Embed Size (px)
Citation preview

Management of Hemolytic Anemia
Following
Allogeneic Stem Cell Transplantation
Andreas Holbro
Swisstransfusion
August 25-26, 2016
Bern, CH

Conditioning
Drug-induced hemolytic anemia (DIHA)
d0
HSCT
Acute hemolysis
Passenger lymphocyte syndrome
Pure red cell aplasia
TA-TMA
AIHA
Transfusion support
D/R ABO-incompatibility:
Diseases
t
Hemolytic Anemia in the context of HCT
Others: relapse, Infections, PTLD, ...
Donor issues

Conditioning
Drug-induced hemolytic anemia (DIHA)
d0
HSCT
Acute hemolysis
Passenger lymphocyte syndrome
Pure red cell aplasia
TA-TMA
AIHA
Transfusion support
D/R ABO-incompatibility:
Diseases
t
Hemolytic Anemia in the context of HCT
Others: relapse, Infections, PTLD, ...
Donor issues

• Knowledge of patient‘s and transfusion history, transplant procedure
• Blood count, reticulocytes, blood smear
• Blood chemistry (LDH, bilirubin, haptoglobin)
• Immunohematological investigations:
- Direct antiglobulin test (DAT)
- Elution
- Adsorption techniques
- Isoagglutinin titering
Diagnostic Workup

• Close collaboration between clinicians, stem cell processing facility and transfusion specialists
• Supportive care:
- Transfusions: according to guidelines/SOP
- Leukocyte-reduced RBC
- γ-irradiated (25-30 Gy) RBC
• Modification of immunosuppression has to be balanced against an increased risk of GVHD and/or relapse
General Considerations for Management
Kopolovic I et al. Blood 2015; Treleaven J et al. BJH 2010

Conditioning
Drug-induced hemolytic anemia (DIHA)
d0
HSCT
Acute hemolysis
Passenger lymphocyte syndrome
Pure red cell aplasia
TA-TMA
AIHA
Transfusion support
D/R ABO-incompatibility:
Diseases
t
D/R ABO-Incompatibility
Others: relapse, Infections, PTLD, ...
Donor issues

D/R ABO-Incompatibility
• Human leukocyte antigens (HLA) genes are located on chromosome 6 (6p21)
• Genes encoding transferases for ABO blood groups are located on chromosome 9 (9q34)
• Independent inheritance of HLA genes and ABO blood groups
• ABO-incompatible HCT occurs in 30-50% of patients
Booth GS et al. BBMT 2013

D/R ABO-Incompatibility
• ABO-incompatibility is not a barrier to HCT but increases the complexity of the procedure
• (Probably) no effect on major transplant outcomes (engraftment, graft failure, GVHD, relapse, TRM, OS)
• Heterogeneous studies: registry studies, retrospective/single center studies
Rowley SD et al. BMT 2011; Seebach JD et al. BBMT 2005; Worel N. Transfus Med Hemother 2016

D/R ABO-Incompatibility
• Major ABO-Incompatibility (20-25%):
• Minor ABO-Incompatibility (20-25%):
• Bidirectional ABO-Incompatibility (3-5%)
Donor Recipient
Donor Recipient
Gajewski JL et al. Blood 2007; Rowley SD et al. BMT 2011; Booth GS et al. BBMT 2013 Daniel-Johnson J et al. Transfusion 2011

Major D/R ABO-Incompatibility
• Acute hemolysis of donor RBC
- Graft source: HPC(M) > HPC(A)/HPC(C)
- Prevention:
- RBC depletion of the graft (apheresis, sedimentation)
- Reduction of isoagglutinins in the recipient
- Hydration, monitoring for acute hemolytic reactions
Sorg N et al. Transfusion 2015; Curley C et al. Transfusion 2012; Stüssi G et al. Haematologica 2009; Schwartz J et al. J Clin Apher 2016; HPC=Hematopoietic progenitor cells
Donor Recipient

Major D/R ABO-Incompatibility
• Delayed RBC engraftment, increased transfusion requirement
• Pure red cell aplasia (PRCA):
- Reticulocytopenia >60 days, absent erythroid precursors in the marrow in a recipient who has otherwise engrafted
- Ongoing isoagglutinin production by persistent recipient plasma cells
- Hemolysis of donor RBC and inhibition of donor erythropoiesis (destruction of erythroid progenitors)
Worel N et a. Transfusion 2000; Rowley SD et al. BMT 2011; Griffith LM et al. BJH 2005; Blacklock HA et al. BJH 1984; Bolan CD et al. Blood 2001
Donor Recipient

