Embed Size (px)
Citation preview
Management of Acute Respiratory Distress Syndrome – an update
DR. HM Cheung
Department of Paediatrics
Prince of Wales Hospital, Hong Kong.
1
2
Pediatric Acute Respiratory Distress Syndrome (PARDS)
• PARDS is one of the most challenging patient populations
• Even more challenging to us is that there is no definitive data to guide clinical management(1)
3
• Infants and children are not small adults(1)
• more compliant chest walls
• Higher sedation requirement
• Higher baseline airway resistance
• Lower functional residual capacity (FRC)
• More vulnerable to ventilator-induced lung injury
4
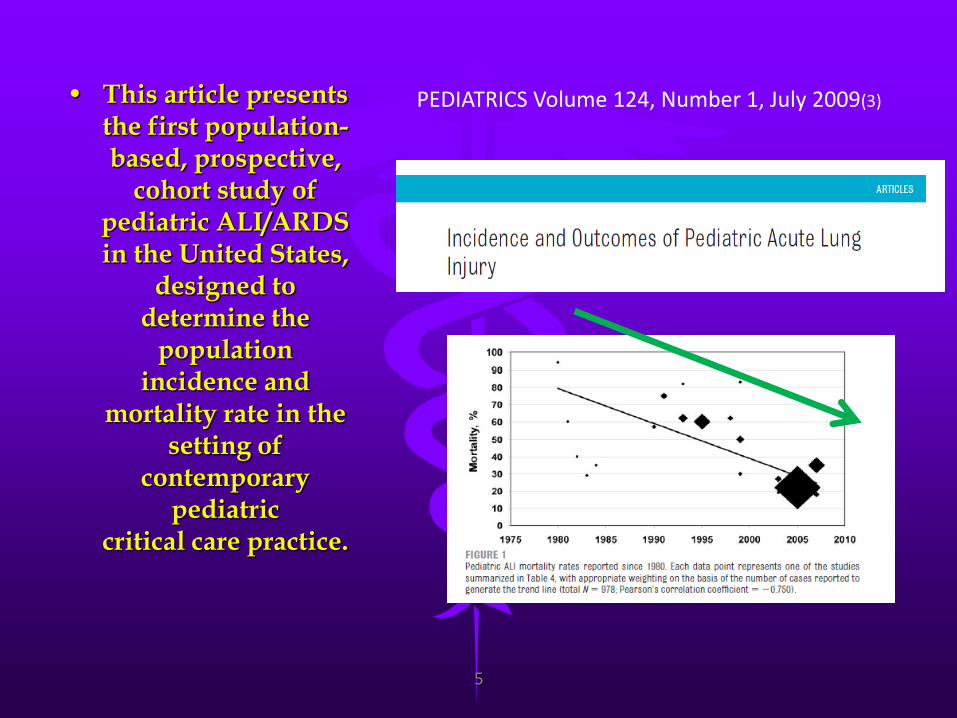
• This article presents the first population-based, prospective,
cohort study of pediatric ALI/ARDS in the United States,
designed to determine the
population incidence and
mortality rate in the setting of
contemporary pediatric
critical care practice.
