Embed Size (px)
Citation preview

MANAGEMENTOFAKIANDCKDINMALIGNANCY
ANITHAVIJAYANMDPROFESSOROFMEDICINEDIVISIONOFNEPHROLOGY
KDIGO

DISCLOSURES
NxStage–Speaker,Scien@ficAdvisoryBoard Sanofi-Speaker
KDIGO

ACUTEKIDNEYINJURY
DEFINITIONCANCERRELATEDAKI
TLSCAST
NEPHROPATHYMANAGEMENT
KDIGO

Defini@onofAKI(KDIGOguidelines)
Anabrupt(within48hours)reduc@oninkidneyfunc@on–Ø riseinserumcrea@nine(SCr)by≥0.3mg/dLØ apercentageincreaseinSCrof≥50%frombaselineoverthepast7daysØ ordocumentedoliguriaoflessthan0.5ml/kg/hourformorethan6hours
Kidney Intl 2: 8-12, 2012
KDIGO

Classifica@on/StagingSystemforAKI
Stage SerumCrea<nineCriteria UrineOutputCriteria
1 RiseinSCr≥0.3mg/dLor≥150-200%frombaseline
<0.5ml/kg/hrfor>6hr
2 RiseinSCr>200-300%frombaseline <0.5ml/kg/hrfor>12hr
3
RiseinSCr>300%frombaseline,orSCr>4mg/dLwithanacuteincreaseofatleast0.5mg/dL
<0.3ml/kg/hrfor>24hroranuria>12hr
Kidney Intl 2: 8-12, 2012
KDIGO

ICUacquiredAKI
Rocha et al, NDT, Jan 2009
0%
10%
20%
30%
40%
50%
60%
Sepsis Ischemia Nephrotoxins Rhabdo Obstruc@on
CAUSESOFAKIAMONGALLPATIENTS Overallincidenceisabout20%
Pa@entswithmalignancy: MostcommoncauseofAKIissepsis Incidence12–50% RequiringRRT–9-30% MortalityinthoseneedingRRT:70–85%
Bouchard et al, CJASN 2015; Campbell et al ACKD 2014
KDIGO

Zengetal,CJASN2014
AKIINSETTINGOFOTHERCO-MORBIDITIES
KDIGO

AKIIncreasesTheRiskOfProgressionToESRD
Hsuetal,CJASN2009
KDIGO

CostofAKIALLAKIPATIENTS AKI-DPATIENTS
Silveretal,JHospMed2017
KDIGO

DIRECTLYRELATEDBYMALIGNANCY
DIRECTEFFECTSOFCHEMOTHERAPY
COMPLICATIONSOFTREATMENTOFMALIGNANCY OTHERFACTORS
ACUTEKIDNEYINJURYKDIGO

Directlycausedbymalignancy
Obstruc@on◦ Prostatecancer◦ Urothelialmalignancy◦ Ovarian/Uterinemalignancy◦ Extrinsiccompressionfrommetastases,lymphadenopathy Infiltra@on◦ Lymphoma/leukemia Intrinsicdamage◦ Mul@plemyelomawithcastnephropathy/lightchaindeposi@ondisease Hypercalcemia
KDIGO

Directtoxicityfromchemotherapyagents
Glomerularinjury/TMA◦ Checkpointinhibitors◦ VEGFinhibitors◦ Gemcitabine
Inters@@alNephri@s◦ Checkpointinhibitors
Tubularinjury◦ Pla@numcompounds◦ Methotrexate◦ Trabec@din(rhabdomyolysis)◦ Pemetrexed
KDIGO

Complica@onsoftreatment
Pre-renalAKI(especiallyifconcomitantlyonNSAIDs,RAASblockers)◦ severediarrheawithirinotecan◦ nausea/vomi@ngwithotherchemotherapyagentsIntrinsicrenalinjury◦ Tumorlysissyndrome
Obstruc@on◦ Urothelialstrictures(previoussurgery/radia@on)
KDIGO

Otherfactors Sepsis ContrastinducedAKI Nephrotoxins◦ Bisphosphonates◦ NSAIDs◦ ACEI◦ ARB◦ Aminoglycosides◦ Vancomycin◦ Amphotericin◦ IVAcyclovir
AKIposthematopoie@cstemcelltransplant
KDIGO

