Embed Size (px)
Citation preview

15Management of Ballistic Trauma tothe Head
Chris J. Neal, Geoffrey S.F. Ling, and James M. Ecklund
325
Introduction
Historically, the vast majority of penetrating head injuries (PHI) resultedfrom military combat operations; however, during the latter part of thetwentieth century, these injuries have increased in incidence in civiliantrauma centers. The difference in military and civilian PHI is often thenature of the penetrating projectile. In a combat situation, a majority ofpenetrating missile wounds are from either explosive munitions producinglow-velocity fragmentation injuries or high-velocity bullets fired from vari-ous ranges.1 Civilian gunshot wounds primarily result from low-velocitybullets fired at close range, typically from handguns.2 This accounts for asignificant proportion of civilian injuries in the form of homicides, suicides,and accidents, with an estimated 2.4 deaths per 100000 each year in theUnited States.3,4 With the recent increased threat of terrorist attacks, thepenetrating and blast injuries traditionally seen during military conflictsmay become more frequently seen in some civilian centers. As a conse-quence of the large number of patients with PHI treated during wartime, anumber of the advances and refinements in the care of these patients haveemerged from the military experience.
Prior to 1900, PHIs generally were considered fatal. MacCleod reporteda 100% mortality in 86 cases of penetrating or perforating head injuryduring the Crimean War. During the American Civil War, the death ratefrom pyremia of wounds to the head was as high as 95% in some series.Few surgical interventions were performed because of the high rate ofinfectious complications. The introduction of Lister’s antiseptic techniquein 1867, more sophisticated understanding of cerebral localization duringthe late 1800s, advances in surgical technique during World War I (WWI),and antibiotics during World War II (WWII) gradually led to new optimismregarding the care of these patients.5,6
Major Harvey Cushing encouraged the systematic evaluation and treat-ment of patients with PHI during WWI. He emphasized the importance ofearly meticulous debridement of all devitalized tissue and removal of all

visualized fragments of bone and/or metal.The application of his techniquesreduced the operative mortality from 56% to 28% within 3 months at BaseCamp 5.5–9
World War II brought with it the broad application of antibiotics and theimportance of dural repair. Operative mortality was reduced to 14.5%during this conflict.10,11
During the Korean War, an improved medical evacuation system and theeventual placement of neurosurgeons in combat zones resulted in moreimmediate surgical interventions. This early intervention proved especiallyefficacious in the treatment of intracranial hematomas and resulted in fewerinfectious complications. Surgical mortality was reduced to as low as 10%in some series during this conflict.12
As a result of anecdotal reports describing delayed abscess developmentin PHI from WWII and Korea, the practice of aggressively removing allbone and metallic fragments in an attempt to reduce postoperative infec-tion was mandated in the U.S. Army during Vietnam. This approach some-times subjected a patient to multiple operations and occasional increasedoperative morbidity for what was felt to be an “adequate” debridement.13
Critical review of the results of patients at five and 14 years in the VietnamHead Injury Study (VHIS) ultimately showed no difference in rates ofinfection or seizures in those patients with retained bone or metallic frag-ments as seen on computed tomography (CT).
This data was applied during the Israeli–Lebanese conflict where Branvold and colleagues14 described a debridement strategy in 113 patientsbased on preservation of viable tissue with limited debridement. Fragmentswere removed with gentle irrigation and fragments that were not easilyobtainable were left. Of the 43 patients with long-term follow up, there wasa 51% incidence of retained fragments and no relationship to the develop-ment of intracranial abscess formation. Additionally, there was not anincreased incidence of posttraumatic epilepsy with retained bone frag-ments.14 These important experiences were instrumental in the evolution ofthe modern surgical management of PHI.
Ballistics
To understand penetrating trauma, it is important to have a basic under-standing of ballistics. Wound ballistics is the study of the projectile’s actionin human tissue. The ballistic properties of a projectile are dependent pri-marily on its velocity, size, and shape. The primary injury to the brain isrelated directly to these properties. Secondary projectiles such as skull frag-ments may cause further damage.
Penetrating head injury can result from both low- and high-velocity pro-jectiles. Lower-velocity sharp projectiles such as arrows (120 to 250 feet persecond) create a tract of primary tissue damage without significant bruis-
326 C.J. Neal et al.

ing or blunt tearing of surrounding tissue. Higher-velocity projectiles arepreceded by a brief (2 ms) sonic shock wave, followed by the penetrationof the projectile. In addition to the destruction of tissue in the projectile’spath, there is a transmission of kinetic energy resulting in a temporary cav-itation effect. In brain tissue, which is relatively inelastic, the cavity is often10 to 20 times the size of the projectile.After expansion, the cavity collapsesunder negative pressure that may draw in external debris.
The size of the cavity is dependent on the kinetic energy of the projec-tile. Kinetic energy (KE) can be expressed in the equation KE = 1/2 mv2.While mass is directly proportional to the kinetic energy, it is the velocitythat is its key determinant.15,16 The shape of the projectile determines theballistic coefficient, which is its ability to overcome air resistance and main-tain velocity. The shape also influences the yaw, which is the projectile’srotation around its long axis. While small amounts of circular motion (pre-cession and nutation) occur during flight, projectiles often will tumble whenstriking tissue.Yaw is maximized when the projectile is rotated at 90 degreesto its long axis.15,16 This imparts more kinetic energy to the tissue, increasesthe size of the temporary cavity, and increases tissue destruction.
For example, a .45 automatic pistol (muzzle velocity of 869 feet persecond and a short round-nosed projectile with little yaw) will create a verysmall temporary cavity; conversely, a 7.62 millimeter North Atlantic TreatyOrganization (NATO) rifle (muzzle velocity 2830 feet per second and a longsharp nose with maximum yaw) will create a very large temporary cavity.
Projectiles also can deform or fragment upon striking tissue. Copper jack-eting lead bullets, as mandated for military rounds by The Hague PeaceConference (1899), helps limit the fragmentation potential. Irregularitiesmade by scoring the surface of the bullet (dum dums) lead to increasedfragmentation, creating multiple injury tracts as each fragment becomes anew projectile. The Glaser round is filled with small pellets that disperse onimpact. Hollow-point rounds, often seen in civilian shootings, expand theirdiameter in the direction of flight upon impact, thus creating a largerprimary wound tract and more destructive temporary cavitation effects.Explosive bullets such as the Devastator round are designed to detonateon impact and thus will produce extensive tissue injury with additionalkinetic energy transfer.17
Injury Classification
Since WWI, PHIs have been classified in an attempt to correlate the typeof injury with prognosis. Cushing’s original classification of nine differentinjury patterns was refined by Matson in WWII to four categories, whichare explained in Table 15-1.
Currently, a PHI is described as a tangential wound, a penetrating wound,or a perforating wound.