PEDIATRICS Volume 124, Number 1, July 2009(3)
5
• First large scale systematic analysis of the incidence and mortality of PARDS, revealing a low incidence but a high mortality(4)
Its result indicate that both incidence and mortality of PARDS have not changed over the past two decades
• Crit Care Med. 2015 Oct 27. [Epub ahead of print], PMID: 26509320
6
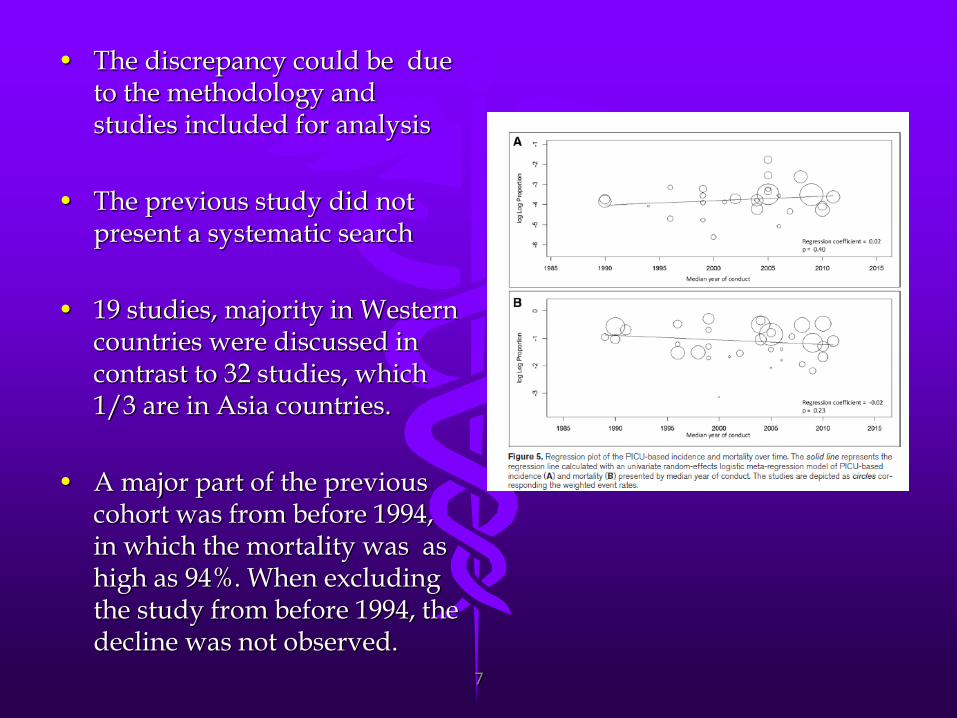
• The discrepancy could be due
to the methodology and studies included for analysis
• The previous study did not present a systematic search
• 19 studies, majority in Western countries were discussed in contrast to 32 studies, which 1/3 are in Asia countries.
• A major part of the previous cohort was from before 1994, in which the mortality was as high as 94%. When excluding the study from before 1994, the decline was not observed.
7
• Goal of management
• Treat the underlying disease
• Achieve adequate tissue and organ oxygenation
• Avoid pulmonary and non-pulmonary complications
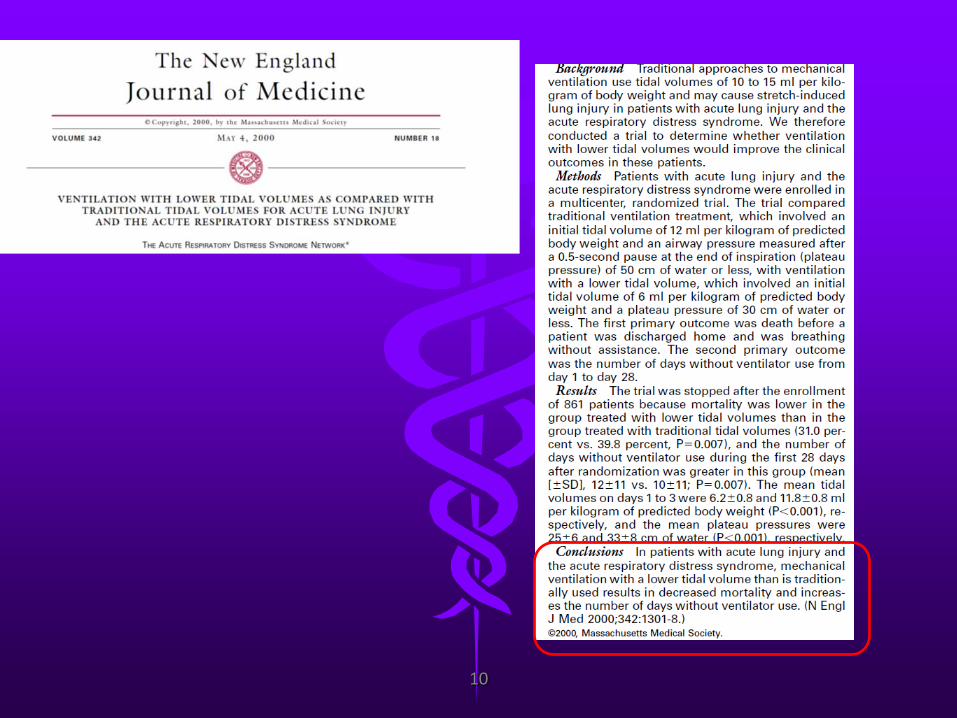
• Increase oxygenation dose not correlate with improve outcome(2)
8
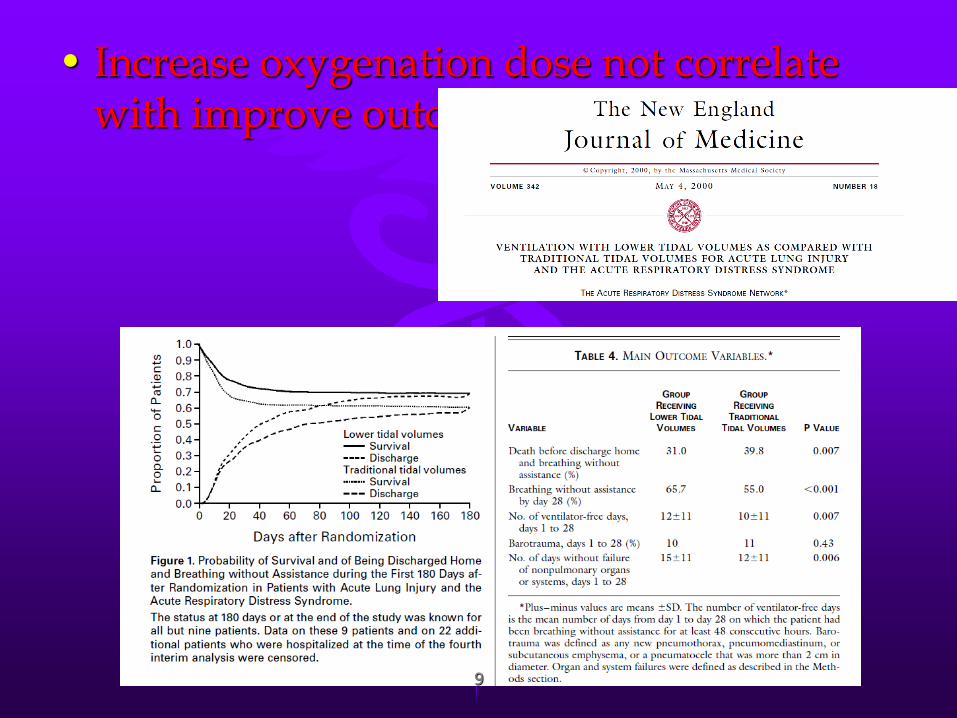
• Increase oxygenation dose not correlate
with improve outcome
9
10
• Permissive hypoxemia(7)
• Accepts lower arterial oxygenation saturation to avoid over
ventilation/ventilation lung injury
• Definitive data to determine the optimal oxygenation level for pediatric patients are not available
• Suggest
