Embed Size (px)
Citation preview
Management of Patients with Stroke
III: Identification andManagement of Dysphagia
A National Clinical Guidelinerecommended for use
in
Scotlandby the
Scottish IntercollegiateGuidelines Network
Pilot EditionNovember 1997
Getting validated guidelines into local practice
SIGN PUBLIC
ATIONNUMBE
R 20
S I G N
First published 1997
© Scottish Intercollegiate Guidelines Network9 Queen Street, Edinburgh EH2 1JQ
ISBN 1 899893 95 4
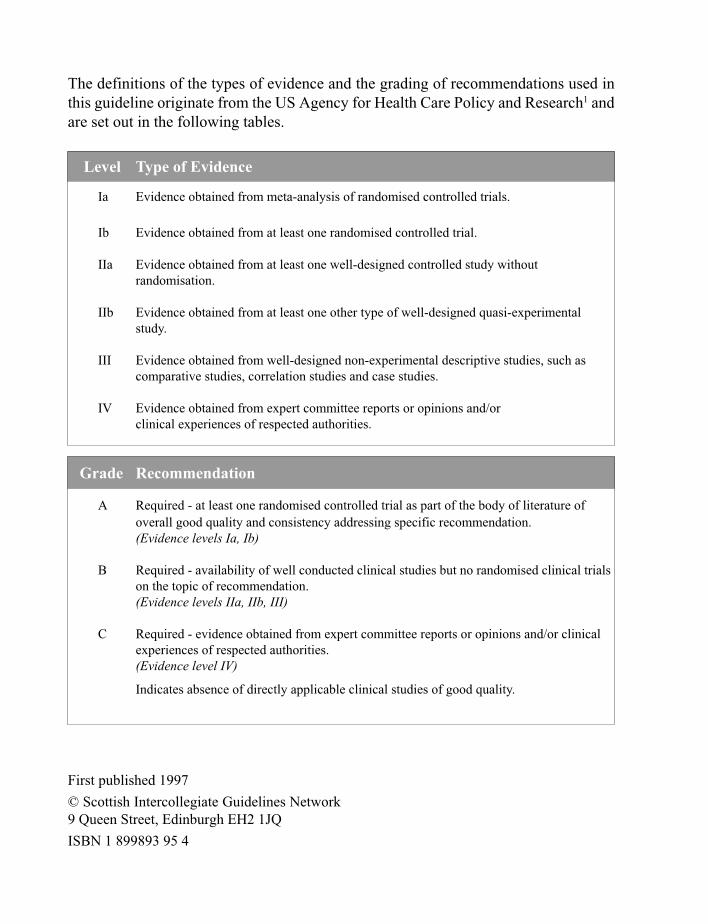
The definitions of the types of evidence and the grading of recommendations used inthis guideline originate from the US Agency for Health Care Policy and Research1 andare set out in the following tables.
Level Type of Evidence
Ia Evidence obtained from meta-analysis of randomised controlled trials.
Ib Evidence obtained from at least one randomised controlled trial.
IIa Evidence obtained from at least one well-designed controlled study withoutrandomisation.
IIb Evidence obtained from at least one other type of well-designed quasi-experimentalstudy.
III Evidence obtained from well-designed non-experimental descriptive studies, such ascomparative studies, correlation studies and case studies.
IV Evidence obtained from expert committee reports or opinions and/orclinical experiences of respected authorities.
Grade Recommendation
A Required - at least one randomised controlled trial as part of the body of literature ofoverall good quality and consistency addressing specific recommendation.(Evidence levels Ia, Ib)
B Required - availability of well conducted clinical studies but no randomised clinical trialson the topic of recommendation.(Evidence levels IIa, IIb, III)
C Required - evidence obtained from expert committee reports or opinions and/or clinicalexperiences of respected authorities.(Evidence level IV)
Indicates absence of directly applicable clinical studies of good quality.
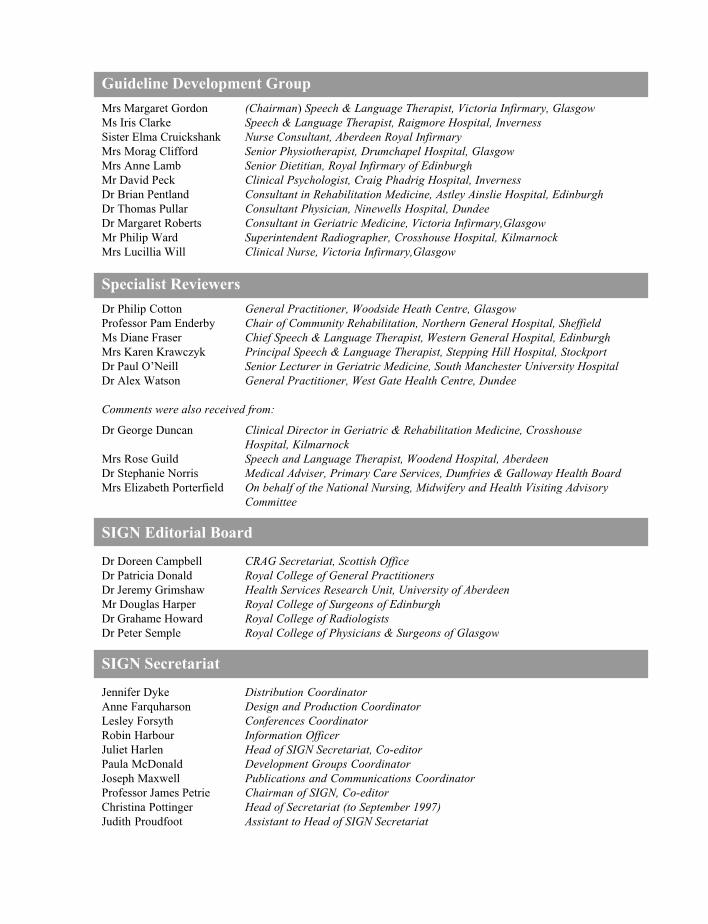
Guideline Development Group
Mrs Margaret Gordon (Chairman) Speech & Language Therapist, Victoria Infirmary, GlasgowMs Iris Clarke Speech & Language Therapist, Raigmore Hospital, InvernessSister Elma Cruickshank Nurse Consultant, Aberdeen Royal InfirmaryMrs Morag Clifford Senior Physiotherapist, Drumchapel Hospital, GlasgowMrs Anne Lamb Senior Dietitian, Royal Infirmary of EdinburghMr David Peck Clinical Psychologist, Craig Phadrig Hospital, InvernessDr Brian Pentland Consultant in Rehabilitation Medicine, Astley Ainslie Hospital, EdinburghDr Thomas Pullar Consultant Physician, Ninewells Hospital, DundeeDr Margaret Roberts Consultant in Geriatric Medicine, Victoria Infirmary,GlasgowMr Philip Ward Superintendent Radiographer, Crosshouse Hospital, KilmarnockMrs Lucillia Will Clinical Nurse, Victoria Infirmary,Glasgow
Specialist Reviewers
Dr Philip Cotton General Practitioner, Woodside Heath Centre, GlasgowProfessor Pam Enderby Chair of Community Rehabilitation, Northern General Hospital, SheffieldMs Diane Fraser Chief Speech & Language Therapist, Western General Hospital, EdinburghMrs Karen Krawczyk Principal Speech & Language Therapist, Stepping Hill Hospital, StockportDr Paul O’Neill Senior Lecturer in Geriatric Medicine, South Manchester University HospitalDr Alex Watson General Practitioner, West Gate Health Centre, Dundee
Comments were also received from:
Dr George Duncan Clinical Director in Geriatric & Rehabilitation Medicine, CrosshouseHospital, Kilmarnock
Mrs Rose Guild Speech and Language Therapist, Woodend Hospital, AberdeenDr Stephanie Norris Medical Adviser, Primary Care Services, Dumfries & Galloway Health BoardMrs Elizabeth Porterfield On behalf of the National Nursing, Midwifery and Health Visiting Advisory
Committee
SIGN Editorial Board
Dr Doreen Campbell CRAG Secretariat, Scottish OfficeDr Patricia Donald Royal College of General PractitionersDr Jeremy Grimshaw Health Services Research Unit, University of AberdeenMr Douglas Harper Royal College of Surgeons of EdinburghDr Grahame Howard Royal College of RadiologistsDr Peter Semple Royal College of Physicians & Surgeons of Glasgow
SIGN Secretariat
Jennifer Dyke Distribution CoordinatorAnne Farquharson Design and Production CoordinatorLesley Forsyth Conferences CoordinatorRobin Harbour Information OfficerJuliet Harlen Head of SIGN Secretariat, Co-editorPaula McDonald Development Groups CoordinatorJoseph Maxwell Publications and Communications CoordinatorProfessor James Petrie Chairman of SIGN, Co-editorChristina Pottinger Head of Secretariat (to September 1997)Judith Proudfoot Assistant to Head of SIGN Secretariat
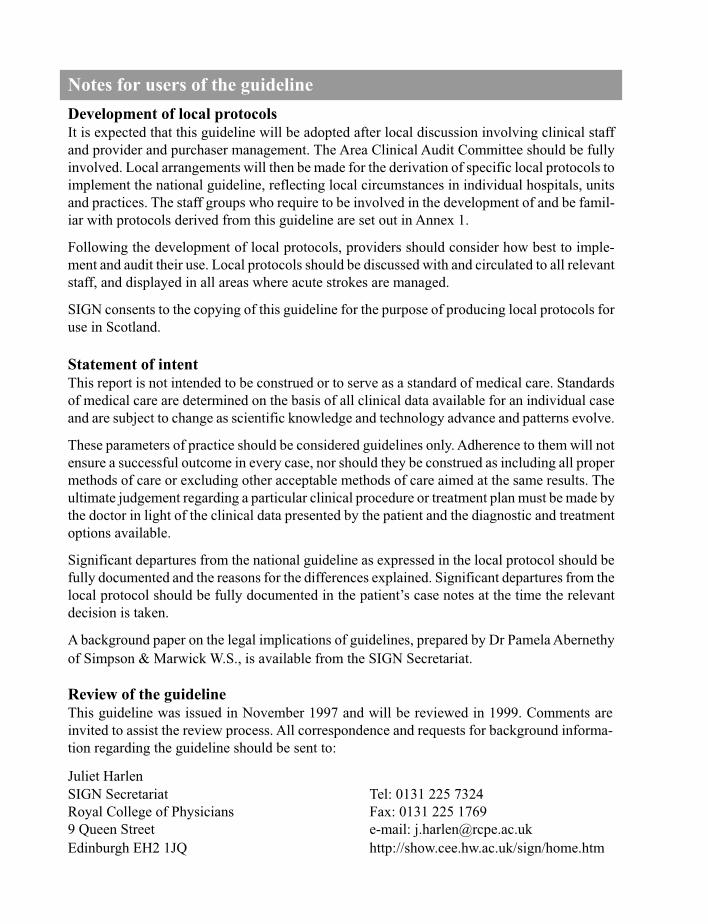
Notes for users of the guideline
Development of local protocolsIt is expected that this guideline will be adopted after local discussion involving clinical staffand provider and purchaser management. The Area Clinical Audit Committee should be fullyinvolved. Local arrangements will then be made for the derivation of specific local protocols toimplement the national guideline, reflecting local circumstances in individual hospitals, unitsand practices. The staff groups who require to be involved in the development of and be famil-iar with protocols derived from this guideline are set out in Annex 1.
