Embed Size (px)
Citation preview
Management of Elevated Cholesterol in the Primary Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese (MEGA) TrialPrevention Group of Adult Japanese (MEGA) Trial
Management of Elevated Cholesterol in the Primary Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese (MEGA) TrialPrevention Group of Adult Japanese (MEGA) Trial
MEGA TrialMEGA TrialMEGA TrialMEGA Trial
Presented atPresented atThe American Heart AssociationThe American Heart Association
Scientific Session 2005Scientific Session 2005
Presented by Dr. Haruo NakamuraPresented by Dr. Haruo Nakamura
www. Clinical trial results.org
MEGA Trial: BackgroundMEGA Trial: BackgroundMEGA Trial: BackgroundMEGA Trial: Background
• In Japan, the incidence of coronary disease is about In Japan, the incidence of coronary disease is about one third lower than the US and Europe, where most of one third lower than the US and Europe, where most of the statin trials have been conductedthe statin trials have been conducted
• The goal of this study was to examine whether the The goal of this study was to examine whether the addition of a low-dose statin to a diet rich in omega-3 addition of a low-dose statin to a diet rich in omega-3 fatty acids could reduce the risk of CHD.fatty acids could reduce the risk of CHD.
• In Japan, the incidence of coronary disease is about In Japan, the incidence of coronary disease is about one third lower than the US and Europe, where most of one third lower than the US and Europe, where most of the statin trials have been conductedthe statin trials have been conducted
• The goal of this study was to examine whether the The goal of this study was to examine whether the addition of a low-dose statin to a diet rich in omega-3 addition of a low-dose statin to a diet rich in omega-3 fatty acids could reduce the risk of CHD.fatty acids could reduce the risk of CHD.
Presented at AHA 2005Presented at AHA 2005
www. Clinical trial results.org
Diet Modification
n=3,966
Diet Modification
n=3,966
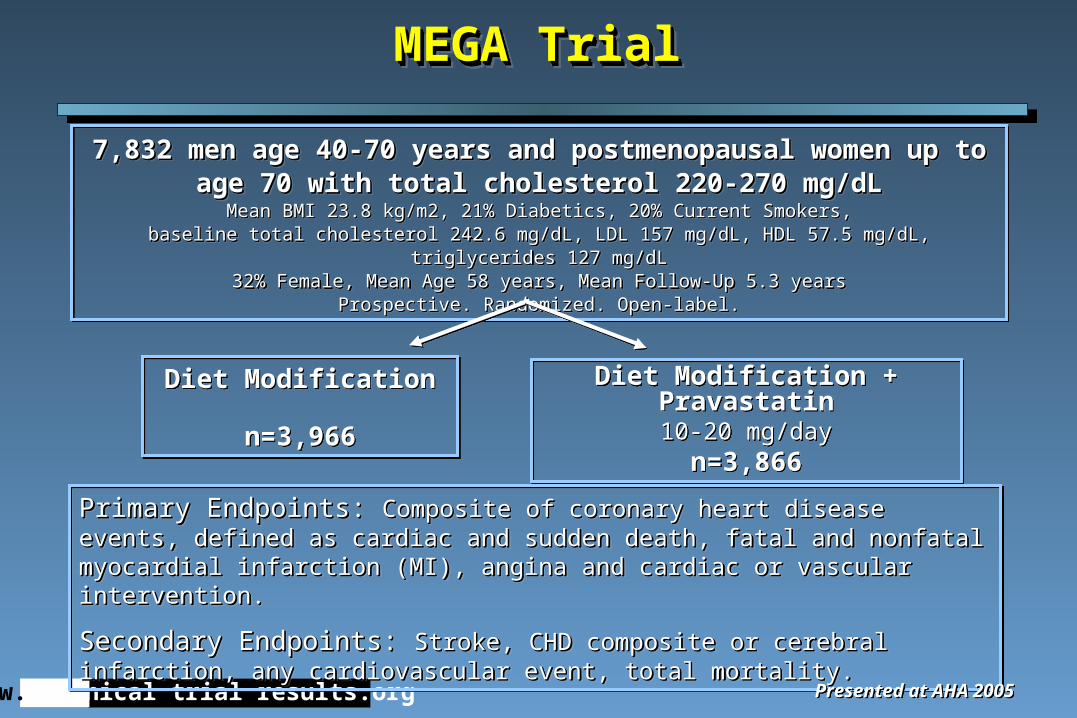
Primary Endpoints: Primary Endpoints: Composite of coronary heart disease events, defined as cardiac Composite of coronary heart disease events, defined as cardiac and sudden death, fatal and nonfatal myocardial infarction (MI), angina and cardiac or and sudden death, fatal and nonfatal myocardial infarction (MI), angina and cardiac or vascular intervention.vascular intervention.