15. Management of Ballistic Trauma to the Head 327
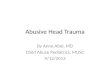
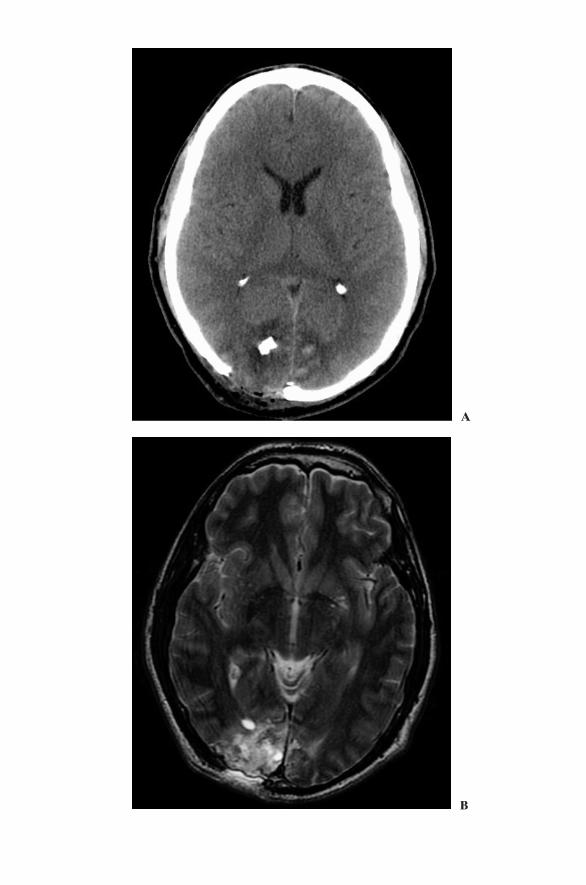
Tangential WoundA tangential wound (Figure 15-1) occurs when a projectile strikes the headat an oblique angle and may produce scalp lacerations, skull fractures, andcerebral contusions. The projectile may traverse the subgaleal space andexit or remain lodged in the scalp. The presence of a hematoma, depressedskull fracture, or cerebrospinal fluid (CSF) leak may necessitate surgicalintervention. Otherwise, local wound care may be applied. These injuriesgenerally carry a better prognosis with less severe neurological deficits, butthey may present with seizures or focal deficit depending on location andextent of injury.
328 C.J. Neal et al.
Table 15-1. Cushing and Matson’s classification of craniocerebral injuriesGrade Cushing (WW I) Grade Matson (WW II)
Description Description
I Scalp lacerations, skull intact I Scalp woundII Skull fractures, dura intact II Skull fracture, dura intactIII Depressed skull fracture and III Skull fracture with dural/brain
dural laceration penetrationA: Gutter-type (grazing)—in-driven
bone with no missile fragmentsB: Penetrating—missile fragments in
brainC: Perforating—through and through
IV In-driven bone fragments IV Complicating factors:V Penetrating wound with A: Ventricular penetration
projectile lodged B: Fractures of orbit or sinusVI Wounds penetrating C: Injury of dural sinus
ventricles with: D: Intracerebral hematomaA: Bone fragmentsB: Projectile
VII Wounds involving :A: Orbitonasal regionB: Auropetrosal region
VIII Perforating WoundsIX Bursting Skull Fracture,
extensive cerebralcontusion
Figure 15-1. (A) CT of tangential wound to right occipital region from AK47 whilewearing military helmet. Wound was emergently debrided at nearby field hospital.Note the in-driven bone fragments. (B) MRI of same patient revealing underlyingcontusion after CT confirmation of no residual metal fragments.
�
A
B

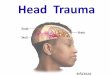
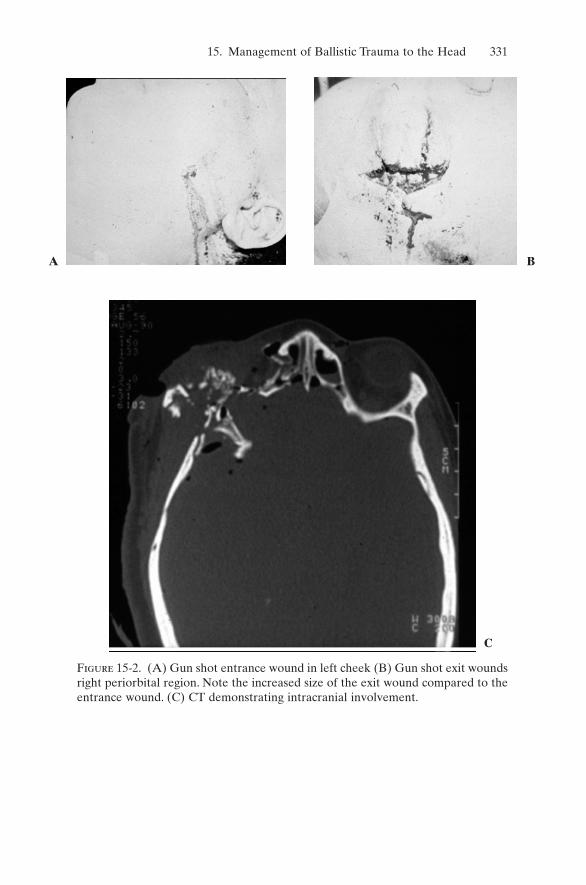
Penetrating WoundThe velocity of the projectile is the main determinant of its energy. If theprojectile has enough energy to only penetrate the brain parenchyma, theinjury is referred to as penetrating. Energy absorbed by the skull oftenresults in fragments of bone that act as secondary projectiles within thebrain. Contusions, lacerations, or hematomas may be caused by theseinjuries (Figure 15-2).
Depending on the amount of energy, the projectile may produce unusualtracts within the calvaria that may be detected on CT, but missed on plainfilms. The projectile may ricochet after hitting the inner table opposite ofits entry, creating a new tract within the parenchyma. It also may changedirections when it hits dura after penetrating the outer and inner tables ofthe skull. This unusual occurrence is called careening. The projectile thentravels along the inner table of the skull, with the potential to damage thevenous sinuses.
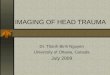
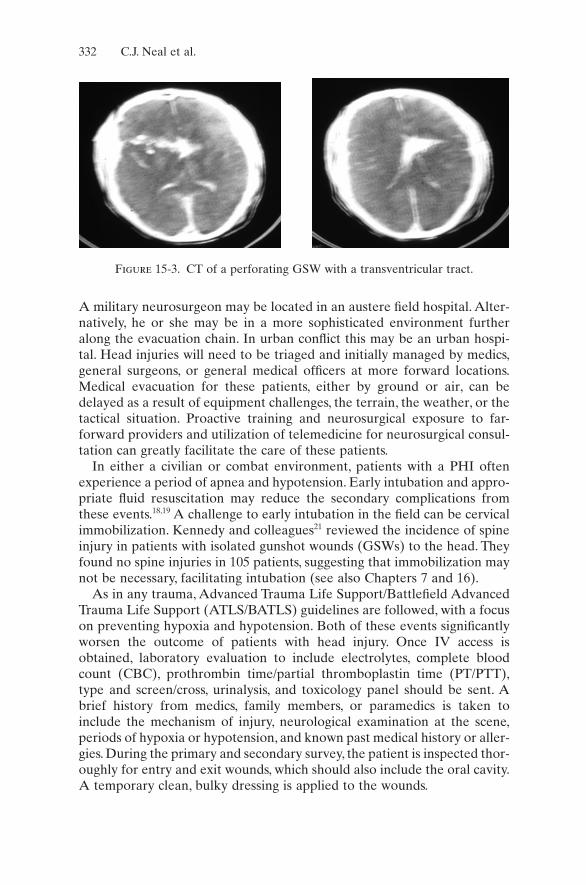
Perforating WoundThe most destructive pattern of injury is the perforating wound (Figure 15-3), which is defined by an entry and exit wound with a tract through brainparenchyma. This injury requires a higher-velocity projectile than with apenetrating injury, and thus imparts a higher amount of kinetic energy tothe tissue. Local and distant structures are damaged from the cavitationeffect the projectile imparts, resulting in multiple fractures, contusions, andhematomas.