MANAGEMENTOFAKIKDIGO

KDIGORECOMMENDATIONSFORMANAGEMENTOFAKI
Discon<nuenephrotoxicagentsEnsureadequatevolumestatusandperfusionpressureConsiderfunc<onalhemodynamicmonitoringMonitorserumcrea<nineandurineoutputAvoidhyperglycemiaConsideralterna<vestoradiocontrastprocedures
Non-invasivediagnos<cworkupConsiderinvasivediagnos<cwork-up
CheckforchangesindrugdosingConsiderRRT
AssessforRRT
HighRisk AKIStage1 AKIStage2 AKIStage3
ICUadmission
Avoidsubclaviancatheters
KidneyInterna@onalSupplements(2012)
KDIGO

TumorlysissyndromeKDIGO

HyperphosphatemiaHyperkalemiaElevatedUricacid
Spontaneous
Ajerchemotherapy
Triggerinflammatorymediators Renalvasoconstric@on
Inflamma@on
Uricacidcrystalliza@onCa-Pnephropathy
AKI
TUMORCELLS CELLLYSIS
KDIGO

Purine catabolism
Hypoxanthine
Xanthine
Uric acid
Excretion
Xanthine oxidase
Xanthine oxidase
ALLANTOIN
EXCRETION
Urateoxidase KDIGO

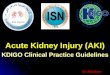
CAIRO-BISHOPCLASSIFICATIONFORTLS
LABORATORYCRITERIA
Ø SerumK>6.0mEq/Lorincreaseby25%frombaseline
Ø SerumCa<7mg/dLordecreaseby25%frombaseline
Ø SerumP>4.5mg/dLorincreaseby25%frombaseline
Ø SerumUA>8.0mg/dLorincreaseby25%frombaseline
CLINICALCRITERIA
Ø AKI:increaseinSCr1.5xULNØ CardiacarrhythmiaØ Seizures
CAVEATS:3daysbeforeorwithin7daysajerchemotherapyInsameInsame24hourperiodMaybedelayedforsolidtumors
KDIGO

RISKFACTORSFORTLS
Tumorcharacteris@cs
• Hematologicalmalignancieswithhightumorburden• WBC>50,000• ElevatedLDH• Burkips’slymphoma• DLBCL• Lymphoblas@cleukemia
• Solidtumorswithverylargetumorburden*
Pa@entcharacteris@cs
• UnderlyingCKD• Concomitantnephrotoxins
• ConcomitantCHF/Liverdisease
• Volumedeple@on• Lympha@c/leukemicinfiltra@onofthekidney
• Hyperuricemiaatbaseline
Chemotherapyfactors
• Specifictargetedtreatments• Venetoclax(BCL-2inhibitor)
• Obinutuzumab(CD-20monoclonalAb)
• Ibru@nib(BTKinhibitor)
• Dinaciclib(CDKinhibitor)
KDIGO

TLSAFTERTREATMENTOFCLLWITHVENETOCLAX
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
%PAT
IENTSW
ITHTLS
TotalTLS LabTLS ClinicalTLS
RobertsetalNEJM2016
KDIGO

RISKSTRATIFICATION
IVFLUIDS–NSorIsotonicfluidAVOIDNEPHROTOXINS
IVFLUIDS–NSorIsotonicfluidAVOIDNEPHROTOXINS
ALLOPURINOLORFEBUXOSTATCONSIDERPROPHYLACTIC
RASBURICASEIFVERYHIGHRISK
LOWRISK MODERATE/HIGHRISK
INITIATIONOFCHEMOTHERAPY
MONITORFORTLS–RenalPanel,UricAcidevery12-24hours
TUMORCHARACTERISTICSPATIENTCHARACTERISTICSTYPEOFCHEMOTHERAPY
IFTLSOCCURS
Rasburicase/Ini@a@onofRRT
URINARYALKALINATIONNOTRECOMMENDED
KDIGO

WilsonandBernsCJASN2012
Randomizedtrialsofrasburicase
KDIGO

CASTNEPHROPATHYKDIGO

CASTNEPHROPATHY
Mul@plemyeloma◦ representsapproximately1%ofallmalignancies◦ Approximately15%ofallhematologicalmalignancies
Approximately20-30%ofMMpa@entshavecastnephropathy MostcommoncauseofAKIinMMIscastnephropathy AKIassociatedwithreducedsurvivalKDIGO

KBasnayakeetal,KidneyInterna@onal(2011)79,1289–1301;
KDIGO

KDIGO

DIFFERENCEINSIEVINGCOEFFICIENTBETWEENHIGH-FLUXandHCODIALYZERS
GondouinBandHutchisonCA,AdvCKD2011
KDIGO