• After optimizing PEEP, low SaO2 in the range of 88-92% should be accepted for PEEP equal to 10cm H2O (8)
11
• Permissive hypercapnia(7)
• Consequence of low tidal volume ventilation
• The degree of respiratory acidosis that can be safely tolerated remains controversial
• Most adverse effects associated with respiratory acidosis are minor and reversible when pH is maintained >7.20
• Suggest(8)
• Permissive hypercapnia should be considered for moderate-to-severe PARDS to minimize ventilator induce lung injury
• Bicarbonate supplementation is not routinely recommended
12
Noninvasive ventilation in PARDS
• Use of mask or other interface to provide ventilatory support through a patient’s nose and/or mouth.
• Reduce atelectasis
• Unloads fatigued respiratory muscles, preserve the child’s natural airway
• Avoids some of the complications of invasive ventilation
13
Noninvasive ventilation
• The use has increased significantly over the last decade, increased use from 0.5% to 12.2% between 1999-2008(9)
• Few prospective controlled trials in pediatrics that can guide the determination and strategies for using it.
• Either continuous or bilevel NIPPV
• Reduce work of breathing
• Facilitate airway opening
• Improve oxygenation
14
Noninvasive ventilation
• CONTINUOUS
• Continuous PEEP, maintains the small airway opening, increase end-expiratory opening volume and improve lung compliance
• BILEVEL
• Addition of PIP raise tidal volumes and support fatigued respiratory muscles.