Initial Resuscitation and Management
In civilian trauma, activation of the local emergency medical service (EMS)system allows initial resuscitation efforts to be made in the field to includeintravenous (IV) access and intubation when warranted. The use of a heli-copter allows for faster transport from the scene or outlying hospital to aneurosurgical center for early intervention.18,19
A combat situation provides a different operating environment for PHIs.Initial care is provided by a medic carrying limited supplies and diagnosticequipment. In contrast to civilian systems, combat injuries are triaged in thefield and at every level of care. Due to limited capabilities, the goal ofcombat medicine is to do the greatest good for the most people, thus main-taining the fighting force. If a patient is triaged as expectant, they are notprioritized for rapid evacuation, allowing those resources to be shifted toother, salvageable patients. Military neurosurgeons are viewed as assets,deployed where most beneficial.20 Depending on the theater of operations,neurosurgical support may be located at a variety of locations or echelons.
330 C.J. Neal et al.
15. Management of Ballistic Trauma to the Head 331
Figure 15-2. (A) Gun shot entrance wound in left cheek (B) Gun shot exit woundsright periorbital region. Note the increased size of the exit wound compared to theentrance wound. (C) CT demonstrating intracranial involvement.
A B
C
A military neurosurgeon may be located in an austere field hospital. Alter-natively, he or she may be in a more sophisticated environment furtheralong the evacuation chain. In urban conflict this may be an urban hospi-tal. Head injuries will need to be triaged and initially managed by medics,general surgeons, or general medical officers at more forward locations.Medical evacuation for these patients, either by ground or air, can bedelayed as a result of equipment challenges, the terrain, the weather, or thetactical situation. Proactive training and neurosurgical exposure to far-forward providers and utilization of telemedicine for neurosurgical consul-tation can greatly facilitate the care of these patients.
In either a civilian or combat environment, patients with a PHI oftenexperience a period of apnea and hypotension. Early intubation and appro-priate fluid resuscitation may reduce the secondary complications fromthese events.18,19 A challenge to early intubation in the field can be cervicalimmobilization. Kennedy and colleagues21 reviewed the incidence of spineinjury in patients with isolated gunshot wounds (GSWs) to the head. Theyfound no spine injuries in 105 patients, suggesting that immobilization maynot be necessary, facilitating intubation (see also Chapters 7 and 16).
As in any trauma, Advanced Trauma Life Support/Battlefield AdvancedTrauma Life Support (ATLS/BATLS) guidelines are followed, with a focuson preventing hypoxia and hypotension. Both of these events significantlyworsen the outcome of patients with head injury. Once IV access isobtained, laboratory evaluation to include electrolytes, complete bloodcount (CBC), prothrombin time/partial thromboplastin time (PT/PTT),type and screen/cross, urinalysis, and toxicology panel should be sent. Abrief history from medics, family members, or paramedics is taken toinclude the mechanism of injury, neurological examination at the scene,periods of hypoxia or hypotension, and known past medical history or aller-gies. During the primary and secondary survey, the patient is inspected thor-oughly for entry and exit wounds, which should also include the oral cavity.A temporary clean, bulky dressing is applied to the wounds.
332 C.J. Neal et al.
Figure 15-3. CT of a perforating GSW with a transventricular tract.
15. Management of Ballistic Trauma to the Head 333
A brief neurological exam is performed, remembering that the patientshould be fully resuscitated before determining a prognosis. The patient’sGlascow Coma Scale (GCS) score, the presence of hypotension or hypoxia,and any use of pharmacological agents should be noted.22 If the patient hasa GCS score of less than 8 or cannot otherwise protect their airway, intu-bation for adequate airway protection, oxygenation, and ventilation shouldbe considered. Brainstem reflexes and pupillary exam, to include size, sym-metry, and reactivity, are noted. Evaluation for CSF leak is performed atthis point, including inspection of the tympanic membranes and nares.Antiepileptic agents and broad-spectrum antibiotics are administered.
Neuroimaging
Plain radiographic studies of the skull can provide a quick impression of thenature of the injury and evaluate for the presence of intracranial fragmentsand air, especially in circumstances where a CT scan is unavailable.The truetrajectory of the fragment may be misleading in the presence of ricochet orcareening fragments (Figures 15-4 and 15-5).23 If rapid access to a CT scanneris possible, plain films are not required. Noncontrast CT with bone windowsallow for precise localization of bone and projectile fragments, identificationof the trajectory, and characterization of brain injury (Figure 15-5). The presence of mass effect and classification of hematomas, either epidural,subdural, parechymal, or intraventricular, can be performed.23
Angiography is recommended when there is a high suspicion for vascu-lar injury. From Aarabi’s experience in the Iran–Iraq war, there was a 4 to 10 time increased risk of traumatic aneurysm development in patientswith facio-orbito or pterional entry, intracranial hematoma, or projectile
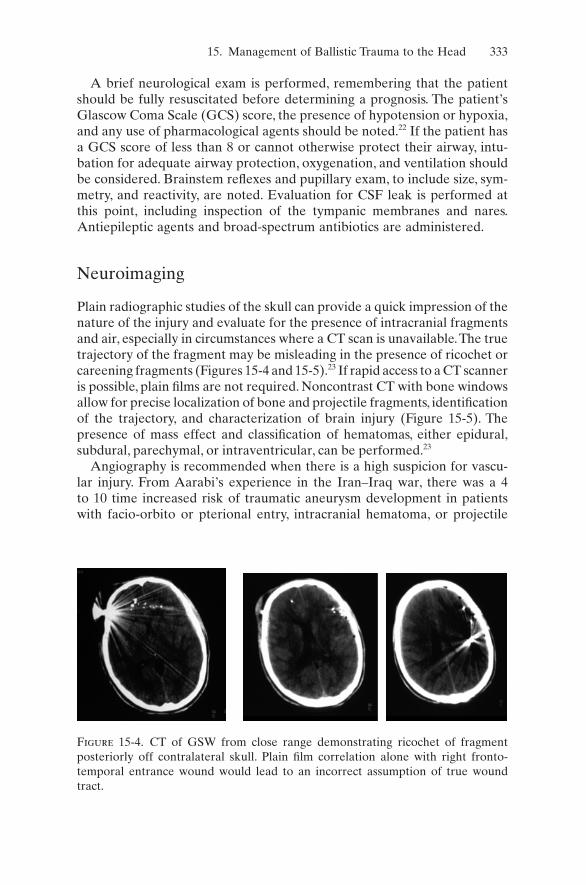
Figure 15-4. CT of GSW from close range demonstrating ricochet of fragment posteriorly off contralateral skull. Plain film correlation alone with right fronto-temporal entrance wound would lead to an incorrect assumption of true woundtract.