Secondary Endpoints: Secondary Endpoints: Stroke, CHD composite or cerebral infarction, any Stroke, CHD composite or cerebral infarction, any cardiovascular event, total mortality.cardiovascular event, total mortality.
Primary Endpoints: Primary Endpoints: Composite of coronary heart disease events, defined as cardiac Composite of coronary heart disease events, defined as cardiac and sudden death, fatal and nonfatal myocardial infarction (MI), angina and cardiac or and sudden death, fatal and nonfatal myocardial infarction (MI), angina and cardiac or vascular intervention.vascular intervention.
Secondary Endpoints: Secondary Endpoints: Stroke, CHD composite or cerebral infarction, any Stroke, CHD composite or cerebral infarction, any cardiovascular event, total mortality.cardiovascular event, total mortality.
MEGA TrialMEGA TrialMEGA TrialMEGA Trial
Presented at AHA 2005Presented at AHA 2005
Diet Modification + Pravastatin10-20 mg/day
n=3,866
Diet Modification + Pravastatin10-20 mg/day
n=3,866
7,832 men age 40-70 years and postmenopausal women up to age 70 7,832 men age 40-70 years and postmenopausal women up to age 70 with total cholesterol 220-270 mg/dLwith total cholesterol 220-270 mg/dL
Mean BMI 23.8 kg/m2, 21% Diabetics, 20% Current Smokers,Mean BMI 23.8 kg/m2, 21% Diabetics, 20% Current Smokers,baseline total cholesterol 242.6 mg/dL, LDL 157 mg/dL, HDL 57.5 mg/dL, triglycerides 127 mg/dLbaseline total cholesterol 242.6 mg/dL, LDL 157 mg/dL, HDL 57.5 mg/dL, triglycerides 127 mg/dL
32% Female, Mean Age 58 years, Mean Follow-Up 5.3 years32% Female, Mean Age 58 years, Mean Follow-Up 5.3 yearsProspective. Randomized. Open-label.Prospective. Randomized. Open-label.
7,832 men age 40-70 years and postmenopausal women up to age 70 7,832 men age 40-70 years and postmenopausal women up to age 70 with total cholesterol 220-270 mg/dLwith total cholesterol 220-270 mg/dL
Mean BMI 23.8 kg/m2, 21% Diabetics, 20% Current Smokers,Mean BMI 23.8 kg/m2, 21% Diabetics, 20% Current Smokers,baseline total cholesterol 242.6 mg/dL, LDL 157 mg/dL, HDL 57.5 mg/dL, triglycerides 127 mg/dLbaseline total cholesterol 242.6 mg/dL, LDL 157 mg/dL, HDL 57.5 mg/dL, triglycerides 127 mg/dL
32% Female, Mean Age 58 years, Mean Follow-Up 5.3 years32% Female, Mean Age 58 years, Mean Follow-Up 5.3 yearsProspective. Randomized. Open-label.Prospective. Randomized. Open-label.
