (e.g. ipratropium bromide)in combination with
systemic glucocorticosteroids (e.g. predniso-lone) and magnesium
sulphate.
Severe Imminent Respiratory
Arrest
(infant-softer
ng;
ing
At rest (infant:
stops drinking)
Gasping
ces Words None
tated Most often agitated Decreased or confused
Often > 30/minute
ncy:
Usually Paradoxal thoracoabdominal
movements
piration Mostly loud in-
and expiratory
Absent
> 120 Bradycardia
Often Absence suggests exhaustion
2040 mm Hg (child)
< 91%
>= 5.6 kPa >= 5.6 kPa
< 8 kPa: possible cyanosis < 8 kPa: possible cyanosis
cy department. Summary of the national asthma education and
prevention program
Thoracic Society 2009;6: 357366.83
rity of status asthmaticus.
idance.
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003
-
Table 2Asthma score
VARIABLE ASTHMA SCORING
1 point 2 points 3 points
Respiratory rate (Breaths/min)
23 yr 34 3539 4045 yr 30 3135 36612 yr 26 2730 31>12 yr 23
2427 28Oxygen saturation (%) >95 with room air 9095 with room
air 70 5070 4years) for intermittent administration. A metered dose
inhalerwith spacer is equally effective as nebulisation, with the
dose beingsix inhalations [total of 600 mcg] or twelve inhalations
[1200 mcg]via spacer respectively.31 However, in contrast to
adults, a recentCochrane review shows some advantages of an
inhalation devicewith holding chamber compared to a nebuliser, with
a significantlyshorter length of stay in the emergency department
for the first
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
group.32,33 Conversely, nebulisation has the added advantage
ofdelivering high flow oxygen. Comparison of the different studies
isdifficult because of the variation in outcome measures and
severityof asthma exacerbations.
If nebulisation fails, salbutamol can also be given
intravenously,on the assumption that with little air entry only a
small amount ofthe drug reaches the target airway receptors. In
children, wellconducted studies concerning pharmacokinetics and
pharmaco-dynamics of intravenous salbutamol are lacking. An early
studyfound that 69% of the patients responded satisfactorily after
aloading dose of 10 mg/kg, followed by a continuous infusion of0.2
mg/kg/min, which was increased by 0.1 mg/kg every 15 min-utes.34
This study included only 14 children and the outcomeparameter was a
decrease of the pCO2, which gives only scarceinformation about the
clinical condition. Another double blindrandomized study in 29
children with severe acute asthmacompared a loading dose of 15
mg/kg intravenous salbutamol tonebulised ipratropium bromide or a
combination of both. Bolussalbutamol was more effective, leading to
earlier cessation ofnebulisation, less oxygen need and earlier
discharge fromhospital.35 Dosing of intravenous salbutamol in
children variesbetween 0.1 and 15 mg/kg/min and there is no
consensus if aloading dose is needed.36,37
Terbutaline is also used as short acting b2-agonist. When
addedto continuous nebulisation, intravenous terbutaline showed a
non-significant decrease in clinical asthma scores, duration
ofcontinuous nebulisation and PICU length of stay compared
tosaline.38 A terbutaline dose of 0.41 mg/kg/min was shown tolower
diastolic blood pressure.39 When terbutaline was adminis-tered
according to a severity related dosing algorithm, it led toshorter
PICU length of stay.40 Although the use of intravenous b2-agonists
varies between countries, it is normally only started afterfailure
of continuous nebulisation. The relationship between doseand effect
has not been studied in children. The drugs are alsoknown for many
side effects including hypokalemia, tachycardia,hyperglycaemia and
hypotension, warranting close monitoring,most often in the PICU
setting. Some children are not as responsiveto b2-agonists as
others; this could be explained by geneticpolymorphisms. Recent
studies suggested that specific b2adrenoreceptor genotypes are
related to shorter ICU length ofstay and shorter duration of
continuous b2-agonist therapy inchildren.41
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003
-
M. Koninckx et al. / Paediatric Respiratory Reviews xxx (2013)
xxxxxx 5
G Model
YPRRV-903; No. of Pages 8
Anticholinergic agents
These agents can decrease secretions, mucosal oedema andreduce
bronchomotor tone. Anticholinergic agents such asipratropium
bromide give less bronchodilation and the effectis slower compared
to short acting b2-agonists. Adding multipledoses of
anticholinergics in moderate and severe acute asthma inchildren to
short acting b2-agonists has an additive effect. Thereis a benefit
