Embed Size (px)
Citation preview

Management of Management of patients with patients with
swallowing difficulty swallowing difficulty and painand pain
Management of Management of patients with patients with
swallowing difficulty swallowing difficulty and painand pain

Topics• Anatomy of the esophagus.• Definitions.• Causes of Dysphagia.• Gastro-Esophageal Reflux Disease (GERD).• Achalasia.• Hiatus Hernia.• Esophageal tumors.

Anatomy of the esophagus
• It is an epithelial lined muscular tube, 25cm long, and extends from the level of C6 to T11.
• Has 3 portions:– Cervical– Thoracic.– Abdominal.
• It’s muscular coat has 2 layers:– Outer longitudinal.– Inner circular.
• The upper 1/3 is composed of striated muscle, while the lower 2/3 is composed of smooth m.

Cont.
• It is lined by keratinized squamous epithelium which changes to columnar epithelium 2cm above the gastro-esophageal junction.
• It has 2 sphincters:– The upper esophageal sphincter.– The lower esophageal sphincter (LES).
• Anatomical areas of narrowing are:– At the level of cricoid cartilage.– In the mid-thorax, from compression by the aortic
arch and left main stem bronchus.– At the level of the esophageal hiatus of the
diaphragm.

Definitions
• Dysphagia: – Difficulty in swallowing.
• Odynophagia:– Painful swallowing.

Causes of dysphagia
Diseases of the mouth and tongue e.g. tonsillitis
Neuromuscular disorderse.g. bulbar palsy, myasthenia gravis
Motility disorderse.g. achalasia, scleroderma, diffuse esoph. Spasm
Intrinsic lesionse.g. FB ,strictures (benign/malignant),
esoph. web/ring
Extrinsic pressuree.g. goiter, pharyngeal pouch, LN,
aortic aneurysm, enlarged left atrium

Gastro-Esophageal Gastro-Esophageal Reflux Disease Reflux Disease
(GERD)(GERD)
Gastro-Esophageal Gastro-Esophageal Reflux Disease Reflux Disease
(GERD)(GERD)

Background• Gastro-esophageal
reflux is a normal phenomenon experienced intermittently by most people.
• GERD occurs when the amount of gastric juice exceeds the normal limit with or without esophageal mucosal injury (esophagitis).

pathophysiology• Factors that prevent gastric juice reflux into
the esophagus:1. LES (normal length and pressure).2. Gastro-esophageal junction must lie intra-
abdominally.3. The angle at which the esophagus joins the stomach
(angle of His).4. Esophageal clearance must be able to neutralize the
acid refluxed from the stomach.5. The stomach must empty properly.6. Contraction of the crural muscle of the diaphragm
(pinchcock-like action).

Cont.• GERD develops due to one or more of the
fallowing:1. Functional (frequent transient LES relaxation) or
mechanical (hypotensive LES) problem of the LES, (most common).
2. Certain foods (eg, coffee, alcohol), medications (eg, calcium channel blockers, nitrates, beta-blockers), or hormones (eg, progesterone) can decrease the pressure of the LES.
3. Reduced esophageal clearance of acid because of poor esophageal peristalsis.
4. Obesity and pregnancy (increased intra-abdominal pressure).
5. Hiatus hernia (impairment of the pinchcock-like action of the diaphragm).
6. Delayed gastric emptying.

Epidemiology• 7% of the general population have
heartburn, and 20-30% of them have GERD.
• No sexual preference.• Affects all age groups.
Clinical features• Heartburn is the major feature, retrosternal,
burning pain, radiating to the epigastrium, aggravated by bending and lying down, and relieved by antacids.
• Regurgitation of food and acid into the mouth.• Waterbrash (salivation).• Dysphagia (stricture, or non-specific motility
disorder).• Respiratory symptoms: cough , nocturnal
asthma, pneumonia.• Clinical examination is usually normal.

DDx• MI.• Peptic ulcer disease.• Cholecystitis.• Esophageal cancer.

Investigation • GERD is a clinical Dx. Patients under 45y
without alarm symptoms should be treated initially without investigations.
• Investigations include:– Barium swallow (ulceration, stricture, hiatus hernia)– Esophagogastroduodenoscopy (EGD)
• Identifies the presence and severity of esophagitis.• Excludes other diseases as peptic ulcer disease.
– Esophageal monometry (function of LES and esoph. Body)
– Ambulatory 24hr pH monitoring (gold standard).

Treatment
Lifestyle modification
Medical treatment:Antacids, H2 blockers, PPI’s,
Prokinetic agents
Surgical treatment:fundoplication

Cont.• Lifestyle modifications includes:
1. Losing weight (if overweight).2. Avoiding alcohol, chocolate, citrus
juice.3. Avoiding large meals.4. Waiting after a meal before lying
down.5. Elevation of the head of the bed.

Cont.• Medical treatment with:
– Antacids.– H2 receptor blockers.– Proton pump inhibitors.– Prokinetic agents.

Cont.• Surgical treatment:
– Fundoplication (most commonly Nissen fundoplication).
• Indications:1. If symptoms cannot be controlled by
medical therapy.2. The presence of Barrett’s esophagus.3. The presence of extra-esophageal
manifestation of GERD (respiratory, ENT, dental).

Cont.• It is performed under
GA and the fundus of the stomach is wrapped around the esophagus to create a new valve at the level of the gastro-esophageal junction.

Complications1. Esophagitis:
• 50%,, M:F is 2-3:1.2. Barrett’s esophagus:
• It is columnar metaplasia of the lower esophagus which extends at least 3cm above the GE junction.
• M:F is 10:1.• Most serious and may progress into cancer.
3. Respiratory complications:– Include pneumonia, asthma, and lung
fibrosis.

