Embed Size (px)
Citation preview
CLINICAL REPORT
aProfessor, DbPostgraduat(UNESP), SãcRadiologist,dPrivate prac
THE JOURNA
Management of accidental swallowing in implant dentistry
Francisley Ávila Souza, DDS, PhD,a Cristian Statkievicz, DDS, MSc,b Ana Laura Guilhem Rosa, MD,c andFabrício da Silveira Bossi, MDd
ABSTRACTThis report describes a protocol for managing the accidental swallowing of dental instruments inimplant dentistry, illustrated by a patient who accidentally swallowed a hexagonal wrench. The firststep was to refer the patient to the medical emergency hospital service for radiographic and clinicalevaluation. The hexagonal wrench was located in the stomach and was immediately removed withan endoscopic procedure. The gastric mucosa was sampled via biopsy and the sample submitted tothe urease test, which was positive for Helicobacter pylori. Triple treatment was instituted forgastritis caused by H pylori to avoid exposing the patient to unnecessary risk. Removal of a foreignbody by means of an endoscopic procedure constitutes a safe and effective treatment. (J ProsthetDent 2015;114:167-170)
The number of accidents in thedental office capable of placingthe patient’s health at risk isrelatively low.1 Nevertheless,when accidents do occur, theyare generally associated withswallowing2 or the aspiration3
of foreign bodies, allergic re-actions to medications4 ordental products,5 or surgical
procedures.6 Implant placement and restoration involvethe handling of small components such as wrenches,connectors, extensions, and rotary instruments that riskbeing accidentally aspirated or swallowed.7 Furthermore,the contact of these instruments with saliva makes themslippery and difficult to handle.7-9Swallowed foreign bodies may migrate through theesophagus, go directly into the stomach, or pass throughthe gastrointestinal tract. However, if the swallowedobject is lodged within the esophagus, it must beimmediately removed because the esophagus is close tothe large thoracic vessels such as the pericardium and thepleura.10 If the object has passed beyond the esophagusinto the stomach, there is a 80% or more probability ofsuccessful progression through the gastrointestinaltract.11,12 The physiological peristaltic waves of thedigestive system will cause the foreign body to beexpelled in 4 to 6 days.12 However, this period mayextend to 14 days,1 and even 40 days.12 The symptomssuggestive of swallowing foreign bodies are dysphagia,discomfort, and retrosternal or abdominal pain,13 and the
epartment of Surgery and Integrated Clinic, Araçatuba Dental School, Sãoe student, Science of Department of Surgery and Integrated Clinic, Araçato Paulo, Brazil.Department of Surgery and Integrated Clinic, Araçatuba Dental School, Sãtice, São Paulo, Brazil.
L OF PROSTHETIC DENTISTRY
complications are hemorrhage, infection, intestinal ob-struction, and perforation.1
If the object is aspirated, it passes through the larynxand trachea. This is a situation with a high risk of suf-focation.14,15 Aspirated foreign bodies tend to lodge inthe right side of the main bronchus,16,17 possibly becauseof the nature of the tracheobronchial tree anatomy.3
Common symptoms of an aspiration are coughing,choking and gasping for breath, acute dyspnea, anddiminished respiratory sounds.14 This clinical report de-scribes the endoscopic procedure used after the acci-dental swallowing of a foreign body.
CLINICAL REPORT
A 65-year-old man was receiving an implant-supporteddental prosthesis for the replacement of a mandibularfirst molar tooth. During the open tray impression, ahexagonal 1.7 wrench for a torque meter (Conexão Sis-temas de Prótese) became detached from the transferscrew after the patient vomited and was swallowed. The
Paulo State University “Júlio de Mesquita Filho” (UNESP), São Paulo, Brazil.uba Dental School, São Paulo State University “Júlio de Mesquita Filho”
o Paulo State University “Júlio de Mesquita Filho” (UNESP), São Paulo, Brazil.