www. Clinical trial results.org
MEGA Trial: Cholesterol and Triglyceride LevelsMEGA Trial: Cholesterol and Triglyceride Levels MEGA Trial: Cholesterol and Triglyceride LevelsMEGA Trial: Cholesterol and Triglyceride Levels
Presented at AHA 2005Presented at AHA 2005
-11.5
-18.0
5.8
-3.1-2.1 -3.2
3.21.3
-20
-16
-12
-8
-4
0
4
Pravastatin+diet Diet
-11.5
-18.0
5.8
-3.1-2.1 -3.2
3.21.3
-20
-16
-12
-8
-4
0
4
Pravastatin+diet Diet
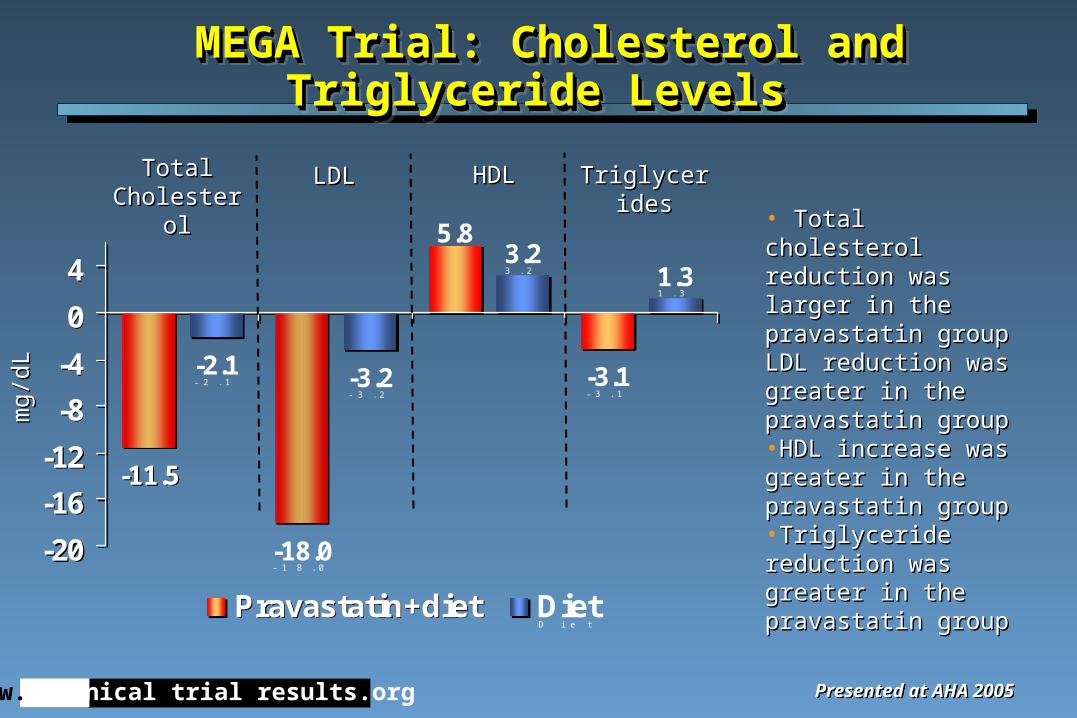
• Total cholesterol Total cholesterol reduction was larger in reduction was larger in the pravastatin groupthe pravastatin groupLDL reduction was LDL reduction was greater in the greater in the pravastatin grouppravastatin group•HDL increase was HDL increase was greater in the greater in the pravastatin grouppravastatin group•Triglyceride reduction Triglyceride reduction was greater in the was greater in the pravastatin grouppravastatin group
Total Total CholesterolCholesterol
LDLLDL HDLHDL TriglyceridesTriglycerides
mg/
dLm
g/dL
www. Clinical trial results.org
MEGA Trial: Primary Composite EndpointMEGA Trial: Primary Composite EndpointMEGA Trial: Primary Composite EndpointMEGA Trial: Primary Composite Endpoint