Following the development of local protocols, providers should consider how best to imple-ment and audit their use. Local protocols should be discussed with and circulated to all relevantstaff, and displayed in all areas where acute strokes are managed.
SIGN consents to the copying of this guideline for the purpose of producing local protocols foruse in Scotland.
Statement of intentThis report is not intended to be construed or to serve as a standard of medical care. Standardsof medical care are determined on the basis of all clinical data available for an individual caseand are subject to change as scientific knowledge and technology advance and patterns evolve.
These parameters of practice should be considered guidelines only. Adherence to them will notensure a successful outcome in every case, nor should they be construed as including all propermethods of care or excluding other acceptable methods of care aimed at the same results. Theultimate judgement regarding a particular clinical procedure or treatment plan must be made bythe doctor in light of the clinical data presented by the patient and the diagnostic and treatmentoptions available.
Significant departures from the national guideline as expressed in the local protocol should befully documented and the reasons for the differences explained. Significant departures from thelocal protocol should be fully documented in the patient’s case notes at the time the relevantdecision is taken.
A background paper on the legal implications of guidelines, prepared by Dr Pamela Abernethyof Simpson & Marwick W.S., is available from the SIGN Secretariat.
Review of the guidelineThis guideline was issued in November 1997 and will be reviewed in 1999. Comments areinvited to assist the review process. All correspondence and requests for background informa-tion regarding the guideline should be sent to:
Juliet HarlenSIGN Secretariat Tel: 0131 225 7324Royal College of Physicians Fax: 0131 225 17699 Queen Street e-mail: [email protected] EH2 1JQ http://show.cee.hw.ac.uk/sign/home.htm
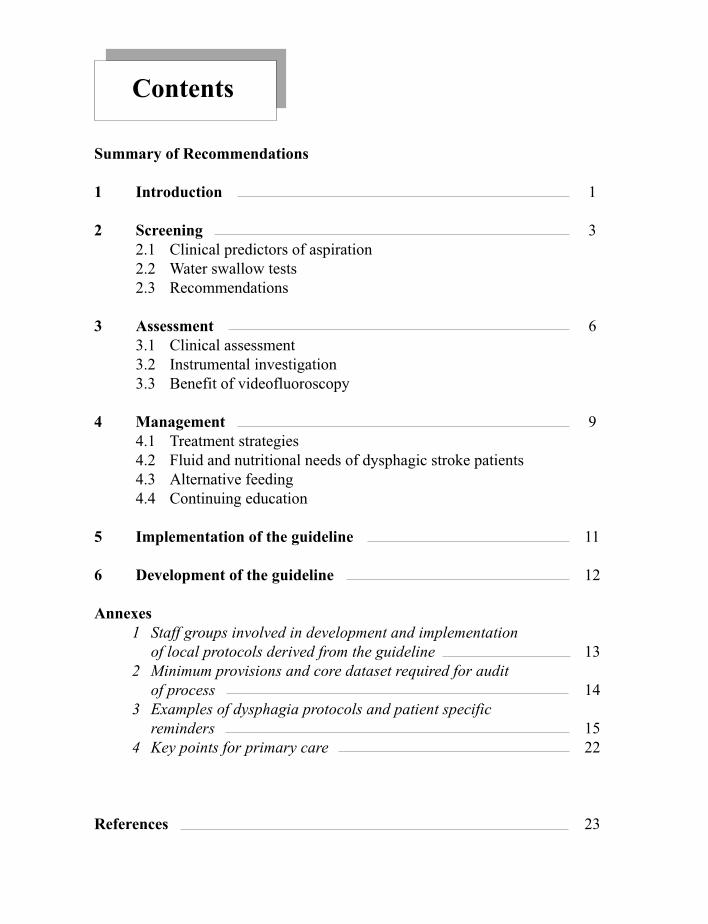
Contents
Summary of Recommendations
1 Introduction 1
2 Screening 32.1 Clinical predictors of aspiration2.2 Water swallow tests2.3 Recommendations
3 Assessment 63.1 Clinical assessment3.2 Instrumental investigation3.3 Benefit of videofluoroscopy
4 Management 94.1 Treatment strategies4.2 Fluid and nutritional needs of dysphagic stroke patients4.3 Alternative feeding4.4 Continuing education
5 Implementation of the guideline 11
6 Development of the guideline 12
Annexes1 Staff groups involved in development and implementation
of local protocols derived from the guideline 132 Minimum provisions and core dataset required for audit
of process 143 Examples of dysphagia protocols and patient specific
reminders 154 Key points for primary care 22
References 23
B
Grade
B
B
B
B
B
C
C
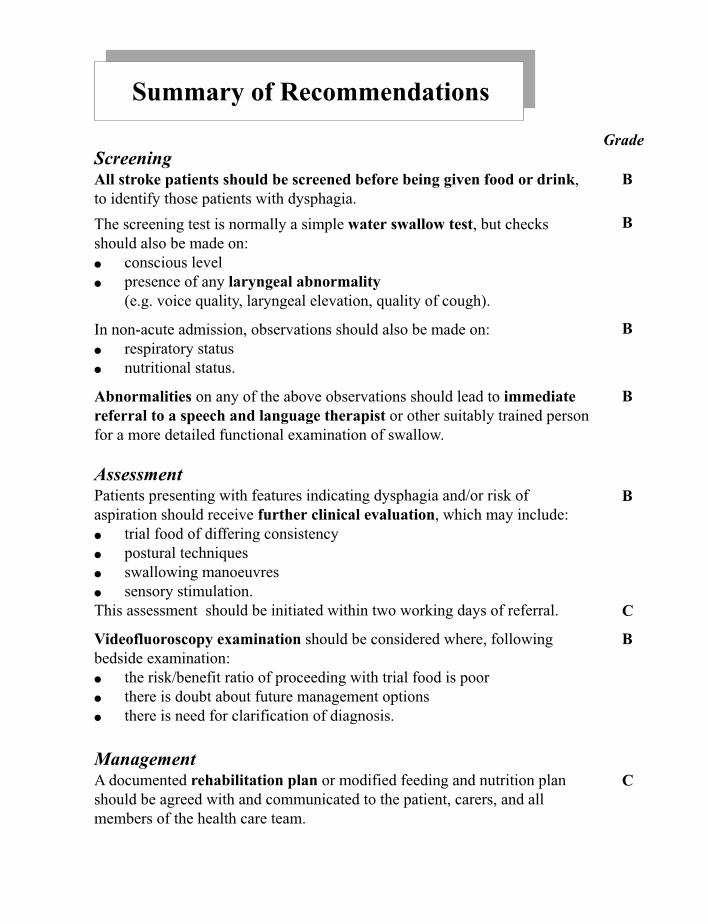
Summary of Recommendations
ScreeningAll stroke patients should be screened before being given food or drink,to identify those patients with dysphagia.
The screening test is normally a simple water swallow test, but checksshould also be made on:● conscious level● presence of any laryngeal abnormality
(e.g. voice quality, laryngeal elevation, quality of cough).
In non-acute admission, observations should also be made on:● respiratory status● nutritional status.
Abnormalities on any of the above observations should lead to immediatereferral to a speech and language therapist or other suitably trained personfor a more detailed functional examination of swallow.
AssessmentPatients presenting with features indicating dysphagia and/or risk ofaspiration should receive further clinical evaluation, which may include:● trial food of differing consistency● postural techniques● swallowing manoeuvres● sensory stimulation.This assessment should be initiated within two working days of referral.
Videofluoroscopy examination should be considered where, followingbedside examination:● the risk/benefit ratio of proceeding with trial food is poor● there is doubt about future management options● there is need for clarification of diagnosis.
ManagementA documented rehabilitation plan or modified feeding and nutrition planshould be agreed with and communicated to the patient, carers, and allmembers of the health care team.

Documentation of each patient’s nutritional status and fluid intake shouldbe routinely entered in the patient’s medical and nursing notes, and regularlyupdated.