334 C.J. Neal et al.
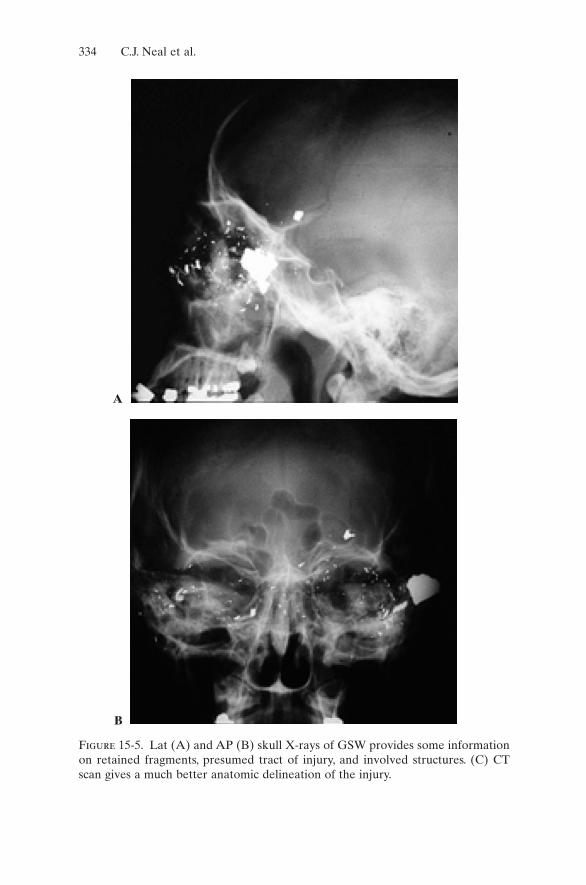
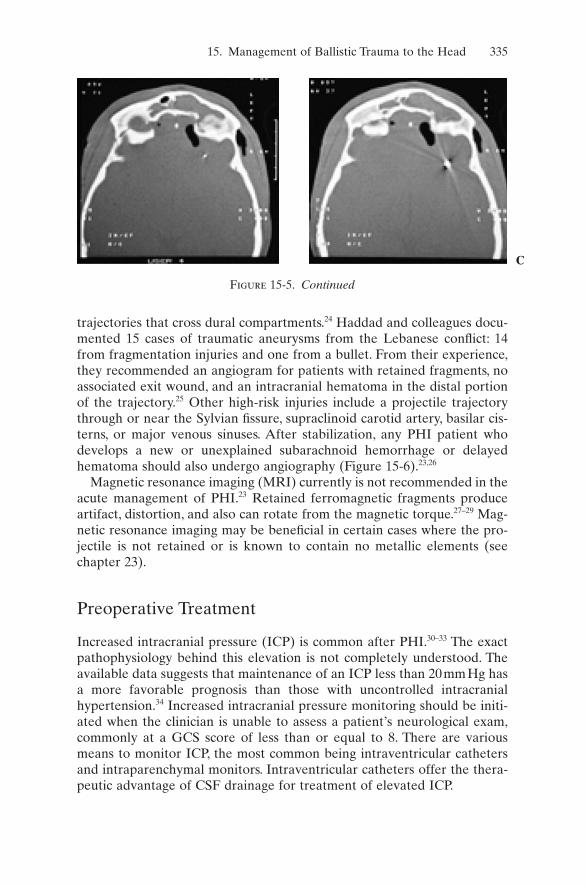
Figure 15-5. Lat (A) and AP (B) skull X-rays of GSW provides some informationon retained fragments, presumed tract of injury, and involved structures. (C) CTscan gives a much better anatomic delineation of the injury.
A
B
15. Management of Ballistic Trauma to the Head 335
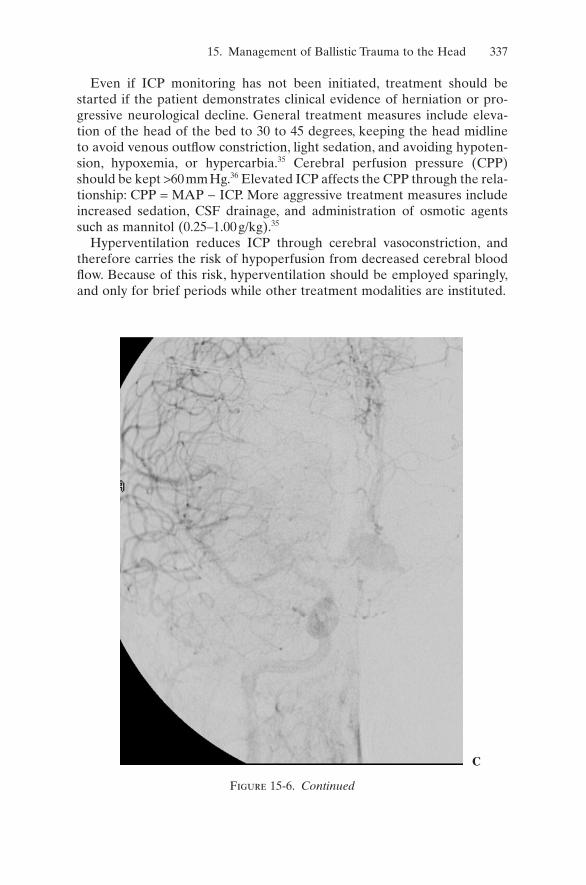
trajectories that cross dural compartments.24 Haddad and colleagues docu-mented 15 cases of traumatic aneurysms from the Lebanese conflict: 14from fragmentation injuries and one from a bullet. From their experience,they recommended an angiogram for patients with retained fragments, noassociated exit wound, and an intracranial hematoma in the distal portionof the trajectory.25 Other high-risk injuries include a projectile trajectorythrough or near the Sylvian fissure, supraclinoid carotid artery, basilar cis-terns, or major venous sinuses. After stabilization, any PHI patient whodevelops a new or unexplained subarachnoid hemorrhage or delayedhematoma should also undergo angiography (Figure 15-6).23,26
Magnetic resonance imaging (MRI) currently is not recommended in theacute management of PHI.23 Retained ferromagnetic fragments produceartifact, distortion, and also can rotate from the magnetic torque.27–29 Mag-netic resonance imaging may be beneficial in certain cases where the pro-jectile is not retained or is known to contain no metallic elements (seechapter 23).
Preoperative Treatment
Increased intracranial pressure (ICP) is common after PHI.30–33 The exactpathophysiology behind this elevation is not completely understood. Theavailable data suggests that maintenance of an ICP less than 20mmHg hasa more favorable prognosis than those with uncontrolled intracranialhypertension.34 Increased intracranial pressure monitoring should be initi-ated when the clinician is unable to assess a patient’s neurological exam,commonly at a GCS score of less than or equal to 8. There are variousmeans to monitor ICP, the most common being intraventricular cathetersand intraparenchymal monitors. Intraventricular catheters offer the thera-peutic advantage of CSF drainage for treatment of elevated ICP.