in terms of lung function and hospital admission.42
Recommended doses are 250-500 mg every 20 minutes for up tothree
times, followed by administration every three hours ifnecessary.43
In cases where salbutamol is given intravenously,addition of
ipratropium bromide does not have an additiveeffect.44,45
Ipratropium bromide has a very low rate of absorp-tion, implying
that systemic side effects are rare. There arereported cases of
bronchoconstriction, but this adverse effect hasnot been described
when current isotonic ipratropium bromidenebuliser solutions are
used.46 In summary, ipratropium bromidehas no additional value when
it is used in combination withintravenous short acting b2-agonists
in the intensive caresetting, but it can have a positive effect in
the emergencydepartment.44,45
Steroids
In most cases of PSA, especially with failure to respond
torepeated short acting b2-agonists, steroids are added. Their
mostimportant effect is controlling, suppressing and reversal
ofinflammation. They also potentiate the effect of b2-agonists
onsmooth muscle relaxation, decrease b-agonist tachyphylaxis,mucus
production and microvascular permeability.47,48 The onsetof action
of steroids is two to four hours with a maximum effectafter twelve
hours. It is important to administer steroids early inthe disease
course of PSA because this can lead to earlier dischargeand fewer
relapses.49 Recommended doses of oral prednisone are1-2 mg/kg/day
with a maximum dose of 60 mg for 5 to 10 days.Methylprednisolone is
dosed 2 to 4 mg/kg/day with a maximum of125 mg per day. Higher
doses are not associated with bettereffects.50 The same effect is
achieved whether steroids are givenintravenously or orally,
although in severely ill and dyspnoeicchildren, the oral form is
often difficult to administer. In mild tomoderate exacerbations a
single dose of intramuscular dexa-methasone has the same effect as
a 5 day oral course withprednisone.51
A study in 100 children with PSA that were randomised eitherto
oral prednisone 2 mg/kg or a single dose of 2 mg fluticasonethrough
inhalation showed a higher FEV1 and a lower rate ofhospitalisation
in the prednisone group.52 In children, adding highdoses of
budesonide (1200-2000 mg) to systemic prednisone(1 mg/kg) and
nebulised albuterol can prevent or shortenhospitalization.53 A more
recent study concluded that adding asingle dose of 2 mg of
budesonide to standard treatment of PSA didnot have a positive
effect on asthma severity score or short termoutcome.54 Adverse
effects of a short course treatment withsystemic steroids are
mostly transient and can include hyperten-sion, hyperglycaemia and
mood disorders among others. Thesereactions are especially
described in high dose steroid pulsetherapy and chronic use.
Overall in PSA, addition of systemicsteroids is recommended orally
or intravenously. Conflictingresults were reported on the addition
of inhaled budesonide tostandard treatment of PSA.
Magnesium
Magnesium sulphate has a proven effect in status asthmaticus.It
works through smooth muscle relaxation secondary to inhibition
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
of calcium uptake leading to bronchodilation. Magnesium can
alsoinhibit mast cell degranulation and in this way
mitigateinflammation55 and decrease acetylcholine release from
nerveterminals. A recent Cochrane review does not support routine
useof intravenous magnesium sulphate in patients with acute
asthmapresenting to the emergency department. However, it can be
usedsafely and is beneficial in patients with severe acute asthma
whenadded to bronchodilators.56 Three studies in children
demon-strated that early administration of intravenous
magnesiumsulphate is beneficial on hospital admission, lung
function andclinical symptom score in children treated with
bronchodilatorsand steroids.5759 Doses vary between 25 mg/kg and 75
mg/kg.Possible adverse effects are muscle weakness,
hypotension,tachycardia, skin flushing and fatigue but these are
mostlynegligible.
ADDITIONAL TREATMENT MODALITIES
Standard treatment of PSA in the emergency departmentshould
include oxygen, short acting b2-agonists and steroids.In case of
further deterioration intravenous salbutamol incombination with
anticholinergics and intravenous magnesiumsulphate should be
considered. When there is no improvementdespite these therapies
there are still some less frequentlyused options. Most of these
therapies are not evidencebased and (large) randomised controlled
trials are not available.These therapies warrant close monitoring
preferably in aPICU.