Gastrostomy is recommended for appropriate patients requiring enteralfeeding, particularly in those where it is required for longer than four weeks,but may be considered earlier in some patients.
Awareness and EducationSpeech and language therapists with responsibility for dysphagiaassessment should have suitable training.
All personnel in contact with stroke patients in the acute stage should bemade aware of the possibility of dysphagia as a complication of stroke.
Nurses and junior doctors should receive appropriate education in therecognition of dysphagia, the prognosis and possible complications.
Catering staff should receive information and training to enable them toappreciate the importance of specific food consistencies and to produce thesewith the required nutritional supplement.
C
Grade
C
C
C
B
B
1 Introduction
1.1 DefinitionDysphagia, a difficulty in swallowing, can be caused by many pathologies,including stroke disease. In stroke it is characterised by difficulty in safely movinga bolus from the mouth to the stomach without aspiration and may also involvedifficulty in oral preparation for the swallow, e.g. chewing, tongue movement.
1.2 IncidenceA prospective study identified dysphagia in 45% of stroke admissions to hospital.2
Subsequent studies found similar high rates.3, 4
1.3 Dysphagia and stroke severityThe severity of stroke and severity of dysphagia are associated, although thepresence of dysphagia may be an indicator of poor prognosis independently of itsassociation with severity of stroke.4
1.4 Duration of dysphagia after strokeDysphagia after stroke is transient in many patients. The fact that many patientsrecover within a few weeks is a further complicating factor in attempts to determinethe prevalence of dysphagia. Reported recovery rates within the first few weeksvary from 43%5 to 86%.2 The different rates may depend on the techniques usedfor assessment: studies using videofluoroscopy report lower rates of recoveryand longer periods of time for recovery than those using bedside evaluation.
1.5 Consequences of dysphagiaPost-stroke dysphagia is a complication associated with excess morbidity andincreased mortality rates compared to strokes without dysphagia.2, 6, 7 Up to onethird of alert stroke patients with dysphagia are reported to die within the first sixmonths following stroke, compared with fewer than 10% of other alert strokepatients.4 Dysphagia is associated with risk of:
● Aspiration and associated bronchopulmonary infections8-13
The most immediate danger to health in most patients is aspiration of materialinto the tracheobronchial tree, which presents a triple threat of chemicalpneumonitis, bacterial pneumonia, and mechanical obstruction of the airways.Dysphagia in acute stroke has been shown to be associated with an increasedrisk of chest infection independent of aspiration.7
1
● Fluid depletion and undernutritionDysphagia has been demonstrated to relate to decline in nutritional status inthe first month following a stroke.7 There is also a risk of fluid depletion.2
1.6 Aim of the guidelineThe aim of this national guideline is to assist practitioners in reducing the morbidityassociated with dysphagia by early detection of swallowing disorders in strokepatients and application of appropriate methods to support food and fluid intake.
This guideline is the third in the series of four SIGN guidelines to assist in thedelivery of good quality clinical care following an acute stroke:
I Assessment, investigation, immediate management, and secondaryprevention
II Management of carotid stenosis and carotid endarterectomy
III Identification and management of dysphagia
IV Prevention and management of complications, rehabilitation and dischargeplanning.
2
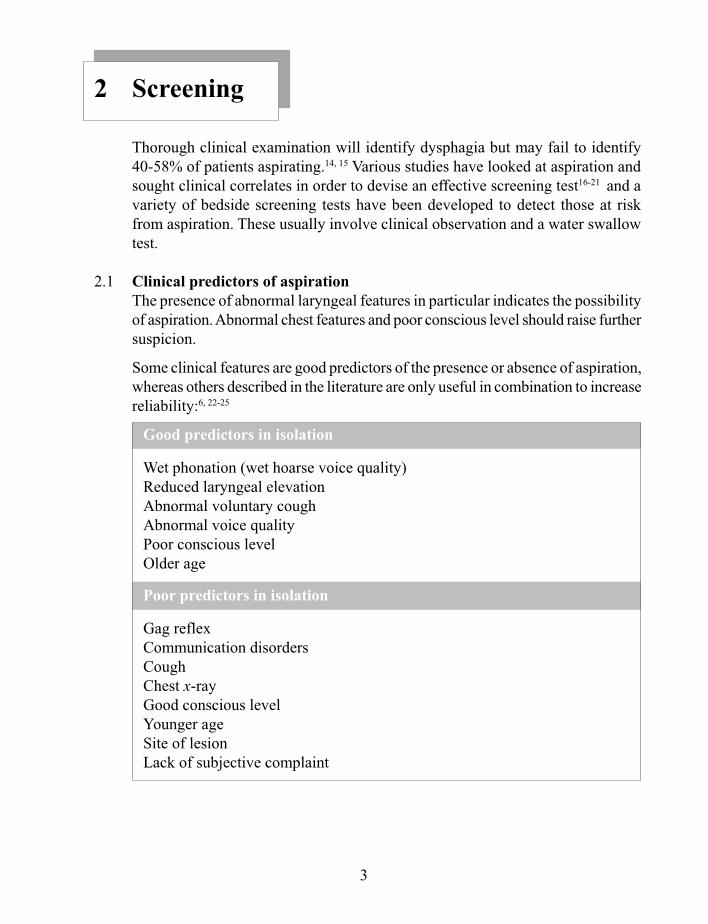
2 Screening
Thorough clinical examination will identify dysphagia but may fail to identify40-58% of patients aspirating.14, 15 Various studies have looked at aspiration andsought clinical correlates in order to devise an effective screening test16-21 and avariety of bedside screening tests have been developed to detect those at riskfrom aspiration. These usually involve clinical observation and a water swallowtest.
2.1 Clinical predictors of aspirationThe presence of abnormal laryngeal features in particular indicates the possibilityof aspiration. Abnormal chest features and poor conscious level should raise furthersuspicion.
Some clinical features are good predictors of the presence or absence of aspiration,whereas others described in the literature are only useful in combination to increasereliability:6, 22-25
Good predictors in isolation
Wet phonation (wet hoarse voice quality)Reduced laryngeal elevationAbnormal voluntary coughAbnormal voice qualityPoor conscious levelOlder age
Poor predictors in isolation
Gag reflexCommunication disordersCoughChest x-rayGood conscious levelYounger ageSite of lesionLack of subjective complaint
3
Combined features for more reliable prediction
Low probability of aspiration:
● Good conscious level, normal voluntary cough and absence of cough on a5ml teaspoon of water24 25
High probability of aspiration:
● Wet hoarse voice quality and impaired pharyngeal gag reflex22
● Reduced pharyngeal sensation and coughing or change in voice qualityon drinking 50ml of water6
● Bilateral stroke, abnormal gag reflex and impaired voluntary cough23
2.2 Water swallow testsSeveral simple tests for swallowing difficulties consist of the patient drinking aspecified volume of water with the examiner observing for choking, coughing,change in voice quality or effortful swallowing. Amounts of 10ml; 50ml in 5mlaliquots; and 90ml presented in a cup to be drunk without interruption have allbeen used.6, 26, 27 Most of these methods detect dysphagia in the majority of casesbut can fail to identify aspiration in between 20-40% of patients on validation byvideofluoroscopy.
The Timed Water Swallow Test consists of the patient drinking 150ml water froma glass as quickly as possible, with the examiner recording time taken and numberof swallows. From this data the speed of swallowing and average volume perswallow can be calculated. The timed water swallow test is reported to have apredictive sensitivity of 96% in identifying the presence of a swallowing disorderbut this has not been validated by videofluoroscopy.28
A combination of clinical observation and a water swallow test has been used inprotocols within hospitals25, 29 and it is anticipated that these tests could be carriedout by medical or nursing staff whether the patient is in hospital or not.
2.3 Recommendations
All stroke patients should be screened before being given food or drink toidentify those with dysphagia
Grade B, level III
4

The screening test is normally a simple water swallow test, but checks shouldalso be made on:
● conscious level
● presence of any laryngeal abnormality(e.g. voice quality, quality of cough or in laryngeal elevation)
● respiratory status
● nutritional status
The presence of abnormalities on any of the above observations should leadto immediate referral to a speech and language therapist or other suitablytrained personnel for a more detailed functional examination
These observations should be written into the protocol for admission notes
Grade B, level III
5
3 Assessment
Assessment of oropharyngeal swallow by trained personnel (currently Speechand Language Therapists) can define the physiological dysfunction or identifythe need for further investigation, which may be instrumental; test the effectivenessof selected treatments; and enable development of a treatment plan, taking intoconsideration the medical diagnosis and history.30-32
3.1 Clinical assessmentA full clinical examination is vital in order to obtain information on the following:14
● History of the patient’s disorder● Nutritional and respiratory status● Oral anatomy● Labial and lingual control● Palatal function● Laryngeal control● Best position of food in the mouth● Best food consistency● Ability to follow directions● Symptoms during attempts to swallow.
This assessment should normally be initiated within two working days of referral.33
Some attempts have been made to structure the clinical assessment in a testformat17, 34 but most evaluators follow their own checklist. This should includenotes on:
● The history and nature of the complaint from the patient, the carer and themedical notes.
● General observations on level of consciousness, posture, cognitive statusand ability to co-operate.
● Orofacial examination to assess the structure, function and sensitivity of theface, lips, tongue, palate, and larynx, including reflexes.
● Results of a direct test of swallowing using different food consistencies andobserving features of the oral and pharyngeal phases. Excursion and timingof the laryngeal movement should be measured by both visual and tactilemonitoring. Voice quality should be assessed. The effects of compensationstrategies should be noted.