Major D/R ABO-Incompatibility
• Pure red cell aplasia (PRCA)
- Incidence: 5-(50)%, risk factors: age, donor blood group A, conditioning (RIC > MAC)
- Management:
- Transfusions (donor and recipient compatible RBCs)
- Immunomodulation:
- Reduction of immunosuppression (graft versus plasma cell effect), donor lymphocyte infusions
- Reduction of isoagglutinins: plasma exchange or rituximab*
Bavaro P et al. BJH 1999; Sora F et al. Transfusion 2005; Mielcarek M et al. Blood 2000; * off-label drug use
Donor Recipient

• Acute hemolysis: donor plasma with high isoagglutinin titers or recipients with small blood volume
- Plasma reduction
- Hydration, monitoring for acute hemolytic reactions
Donor Recipient
Minor D/R ABO-Incompatibility
Fung MK et al. AABB Technical Manual 2014

• Passenger lymphocyte syndrome: viable „passenger“ lymphocytes in the graft secrete anti-host isoagglutinins
- Delayed transfusion reaction 5-15 days after HCT
- Incidence: 10-15% of minor ABO-incompatible HCT
- Risk factors: HPC(A) > HPC (M), D/R: O/A, CYA alone as
GVHD prophylaxis, RIC > MAC
- DAT +, donor-derived isoagglutinins, positive eluate against recipient‘s blood group
Donor Recipient
Minor D/R ABO-Incompatibility
Bolan CD et al. BJH 2001

• Passenger lymphocyte syndrome
- Prevention/Management:
- Beginning pre HCT to dilute recipient‘s RBC < 30%:
- Transfusions (blood group O)
- RBC exchange
- Monitoring for delayed hemolytic reactions
- Hydration, preservation of kidney function, transfusions
Donor Recipient
Minor D/R ABO-Incompatibility
Worel N et al. Transfusion 2007; Schwartz J et al. J Clin Apher 2016

• Less frequent, as donors and recipients lack „naturally“ formed antibodies against non-ABO RBC antigens
• Anti-D alloimmunization after D-mismatched HCT and development of other new non-ABO RBC alloantibodies is rare
• Involved systems: Rhesus/Kell/Kidd/Duffy/MNSs/Lewis
• Delayed hemolytic anemia or passenger lymphocyte syndrome (2-9%)
• Antibodies against third party antigens (transfused RBC)
Non-ABO D/R RBC-Incompatibility
Franchini M et al. BMT 1998; de la Rubia J et al. Transfusion 2001; Young PP et al. BMT 2001; Cid J et al. Transfusion 2006

• Platelet transfusions: platelet components contain plasma and thus isoagglutinins
• Platelets express ABO blood groups
• Plasma: transfusion of both donor- and recipient-compatible plasma
• IVIG may cause hemolysis
• Consider always potential transfusion errors
Platelet/Plasma Transfusion and...
Bonilla FA Clin Exp Immunol 2014

Transfusions
Gajewski JL et al. Blood 2008; Worel N et al. Vox Sang 2011; Booth GS et al. BBMT 2013

Conditioning
Drug-induced hemolytic anemia (DIHA)
d0
HSCT
Acute hemolysis
Passenger lymphocyte syndrome
Pure red cell aplasia
TA-TMA
AIHA
Transfusion support
D/R ABO-incompatibility:
Diseases
t
Transplantation-Associated Thrombotic Microangiopathy
Others: relapse, Infections, PTLD, ...
Donor issues

• TA-TMA is a severe complication after HCT associated with long-term morbidity, chronic organ injury and high mortality
• Incidence: 10-35%
• The pathogenesis of this multi-system disorder is unknown
• Various triggers (including chemotherapy, irradiation, immunosuppressive agents, GVHD, infections) cause endothelial injury leading to organ damage
• Increasing evidence of dysregulation/activation of the complement system (≈aHUS)
• Role of complement gene variants (genes & environment)
Transplantation-Associated Thrombotic Microangiopathy
Laskin BL et al. Blood 2011; Jodele S et al. Blood 2013; Jodele S et al. Blood Rev 2015; Jodele S et al. Blood 2016

