-
7/26/2019 Management of Neuroendocrine Tumors
1/3
Management of Neuroendocrine Tumors: NETs of LungOriginMarianne
Pavel, MD; Piero Ferolla, MD, PhD
Faculty and Disclosures
CME Released: 05/13/2011; Valid for credit through
05/13/2012
CME Information
Download Audio
Download Slides
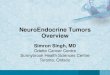
An estimated 25% to 30% of all neuroendocrine tumors (NETs) have
their origin in the bronchialtract and lungs.[1,2]Although lung
NETs account for fewer than 1% of all pulmonary neoplasms,
the incidence of these neoplasms has risen precipitously since
the mid 1970s (Figure).[3]
Figure.Rising incidence of neuroendocrine tumors of the lung
(United States, 1973-2005).From Yao JC, et al. J Clin
Oncol.2008;26(18):3063-3072.[3]
Differential DiagnosisLung NETs vary widely in their pathology,
from low- and intermediate-grade NETs (typical andatypical
carcinoid, respectively) to aggressive and rapidly fatal small cell
lung cancer(SCLC).[1,4]Histologic differentiation of these tumors
can be challenging and is critical to effectivetreatment
(Table).
Table. Neuroendocrine Tumors of the Lung
Tumor Type Diagnostic Criteria
Typical carcinoid < 0.5 cm< 2 mitoses per 2 mm2(10
HPF*)
No necrosis
Carcinoid morphology
Atypical carcinoid 2-10 mitoses per 2 mm2(10 HPF) or necrosis
(punctate)
Carcinoid morphology
Large cell neuroendocrinecarcinoma
11 mitoses per 2 mm2
(10 HPF), median 70 per 2 mm2
(10HPF)Necrosis (large zone)
Neuroendocrine morphology (organoid nesting, palisading,
rosettes, trabeculae)Cytologic features of a non-small cell lung
carcinoma
Small cell carcinoma 11 mitoses per 2 mm2(10 HPF), median 80 per
2 mm2(10
http://www.medscape.org/px/trk.svr/742300?exturl=http://img.medscape.com/images/742/300/NETs_LungOrigin_742300.mp3http://www.medscape.org/px/trk.svr/742300?exturl=http://img.medscape.com/images/742/300/NETs_LungOrigin_742300.mp3http://www.medscape.org/px/trk.svr/742300?exturl=http://img.medscape.com/images/742/300/NETs_Lung-Origin_742300_2.ppthttp://www.medscape.org/px/trk.svr/742300?exturl=http://img.medscape.com/images/742/300/NETs_Lung-Origin_742300_2.ppthttp://www.medscape.org/px/trk.svr/742300?exturl=http://img.medscape.com/images/742/300/NETs_Lung-Origin_742300_2.ppthttp://www.medscape.org/px/trk.svr/742300?exturl=http://img.medscape.com/images/742/300/NETs_LungOrigin_742300.mp3
-
7/26/2019 Management of Neuroendocrine Tumors
2/3
HPF)
Necrosis (large zones)
Scant cytoplasm, finely granular nuclear chromatin, absent
or
faint nucleoli
*10 high-power fields (HPF) in a microscope with field of view
of 0.2 mm 2
From Travis WD.Annals of Oncology. 2010;21(Supplement
7):vii65vii71[2];Bertino EM, etal. Cancer.
2009;115:4434-4441.[4]
Although NETs of the lung arise from cells capable of producing
serotonin andadrenocorticotropin hormone, hypersecretion of
bioactive amines is comparatively rare in typicaland atypical
carcinoids of the lung.[1,4]Symptoms characteristic of carcinoid
lung NETs --including obstructive pneumonia, atelectasis, and
wheezing -- are more commonly the result ofcentral airway
obstruction due to tumor mass.[4]
TreatmentSurgery is the primary treatment for typical and
atypical carcinoid lung NETs. Up to 64% ofpatients with atypical
carcinoid lung NETs present with lymph node metastases, and
5-year
survival ranges from 61% to 88%. In contrast, lymph node
metastases are present in fewer than15% of cases of typical
carcinoid lung NETs, and 5-year survival exceeds 90%.[2]
Lung NETs are typically underrepresented in clinical trials of
NET treatments. In recent years,only a phase 2 retrospective study
of the dacarbazine derivative temozolomide[5]and the phase3 RAD001
in Advanced Neuroendocrine Tumors Trial 2 (RADIANT-2)[6]have
reported resultsspecific to lung NETs. Ekeblad and colleagues
performed a retrospective analysis of 36 patientswith
histologically confirmed metastatic or inoperable malignant NETs
treated with oraltemozolomide (100-200 mg/m2/d for 5 days every 28
days). The study group included 10patients with typical carcinoid
NETs and 3 with atypical carcinoid NETs. After a median follow-up
of 7 months (range, 217 months), 31% of patients with lung
carcinoids had stable diseaseand 31% showed a partial radiologic
response. The most frequently reported adverse event was
grade 1-2 stomachache (N = 6), and 4 patients required dose
reductions due to hematologictoxicity.[5]
In RADIANT-2, which evaluated the impact of combination therapy
with the oral mammaliantarget of rapamycin (mTOR) inhibitor
everolimus and the somatostatin analogue octreotide LARin patients
with advanced NET and carcinoid symptoms, only 6.9% of patients in
theexperimental arm and 2.3% of patients in the control arm were
diagnosed with lung NETs.Patients were randomly assigned to receive
octreotide LAR 30 mg intramuscularly every 28days plus everolimus
10 mg per day (N = 216) or octreotide LAR plus placebo (N =
213).
Although treatment with everolimus plus octreotide was
associated with longer progression-freesurvival overall -- 16.4
months vs 11.3 months in control patients (P= 0.026) -- patients
withlung NETs had more favorable outcomes with octreotide plus
placebo.[6]
SummaryThe role of targeted therapy for typical and atypical
carcinoid lung NETs remains incompletelydefined, with data from
relatively few clinical trials to help guide clinical decision
making. Recentin vitro studies indicate that somatostatin receptors
are overexpressed in metastatic typicalcarcinoid tumors of the
lung[7]and that the mTOR is found in most lung NETs -- with
higherexpression in typical and atypical carcinoids.[8]In addition,
a recent preclinical study of theimpact of the mTOR inhibitor
everolimus found that it suppressed the viability of typical
andatypical carcinoid lung cells in culture.[9]Further research is
needed to clarify the role of
-
7/26/2019 Management of Neuroendocrine Tumors
3/3
somatostatin analogues, mTOR inhibitors, and other targeted
therapies on these diverse andclinically challenging tumors.
In the accompanying discussion, Drs. Marianne Pavel and Piero
Ferolla review a case thatillustrates the challenges inherent in
the management of patients with lung NETs.