6

Clinical assessment should normally be initiated within two working days ofreferral
Grade C
Patients presenting with features indicating dysphagia and/or risk ofaspiration should receive further clinical evaluation, which may include trialfood of differing consistency, postural techniques, swallowing manoeuvresor sensory stimulation
Grade B, level IIa & IIb
3.2 Instrumental investigationA limitation of clinical examination is that information on the pharyngeal stageof swallow can only be inferred and ‘silent’ aspiration may go undetected. Findingsfrom clinical assessment should be confirmed using a complementary techniquewhen there is any doubt about management.
3.2.1 VideofluoroscopyVideofluoroscopy (the modified barium swallow) identifies aspiration inpatients which cannot be identified clinically18 and remains the gold standardin patients who require a complete evaluation of pharyngeal dysfunction.35
3.2.2 Other instrumental investigationsAlternative methods of examination, e.g. videoendoscopy and cervicalauscultation, may be employed where the patient’s mobility precludesvideofluoroscopy, although videofluoroscopy remains the most common,reliable and easily available assessment at present.36-38
This will confirm subsequent patient management, either to work directly onswallowing using food and drink, postural techniques, swallowing manoeuvres,sensory stimulation, or changing food consistencies; or to work indirectly withoral motor exercises and facilitation techniques, giving nil by mouth.16, 19, 31, 32, 39
3.3 Benefit of videofluoroscopyThere have been no clinical trials to examine if changes in treatment followingvideofluoroscopy examination improve outcome. A retrospective study ofvideofluoroscopy in a variety of clinical disorders showed a significant increasein aspiration pneumonia in one group for which there was no specific managementof dysphagia compared with a group where dysphagia was actively managedfollowing videofluoroscopic identification of aspiration.40 A number of descriptivestudies support the view that videofluoroscopy has an important role in monitoringthe effectiveness of different therapy techniques.41-44
7

Videofluoroscopy examination should be considered where, following bedsideexamination, the risk/benefit ratio of proceeding with trial food is poor, wherethere is doubt about future management options, or where there is need forclarification of diagnosis
Grade B, level II & III
8
4 Management
4.1 Treatment strategiesThe decision whether to work directly on swallowing (i.e. to use food and/ordrink) or to work indirectly (i.e. to provide exercises to improve motor controlwithout the need to swallow) is based largely on the patient’s level of aspirationrisk and susceptibility to complicating sequelae.
● Oral feeding is best where possible.45
● Modification of food consistencies can significantly reduce the incidenceof aspiration pneumonia.46
● Posture techniques have a significant impact on the safety of the swallow.32
● Sensory enhancement can facilitate the triggering of the swallow in somecases.31, 47
● Swallow manoeuvres alter selected aspects of pharyngeal swallow.48, 49
4.2 Fluid and nutritional needs of dysphagic stroke patientsPrevention of dehydration is a priority when a patient is unable to manage anadequate fluid intake. Videofluoroscopic evaluation of aspiration predictspneumonia and death but not dehydration following stroke50 and regularmonitoring for evidence of fluid depletion is required (e.g. fluid balance charts,serum electrolytes).
Protein energy malnutrition is found in up to 16% of stroke patients admitted tohospital,51 and in other patient groups this is associated with poor recovery andrehabilitation.52-54 Although no specific studies have been carried out with strokepatients, early recognition of malnutrition and prompt nutritional interventionhas been shown in other patient groups to improve recovery and lead to a reducedhospital stay.55-58 Documentation of nutritional status aids early identification ofnutritional problems.59 The hospital menu should be adapted to provide suitablechoices for patients requiring modification of food consistencies.
4.3 Alternative feedingArtificial nutritional support may be required in those patients who are not in aterminal state where oral intake is considered to lead to high risk of aspiration orwhere oral intake does not meet nutritional requirements. An initial trial ofnasogastric (NG) feeding is appropriate, particularly if feeding may be requiredfor only a few days. However the risk of aspiration, which persists with both NGand gastrostomy feeding, may be exacerbated with NG feeding.60
9
Endoscopic gastrostomy has been demonstrated to be a safe technique in thosewith persisting neurological dysphagia.61 One study has shown that gastrostomyfeeding introduced two weeks post-stroke in those with persisting dysphagiareduces mortality and improves nutritional indices compared to nasogastricfeeding.62 However, the mean survival time for patients post-gastrostomy appearsto be poor63 and more research is required to clarify the timing and type ofnutritional support and the benefits to be found.
A rehabilitation plan or modified feeding and nutrition plan should be agreedwith, documented and communicated effectively to the patient, carers andall members of the health care team
Documentation of each patient’s nutritional status and fluid intake shouldbe routinely entered in the patient’s medical and nursing notes, and regularlyupdated
Gastrostomy is recommended for appropriate patients requiring enteralfeeding, particularly in those where it is required for longer than four weeks,but may be considered earlier in some patients
Grade C
4.4 Continuing educationAll personnel in contact with stroke patients in the acute stage should be aware ofthe possibility of dysphagia as a complication of stroke. Multidisciplinary trainingopportunities improve staff awareness and understanding of dysphagia patients’needs with regard to food texture, safety, dignity, psychological and physicalwell-being.33, 64, 65
All personnel in contact with stroke patients in the acute stage should bemade aware of the possibility of dysphagia as a complication of stroke
Nurses and junior doctors should receive appropriate education in screeningfor dysphagia, the prognosis and possible short and long term complications
Speech and language therapists with responsibility for dysphagia assessmentshould have suitable training as recommended by the Royal College of Speech& Language Therapists33
Catering staff should receive information and training to enable them toappreciate the importance of specific food consistencies and to prepareappropriate meals or food items, with any necessary nutritionalsupplementation advised by a dietitian
Grade C
10
5 Implementation of the Guideline
5.1 Health gain which may accrue from the implementation of this guideline:
● Prompt identification of dysphagia may minimise the risk of pulmonaryproblems.
● Therapeutic strategies may enable patients to swallow safely, while protectingthe airway.
● Videofluoroscopic assessment may identify silent aspiration which cannotbe diagnosed from bedside assessment.
● Prompt nutritional intervention may lead to improved recovery and reducedstay in hospital.
5.2 Appropriate management of dysphagia may be promoted in the following ways:
● Patient-specific reminders at time of consultation or admissionSeveral examples of dysphagia protocols and patient specific reminders whichmay serve as the basis for development of local protocols are shown at Annex3.
● Audit of key outcome indicatorsIdentification of suitable outcome indicators is difficult as dysphagia is onlyone of many possible causes of bronchopulmonary infection. The nutritionalstatus and quality of life of surviving patients should also be considered.
● Audit of processThe minimum provisions and clinical core dataset required for audit of processare listed at Annex 2.
11
6 Development of the Guideline
6.1 Responsible bodiesThe series of SIGN guidelines on management of patients with stroke wasdeveloped through the Royal College of Physicians and Surgeons of Glasgow,under the chairmanship of Dr Margaret Roberts, acting on behalf of the ScottishIntercollegiate Guidelines Network (SIGN) and these have been accepted by SIGNas the Scottish National Guidelines from which local protocols should be derived.Membership of the dysphagia guideline development group is listed at the frontof the guideline. Declarations of interest of guideline development group membersare held by the SIGN secretariat.
6.2 Development processSuccessive drafts were developed by synthesis of the literature (identified byMedline search with references in key papers followed up), correspondence andfull discussion. The draft recommendations were discussed at two consensusconferences held in Glasgow and Edinburgh, attended by 350 health careprofessionals and representatives of Chest, Heart & Stroke Scotland.
6.3 Recommendations for further research
● Development of new techniques for assessment and non-invasive tests formeasurement of outcomes of dysphagia management
● The relative risks of aspiration, silent and overt, to a stroke patient
● Home care needs of patients with dysphagia
● The effect of dysphagia therapy and management on the incidence ofpneumonia and other morbidity
● Communication and compliance, involving the dysphagia team, patients andcarers
● Timing and type of nutritional support required in dysphagic patients.
12
Annex 1
Staff groups who require to be involved in development and implementation of localprotocols derived from this national guideline.
● Hospital and primary care medical staff
● Nursing staff in hospital and community
● Pharmacy staff
● Occupational Therapy staff
● Physiotherapy staff
● Speech & Language Therapy staff
● Dietetic staff
● Catering staff
● Area audit committees
● Deans and Postgraduate Deans of University Faculties of Medicine inScotland and other relevant professional educational bodies
● Radiologists and radiographers
13
Annex 2
Minimum provisions and core dataset required for audit of process
1 All stroke patients screened by trained nursing or medical staff on receivingward for aspiration risk prior to presentation of food or drink
2 Patients presenting with risk features referred to speech and language therapistfor specialist evaluation, with involvement of other members of themultidisciplinary team as appropriate
3 Speech and language therapy and dietetics response to referral within agreedresponse time
4 Outcome of speech and language therapy assessment and dietetic assessmentrecorded in the medical/nursing notes
5 Availability and appropriate use of videofluoroscopy to clarify risk/benefitof oral intake
6 Management plan for oral intake agreed by multidisciplinary team anddocumented
7 Completeness of food record chart in notes
8 Availability of appropriate diet of recommended consistency and nutritionalcontent for next meal, provided 1.5 hours’ notice given