Methylxanthines
Methylxanthines (theophylline, aminophylline) act
throughnon-selective inhibition of a phosphodiesterase [enzyme]and
antagonise adenosine receptors in smooth muscle andinflammatory
cells. They result in bronchodilation, improvedmucociliary
clearance and down-regulation of inflammationand immune cell
infiltration. In children, the addition ofaminophylline to short
acting b2-agonists and corticosteroidsin an acute asthma
exacerbation improves lung function (FEV1and PEF), but there is no
reduction in symptoms, number ofnebulised treatments and length of
hospital stay.60 In criticallyill children with status asthmaticus
admitted to the intensivecare unit with impending respiratory
failure, intravenoustheophylline is as safe and effective as
intravenously adminis-tered terbutaline.61 Methylxanthines have a
small therapeuticwindow with many side-effects including headache,
nausea,palpitations and anxiety.62 High theophylline concentrations
canresult in severe toxicity and in cardiac arrhythmias,
hypotension,seizures and even death. Given the small clinical
effect,methylxanthines should be used with caution and only
inrefractory PSA.
Deoxyribonuclease (DNase)
Mucus plugging and atelectasis are an important clinicalproblem
in PSA. Since inflammation might lead to a high DNAcontent in
mucus, the use of recombinant human (rh) DNase astreatment modality
has been hypothesized. In children there areonly a few case reports
(but no good evidence) which describedpositive effects after
intratracheal delivery of DNase in mechani-cally ventilated
asthmatic children.63,64 There is no place forroutine addition of
nebulised rhDNase to conventional treatmentin children with PSA
presenting at the emergency department.65
Treatment with rhDNase might rarely have a place in the PICU
forpatients with refractory PSA, sometimes in combination
withbronchoscopy.
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003
-
M. Koninckx et al. / Paediatric Respiratory Reviews xxx (2013)
xxxxxx6
G Model
YPRRV-903; No. of Pages 8
Ketamine
Ketamine has bronchodilating properties through
increasingcirculating catecholamines after inhibition of the
re-uptake ofnoradrenaline in the presynaptic neurons. Ketamine
wassuccessfully used to prevent intubation in two children
withstatus asthmaticus who received a loading dose of ketamine(2
mg/kg) followed by continuous infusion of ketamine (2 mg/kg/h).66
However, a study in 68 paediatric patients could notdemonstrate an
additional benefit of ketamine over conventionalemergency
department therapy in PSA. A rather low loadingdose of 0.2 mg/kg
followed by continuous infusion of 0.5 mg/kg/h was used in this
study.67 In refractory PSA ketamine mighthave a place, especially
when sedation and/or intubation areconsidered.
Sodium bicarbonate
Respiratory or metabolic acidosis can be seen in PSA.
Thepresence of acidosis can diminish the effect of
catecholamines.Therefore, treatment of acidosis with sodium
bicarbonate could bebeneficial. Administration of sodium
bicarbonate in 17 patientswith life threatening asthma admitted to
the PICU showed asignificant decrease in mean pCO2 and a
significant increase ofmean pH. Clinical improvement of respiratory
distress and level ofconsciousness was seen in individual
patients.68 This smallretrospective study suggests sodium
bicarbonate could beconsidered in life threatening asthma with
severe acidosis (pH
-
M. Koninckx et al. / Paediatric Respiratory Reviews xxx (2013)
xxxxxx 7
G Model
YPRRV-903; No. of Pages 8
2. Werner HA. Status asthmaticus in children: a review. Chest
2001;119:191329.
3. Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical
review: severe asthma.Crit Care 2002;6:3044.
4. Carroll CL, Zucker AR. The increased cost of complications in
children withstatus asthmaticus. Pediatric pulmonology
2007;42:9149.
5. CDC Vital Signs: Asthma prevalence, disease characteristics
and self-manage-ment education. United States 20012009 MMWR. 2011;
60:54752.
6. Hartert TV, Peebles Jr RS. Epidemiology of asthma: the year
in review. Curr OpinPulm Med 2000;6:49.
7. Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in
admissions forpediatric status asthmaticus in New Jersey over a
15-year period. Pediatrics2010;126:e90411.
