Embed Size (px)
Citation preview

Case Report/Clinical Techniques
Management of Dens Invaginatus Type IIAssociated with Immature Apex and LargePeriradicular Lesion Using Platelet-rich Fibrin andBiodentine
Shruti Goel, MDS,1Ruchika Roongta Nawal, MDS, and Sangeeta Talwar, MDS
Abstract
SignificanceThis case report describes possibilities of bettermanagement and improved prognosis forendodontically complex cases owing to advance-ments in technology (CBCT) and biomaterials (Bio-dentine and PRF). This approach could helpclinicianswhocomeacrosssimilar anomalieswhilecaring for patients.
Dens invaginatus (DI) poses peculiar challenges in end-odontic treatment of teeth because of distortion of pulpalspace. A case of Oehlers type II DI with open apex andlarge periapical lesion is reported. The case was managedusing cone-beam computed tomography (CBCT), oper-ating microscope, platelet-rich fibrin (PRF), and Bio-dentine. A 15-year-old male patient presented withpalatal swelling. Pulp sensibility testing of right maxillarylateral incisor was negative. Intraoral periapical digitalradiograph revealed an Oehlers type II DI with openapex and periapical radiolucency. A CBCT scan was per-formed to study the anatomy, determine the true extentof the periapical lesion, and form a treatment plan. Adiagnosis of Oehlers type II DI with pulp necrosis andacute periapical abscess was made. Two-visit endodontictreatment was performed. In the first visit, the invagi-nated central mass was removed under operating micro-scope, chemo-mechanical preparation was done, anddouble antibiotic paste dressing was placed. In the sec-ond visit, the canal was sealed with apical matrices ofPRF and Biodentine as filling material. The patient wasasymptomatic and radiographs revealed continued heal-ing of the osseous defect at follow-up visits. A CBCTscan at 30 months showed complete continuity of peri-odontal ligament space, healing of labial and palatalcortical plates, and formation of intercortical bone. Theadvances in endodontic armamentarium and technology,like CBCT and operating microscope, have made success-ful treatment of challenging cases possible. PRF andBiodentine as apical matrices and filling material, respec-tively, proved to be effective in the present case. (J Endod2017;43:1750–1755)
Key WordsApexification, Biodentine, cone-beam computedtomography, dens invaginatus, platelet-rich fibrin
Department of Conservative Dentistry and Endodontics, Maulan1Permanent address: 54, Shanti Vihar, Delhi-92, India.Address requests for reprints to Ruchika Roongta Nawal, Departm
Shah Zafar Marg, Delhi 110002, India. E-mail address: ruchika.roon0099-2399/$ - see front matter
Copyright ª 2017 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2017.04.005
1750 Goel et al.
Endodontists are oftenchallenged by teeth
with anomalous and com-plex root canal morphol-ogies. The knowledge ofsuch anatomic variationsand thorough understand-ing of basic endodonticprinciples is essential formanagement of such cases.
Dens invaginatus (DI) is a well-known dental anomaly occurring most commonly inmaxillary lateral incisors (1). It is characterized by invagination of the enamel organinto the dental papilla before calcification has occurred (2). The incidence of DI rangesfrom 0.04% to 10% (3).DI refers to a congenital infolding of a toothlike structure within a tooth. The mostcommonly accepted classification of DI was given by Oehlers in 1957 (4). Three sub-types are designated, which are based on the extent of apical migration of an enamel-lined invagination. In type I, the invagination is minimal and enamel-lined, it is confinedwithin the crown of the tooth and does not extend beyond the level of the externalcemento-enamel junction. In type II, the enamel-lined invagination invades into theroot but remains confined within it as a blind sac. There may, however, be a commu-nication with the pulp. The invagination may or may not be grossly dilated; in the formercase, there is often a corresponding dilatation of the root or crown. In type III, the invag-ination penetrates through the root and ‘‘bursts’’ apically or laterally at foramen, some-times referred to as a ‘‘second foramen’’ in the root. There is usually no communicationwith the pulp, which lies compressed within the wall around the invagination process.