• Avoid the complications associated with endotracheal intubation and invasive ventilation
• Less patient sedation
15
Noninvasive ventilation
16
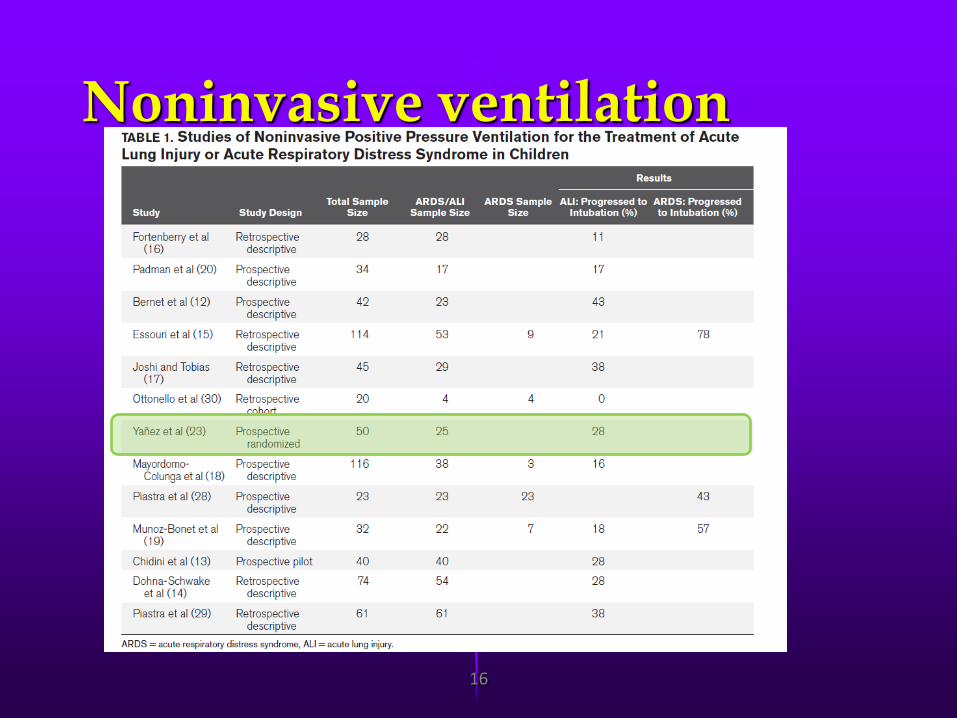
Noninvasive ventilation
• Only one RCT , 50 children with acute hypoxemia respiratory failure, comparing NPPV and standard care. (Yañez LJ, Yunge M, Emilfork M, et al: A prospective, randomized, controlled trial of noninvasive
ventilation in pediatric acute respiratory failure. Pediatr Crit Care Med 2008; 9:484–489)
• Frequency of intubation was significantly lower in NPPV group
• Heart rate and respiratory rate also improved much
17
Noninvasive ventilation(6)
18
Noninvasive ventilation
• Recommendation(5)
• NPPV early in disease in children at risk for PARDS
• Selected group of patients, at greater risk of complication from invasive mechanical ventilation, benefit more from earlier NPPV
• Not recommended for severe disease
19
Noninvasive ventilation
• Little published data to support the routine use of NPPV for treatment of PARDS
• Selected population, mild PARDS, addition of NPPV may prevent intubation and mechanical ventilation
• Moderate and severe PARDS, NPPV not indicated
20
Noninvasive ventilation
• Bilevel NPPV superior than continuous NPPV.
• Can improve oxygenation, alveolar recruitment and provide
additional support during inspiration and unloading the respiratory muscles, reduces the increased work of
breathing.