8. Triasih R, Duke T, Robertson CF. Outcomes following admission
to intensive carefor asthma. Arch Dis Child 2011;96:72934.
9. Malmstrom K, Kaila M, Korhonen K, Dunder T, Nermes M, Klaukka
T, et al.Mechanical ventilation in children with severe asthma.
Pediatric pulmonology2001;31:40511.
10. Peebles Jr RS, Hartert TV. Respiratory viruses and asthma.
Curr Opin Pulm Med2000;6:104.
11. Kikuchi Y, Okabe S, Tamura G, Hida W, Homma M, Shirato K, et
al. Chemo-sensitivity and perception of dyspnea in patients with a
history of near-fatalasthma. N Engl J Med 1994;330:132934.
12. Verbruggen SC, Corel LJ, Tiddens HA, Joosten KF, de Hoog M.
[Fatal asthma inchildhood preventable by recognizing risk factors
and presenting features]Fataal astma op de kinderleeftijd te
voorkomen door herkenning van risico-factoren en presentatiewijze.
Ned Tijdschr Geneeskd 2006;150:2259.
13. Picado C. Classification of severe asthma exacerbations: a
proposal. Eur Respir J1996;9:17758.
14. Sur S, Crotty TB, Kephart GM, Hyma BA, Colby TV, Reed CE, et
al. Sudden-onsetfatal asthma. A distinct entity with few
eosinophils and relatively moreneutrophils in the airway submucosa?
Am Rev Respir Dis 1993;148:7139.
15. Plaza V, Serrano J, Picado C, Sanchis J. High Risk Asthma
Research G. Frequencyand clinical characteristics of rapid-onset
fatal and near-fatal asthma. Eur RespirJ 2002;19:84652.
16. Shugg AW, Kerr S, Butt WW. Mechanical ventilation of
paediatric patients withasthma: short and long term outcome. J
Paediatr Child Health 1990;26:3436.
17. Corbridge TC, Hall JB. The assessment and management of
adults with statusasthmaticus. Am J Respir Crit Care Med
1995;151:1296316.
18. Gorelick MH, Stevens MW, Schultz T, Scribano PV. Difficulty
in obtaining peakexpiratory flow measurements in children with
acute asthma. Pediatric Emer-gency Care 2004;20:226.
19. Saetta M, Thiene G, Crescioli S, Fabbri LM. Fatal asthma in
a young patient withsevere bronchial hyperresponsiveness but stable
peak flow records. Eur Respir J1989;2:100812.
20. Geelhoed GC, Landau LI, Le Souef PN. Evaluation of SaO2 as a
predictor ofoutcome in 280 children presenting with acute asthma.
Ann Emerg Med1994;23:123641.
21. Keahey L, Bulloch B, Becker AB, Pollack Jr CV, Clark S,
Camargo Jr CA, et al. Initialoxygen saturation as a predictor of
admission in children presenting to theemergency department with
acute asthma. Ann Emerg Med 2002;40:3007.
22. Qureshi F, Pestian J, Davis P, Zaritsky A. Effect of
nebulized ipratropium on thehospitalization rates of children with
asthma. N Engl J Med 1998;339:10305.
23. Gorelick MH, Stevens MW, Schultz TR, Scribano PV.
Performance of a novelclinical score, the Pediatric Asthma Severity
Score (PASS), in the evaluation ofacute asthma. Acad Emerg Med
2004;11:108.
24. Belessis Y, Dixon S, Thomsen A, Duffy B, Rawlinson W, Henry
R, et al. Risk factorsfor an intensive care unit admission in
children with asthma. Pediatric pulmo-nology 2004;37:2019.
25. van den Bosch GE, Merkus P, Buysse C, Boehmer A,
Vaessen-Verberne A, vanVeen LN, et al. Risk Factors for Pediatric
Intensive Care Admission in ChildrenWith Acute. Asthma Respir Care
2012;57:13917.
26. Molfino NA, Nannini LJ, Martelli AN, Slutsky AS. Respiratory
arrest in near-fatalasthma. N Engl J Med 1991;324:2858.
27. Inwald D, Roland M, Kuitert L, McKenzie SA, Petros A. Oxygen
treatment foracute severe asthma. BMJ 2001;323:98100.
28. Morgan DJ. Clinical pharmacokinetics of beta-agonists. Clin
Pharmacokinet1990;18:27094.