AchalasiaAchalasiaAchalasiaAchalasia

Definition• Is a primary oesophageal motility
disorder characterised by failure of LES to relax and the absence of peristalsis .

pathophysiology
LES pressure
Excitatory(acetylcholine, Substance B)
Inhibitory(nitric oxide)

• incidence:1/100,000 per year in US• No sex difference• Typically 25-60 years• Cause:unkown but one theory
suggest degenerative changes in the vagal nerve

C/F• Dysphagia (gradual)• Regurgitation• Chest pain• Weight loss• Stomach cancer
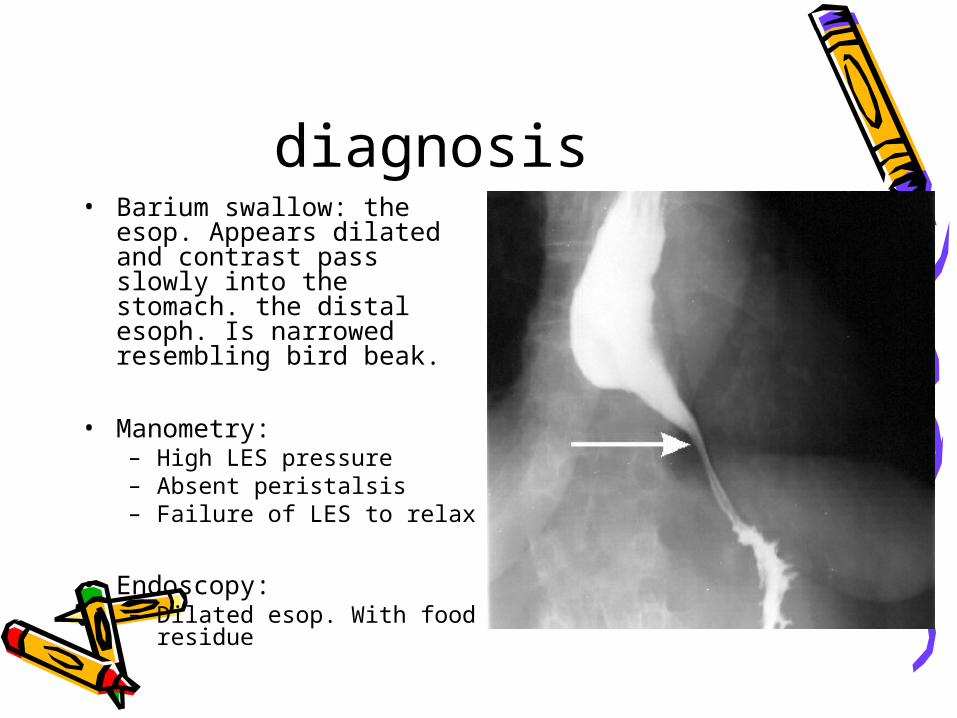
diagnosis• Barium swallow: the esop.
Appears dilated and contrast pass slowly into the stomach. the distal esoph. Is narrowed resembling bird beak.
• Manometry:– High LES pressure– Absent peristalsis– Failure of LES to relax
• Endoscopy:– Dilated esop. With food
residue

treatment• Drug therapy:
– Smooth muscle relaxant (nitrate ,calcium channel blocker,,anticholinergic))– 10% of pts. Benefit from this treatment (elderly)
• Pneumatic dilation:– A balloon is insuflatted at the level of the G.O junction to rupture the muscle fibre– Success rate 70_80%– 50% will require more than 1 dilation.

Cont.• Surgery:
– Used when the dilation fails– Heller’s Myotomy(open or laparoscopic)– Done by making division of the muscle fibre of the
lower esoph. And proximal stomach followed by partial fundiplication to prevent reflux(10%)
– Relieve symptoms in 85 _95% of pts.
• If surgery fails →dilation2nd operation ---esophagectomy

Hiatus HerniaHiatus HerniaHiatus HerniaHiatus Hernia

• Def: it is an abnormal protrusion of the stomach through esoph. Diphramatic hiatus into the thorax.
• Caused by weakness mucsles around the hiatus.
• More common in females ,obes ,middle aged and elderly.

types• Type I: sliding hiatus hernia(90%)
• Type II: paraesophageal hiatus hernia(10%)
• Type III: combination of both (rare)

Sliding hiatus hernia• Occurs when the stomach slides
through the diaphragmatic hiatus and the G .O . Junction lies within the chest.

C/f• Asymptomatic• Heart burn and regurgitation: the most
common, due to incompetent LES, aggrivated by bending or lying down and relieved by antacid
• Dysphagia• Large herniation may cause cough,
palpitation or hiccups by mechanical effect

investigation• Upper GI endoscope
• Barium swallow
• Complication:
Refluxesophagitisbarret’s esophagus-ca
• Treatment: – Same as GERD

Paraesophageal hiatus hernia
• Here the G.O. junction lies in its position but the fundus of the stomach has herniated through diaphragmatic hiatus.

C/F
• Usually not associated with reflux• Dysphagia• Epigastric and lower chest pain• Palpitation• Hiccups• Quick fullness and chest
compression after eating

• Investigation:– Chest x-ray confirmed by barium swallow.
• Complication:– Obstruction– Volvulus– Strangulation– Acute or chronic bleeding– perforation

Treatment• Surgical:
– Operative reduction of the stomach, approximation of the diaphragmatic defect around the hiatus
– Fundoplication frequently added to reduce the hernaition recurrence and to prevent GE reflux