Embed Size (px)
Citation preview
Management of Mild Cognitive Impairment (MCI)
Introduction It is estimated that 520% of people over 65 have MCI, with 510% of those converting annually to Dementia, usually Alzheimer's disease1 There are currently no clear and consistent guidelines for dealing with this condition, and practice varies from area to area. Dementia was found in a recent survey to be the most feared diagnosis in over 50s, yet we often currently give patients with a diagnosis of MCI no support, and can increase their anxiety by giving them the diagnosis. Following the Blackfriars consensus2, we now have clear evidence of interventions which reduce the risk of developing dementia. We have clinics, generally nurseled, currently embedded in primary care to monitor other longterm conditions embedded in all practices. We also have the IT support which allows an efficient recall of patients coded as having MCI, although coding remains an issue in the field of dementia. In addition, the message of prevention is consistent with messages already given by our current chronic disease nurses, as "what is good for the heart is good for the brain", and we already give the same message contained in the Blackfriars consensus to current patients with hypertension, CHD and diabetes. In addition, this group of patients is an important cohort for future trials, and having them systematically coded and monitored would have additional benefits in terms of accessibility for such trials. This paper gives recommended guidelines for the management of MCI in primary and secondary care. Background People with a memory or other cognitive complaint where dementia is considered a possible cause may be referred to one of a number of specialists (geriatrician, neurologist, old age psychiatrist), to memory clinics, or diagnosed in Primary Care. The outcomes of the referral include:
Diagnosis of a subtype of dementia Depression, or other nonneurodegenerative cause of cognitive
complaint Cognitive impairment that does not meet criteria for dementia
diagnosis Other possible neurodegenerative disorder that requires further
evaluation No definitive diagnosis, patient to be reviewed Reassurance that nothing is wrong
The groups of people diagnosed with depression or a cognitive impairment that do not meet criteria for dementia are among people at greater risk of
1 JL\SCN_Dementia\MCI\ManagementMCI_V2

developing dementia in future. Within the group that has a cognitive impairment there is a recognized spectrum (see Figure 1): 1. Subjective Memory Complaint: no associated functional deficit or
evidence of cognitive impairment on detailed testing 2. Objective Cognitive Impairment: evidence of cognitive impairment on
detailed testing (subtypes, amnestic, nonamnestic, multi domain), but also NO associated functional deficit. The amnestic and multidomain subtypes are at greatest risk of converting to dementia.
People fulfilling criteria for Group 2 are frequently given a diagnosis of Mild Cognitive Impairment (MCI). This is a clinical diagnosis, and the proportion of those given this diagnosis varies widely in different services. In addition to their cognitive impairment these people may have other factors that increase their risk for converting to dementia:
Age ApoE status (homo or heterozygous for E4) Family History Vascular Index
Conversion from MCI To dementia varies considerably depending on the population considered. A recent metaanalysis of 41 cohort studies suggests that the annual conversion rate is approximately 5–10% and most people with MCI will not progress to dementia even after 10 years of followup (Mitchell 2008). This is an important message to health professionals and people concerned about dementia.
Issues
Concerns have been expressed that attempts to reach the national aspiration of a dementia diagnosis rate of 66.7% may result in inappropriate dementia diagnoses. Preliminary evidence shows that although the percentages vary considerably up to 50% of people referred to Memory Assessment Clinics are given a diagnosis of Mild Cognitive Impairment (MCI). In those clinics with an inappropriately high MCI rate, several factors may play a role:
Assessments in Memory Assessment Services (MAS) are not be properly standardized
Atypical cases of dementia are being misclassified Referrals early in disease where there the person has a concern
about loss of some cognitive abilities without effect on function. There is no agreed pathway, and a poor evidence base, for the review and management of people with MCI or atypical presentations. There is a risk of offering these patients a diagnosis with an uncertain future, no proven intervention, no clear management plan or followup, and a distinct danger of causing more harm than good.
2 JL\SCN_Dementia\MCI\ManagementMCI_V2

