Embed Size (px)
Citation preview
MANAGEMENT OF ANAPHYLAXIS GUIDELINES FEBRUARY 2017
This policy supersedes all previous policies for Management of Anaphylaxis

I ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Policy title Management of Anaphylaxis Guidelines
Policy reference
PHA21
Policy category Clinical
Relevant to Clinical staff
Date published February 2017
Implementation date
February 2017
Date last reviewed
February 2017
Next review date
February 2019
Policy lead Lucy Reeves, Chief Pharmacist
Contact details Email: [email protected]
Accountable director
Dr Vincent Kirchner, Medical Director
Approved by (Group):
DTC
Approved by (Committee):
Quality Committee
Document history
Date Version Summary of amendments
Feb 2017 4 Inclusion of a list of locations where the anaphylaxis kits are held.
May 2014 3 Routine review
Jun 2011 2 Routine review
Nov 2008 1 New Guidelines
Membership of the policy development/ review team
Lucy Reeves, Chief Pharmacist
Consultation
Kevin Cann, Resuscitation Lead, Simon Peel lead Nurse from Medicines Management, DTC
DO NOT AMEND THIS DOCUMENT
Further copies of this document can be found on the Foundation Trust intranet.

II ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Contents Page
1 Introduction 3
2 Aims and objectives 3
3 Scope of the policy 3
4 Duties and responsibilities 3
5 Key points 3
6 Triggers 4
7 Recognition of anaphylaxis 4
8 Treatment of anaphylactic reaction 6
9 Recommended Dosage of adrenaline 7
10 Supply and access to adrenaline 8
11 Documentation 9
12 Dissemination and implementation arrangements 9
13 Training requirements 9
14 Review of the policy 9
15 References 10
16 Associated documents 10
Appendix 1: Anaphylaxis risk assessment checklist 11
Appendix 2: Treatment of anaphylaxis – summary chart 12
Appendix 3: Anaphylaxis Algorithm (Resuscitation Council (UK) 13
Appendix 4: Anaphylaxis packs and Emergency bags locations 14
Appendix 5: Equality impact assessment 15

3 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
1 Introduction
Anaphylaxis is a severe, life threatening, generalised or systemic hypersensitivity reaction. It is characterised by rapidly developing, life threatening problems involving: the airway (pharyngeal or laryngeal oedema) and / or breathing (bronchospasm and tachypnoea) and/or circulation (hypotension and/or tachycardia). In most cases, there are associated skin and mucosal changes 1
The acute reaction that occurs usually happens within seconds or minutes of an exposure to the antigen.
All clinical staff must be prepared and equipped to recognise and provide initial treatment of anaphylactic reactions part icular ly after the introduction of substances (e.g. medicines) by injection or other routes with rapid absorption. This is particularly important where this takes place without emergency equipment and medical personnel.
Initial drug treatment of anaphylaxis is adrenaline only. Further drug treatment is given by paramedic or Accident and Emergency staff. Adrenaline (epinephrine) injection may legally be administered without a prescription only for the purpose of saving life in an emergency (Medicines Act 1968).
This document provides guidance in the recognition and treatment of an anaphylactic reaction, and should be read in conjunction with the Trust Cardiopulmonary resuscitation (CPR) and the management of the deteriorating patient policy.
The guidance in this document is based on the current Resuscitation Council (UK) Emergency treatment of anaphylactic reactions: Guidelines for healthcare providers (www.resus.org.uk, last updated in 2017).
2 Aims and objectives
To provide guidance to staff in the recognition of anaphylactic reactions.
To provide guidance on the appropriate treatment of an anaphylactic reaction
3 Scope of the guidelines
These guidelines are applicable to all staff working within Camden & Islington NHS Foundation Trust who are involved in the care of service users.
4 Duties and responsibilities
All clinical staff must be prepared and equipped to recognise and provide initial treatment of anaphylactic reactions part icular ly after the introduction of substances (e.g. medicines) by injection or other routes with rapid absorption. This is particularly important where this takes place without emergency equipment and medical personnel.