3.3
5.0
0
1
2
3
4
5
Pravastatin+diet Diet
3.3
5.0
0
1
2
3
4
5
Pravastatin+diet Diet
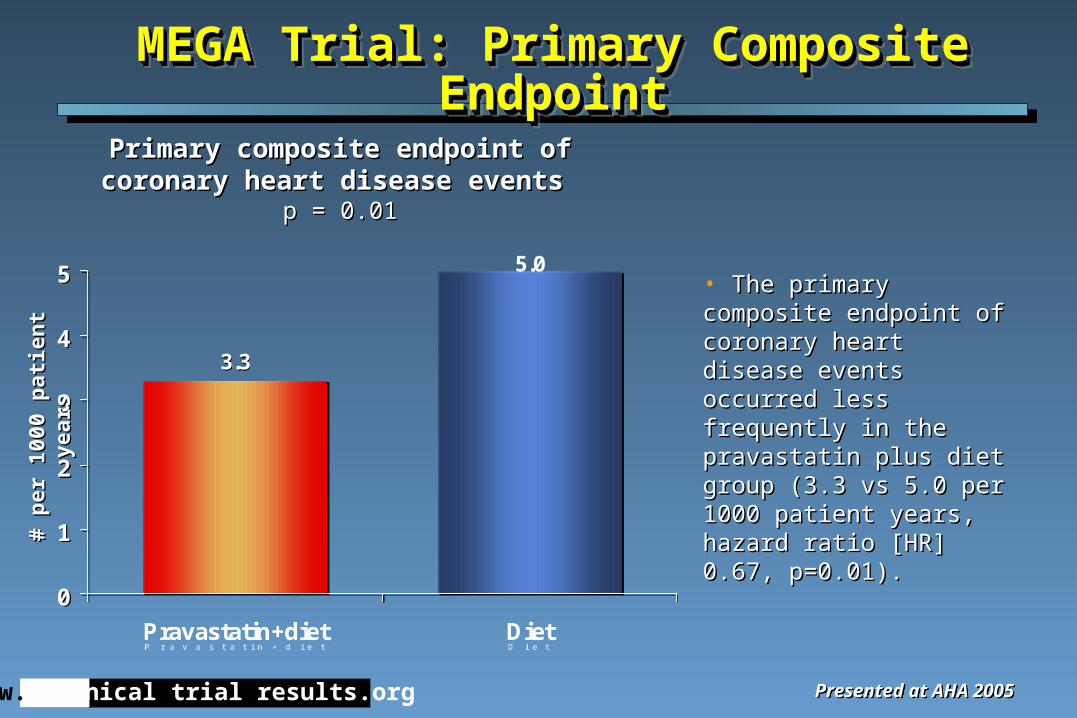
• The primary composite The primary composite endpoint of coronary heart endpoint of coronary heart disease events occurred less disease events occurred less frequently in the pravastatin frequently in the pravastatin plus diet group (3.3 vs 5.0 plus diet group (3.3 vs 5.0 per 1000 patient years, per 1000 patient years, hazard ratio [HR] 0.67, hazard ratio [HR] 0.67, p=0.01).p=0.01).
Primary composite endpoint of coronary Primary composite endpoint of coronary heart disease events heart disease events
p = 0.01p = 0.01
Presented at AHA 2005Presented at AHA 2005
# p
er 1
000
pat
ien
t ye
ars
# p
er 1
000
pat
ien
t ye
ars
www. Clinical trial results.org
MEGA Trial: Secondary EndpointsMEGA Trial: Secondary EndpointsMEGA Trial: Secondary EndpointsMEGA Trial: Secondary Endpoints
2.7
0.9
2.5
2.0
3.8
1.6
3.02.6
0
1
2
3
4
Total mortality MI Stroke Cerebralinfarction+TIA
Pravastatin+diet Diet
2.7
0.9
2.5
2.0