29. Wang XF, Hong JG. Management of severe asthma exacerbation
in children.World J Pediatr 2011;7:293301.
30. Papo MC, Frank J, Thompson AE. A prospective, randomized
study of continuousversus intermittent nebulized albuterol for
severe status asthmaticus in chil-dren. Critical Care Medicine
1993;21:147986.
31. Leversha AM, Campanella SG, Aickin RP, Asher MI. Costs and
effectiveness ofspacer versus nebulizer in young children with
moderate and severe acuteasthma. J Pediatr 2000;136:497502.
32. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers)
versus nebulisers forbeta-agonist treatment of acute asthma.
Cochrane Database Syst Rev 2006.CD000052.
33. Castro-Rodriguez JA, Rodrigo GJ. beta-agonists through
metered-dose inhalerwith valved holding chamber versus nebulizer
for acute exacerbation ofwheezing or asthma in children under 5
years of age: a systematic reviewwith meta-analysis. J Pediatr
2004;145:1727.
34. Bohn D, Kalloghlian A, Jenkins J, Edmonds J, Barker G.
Intravenous salbutamol inthe treatment of status asthmaticus in
children. Critical Care Medicine1984;12:8926.
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
35. Browne GJ, Penna AS, Phung X, Soo M. Randomised trial of
intravenoussalbutamol in early management of acute severe asthma in
children. Lancet1997;349:3015.
36. Shann F. Dose of intravenous infusions of terbutaline and
salbutamol. CriticalCare Medicine 2000;28:217980.
37. Sellers WF, Messahel B. Rapidly repeated intravenous boluses
of salbutamol foracute severe asthma. Anaesthesia 2003;58:6803.
38. Bogie AL, Towne D, Luckett PM, Abramo TJ, Wiebe RA.
Comparison of intrave-nous terbutaline versus normal saline in
pediatric patients on continuous high-dose nebulized albuterol for
status asthmaticus. Pediatric Emergency Care2007;23:35561.
39. Stephanopoulos DE, Monge R, Schell KH, Wyckoff P, Peterson
BM. Continuousintravenous terbutaline for pediatric status
asthmaticus. Critical Care Medicine1998;26:17448.
40. Carroll CL, Schramm CM. Protocol-based titration of
intravenous terbutalinedecreases length of stay in pediatric status
asthmaticus. Pediatric Pulmonology2006;41:3506.
41. Carroll CL, Sala KA, Zucker AR, Schramm CM. Beta-adrenergic
receptor poly-morphisms associated with length of ICU stay in
pediatric status asthmaticus.Pediatric Pulmonology
2012;47:2339.
42. Plotnick LH, Ducharme FM. Should inhaled anticholinergics be
added to beta2agonists for treating acute childhood and adolescent
asthma? A systematicreview. BMJ 1998;317:9717.
43. Health NIo. 3rd expert panel summary report from the
national asthmaeducation and prevention programm 2007.
44. Browne GJ, Trieu L, Van Asperen P. Randomized, double-blind,
placebo-con-trolled trial of intravenous salbutamol and nebulized
ipratropium bromide inearly management of severe acute asthma in
children presenting to an emer-gency department. Critical Care
Medicine 2002;30:44853.
45. Rodrigo GJ, Castro-Rodriguez JA. Anticholinergics in the
treatment of childrenand adults with acute asthma: a systematic
review with meta-analysis. Thorax2005;60:7406.
46. Rafferty P, Beasley R, Howarth PH, Mann JS, Holgate ST.
Bronchoconstrictioninduced by nebulised ipratropium bromide:
relation to the bromide ion. Br MedJ (Clin Res Ed)
1986;293:15389.
47. Barnes NC. Effects of corticosteroids in acute severe
asthma. Thorax 1992;47:5823.
48. Boschetto P, Rogers DF, Fabbri LM, Barnes PJ. Corticosteroid
inhibition of airwaymicrovascular leakage. Am Rev Respir Dis
1991;143:6059.
49. Smith M, Iqbal S, Elliott TM, Everard M, Rowe BH.
Corticosteroids for hospi-talised children with acute asthma.
Cochrane Database Syst Rev 2003;CD002886.
50. Chipps BE, Murphy KR. Assessment and treatment of acute
asthma in children. JPediatr 2005;147:28894.