Subjective Memory Complaints (SMC), Mild Cognitive Impairment (MCI) and Dementia
Dementia is a clinical diagnosis that should consider all aspects – degree of functional impairment, neuropsychological profile, neuroimaging findings, other relevant data from person or informants. The key feature that differentiates people with SMC and MCI from those with dementia is the lack of association of the memory complaint with functional impairment. Therefore, it seems appropriate that the review of people with SMC and MCI both at the first presentation at a MAS and subsequently either in primary care of in the MAS should include both a cognitive and a functional assessment. Assessments that include a functional component are the GPCOG and the Clinical Dementia Rating scale sum of boxes (CDRSB, see Appendix A). The latter distinguishes MCI from dementia and has been validated as a semistructured telephone interview but not as a selfreport. Whatever assessments are used to assess cognition and function longitudinally the informant must remain consistent. People with SMC or MCI should also be classified according to their individual “risk factors” for conversion to dementia. These include vascular risk factors, age and ApoE4 status (if known).
Diagnosis and Review of People with Subjective Memory Complaints (SMC), Mild Cognitive Impairment (MCI).
A diagnosis of SMC or MCI should only be given after discussion and consideration by the “team” of all available information degree of functional impairment (pt and informant), neuropsychological profile, and appropriate neuroimaging findings. The MAS should then communicate the diagnosis:
Clearly and sensitively to the patient and their family and/or carers, including written information on the diagnosis, implications for the future and beneficial lifestyle measures to take.
Identifying Diagnostic code(s) to be used (CTV codes or equivalent to be agreed) in primary care: Mild cognitive impairment Read code 28E0. Other Read codes
include Very Mild Cognitive Decline 3AE1 and Mild Cognitive Decline 3AE2
With a timeframe for review and guidance on how that review should be done and where.
With a risk category (high or low) for conversion to dementia
Protocol for managing MCI in primary care 1 Patients given a diagnosis of MCI by the local memory clinic should be appropriately coded 28E0 in the GPs computer system. MCI is not a diagnosis that should be made by the GP.
3 JL\SCN_Dementia\MCI\ManagementMCI_V2

2 If not followed up by memory clinics, they should be invited to annual clinics with the practice nurses who currently run chronic disease clinics. They would have blood pressure and BMI measured, smoking, drinking and exercise recorded, and blood tests including fasting glucose, lipid profile and renal function. (This is in line with current practice for other chronic diseases, and many would overlap and already be under review) 3 Where appropriate they would receive advice on exercise, smoking, diet and alcohol use in line with the Blackfriars consensus. In addition, they would be asked "do you feel your memory has improved, stayed stable or deteriorated in the last year". If the latter, or they drop by a point in their GPcog, they would be referred back to the memory clinic for standardised retesting and appropriate action. As a highly motivated group, lifestyle advice is more likely to be heeded. 4 Clinic nurses would not need additional training, as they would not themselves carry out a memory test. However it would be useful to supply them with documentation giving them basic information on dementia to respond to patient enquiries. 5 This programme would need to be costed, but is likely to be relatively small as it piggybacks an existing service. It represents an additional workload on primary care, and should be remunerated accordingly. The programme should be funded by CCG’s as there are likely to be savings in other areas: by prompt recognition of dementia, a likely small reduction in conversion rates, and from memory service time in areas where they currently follow up MCI. However the primary motivation is quality of life, not economic. At worst, this approach would identify an at risk population for research, provide support for a group often felt abandoned, and would do no harm. At best, it could delay progression to frank dementia, and enable early diagnosis in this high risk group, and could provide savings both financially and in terms of reduced distress. Recent CFAS data shows that interventions are reducing the predicted increase in dementia by 20%; a properly evidenced and consistent approach to MCI could make further advances in reducing the burden of this uniquely distressing chronic disease
Other Points
Evaluation and Review in Clinics It should be a standard practice in all MAS clinics that there is concordance between staff in cognitive and functional assessments.
4 JL\SCN_Dementia\MCI\ManagementMCI_V2

