Embed Size (px)
Citation preview
EXECUTIVEManagedHealthcareExecutive.com The C-Suite Advisor
Managed H
ealthcare Executive
April 2016 VOL. 26 NO. 4
What’s new in diabetes drugs?
Five reasons diabetic patients don’t adhere
Applying predictive modeling to diabetes care
HOW TO MAXIMIZE
DIABETES DOLLARSEarly detection, strategic investments are key
AP
RIL 2016
How
to maxim
ize diabetes dollars | Advancing collaborative care m
odels | Big data’s exploding legal environm
ent | Are E
HR
s delivering on expectations? VO
LUM
E 26 | N
UM
BE
R 4
PAGE 8

MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 ManagedHealthcareExecutive.com2
Opinion
ommon scenario: A doctor sees a
patient who is overweight and com-
plaining of fatigue, increased thirst and
occasional blurred vision. Th e doctor
immediately recognizes these signs and
symptoms and suggests a screening for
diabetes.
Q: What if we could have prevented this doctor appointment altogether?
Most healthcare models today are in a reactive model—
meaning once a patient starts showing symptoms of type
2 diabetes, the doctor orders the necessary screenings and
recommends the appropriate prescriptions. New recom-
mendations from Th e United States Preventive Services
Task Force advise providers to screen all overweight and
obese adults between ages 40 and 70 for abnormal blood
sugar levels. In other words, once a person has a risk fac-
tor—in this case, overweight—then the screening is done.
However, some at-risk Americans won’t have an interac-
tion with a provider this year. Others who are not classifi ed
as overweight, or who are younger than age 40, won’t be
screened but could still have the abnormal blood sugar
levels that characterize prediabetes. Without intervention,
prediabetes is likely to progress to diabetes within 10 years,
according to the Mayo Clinic. But with lifestyle modifi ca-
tions, such as changes to diet, people with prediabetes can
delay or even prevent type 2 diabetes.
Where we are vs. where we’re goingEnter the advanced predictive model of diabetes preven-
tion. Th is model takes an in-depth look at past health
assessments, old medical claims, lab results and electronic
health records to anticipate who is at risk for the disease
and allows providers to intervene. So instead of relying on
the patient to complain of symptoms, at Humana, we’re get-
ting ahead of the process and using past evidence to inform
proactive preventive care.
Our predictive model came about during our partner-
ship with Omada Health and the CDC’s National Diabetes
Prevention Program (DPP), when we found we were strug-
gling to identify individuals predisposed to diabetes. Of
our more than 3 million Medicare Advantage members, we
could identify only about 9,000 who were at risk.
So we created a model that uses multiple data points
and analytics to fi nd more people at risk. We use this
model to inform as many as 800,000 people of their risk and
to connect them to resources that help them reduce their
risk. Th e intervention components include small-group
support, health coaching, DPP curriculum, and digital
tracking tools. Six months after starting the program, mem-
bers reported an average weight loss of 8.7% of their total
body weight and more than 85% of participants maintained
adequate activity levels.
Others are using predictive models, too. At the state
level, organizations are beginning to implement programs
and engage in partnerships that use a predictive model by
using historical data to better inform patient outcomes. For
example, the Commonwealth of Kentucky (state govern-
ment) implemented the DPP for its employees, which
includes a CDC-approved, evidence-based lifestyle program
to prevent or delay onset of type 2 diabetes. More than 680
organizations are enrolled in the program, and it reaches
more than 30,000 participants.
Getting ahead of itIdentifying individuals at risk for type 2 diabetes in a
timely fashion could, over time, be a catalyst to a smaller
population of disease diagnoses. If we can connect the dots
between the technology at patients’ fi ngertips and link
it to the medical history, we can make more prescriptive
decisions, engage in early intervention and help stop this
lifestyle disease in its tracks.
from ROY BEVERIDGE, MD
ABOUT THE AUTHOR ❚
Roy Beveridge, MD, a member of the Managed Healthcare
Executive Editorial Advisory Board, is the chief medical
offi cer for Humana.
Past evidence informs proactive preventive care
CA step ahead of diabetes
ManagedHealthcareExecutive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 3
EXECUTIVEEditorial Advisory Board
David Calabrese, RPh, MHP, is vice president and
chief pharmacy offi cer of OptumRx, a pharmacy benefi ts fi rm that
manages more than 200 million prescriptions each year on behalf
of 25 million members.
Kevin Ronneberg, MD, is vice president and associate
medical director for health initiatives at HealthPartners, an
integrated, nonprofi t healthcare provider and health insurance
company located in Bloomington, Minnesota.
Mark Boxer, PhD, is executive vice president and global
chief information offi cer for CIGNA, where he is responsible for
driving the company’s worldwide technology strategy.
Daniel J. Hilferty, MPA, is president and chief
executive offi cer of Independence Blue Cross, a leading health
insurer in southeastern Pennsylvania with nearly 10 million
members in 25 states.
Joel V. Brill, MD, is the chief medical offi cer for Predictive
Health, LLC, which partners with stakeholders to improve coverage
of value-driven care that optimizes health for people.