TA-TMA Diagnosis: Histology
Siami K et al. Transplantation 2008

BMT CTN IWG EBMT/ELN Cincinnati/Philadelphia
Schistocytes Schistocytes (>4%) Schistocytes
LDH LDH LDH
Renal ± neurologic dysfunction
Thrombocytopenia
Thrombocytopenia
DAT negative Anemia Anemia
Haptoglobin Hypertension
Proteinuria*
sC5b-9 *
TA-TMA Diagnosis: non-invasive
• No universally accepted criteria, high index suspicion
• Laboratory and clinical markers:
George JN et al. Transfusion 2004; Ho VT et al. BBMT 2005; Ruutu T et al. Haematologica 2007; Cho BS et al. Transplantation 2010; Jodele S et al. Blood Rev 2015; Jodele S et al. Blood 2014; *poor outcome

TA-TMA Diagnosis: non-invasive
Ho VT et al. BBMT 2005; Ruutu T et al. Haematologica 2007; Jodele S et al. Blood Rev 2015; Cho BS et al. Transplantation 2010
Schistocytes LDH
Hypertension Proteinuria sC5b-9
Haptoglobin
Cincinnati/ Philadelphia
EBMT/ELN
BMT CTN
Renal ± neurologic dysfunction
No DIC
Cho et al. Thrombocytopenia Anemia
DAT negative

TA-TMA Diagnosis
Laskin BL et al. BMT 2011; Jodele S et al. Blood 2014
with TMA ascompared with thosewithout TMA were332.9 ng/mL
(IQR 274.45-445.05 ng/mL) and 201.4 ng/ mL (IQR 171.7-273.9
ng/mL), respectively (P 5 .03).
AcuteGVHD of any gradewasnot arisk factor for thesubsequent
development of TMA (P 5 .61). Infections documented prior to
TMA diagnosis were also not associated with an increased risk of
TMA. Subjects with TMA required more medications to maintain
a systolic blood pressure index , 1 and were more likely to be
admitted to the intensive care unit and develop respiratory failure,
gastrointestinal bleeding, andpulmonary hypertension (Table2). We
explored several multivariable models to examine independent risk
factors for thedevelopment of TMA, but none identified significant
associations.
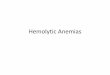
Time course of TMA diagnosis
We plotted the time-course of diagnostic markers for TMA
(Figure 1). Systolic hypertension, an elevated LDH, and proteinuria
occurred 10 to 14 days prior to TMA diagnosis. A decreased
haptoglobin laggedthefirst elevation inLDH by almost 2weeks, and
AKI, defined asdoubling of theserum creatinine, did not occur until
almost amonth after TMA diagnosis.
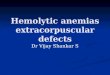
Risk factors for death in those diagnosed with TMA
Of the 39 subjects with TMA, 18 (46.2%) died by 1 year post-
transplant in comparison with only 5 of 51 (9.8%) without TMA
(P , .01). Subjects with TMA had a significantly higher risk of
1-year NRM (43.6%6 8%vs7.8% 6 3.8%, P , .0001) compared
with those without TMA (Figure 2). In the 18 subjects that died
with active TMA, the median time to death was 116 days after
HSCT (IQR 71-195 days).
All subjects who died after a TMA diagnosis had active lab-
oratory or histologic signs of microangiopathy at the time of death.
Thecauseof death in these18 subjects was listed asfollows: TMA/
multiorgan failure (n 5 4), TMA/pulmonary hypertension (n 5 3),
TMA/sinusoidal obstructive syndrome (n 5 1), acute GVHD/
multiorgan failure(n 5 6), infection (n5 1), posttransplant lympho-
proliferativedisorder (n5 1), acutemyeloid leukemiarelapse(n5 1),
andnecrotizing encephalopathy (n5 1). Twosubjectshadanautopsy
showing severe multiorgan TMA involving the kidney, lung,
bowel, andheart.Bothsubjectshadclinical andhistologicevidence
of pulmonary hypertension and histologic evidence of TMA in
mesenteric arteriolesand denuded bowel mucosa. Laboratory studies
at TMA diagnosisshowed elevated serum sC5b-9 concentrationsand
proteinuria . 30 mg/dL.
Factors associated with a higher risk of death among those
diagnosed withTMA areshown insupplemental Table1availableat
theBlood Web site. Subjectswith proteinuria$ 30mg/dL (P5 .01),
proteinuria persisting . 2 weeks (P 5 .04), higher median urine
protein to creatinine ratio (1.8 vs0.8 mg/mg, P 5 .03), and elevated
sC5b-9 above normal at TMA diagnosis (P 5 .005) were at higher
risk of death. There were no significant differences in demographic
andHSCT characteristics insubjectswithelevatedvsnormal sC5b-9
at TMA diagnosis, but overall outcomes were significantly worse
in subjects with elevated sC5b-9. Of the 28 subjects with elevated
Figure 1. Time course of clinical and laboratory markers in relation to date of TMA diagnosis. The date of TMA diagnosis is marked as day 0 (black vertical line)
and represents the posttransplant day when study diagnostic criteria for TMA were fulfilled, including elevated LDH and schistocytosis. We additionally included
the timing of proteinuria ($ 30 mg/dL on random urinalysis), hypertension (defined as a systolic blood pressure . 95th percentile for age, sex, and height), AKI
(doubling of the pretransplant serum creatinine), and a haptoglobin less than the lower limit of normal. For each variable, the white vertical lines represent the median
day the criterion became positive and the gray area the IQR. Hypertension (day 2 14) and an elevated LDH (day 2 13) were the first markers of TMA, followed by
proteinuria (day 2 10). Schistocytosis occurred on day 0, because this was typically the last criterion to turn positive and thus defined the TMA diagnosis date.
A decreased haptoglobin lagged the first elevation in LDH by almost 2 weeks. AKI, defined using serum creatinine, occurred a median of almost 28 days after TMA was
diagnosed.
Figure 2. NRM among study subjects with and without TMA at 1 year after
HSCT. Gray’s competing risk method was used to obtain the cumulative incidence of
NRM. The 1-year NRM was 43.6% 6 8% in subjects with TMA and 7.8% 6 3.8% in
HSCT subjects without TMA (P , .0001).
648 JODELE et al BLOOD, 24 JULY 2014 x VOLUME 124, NUMBER 4
For personal use only.on November 17, 2015. by guest www.bloodjournal.orgFrom
• Proteinuria, sC5b-9 (and anemia <80g/l) at the time of TMA diagnosis are associated with increased risk of death