21
Noninvasive ventilation
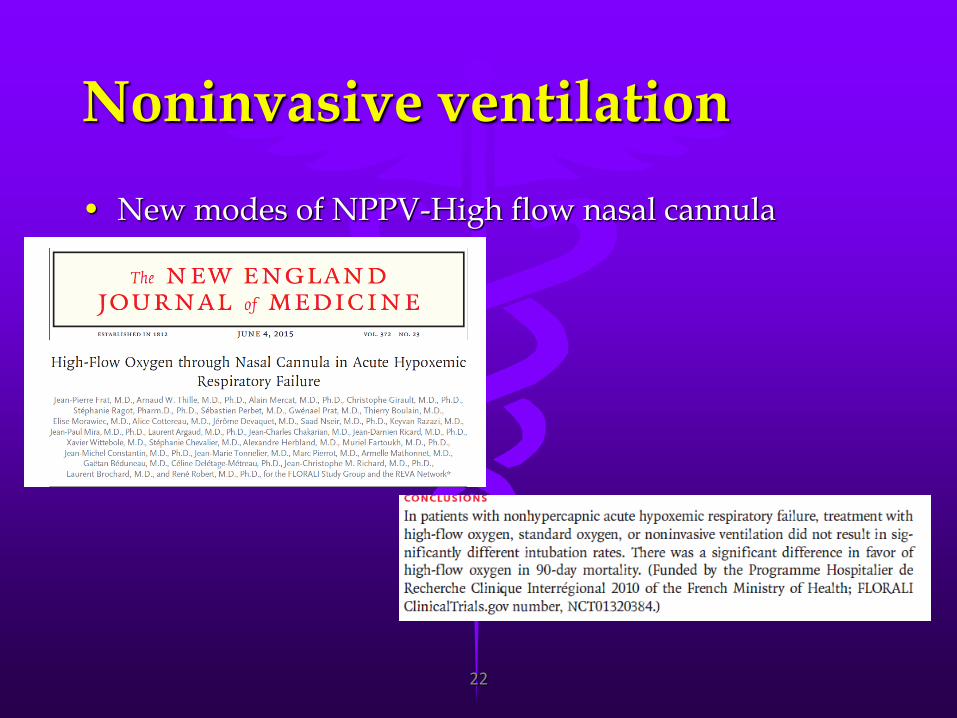
• New modes of NPPV-High flow nasal cannula
22
Invasive Ventilation
• mechanical ventilation to assure adequate gas exchange
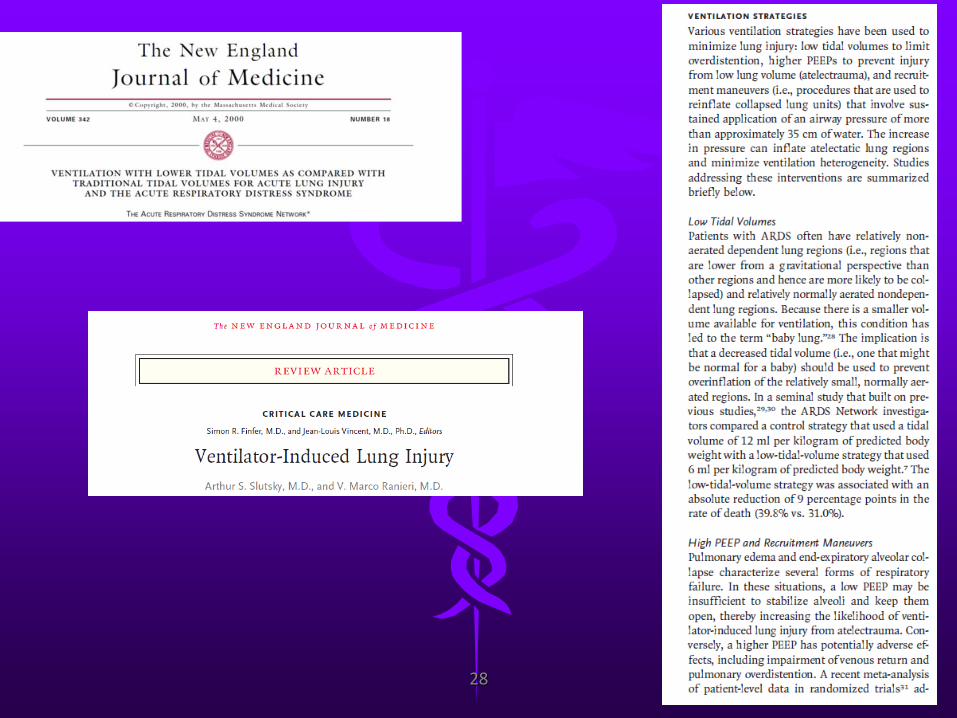
• Ventilator-induced lung injury
• Avoid over-distension(volutrauma)
• Avoid cyclic opening and closing of alveoli(atelectrauma)
• No specific pediatric outcome data on lung protection strategy
23
Invasive Ventilation
• Mode of ventilation(8)
• No outcome data to recommend the mode to be used
• Mostly volume-cycle or pressure-cycle mode
• Maintenance of spontaneous respiration and improve patient-ventilator synchrony
•NAVA- Neurally adjusted Ventilatory assist
•PAV-proportional assist ventilation
•APRV-airway pressure release ventilation 24
Invasive Ventilation
• APRV(7)
• Allows spontaneous breathing throughout all phases of machine imposed respiratory cycle.