3.8
1.6
3.02.6
0
1
2
3
4
Total mortality MI Stroke Cerebralinfarction+TIA
Pravastatin+diet Diet
Presented at AHA 2005Presented at AHA 2005
p=0.055
p=0.03
p=0.33
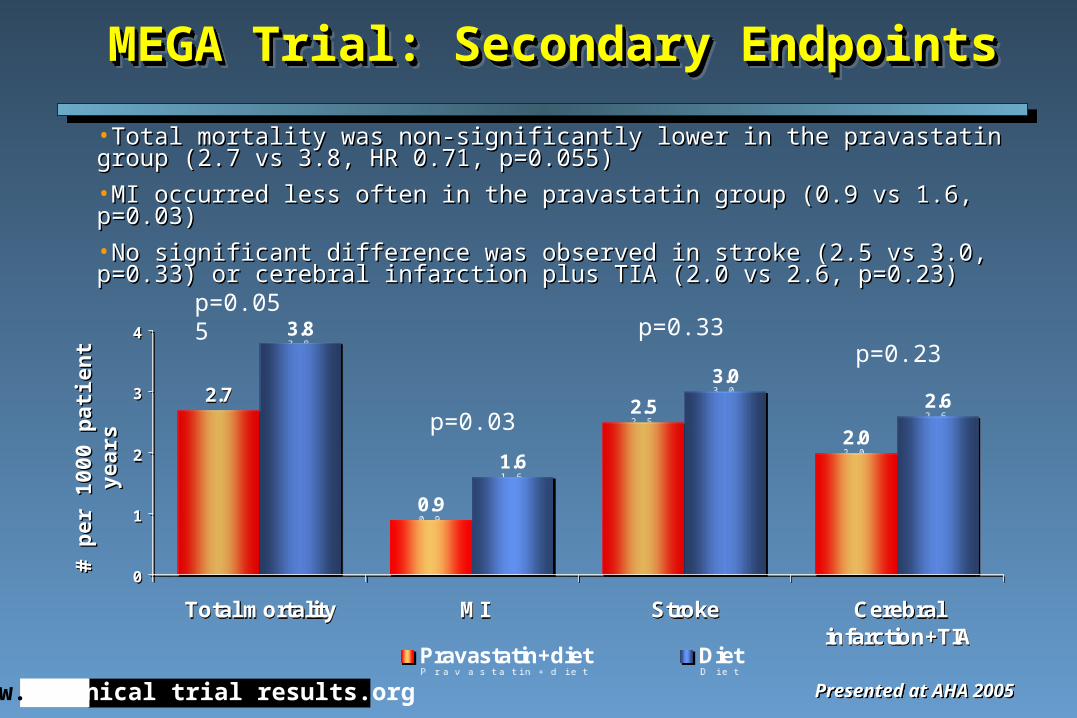
•Total mortality was non-significantly lower in the pravastatin group (2.7 vs 3.8, HR Total mortality was non-significantly lower in the pravastatin group (2.7 vs 3.8, HR 0.71, p=0.055)0.71, p=0.055)
•MI occurred less often in the pravastatin group (0.9 vs 1.6, p=0.03)MI occurred less often in the pravastatin group (0.9 vs 1.6, p=0.03)
•No significant difference was observed in stroke (2.5 vs 3.0, p=0.33) or cerebral No significant difference was observed in stroke (2.5 vs 3.0, p=0.33) or cerebral infarction plus TIA (2.0 vs 2.6, p=0.23)infarction plus TIA (2.0 vs 2.6, p=0.23)
# p
er 1
000
pat
ien
t ye
ars
# p
er 1
000
pat
ien
t ye
ars p=0.23
www. Clinical trial results.org
5.0
7.1
0
2
4
6
8
Pravastatin+diet Diet
5.0
7.1
0
2
4
6
8
Pravastatin+diet Diet
MEGA Trial: Secondary Endpoints cont.MEGA Trial: Secondary Endpoints cont.MEGA Trial: Secondary Endpoints cont.MEGA Trial: Secondary Endpoints cont.