Figure 15-5. Continued
C
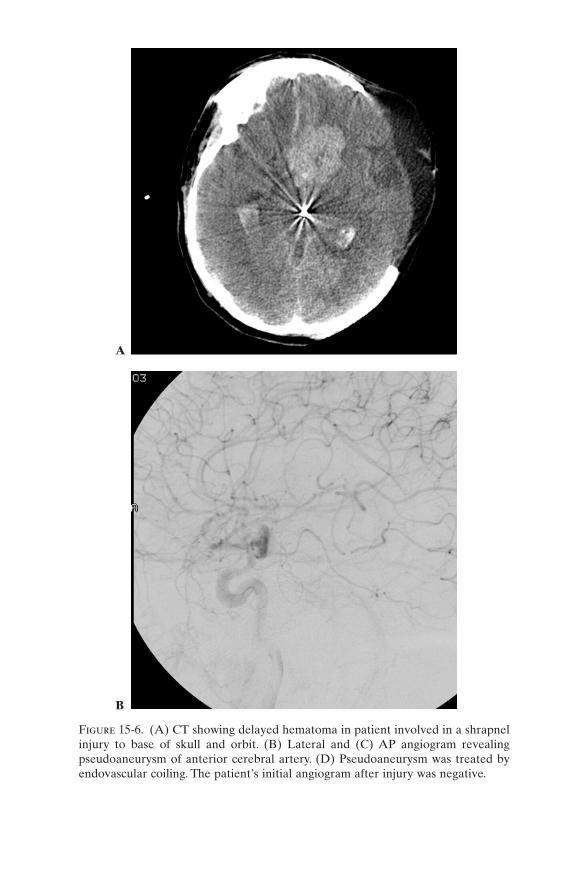
Figure 15-6. (A) CT showing delayed hematoma in patient involved in a shrapnelinjury to base of skull and orbit. (B) Lateral and (C) AP angiogram revealingpseudoaneurysm of anterior cerebral artery. (D) Pseudoaneurysm was treated byendovascular coiling. The patient’s initial angiogram after injury was negative.
A
B
15. Management of Ballistic Trauma to the Head 337
Even if ICP monitoring has not been initiated, treatment should bestarted if the patient demonstrates clinical evidence of herniation or pro-gressive neurological decline. General treatment measures include eleva-tion of the head of the bed to 30 to 45 degrees, keeping the head midlineto avoid venous outflow constriction, light sedation, and avoiding hypoten-sion, hypoxemia, or hypercarbia.35 Cerebral perfusion pressure (CPP)should be kept >60mmHg.36 Elevated ICP affects the CPP through the rela-tionship: CPP = MAP - ICP. More aggressive treatment measures includeincreased sedation, CSF drainage, and administration of osmotic agentssuch as mannitol (0.25–1.00g/kg).35
Hyperventilation reduces ICP through cerebral vasoconstriction, andtherefore carries the risk of hypoperfusion from decreased cerebral bloodflow. Because of this risk, hyperventilation should be employed sparingly,and only for brief periods while other treatment modalities are instituted.
Figure 15-6. Continued
C
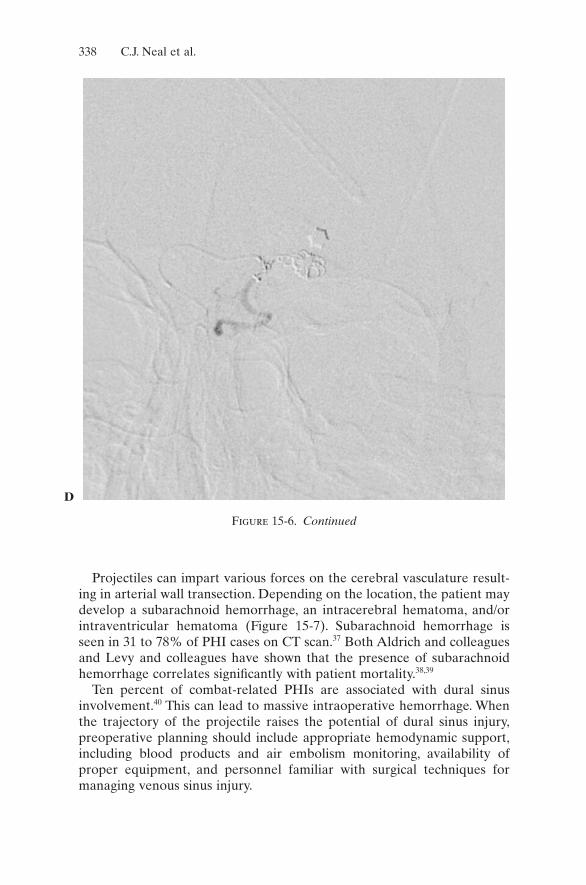
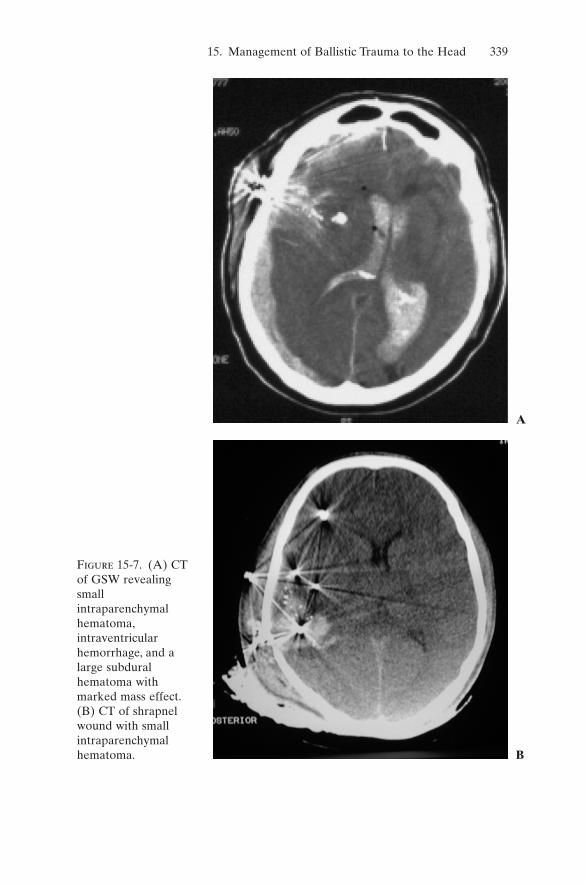
Projectiles can impart various forces on the cerebral vasculature result-ing in arterial wall transection. Depending on the location, the patient maydevelop a subarachnoid hemorrhage, an intracerebral hematoma, and/orintraventricular hematoma (Figure 15-7). Subarachnoid hemorrhage is seen in 31 to 78% of PHI cases on CT scan.37 Both Aldrich and colleaguesand Levy and colleagues have shown that the presence of subarachnoidhemorrhage correlates significantly with patient mortality.38,39
Ten percent of combat-related PHIs are associated with dural sinusinvolvement.40 This can lead to massive intraoperative hemorrhage. Whenthe trajectory of the projectile raises the potential of dural sinus injury,preoperative planning should include appropriate hemodynamic support,including blood products and air embolism monitoring, availability ofproper equipment, and personnel familiar with surgical techniques for managing venous sinus injury.
338 C.J. Neal et al.
Figure 15-6. Continued
D
15. Management of Ballistic Trauma to the Head 339
Figure 15-7. (A) CTof GSW revealingsmallintraparenchymalhematoma,intraventricularhemorrhage, and alarge subduralhematoma withmarked mass effect.(B) CT of shrapnelwound with smallintraparenchymalhematoma. B
A

Traumatically induced pseudoaneurysms or traumatic intracranialaneurysms (TICA) may occur, with 0.4 to 0.7% of all intracranialaneurysms caused by trauma, 20% of these from PHI.24,37 The incidence ofTICAs is reported between 3 and 33.3% in PHI patients.24,26,41,42 Angiog-raphy is the standard in detection of vascular injuries, but a singleangiogram does not rule out the possibility of a TICA.24,26,41 Since TICAsare not usually true aneurysms, clipping may not be effective. Endovascu-lar techniques or trapping of the lesion are alternative treatment options.