9 Availability of appropriate snacks between meals
10 Appropriate use of alternative feeding
11 All disciplines adhere to management plan
12 Evidence of communication with patient and/or carers about dysphagia.
14
Annex 3
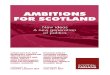
Examples of dysphagia protocols and patient specific reminderswhich may serve as the basis for development of local protocols
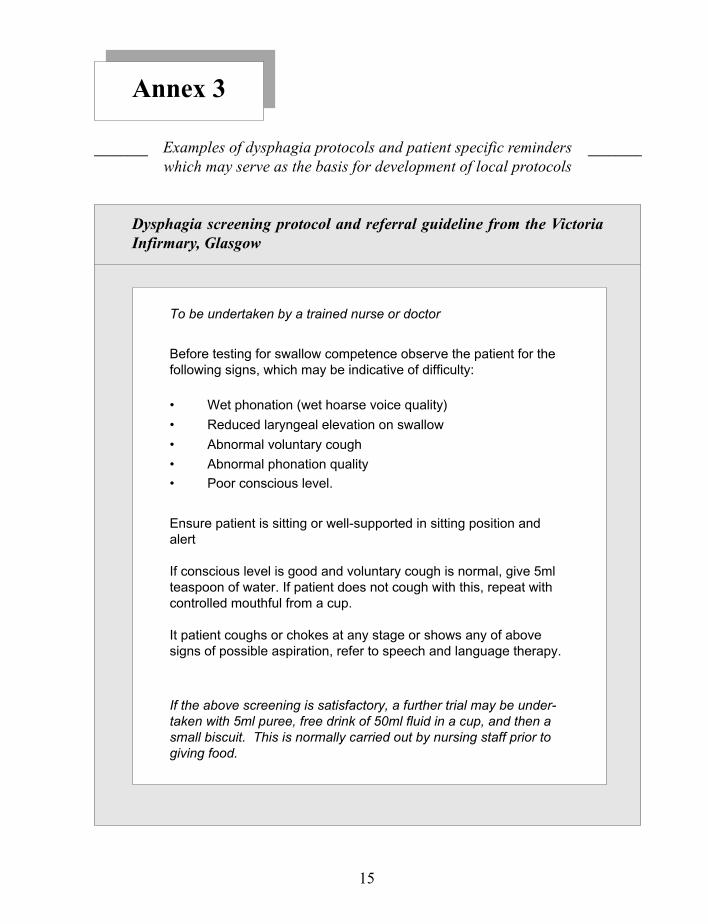
Dysphagia screening protocol and referral guideline from the VictoriaInfirmary, Glasgow
To be undertaken by a trained nurse or doctor
Before testing for swallow competence observe the patient for thefollowing signs, which may be indicative of difficulty:
• Wet phonation (wet hoarse voice quality)
• Reduced laryngeal elevation on swallow
• Abnormal voluntary cough
• Abnormal phonation quality
________ ________
15
• Poor conscious level.
Ensure patient is sitting or well-supported in sitting position andalert
If conscious level is good and voluntary cough is normal, give 5mlteaspoon of water. If patient does not cough with this, repeat withcontrolled mouthful from a cup.
It patient coughs or chokes at any stage or shows any of abovesigns of possible aspiration, refer to speech and language therapy.
If the above screening is satisfactory, a further trial may be under-taken with 5ml puree, free drink of 50ml fluid in a cup, and then asmall biscuit. This is normally carried out by nursing staff prior togiving food.
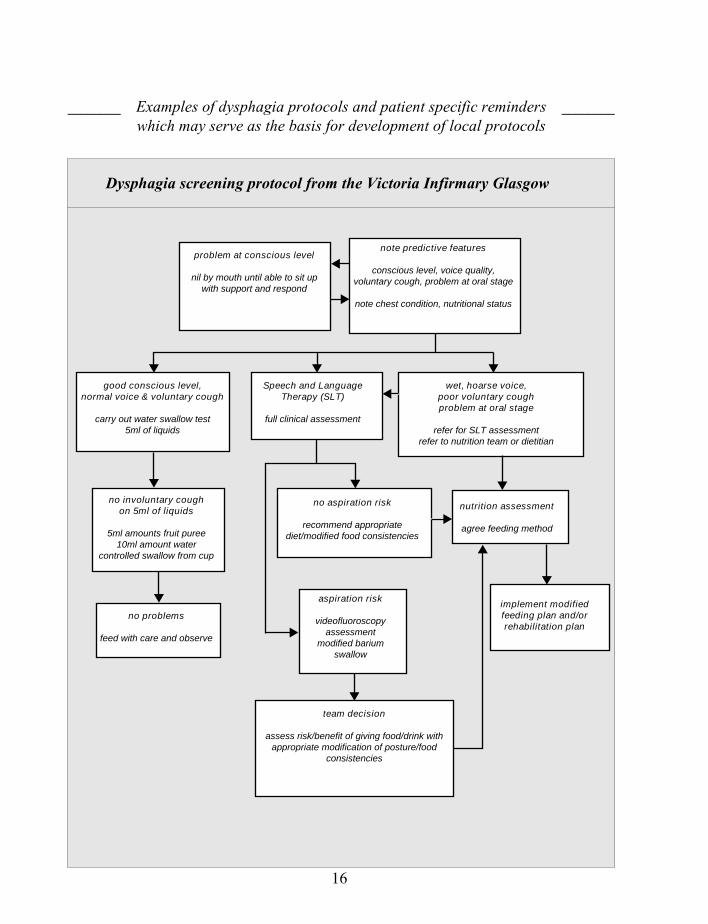
team decision
assess risk/benefit of giving food/drink withappropriate modification of posture/food
consistencies
implement modifiedfeeding plan and/orrehabilitation plan
aspiration risk
videofluoroscopyassessment
modified bariumswallow
no problems
feed with care and observe
nutrition assessment
agree feeding method
no aspiration risk
recommend appropriatediet/modified food consistencies
no involuntary coughon 5ml of liquids
5ml amounts fruit puree10ml amount water
controlled swallow from cup
wet, hoarse voice,poor voluntary coughproblem at oral stage
refer for SLT assessmentrefer to nutrition team or dietitian
Speech and LanguageTherapy (SLT)
full clinical assessment
good conscious level,normal voice & voluntary cough
carry out water swallow test5ml of liquids
note predictive features
conscious level, voice quality,voluntary cough, problem at oral stage
note chest condition, nutritional status
problem at conscious level
nil by mouth until able to sit upwith support and respond
Examples of dysphagia protocols and patient specific reminderswhich may serve as the basis for development of local protocols
Dysphagia screening protocol from the Victoria Infirmary Glasgow
________ ________
16
Examples of dysphagia protocols and patient specific reminderswhich may serve as the basis for development of local protocols
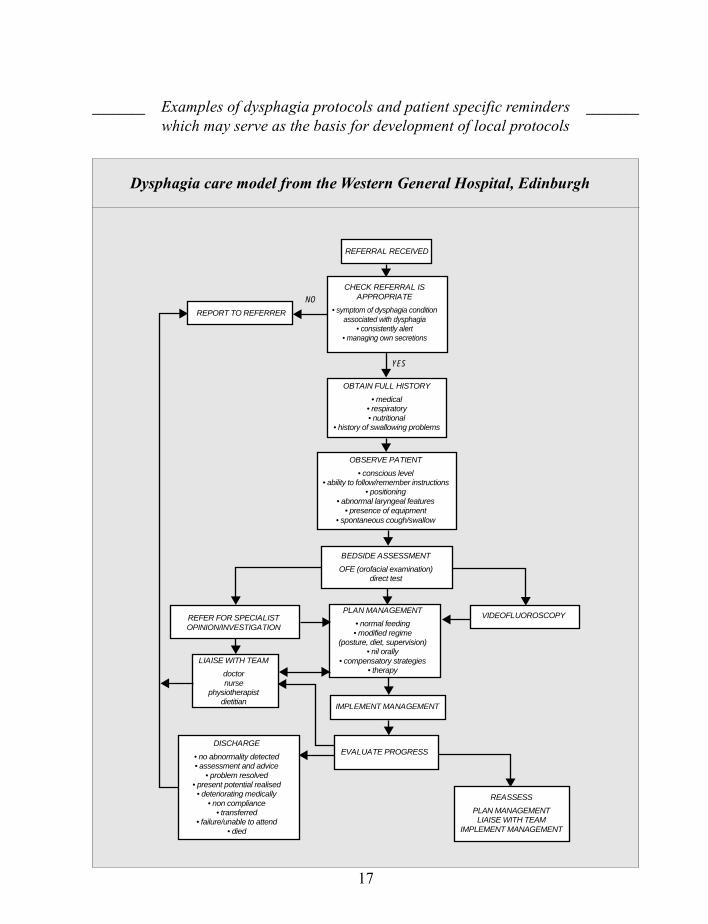
Dysphagia care model from the Western General Hospital, Edinburgh
________ ________
CHECK REFERRAL ISAPPROPRIATE
• symptom of dysphagia conditionassociated with dysphagia
• consistently alert• managing own secretions
OBTAIN FULL HISTORY
• medical• respiratory• nutritional
• history of swallowing problems
REPORT TO REFERRER
OBSERVE PATIENT
• conscious level• ability to follow/remember instructions
• positioning• abnormal laryngeal features
• presence of equipment• spontaneous cough/swallow
BEDSIDE ASSESSMENT
OFE (orofacial examination)direct test
REFER FOR SPECIALISTOPINION/INVESTIGATION
PLAN MANAGEMENT
• normal feeding• modified regime
(posture, diet, supervision)• nil orally
• compensatory strategies• therapy
VIDEOFLUOROSCOPY
LIAISE WITH TEAM
doctornurse
physiotherapistdietitian
IMPLEMENT MANAGEMENT
EVALUATE PROGRESSDISCHARGE
• no abnormality detected• assessment and advice
• problem resolved• present potential realised• deteriorating medically
• non compliance• transferred
• failure/unable to attend• died
REASSESS
PLAN MANAGEMENTLIAISE WITH TEAM
IMPLEMENT MANAGEMENT
NO
YES
REFERRAL RECEIVED
17
18
________ ________Examples of dysphagia protocols and patient specific reminderswhich may serve as the basis for development of local protocols
Example of a dysphagia protocol from the Western General Hospital, Edinburgh
Aims of ServiceTo provide a comprehensive and responsive service to clients presenting or at risk of presentingwith oropharyngeal swallowing disorders.To facilitate intervention as part of the multidisciplinary team.