Presented at AHA 2005Presented at AHA 2005
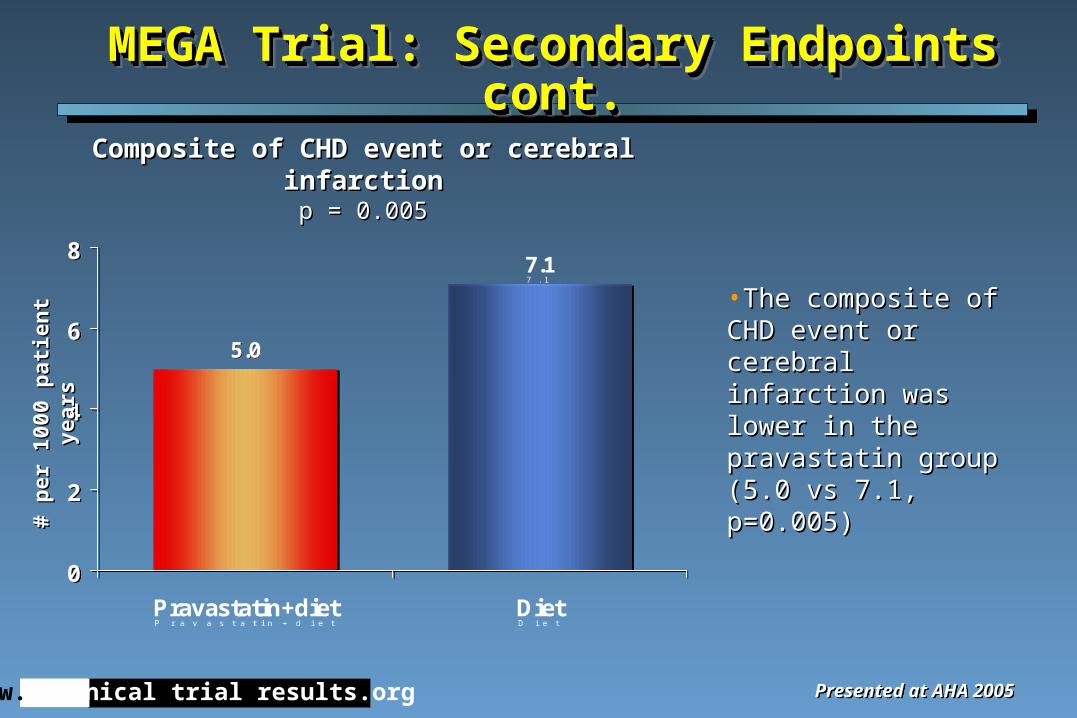
•The composite of CHD The composite of CHD event or cerebral event or cerebral infarction was lower in infarction was lower in the pravastatin group the pravastatin group (5.0 vs 7.1, p=0.005)(5.0 vs 7.1, p=0.005)
# p
er 1
000
pat
ien
t ye
ars
# p
er 1
000
pat
ien
t ye
ars
Composite of CHD event or cerebral infarctionComposite of CHD event or cerebral infarctionp = 0.005p = 0.005
www. Clinical trial results.org
5.5 5.7
0
1
2
3
4
5
6
Pravastatin+diet Diet
5.5 5.7
0
1
2
3
4
5
6
Pravastatin+diet Diet
MEGA Trial: Safety Data MEGA Trial: Safety Data MEGA Trial: Safety Data MEGA Trial: Safety Data
Presented at AHA 2005Presented at AHA 2005
# p
er 1
000
pat
ien
t ye
ars
# p
er 1
000
pat
ien
t ye
ars
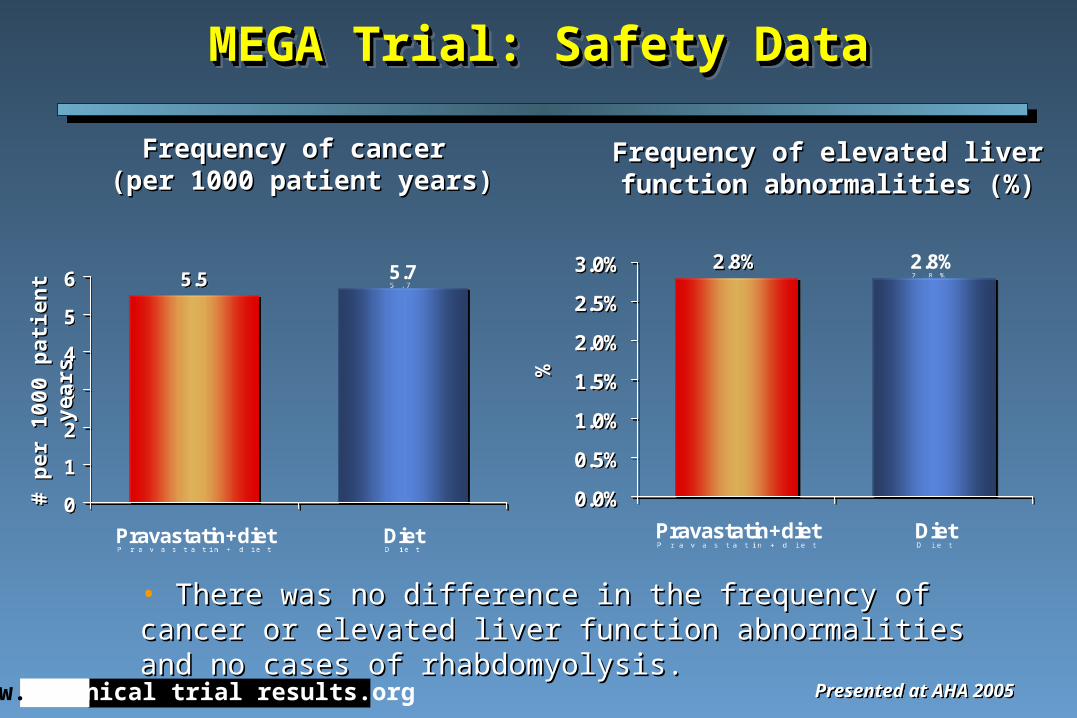
• There was no difference in the frequency of cancer or elevated There was no difference in the frequency of cancer or elevated liver function abnormalities and no cases of rhabdomyolysis.liver function abnormalities and no cases of rhabdomyolysis.