167
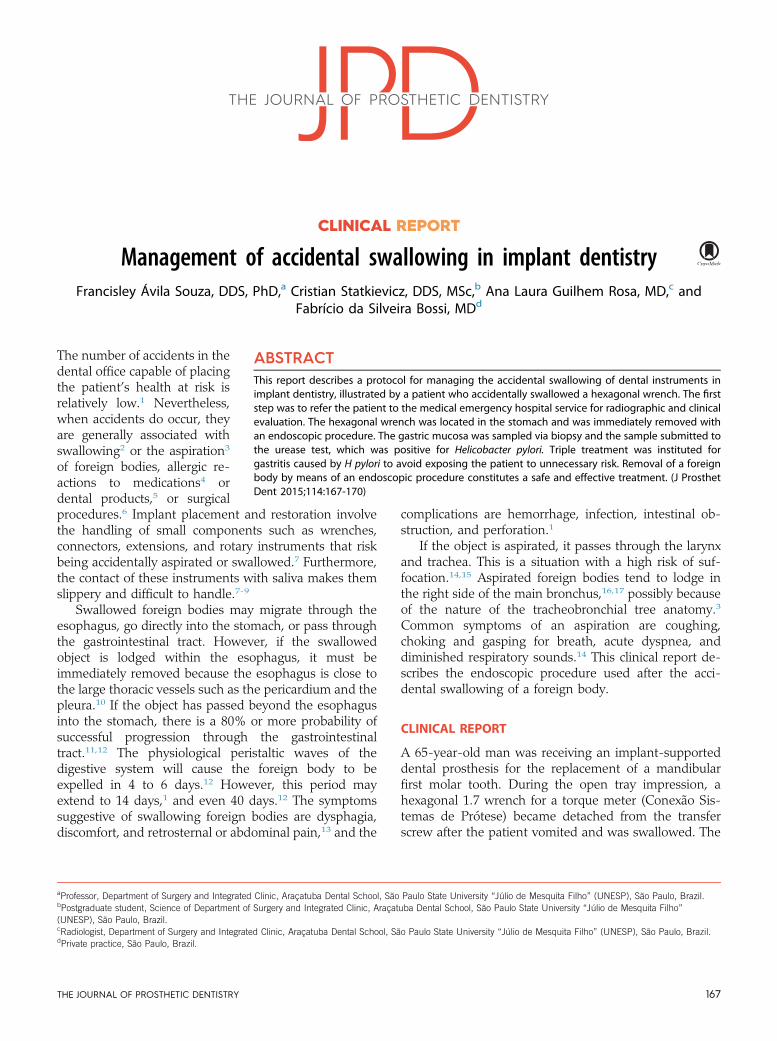
Figure 1. Cervical neck radiograph.
Figure 2. Posterior-anterior thorax radiograph.
Figure 3. Posterior-anterior abdomen radiograph. Red arrow:Radiopacity suggestive of hexagonal wrench.
Figure 4. Beginning of endoscopic procedure.
168 Volume 114 Issue 2
patient was reassured and immediately taken to anemergency room. Radiographs of the cervical spine,thorax, and abdomen were requested.
The profile cervical radiograph showed accentuateddegenerative bone alterations but no signs of compro-mise of the soft tissues or anything suggestive of theforeign body (Fig. 1). The thorax radiograph showednormal transparency of the pulmonary fields. No imagesuggestive of a radiopaque foreign body was observed
THE JOURNAL OF PROSTHETIC DENTISTRY
(Fig. 2). The simple radiograph of the abdomen, madewith the patient lying face up, showed a radiopaqueimage with an elongated morphology situated in thegastric topography and suggestive of the hexagonalwrench (Fig. 3).