ReferralsInpatients:Verbal referral by nurse or paramedical team member must be supported by a doctor’s writtenconsent. A consultant may agree to blanket referrals for his patients where individual writtenconsent is not necessary.
Outpatients:A written request by the consultant or GP is required.
Videofluoroscopy:If the referral is from outwith the trust, a Speech & Language Therapy report isrequested in addition to the doctor’s letter.
Patients will be accepted into the service who:
• have a presenting symptom of oropharyngeal dysphagia
• are at risk of having a presenting symptom as a result of having a condition associated withdysphagia
• are consistently alert for periods of 15-20 minutes
• are able to manage their own secretions
To provide a dysphagia service, the department must have:
• appropriate staffing
• appropriate skillmix
in order to discharge the ‘duty of care’ in full.
AetiologiesPatients with oropharyngeal dysphagia arising from neurological, structural or psychogenicorigins will be seen. Only adult patients will be seen as there are specialist services for childrenelsewhere in the area.
Response TimesStandards:• All inpatients to be seen within one full working day of receipt of referral.
• All outpatients to be sent an appointment within one working week of receipt of referral and willbe seen within three working weeks of referral receipt.
On receipt of referrals, close liaison with the relevant health and social care teams should beinstituted in order to gain the maximum information regarding the client and presenting disorderand to assess urgency.
The service should be flexible enough to respond to urgent outpatient referrals within oneworking week, provided sufficient information is available to contact the patient.
SettingsPatients will be seen within the trust as inpatients and outpatients. Domiciliary visits may becarried out, but a full assessment may not be carried if the risk to the patient is considered toogreat.
Reporting/DocumentationEach intervention, including assessment results and therapy given (including consistencies andvolumes taken), will be reported in the Speech & Language Therapy notes within 24 hours ofthe event.
Written summary reports of assessment results progress, management changes and dischargewill be submitted to the medical notes at appropriate intervals.
A written, individualised care plan will be placed in the nursing notes or at the bedside forinpatients or given to the patient or carer in the case of outpatients.
Verbal reports will be made to medical, nursing and other appropriate staff.
Safety Procedures
1. Full history should be obtained and patient should be observed before direct testing takes
place.
2. A physiotherapist should be present when assessing unknown patients initially. Considerationto having a physiotherapist present should be given during subsequent assessments andtherapy.
3. Therapists should adhere to the requirements of the Food Handling Act (1990).4. Therapists should follow the trust infection control policy.5. Therapists should observe manual handling guidelines.6. Therapists should comply with radiation protection standards.7. Therapists should be familiar with emergency procedures in the trust.
Professional RelationshipsThe therapist will liaise with other professionals, carers and relevant voluntary agencies toachieve the best, integrated care for the patient.
The dysphagia team may include: doctor, nurse, auxiliary nurse, physiotherapist, dietitian, dietcook, and occupational therapist (amongst others), as well as the patient and their carers.
* Where disputes concerning management occur, the therapist should aim to resolve thediscussion. If the dispute cannot be resolved, the therapist may have to consider withdrawingfrom the case.
DischargeThe patient is discharged from the service under the following circumstances:
• assessment complete and advice given• problem resolved• modified regime established - potential realised• deteriorating medical condition• non-compliance• transferred• deceased• therapist withdrawalTeam members, the patient and family/carers should be involved in the decision to discharge.
The procedure for further contact with the department should be made clear to patient/carerswhere required.
19
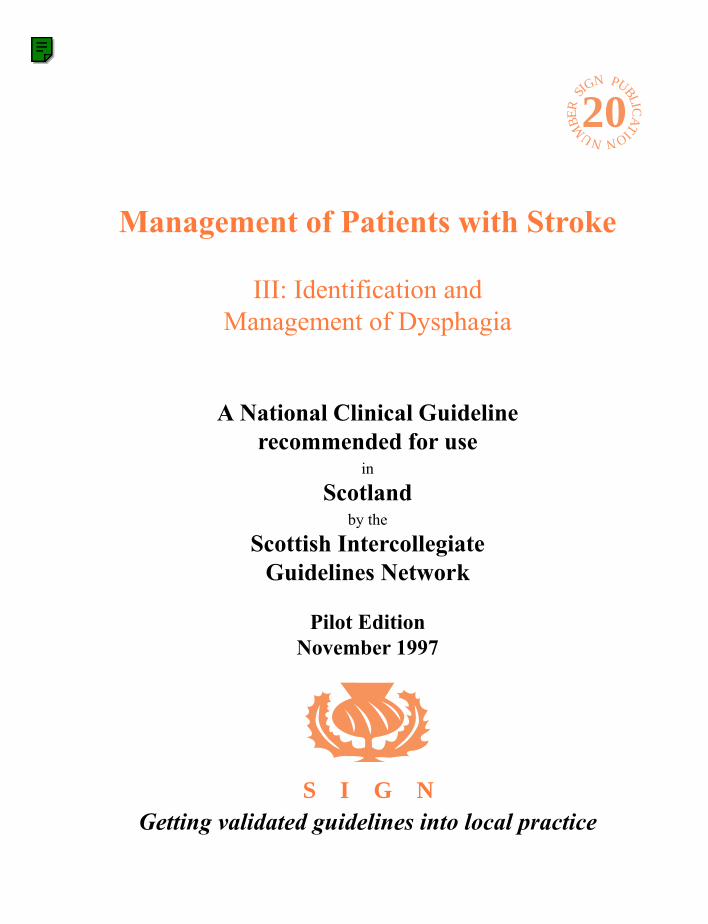
Examples of dysphagia protocols and patient specific reminderswhich may serve as the basis for development of local protocols
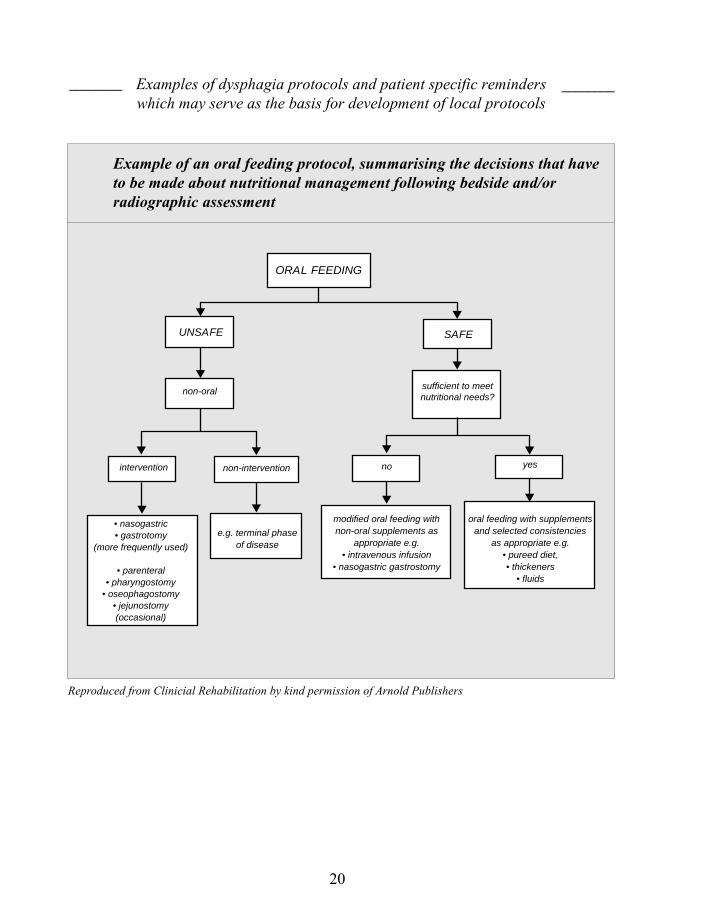
Example of an oral feeding protocol, summarising the decisions that haveto be made about nutritional management following bedside and/orradiographic assessment
________ ________
Reproduced from Clinicial Rehabilitation by kind permission of Arnold Publishers
20
ORAL FEEDING
UNSAFE SAFE
non-oral sufficient to meetnutritional needs?