TA-TMA Manifestations
Organ Manifestation Differential diagnosis
Kidneys Proteinuria, hypertension, decreased function
Nephrotoxic drugs, infections, steroids, CYA
Lungs Pulmonary hypertension, Hypoxia
Infections, BOS/GVHD
GI Diarrhea, vomiting, abdominal pain, bleeding, ileus
Infections, GVHD, thrombocytopenic bleeding
CNS Confusion, headache, hallucinations, seizures
Drugs, infections, bleeding, PRES, CNS-disease
Changsirikulchai S et al. Clin J Am Soc Nephrol 2009; Inamoto Y et al. BMT 2009

• Supportive:
- withdrawal/reduction/replacement of immunosuppression (CYA/tacrolimus/sirolimus steroids? Mycophenolate?)
- Antihypertensive medication (ACE inhibitors; angiotensin receptor blockers)
- Treatment of infections and/or GVHD
- Dialysis
- Transfusions
TA-TMA Treatment
Al-Nouri ZL et al. Blood 2015; Kim SS et al. Transfusion 2015; Obut F et al. BMT 2016

• Causative:
- Eculizumab* (complement blockade)
Indication: patients with proteinuria and sC5b-9 Consider dosage regimen
- Others (case reports)*: rituximab, defibrotide, vincristine, pravastatin, rTM
Plasma infusions and TPE are generally not recommended
(ASFA 2016: 2C/III)
TA-TMA Treatment
Jodele S et al. Blood Rev 2015; Kim SS et al. Transfusion 2015; Jodele S et al. BBMT 2014; Schwartz J et al. J Clin Apher 2016; Kojouri K et al. Curr Opin Oncol 2007; Ho VT et al. BBMT 2005; * off-label drug use

• Common definition criteria
• Promote further prospective, multi-center studies to
- identify more specific and early disease markers
and
- evaluate new therapeutic agents
TA-TMA Issues

Conditioning
Drug-induced hemolytic anemia (DIHA)
d0
HSCT
TA-TMA
AIHA
Transfusion support
Diseases
t
Autoimmune Hemolytic Anemia after HCT
Others: relapse, Infections, PTLD, ...
Donor issues
D/R ABO-incompatibility:
Acute hemolysis
Passenger lymphocyte syndrome
Pure red cell aplasia