2.8% 2.8%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
Pravastatin+diet Diet
2.8% 2.8%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
Pravastatin+diet Diet%%
Frequency of cancer Frequency of cancer (per 1000 patient years)(per 1000 patient years)
Frequency of elevated liver Frequency of elevated liver function abnormalities (%)function abnormalities (%)
www. Clinical trial results.org
MEGA Trial: SummaryMEGA Trial: SummaryMEGA Trial: SummaryMEGA Trial: Summary
• Among Japanese patients with hypercholesterolemia, treatment with Among Japanese patients with hypercholesterolemia, treatment with pravastatin therapy in addition to diet modification was associated with a pravastatin therapy in addition to diet modification was associated with a reduction in the primary composite endpoint of coronary heart disease reduction in the primary composite endpoint of coronary heart disease events compared with diet modification alone at a mean 5.3 year follow-events compared with diet modification alone at a mean 5.3 year follow-up.up.
• Previous studies conducted in western populations have shown Previous studies conducted in western populations have shown reductions in adverse coronary events associated with statin therapy use; reductions in adverse coronary events associated with statin therapy use; however, the cardiac morbidity and mortality in Japan is much lower than however, the cardiac morbidity and mortality in Japan is much lower than in the U.S. and other western countries where statin therapy has been in the U.S. and other western countries where statin therapy has been predominantly studied.predominantly studied.
• The present study demonstrated that even in this lower risk population, The present study demonstrated that even in this lower risk population, primary prevention with low-dose statin therapy can be effective in primary prevention with low-dose statin therapy can be effective in reducing cardiac events, with a modest reduction in lipid parameters.reducing cardiac events, with a modest reduction in lipid parameters.
• Among Japanese patients with hypercholesterolemia, treatment with Among Japanese patients with hypercholesterolemia, treatment with pravastatin therapy in addition to diet modification was associated with a pravastatin therapy in addition to diet modification was associated with a reduction in the primary composite endpoint of coronary heart disease reduction in the primary composite endpoint of coronary heart disease events compared with diet modification alone at a mean 5.3 year follow-events compared with diet modification alone at a mean 5.3 year follow-up.up.
• Previous studies conducted in western populations have shown Previous studies conducted in western populations have shown reductions in adverse coronary events associated with statin therapy use; reductions in adverse coronary events associated with statin therapy use; however, the cardiac morbidity and mortality in Japan is much lower than however, the cardiac morbidity and mortality in Japan is much lower than in the U.S. and other western countries where statin therapy has been in the U.S. and other western countries where statin therapy has been predominantly studied.predominantly studied.
• The present study demonstrated that even in this lower risk population, The present study demonstrated that even in this lower risk population, primary prevention with low-dose statin therapy can be effective in primary prevention with low-dose statin therapy can be effective in reducing cardiac events, with a modest reduction in lipid parameters.reducing cardiac events, with a modest reduction in lipid parameters.
Presented at AHA 2005Presented at AHA 2005