5 Key Points
Treatment of an anaphylactic reaction should be based on general life support principles 1:
Use the Airway, Breathing, Circulation, Disability, Exposure (ABCDE*) approach to recognise and treat problems.
Call for help early.
Treat the greatest threat to life first.
4 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Initial treatments should not be delayed by the lack of a complete history or definite diagnosis.
Patients having an anaphylactic reaction in any setting should expect the following as a minimum:
• Recognition that they are seriously unwell. • An early call for help. • Initial assessment and treatments based on an ABCDE* approach. • Adrenaline therapy if indicated. • Investigation and follow-up by an allergy specialist.
6 Triggers
Anaphylaxis can be triggered by any of a very broad range of triggers, but those most commonly identified include food, drugs and venom. The relative importance of these varies very considerably with age, with food being particularly important in children and medicinal products being much more common triggers in older people. Virtually any food or class of drug can be implicated, although the classes of foods and drugs responsible for the majority of reactions are well described. Of foods, nuts are the most common cause; muscle relaxants, antibiotics, NSAIDs and aspirin are the most commonly implicated drugs. It is important to note that, in many cases, no cause can be identified. A significant number of cases of anaphylaxis are idiopathic (non-IgE mediated).1
7 Recognition of Anaphylaxis
7.1 Mortality
The overall prognosis of anaphylaxis is good, with a case fatality ratio of less than 1% reported in most population-based studies. Risk of death is, however, increased in those with pre-existing asthma, particularly if the asthma is poorly controlled or in those asthmatics who fail to use, or delay treatment with, adrenaline. There are approximately 20 anaphylaxis deaths reported each year in the UK, although this may be a substantial under-estimate1.
7.2 Risk of recurrence
The risk of an individual suffering recurrent anaphylactic reaction appears to be quite substantial, being estimated at approximately 1 in 12 per year 1.
7.3 Assessing the risk of occurrence
Anaphylaxis may be iatrogenic (due to the action of the clinician) in cause. The health assessment must therefore include a comprehensive history of:-
• Previous reactions to medicines • Medicine contra-indications • Adverse reactions to other environmental substances • Allergic reactions.
Practitioners should ensure that these findings are documented in the patient’s electronic record and drug chart for subsequent reference. By default, the allergy section on Care Notes states “No data entered - Use the Core Assessment to record Allergies”. This does not mean that the patient has no known allergy and should not be used as a source unless it has been updated. This can be done by going into the Assessment tab and opening a C&I Core Assessment form (Allergies and Adverse Reactions section)

5 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
A history of hay fever, asthma, eczema, or mild reactions with any vaccine is not a contraindication to further doses of that vaccine or any other vaccine.
7.4 Check List (See Appendix 1)
The check list is designed to be used by the clinician with patients prior to the administration of vaccinations or drugs administered by a rapid absorption route. Patients who answer yes to questions marked * on the checklist have a greater risk of anaphylaxis, and therefore, prior to giving any injection, the clinician must consult with the medical team in charge of the patient’s care. An anaphylactic shock kit and a telephone must be available whenever drugs are administered by injection or other routes with rapid absorption, even when the patient/client is not considered at risk. If no contra-indications exist, clinicians should make preparations by ensuring that:
• Adrenaline (epinephrine) is placed in an accessible position • The dose required is known • The ampoules of adrenaline (epinephrine) and contents are suitable for use • The position of the nearest telephone is known
7.5 Identification of an anaphylactic reaction
Medical and nursing staff are responsible for assessing the patient and identifying an anaphylactic reaction. If the following 2 criteria are present, anaphylaxis is likely:
• sudden onset and rapid progression of symptoms • life threatening airway and / or breathing and / or circulation problems
Skin and/or mucosal changes (flushing, urticaria, angioedema) are also very common but may not present in all cases.