Margaret A. Murray, MPA, is the founding chief
executive offi cer of the Association for Community Affi liated Plans,
which represents 54 nonprofi t safety net health plans in 26 states.
Roy Beveridge, MD, is senior vice president and chief
medical offi cer for Humana, where he’s responsible for developing
and implementing Humana’s clinical strategy with an emphasis on
advancing the company’s integrated care delivery model.
Don Hall, MPH, is principal of DeltaSigma LLC, a consulting
practice specializing in strategic problem solving for managed
care organizations. He most recently served as president and chief
executive offi cer of a nonprofi t, provider-sponsored health plan.
Douglas L. Chaet, FACHE, is senior vice president of
contracting and provider networks at Independence Blue Cross in
Philadelphia. He is also the founder and chairman emeritus of the
American Association of Integrated Healthcare Delivery Systems.
Dennis Schmuland, MD, is chief health strategy offi cer,
U.S. Health & Life Sciences division of Microsoft Corp., where he
is responsible for setting the company’s strategy and overseeing
solutions for the managed care industry.
Perry Cohen, PharmD, is chief executive offi cer of The
Pharmacy Group and the TPG family of companies, which provides
services to associations, healthcare and information technology
organizations, payers and pharmaceutical companies.
Paul J. Setlak, PharmD, MBA, is associate director,
Outcomes Solutions, at Astellas Pharma, where he focuses on
strategic market access, pricing and reimbursement.
Mission Managed Healthcare Executive provides healthcare executives at health plans and provider organizations with analysis, insights, and strategies to pursue value-driven solutions.
CONTENT
SARA MICHAELVP, Content & Strategy
AUBREY WESTGATEExecutive Editor(203) 523-7116, [email protected]
TRACEY L. WALKER Content Manager(440) 891-2732, [email protected]
NANCY BITTEKERDirector, Design and Digital Production(203) 523-7074, nancy.bitteker.ubm.com
ROBERT MCGARRGroup Art Director(440) 891-2628, [email protected]
PUBLISHING & SALES
GEORGIANN DECENZOExecutive Vice President, Managing Director
KEN SYLVIAVice President, Group Publisher
WILLIAM MULDERRYGroup Publisher(732) 346-3071, [email protected]
TOD MCCLOSKEYSales Manager Classifi ed/Display Adv(440) 891-2739, [email protected]
PATRICK CARMODYAccount Manager Classifi ed /Display(440) 891-2621, [email protected]
JOANNA SHIPPOLIAccount Manager, Recruitment Advertising(440) 891-2615, [email protected]
SARAH CAMERON MIFSUDVP, Digital Solutions
DON BERMANSales Director, Digital Media
ALEX CALAccount Director, Digital (203) 523-7042, [email protected]
TERRY TETZLAFFDigital Traffi c Coordinator(218) 740-6585, [email protected]
DAVID DONOVANVP, Digital Products
MEG BENSONSpecial Projects Director
AMY ERDMANVP, Marketing
GAIL KAYEDirector of Marketing & Research Services
RENEE SCHUSTERList Account Executive(440) 891-2613, [email protected]
MAUREEN CANNONPermissions(440) 891-2742, [email protected]
PRODUCTION
KAREN LENZENProduction Director(218) 740-6371, [email protected]
AUDIENCE DEVELOPMENT
JOY PUZZOVP, Marketing & Audience Development
CHRISTINE SHAPPELLDirector, Audience Development
KELLY KEMPERAudience Development Manager
REPRINTS: 877-652-5295 ext. 121, [email protected]. Outside US, UK, direct dial: (281) 419-5725. Ext. 121 SUBSCRIPTION SERVICES: 888-527-7008
EXECUTIVE
MANAGED HEALTHCARE EXECUTIVE ] APRIL 2016 Managed Healthcare Executive.com4
ESSENTIALS
20 TECHNOLOGY Are EHRs delivering on expectations?
by Donna Marbury
22 HEALTH MANAGEMENT Five reasons diabetic patients don’t
adhere
by Karen Appold
28 HOSPITALS AND PROVIDERS Advancing collaborative care models
by Aine Cryts
30 Q&A Calculating diabetes costs
by Karen Appold
32 POLICY OUTLOOK Do prescription drug monitoring
programs work?
by Rachael Zimlich
36 DRUGS IN THE PIPELINE Patient volume, price increases drive
rising diabetes drug spend
by Tracey Walker
38 PHARMACY BEST PRACTICES Managing costs: specialty infusibles
by Mari Edlin
COMMENTARY
2 OPINION A step ahead of diabetes
by Roy Beveridge, MD
5 LETTER OF THE LAW Big data’s exploding legal environment
by Basil Kim
19 MANAGED CARE OUTLOOK Undiagnosed diabetes: A high cost for the
health system
by Edmund J. Pezalla, MD
DEPARTMENTS
3 EDITORIAL ADVISORS
Cove
r: G
etty
Imag
es/D
igita
lVisi
on/A
tom
ic Im
ager
y
Volume 26 Issue 4
APRIL 2016
HOW TO MAXIMIZE
DIABETES DOLLARS
10 Telemedicine expands reach 12 Prediabetes program makes gains
8 Care management initiatives 9 Rates by state
Early detection, strategic investments are key
© 2016 UBM. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission in writing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specifi c clients is granted by UBM for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: [email protected].