Neuroimaging outcomes should be reviewed by suitably qualified personnel who have access to all relevant information.
Monitoring of Referrals and Outcomes All clinics where people are referred for evaluation of cognitive impairment should provide data about number or referrals, and outcome. Ideally there should be an agreed uniform definition for MCI against which clinics could be audited. In the absence of such a definition each clinic should define clearly their criteria for MCI that includes high and low risk for conversion and for diagnosis of dementia. This should be the basis for decisionmaking about diagnosis (MCI, dementia or other possibilities) and recommendations for followup. Outliers for diagnostic categories from accepted criteria should be scrutinized for the reason for their results.
Recommendations:
1. The communication to Primary care about the outcome of referrals to a MAS should include: For people with dementia:
Dementia subtype diagnostic code (READ / CTV) Advice about followup, treatment (including involvement in
postdiagnosis group interventions) and whether referred to local dementia support/adviser service.
For people with SMC or MCI Diagnostic code Risk categorization for conversion Guidance about longitudinal assessment of cognition and function Advice about nonpharmacological interventions and lifestyle
Atypical cases: Information about next steps
2. MAS should: Ensure concordance between staff for cognitive and functional
assessments Ensure all relevant data are considered when making a diagnosis Either review nondementia diagnoses regularly or hold a “team
meeting” to agree classification of SMC / MCI and risk for conversion Provide data about the outcome of referrals that includes percentages
of dementia, SMC and MCI diagnoses 3. Commissioners need to ensure that pathways and service specifications
for the evaluation of people with cognitive impairment include provision for: Atypical cases that are likely to require neurologist/ subspecialist
review and specialist investigations. Evidencebased nonpharmacological interventions for SMC and MCI
5 JL\SCN_Dementia\MCI\ManagementMCI_V2

Prepared by Dr Jill Rasmussen RCGP Clinical Champion Dementia, SCN SE Coast Clinical Lead Dementia Dr Christopher Kipps Consultant Neurologist & Honorary Clinical Lecturer University Hospital Southampton NHS Foundation Trust Dr Nick Cartmell SCN SW Clinical Lead Dementia Dr Peter Bagshaw SCN SW Clinical Lead Dementia, National Expert Panel, CCGIAF
References:
1. Alzheimer's society, 2016
2. http://nhfshare.heartforum.org.uk/RMAssets/Reports/Blackfriars%20consensus%20%20_V18.pdf
3. Mitchell et al. Acta Psychiatr Scand 2009: 119: 252–265. Rate of
progression of mild cognitive impairment to dementia – metaanalysis of 41 robust inception cohort studies.
4. O’Bryant et al. Arch Neurol. 2010;67(6):746749. Validation of the New Interpretive Guidelines for the Clinical Dementia Rating Scale Sum of Boxes Score in the National Alzheimer’s Coordinating Center Database
6 JL\SCN_Dementia\MCI\ManagementMCI_V2
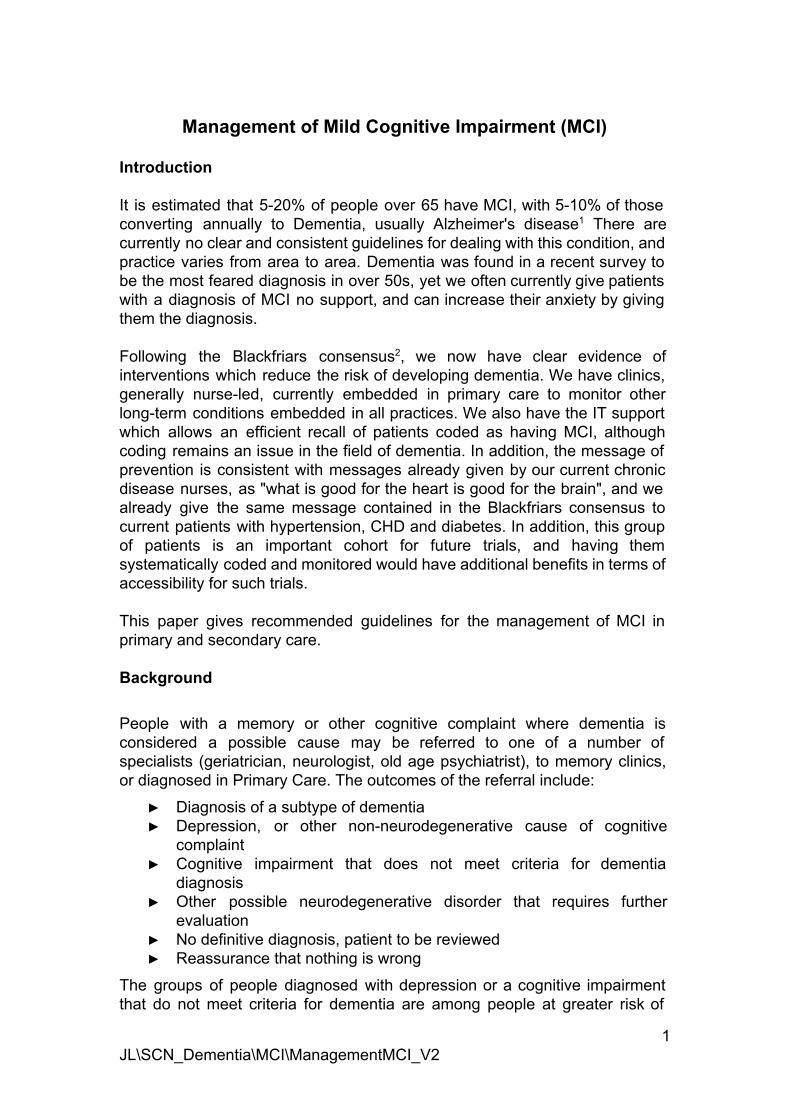
Appendix A: Additional notes 1. Mild Cognitive Impairment Definitions. At both the MCI and dementia stages the NIAAA diagnostic framework provides different levels of probabilistic likelihood (high, intermediate or unlikely) that the syndrome is due to Alzheimer’s disease based on biomarker information. The NIAAA criteria have the advantage of being applicable when no supportive biomarkers are available, albeit at the expense of diagnostic specificity. The International Working Group (IWG) criteria are less complex in their semiology, have the advantage of consistency, and are more readily applicable in clinical trials and in clinical diagnosis when biomarkers are available. Refs: 1. Dubois Lancet 2010, 2. Dubois Lancet Neurology 2010. 2. Criteria for MCI
NIAAA criteria for MCI Ref Albert, Alz & Dem, 2011
** Note a range of MCI cognitive performance tests are specified in this article
NIAAA criteria for MCI including biomarker information
Ref: Albert, Alz & Dem, 2011)
7 JL\SCN_Dementia\MCI\ManagementMCI_V2