Signs and Symptoms of an anaphylactic reaction The patient will:
• feel and look unwell • feel anxious • may have a sense of impending doom
Use the ABCDE approach to identify the signs of anaphylaxis A – Airway Throat & tongue swelling, hoarse voice, stridor (noise heard on inspiration) B – Breathing Shortness of breath, wheeze, tiredness, cyanosis, respiratory arrest C – Circulation Pallor, clammy, tachycardia, hypotension, faint (vaso-vagal), dizziness, collapse, cardiac arrest. D – Disability Confusion (due to hypoxia), decreased level of consciousness, agitation, gastro- intestinal disturbances E – Exposure Urticaria, skin changes

6 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Although the onset is usually within five to ten minutes of exposure, the time taken for a full blown reaction to evolve varies. It would rarely be more than thirty minutes.
7.6 Other Potential Diagnoses
Acute asthma attack
Septic shock
Faint (vaso-vagal)
Panic attack
Idiopathic (non-allergic) urticaria or angioedema.
Skin and / or mucosal changes (flushing, urticaria, angioedema) are also likely but these alone are not a sign of an anaphylactic reaction and that may be very subtle. Local reactions such as swelling, itching and redness at the administration site, or mild allergic reactions with headache, itching skin, nausea and general malaise, are not anaphylactic reactions. The treatment for these is reassurance, paracetemol and oral antihistamine as required.
8 Treatment of Anaphylactic Reaction
See also summary chart in Appendix 2 and algorithm in Appendix 3 Treatment of an anaphylactic reaction should be based on general life support principles:
• Use the Airway, Breathing, Circulation, Disability, Exposure (ABCDE) approach • Call for help early – but do not delay next steps by phoning ambulance yourself. • Treat the greatest threat to life first. • Initial treatments should not be delayed by the lack of a complete history or definite
diagnosis - at any age, if in doubt, treat the patient for anaphylaxis. • Where applicable, discontinue the causative agent. • Reassure the patient. • Lie the patient on a flat surface and raise legs.
A – Airway Establish and maintain an airway. Use of a mechanical airway may not always be necessary and airways may not be available. B – Breathing Administer oxygen (>10 litres per minute), where skills and equipment are available Patients with breathing difficulties may prefer to sit up, but beware of exacerbating hypotension. If the patient feels faint do not sit or stand them up as this can cause cardiac arrest. C – Circulation Check the patient’s carotid pulse - check brachial pulse in infants under one year. A strong central carotid pulse which persists is more likely to be a collapse/faint In the case of a weak central carotid pulse or breathing difficulties, start to administer intra-muscular adrenaline (epinephrine). If the patient is not breathing and has no pulse, commence cardiopulmonary resuscitation
8.1 Adrenaline (epinephrine)
Adrenaline is the most important drug in treating anaphylaxis. It reverses peripheral vasodilation, reduces oedema, dilates airways, increases force of myocardial contraction, and suppresses histamine and leukotriene release. Early administration of adrenaline

7 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
(epinephrine) lessens the severity of IgE mediated allergic reactions. Members of staff who have received anaphylaxis training should administer adrenaline. Adrenaline (epinephrine) should be administered by INTRAMUSCULAR (IM) injection. The preferred site in initial treatment of anaphylaxis is the mid-point of the thigh, anterolateral aspect. An intramuscular injection has a greater margin of safety and is easier to administer. Intravenous (IV) administration should only be carried out by experienced specialists i.e. anaesthetists, emergency or intensive care physicians. Adrenaline (epinephrine) should be injected as slowly as possible, taking care to ensure that this is not directly into a blood vessel. Administering IM adrenaline (epinephrine) should not do any harm even if an incorrect diagnosis of anaphylaxis has been made.
8.2 Calling for help
An ambulance must be called early and the patient transported to an emergency department for medical assessment and follow up treatment and monitoring, in accordance with NICE clinical guidance 2
• Shout if someone is within calling distance, ask them to call for an ambulance
• On an in-patient site, activate the emergency button/alarm, to quickly summon help to call the ambulance, and then to assist as required.