The first choice of treatment to remove the wrenchwas an endoscopic procedure. Another treatment optionwas clinical follow-up to wait for passage through thegastrointestinal tract. The patient was positioned lying onhis left side, with a nasal catheter providing 100% oxygen(White Martins Praxair) in the ratio of 2 L/min and pe-ripheral venous access in the right upper limb infusing a5% glucose solution. He was sedated with 0.05 mg/kg ofmidazolam (Dormonid; Roche Laboratories), 0.5 mg/kg offentanyl hydrochloride (Fentanil; Cristalia Laboratories),and 0.5 mg/kg of propofol (Diprivan 1%; AstraZenecaLaboratories). An occlusal device was placed in thepatient’s oral cavity (Fig. 4), and a video gastroscope590 WR (Fujinon Co) was introduced with free passagethrough the oropharynx, esophagus, and stomach.The gastric mucosa presented the usual shape, exceptfor evidence in the antrum region of an erythematoussegmental area associated with the hexagonal wrench
Souza et al
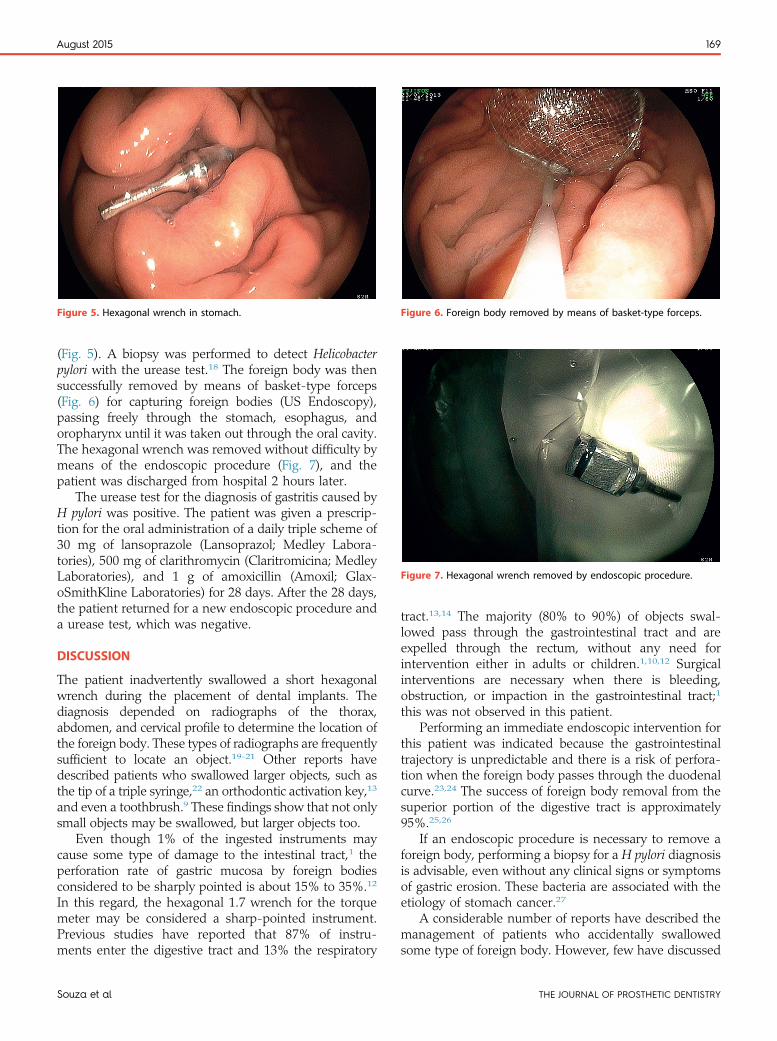
Figure 6. Foreign body removed by means of basket-type forceps.
Figure 7. Hexagonal wrench removed by endoscopic procedure.
Figure 5. Hexagonal wrench in stomach.
August 2015 169
(Fig. 5). A biopsy was performed to detect Helicobacterpylori with the urease test.18 The foreign body was thensuccessfully removed by means of basket-type forceps(Fig. 6) for capturing foreign bodies (US Endoscopy),passing freely through the stomach, esophagus, andoropharynx until it was taken out through the oral cavity.The hexagonal wrench was removed without difficulty bymeans of the endoscopic procedure (Fig. 7), and thepatient was discharged from hospital 2 hours later.
The urease test for the diagnosis of gastritis caused byH pylori was positive. The patient was given a prescrip-tion for the oral administration of a daily triple scheme of30 mg of lansoprazole (Lansoprazol; Medley Labora-tories), 500 mg of clarithromycin (Claritromicina; MedleyLaboratories), and 1 g of amoxicillin (Amoxil; Glax-oSmithKline Laboratories) for 28 days. After the 28 days,the patient returned for a new endoscopic procedure anda urease test, which was negative.