HutchisonCAetal,CJASN2009
KDIGO

P<0.001
HutchisonCAetal,CJASN2009
KDIGO

MYRESTUDY
Highfluxdialyzer 33.3% 35.4%
Highcutoffdialyzer 41.3% 56.5%
98pa@ents
Dialysisindependenceat3mo
Dialysisindependenceat6mo
P=0.04P=0.42
Bridouxetal,JAMA2017
KDIGO

FinkelandFabbrini_JOncoNeph2017
KDIGO

RRTINAKI KDIGO

CONSIDERATIONSREGARDINGRRTINPATIENTSWITHMALIGNANCYANDAKI
SHOULDRRTBEINITIATED?◦ Ethicalconcernsinterminalmalignancy◦ Ifcurrentillnessfelttobereversible,thenRRTshouldbeconsidered TIMINGOFRRT
MODALITY
DOSEOFRRT
KDIGO

Darmonetal,NDT2015
Mortalityincri@callyillpa@entswithhematologicalmalignanciesandAKI
KDIGO

DifferencesbetweenCRRTandIHDCRRT IHD
Hemodynamicstability + - Fluidbalanceachievement + - Superiormetaboliccontrol + - Con<nuousremovaloftoxins + - Stableintracranialpressure + - Unlimitednutri<on + - Needforintensivecarenursingsupport + - Simpletoperform ± - Rapidremovalofpoisons - + Limitedan<coagula<on - + Needforhemodialysisnursingsupport ± + Pa<entmobility - +
KDIGO

OUTCOMES:HDVSCRRT
Nodifferenceinmortalitybetweenpa@entsini@atedonCRRTvsIHD Nodifferenceinrenalrecovery NodifferenceinICU/hospitalLOS
KDIGO

KDIGORecommenda@onsforRRTinAKI
Usecon@nuousandintermipentRRTascomplementarytherapiesinAKIpa@ents(Notgraded)
WesuggestusingCRRT,ratherthanstandardintermipentRRT,forhemodynamicallyunstablepa@ents(Grade2b)
WesuggestusingCRRT,ratherthanintermipentRRT,forAKIpa@entswithacutebraininjuryorothercausesofincreasedintracranialpressureorgeneralizedbrainedema(Grade2b)
KidneyInterna@onal2:(1)2012
KDIGO

Edrees,Li,Vijayan,ACKD2016
COMPARISONOFDIFFERENTMODALITIES
KDIGO

DOSINGOFRRTINIHDANDCRRT
IHD◦ GoalisspKt/Vureaof1.3/treatment,3@mes/week
CRRT◦ Effluentvolumeof20-25ml/kg/hour
KDIGO

MANAGEMENTOFCKDINMALIGNANCYKDIGO

Toxicityfromotherdrugs Chemotherapytoxicity
Lossofnephronmass Mechanicalissues
ChronicKidneyDisease
KDIGO

CAUSESOFCKDINCANCERPATIENTS
Chemotherapytoxicity
VEGFinhibitors
Tyrosinekinaseinhibitors
Pla@numbaseddrugs
Gemcitabine
Checkpointinhibitors
Pemetrexed
Othernephrotoxins
Bisphosphonates
NSAIDs
IVcontrast
Nephronloss
Par@alnephrectomy
Unilateralnephrectomy
Mechanicalissues
Intrinsicobstruc@onof
ureter
Extrinsiccompressionof
ureter
Infiltra@onofthekidney
OTHER
DM
HTN
GN
KDIGO

ManagementofCKDinpa@entswithmalignancy
BPcontrol Managementofproteinuria
UseofACEI/ARB ManagementofanemiaofCKD
OtherCKDrelatedissues◦ Boneandmineralmetabolism◦ Metabolicacidosis
Chemotherapyassociatedcomplica@ons
Glomerulonephri@sassociatedwithmalignancy
KDIGO

PerazellaandIzzedine,KidneyInterna@onal(2015)87,909–917
KDIGO

HypertensionandProteinuriawithVEGFinhibi@on
Hypertension◦ Dosedependent◦ Rangefrom20–40%◦ Treatment–standardan@HTNmedica@ons◦ Chemotherapyshouldnotbeinterruptedforhypertension
Proteinuria◦ Endotheliosis,focalfootprocesseffacement,GBMdamage–doublecontouring,mesangiolysis.◦ Inseverecases–TMAnoted(fibrindeposi@onandredbloodcellentrapment)◦ Dosedependent◦ *Incidencerangefrom5-10%withbevacizumab,dependingondose,typeoftumorandconcomitanttx◦ Treatment:JudicioususeofRAASblockers.◦ Con@nuechemotherapyunlessrapidworseningofrenalfunc@onorheavyproteinuria◦ Proteinuriacorrelateswithregressionofmalignancy
*Wuetal,JAmSocNephrol.2010Aug;21(8):1381–1389
KDIGO