• Where there is no one available to dial 999, e.g. the clinician is alone in a patient’s
home, call ambulance straight after giving the first dose of adrenaline (epinephrine).
8.3 Patient Positioning
All patients should be placed in a comfortable position. The following factors should be considered:
• Patients with Airway and Breathing problems may prefer to sit up as this will make breathing easier.
• Lying flat with or without leg elevation is helpful for patients with a low blood pressure (Circulation problem). If the patient feels faint, do not sit or stand them up - this can cause cardiac arrest.
• Patients who are breathing and unconscious should be placed on their side (recovery position).
• Pregnant patients should lie on their left side to prevent caval compression.
9 Recommended Dosage of Adrenaline (Epinephrine)
Intramuscular route
Dose of intramuscular injection of adrenaline (epinephrine) for the emergency treatment of anaphylaxis by healthcare professionals 3
Age Dose Volume of adrenaline 1 in 1000 (1mg/ml)
Adult & child 12-18 years 500 micrograms 0.5ml
Doses may be repeated several times if necessary at 5 minute intervals according to blood pressure, pulse and respiratory function.
8 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Pharmacy should be notified of the use of adrenaline as soon as possible during opening hours, or the next working day if out of hours, so that a replacement can be supplied as soon as possible. Intravenous route There is a much greater risk of causing harmful side effects by inappropriate dosage or misdiagnosis of anaphylaxis when using IV adrenaline. Therefore the intravenous route should not be used.
9.1 Adrenaline in special populations
Previous Resuscitation Council (UK) guidelines recommended adrenaline (epinephrine) dose adjustments in certain circumstances (e.g. in patients taking tricyclic antidepressants) – they no longer consider this helpful in the setting of an acute anaphylactic reaction and state that: There is large inter-individual variability in the response to adrenaline (epinephrine). In clinical practice, it is important to monitor the response; start with a safe dose (as shown in the tables) and give further doses if a greater response is needed, i.e. titrate the dose according to effect. Adrenaline (epinephrine) may fail to reverse the clinical manifestation of anaphylaxis, especially when its use is delayed or in patients treated with beta-blockers. Therefore the response needs to be carefully monitored.
9.2 Patients’ own auto-injectors (for self-administration)
The 500micrograms dose is recommended for adults and children over 30kg of weight. Adrenaline auto-injector pens for self-administration are available as 300 microgram and 500 microgram preparations. If the patient’s own auto-injector is the only available adrenaline preparation then the healthcare professional should use it. Inpatients with known allergies, who are routinely prescribed an auto-injector, should be risk assessed to decide whether it is appropriate for them to hold the auto-injector in their possession during their admission. The medical and nursing staff should undertake a risk assessment (including to other patients) prior to the patient taking custody of the auto-injector. The risk assessment should be documented in the electronic patient record (Carenotes). The patient should be able to carry it on their person or store securely their room. If there is no lockable cabinet in their room then it should be stored in the clinic room. Where the trust supplies 500 microgram adrenaline auto-injectors for emergency use, and the staff member is trained, then the dose of 500micrograms using this preparation should be administered.
10 Supply and Access to Adrenaline
10.1 Anaphylaxis Treatment
Anaphylaxis treatment must be available in all locations where medicines with a risk of anaphylactic reactions may be used (e.g. antibiotics, Pabrinex®, vaccines). Anaphylaxis treatment is supplied by pharmacy: 2 x Adrenaline IM injection 500mcg auto-injectors (Emerade®)

9 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Adrenaline (epinephrine) must be stored in a cool place away from light. Instructions for its use should always be visible. The expiry date should also be visible and checked at regular intervals. Adrenaline solution should be colourless. If it is observed to have turned yellow or brown then it must be replaced, regardless of the expiry date. The pharmacy department keeps a central list of all locations holding anaphylaxis treatment (see Appendix 4). Replacement treatment (e.g. following use or damage) must be ordered directly from pharmacy at the earliest opportunity. Expired medication should be returned to pharmacy.