UBM Medica provides certain customer contact data (such as customer’s name, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities that may be of interest to you. If you do not want UBM Medica to make your contact information available to third parties for marketing purposes, simply call toll-free 866-529-2922 between
the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from UBM Medica’s lists. Outside the U.S., please phone 218-740-6477.
MANAGED HEALTHCARE EXECUTIVE does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.
MANAGED HEALTHCARE EXECUTIVE welcomes unsolicited articles, manuscripts, photographs, illustrations and other materials but cannot be held responsible for their safekeeping or return.
Library Access Libraries off er online access to current and back issues of Managed Healthcare Executive through the EBSCO host databases.
To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
Managed Healthcare Executive (ISSN 1533-9300, Digital ISSN 2150-7120) is published monthly by UBM Medica 131 W First St., Duluth MN 55802-2065. Subscription rates: 1 year $99.00, 2 years $145.00 in the United States & Possessions; 1 year $122.00, 2 years $173.25 in Canada and Mexico; 1 year $192.00, 2 years $295.00 in all other countries. For air-expedited service, include an additional $87.00 per order annually. Single copies (prepaid only): $9.00 in the United States, $22.00 all other countries. Back issues, if available: $15.00 in the U.S.; $17.00 all other countries. Include $6.85 per order plus $2 per additional copy for U.S. postage and handling. If shipping outside the U.S., include an additional $10 per order plus $3 per additional copy. Periodicals postage paid at Duluth MN 55806 and additional mailing offi ces. POSTMASTER: Please send address changes to Managed Healthcare Executive, P.O. Box 6178, Duluth, MN 55806-6178. Canadian GST number: R-124213133RT001, PUBLICATIONS MAIL AGREEMENT NO. 40612608, Return Undeliverable Canadian Addresses to: IMEX Global Solutions, P. O. Box 25542, London, ON N6C 6B2, CANADA. Printed in the U.S.A.

ManagedHealthcareExecutive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 5
Letter of the Lawthoughts from BASIL KIM
he use of big data continues to be
explored with enthusiasm across
all facets of the healthcare ecosys-
tem, with much of the discussion
surrounding new technologies and
their potential impact on healthcare
stakeholders’ bottom lines. How-
ever, with several high-profi le data
system breach reports, as well as a recent Supreme Court
decision highlighting the complexity surrounding the
management of health information, understanding the
legal and compliance considerations in the current envi-
ronment is imperative.
“Big data” is a term used to describe large volumes of
information, whether structured or unstructured, gener-
ated on an everyday basis. It is not the amount of data that
is signifi cant, however; rather, it is what healthcare enti-
ties (managed care plans, providers, government agen-
cies, etc.) decide to do with it. Big data can be mined for
insights that lead to informed decision-making, leading to
cost savings and better outcomes, whether the metric is
performance-based or fi nancial.
Complex legal questionsTh e amount of information being generated is substan-
tial, yet the full potential of such data remains untapped.
Current trends regarding the use of such data include ev-
idence-based decision-making, a move toward outcome-
based reimbursement, and the use of predictive analytics.
However, in the midst of the big data storm, legal ex-
perts continue to debate how data should be collected and
used. For example, Gobeille vs. Liberty Mutual Insurance
Company, just decided by the Supreme Court, answered
the question of whether the Employee Retirement Income
Security Act (ERISA) preempts Vermont's healthcare data-
base law as applied to the third-party administrator (TPA)
for a self-funded ERISA plan (the short answer: it does).
While the decision ultimately was about the scope of
ERISA preemption, of greater interest is its impact on the
management of big data sources maintained by health
plans. Th e case also brought to light increasingly com-
plex questions regarding the interplay of federal and state
laws on the control of health information. Justice Breyer
suggested that the Departments of Labor or Health and
Human Services be the ones to develop uniform rules to
procure data in a simpler way.
Nuances in other issues of data ownership and ana-
lytic use are highlighted when healthcare entities further
consider similar circumstances; “ownership” analysis dif-
fers signifi cantly for insurers dealing with member data
versus insurers dealing with data they receive as TPAs.
Adding yet another layer of complexity is the potential for
misuse, as evidenced by the fact that three of the largest
historical healthcare data breaches were reported in 2015.
Th e amount of data being collected and maintained by
healthcare organizations will continue to grow, as will the
number of individuals seeking to gain access to the same
increasingly valuable information.
Future outlookTh e value of big data in healthcare is becoming even more
apparent as numerous sophisticated analytical tools are
developed. However, it is important to keep tabs on the
legal and compliance conversation that surrounds the
use of such data. While still in fl ux, privacy and security
concerns (counterbalanced against the transparency and
collaboration interests of all parties) will continue to be
crucial to understand and overcome.
ABOUT THE AUTHOR ❚
Basil H. Kim is an associate in the Health Care and Life
Sciences practice, in the New York offi ce of Epstein Becker
Green. He concentrates on the areas of managed care,
healthcare law, and transactional/regulatory matters.
State and federal regulations, health information
breaches create a minefi eld of issues
This column is written for informational purposes only and should not be construed as legal advice.