Endodontic treatment can be predictable only when the entire root canal system isdebrided and disinfected. Many previously published cases have shown the struggle intreatment of teeth with the DI (5–7). Earlier, imaging in endodontics was limited to2-dimensional intraoral periapical radiographs. Although DI can be detected by routineradiographs, cone-beam computed tomography (CBCT), a 3-dimensional imaging mo-dality, has aided not only in diagnosis and classification, but also in improved treatmentplanning of complicated cases (6,8–10). Various previous authors have reported thebenefits of CBCT in management of complex endodontic cases (11, 12).
Biodentine is a calcium-silicate–based cement. Its powder is composed of trical-cium silicate, dicalcium silicate, calcium carbonate, and zirconium oxide. The liquid
a Azad Institute of Dental Sciences, Bahadur Shah Zafar Marg, Delhi, India.
ent of Conservative Dentistry and Endodontics, Maulana Azad Institute of Dental Sciences, [email protected]
JOE — Volume 43, Number 10, October 2017

Case Report/Clinical Techniques
consists of calcium chloride and a hydrosoluble polymer (13). Bio-dentine has been shown as an excellent material for apexification(14, 15). An apical matrix is used to control apical placement ofBiodentine and to prevent its extrusion beyond the apex. Severalbiocompatible materials had been used earlier as an apical matrix,including tricalcium phosphate, calcium hydroxide, freeze-driedbone, freeze-dried dentin, collagen, and calcium phosphate (16).The platelet-rich fibrin (PRF) of Choukroun et al (17) is a second-generation platelet concentrate composed of fibrin membraneaugmented with growth factors. In the current case, PRF was used asbiological apical matrices.The purpose of this case report was to present successful nonsur-gical endodontic management of a complex case of type II DI associatedwith immature apex and an extensive periradicular lesion, using CBCTfor diagnosis and PRF and Biodentine as apical matrices and filling ma-terial, respectively.
Case ReportA 15-year-old male patient reported to the Department of Conser-
vative Dentistry and Endodontics, Maulana Azad Institute of Dental Sci-ences, New Delhi, India, with chief complaint of pain associated withrecurrent palatal swelling on right side of the palate for 2 months.The patient’s previous medical and dental history was noncontributory.There was no history of trauma. On examination, a fluctuant palatalswelling extending from the upper right canine to the mesial aspectof the upper right first molar was observed (Fig. 1A). Tooth #7 showeda peg-shaped clinical crown with a prominent depression and pit on itsmesiolabial aspect (Fig. 1B). The pit was negotiable with a 15# K-file(Fig. 1C). The contralateral lateral incisor was congenitally missing.
Tooth #7 was caries and restoration free. Response to percussionwas negative. The periodontal probing depths were in the normal rangewith no mobility. The tooth gave no response to cold testing using EndoIce (Hygenic, Akron, OH) and electric pulp testing (Analytic Technol-ogy, Redmond, WA). Tooth #6 and tooth #8 gave normal responsesto both electrical and thermal pulp sensibility testing. The patient’s over-all oral health appeared to be good with normal occlusion.
Radiographic evaluation of the tooth in question revealed an invag-ination of dentin lined by enamel into the pulpal space, extending to themiddle third of the root. The tooth showed an immature root with openapex, associated with a large periapical radiolucent lesion (Fig. 1D).
Because of the complex anatomy of tooth #7, as revealed by theperiapical radiograph, a CBCT scan (I-CAT; Imaging Sciences, Hatfield,PA) was advised for the patient as supplemental examination. The CBCT(Fig. 4A–D) revealed an invagination into the root, without any commu-nication with the laterally recessed root canal. The invagination commu-nicatedwith the periodontal ligament space apically through the widenedapical foramen. A well-defined unilocular periapical radiolucent lesion
Figure 1. Preoperative images. (A) Palatal view of maxilla showing a soft swellinmesiolabial aspect. (C) A 15# K-file could be inserted to a depth of 10 mm. (D) Radlesion.