• Pressure-limited, time-triggered, and time-cycled mode
25
Invasive ventilation
• HFOV • When toxic conventional mechanical ventilation is required
• 1994
• RCT pediatric HFOV showed improved oxygenation and reduced supplemental oxygen
• Meta-analysis concluded HFOV might improve survival and is unlikely to cause harm
26
Invasive Ventilation
• Tidal volume • In controlled ventilation, use tidal volumes in or below the
range of physiologic tidal volumes for age/body weight(5-8ml/kg predicted body weight)
• Use of patient-specific tidal volumes according to disease severity
• 3-6ml/kg PBW for patients with poor respiratory system compliance
• 5-8ml/Kg PBW for patients with better preserved respiratory system
27
28
Invasive Ventilation
• Pediatric obesity
• Must use ideal body weight
• Predicted body weight
• Using the 50% percentile weight for height
29
Invasive Ventilation
• Positive End Expiratory Pressure (PEEP)
• PEEP maintains the alveolar patency
• Restore functional residual capacity(FRC)
• Maintains trans-thoracic pressure
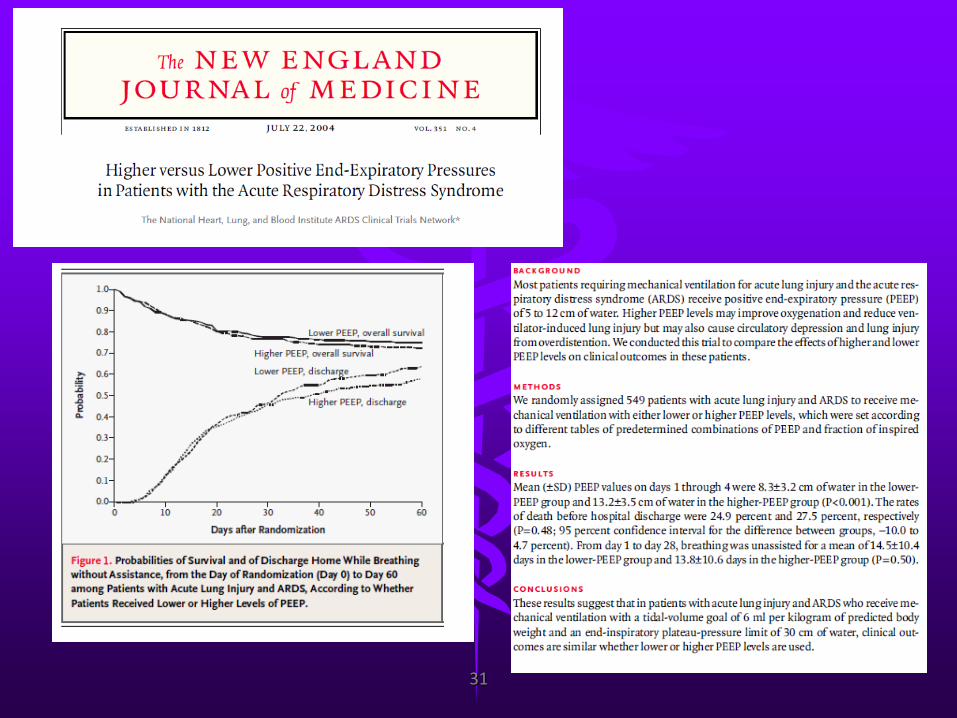
• RCT from ARDS network showed
• Aggressive PEEP strategy resulted in similar survival, although the arterial oxygenation improved with higher PEEP
•Once appropriate PEEP is applied to maintain the lungs at ideal lung volume, further increase in PEEP do not improve outcome
30
31
Invasive Ventilation
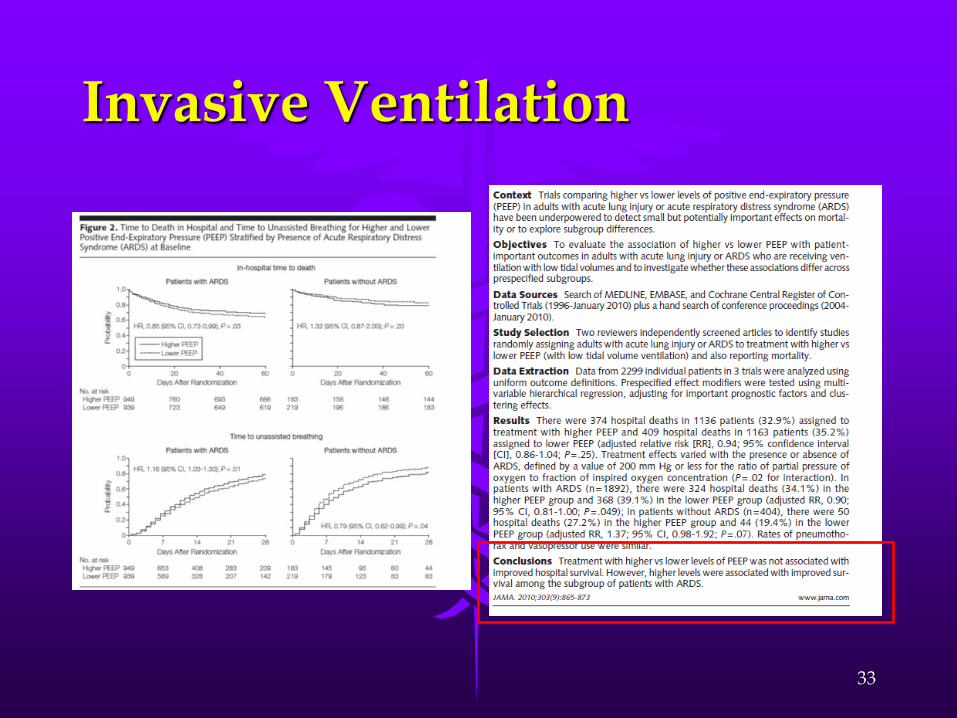
• Matthias Briel in JAMA showed that
• Higher PEEP strategy benefit those with more severe lung injury only(10)
32
Invasive Ventilation
33
Invasive Ventilation
• PEEP
• With no pediatric data, PEEP is now increased to a level that
allows adequate oxygenation at an acceptable FiO2. Severe PEEP of 10-15 cm H2O may be required.
• Excessive PEEP with resultant increase in mean airway
pressure can adversely affect cardiac output.