Big data’s exploding legal environment
O=�N=�KH=FL��)*�Q=9JK
D=9JFAF?�@GO��LG�C==H�QGMJ��
H9LA=FLKGML�G>�QGMJ��=P9E�JGGE&HGHMD9LAGF@=9DL@A=J
=PH=JA=F;=�L@=�F=LOGJCOAL@�J=9D�HGHMD9LAGF��
@=9DL@�J=KMDLK
LEARN MORE AT ATHENAHEALTH.COM/POPULATION-HEALTH
55%REDUCTION
IN SPENDINGGROWTH1
16%INCREASE
IN NETWORKUTILIZATION2
63%RECEIVED
MSSP PAYMENTVS. 25%
NATIONWIDE3
MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com8
HOW TO MAXIMIZE
Early detection, strategic investments are key
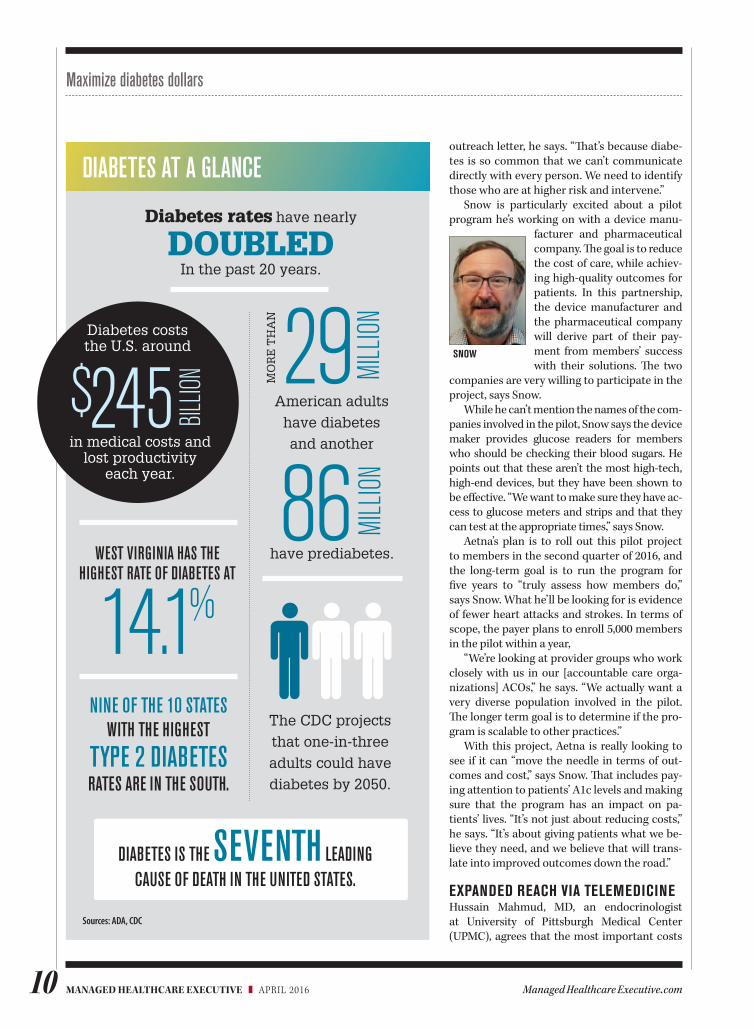
HE TOTAL COST to treat patients diag-nosed with diabetes in the United States jumped from $174 billion in 2007 to $245
billion in 2012 (the last year for which numbers are available). Th at’s a staggering 41% increase over a fi ve-year period, according to the Ameri-can Diabetes Association (ADA).
Hospital inpatient care represents 43% of the total cost of treating diabetes, whereas prescrip-tion medications to treat the chronic disease are 18% of that total. Additional costs include anti-diabetic agents and diabetes supplies (at 12%), physician offi ce visits (at 9%), and nursing or residential facility stays (at 8%).
People with diabetes will have medical ex-penses of about $13,700 a year, which includes $7,900 that are directly associated with the dis-ease—and that’s about 2.3 times higher than the medical costs incurred by people who don’t have diabetes, according to the ADA.
In terms of sheer numbers, more than 29 million people in this country have diabetes, according to the Centers for Disease Control and Prevention (CDC). Perhaps even more trou-bling, the CDC highlights that another 86 mil-
lion people, one in three U.S. adults, have predi-abetes, which means a person has blood sugar levels that are higher than normal but not high enough to be diagnosed as diabetes. Taking a look at the next fi ve years, the CDC says that—absent weight loss and moderate physical activ-ity—15% to 30% of those with prediabetes will develop type 2 diabetes.
Here are some of the innovative approaches payers and providers are taking to quell this epi-demic, and curb the costs associated with it.
CARE MANAGEMENT PLUS INDUSTRY PARTNERSHIPSWhile the cost of treating diabetes itself is sig-nifi cant, it’s the cost of treating the disease inad-equately or poorly that really concerns Kenneth Snow, MD, medical director at Aetna. Th at’s because of the long-term complications—such as blindness, end-stage renal disease, heart dis-ease, and the need for amputations. “Not only is diabetes catastrophic for patients in the long term, it’s extraordinarily expensive,” he says.