Seizures are common after PHI. They are typically divided into early andlate; early defined loosely in the literature as within the first seven days.Between 30 and 50% of PHI patients develop seizures. Four to 10% of theseare early seizures while 80% occur within the first two years.43,44 Data fromthe VHIS indicated that after 15 years of follow up, nearly 50% of PHIpatients with epilepsy stopped having seizures.44 If PHI patients do not haveseizures within the first three years, 95% will remain seizure free.45 Fewstudies exist that examine only PHI patients and the use of prophylacticantiepileptic drugs. The current guidelines extrapolated from those patientswith nonpenetrating traumatic brain injury recommend antiepileptic drugsduring the first week to prevent early posttraumatic seizures. No data sup-ports the use of these medications prophylatically beyond the first sevendays in the PHI population to prevent late posttraumatic seizures.46
Penetrating head injury wounds are considered contaminated, bothsuperficially and deep. Negative pressure from the cavity caused by the projectile can draw superficial contaminant and debris deep into the wound.The primary projectile, either bullet or fragment, that remains intracranialis not sterile; insufficient heat is generated from the firing mechanism andhigh velocity for adequate sterilization.47,48 Broad-spectrum antibiotics areinitiated as soon as possible. In civilian PHI, coverage for Staphylococcusand Streptococcus should be of primary concern. With military combatinjuries, coverage should also include Acinetobacter, and may be furtherbroadened depending on the area of operations.49,50
Surgical Management
The foundation for surgical management of PHI is found in the work per-formed by Cushing during WWI: craniectomy, thorough debridement ofdevitalized scalp, bone, brain, metal and bony fragments, and meticulousclosure. This approach remained relatively unchanged through Vietnam.Data from the VHIS and modern military conflicts do not support vigor-ous removal of all bone and metallic fragments or repeat craniotomiessolely for removal of additional fragments. Debridement should be confinedto nonviable brain, with removal of readily accessible fragments of boneand metal.51
340 C.J. Neal et al.
Taha and colleagues reported on a subset of PHI patients that weretreated with simple wound closure and a three-day course of IV antibi-otics.52 Patients met the following criteria: initial GCS score greater than 10,presented within six hours of injury, entry wound less than two centimeters,no exit wound, trajectory not through the proximal Sylvain fissure, and nosignificant intracranial hematoma. These criteria attempted to eliminatepatients whose injury would produce a significant amount of devitalizedtissue. Out of 32 patients, they reported no deaths and one brain abscessthat ultimately was treated without complication. Local wound care andclosure is a treatment option recognized by the Guidelines of PenetratingBrain Injury for similarly selected patients.
The early identification and evacuation of hematomas is important ineffecting the outcome of PBI. Some authors have stated that the only indi-cation for surgery, outside of wound care, is the reduction of mass effect,and thus intracranial pressure, from a hematoma.33,54 The rapid evacuationof hematomas creating significant mass effect is the standard practice. If ahematoma is not removed in a salvageable patient, ICP monitoring shouldbe considered to confirm the decision and to guide further therapy.
All PHI patients should be evaluated vigorously and monitored contin-uously for the presence of a CSF leak. In a report based on the VHIS, only50% of CSF leaks were located at the wound site. The remaining wereassumed to be caused by injury from the projectile’s concussive effect.32
Mortality for these patients was 22.8% versus 5.1% for those without a CSFleak. The presence of a CSF leak is the variable most highly correlated withintracranial infection in PHI patients. In the VHIS, 44% of the fistulasclosed spontaneously.55 However, if the leak is persistent or delayed inonset, treatment with either CSF diversion or direct surgical repair shouldbe instituted. During any primary surgical treatment of PHI a meticulous,watertight closure of the dura, including the use of temporalis fascia, fascialata, or graft material, is essential.
Air sinus injuries present an increased risk for CSF leak, especially withan orbital-facial wound. Analysis of a two-year period during the KoreanWar revealed a 15% incidence of air sinus injury with combat PHI.56 Delayin repair of this injury increases the risk of infection.7,8,10,56 Management mayinclude craniotomy and anterior fossa reconstruction, exoneration of thefrontal sinus, and watertight dural closure. For temporal bone injuries, amastoidectomy or middle ear exploration with Eustachian tube packingmay be required.
Postoperative Care
Postoperatively, the patient is monitored in an intensive-care setting. Asmentioned, ICP is monitored and treated for a goal ICP of less than 20mmHg and CPP of greater than 60mmHg.36 Any persistent, unexplained
15. Management of Ballistic Trauma to the Head 341

elevation in ICP or deterioration in neurologic status warrants an emergentCT scan of the head to identify a new mass lesion, most typically a delayedhematoma. A new hemorrhage after surgery should raise the suspicion ofan underlying vascular injury or coagulopathy. In certain cases, typicallyyoung patients with nondominant hemisphere lesions, a decompressivecraniectomy, and duroplasty may be considered in refractory increasedintracranial pressure.
The development of hydrocephalus is another potential complication. Ina patient with a ventriculostomy, the inability to wean over 7 to 14 days withpersistent high CSF outflow at normal pressure is a good indication thepatient will need CSF diversion. Hydrocephalus also may develop in adelayed fashion with a slowly deteriorating neurological exam. If the CTreveals ventriculomegaly, including an enlarged fourth ventricle with nofocal mass effect, a lumbar puncture may be performed to record an openingpressure. The final timing for definitive CSF diversion is determined by thepresence of other injuries, nutritional status, and infectious complications.
The presence of fever, elevated white cell count, and meningeal signs areconcerns for postoperative meningitis. If a ventriculostomy is in place, CSFmay be sent for laboratory inquiry. In addition to evaluating the ICP mon-itoring system, a thorough examination for a CSF fistula should be per-formed. Not all CSF leaks are present on admission. In a review of theVHIS, 72% of CSF leaks appear within the first two weeks of injury.55
In the initial evaluation and postoperative period, a coagulation panelshould be evaluated, as PHI is a known etiology for coagulopathy.The brainparenchyma contains thromboplastin that can activate the extrinsic coagu-lation cascade. If high levels are released, the patient may develop a dis-seminated intravascular coagulopathy (DIC). Because the degree of thecoagulopathy is related to the amount of thromboplastin released frominjured tissue, the presence of DIC represents a large area of parechymalinjury and portends a worse prognosis.19,57
As discussed above, the patient should remain on antiepileptic medica-tion for seven days post injury for the prevention of early seizures. Antibi-otics generally are used for a 7 to 14 day course for isolated PHI. A longerduration may be required based on systemic infection or other complicat-ing factors.
Prognosis
In comparing outcomes with PHI patients and those with nonpenetratingtraumatic brain injuries, PHI patients fare worse.They have an overall mor-tality of 88%, compared to 32.5% in nonpenetrating traumatic braininjury.38,58 Typically, death occurs soon after the injury, with 70% occurringwithin the first 24 hours.58 An accurate assessment of prognosis for each
342 C.J. Neal et al.

patient is essential to determine the appropriateness of treatment, espe-cially in a military or other resource-constrained environment.
The Guidelines to Penetrating Brain Injuries evaluated the literature onfive prognostic variables: age, epidemiology, systemic measures, neurologi-cal measures, and neuroimaging measures. An understanding of these vari-ables and their outcome can help provide direction in the treatment of thepatient and counseling family members on what can be expected.