MembranousGN Malignancymaybeseenin5–20%ofpa@entswithmembranousGN
Mostcommon–Solidtumors(lung,prostate,breast,GI)Lesslikelyhematological
MembranousGNmaybeseenwithGVHDaswell
DeVrieseetalJASN2017
KDIGO

ManagementofCKDinpa@entswithmalignancy
BPcontrol Managementofproteinuria
UseofACEI/ARB ManagementofanemiaofCKD
OtherCKDrelatedissues◦ Boneandmineralmetabolism◦ Metabolicacidosis
Chemotherapyassociatedcomplica@ons
Glomerulonephri@sassociatedwithmalignancy
KDIGO

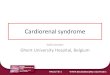
USEOFESAFORANEMIAOFCKDINCANCERPATIENTS CONCERNS◦ Increasedriskformortalityandprogressionofmalignancy
◦ Increasedriskforthromboembolicevents TREATSTUDY◦ RCTofpatentswithDM,CKDandanemia◦ RandomizedtoDarbepoe@ntogetHbto13g/dL
◦ orPlacebowithrescueDarbepoe@nifHb<9.0g/dL
RESULTS◦ PrimaryEP–DeathorCVeventsnodifference
◦ Stroke–higherincidenceinDarbepoe@ngroup.(HR1.92,P<0.001)
6.9% 6.4%1.9% 1.2%7.4% 0.6%0%
1%
2%
3%
4%
5%
6%
7%
8%
Darbepoei@n Placebo
CANCEROUTCOMESINTREATTRIAL
CancerrelatedAE
Deathsapributedtocancer
Deathsapributedtocancerinthosewithmalignancyatbaseline
P=0.002
P=0.08
P=0.53
KDIGO

TreatmentofanemiawithESAinCKD
Nohistoryofmalignancy
StartESAperguidelinesifHb<9Primarygoal–preven@onoftransfusion
KeepHb9-11AvoidexcessivedosesofESAEnsureironreplete
Ac@vemalignancyormalignancyinremission(notconsideredcured)
BloodtransfusionforsevereanemiaIronsupplementa@on
AvoidESAifpossibleIfunabletoavoidESA-discusswithoncologistbenefits/risksUselowestdosepossibletokeepHb>9
Historyofmalignancy(“cured”)
Ifs@llfollowingoncology,d/woncologistbeforeini@a@ngESAStartatlowestpossibledoseEnsureironreplete
MaintainatlowestpossibleESAdosetokeepHb>9andreduceriskfortransfusion
KDIGO

ManagementofBPandMetabolicAcidosis
BLOODPRESSURE GoalBP<130/80mmHg
(JNCVIIIof<120/80mightbetoostringentandhigherriskforAKI)
Pa@entswithmalignancyathighriskforvolumedeple@onandAKI
Judicioususeofdiure@csandACEI/ARB,unlessthereisclearbenefit
METABOLICACIDOSIS
MaintainHCO3>22todelayprogressionofCKD
UseNaHCO3tabletsastolerated–upto1300mg@d
KDIGO

SUMMARY MalignancyiscomplicatedbyAKIandCKDfromvariouscauses
E@ologycanbedirectlyrelatedtomalignancyorchemotherapy
AKI◦ ConcomitantfactorssuchasothernephrotoxinsandsepsisalsocontributetoAKI◦ TLS–recogni@onofriskfactors,intravenoushydra@onandappropriateuseofrasburicaseiskey◦ Castnephropathy–HCOdialyzershaveshownsomepromiseinmanagement,butnotapprovedforuseinUS◦ RenalreplacementtherapyinAKI–ethicalissuesshouldbeconsidered◦ Dose,@ming,andmodalityrecommenda@onsaresimilartopa@entswithoutmalignancy
Concomitantdiseases–DMandHTN–contributetoCKD◦ VEGFinhibitorsleadtoproteinuriaandHTNfromFSGS,TMAorotherpodocyteinjury.◦ Chemotherapyshouldnotbeinterruptedformostpa@entswithproteinuriaandHTN◦ MembranousGNisassociatedwithmalignancy.Pa@entswithMembGNwithnega@vePLA2Rtes@ngshouldbescreenedformalignancy
◦ ESAshouldbeusedcau@ouslyinpa@entswithahistoryofmalignancyandavoidedifpossibleinthosewithmalignancy◦ BPgoalis<130/80.Cau@onwithRAASblockersifpa@enthasrecurrentepisodesofvolumedeple@onandAKI
KDIGO