JOE — Volume 43, Number 10, October 2017
1.4 cm (mesiodistal)� 1.1 cm (labiopalatal)� 1.5 cm (craniocaudal)was observed in relation to tooth #7. There was labiopalatal expansion ofthe maxilla with dehiscence of the labial and palatal cortical platesbeyond the middle third of the root of tooth #7. Superiorly, the lesionextended until the nasal floor. A diagnosis of Oehlers type II DI withpulp necrosis and acute periapical abscess was made.
After discussing the treatment options with the patient and hisparent, removal of the DI, followed by nonsurgical endodontic treat-ment for open apex was decided on.
Under rubber dam isolation, a labial access cavity was preparedfor tooth #7 using a surgical operating microscope (Proergo; CarlZeiss) (Fig. 2A). A high-speed diamond tapered fissure bur was usedto remove the DI. A large volume of pale-yellowish fluid drained fromthe canal. The root canal was irrigated copiously with 1% sodium hypo-chlorite using a 27-gauge side-venting needle, 2 mm short of the canal.The canal was debrided using an 80# K-file (Dentsply Maillefer, Bal-laigues, Switzerland). The root canal was dried with paper points anda double antibiotic paste (ciprofloxacin and metronidazole) was placedinside the root canal using lentulo spirals. The access opening wasclosed with a 3-mm-thick temporary restorative material (Coltosol F;Coltene/Whaledent Inc, Cuyahoga Falls, OH). The patient was scheduledto return after 2 weeks.
The patient was completely asymptomatic at the recall appoint-ment. Under rubber dam isolation, the temporary restorative materialwas carefully removed by using the #2 diamond round bur (LA Axessbur; SybronEndo). Sodium hypochlorite irrigation (5.25%) and size#60 stainless steel hand files were used to remove the double antibioticpaste. The tooth was evaluated under surgical operating microscope toensure that no remnants of the double antibiotic paste remained. Theroot canal was irrigated thoroughly with 5.25% sodium hypochloritefollowed by 17% EDTA. A final rinse with normal saline was doneand the canal was dried using paper points.
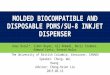
The technique described by Choukroun et al (17) was used to pre-pare PRF. Five milliliters of blood was extracted from patient’s forearmand transferred to a 10-mL test tube containing no anticoagulant. Theblood sample was centrifuged (REMI Laboratories, Mumbai, India)at 3000 revolutions per minute for 10 minutes. Sterile tweezers wereinserted into the tube to gently grab and remove the fibrin clot(Fig. 2B). The PRF clot was squeezed between sterile gauze pieces toremove excess fluid. PRF was placed as apical matrices in the tooth(Fig. 2C). Biodentine (Septodont, Saint Maur des Fosse’s, France)was mixed according to the manufacturer’s instructions and condensedincrementally against PRF matrices. Biodentine was placed until thejunction of the middle third and cervical third of the canal. After initialsetting, resin-modified glass ionomer cement (Vitrebond; 3M ESPE)was directly placed on top of the Biodentine, filling the cervical thirdof the canal and light-cured. The access cavity was restored withnano-hybrid composite resin (Filtek Z250 XT; 3M ESPE). The tooth
g on the right side. (B) Malformed right lateral incisor with a depression oniograph showing presence of dens invaginatus associated with large periapical
DI Type II Management Using PRF and Biodentine 1751

Figure 2. Intraoperative and immediate postoperative images. (A) Invagination inside the root canal. (B) Platelet-rich fibrin. (C) Invagination removed andplatelet-rich fibrin placed inside the canal. (D) Immediate postoperative radiograph. (E) Composite buildup of tooth #7. (F) Immediate postoperative photographdepicting complete resolution of palatal swelling.
Figure 3. Follow-up photographs and radiographs. (A) All-ceramic crown placement after 6 months. (B) Twelve-month recall radiograph. (C) Thirty-monthrecall labial view. (D) Thirty-month recall palatal view. (E) Thirty-month recall radiograph.