intervention non-intervention no yes
• nasogastric• gastrotomy
(more frequently used)
• parenteral• pharyngostomy
• oseophagostomy• jejunostomy(occasional)
e.g. terminal phaseof disease
modified oral feeding withnon-oral supplements as
appropriate e.g.• intravenous infusion
• nasogastric gastrostomy
oral feeding with supplementsand selected consistencies
as appropriate e.g.• pureed diet,• thickeners
• fluids
Points to Note
• food thickeners can be added toliquids (cold or hot)
• smooth, thick and uniformconsistency with no hard lumps
• restricted in quantity• think of it as a “tool” which
allows the patient to practiseswallowing
• smooth, thick and uniformconsistency with no hard lumps
• larger quantities than in ‘practicestage’
• no separate liquid from food• do not mix food textures to eat
at the same time e.g. ice-creamand jelly or liquidised porridgeand milk
• foods can be easily mashed witha fork
• foods likely to need a thicksauce or gravy
• foods can be easily chewed• avoid patient becoming tired
from chewing
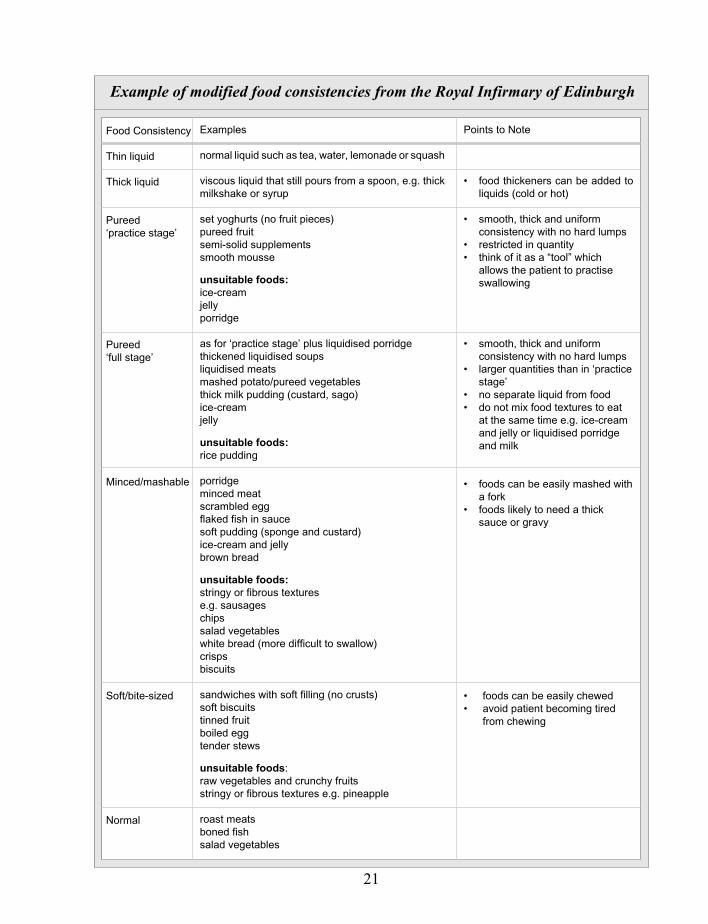
Example of modified food consistencies from the Royal Infirmary of Edinburgh
Examples
normal liquid such as tea, water, lemonade or squash
viscous liquid that still pours from a spoon, e.g. thickmilkshake or syrup
set yoghurts (no fruit pieces)pureed fruitsemi-solid supplementssmooth mousse
unsuitable foods:ice-creamjellyporridge
as for ‘practice stage’ plus liquidised porridgethickened liquidised soupsliquidised meatsmashed potato/pureed vegetablesthick milk pudding (custard, sago)ice-creamjelly
unsuitable foods:rice pudding
porridgeminced meatscrambled eggflaked fish in saucesoft pudding (sponge and custard)ice-cream and jellybrown bread
unsuitable foods:stringy or fibrous texturese.g. sausageschipssalad vegetableswhite bread (more difficult to swallow)crispsbiscuits
sandwiches with soft filling (no crusts)soft biscuitstinned fruitboiled eggtender stews
unsuitable foods:raw vegetables and crunchy fruitsstringy or fibrous textures e.g. pineapple
roast meatsboned fishsalad vegetables
Food Consistency
Thin liquid
Thick liquid
Pureed‘practice stage’
Pureed‘full stage’
Minced/mashable
Soft/bite-sized
Normal
21

Annex 4
Key points for primary care
● All personnel in contact with stroke patients in the acute stage should bemade aware of the possibility of dysphagia as a complication of stroke.
● A prospective study identified dysphagia in 45% of stroke patients admittedto hospital.2 Subsequent studies found similar high rates.3
● Up to one third of alert stroke patients with dysphagia are reported to diewithin the first six months following stroke, compared with fewer than 10%of other alert stroke patients.4
● The most immediate danger to health in most patients is aspiration of materialinto the tracheobronchial tree, which presents a triple threat of chemicalpneumonitis, bacterial pneumonia, and mechanical obstruction of theairways.8-13
● Thorough clinical examination will identify dysphagia but fail to identify40-58% of patients aspirating.14, 15
● A simple water swallow test is feasible in the primary care setting to screenfor stroke-associated dysphagia.
22
1 US Department of Health and Human Services, Agency for Health Care Policy and Research. Acute PainManagement: operative or medical procedures and trauma. Rockville (MD): The Agency; 1993. ClinicalPractice Guideline No.1. AHCPR Pub 92-0023. p.107.
2 Gordon C, Hewer RL, Wade DT. Dysphagia in acute stroke. BMJ 1987; 295: 411-414.
3 Penington GR, Krutsch JA. Swallowing disorders: assessment and rehabilitation. Brit J Hosp Med 1990; 44:17-22.
4 Barer DH. The natural history and functional consequences of dysphagia after hemispheric stroke. J NeurolNeurosurg & Psych 1989; 52: 236-241.
5 Teasell RW, Bach D, McRrae M. Prevalence and recovery of aspiration post stroke. A retrospective analysis.Dysphagia 1994; 9: 35-39.
6 Kidd D, Lawson J, Nesbitt R, MacMahon J. Aspiration in acute stroke: a clinical study with videofluoroscopy.QJM 1993; 86: 825-829.
7 Smithard DG, O’Neill PA, Parks C, Morris J. Complications and outcome after acute stroke: does dysphagiamatter? Stroke 1996; 27: 1-5.
8 Johnson ER, McKenzie SW, Sievers A. Aspiration in pnuemonia in stroke. Arch Phys Med Rehab 1993; 74:973-976.
9 Martin BJ, Corlew MM, Wood H, Olsen D, Golopol LA, Wing OM, et al. The association of swallowingdysfunction and aspiration pneumonia. Dysphagia 1994; 9: 1-16.
10 Loughlin GM. Respiratory consequences of dysfunctional swallowing and aspiration. Dysphagia 1989; 3:126-130.
11 Ekberg O, Hilderfoers H. Defective closure of the laryngeal vestibule: frequency of pulmonary complications.Am J Roentgenol 1985; 145: 1159-1164.
12 Silver FL, Norris JW, Lewis AJ, Hachinski VC. Early mortality following stroke: a prospective review. Stroke1984 15; 492-496.
13 Nahum AM, Harris JP, Davidson TM. The patient who aspirates: diagnosis and management. JOtolaryngol 1981; 10: 10-16.
14 Logemann JA. Evaluation and treatment of swallowing disorders. San Diego, College Hill Press 1983.
15 Logemann JA. Treatment of aspiration related to dysphagia: an overview. Dysphagia 1986; 1: 34-38.
16 Horner J, Buoyer FG, Alberts MJ, Helms MJ. Dyspagia following brainstem stroke. Clinical correlates andoutcome. Arch Neurol 1991; 48: 1170-1173.
17 Linden P, Kuhlemeier KV, Patterson C. The probability of correctly predicting subglottic penetration fromclinical observations. Dysphagia 1993; 8: 170-179.
18 Horner J, Massey EW. Silent aspiration following stroke. Neurology 1988; 38: 317-319.
19 Horner J, Massey EW, Riski JE, Lathrop DL, Chase KN. Aspiration following stroke. Clinical correlates andoutcome. Neurology 1988; 38: 1359-1362.
20 Huxley EJ, Viroslav J, Gray WR, Pierce AK. Pharyngeal aspiration in normal adults and patients with depressedconsciousness. Am J Med 1978; 64: 564-568.
21 Kuhlemeier KV, Rieve JE, Kirby NA, Siebens AA. Clinical correlates of dysphagia in stroke patients. ArchPhys Med Rehabil 1989; 70: A-56.
22 Linden P, Siebens AA. Dysphagia: predicting laryngeal penetration. Arch Phys Med Rehabil 1983; 64: 281-284.
23 Horner J, Braser SR, Massey EW. Aspiration in bilateral stroke patients: a validation study. Neurology 1993;43: 430-433.
References
23
24 Park C, O’Neill PA. Management of neurological dysphagia. Clin Rehab 1994; 8: 166-174.
25 Smithard DG, Crockford C. Dysphagia: Are speech and language therapists coping with increasing referrals?CSLT Bulletin 1995; March 8-9.
26 Sonies BC, Weiffenbach J, Atkinson JC, Brahim J, Macynski A, Fox PC. Clinical examination of motor andsensory functions of the adult oral cavity. Dysphagia 1987; 1: 178-186.
27 DePippo KL, Holas MA, Reding MJ. Validation of the 3 oz water swallow test for aspiration following stroke.Arch Neurol 1992; 49: 1259-1261.
28 Nathadwarawala KM, Nicklin J, Wiles CM. A timed test of swallowing capacity for neurological patients. JNeurol Neurosurg Psychiatry 1992; 55: 822-825.
29 Gottlieb D, Kipnis M, Sister E, Vardi Y, Brill S. Validation of the 50ml drinking test for evaluation of post-stroke dysphagia. Disabil Rehabil 1996; 18: 529-532.
30 Logemann JA. The dysphagia diagnostic procedure as a treatment efficacy trial. Clin Commun Disord 1993;3: 1-10.
31 Lazarus CL, Logemann JA, Rademaker AW, Kahrilas PJ, Pajak T, Lazar R, et al. Effects of bolus volume,viscosity and repeated swallows in non stroke subjects and stroke patients. Arch Phys Med Rehabil 1993; 74:1066-1070.
32 Logemann JA, Kahrilas PJ, Kobara M, Vakil NB. The benefit of head rotation on pharyngoesophagealdysphagia. Arch Phys Med Rehabil 1989; 70: 767-771.
33 Van der Graay A. Communicating Quality: professional standards for speech and language therapists. 2nd ed.London: Royal College of Speech and Language Therapists; 1997.
34 Cherney LR, Cantieri CA, Pannel JJ. Clinical evaluation of dysphagia. Rehabilitation Institute of Chicagoprocedure manual. Maryland: Aspen Systems Corporation, 1986.
35 Mendelsohn M. New concepts in dysphagia management. J Otolaryngol 1993; 22 (Suppl 1) 1-24.
36 Bastian RW. Videoendoscopic evaluation of patients with dysphagia: an adjunct to the modified barium swallow.Otolaryngol Head Neck Surg 1991; 104: 339-349.