10.2 Yellow Emergency Medicine Bags
The yellow emergency medicine bags contain the following adrenaline preparations for use in case of anaphylaxis:
• 2 x Adrenaline IM injection 500mcg auto-injectors (Emerade®) Locations where emergency bags are held are listed in Appendix 4.
11 Documentation
If a patient has a reaction to a medication, or if adrenaline (epinephrine) is administered to a patient in an emergency, the details of the reaction, dose(s) administered, batch number(s) and time(s) should be recorded and confirmed/signed in the patient’s electronic record and prescription chart by the administering practitioner. The emergency services and the patient’s GP should be given details of:
• The probable cause of the reaction, i.e. the medicines(s) previously administered, along with dose and route of administration
• Any other medication that the patient is known to be taking • The action taken and details of adrenaline (epinephrine) given by the practitioner
12 Dissemination and implementation arrangements
This document will be circulated to all managers who will be required to cascade the information to members of their teams. It will be available to all staff via the Trust intranet. Managers will ensure that all staff are briefed on its contents and on what it means for them.
13 Training requirements
Training on the recognition and treatment of anaphylaxis will be provided as part of the Trust Immediate Life Support training.
14 Review of the policy
2 years (February 2019)
10 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
15 References
1. Resuscitation Council (UK) Emergency treatment of anaphylactic reactions: Guidelines for healthcare providers. www.resus.org.uk. January 2008 (annotated with links to NICE guidance in July 2012) 2. NICE clinical guidance 134: Anaphylaxis: assessment to confirm an anaphylactic episode and the decision to refer after emergency treatment for a suspected anaphylactic episode. Guidance.nice.org.uk/cg134 3. British National Formulary (BNF) www.bnf.org
16 Associated documents
Cardiopulmonary resuscitation (CPR) and the management of the deteriorating patient policy.
Medicines Management Policy.
11 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
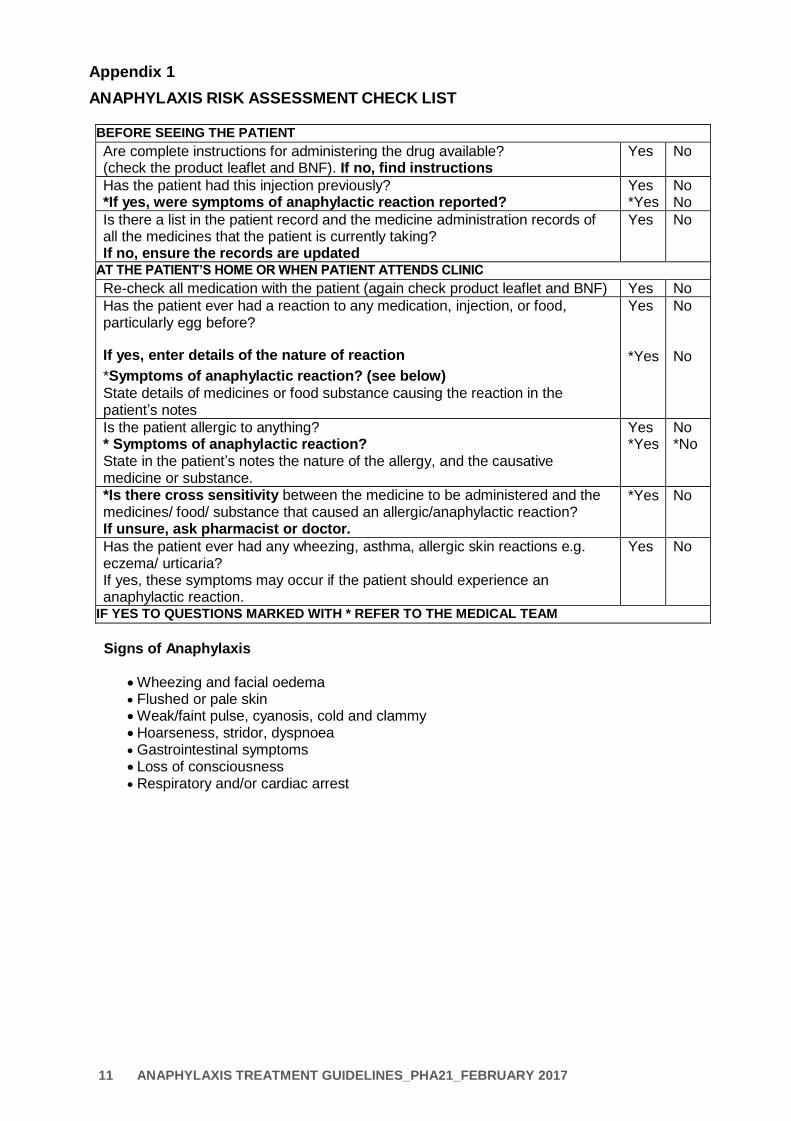
Appendix 1
ANAPHYLAXIS RISK ASSESSMENT CHECK LIST BEFORE SEEING THE PATIENT
Are complete instructions for administering the drug available? (check the product leaflet and BNF). If no, find instructions
Yes No