In general, the older a patient is, the higher mortality they typically have.In the limited studies that evaluated age and prognosis, age greater than 50years was associated with increased mortality. However, a majority of PHIpatients are in their second to third decade.58
In the civilian population, gunshot wounds are the most common type ofPHI, with a majority of these being suicide attempts. Suicide PHIs are asso-ciated with a higher mortality.58 The question has been raised whethersuicide outcomes are based on the injury pattern or the degree of resusci-tation based on the belief of a worse outcome.59 This pattern is different inmilitary PHI, where fragmentation injuries instead of gunshot wounds, arefound in those patients who survive transport to higher echelons of care.The high velocity associated with military bullet wounds typically causes adevastating intracranial wound. One series reported a mortality with thiswound to be 82% higher than with fragmentation wounds.14
Given the velocity, and hence the amount of energy imparted by a pro-jectile to achieve a perforating wound, it is not surprising that these injuriesare associated with the highest mortality. While no statistically significantdata exists, penetrating wounds tend to have a higher mortality than tan-gential.58 Surprisingly, there does not tend to be a correlation betweenoutcome and caliber of weapon. This is likely because the energy impartedto the tissue is also related to the velocity, which can be quite variable.58
From the patient’s presentation and neurological status, several poorprognostic indicators can be determined. Systemic insults after a PHI canworsen the patient’s outcome. Periods of hypotension, respiratory distress,and the presence of a coagulopathy are all associated with increased mor-tality.58 From a neurologic perspective, the patient’s GCS is one of thestrongest predictors of mortality and outcome.58 In civilian settings, mostpatients present with a GCS of 3 to 5. These patients have the highest rateof mortality and poor outcome. In military series, more patients presentwith GCS of 13 to 15, and thus have a better outcome. This reflects morefragment injuries, a more rigid field triage system, and a slower evacuationsystem. An abnormal pupillary exam is common after PHI and can resultfrom orbital trauma, medications, cerebral herniation, or brainstem injury.Patient who present with unequal or fixed and dilated pupils have anincreased mortality.58 There is little data that exists on the prognostic valueof ICP in PHI. What is available suggests that elevated ICP within the first72 hours predicts higher mortality.58
15. Management of Ballistic Trauma to the Head 343

As previously discussed, a CT scan is the diagnostic modality of choice.Three prognostic indicators can be determined from the patient’s initialscan: projectile track, evidence of increased ICP, and the presence of hem-orrhage or mass lesion. Projectile trajectories associated with increasedmortality include bihemispheric lesions, multilobar lesions, and those thatinvolve the ventricular system. One exception may be a bifrontal injury.Basilar cistern effacement on CT, indicative of elevated ICP, is associatedwith increased mortality. Midline shift alone, however, is not. The presenceof large contusions and/or subarachnoid hemorrhage is associated withincreased mortality. A stronger correlation, however, exists betweenincreased mortality and the presence of intraventricular hemorrhage.58
Given these prognostic indicators, the provider must decide on whowould benefit from surgery and aggressive management. Grahm and col-leagues reported on 100 consecutive cases of gunshot wounds to the headin an attempt to answer this question.18 No patient with a postresuscitationGCS of 3 to 5 and only 20% of those with GCS of 6 to 8 had a satisfactoryoutcome, defined as either good or moderately impaired on the GlasgowOutcome Scale. From their experience, they recommend that all patientswith gunshot wounds to the head be resuscitated aggressively and trans-ferred to a trauma center. Patients with a large, extraaxial hematoma,despite their GCS, should undergo surgical therapy. In those patientswithout a hematoma and a GCS of 3 to 5, no further treatment should beoffered. In patients with a GCS score of 6 to 8 and transventricular or dom-inant hemisphere multilobar injuries in the absence of an extraaxialhematoma, further treatment should not be offered. A patient with a GCSof 6 to 8 without these findings on CT and all those with GCS of 9 to 15should be offered aggressive therapy, as this is the population with the bestchance at a satisfactory outcome.18
The management of the patient with ballistic trauma to the head requiresaggressive resuscitation and accurate triage based on clinical and CT findings. When surgical intervention is required, strict attention must bepaid to the principles of watertight dural closure and wound coverage afteran adequate debridement of devitalized tissue and easily accessible frag-ments is completed. Aggressive intensive care unit management includesavoidance of hypotension, hypoxia, control of ICP and CPP, use of antibi-otics and anticonvulsants, and vigilant monitoring for CSF fistulas andpseudoaneurysms. Unfortunately, this current era of terrorist threats man-dates that all physicians should have a basic understanding of ballistictrauma to the head.
References1. Berman JM, Butterworth JF, Prough DS. Neurological injuries. In: Zajtchuk R,
Bellamy RF, eds. Textbook of Military Medicine. Vol. 1. Washington: Office ofthe Surgeon General; 1995:375–424.
344 C.J. Neal et al.

2. Shaffrey ME, Polin RS, Phillips CD, Germanson T, Shaffrey CI, Jane JA. Clas-sification of civilian craniocerebral gunshot wounds: A multivariate analysis predictive of mortality. J Neurotrauma. 1992;9(Suppl 1):S279–S285.
3. Cooper P. Gunshot wounds of the brain. In: Cooper P, ed. Head Injury. 2nd ed.Baltimore, MD: Williams and Wilkins; 1987:313–326.
4. Sosin D, Sacks J, Smith S. Head injury associated deaths in the United Statesfrom 1979–1986. JAMA. 1989;262L:2251–2255.
5. West CGH. A short history of the management of penetrating missile injuriesof the head. Surg Neurol. 1981;16:145–149.
6. Schmidek, Sweet. Operative neurosurgical techniques. Missile injury to headchapter.
7. Cushing H. Notes on penetrating wounds of the brain. Brit Med J. February1918;221–226.
8. Cushing H. A study of a series of wounds involving the brain and its envelop-ing structures. Br J Surg. 1918;5:558–684.
9. Tilney NL. The marrow of tragedy. Surg Gynecol Obstet. 1983:157:380–388.10. Matson DD. The Treatment of Acute Craniocerebral Injuries Due to Missiles.
Springfield, IL: Charles C Thomas; 1948.11. War Surgery Supplement. Br J Surg. 1947;34(137).12. Lewin W, Gibson MR. Missile head wounds in the Korean campaign: A survey
of British casualties. Br J Surg. 1956;43:628–632.13. Carey ME, Young HF, Mathis JL. The neurosurgical treatment of craniocere-
bral missile wounds in Vietnam. Surg Gynecol Obstet. 1972;135:386–390.14. Brandvold B, Levi L, Feinsod M, George E. Penetrating craniocerebral injuries
in the Israeli involvement in the Lebanese conflict, 1982–1985. J Neurosurg.1990;72:15–21.
15. Ordog, GJ. Wound ballistics: Theory and practice. Ann Emerg Med. 1984;13(12):1113–1122.
16. Barach E, Tomlanovich M, Nowak R. Ballistics: A pathophysiologic examina-tion of the wounding mechanisms of firearm: part 1. J Trauma. 1986;26(3):225–235.
17. Sykes LN, Champion HR, Fouty WJ. Dum-dums, hollow-points, and devastors:Techniques dsigned to increase wounding potential of bullets. J Trauma.1988;28(5):618–623.
18. Grahm T, Williams F Jr, Harrington T, Spetzler R. Civilian gunshot wounds tothe head: A prospective study. Neurosurgery. 1990;27:696–700.