Case Report/Clinical Techniques
1752 Goel et al. JOE — Volume 43, Number 10, October 2017

Case Report/Clinical Techniques
was shaped in the form of a normal lateral incisor using nano-hybridcomposite restorative material (Filtek Z250 XT; 3M ESPE) (Fig. 2Eand 2F). A postoperative radiograph was taken (Fig. 2D), and the pa-tient was instructed to take an analgesic (diclofenac sodium 50 mg)medication if required.At the 1-week follow-up visit, the patient was free of symptoms. Thetooth was not tender to percussion or palpation. At 6 months, the radio-graph revealed resolution of periapical radiolucency. An all-ceramiccrown was placed, to satisfy the esthetic needs of the patient
Figure 4. Cone-beam computed tomography images. (A) Transverse view shows rlarge periapical radiolucency. (C) Three-dimensional reconstruction indicating losslabial and lingual cortical plates, and loss of trabecular pattern surrounding tooth #7pattern at 30-month follow-up. (F) Coronal section indicating resolution of periapicshows healed labial cortical plates at 30-month follow-up. (H) Sagittal section reveabone at 30-month follow-up. (A-D) Arrows indicate areas of bone loss. (E-F) Arr
JOE — Volume 43, Number 10, October 2017
(Fig. 3A). At 12 months, the periapical area showed normal trabecula-tion (Fig. 3B). Because intraoral periapical digital radiographs (IOPAs)may overestimate bony healing (18) and give a 2-dimensional picture,at the 30-month recall appointment (Fig. 3C–E), a CBCT scan was takenagain to evaluate the actual extent of bony healing. The CBCT (Fig. 4E–H) revealed that there was resolution of the labio-palatal expansion ofcortical plates around tooth #7 and both the labial and palatal corticalplates had completely healed. Normal trabecular pattern was seen in thecancellous bone around the tooth.
adiolucency surrounding #7. (B) Coronal view showing dens invaginatus andof labial cortical plate. (D) Sagittal sections revealing dens invaginatus, loss of. (E) Transverse section of bone showing cortical plates and normal trabecularal radiolucency at 30-month follow-up. (G) Three-dimensional reconstructionling completely formed labial and lingual cortical plates and healing cancellousows indicate areas of bony healing.
DI Type II Management Using PRF and Biodentine 1753

Case Report/Clinical Techniques
DiscussionDI is a developmental anomaly of the tooth. During tooth forma-
tion, the enamel organ is invaginated into the dental papilla, resultingin the formation of a pit lined by enamel and dentin invaginating thepulp. This pit acts as an area of stagnation of organic matter and pro-vides a hospitable environment formicroorganisms (19). Enamel liningin these defects is often malformed or may have fine canals that act aspotential pathways for bacterial contamination of pulp tissue.
In the present case, the tooth revealed Oehlers type II anatomy,composed of an invagination invading the root while remaining confinedwithin it as a blind sac. The tooth was free from any detectable caries andno history of trauma was reported by the patient. The pulpal necrosis ofthe tooth could have resulted from infiltration of bacteria in the pulpchamber through microscopic channels present in the pit. This early ne-crosis of the pulp could have interfered with complete root formation.
An initial examination of the concerned case revealed several end-odontic complications associated with its management. The invaginatedcentral mass of hard tissue occupied much of the pulpal space and ob-structed debridement of the remaining canal. The large periapicallesion caused constant drainage of fluid into the canal space. Further,the presence of a wide-open apex made sealing of the canal difficult.
Anatomic complexity in such cases may show multiple variations,and requires detailed study before treatment planning. To aid in detec-tion of the anatomy of DI and in determining the exact extent of periap-ical pathology, a supplementary CBCT scan was advised.
In this case, CBCT reinforced the finding that the DI was sur-rounded by pulp from all sides. It had to be removed to allow cleaningof otherwise inaccessible pulpal space. Because the DI was not attachedto the root dentin, it could be carefully removed under magnificationand illumination using an operating microscope without harming thealready thin root canal walls.
To eliminate the long-standing infection, basic principles of end-odontic treatment were followed. Biomechanical preparation was donewith K-files to remove tissue tags adhering to canal walls. Copious irri-gation with 5.25%NaOCl provided chemical disinfection. Because of thepresence of acute apical abscess associated with palatal swelling, a dou-ble antibiotic paste intracanal dressing was used instead of providingsingle-visit root canal treatment. Previous studies have reported thatdouble antibiotic paste is capable of eliminating bacteria from infecteddental tissues (20).