Has the patient had this injection previously? *If yes, were symptoms of anaphylactic reaction reported?
Yes *Yes
No No
Is there a list in the patient record and the medicine administration records of all the medicines that the patient is currently taking? If no, ensure the records are updated
Yes No
AT THE PATIENT’S HOME OR WHEN PATIENT ATTENDS CLINIC
Re-check all medication with the patient (again check product leaflet and BNF) Yes No
Has the patient ever had a reaction to any medication, injection, or food, particularly egg before?
If yes, enter details of the nature of reaction
*Symptoms of anaphylactic reaction? (see below)
State details of medicines or food substance causing the reaction in the patient’s notes
Yes
*Yes
No
No
Is the patient allergic to anything? * Symptoms of anaphylactic reaction? State in the patient’s notes the nature of the allergy, and the causative medicine or substance.
Yes *Yes
No *No
*Is there cross sensitivity between the medicine to be administered and the medicines/ food/ substance that caused an allergic/anaphylactic reaction? If unsure, ask pharmacist or doctor.
*Yes No
Has the patient ever had any wheezing, asthma, allergic skin reactions e.g. eczema/ urticaria? If yes, these symptoms may occur if the patient should experience an anaphylactic reaction.
Yes No
IF YES TO QUESTIONS MARKED WITH * REFER TO THE MEDICAL TEAM
Signs of Anaphylaxis
Wheezing and facial oedema Flushed or pale skin
Weak/faint pulse, cyanosis, cold and clammy Hoarseness, stridor, dyspnoea Gastrointestinal symptoms
Loss of consciousness Respiratory and/or cardiac arrest

12 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Appendix 2:
TREATMENT OF ANAPHYLAXIS – SUMMARY CHART
Where applicable, stop administration of the drug suspected of causing the reaction
Lay the patient on a flat surface, raise legs. Patients with respiratory (breathing)
distress may prefer to sit up
Maintain an airway.
On Trust sites, activate emergency button to quickly summon help to call an ambulance and then to assist. Do not delay next steps by phoning the ambulance yourself.
Symptoms of anaphylaxis – see Appendix 3.
At any age, if doubt, treat the patient for anaphylaxis.
Administer adrenaline intramuscularly. The preferred site in initial treatment of anaphylaxis is the mid point of the thigh, anterolateral aspect.
Inject as slowly as possible, taking care to ensure it is not directly into a blood vessel.
Call ambulance if another person is not available to do so.
If the patient is not breathing and has no pulse, commence cardiopulmonary resuscitation.