19. Kauffman HH, Makela ME, Lee KF, Haid RW Jr, Gildenberg PL. Gunshotwounds to the head: A perspective. Neurosurgery. 1986;18:689–695.
20. Knightly JJ, Pullliam MW. Military head injuries. In: Narayan RK, WillbergerJE, Povlishock JT, eds. Neurotrauma. New York: McGraw-Hill; 1996:891–902.
21. Kennedy FR, Gonzalez P, Beitler A, Sterling-Scott R, Fleming AW. Incidenceof cervical spine injury in patients with gunshot wounds to the head. South MedJ. 1994;87:621–623.
22. Trask T, Narayan RK. Civilian penetrating head injury. In: Narayan RK,Wilberger JE, Povlishock JT, eds. Neurotrauma. New York: McGraw-Hill,1996:869–889.
23. Neuroimaging in the management of penetrating brain injury. J Trauma.2001;51:S7–S11.
15. Management of Ballistic Trauma to the Head 345
24. Aarabi B. Management of traumatic aneurysms caused by high-velocity missilehead wounds. Neurosurg Clin North Am. 1995;6:775–797.
25. Haddad FS, Haddad GF, Taha J. Traumatic intracranial aneurysms caused bymissiles: Their presentation and management. Neurosurgery. 1991;28:1–7.
26. Amirjamshidi A, Rahmat H, Abbassioun K. Traumatic aneurysms and arteri-ovenous fistulas of intracranial vessels associated with penetrating head injuriesoccuring during war: Principles and pitfalls in diagnosis and management. JNeurosurg. 1996;84:769–780.
27. Oliver C, Kabala J. Air gun pellet injury: the safety of MR imaging. Clin Radiol.1997;52:299–300.
28. Smith AS, Hurst GC, Durek JL, Diaz PJ. MR of ballistic materials: Imaging arti-facts and potential hazards. Am J Neruoradiol. 1991;12:567–572.
29. Teitelbaum GP, Yee CA, Van Horn DD, Kim HS, Colletti PM. Metallic ballisticfragments: MR imaging safety and artifacts. Radiology. 1990;175:855–859.
30. Crockard HA. Early intracranial pressure studies in gunshot wounds of thebrain. J Trauma. 1975;15:339–347.
31. Lillard PL. Five year experience with penetrating craniocerebral gunshotwounds. Surg Neurol. 1978;9:79–83.
32. Nagib MG, Rockswold GL, Sherman RS, Lagaard MW. Civilian gunshot woundsto the brain: Prognosis and management. Neurosurgery. 1986;18:533–537.
33. Sarnaik AP, Kopec J, Moylan P, Alvarez D, Canady A. Role of aggressiveintracranial pressure in management of pediatric craniocerebral gunshotwounds with unfavorable features. J Trauma. 1989;29:1424–1437.
34. Intracranial pressure monitoring in the management of penetrating brain injury.J Trauma. 2001:51:S12–S15.
35. Bullock R, Chesnut RM, Clifton G, Ghajar J, Marion DW, Narayan RK, NewellDW, Pitts LH, Rosner MJ, Wilberger JW. Guidelines for the management ofsevere head injury. Eur J Ernerg Med. 1996;3:109–127.
36. BTF Website.37. Vascular complications of penetrating brain injury. J Trauma. 2001;51;S26–
S28.38. Aldrich EF, Eisnberg HM, Saydjari C, Foulkes MA, Jane JA, Marshall LF,Young
H, Marmarou A. Predictors of mortality in severely head-injured patients withcivilian gunshot wound: A report from the NIH Traumatic Coma Data Bank.Surg Neurol. 1992;38:418–423.
39. Levy ML, Rezai A, Masri LS, Litofsky SN, Giannotta SL, Apuzzo ML, WeissMH. The significance of subarachnoid hemorrhage after penetrating cranio-cerebral injury: Correlations with angiography and outcome in civilian popula-tion. Neurosurgery. 1993;32:532–540.
40. Kapp JP, Gielchinsky I. Management of combat wounds of the dural venoussinuses. Surgery. 1972;71:913–917.
41. Aarabi B. Traumatic aneurysms of brain due to high velocity missile headwounds. Neurosurgery. 1988;22:1056–1063.
42. Jinkins JR, Dadsetan MR, Sener RN, Desai S, Williams RG. Value of acute-phase angiography in the detection of vascular injuries caused by gunshotwounds to the head: Analysis of 12 cases. AJR Am J Roentgenol. 1992;159:365–368.
43. Caverness WF, Meirowsky AM, Rish BL, et al. The nature of posttraumaticepilepsy. J Neurosurg. 1979;50:545–553.
346 C.J. Neal et al.

44. Salazar AM, Jabbari B, Vance SC, Grafman J, Amin D, Dillon JD. Epilepsy afterpenetrating head injury, I: Clinical correlates—a report of the Vietnam HeadInjury Study. Neurology. 1985;35:1406–1414.
45. Weiss GH, Salazar AM, Vance SC, Grafman JH, Jabbian B. Predicting post-traumatic epilepsy in penetrating head injury patients. Arch Neurol. 1986;43:771–773.
46. Antiseizure prophylaxis for penetrating brain injury. J Trauma. 2001;51:241–243.47. Thoreby FP, Darlow HM.The mechanism of primary infection of bullet wounds.
Br J Surg. 1967;54:359.48. Wolf AW. Autosterilization in low-velocity bullets. J Trauma. 1978;18:63.49. Taha JM, Saba MI, Brown JA. Missile injuries to the brain treated by simple
wound closure: Results of a protocol during the Lebanese conflict. Neuro-surgery. 1991;29:380–383.
50. Taha JM, Haddad FS, Brown JA. Intracranial infection after missile injuries tothe brain: Report of 30 cases from the Lebanon conflict. Neurosurgery.1991;29:864–868.
51. Surgical management of penetrating brain injury. J Trauma. 2001;51:S16–S25.52. Suddaby L, Weir B, Forsyth C. The management of .22 caliber gunshot wounds
of the brain: A review of 49 cases. Can J Neurol Sci. 1987;14:268–272.53. Shoung HM, Sichez JP, Pertuiset B. The early prognosis of craniocerebral
gunshot wounds in civilian practice as an aid to the choice of treatment. ActaNeurochir (Wien). 1985;74:27–30.
54. Arendall REH, Meirowsky AM. Air sinus wounds: an analysis of 163 consecu-tive cases incurred in the Korean War, 1950–1952. Neurosurgery. 1983;13:377–380.
55. Kearney TJ, Bentt L, Grode M, Lee S, Hiatt JR, Shabot MM. Coagulopathy andcatecholamines in severe head injury. J Trauma. 1992:32:608–612.
56. Part 2: Prognosis in penetrating brain injury [review]. J Trauma. August2001;51(suppl 2):S44–S86.
57. Marshall LF, Maas AI, Marshall SB, Bricolo A, Fearnside M, Iannotti F, KlauberMR, Lagarrigue J, Lobato R, Persson L, Pickard JD, Piek J, Servadei F, WellisGN, Morris GF, Means ED, Musch B.A mutlicenter trial on the efficacy of usingtirilazad mesylatein cases of head injury. J Neurosurg. 1998;89:519–525.
58. Kaufman HH, Schwab K, Salazar AM. A national survery of neurosurgical carefor penetrating head injury. Surg Neurol. 1991;36370–377.
15. Management of Ballistic Trauma to the Head 347