3. Risk Factors for Conversion to Dementia
Rotterdam Study In the Rotterdam study (Ref de Bruijn)) increased risk for MCI was associated with:
older age positive APOEɛ4 status low total cholesterol levels stroke specific MRI correlates of cerebrovascular disease.
Participants diagnosed with MCI had a 4fold increased risk of developing dementia or Alzheimer disease (AD) compared to cognitively healthy individuals. The risk of dementia and AD was particularly high for those with amnestic MCI and participants with MCI also had a somewhat higher risk of death. Ref: de Bruijn RFAG, Akoudad S, Cremers LGM, et al. Determinants, MRI correlates, and prognosis of mild cognitive impairment: the Rotterdam Study. J Alzheimers Dis. 2014;42(Suppl 3) DOI:10.3233/JAD132558
The association of angiotensinconverting enzyme with biomarkers for Alzheimer’s disease A link has been proposed between inheritance of a specific allele associated with low plasma angiotensinconverting enzyme (ACE) and increased risk of AD. What is known is that ACE in the central nervous system degrades amyloid beta (Aβ), the plaqueforming protein associated with AD, and that administration of ACE inhibitors promotes accumulation of Aβ. ACE inhibitor therapy may not be the right choice for some patients with hypertension. If ACE in the human brain prevents Aβ accumulation then the results support the suggestion that administering ACE inhibitors as antihypertensive agents might compromise this protective effect. Angiotensinreceptor blockers may be an alternate choice for patients at risk for AD. Ref: Jochemsen. Alzheimer's Res & Ther. 2014;6:27
Vitamin D Recent metaanalyses confirm that low serum vitamin D concentrations are associated with prevalent Alzheimer disease (AD) dementia and cognitive impairment. This is cause for concern given the high rates of vitamin D deficiency in older adults and continued uncertainty about the causes of AD and other forms of dementia. The findings support the hypothesis that vitamin D may be neuroprotective and that “sufficiency” in the context of dementia risk may be in the region of 50 nmol/L. Ref: Littlejohns Amer Academy of Neurology Aug 2014.
8 JL\SCN_Dementia\MCI\ManagementMCI_V2

Appendix B
General practitioner assessment of cognition (GPCOG) The GPCOG is a reliable, valid and efficient tool to use to screen for dementia in primary care settings for people with carers. It takes less than four minutes to carry out the patient assessment and two minutes to interview the carer. There is some evidence that interviewing both carers and patients improves accuracy. The GPCOG is not influenced by someone’s cultural and linguistic background, making it useful in multicultural patient settings. Guidance and further information: www.gpcog.com.au/info.php#3
9 JL\SCN_Dementia\MCI\ManagementMCI_V2