Doses of adrenaline (epinephrine) 1: 1000 Adult dosage: 500micrograms (0.5ml) IM
Further doses can be given at 5 minute intervals if the patient’s condition dictates (monitor breathing, blood pressure and pulse) If the auto-injector is the only adrenaline preparation, then the healthcare professional should use it.
l L l l l l l l l l
0.15 ml 0.3 ml 0.5 ml 1 ml
1ml syringe (not to scale)
Resuscitation Council (UK) 2008 recommends that the normal dose (table above) is given to all individuals regardless of any medication they are currently taking. Monitor response closely.

13 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Appendix 3: Anaphylaxis Algorithm (Resuscitation Council (UK)
Anaphylaxis reactions: Initial treatment
Anaphylactic reaction?
Airway, Breathing, Circulation, Disability, Exposure
Diagnosis – look for: Acute onset of illness
Life threatening Airway and/or Breathing and/or Circulation problems 1
And usually skin changes
Call for help Lie patient flat
Raise patient’s legs (if breathing not impaired)
Intramuscular Adrenaline (Epinephrine) 2
Monitor (if equipment available):
Pulse oximetry
Blood Pressure
ECG
1 Life Threatening problems: Airway: swelling hoarseness, stridor Breathing: rapid breathing, wheeze, fatigue, cyanosis, SpO2 <92%, confusion Circulation: pale, clammy, low blood pressure, faintness, drowsy/coma
2 Intramuscular Adrenaline IM doses of 1in 1000 (1mg/ml) adrenaline (repeat after 5 minutes if no better)
Adult & child 12-18 years: 500micrograms IM (0.5ml)
14 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
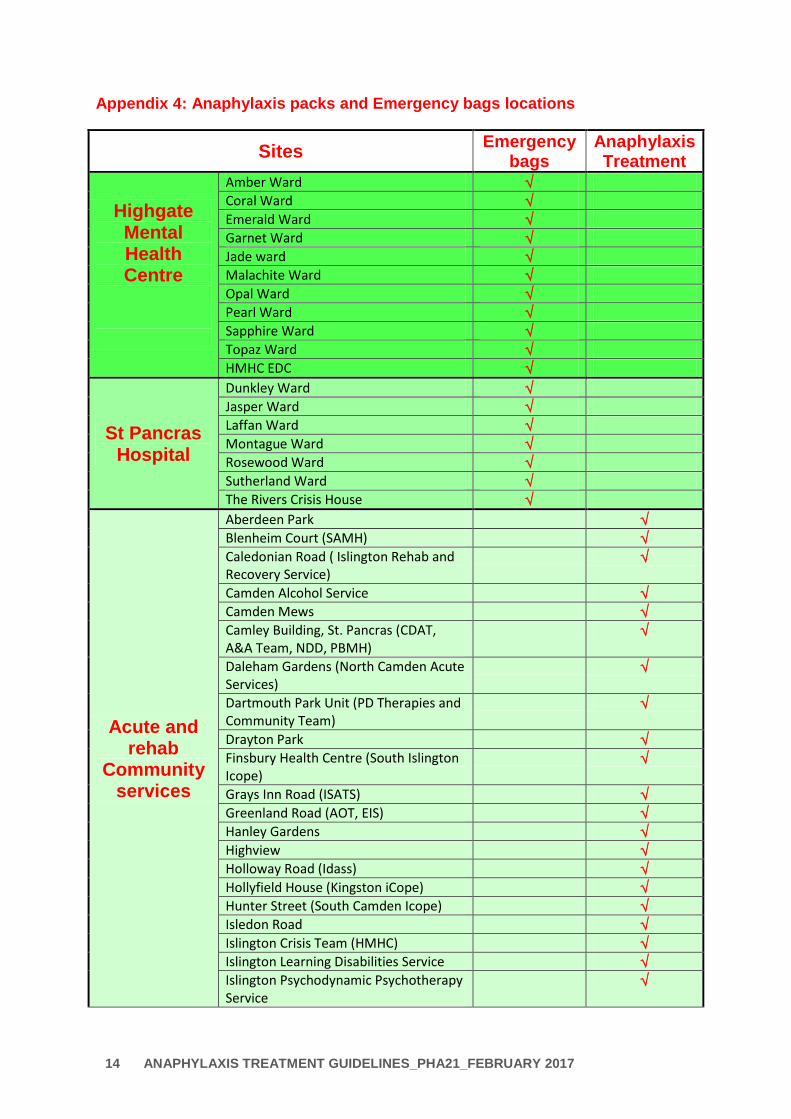
Appendix 4: Anaphylaxis packs and Emergency bags locations
Sites Emergency
bags Anaphylaxis Treatment
Highgate Mental Health Centre
Amber Ward
Coral Ward
Emerald Ward
Garnet Ward
Jade ward
Malachite Ward
Opal Ward
Pearl Ward
Sapphire Ward
Topaz Ward
HMHC EDC
St Pancras Hospital
Dunkley Ward
Jasper Ward
Laffan Ward
Montague Ward
Rosewood Ward
Sutherland Ward
The Rivers Crisis House
Acute and rehab
Community services
Aberdeen Park
Blenheim Court (SAMH)
Caledonian Road ( Islington Rehab and Recovery Service)
Camden Alcohol Service
Camden Mews
Camley Building, St. Pancras (CDAT, A&A Team, NDD, PBMH)
Daleham Gardens (North Camden Acute Services)