51. Gries DM, Moffitt DR, Pulos E, Carter ER. A single dose of
intramuscularlyadministered dexamethasone acetate is as effective
as oral prednisone to treatasthma exacerbations in young children.
J Pediatr 2000;136:298303.
52. Schuh S, Reisman J, Alshehri M, Dupuis A, Corey M,
Arseneault R, et al. Acomparison of inhaled fluticasone and oral
prednisone for children with severeacute asthma. N Engl J Med
2000;343:68994.
53. Schramm CM, Carroll CL. Advances in treating acute asthma
exacerbations inchildren. Curr Opin Pediatr 2009;21:32632.
54. Upham BD, Mollen CJ, Scarfone RJ, Seiden J, Chew A, Zorc JJ.
Nebulizedbudesonide added to standard pediatric emergency
department treatment ofacute asthma: a randomized, double-blind
trial. Acad Emerg Med 2011;18:66573.
55. Skobeloff EM. An ion for the lungs. Acad Emerg Med 1996
Dec;3:10824.56. Rowe B, Bretzlaff J, Bourdon C, Bota G, Camargo C.
Magnesium sulfate is
effective for severe acute asthma treated in the emergency
department. WestJ Med 2000;172:96.
57. Cheuk DK, Chau TC, Lee SL. A meta-analysis on intravenous
magnesiumsulphate for treating acute asthma. Arch Dis Child
2005;90:747.
58. Ciarallo L, Sauer AH, Shannon MW. Intravenous magnesium
therapy for mod-erate to severe pediatric asthma: results of a
randomized, placebo-controlledtrial. J Pediatr 1996;129:80914.
59. Devi RR KL, Singhi SC, Prasad R, Singh M. Intravenous
magnesium sulfate inacute severe asthma not responding to
conventional therapy. Indian Pediatr.1997; 34:38997.
60. Mitra A, Bassler D, Goodman K, Lasserson TJ, Ducharme FM.
Intravenousaminophylline for acute severe asthma in children over
two years receivinginhaled bronchodilators. Cochrane Database Syst
Rev 2005. CD001276.
61. Wheeler DS, Jacobs BR, Kenreigh CA, Bean JA, Hutson TK,
Brilli RJ. Theophyllineversus terbutaline in treating critically
ill children with status asthmaticus: aprospective, randomized,
controlled trial. Pediatr Crit Care Med 2005;6:1427.
62. Rodrigo C, Rodrigo G. Treatment of acute asthma. Lack of
therapeutic benefitand increase of the toxicity from aminophylline
given in addition to high dosesof salbutamol delivered by
metered-dose inhaler with a spacer. Chest1994;106:10716.
63. Durward A, Forte V, Shemie SD. Resolution of mucus plugging
and atelectasisafter intratracheal rhDNase therapy in a
mechanically ventilated child withrefractory status asthmaticus.
Critical Care Medicine 2000;28:5602.
64. Greally P. Human recombinant DNase for mucus plugging in
status asthma-ticus. Lancet 1995;346:14234.
65. Boogaard R, Smit F, Schornagel R, Vaessen-Verberne AA,
Kouwenberg JM,Hekkelaan M, et al. Recombinant human
deoxyribonuclease for the treatmentof acute asthma in children.
Thorax 2008;63:1416.
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003
-
M. Koninckx et al. / Paediatric Respiratory Reviews xxx (2013)
xxxxxx8
G Model
YPRRV-903; No. of Pages 8
66. Denmark TK, Crane HA, Brown L. Ketamine to avoid mechanical
ventilation insevere pediatric asthma. J Emerg Med
2006;30:1636.
67. Allen JY, Macias CG. The efficacy of ketamine in pediatric
emergency depart-ment patients who present with acute severe
asthma. Ann Emerg Med2005;46:4350.
68. Buysse CM, de Jongste JC, de Hoog M. Life-threatening asthma
in children:treatment with sodium bicarbonate reduces PCO2. Chest
2005;127:86670.
69. Caroll. Heliox for children with acute asthma: Has the sun
set on this therapy?Pediatr Crit Care Med 2010;11:4289.
70. Kim IK, Phrampus E, Venkataraman S, Pitetti R, Saville A,
Corcoran T, et al.Helium/oxygen-driven albuterol nebulization in
the treatment of children withmoderate to severe asthma
exacerbations: a randomized, controlled trial.Pediatrics
2005;116:112733.