DISCUSSION
The patient inadvertently swallowed a short hexagonalwrench during the placement of dental implants. Thediagnosis depended on radiographs of the thorax,abdomen, and cervical profile to determine the location ofthe foreign body. These types of radiographs are frequentlysufficient to locate an object.19-21 Other reports havedescribed patients who swallowed larger objects, such asthe tip of a triple syringe,22 an orthodontic activation key,13
and even a toothbrush.9 These findings show that not onlysmall objects may be swallowed, but larger objects too.
Even though 1% of the ingested instruments maycause some type of damage to the intestinal tract,1 theperforation rate of gastric mucosa by foreign bodiesconsidered to be sharply pointed is about 15% to 35%.12
In this regard, the hexagonal 1.7 wrench for the torquemeter may be considered a sharp-pointed instrument.Previous studies have reported that 87% of instru-ments enter the digestive tract and 13% the respiratory
Souza et al
tract.13,14 The majority (80% to 90%) of objects swal-lowed pass through the gastrointestinal tract and areexpelled through the rectum, without any need forintervention either in adults or children.1,10,12 Surgicalinterventions are necessary when there is bleeding,obstruction, or impaction in the gastrointestinal tract;1
this was not observed in this patient.Performing an immediate endoscopic intervention for
this patient was indicated because the gastrointestinaltrajectory is unpredictable and there is a risk of perfora-tion when the foreign body passes through the duodenalcurve.23,24 The success of foreign body removal from thesuperior portion of the digestive tract is approximately95%.25,26
If an endoscopic procedure is necessary to remove aforeign body, performing a biopsy for a H pylori diagnosisis advisable, even without any clinical signs or symptomsof gastric erosion. These bacteria are associated with theetiology of stomach cancer.27
A considerable number of reports have described themanagement of patients who accidentally swallowedsome type of foreign body. However, few have discussed
THE JOURNAL OF PROSTHETIC DENTISTRY

170 Volume 114 Issue 2
the prevention of these complications. Some have sug-gested using of a rubber dam or the use of a gauze screento protect the oropharynx as a barrier, providing in-structions to the patient before the procedure, ensuringproper positioning of the patient, using powerful suctionequipment, keeping a firm grip on instruments duringthe dental procedure, and attaching dental floss to smallobjects.7,28 For this patient, the use of dental flossattached to the hexagonal wrench for a torque metercould have prevented this accident.
REFERENCES
1. De Souza JG, Schuldt Filho G, Pereira Neto AR, Lyra HF, Bianchini MA,Cardoso AC. Accident in implant dentistry: involuntary screwdriveringestion during surgical procedure. A clinical report. J Prosthodont 2012;2:191-3.
2. Kuo SC, Chen YL. Accidental swallowing of an endodontic file. Int Endod J2008;41:617-22.
3. Adewumi A, Kays DW. Stainless steel crown aspiration during sedation inpediatric dentistry. Pediatr Dent 2008;30:59-62.
4. Haïkel Y, Braun JJ, Zana H, Boukari A, De Blay F, Pauli G. Anaphylactic shockduring endodontic treatment due to allergy to formaldehyde in a root canalsealant. J Endod 2000;26:529-31.
5. Levi L, Barak S, Katz J. Allergic reactions associated with metal alloys inporcelain-fused-to-metal fixed prosthodontic devices-a systematic review.Quintessence Int 2012;43:871-7.
6. Schwartz AB, Larson EL. Antibiotic prophylaxis and postoperative compli-cations after tooth extraction and implant placement: a review of the litera-ture. J Dent 2007;35:881-8.
7. Umesan UK, Chua KL, Balakrishnan P. Prevention and management ofaccidental foreign body ingestion and aspiration in orthodontic practice. TherClin Risk Manag 2012;8:245-52.
8. Mohan R, Rao S, Benjamin M, Bhagavan RK. Accidental ingestion of abarbed wire broach and its endoscopic retrieval: prevention better than cure.Indian J Dent Res 2011;22:839-42.