Th e disease now impacts more than 9% of the adult population, and 1.5 million more peo-
By AINE CRYTS

ManagedHealthcareExecutive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 9
Maximize diabetes dollars
ple are diagnosed every year, says Snow, noting that minority populations are far more likely to suff er from the disease. Th is is particularly the case for African Americans, Native Americans, Asian Americans, and Hispanics. Further, 28% of Medicare patients have been diagnosed with diabetes, he says.
Diabetes cases will continue to trend upward, particularly as demographic trends change here in the United States—both in terms of ethnicity and as our population ages, says Snow. He notes that the obesity epidemic is also a signifi cant risk factor in the growth of diabetes over the last few decades. Th e incidence of diabetes in-creases in people who earn less money and have less education, he says.
One of Aetna’s traditional programs for re-ducing the cost of diabetes care includes lim-iting drugs in its formulary—as other payers have done. “Th at was limited, though, in terms of treating diabetes and controlling costs,” says Snow. “Th at’s because the greatest expense in treating diabetes doesn’t come from the short-term costs of treating diabetes; rather, it’s the long-term burden of caring for people suff er-ing from the complications associated with the disease.”
Aetna’s focus on preventing those long-term
complications has led it to invest in member case management. Th e payer uses data analy-sis to determine appropriate members to in-clude in the program, in addition to including patients who self-select or are referred by clini-cians. Th e goal is to improve medication adher-ence and ensure that members are getting the appropriate therapies.
“We make sure that members are having their A1c levels checked and having their an-nual eye exams, because the number one cause of preventative blindness is diabetes,” Snow says. “We also want to make sure that folks are screened for kidney disease, since diabetes is a signifi cant cause for renal failure, which is a very expensive condition to treat.”
Patients’ engagement with the case manage-ment team typically begins with a phone call from a case manager, says Snow. Often, that call is precipitated by an emergency room visit associated with the patient’s diabetes. Th e case manager—generally, a nurse hired specifi cally for this role—will talk to the patient about ser-vices that can help them manage their disease. Th ese phone conversations focus on problems with patients’ medications, such as medication adherence and adverse drug reactions. Patients who are identifi ed as less acute may receive an
EXECUTIVE V IEW
Healthcare executives can help rein in diabetes costs by:
❚ Expanding diabetes management programs
❚ Exploring how telemedicine can improve access
❚ Addressing environmental factors that affect engagement
Source: Trust for America’s Health and Robert Wood Johnson Foundation
TX LA
MS AL GA
SC
NC
VA
FL
OR
NV
CA
NH
VT
AK
OHPA
MI
IL
KYWV
NY
WA
MT
ID
UT
WYSD
NE
KS MO
OKAZ NM
CO
NDMN
WI
IA
ARTN
IN NJ
DE
MD
DC
HI
MA
ME
RI
CT
4 - 7.9 % 8 - 11.9 % 12 - 15.9 %PERCENT OF ADULTS WITH DIABETES
Diabetes rate by state, 2014
MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com10
outreach letter, he says. “Th at’s because diabe-tes is so common that we can’t communicate directly with every person. We need to identify those who are at higher risk and intervene.”
Snow is particularly excited about a pilot program he’s working on with a device manu-
facturer and pharmaceutical company. Th e goal is to reduce the cost of care, while achiev-ing high-quality outcomes for patients. In this partnership, the device manufacturer and the pharmaceutical company will derive part of their pay-ment from members’ success with their solutions. Th e two
companies are very willing to participate in the project, says Snow.
While he can’t mention the names of the com-panies involved in the pilot, Snow says the device maker provides glucose readers for members who should be checking their blood sugars. He points out that these aren’t the most high-tech, high-end devices, but they have been shown to be eff ective. “We want to make sure they have ac-cess to glucose meters and strips and that they can test at the appropriate times,” says Snow.
Aetna’s plan is to roll out this pilot project to members in the second quarter of 2016, and the long-term goal is to run the program for fi ve years to “truly assess how members do,” says Snow. What he’ll be looking for is evidence of fewer heart attacks and strokes. In terms of scope, the payer plans to enroll 5,000 members in the pilot within a year,
“We’re looking at provider groups who work closely with us in our [accountable care orga-nizations] ACOs,” he says. “We actually want a very diverse population involved in the pilot. Th e longer term goal is to determine if the pro-gram is scalable to other practices.”
With this project, Aetna is really looking to see if it can “move the needle in terms of out-comes and cost,” says Snow. Th at includes pay-ing attention to patients’ A1c levels and making sure that the program has an impact on pa-tients’ lives. “It’s not just about reducing costs,” he says. “It’s about giving patients what we be-lieve they need, and we believe that will trans-late into improved outcomes down the road.”
EXPANDED REACH VIA TELEMEDICINEHussain Mahmud, MD, an endocrinologist at University of Pittsburgh Medical Center (UPMC), agrees that the most important costs
Maximize diabetes dollars
Diabetes costs the U.S. around
in medical costs and lost productivity
each year.