34
Invasive Ventilation
• PEEP titration
• Titrated until the best possible balance of lowest PIP, deliver the desired tidal volume, highest pulmonary compliance and optimal oxygen delivery
• Gradually increase while assessing the cardiorespiratory
parameters
• Rapid increase with a gradual reduction until the optimal
• As an appropriate PEEP is set, a lower PIP is required
35
Pulmonary specific adjunct threapy • NITRIC OXIDE (NO)
• Hypothesized that iNO should benefit PARDS patients by improving oxygenation, thus minimizing the occurrence of ventilator-induced lung injury.
• Studies only showed short term improvement in gas exchange, but no benefit on length of ventilation, ICU length of stay
• Did not improve mortality
36
Pulmonary specific adjunct threapy • PRONE POSITIONING
• Associated with a significant improvement in oxygenation within 2 hours of placement, with no serious adverse effects noticed
• No difference could be detected between two treatment arms in terms of ventilator-free days, mortality, time to recovery from lung injury
• Cannot be recommended as routine therapy, but should be considered an option in case of severe PARDS 37
Pulmonary specific adjunct threapy • EXOGENOUS SURFACTANT
• No significant decreases in length of mechanical ventilation, hospital stay were seen.
• Did not improve outcome and increase mortality and adverse effects.
38
Pulmonary specific adjunct threapy
• Endotracheal suctioning
• No reported RCT demonstrating a positive contribution of ET
suction using uncontrolled negative pressure
• Recommend
• Maintain a clear airway is essential . ET suction must be performed with caution
• Insufficient data to support the use of open or closed suctioning system. In severe PARDS, should consider giving the suction technique carefully to minimize the potential for derecruitment.
