Embed Size (px)
Citation preview

Surgical Management Surgical Management of Necrotizing of Necrotizing PancreatitisPancreatitis
James CromieJames Cromie8/16/108/16/10
“The past is only the present become invisible and mute.” -M. Webb

Background: Acute PancreatitisBackground: Acute Pancreatitis
250,000 hospitalizations 250,000 hospitalizations annuallyannually
> 90% cases caused by > 90% cases caused by EtOH or gallstonesEtOH or gallstones
Annual costs > $2 billionAnnual costs > $2 billion
Acute Necrotizing Acute Necrotizing pancreatitis (ANP)pancreatitis (ANP)
1010--20% of cases20% of cases
12% mortality, sterile12% mortality, sterile
30% mortality, infected30% mortality, infected
Hughes, et al.Gastroenterology Clinics of North America 2007; 36(2): 313-23

Necrotizing Necrotizing pancreatitispancreatitis
Two phase disease processTwo phase disease process
Early phase < 14 days: Early phase < 14 days:
hypovolemia,hypovolemia,
Systemic inflammatory responseSystemic inflammatory response
Multiple organ dysfunctionMultiple organ dysfunction
Late phaseLate phase
Septic phase Septic phase –– infected necrosis in 40 infected necrosis in 40 –– 70% of 70% of casescases
–– Nonoperative mortality approaches 100%Nonoperative mortality approaches 100%–– Operative mortality 20 Operative mortality 20 –– 36%36%

HistoryHistory
1652: 1652:
NikolausNikolaus TulpTulp, Dutch anatomist., Dutch anatomist.
First recorded description of necrotizing First recorded description of necrotizing pancreatitis. Postmortem exam on young pancreatitis. Postmortem exam on young man with man with ““apocalyptic attack of apocalyptic attack of abominalabominal painpain””, fatal after 5 days. Pancreas found , fatal after 5 days. Pancreas found to be to be ““rottenrotten””
• Mid-late 19th century• Sporadic surgical case reports uniformly ending in death• 1886: Senn. Animal experiments on necrotizing pancreatitis.
• “… gangrene as one of the diseases of the pancreas which should be treated by operative measures…”
Nikolas Senn

18891889
Reginald Fitz, Professor of Reginald Fitz, Professor of Pathoanatomy at Harvard, Pathoanatomy at Harvard, student of Virchow and Billroth.student of Virchow and Billroth.
First First clinicoclinico--pathologic pathologic classification system.classification system.
Surgery would not benefit patients Surgery would not benefit patients with acute pancreatitis, and with acute pancreatitis, and mortality is not prevented by mortality is not prevented by ““operative meddlingoperative meddling””..
Later admitted that surgical Later admitted that surgical debridement in some severe debridement in some severe cases was beneficialcases was beneficial

1894:1894:
48 y/o obese F, severe pancreatitis48 y/o obese F, severe pancreatitis
Debridement of large pancreatic abscess Debridement of large pancreatic abscess 1 month after onset1 month after onset
Placed iodoform gauzePlaced iodoform gauze--wrapped drains, wrapped drains, with repetitive changes. with repetitive changes.
Discharged 5 months later.Discharged 5 months later.
“In the acute stage, surgical treatment is not recommended, wherein patients have the propensity for cardiovascular collapse. If pancreatic apoplexy occurs, surgical treatment cannot help. Later, when we can prove that a purulent collection is arising from the gland, surgery is indicated.”
Werner Koerte

Early 1900Early 1900’’ss
1927: 1927: SchmiedonSchmiedon, et al., et al.
1278 cases of surgical management for ANP1278 cases of surgical management for ANP
Overall mortality: 51%Overall mortality: 51%
compared to 60% prior to surgical managementcompared to 60% prior to surgical management
Advocated early surgical intervention within days Advocated early surgical intervention within days of onset.of onset.
1929: 1929: ElmanElman (surgical resident)(surgical resident)
Introduced serum amylase assay as a means of Introduced serum amylase assay as a means of diagnosing pancreatitisdiagnosing pancreatitis
Surgical management of pancreatitis became Surgical management of pancreatitis became extremely rare until 1950extremely rare until 1950’’ss
Schmeiden, et al. Surg Gynecol Obstet. 1928; 46:735-51

