Embed Size (px)
Citation preview

Management of Hypertensionafter SPRINT
Richard J. Glassock, MD, MACP
Professor Emeritus
Geffen School of Medicine at UCLA

Richard J. Glassock, MD, MACP, FRCP (Hon), FASN
◼ Dr. Glassock is currently Professor Emeritus at the Geffen School of Medicine at UCLA. He has had a long standing interest in clinical nephrology (glomerular diseases) and hypertension and has published over 750 papers, books chapters and monographs. He is a former President of the ASN and NKF

DISCLOSURES
◼ Nothing to Disclose

CASE and QUESTION
◼ An 83 year old woman is referred to you for advice concerning blood pressure control. She is active and has no symptoms, other than a painful hip from osteoarthritis. She is a life long non-smoker. Her BP taken in the office by the nurse using an anaeroidsphygmomanometer is 144/60mmHg, pulse 72 and regular. Other than cataracts and dry skin her examination is unremarkable. Her BMI is 24Kg/m2. The blood sugar (fasting) is 90mg/dL and a Hemoglobin A1c is 5.1%. A serum creatinine is 1.08mg/dL (eGFR= 55ml/min/1.73m2) and a urinalysis is negative for blood and protein (dipstick). The LDL-C is 96mg/dL and the HDL-C is 60mg/dL

CASE AND QUESTION
◼ Which ONE of the following would you now recommend?
A. Start a thiazide diuretic
B. Start an angiotensin receptor inhibitor
C. Initiate a DASH- style diet
D. Start a Beta-adrenergic blocker

OUTLINE
◼ Part I- Description of SPRINT
◼ Part II- Initial Guidelines built on SPRINT (AHA/ACC- 2017)
◼ Part III- Post-Hoc SPRINT Studies
◼ Part IV- Recent Guidelines based on Sprint (ISH- 2020; KDIGO- 2021)

PART I-
SPRINT 2015-2021:The gift that keeps on giving!


BP Measurement in SPRINT
◼ Mean of 3 measurements in office, seated position after 5 minutes of quite rest by an automated oscillo-metric system* (physician/or nurse not required to be present)
*Omron Healthcare (model 907)

AUTOMATED DEVICE (Omron-Model 907)

SPRINT
Primary End Point=
Composite of Myocardial Infarction, Acute Coronary Syndrome, Stroke, Congestive Heart Failure, or Death
from CVD (not a renal end point study!)


SPRINT(NEJM; November, 2015)
◼ 9361 patients Randomized (4678-Intensive; 4683-Standard)
◼ Non-Diabetic ; 91% already on anti-hypertensive treatment- mainly RASi
◼ CKD – 28% (eGFR >20ml/min/1.73m2; uPER <1gm/d; average uACR- 43mg/gm)
◼ Non-Hispanic Black- 30%
◼ Average Age- 68 years (28% ≥ 75 years)
◼ Pre-existing CVD- 22% (high risk population)
◼ Follow-Up -3.26 years- Stopped prematurely for Efficacy



SPRINT:Primary and Secondary Outcomes
Intensive(n=4678)
Standard(n=4683)
Hazard Ratio
Primary Composite Outcome
1.65%/yr 2.19%/yr 0.75 (p<0.001)
Myocardial Infarction
0.65%/yr 0.78%/yr 0.83 (ns)
Acute Coronary Syndrome
0.27%/yr 0.27%/yr 0.99 (ns)
Stroke 0.41%/yr 0.47%/yr 0.89 (ns)
Congestive Heart Failure 0.41%/yr 0.67%/yr 0.62 (p=0.002)
CVD Death 0.25%/yr 0.43%/yr 0.57 (p=0.003)
All Cause Death 1.03%/yr 1.40%/yr 0.78 (p<0.001)

SPRINT
Renal Outcomes-
For patients with CKD at baseline (n=2646)- first occurrence of
reduction of eGFR by 50% or more from BL, Dialysis or Transplantation

SPRINT:Renal Outcomes-
in patients with CKD at BL
Intensive (n=1330)
Standard(n =1316)
Hazard Ratio
Composite Renal Outcome
0.33%/yr 0.36%/yr 0.89 (ns)
≥50% decline in eGFR
0.23%/yr 0.26%/yr 0.87 (ns)
Dialysis 0.14%/yr 0.24%/yr 0.57 (ns)
Transplantation 0 0 NA
New OnsetAlbuminuria
3.02%/yr 3.90%/yr 0.72 (ns)

SPRINTRenal Outcomes-
in Patients without CKD at BL
Intensive(n=3332)
Standard(n=3345)
Hazard Ratio
≥30% decline in eGFR to <60ml/min/1.73m2
1.21%/yr 0.35%/yr 3.49 (p<0.001)
New onset albuminuria
2.00%/yr 2.41%/yr 0.81 (ns)