245$ BILLIO
N
DOUBLEDDiabetes rates have nearly
In the past 20 years.
29 MILL
ION
MO
RE
TH
AN
American adults
have diabetes
and another
have prediabetes.
86 MILL
ION
WEST VIRGINIA HAS THE HIGHEST RATE OF DIABETES AT
14.1%
The CDC projects
that one-in-three
adults could have
diabetes by 2050.
Sources: ADA, CDC
NINE OF THE 10 STATESWITH THE HIGHEST
TYPE 2 DIABETES RATES ARE IN THE SOUTH.
DIABETES IS THE SEVENTH LEADING CAUSE OF DEATH IN THE UNITED STATES.
SNOW
DIABETES AT A GLANCE

ManagedHealthcareExecutive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 11
associated with diabetes are the long-term com-plications of not managing it—and that’s exact-ly what UPMC wants to address with its diabe-tes patients. While Mahmud notes that the cost of insulin has doubled over the last few years, he agrees with Snow that roughly half the cost of diabetes is associated with complications.
UPMC’s approach is to get a better diagno-sis up front, which should translate into better control of symptoms for patients, he says. One of the key drivers of improved care for diabetes patients is making patients’ A1c levels a quality control measure, and linking that measure to provider incentives, says Mahmud.
Primary care physicians are on the front lines in diabetes treatment, he says, adding that challenges associated with treating diabetes are particularly acute for physicians in rural areas where there isn’t as much access to spe-cialty care. “Physicians are crammed for time and typically only have 15 or 20 minutes where they’re troubleshooting seven different things during an appointment,” he says. “Pittsburgh is the biggest city. For some parts of Pennsylvania, there’s no other big city within 150 or 200 miles; and there’s also a shortage of endocrinologists to serve patients in these rural areas.”
To address this care shortage, UPMC uses telemedicine to expand the reach of endocri-nologists to rural parts of the state. A 2012 study of the program published in the Journal of Medi-
cal Internet Research included 25 rural patients whose glycemic control had been unsuccessful under their primary care physicians’ care. These patients were then re-ferred to an endocrinologist at UPMC in Pittsburgh, who provided care via teleconsult. Diabetes nurses were on-site with the patients and facili-
tated the 45-minute consult while taking the patients’ vitals.
The teleconsults included medical inter-views and reviews of the patients’ laboratory data, in addition to treatment recommenda-tions provided by the endocrinologists. After the appointment, the treatment plans—which could include medication adjustments, lifestyle modifications, self-monitoring, and laboratory tests—were then shared with the patients’ pri-mary care physicians.
A1c levels after the teleconsults were avail-able for 16 of the 25 patients. After the telecon-sults, the proportion of patients with A1c lev-
els higher than or equal to 8% decreased from 88% to 50%. Seventy-five percent of patients achieved a decrease in A1c levels of at least .5%, according to the study.
While there’s a cost associated with build-ing the infrastructure behind the teleconsults, it is less expensive than trying to recruit endo-crinologists to rural communities, according to researchers. They further concluded that con-tinued success of the program would be con-tingent on determining appropriate reimburse-ment for physicians providing the teleconsults.
TELEPHONIC CARE COORDINATION Montefiore Medical Center is located in the Bronx, New York City, where 14% of the popu-lation has diabetes, according to the New York City Department of Health and Mental Hygiene. One way the center is addressing the diabetes challenge is through an extensive care coordi-nation program.
Vanessa Pratomo, MD, medical director for ACO quality improvement and chronic illness management at Montefiore, says dia-betic patients are introduced to Montefiore’s
Maximize diabetes dollars
MAHMUD
As technology evolves and data analytics capabilities
improve, payers and providers have an opportunity to share
data that help keep diabetes patients healthier and saves
money, says David Williams, cofounder of Health Business
Group and MedPharma Partners in Cambridge, Massa-
chusetts. Those useful data now include information that’s
generated outside of the healthcare systems, such as
glucose readings from wearable devices.
The challenge that lies ahead for payers and providers is
to figure out how to integrate these clinical and claims data
in a way that helps reduce the cost of care while providing
high-quality outcomes for patients, says Williams. “There
are some illnesses that have very expensive biologic drugs
that cost thousands of dollars a year. Diabetes isn’t like
that…the issue here is whether people are taking their
medications.”
DATA IMPROVE DIABETES MANAGEMENT

MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com12
Maximize diabetes dollars
telephonic care coordination program through a very extensive baseline interview that can take a few hours. During this interview, a care coordinator captures details about the medical background and any social, environmental, and mental health issues that may be impacting the patient’s ability to manage their diabetes. Care coordinators typically have a degree in nursing, social work, or pharmacy, according to a Mon-
tefiore spokesperson.Understanding these as-
pects of patients’ lives helps care coordinators figure out what could help patients bet-ter manage their disease, says Pratomo. If patients are at risk of losing their homes or they don’t have a way to get to their
appointments and require special accommoda-tions, the care coordination team can help deter-mine solutions to those problems with various social services agencies, she says. Homelessness, for example, is a huge barrier to patients’ ability to care for themselves. Care coordinators can help these patients by contacting the local housing agency to find suitable accommodations where patients can manage their illness, says Pratomo.