Late 1900Late 1900’’ss
Extensive resections frequently found to Extensive resections frequently found to have areas of viable tissuehave areas of viable tissue
Evolution of Evolution of necrosectomynecrosectomy –– limited limited debridement, with multiple redebridement, with multiple re-- operationsoperations
Advances in diagnosis and severity Advances in diagnosis and severity assessmentassessment
Smadja, et al. Br J Surg. 1980; 23: 408 - 410

Evaluating severity / prognosisEvaluating severity / prognosis
RansonRanson’’s Criteria for prediction of severe s Criteria for prediction of severe acute pancreatitis acute pancreatitis
At presentation:At presentation:
Age Age > 55yrs> 55yrs
Blood Glucose > 200 mg/dLBlood Glucose > 200 mg/dL
WBCWBC > 16,000/mm3> 16,000/mm3
LDHLDH > 250 U/L> 250 U/L
At 48hrsAt 48hrs
HctHct > 10% decrease> 10% decrease
CalciumCalcium < 8 mg/dL< 8 mg/dL
Base deficitBase deficit > 4 mEq/L> 4 mEq/L
BUNBUN > 5mg/dL increase> 5mg/dL increase
Fluid Fluid sequestsequest.. > 6L> 6L
PaO2 PaO2 < 60 mmHg< 60 mmHg
Score > 3-4 =
Severe pancreatitis
Mortality > 16%
Ranson, et al. Surg Gynecol Obstet. 1974; 139: 69 - 81

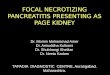
65 M necrotizing pancreatitis.
A= admission
B= 7 days later
C = 14 days later
IV contrast CTIV contrast CT1984: 1984: > 90% diagnostic > 90% diagnostic accuracyaccuracy

Development of current open Development of current open necrosectomynecrosectomy techniquetechnique
Hans Hans BegerBeger, Germany: , Germany:
= 5.1 days from symptomatic onset= 5.1 days from symptomatic onset
Surgery indicated for all patients with CT evidence Surgery indicated for all patients with CT evidence of necrosis, regardless of infectionof necrosis, regardless of infection
Overall mortality 8.1%Overall mortality 8.1%
2005 collective experience;2005 collective experience;
13.1% Mortality in 107 operated patients13.1% Mortality in 107 operated patients
> 25% required re> 25% required re--operative managementoperative management
6.2% mortality in non6.2% mortality in non--operative patientsoperative patients
Beger, et al. World J Surg. 1985; 6: 972 - 979

Necrosis occurs in 10 Necrosis occurs in 10 –– 20% of severe pancreatitis 20% of severe pancreatitis casescases
NonNon--operative mortality approaches 100% operative mortality approaches 100%
Infection arises in 40 Infection arises in 40 –– 70% of cases70% of cases
> 50% necrosis associated with 8x increase rate of > 50% necrosis associated with 8x increase rate of infection.infection.
Infected necrosisInfected necrosis

Open Open NecrosectomyNecrosectomy

Open vs. Closed drainageOpen vs. Closed drainageMethodMethod FistulaFistula HerniaHernia BleedingBleeding AbscessAbscess MortalityMortality
Open Open Packing Packing (n=138)(n=138)
50%50% 32%32% 17%17% 12.7%12.7% 26.8%26.8%
Closed Closed Drainage Drainage (n = 64)(n = 64)
15.6%15.6% ---- 5.7%5.7% 10.7%10.7% 18.8%18.8%
Review of 5 prospective trials using open packing technique vs 2 trials using closed drainage technique, as described by Beger.Heinrich, et al. Annals of Surgery 2006; 243: 154-168

Early vs. Late Early vs. Late NecrosectomyNecrosectomy
Prospective Prospective randomized Study randomized Study 1997:1997:
Early Surgery (48 Early Surgery (48 –– 72 hrs)72 hrs)
N = 25N = 25
56% mortality56% mortality
Delayed surgery Delayed surgery (>12 days)(>12 days)
N = 11N = 11
3 additional pts. 3 additional pts. Avoided surgeryAvoided surgery
27% mortality27% mortality
NecrosectomyNecrosectomy ideally ideally delayed 2delayed 2--4 weeks to 4 weeks to allow demarcationallow demarcation
Mier, et al. Am J Surg. 1997; 173: 71-75
Study terminated early because of OR of 3.39, in favor of delayed necrosectomy

Minimally Invasive TechniquesMinimally Invasive Techniques
Percutaneous drainage / Percutaneous drainage / necrosectomynecrosectomy
EndoscopicEndoscopic
Video Assisted Retroperitoneal Video Assisted Retroperitoneal Debridement Debridement ““VARDVARD””