SPRINT:Main Conclusions-I
◼ In elderly, non-diabetic subjects, without a prior history of Stroke but with increased CVD risk, intensive BP lowering improves CV and mortality outcomes, at least for up to 3.2 years
◼ In a subgroup analysis (hypothesis generating) no benefits were seen for the primary composite CV outcome in subjects with CKD at BL (?underpowered)

◼ No benefit observed on CKD progression in patients with CKD at BL and a potential harmful effect on eGFR seen in those without CKD at baseline. No clear effects on albuminuria was observed
◼ Adverse events (hypotension, electrolyte abnormalities [hyperkalemia] and AKI) were “common” in the intensive arm
SPRINT:Main Conclusions-II

PART II-Translating SPRINT into
Practice (Guidelines)

ACC/AHA* Guideline for Prevention, Detection, Evaluation and Management of High Blood
Pressure in Adults (Whelton P, et al- 481 pages-Synopsis JAMA,
November 2017)
(ACC, AHA, AAPA, ABC, ACPM, AGS/APHA, ASH, ASPC, NMA/PCNA- No ASN, KDIGO, NKF, ACP or AAFP
participation in development- Consensus Driven)

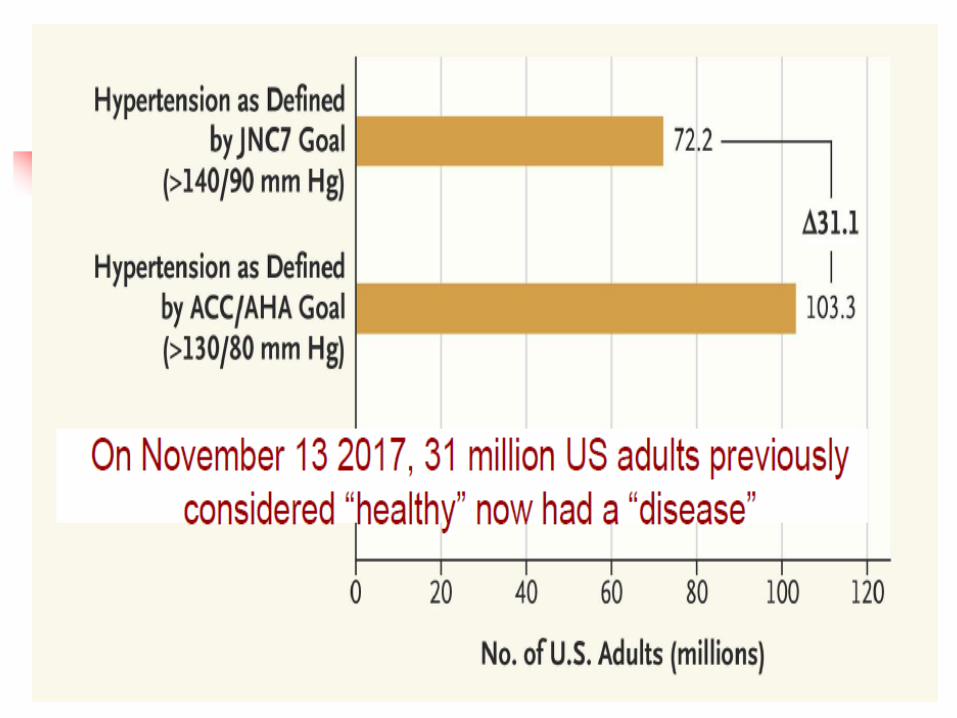

Of 31 million “new” hypertensives the great majority will be
diagnosed and managed by PCP- 27million by lifestyle modifications
and 4 million by drugs

BP Measurement and Diagnosis of Hypertension
◼ Out-of-office measurement of BP using Automated (calibrated) devices (arm cuff preferred) is recommended for diagnosis and titration of therapy (evidence level high)-observed in office BP overestimates automated SBP by about 10mmHg
◼ Ambulatory BP monitoring required for accurate classification of subtypes


Non-Pharmacologic Treatment of Hypertension
(“Life Style Modifications”)
Modification SBP Effect
in Hypertensives (mmHg)
Weight Loss -5
Heathy Diet (DASH) -11
Reduced NaCl (<3.5gms/d) -5
Increased K (3.5-5gm/d) -5
Exercise (Aerobic,Dynamic
Resistance or Isometric) -4/-8
Reduced Alcohol -4



Impact of SBP Control on Incident CKD with and without Diabetes:
ACCORD and SPRINT(Beddhu S, et al. Lancet Diab Endo, April, 2018; 3 yr FU)
Intensive Standard AbsoluteDifference
ACCORD (Diabetes)
10.0% 4.1% +5.9%
SPRINT (No Diabetes)
3.5% 1.0% +1.5%