Clinical Dementia Rating Scale Sum of Boxes (CDRSB) A recent article about the validation of the “New Interpretive Guidelines for the Clinical Dementia Rating Scale Sum of Boxes Score’ (Ref O’bryant 2010) shows there is a 3fold increase (odds ratio, 3.32) in the likelihood of being diagnosed with some form of dementia with every 1point increase in CDRSB score. These findings supports the use of CDRSB as an important tool in distinguishing MCI from early dementia as well as its utility in tracking progression from MCI to dementia. Further it is likely that the combination of CDRSB together with a cognitive screening instrument will improve diagnostic accuracy.
CDRSB Range Staging Category 0 Normal 0.5 4.0 Questionable cognitive impairment
0.5 2.0 Questionable impairment 2.5 4.0 Very mild dementia
4.5 9.0 Mild dementia 9.5 15.5 Moderate dementia 16.0 18.0 Severe dementia
10 JL\SCN_Dementia\MCI\ManagementMCI_V2

11 JL\SCN_Dementia\MCI\ManagementMCI_V2
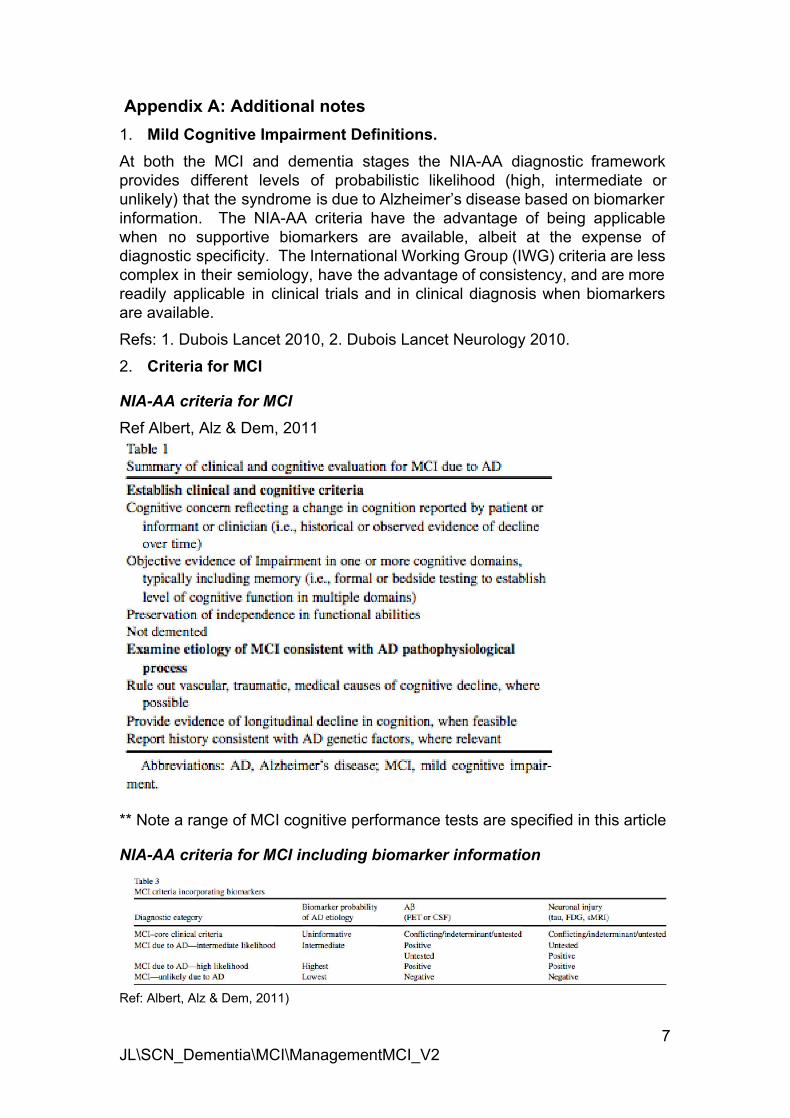
Brief Dementia Screening Indicator for Primary Care
ref Barnes Alzheimer’s & Dementia 10 (2014) 656–665
12 JL\SCN_Dementia\MCI\ManagementMCI_V2



![Small-World Properties in Mild Cognitive Impairment and ...downloads.hindawi.com/journals/isrn.geriatrics/2013/542080.pdf · incidence rate of MCI [23]) have identified certain brain](https://img.pdfslide.us/doc/110x75/60604afe479a8d5cb4737a54/small-world-properties-in-mild-cognitive-impairment-and-incidence-rate-of-mci.jpg)