Percutaneous Drainage / Percutaneous Drainage / NecrosectomyNecrosectomy
1997: First report of percutaneous 1997: First report of percutaneous necrosectomynecrosectomy and drainage for INPand drainage for INP
European International HepatoEuropean International Hepato--pancreatopancreato--biliary Association biliary Association Congress, BolognaCongress, Bologna
RegensbergRegensberg, Germany experience, Germany experience
Retrospective single institution reviewRetrospective single institution review
18 patients between 1992 18 patients between 1992 –– 20042004
Median RansonMedian Ranson’’s at admission: 2s at admission: 2
Median APACHE II : 22Median APACHE II : 22

•30 Fr catheter used for necrosectomy
•56% (10 / 18) patients required surgical debridement
•Overall Mortality 22%
Bruennler, et al. Eur Radiol 2008; 18: 1604 - 1610
Dormia basket: for necrosectomy
Percutaneous Necrosectomy

Percutaneous technique:
• Necrotic cavity defined by contrast
• Necrosectomy performed with Dormia Basket and soft tip catheters
Percutaneous Necrosectomy

FreenyFreeny: aggressive irrigation and drainage alone: aggressive irrigation and drainage alone
29% success in patients with 29% success in patients with centralcentral gland necrosis. gland necrosis.
Mann: use of Mann: use of dormiadormia baskets and continuous lavagebaskets and continuous lavage
EcheniqueEchenique: similar technique. : similar technique.
None had hemodynamic instability preNone had hemodynamic instability pre--procedureprocedure
lesser disease severitylesser disease severity
Mean fistula complication rate: 50%Mean fistula complication rate: 50%
Percutaneous Necrosectomy
Percutaneous Necrosectomy Trials. 1998 - 2001

Endoscopic Endoscopic NecrosectomyNecrosectomy
First reported by Baron et al. 1996First reported by Baron et al. 1996
All retrospective reportsAll retrospective reports
Transgastric or transduodenal drainage catheters placed Transgastric or transduodenal drainage catheters placed nasally, +/nasally, +/-- EUS guidanceEUS guidance
Tract dilated up to 18 Tract dilated up to 18 -- 20 mm20 mm
Require median of 3 Require median of 3 -- 4 procedures4 procedures
Summary of Endoscopic Trials 1996 - 2008

Endoscopic Endoscopic NecrosectomyNecrosectomy
VoermansVoermans, et al. 2007, et al. 2007
25 patients with organized pancreatic necrosis25 patients with organized pancreatic necrosis
EUS guided drainage using EUS guided drainage using cystoenterostomycystoenterostomy or or cystogastrostomycystogastrostomy
93% overall success rate (2/25 needing surgery)93% overall success rate (2/25 needing surgery)
All endoscopic reports demonstrate high success All endoscopic reports demonstrate high success ratesrates
Limitations:Limitations:
Possible only for contiguous walled off pancreatic necrosisPossible only for contiguous walled off pancreatic necrosis
Require high level of expertiseRequire high level of expertise
Transgastric approach may be dangerous, causing continuous Transgastric approach may be dangerous, causing continuous retroperitoneal contamination retroperitoneal contamination
Frequent inadequate debridementFrequent inadequate debridement

Laparoscopic Laparoscopic NecrosectomyNecrosectomy
2008: prospective review of 8 patients with 2008: prospective review of 8 patients with INPINP
Ranson score 2Ranson score 2--44
20 20 -- 90% pancreatic necrosis90% pancreatic necrosis
Preoperative drainage in all patientsPreoperative drainage in all patients
75% underwent prior laparotomy75% underwent prior laparotomy
Laparoscopic Laparoscopic necrosectomynecrosectomy delay:delay:
31 d (13 31 d (13 -- 59 days)59 days)
Procedure indicated in patients with continued Procedure indicated in patients with continued sepsis despite prior laparotomy or percutaneous sepsis despite prior laparotomy or percutaneous drainage.drainage.
0% mortality, 1 patient required repeat laparoscopy0% mortality, 1 patient required repeat laparoscopy
Bucher, et al. Pancreas. 2008; 36: 113-119