• Autoimmune diseases after HCT ≈ GVHD (?)
• Incidence of AIHA: 1-4%
• Risk factors: unrelated donor, cGVHD, lymphodepletion, non-malignant disease
• Median time of onset of AIHA after HCT: 5-12 months
• Therapy resistant and associated with increased mortality
Autoimmune Hemolytic Anemia
Daikeler T et al. Blood 2011/2013; Dertschnig S et al. Blood 2015; Holbro A et al. BJH 2012 Drobyski WR et al. BMT 1996; Sanz J et al. BMT 2007; Faraci M et al. BBMT 2014; Wang M et al. BBMT 2015

• AIHA diagnosis may be difficult
AIHA Diagnosis
Autoimmune hemolytic anemia
• (normocytic) Anemia (and reticulocytosis)?
• Hemolysis? Bilirubin , LDH , haptoglobin , hemoglobinemia, hemoglobinuria
• Autoimmune: DAT (usually) + for C3d, IgG/IgM or both
• And: don‘t forget the blood smear!
Rovira J et al. Transfus Med Rev 2013

AIHA Differential Diagnosis
Adapted from Transfusion Therapy: Clinical Principles and Practice, 3rd edition, Bethesda, MD: AABB Press, 2011 and Gehrs BC et al. Am J Hematol 2002
Warm AIHA
Cold AIHA
Mixed
Autoantibody (Antigen)
IgG (Rh)
IgM (I/i)
IgG & IgM
Clinic Extravascular Intravascular Combined
DAT IgG +/- C3
(IgG1, IgG3) C3 alone IgG + C3

• Supportive:
- Transfusions: serologic incompatibility of (all) crossmatched donor erythrocytes Labor-intensive and time consuming techniques
- Do not withhold transfusions in critical cases!
- Physician‘s decision (and responsibility), close monitoring
- Selection of RBC depending on urgency
AIHA Treatment
Petz LD. Br J Haematol 2004

• Causative:
- Immunosuppression has to be balanced against a possible increased risk of disease relapse
- No consensus on the optimal therapeutic approach, very low evidence (case reports, case series)
A) WAIHA: - First-line: corticosteroids
- Second-line: rituximab* or splenectomy
- Others: danazol, cyclophosphamide, azathioprine, mycophenolate mofetil, cyclosporine, sirolimus
AIHA Treatment
Crowther M et al. Blood 2011; Lechner K et al. Blood 2010; Zanella A et al. Haematologica 2014; Dierickx D et al. Blood 2015; Birgens H et al. Br J Haematol 2013; Park JA et al. Transfus Med Rev. 2015; * off-label drug use

B) CAIHA: - Avoidance of cold temperatures, warm transfusions (if needed) and infusions
- Indications for treatment: symptomatic anemia, transfusion dependence, disabling circulatory symptoms
- Rituximab* (+/- fludarabine)
- Plasma exchange (ASFA 2016: 2C/II)
- Eculizumab*
AIHA Treatment
Swiecicki PL et al. Blood 2013; Berentsen S. Br J Haematol 2011; Schwartz J et al. J Clin Apher 2016; Berentsen S et al. Blood 2004; Berentsen S et al. Blood 2010; Roth A et al. Blood 2009; Brodsky RA Blood 2015; * off-label drug use

Conditioning
Drug-induced hemolytic anemia (DIHA)
d0
HSCT
Acute hemolysis
Passenger lymphocyte syndrome
Pure red cell aplasia
TA-TMA
AIHA
Transfusion support
D/R ABO-incompatibility:
Diseases
t
Summary
Others: relapse, Infections, PTLD, ...
Donor issues

Thank you!


TA-TMA Differential Diagnosis
• Thrombotic thrombocytopenic purpura (inherited, acquired)
• Classical hemolytic uremic syndrome (Shiga toxin-producing Escherichia coli)
• Atypical hemolytic uremic syndrome (complement mediated)
• Transplantation-associated thrombotic microangiopathy*
• Pregnancy associated (HELLP-syndrome, Pre-eclampsia, Eclampsia)
• Disseminated intravascular coagulation*
• Drug-induced thrombotic microangiopathy (immune mediated, toxic)*
• Infections*
• Malignant hypertension*
• Malignancy
• Autoimmune