71. Rodrigo G, Pollack C, Rodrigo C, Rowe BH. Heliox for
nonintubated acute asthmapatients. Cochrane Database Syst Rev 2006.
CD002884.
72. Walker DM. Update on epinephrine (adrenaline) for pediatric
emergencies. CurrOpin Pediatr 2009;21:3139.
73. Wiebe K, Rowe BH. Nebulized racemic epinephrine used in the
treatment ofsevere asthmatic exacerbation: a case report and
literature review. CJEM2007;9:3048.
74. Asthma: follow-up statement from an international paediatric
asthma con-sensus group. Arch Dis Child 1992; 67:2468.
75. Mayordomo-Colunga J, Medina A, Rey C, Concha A, Menendez S,
Arcos ML, et al.Non-invasive ventilation in pediatric status
asthmaticus: a prospective obser-vational study. Pediatric
Pulmonology 2011;46:94955.
Please cite this article in press as: Koninckx M, et al.
Management of stdx.doi.org/10.1016/j.prrv.2013.03.003
76. Thill PJ, McGuire JK, Baden HP, Green TP, Checchia PA.
Noninvasive positive-pressure ventilation in children with lower
airway obstruction. Pediatr Crit CareMed 2004;5:33742.
77. Basnet S, Mander G, Andoh J, Klaska H, Verhulst S, Koirala
J. Safety, efficacy, andtolerability of early initiation of
noninvasive positive pressure ventilation inpediatric patients
admitted with status asthmaticus: A pilot study. Pediatr CritCare
Med 2012;13:3938.
78. Tobias JD. Inhalational anesthesia: basic pharmacology, end
organ effects, andapplications in the treatment of status
asthmaticus. J Intensive Care Med2009;24:36171.
79. Wheeler DS, Clapp CR, Ponaman ML, Bsn HM, Poss WB.
Isoflurane therapy forstatus asthmaticus in children: A case series
and protocol. Pediatr Crit Care Med2000;1:559.
80. Shankar V, Churchwell KB, Deshpande JK. Isoflurane therapy
for severe refrac-tory status asthmaticus in children. Intensive
Care Med 2006;32:92733.
81. Mikkelsen ME WY, Sager JS, Fuchs BD, Christie JD. Outcomes
using extracor-poreal life support for adult respiratory failure
due to status asthmaticus. ASAIOJournal 2009;55:4752.
82. Hebbar KB, Petrillo-Albarano T, Coto-Puckett W, Heard M,
Rycus PT, Forten-berry JD. Experience with use of extracorporeal
life support for severe refrac-tory status asthmaticus in children.
Crit Care 2009;13:R29.
83. Camargo CA, Rachelefsky G, Schatz M. Managing asthma
exacerbations in theemergency department. Summary of the national
asthma education and pre-vention program expert panel report 3
guidelines for the management ofasthma exacerbations. Proc Am
Thoracic Society 2009;6:35766.
atus asthmaticus in children. Paediatr. Respir. Rev. (2013),
http://
http://dx.doi.org/10.1016/j.prrv.2013.03.003http://dx.doi.org/10.1016/j.prrv.2013.03.003Management
of status asthmaticus in childrenEducational AimsPathophysiology of
status asthmaticusDetermination of asthma severityPeak flow
measurements and serial lung function measurementsPulse
oximetryClinical scoring systemsTherapyOxygenShort acting
2-agonistsAnticholinergic agentsSteroidsMagnesiumAdditional
treatment modalitiesMethylxanthinesDeoxyribonuclease
(DNase)KetamineSodium bicarbonateHelioxEpinephrine
(Adrenaline)Non-invasive respiratory supportMechanical
ventilationInhalational anaestheticsExtracorporeal membrane
oxygenation (ECMO)ConclusionReferences


![Status asthmaticus - pdfs.semanticscholar.org · Status asthmaticus influenced by reduced exposure to stimuli and by regular effective treatment [8]. C currently pathologists have](https://img.pdfslide.us/doc/110x75/5e0e2e4f584564357a38ccc6/status-asthmaticus-pdfs-status-asthmaticus-influenced-by-reduced-exposure-to.jpg)