Laparoscopic Laparoscopic NecrosectomyNecrosectomy
Critically ill patients may not tolerate Critically ill patients may not tolerate pneumoperitoneumpneumoperitoneum
Risk of infection transmission through Risk of infection transmission through peritoneal cavity or bowel injuryperitoneal cavity or bowel injury
Vast majority of patients had prior drainageVast majority of patients had prior drainage
Poor patient characterization in all studies, Poor patient characterization in all studies, and no description of degree of necrosisand no description of degree of necrosis

Retrospective review of Retrospective review of necrosectomiesnecrosectomies 1997 1997 -- 20032003
•Early and Late outcomes
•88 patients, non-randomized
•Open versus minimally invasive necrosectomy
Connor, et al. Surgery. 2005; 137:499
i

In hospital complications in 88 patients who In hospital complications in 88 patients who underwent pancreatic underwent pancreatic necrosectomynecrosectomy
•Overall mortality: 28%
•In-hospital complication rate: 92%
•Long term complication rate: 62% (of 63 survivals)
•MIPN group: 12 / 47 (26%) required subsequent debridement

Comparison of minimally invasive Comparison of minimally invasive necrosectomynecrosectomy to open to open necrosectomynecrosectomy. .
Comparison of outcomesComparison of outcomes

• Shortcomings of MIPN:
• Inadequacy for pancreatic head or uncinate process necrosis debridement
• Inability to assess for evaluation and treatment of evaluation of coexisting disease

PANTER: 2010 Multicenter randomized PANTER: 2010 Multicenter randomized controlled trialcontrolled trial
Intent to treatIntent to treat
88 patients randomized between 2005 88 patients randomized between 2005 -- 20082008
N = 43. N = 43. ““StepStep--upup”” necrosectomynecrosectomy (primary percutaneous (primary percutaneous drainage followed by MIPN)drainage followed by MIPN)
N = 45. Primary open N = 45. Primary open necrosectomynecrosectomy
Surgery delayed > 4 weeks if possibleSurgery delayed > 4 weeks if possible

Exclusion:Exclusion:Flare up of chronic Flare up of chronic pancreatitispancreatitis
Previous laparotomy during Previous laparotomy during current episodecurrent episode
Previous drainage or Previous drainage or surgerysurgery
Pancreatitis caused by Pancreatitis caused by abdominal surgeryabdominal surgery
Acute intraAcute intra--abdominal abdominal event (ACS)event (ACS)
Combined primary Combined primary endpoint:endpoint:
NewNew--onset MOFonset MOF
EnterocutanousEnterocutanous fistulaefistulae
Visceral perorationVisceral peroration
IntraIntra--abdominal abdominal hemorrhagehemorrhage

•Only major complication significantly lower for Step Up approach is for new onset MOF: 12% vs 42%
•Mortality not significantly different

Health Care UtilizationHealth Care Utilization
Open Open necrosectomynecrosectomy: 40% requiring new : 40% requiring new ICU admissionICU admission
Step UpStep Up :16%:16%
Cost / patient:Cost / patient:Admission, and 6 month follow upAdmission, and 6 month follow up
Step up: Step up: $116,016$116,016
Open Open necrosectomynecrosectomy:: $131,979$131,979

Does not provide direct comparison of Does not provide direct comparison of minimally invasive to open minimally invasive to open necrosectomynecrosectomy
No mortality benefit demonstrated for No mortality benefit demonstrated for minimally invasive procedureminimally invasive procedure

ConclusionsConclusions
Surgery indicated for infected necrotizing pancreatitis Surgery indicated for infected necrotizing pancreatitis or sterile disease not improving over timeor sterile disease not improving over time
Delayed Open Delayed Open necrosectomynecrosectomy with closed drainage with closed drainage remains the standard surgical treatmentremains the standard surgical treatment
Percutaneous drainage / Percutaneous drainage / necrosectomynecrosectomy may reduce may reduce
Endoscopic Endoscopic necrosectomynecrosectomy effective in WOPN, but effective in WOPN, but limited to centers of excellencelimited to centers of excellence
VARD: VARD:
As early nonAs early non--operative management evolves, more operative management evolves, more localized patterns of necrosis are being observed, localized patterns of necrosis are being observed, making minimal access management more feasible.making minimal access management more feasible.














![ABSTRACT NO-145. LEARNING OBJECTIVES To Define acute pancreatitis phases and its types [interstitial edematous and necrotizing] and naming the various](https://img.pdfslide.us/doc/110x75/5697bfd41a28abf838cac83d/abstract-no-145-learning-objectives-to-define-acute-pancreatitis-phases-and.jpg)