AHA/ACC Guidelines:Caveats
◼ Not endorsed by ACP or AAFP (yet)
◼ Not applicable to practices using Office Based non-automated BP measurements
◼ Largely based on Expert Opinion and Consensus
◼ Ignores dangers of DBP <60-65mmHg in DM and CVD
◼ In very low-risk subjects <140/90mmHg is a “reasonable” target
◼ Do not apply to eGFR <20-30ml/min/1.73m2 (CKD Category 4/5/5D)
◼ Creates 31 Million new “hypertensives” (in the USA)-$Billions of added costs and burden to PCP
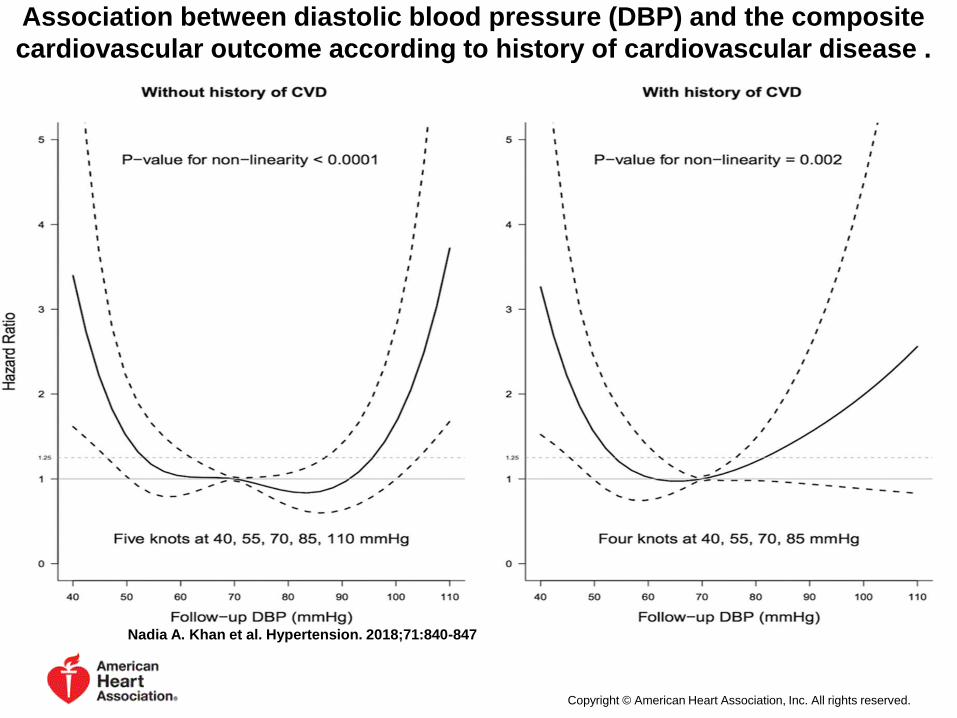
Association between diastolic blood pressure (DBP) and the composite
cardiovascular outcome according to history of cardiovascular disease .
Nadia A. Khan et al. Hypertension. 2018;71:840-847
Copyright © American Heart Association, Inc. All rights reserved.

Part III-Post-Hoc SPRINT Studies

POST-HOC SPRINT STUDIES(all hypothesis generating)
◼ SPRINT-MIND (JAMA,2019)- Intensive BP control reduces onset of Mild Cognitive
Impairment but not Probable Dementia
◼ SPRINT-HEART (Am J Hypertension, 2019)-both intensive and standard BP
control reduce LVM equally
◼ SPRINT DBP- (J Clin Hypertension, 2019)- a level of 60-70mmHg DBP is safe
◼ SPRINT CVD in CKD- (JASN, 2019)- reduced Risk of CVD not attenuated by a decline
of eGFR >20% (10.3% in intensive vs 4.4% in standard BP control)
◼ CKD- (AASK,MDRD,ACCORD, SPRINT-Hypertension, 2019)- CKD with
eGFR>60 and no intensive glycemic control associated with reduced ACM risk
◼ ALBUMINURIA as a modifying factor (CJASN, 2020)- albuminuria did not modify
the beneficial effects of intensive SBP control on CVD events
◼ ORTHOSTATIC HYPOTENSION-(Hypertension, 2020) orthostatic hypotension
was not associated with a higher risk of CV events

SPRINT-Albuminuria and CVD outcomes
(Chang A, et al CJASN, 2020)

SPRINT-Orthostatic Hypotension
(Juraschek SP, et al Hypertension 2020; 75:660-667)

PART IV-Recent Guidelines

International Society of Hypertension (ISH)-
(Unger T, et al. Hypertension 2020; 75:1334-1357
◼ Normal SBP= <130mmHg; DBP= <85mmHg; High-normal BP= 130-139mmHg; DBP= 85-89mmHg; Hypertension=SBP≥ 140 mmHg and or DBP≥ 90mmHg- confirmed X2-3
◼ Office Based BP measurement; quiet room, seated 3-5 min, no smoking, caffeine or exercise; automated oscillo-metric (calibrated) upper arm device preferred
◼ 3 measurements, last 2 averaged