Dartmouth Park Unit (PD Therapies and Community Team)
Drayton Park
Finsbury Health Centre (South Islington Icope)
Grays Inn Road (ISATS)
Greenland Road (AOT, EIS)
Hanley Gardens
Highview
Holloway Road (Idass)
Hollyfield House (Kingston iCope)
Hunter Street (South Camden Icope)
Isledon Road
Islington Crisis Team (HMHC)
Islington Learning Disabilities Service
Islington Psychodynamic Psychotherapy Service
15 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Jules Thorn (South Camden Recovery Centre)
Lowther Road (NIRT, Islington Re-ablement Team)
Manor Gardens (North Islington iCope)
Margarete Centre
Neatherwood Day Centre
North Camden Rehab
Peckwater Centre (South Camden R&R)
South Wing, St. Pancras (South Camden iCope)
Southwood Smith Centre (South Islongton Recovery Team)
Stacey Street Nursing Home
Surbiton Health Centre (Kingston Wellbeing SMS)
The Hoo (North Camden Recovery and Rehabilitation)
Transitions Service
West Wing, St. Pancras (Traumatic Stress Team, Psychotherapy)
Highgate Day Centre
Raglan House

16 ANAPHYLAXIS TREATMENT GUIDELINES_PHA21_FEBRUARY 2017
Appendix 5
Equality Impact Assessment Tool
Yes/No Comments
1. Does the policy/guidance affect one group less or more favourably than another on the basis of:
Race No
Ethnic origins (including gypsies and travellers) No
Nationality No
Gender No
Culture No
Religion or belief No
Sexual orientation including lesbian, gay and bisexual people
No
Age No
Disability - learning disabilities, physical disability, sensory impairment and mental health problems
No
2. Is there any evidence that some groups are affected differently?
No
3. If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
N/A
4. Is the impact of the policy/guidance likely to be negative?
N/A
5. If so can the impact be avoided? N/A
6. What alternatives are there to achieving the policy/guidance without the impact?
N/A
7. Can we reduce the impact by taking different action?
N/A













![Anaphylaxis: assessment to confirm an …...venom-induced anaphylactic reaction and 220,000 people up to the age of 44 have had a nut induced anaphylactic reaction [ 2 ] . There is](https://img.pdfslide.us/doc/110x75/5f08c23d7e708231d42394e2/anaphylaxis-assessment-to-confirm-an-venom-induced-anaphylactic-reaction-and.jpg)