The goal is to help patients manage their dia-betes during the early stage of their disease to prevent the end-stage complications that entail the highest cost. If patients are having an acute issue, the care coordinator can connect them with the medical resources they need, she says. Absent an acute issue, patients typically receive a phone call from their care coordinator every month or every other month.
While Montefiore doesn’t have specific data that demonstrate the investment in telephonic care coordination led to specific outcomes with its diabetic patients, the Montefiore Pioneer ACO has saved Medicare $61 million since the start of the program, according to a spokesper-son. During a time when the health system’s in-patient admission rates went down by 10.4%, in-patient readmissions for diabetes patients went down by 45.7%, she said.
LONG-TERM INVESTMENTS California-based CareMore Health System (a subsidiary of Anthem), launched a prediabetes program in June 2015. Members are considered for participation in the prediabetes program if they have a body mass index considered to be obese, and have physical inactivity, a family his-tory of diabetes, and A1c levels in the prediabet-ic range. In addition to group support, members have access to monthly scheduled classes with a registered dietician, structured exercise pro-grams, and visits with either a nurse practitio-ner or a physician assistant where labs and vital signs are taken and discussed.
Out of CareMore’s 100,000 members, 2,000 patients were identified for participation in the program, which is now based in California and Arizona. While there’s not much data available about the program at the moment, CareMore is hearing from patients that their A1c levels are returning to the normal range, some within just three months of their involvement with the pro-gram, says Sachin Jain, MD, chief medical offi-cer at CareMore Health System.
“CareMore believes that every hospitaliza-tion is a failure of our system,” says Jain. “It costs on average $3,000 a day for a patient to be in a hospital. It costs only $500 over six months to administer a diabetes prevention program to patients. When you think about those econom-ics, there is a natural business case for investing in prevention. If I can avoid just one hospitaliza-tion, I’ve paid for delivering a diabetes preven-tion program to six patients. That’s dramatic.”
Payers hoping to better manage diabetes costs need to take a much longer term view of patients and their relationship with patients, says Jain. “It costs us a lot more to bring on a new member than it costs to retain a member … I think our members are with us an average of nine years. There’s an opportunity for us to both improve their health and lower the total cost of care. For managed care executives, those are magic words these days.”
Aine Cryts is a writer based in Boston.
“It costs on average $3,000 a day for a patient to be in a hospital. It costs only $500 over six months to administer a diabetes prevention program to patients.”—SACHIN JAIN, MD, CAREMORE HEALTH SYSTEM
PRATOMO
ManagedHealthcareExecutive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 19
Managed Care Outlookthoughts from EDMUND J. PEZALLA, MD, MPH
n immediate issue, and one of
tremendous importance, is the under diagnosis of diabe-
tes. A recent estimate from the National Diabetes Statis-
tics Report puts the number of undiagnosed diabetics in
the U.S. at 8.7 million.
People who are unaware they have diabetes are at risk
for progression to serious complications of high blood
sugar such as cardiovascular and renal disease. Th ere are
few publications on the causes of under diagnosis. How-
ever, we can postulate that they fall into three general
groupings:
1 Lack of access to care;
2 Failure to obtain screening for diabetes;
3 Inaction on the part of patients who screen positive but do not
follow up, or do not understand that they have diabetes.
Access to care, as measured by those with insurance
coverage, has clearly improved with the implementation
of insurance exchanges and the Medicaid Expansion un-
der the Aff ordable Care Act. However, it is not yet clear
how many people are actually seeing primary care and
other physicians for check ups and screenings.
Failure to obtain screening is directly related to access
to care, but also to what happens during encounters with
the healthcare system. If a patient’s encounters primarily
consist of emergency or acute care visits, that patient will
not likely receive screening for diabetes, breast cancer,
colon cancer or a range of other conditions. Even within
the context of a primary care visit it is unclear how many
Americans receive appropriate screening.
In a positive step, the U.S. Preventive Services Task
Force has included screening for overweight/obese adults
ages 40 to 70 years. However, the impact of this screening
recommendation on the number of undiagnosed persons
is currently unknown.
It is also possible that some patients who screen posi-
tive do not follow up on the screening. Th is may be be-
cause of a misunderstanding of what the results mean, or
fear of what comes next. In any case, this is clearly a fail-
ure of our healthcare system and of our eff orts to improve
health literacy in the U.S.
Th ere are positive steps that we can take to reduce the
number of undiagnosed people:
❚ Encourage preventive service visits with healthcare providers.
Most people with health insurance can receive screenings and
other preventive services covered at fi rst dollar with no or low
copays.
❚ Promote the use of screening tests, especially in those at risk for
developing type 2 diabetes (overweight or obese adults over
age 45 years, those who do not regularly exercise three times
per week, or women who have had gestational diabetes).
❚ Increase awareness of the serious problems caused by diabetes
and encourage the deployment of the CDC programs on the
detection and treatment of pre-diabetes.
In conclusion, we need to take a patient-centric view of di-
abetes prevention and treatment that includes increased
opportunities for screening and an increased focus on pre-
vention via diet and exercise.