An open apex might cause difficulties due to overfilling or an inad-equate apical seal. Apexification with calcium hydroxide is time-consuming and increases fracture susceptibility of roots. Therefore,1-step apexification with calcium silicate–based cement was the treat-ment of choice (21). In the present case, Biodentine was used for apex-ification. Biodentine has been reported to have good sealing ability, highcompressive strength, excellent biocompatibility (22), a very shortsetting time (6 minutes) (23), and better handling properties (24)as compared with mineral trioxide aggregate.
To prevent overfilling, PRF was used as the apical matrices againstwhich Biodentine was condensed. PRF is commonly used in implantand periodontal surgeries to boost bone regeneration and soft tissuewound healing. It has been shown to stimulate osteoblast cells (25),gingival fibroblasts (26), pulp cells (27), and periodontal ligamentcell proliferation. It forms an excellent matrix for growth of bone,acting as both an osteoconductive and osteoinductive substance. Afew other case reports have described the use of PRF as biological api-cal matrices (28–30).
Clinical signs and symptoms resolved after the treatment. Periapicalradiographs taken at follow-up visits at 6 months, 12months, 18months,and 24 months showed progressive healing of periapical bone and
1754 Goel et al.
periodontal tissue. IOPA at 24 months showed complete healing of theperiapical lesion. It has been shown that IOPAs overestimate bony healing(18). Therefore, a CBCT scan was done at the 30-month follow-up visit toevaluate the true extent of formation of periapical bone. The results of theCBCT scan were very encouraging (Fig. 4E–H). Continuity of periodontalligament space was observed. Labial and palatal cortical plates hadformed completely. Intercortical bone had also formed.
Earlier, nonsurgical root canal treatment of teeth with severe DIwas considered unfeasible. The treatment options were limited to end-odontic surgery or extraction. The advances in endodontic armamen-tarium and technology have made minimally invasive treatment ofsuch anomalies possible. This case shows that class II DI with anopen apex associated with extensive periapical lesion can be treatednonsurgically with aid of CBCT, operating microscope, PRF, and Bio-dentine with a successful 30-month follow-up.
AcknowledgmentsThe authors deny any conflicts of interest related to this study.
References1. Hulsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and
treatment considerations. Int Endod J 1997;30:79–90.2. Shafer WG, Hine MK, Levy BM. A textbook of pathology, 4th ed. Philadelphia: WB
Saunders; 1983.3. Hovland EJ, Block R. Nonrecognition and subsequent endodontic treatment of dens
invaginatus. J Endod 1977;3:360–2.4. Oehlers FA. Dens Invaginatus (dilated composite odontome): variations of the
invagination process and associated anterior crown forms. Oral Surg Oral MedOral Pathol 1957;10:1204–18.
5. Nallapati S. Clinical management of a maxillary lateral incisor with vital pulp andtype 3 dens invaginatus: a case report. J Endod 2004;30:726–31.
6. Kaneko T, Sakaue H, Okiji T, Suda H. Clinical management of dens invaginatus in amaxillary lateral incisor with the aid of cone-beam computed tomography: a casereport. Dent Traumatol 2011;27:478–83.
7. Patel S. The use of cone beam computed tomography in the conservative manage-ment of dens invaginatus: a case report. Int Endod J 2010;43:707–13.
8. VannierW, Hildebolt C, Conover G, et al. Three-dimensional dental imaging by spiral CT: aprogress report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84:561–70.
9. Sponchiado ECJ, Ismail HA, Braga MR, et al. Maxillary central incisor with two rootcanals: a case report. J Endod 2006;32:1002–4.
10. Mortman RE. Technologic advances in endodontics. Dent Clin North Am 2011;55:461–80. vii–viii.
11. Roth JS. CBCT technology: endodontics and beyond, part I. Dent Today 2011;30:146, 148, 150–1.
12. Roth JS. CBCT technology: endodontics and beyond, part 2. Dent Today 2011;30:78.80–3.
13. Biodentine. Scientific file. Active Biosilicate TechnologyTM. Saint-Maur-des-Fosses Cedex. France: Septodont R&D Department; 2010.