39

Nonpulmonary treatments for PARDS
• SEDATIONS
• Should receive minimal yet effective targeted sedation to facilitate their tolerance to mechanical ventilation
• Valid and reliable pain and sedation scales used
• Sedation monitoring and weaning should be managed by a goal-directed protocol
• Individualized sedation weaning plan.
40
Nonpulmonary treatments for PARDS
• NEURO-MUSCULAR BLOCKADE
• If sedation alone is inadequate to achieve effective mechanical ventilation, NMB should be considered.
41
Nonpulmonary treatments for PARDS
• NUTRITION • Receive a nutrition plan to facilitate recovery, by a
goal-directed protocol
• Early enteral nutrition may be beneficial
• In general, there is consensus that early trophic enteral feeds should be initiated as soon as shock is resolved
• Enteral feeding is generally preferred over parenteral nutrition
• In general, if target enteral nutrition is not achieved within 72 hours, initiation of parenteral nutrition should be considered 42
Nonpulmonary treatments for PARDS
• FLUID MANAGEMENT • Receive total fluid to maintain adequate
intravascular volume, end-organ perfusion, optimal delivery of oxygen
• Minimizing fluid administration would decrease intravascular pressure
• Excessive fluid administration after initial resuscitation may lead to poor outcome
43
Nonpulmonary treatments for PARDS
• BLOOD TRANSFUSION
• RBC transfusion can be lifesaving, but also
associated with short term and long term complications
• A restrictive transfusion strategy, using hemoglobin threshold of 7g/dl has been shown to reduce transfusion with no impact on mortality
44
Extracorporeal life support ECMO
• ECMO was pioneered as a technique to support term or near-term neonates with severe respiratory failure unresponsive to maximal conventional management
• Cochrane database review confirmed the benefit of ECMO in neonates with respiratory failure
• Much of data from ELSO data registry
• High-quality clinical trials evidence exists only in support of the use of ECMO in neonates(0-30days), and adults (>18 years) with severe respiratory failure
45
Extracorporeal life support ECMO
• No agreed criteria for provision of ECMO
• Useful guide
• Oxygenation Index (OI) – reflect oxygenation and level of ventilatory support(surrogate of compliance)
• PaO2/FiO2 (P/F) ratio – measure of lung ability to oxygenate
• OI at which ECMO might considered may be much lower than the historical levels (>40).
46
conclusion
• PARDS with low incidence but high mortality
• With very few high quality pediatric studies on PARDS
• There is no definitive pediatric guideline on the management of PARDS
• Many of the present recommendations refer to studies, data from adult patients
• Further studies would help to establish pediatric specific management guidelines.
47

Reference
1. Ira M Cheifetz, Pediatric Acute Respiratory Distress Syndrome, Respiratory Care 2011;56;10;1589-1599
2. The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342(18):1301–8.
3. Zimmerman JJ, Akhtar SR, Caldwell E, et al. Incidence and outcomes of pediatric acute lung injury. Pediatrics 2009;124:87–95.
4. Laura R. A. Schouten, MD; Floor Veltkamp, MSc; Incidence and Mortality of Acute Respiratory Distress Syndrome in Children: A Systematic Review and Meta-Analysis. Crit Care Med 2016; XX:00–00)
5. Sandrine Essouri, MD, PhD1; Christopher Carroll, MD, MS2; for the Pediatric Acute Lung Injury Consensus Conference Group. Pediatr Crit Care Med 2015;16:S102–S110)
6. Yañez LJ, Yunge M, Emilfork M, et al: A prospective, randomized controlled trial of noninvasive ventilation in pediatric acute respiratory failure. Pediatr Crit Care Med 2008; 9:484–489
7. Ira M Cheifetz, Advance in Monitoring and Management of Pediatric Acute Lung Injury, Pediatric clinic of N. America 2013;60;621-639
48
Reference
8. Peter Reminsberger, Ira M Cheifetz, Ventilatory support in Children with PARDS: proceedings from the Pediatric Acute Lung Injury Consensus Conference. Pediatric Critical Care Medicine2015;16;supplement S51-60
9. Fernandez A, Monteverde E, Farias J: Changes in the practice of mechanical ventilation that took place in cohorts between 1999 and 2008 in PICUs: A multicenter study. Pediatr Crit Care 2012; 13:620
10. Briel M, Meade M, Mercat A, et al: Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: Systematic review and meta-analysis. JAMA 2010; 303:865–873
49