9. Kim IH, Kim HC, Koh KH, Kim SH, Kim SW, Lee SO, et al. Journey of aswallowed toothbrush to the colon. Korean J Intern Med 2007;22:106-8.
10. Samdani T, Singhal T, Balakrishnan S, Hussain A, Grandy-Smith S, El-Hasani S. An apricot story: view through a keyhole. World J Emerg Surg2007;2:20.
11. Smith MT, Wong RKH. Esophageal foreign bodies: types and techniques forremoval. Curr Treat Options Gastroenterol 2006;9:75-84.
12. American Society for Gastrointestinal Endoscopy. Guidelines for the man-agement of ingested foreign bodies ond food impactions. GastrointestEndosc 2011;73:1085-91.
THE JOURNAL OF PROSTHETIC DENTISTRY
13. Monini AC, Maia LG, Jacob HB, Gandini LG. Accidental swallowing of or-thodontic expansion appliance key. Am J Orthod Dentofacial Orthop2011;140:266-8.
14. Milton TM, Hearing SD, Ireland AJ. Ingested foreign bodies associated withorthodontic treatment: report of three cases and review of ingestion/aspira-tion incident management. Br Dent J 2001;190:592-6.
15. Tripathi T, Rai P, Singh H. Foreign body ingestion of orthodontic origin. Am JOrthod Dentofacial Orthop 2011;139:279-83.
16. Black RE, Johnson DG, Matlack ME. Bronchoscopic removal of aspiratedforeign bodies in children. J Pediatr Surg 1994;29:682-4.
17. de Oliveira CF, Almeida JF, Troster EJ, Vas FA. Complications of trachoe-bronchial foreign body aspiration in children: report of 5 cases and review ofliterature. Rev Hosp Clin Fac Med Sao Paulo 2002;57:108-11.
18. Wong AS, Ching SS, Long AS. The use of a second biopsy from the gastricbody for the detection of Helicobacter pylori using rapid urease test. SingaporeMed J 2014;55:644-7.
19. O’Connor TE, Cooney T. Oesophageal foreign body and a double aortic arch:rare dual pathology. J Laryngol Otol 2009;123:1404-6.
20. Worthington P. Ingested foreign body associated with oral implant treat-ment: report of a case. Int J Oral Maxillofac Implants 1996;11:679-81.
21. Ikenberry SO, Jue TL, Anderson MA, Appalaneni V, Banerjee S, Ben-Menachem T, et al. Management of ingested foreign bodies and food im-pactions. Gastrointest Endosc 2011;73:1085-91.
22. Govila CP. Accidental swallowing of an endodontic instrument. A report oftwo cases. Oral Surg Oral Med Oral Pathol 1979;48:269-71.
23. Spitz L. Management of ingested foreign bodies in childhood. Br Med J1971;4:469-72.
24. Suita S, Ohgami H, Nagasaki A, Yakabe S. Management of pediatric patientswho have swallowed foreign objects. Am Surg 1989;55:585-90.
25. Mosca S, Manes G, Martino R, Amitrano L, Bottino V, Bove A, et al.Endoscopic management of foreign bodies in the upper gastrointestinal tract:report on a series of 414 adult patients. Endoscopy 2001;33:692-6.
26. Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, Liao Z. Endoscopic management offoreign bodies in the upper-GI tract: experience with 1088 cases in China.Gastrointest Endosc 2006;64:485-92.
27. Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S,Yamakido M, et al. Helicobacter pylori infection and the development of gastriccancer. N Engl J Med 2001;13:784-9.
28. Zitzmann NU, Elsasser S, Fried R, Marinello CP. Foreign body ingestion andaspiration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88:657-60.
Corresponding author:Dr Francisley Ávila SouzaDepartment of Surgery and Integrated ClinicSão Paulo State University “Júlio de Mesquita Filho” (UNESP)Araçatuba, São PauloBRAZILEmail: [email protected]
Copyright © 2015 by the Editorial Council for The Journal of Prosthetic Dentistry.
Souza et al