Hypertension and CKD-(ISH- 2020)
◼ BP should be lowered if ≥ 140/90mmHg and treated to a target of <130/80mmHg, in both Diabetic and non-Diabetic subjects (<140/90mmHg in elderly subjects)
◼ RASi first-line agents. CCB and diuretics can be added. Loop diuretics preferred if eGFR <30ml/min/1.73m2

KDIGO Practice Guidelines for Management of Blood Pressure in CKD
(KDIGO- 2021; KI Supplements 99:#35; s1-s85; abbreviated summary)
◼ “Standardized” office BP measurement
recommended: ➢ Sitting, feet on floor, “relaxed” for 5 minutes
➢ Empty bladder
➢ No talking
➢ Clothing on upper arm removed
➢ Calibrated oscillo-metric device preferred; but calibrated auscultatory (Korotkoff sounds), anaeroid device acceptable
➢ Cuff size appropriate to arm circumference
➢ At first visit, measure BP in both arms; use highest value
➢ Average of ≥2 readings on ≥2 visits

KDIGO Practice Guidelines for Management of Blood Pressure in CKD (2021)
(KDIGO- KI Supplements 99:#35; s1-s85; abbreviated summary)
◼ Suggests that out-of-office BP measurements (Either ambulatory or home monitoring) be used to complement standardized office-based BP readings for management (2B).
◼ Patients should be classified as White Coat Hypertension, Masked Hypertension, Sustained Hypertensioin or Normotension based on the office and out-of-office recordings.

KDIGO Practice Guidelines for Management of Blood Pressure in CKD (2021)
(KDIGO- KI Supplements 99:#35; s1-s85; abbreviated summary)
◼ Suggests that adult subjects (age above 18 years) with high BP (SBP=≥130mmHg ) be treated to a target SBP of <120mmHg, when tolerated using standardized office BP measurement (2B)
◼ This suggestion is not dependent on etiology of CKD. Except patients with ADPCKD who may derive benefits of SBP <120mmHg

KDIGO-CKD-Uncertainties concerning the balance of
benefits and harms
◼ Applicability to CKD Categories G4/G5 (G5D)
◼ Diabetic vs Non-Diabetic CKD
◼ Patients with SBP of 120-129mmHG
◼ Patients with very low DBP (<50mmHg)
◼ Etiology of CKD not important; except ADPCKD who may derive renal benefits at SBP of 95-110mmHg
◼ Older age, frailty
◼ Patients at low risk of CVD
◼ “White –Coat” hypertension; Multi-drug resistant Hypertension
◼ Severe hypertension (SBP ≥180mmHg)

KDIGO- CKDTreatment modalities
◼ RASi strongly preferred for non-diabetic subjects with G1-4/A3 CKD (1B)
◼ RASi strongly preferred for Diabetic subjects with G1-4/A2 or A3 CKD (1B)
◼ RASi weakly preferred for non- diabetic subjects with G1-4/A2 (2C)

CASE and QUESTION
◼ An 87 year old woman is referred to you for advice concerning blood pressure control. She is active and has no symptoms. Her BP taken in the office by a nurse is 142/60mmHg, pulse 72 and regular. Other than cataracts and dry skin her examination is unremarkable. Her BMI is 24Kg/m2. The blood sugar (fasting) is 95mg/dL and a Hemoglobin A1c is 5.1%. A serum creatinine is 1.08mg/dL (eGFR by CKD-EPI= 55ml/min/1.73m2) and a urinalysis is negative for blood and protein (dipstick). The LDL-C is 96mg/dL and the HDL-C is 60mg/dL

CASE AND QUESTION
◼ Which ONE of the following would you now recommend?
A. Start a thiazide diuretic
B. Start an angiotensin receptor inhibitor
C. Initiate a DASH- style diet
D. Start a Beta-adrenergic blocker
The correct answer (in my opinion) is C

References◼ SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, et al. A Randomized
Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373:2103-16
◼ Whelton PK,2, Carey RM. The 2017 Clinical Practice Guideline for High Blood Pressure. JAMA. 2017;318:2073-2074.
◼ Whelton PK, Williams B. The 2018 European Society of Cardiology/European Society of Hypertension and 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines: More Similar Than Different. JAMA. 2018;320:1749-1750.
◼ Chang AR, et al Effects of intensive blood pressure control in patients with and without albuminuria. CJASN 2020; 15
◼ Unger T, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020; 75: 1334-1357
◼ KDIGO 2021 Clinical Practice Guidelines for Management of Blood Pressure in Chronic Kidney Disease. Kidney Int Supplements. 2021; 35: s1-s85





