37 Langmore SE, Schatz K, Olson N. Endoscopic and videofluoroscopic evaluation of swallowing and aspiration.Ann Otol Rhinol Laryngol 1991; 100: 678-681.
38 Zenner PM, Losinski DS, Mills RH. Using cervical auscultation in the clinical dysphagia examination inlong-term care. Dysphagia 1995; 10: 27-31.
39 Shanahan TK, Logemann JA, Rademaker AW, Pauloski BR, Kahrilas PJ. Chin-down posture effect on aspirationin dysphagic patients. Arch Phys Med Rehabil 1993; 74: 736-739.
40 Kasprisin AT, Clumeck H, Nino-Murcia M. Efficacy of the rehabilitative management of dysphagia. Dysphagia1989; 4: 48-52.
41 Splaingard ML, Hutchins B, Sulton LD, Chaudhuri G. Aspiration in rehabilitation patients: videofluoroscopyvs bedside clinical assessment. Arch Phys Med Rehabil 1988; 69: 637-640.
42 Logemann JA. Dysphagia: evaluation and treatment. Folia Phoniatr Logop 1995; 47: 140-164.
43 Sorin R, Somers S, Austin W, Bester S. The influence of videofluoroscopy on the management of the dysphagicpatient. Dysphagia 1988; 2: 127-135.
44 Neumann S. Swallowing therapy with neurological patients: results of direct and indirect therapy methods in66 patients suffering from neurological disorders. Dysphagia 1993; 8: 150-153
45 Pardoe EM. Development of a multistage diet for dysphagia. J Am Diet Assoc 1993; 93: 568-571.
46 Groher ME. Bolus management and aspiration: pneumonia in patients with pseudobulbar dysphagia. Dysphagia1987; 1: 215-216.
47 Kahrilas PJ, Logemann JA, Krugler C, Flanagan E. Volitional augmentation of upper oesophageal sphincteropening during swallow. Am J Physiol 1991; 260 G450-456.
48 Kahrilas PJ, Logemann JA. Volume accommodation during swallowing. Dysphagia 1993; 8: 259-265.
24
25
49 Martin BJ, Logemann JA, Shaker R, Dodds WJ. Normal laryngeal valving patterns during three breath-holdmanoeuvres: a pilot investigation. Dysphagia 1993; 8: 11-20.
50 Schmidt J, Holas M, Halvorson K, Reding M. Videofluoroscopic evidence of aspiration predicts pneumoniaand death but not dehydration following stroke. Dysphagia 1994; 9: 7-11.
51 Axelsson K, Asplund K, Norberg A, Alafuzoff I. Nutritional status in patients with acute stroke. Acta MedScand 1988; 224: 217-224.
52 McWhirter JP, Pennington CR. Incidence and recognition of malnutrition in hospital. BMJ 1994; 308: 945-948.
53 Larsson J, Unosson M, Ek AC, Nilsson L, Thorslund S, Bjurulf P. Effect of dietary supplement on nutritionalstatus and clinical outcome in 501 geriatric patients - a randomised study. Clin Nutrition 1990; 9: 179-184.
54 Axelsson K, Asplund K, Norberg A, Eriksson S. Eating problems and nutritional status during hospital stay ofpatients with severe stroke. J Am Diet Assoc 1989; 89: 1092-1096.
55 Robinson G, Goldstein M, Levine GM. Impact of nutritional status on DRG length of stay. J ParenterEnteral Nutr 1987; 11: 49-51.
56 Nyswonger GD, Helmchen RH. Early enteral nutrition and length of stay in stroke patients. J Neurosci Nurs1992; 24: 220-223.
57 Allison SP. Review: The uses and limitation of nutritional support. Eur J Clin Nutr 1992; 11: 319-20.
58 Unosson M, Ek AC, Bjurulf P, von Schenck H, Larsson J. Feeding dependence and nutritional status afteracute stroke. Stroke 1994; 25: 366-371.
59 Silk DB, Cottam TK, Neilsen MS, Elcoat C, Fawcett H, Furness KM, et al. Organisation of nutritional supportin hospitals, nutrition steering committee and nutrition support teams: needs, structure and roles. BritishAssociation for Parenteral and Enteral Nutrition working party report. PO Box 22, Maidenhead, Berks SL64SH, 1994.
60 Finucane TE, Bynum JP. Use of tube feeding to prevent aspiration pneumonia. Lancet 1996; 348: 1421-1424.
61 Park RH, Allison MC, Lang J, Spence E, Morris AJ, Danesh BJ, et al. Randomised comparison of percutaneousendoscopic gastrostomy and nasogastric tube feeding in patients with persisting neurological dysphagia. BMJ1992; 304: 1406-1409.
62 Norton B, Homer-Ward M, Donnelly MT, Long RG, Holmes GK. A randomised prospective comparison ofpercutaneous endoscopic gastrostomy and nasogastric tube feeding after acute dysphagic stroke. BMJ 1996;312: 13-16.
63 Wanklyn P, Cox N, Belfield P. Outcome in patients who require gastrostomy after a stroke. Age Ageing 1995;24: 510-514.
64 Lombard M. Using a team approach to improve the management of dysphagic clients. The Golden HelixAward for Total Quality in Health Care 1994/5. Report from the States of Jersey Health and Social Services.
65 Scottish Health Service Advisory Council. The management of patients with stroke: report of a workinggroup of the National Medical Advisory Committee, Edinburgh, HMSO 1993.
SIGN PUBLIC
ATIONNUMBE
R 20
Additional copies of this Quick Reference Guide and the full guideline are available from
SIGN Secretariat, 9 Queen Street, Edinburgh, EH2 1JQThis Quick Reference Guide was issued in November 1997 and will be reviewed in 1999
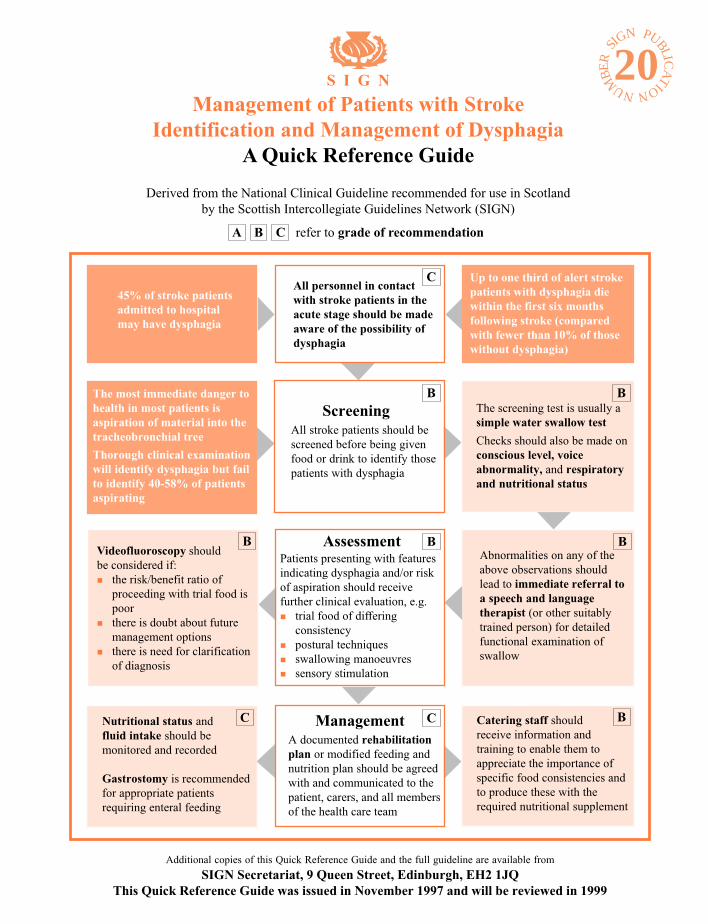
45% of stroke patientsadmitted to hospitalmay have dysphagia
The most immediate danger tohealth in most patients isaspiration of material into thetracheobronchial tree
Thorough clinical examinationwill identify dysphagia but failto identify 40-58% of patientsaspirating
Up to one third of alert strokepatients with dysphagia diewithin the first six monthsfollowing stroke (comparedwith fewer than 10% of thosewithout dysphagia)
Abnormalities on any of theabove observations shouldlead to immediate referral toa speech and languagetherapist (or other suitablytrained person) for detailedfunctional examination ofswallow
Videofluoroscopy shouldbe considered if:n the risk/benefit ratio of
proceeding with trial food ispoor
n there is doubt about futuremanagement options
n there is need for clarificationof diagnosis
ManagementA documented rehabilitationplan or modified feeding andnutrition plan should be agreedwith and communicated to thepatient, carers, and all membersof the health care team
Catering staff shouldreceive information andtraining to enable them toappreciate the importance ofspecific food consistencies andto produce these with therequired nutritional supplement
The screening test is usually asimple water swallow test
Checks should also be made onconscious level, voiceabnormality, and respiratoryand nutritional status
Nutritional status andfluid intake should bemonitored and recorded
Gastrostomy is recommendedfor appropriate patientsrequiring enteral feeding
C
B
B
CC
B
B
B
B
ScreeningAll stroke patients should bescreened before being givenfood or drink to identify thosepatients with dysphagia
All personnel in contactwith stroke patients in theacute stage should be madeaware of the possibility ofdysphagia
AssessmentPatients presenting with featuresindicating dysphagia and/or riskof aspiration should receivefurther clinical evaluation, e.g.n trial food of differing
consistencyn postural techniquesn swallowing manoeuvresn sensory stimulation
A B C refer to grade of recommendation
S I G N
Management of Patients with StrokeIdentification and Management of Dysphagia
A Quick Reference Guide
Derived from the National Clinical Guideline recommended for use in Scotlandby the Scottish Intercollegiate Guidelines Network (SIGN)