14. Nayak G, Hasan MF. Biodentine—a novel dentinal substitute for single visit apexi-fication. Restor Dent Endod 2014;39:120–5.
15. Vidal K, Martin G, Lozano O, et al. Apical closure in apexification: a review and casereport of apexification treatment of an immature permanent tooth with Biodentine.J Endod 2016;42:730–4.
16. Chande KP, Manwar NU, Chandak MG, Lokade J. Retreatment of a mutilated toothwith open apex by using PRF, MTA and anatomic post. Int J Prosthodont RestorDent 2013;3:105–10.
17. Choukroun J, Adda F, Schoeffer C, Vervelle A. PRF: an opportunity in perio-implan-tology. Implantodontie 2000;42:55–62 [in French].
18. Davies A, Patel S, Foschi F, et al. The detection of periapical pathoses using digital peri-apical radiography and cone beam computed tomography in endodontically retreatedteeth—part 2: a 1-year post-treatment follow-up. Int Endod J 2016;49:623–35.
19. Greenfeld RS, Cambruzzi JV. Complexities of endodontic treatment of maxillarylateral incisors with anomalous root formation. Oral Surg Oral Med Oral PatholOral Radiol Endod 1986;62:82–8.
20. Sabrah AH, Yassen GH, Spolnik KJ, et al. Evaluation of residual antibacterial effect ofhuman radicular dentin treated with triple and double antibiotic pastes. J Endod2015;41:1081–4.
JOE — Volume 43, Number 10, October 2017

Case Report/Clinical Techniques
21. Bonte E, Beslot A, Boukpessi T, Lasfargues JJ. MTA versus Ca(OH)2 in apexificationof non-vital immature permanent teeth: a randomized clinical trial comparison. ClinOral Investig 2015;19:1381–8.
22. Margunato S, Taslı PN, Aydın S, et al. In vitro evaluation of ProRoot MTA, Bio-dentine, and MM-MTA on human alveolar bone marrow stem cells in terms ofbiocompatibility and mineralization. J Endod 2015;41:1646–52.
23. Jang YE, Lee BN, Koh JT, et al. Cytotoxicity and physical properties of tricalciumsilicate-based endodontic materials. Restor Dent Endod 2014;39:89–94.
24. Butt N, Talwar S, Chaudhry S, et al. Comparison of physical and mechanical proper-ties of mineral trioxide aggregate and Biodentine. Indian J Dent Res 2014;25:692–7.
25. Chang IC, Tsai CH, Chang YC. Platelet-rich fibrin modulates the expression of extra-cellular signal-regulated protein kinase and osteoprotegerin in human osteoblasts.J Biomed Mater Res A 2010;95:327–32.
JOE — Volume 43, Number 10, October 2017
26. Tsai CH, Shen SY, Zhao JH, Chang YC. Platelet-rich fibrin modulates cell prolifera-tion of human periodontally related cells in vitro. J Dent Sci 2009;4:130–5.
27. Huang FM, Yang SF, Zhao JH, Chang YC. Platelet-rich fibrin increases proliferationand differentiation of human dental pulp cells. J Endod 2010;36:1628–32.
28. Agrawal PK, Wankhade J, Warhadpande M. A rare case of type III dens invaginatus ina mandibular second premolar and its nonsurgical endodontic management by us-ing cone-beam computed tomography: a case report. J Endod 2016;42:669–72.
29. Yadav P, Pruthi PJ, Naval RR, et al. Novel use of platelet-rich fibrin matrix and MTA asan apical barrier in the management of a failed revascularization case. Dent Trau-matol 2015;21:328–31.
30. Rudagi KB, Rudagi B. One-step apexification in immature tooth using grey mineraltrioxide aggregate as an apical barrier and autologous platelet rich fibrin membraneas an internal matrix. J Conserv Dent 2012;15:196–9.
DI Type II Management Using PRF and Biodentine 1755