ABOUT THE AUTHOR ❚
Edmund J. Pezalla, MD, MPH, is vice president and
national medical director for pharmaceutical policy and
strategy, Aetna.
Consequences range from cardiovascular disease to renal disease
Undiagnosed diabetes: A high cost for the health system
A

ManagedHealthcareExecutive.com20 MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016
TRANSFORMING CARE THROUGH HEALTH IT
Technology
lectronic health records (EHRs) were supposed to make healthcare easier and more efficient. But
healthcare executives are realizing that many systems
are not running as efficiently as expected, and that some staff members believe that the tech-nology has made their jobs more difficult.
Only 34% of physicians report being satisfied or very satisfied with their EHRs, 54% say their EHR system has increased their total operating costs, and 43% say they have yet to overcome productivity challenges related to their EHR system, according to a survey of nearly 1,000 physicians by the American Medical Association and AmericanEHR Partners released in August 2015.
Many physicians, staff mem-bers, executives, and lawmak-ers believe that in order for the information highway to run more smoothly between healthcare systems, EHRs must be revamped in the future.
“I think that all EHRs today sort of suck, at least from a pro-vider point of view,” says Ed Park,
executive vice president and chief operating officer of athenahealth.
“Part of the issue here is that EHRs have multiple masters—more than half of EHR functionality is there to support the lawyers and insurance com-
panies, not the providers of care. In order to get to a perfect EHR system, we’d have to change the requirements for the amount of documentation required so there’s more signal and less noise.”
When asked, “What makes the perfect EHR system and how long until it exists?” experts say that the mix between government regula-tions, interoperability and costs must be retooled, and it’s hard to predict when that will be.
“Unfortunately, the phrase ‘electronic health record’ has been so tainted, I doubt physicians will ever love EHRs,” says Charles Web-ster, MD, MSIE, MSIS, a medical informatics marketing/work flow technology expert, and president of EHR Workflow, Inc. “Over time, alternatives to EHRs will appear
and gain adherents in the medical community. These will be work flow-based systems, laid down atop current database systems, increasingly relegating EHRs to commoditized plumbing.”
Meaningful useMeaningful use, which has pro-pelled many physicians to imple-ment EHRs, isn’t going away, yet. In January, the Centers for Medicare and Medicaid Services (CMS) Acting Administrator Andy Slavitt said that meaningful use would be “effectively over” in 2016 and “replaced with something better.” Slavitt has since dialed back his definitive comments, writing on the CMS blog that EHR incentive programs will be more focused on care and rewarding providers on outcomes in the future.
A common sentiment among the healthcare IT community is that meaningful use has stunted the EHR progression. “In the words of more than one hospital CIO I’ve spoken with, meaningful use ‘sucked the air out of the room,’” Webster says. “Between meaning-ful use, ICD-10, and other govern-ment mandates, there were no resources left over to address other needs or to think creatively and experiment.”
Patricia Wise, RN, MS, MA, FHIMSS, vice president of health
information systems for the Healthcare Infor-mation and Man-agement Systems Society, says that the shifting mindset that EHR technology
is ruled by regulation and data collection, when it should inform work flow and improve outcomes,
Are EHRs delivering on expectations?
E
Concerns among stakeholders may call
for revamping by DONNA MARBURY
PARK
WISE

ManagedHealthcareExecutive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 21
Technology
will be significant. “Before the goal was to keep software in line with regulatory demands,” Wise says. “Clients’ needs and requests didn’t receive priority. The significant amount of regulations has been a challenge.”
InteroperabilityPark says communication between providers is the most essential part of EHR technology, a part that he admits the industry has lost sight of.
“The majority of patients no longer get seen at one institution—they go to urgent care clinics, specialists, or primary care physi-cians unaffiliated with hospitals. And every provider is looking at the world through a toilet paper tube, getting only a fine slice view of the patient,” Park says. “What we need to solve for now is opening up providers’ lens to view the whole patient while not overwhelming them with unnecessary informa-tion and wreaking havoc with their work flow.”
Webster says that the next five years will build on the kind of interoperability that actually gets work done. “Most health-care interoperability to date has focused on syntactic and semantic interoperability. Syntax is message structure. Semantics is message meaning. You need both to move data between systems and have it mean the same thing in both systems,” Webster says. “What’s
been missing from healthcare interoperability has been what is called task, work flow, or pragmatic in-teroperability. To understand prag-
matic interoperability you need to understand syntactic and semantic interoperability.”
Wise says that the Office of the National Coordinator for Health
Information Technology hopes to incentivize EHR vendors who are extending their platforms to include application program interfaces (APIs). This will help consolidate the industry and give providers a way to better custom-ize their systems, she says.
An API is a set of programming instructions and standards that software companies can release so that other software applications can be built to interface with each other using the web.
Long-term outlookWith all of the EHR challenges and complaints associated with them, many healthcare executives fear that they will have to make dramatic and costly overhauls to their current systems. Park says, however, that trends in technol-ogy bend toward rental content and adaptations to pre-existing systems with lower costs.
“By way of example, in Silicon
Valley new startups today don’t make ‘big iron’ technology purchases of servers to run their businesses,” Park says. “Similarly in the consumer world, the trend is away from purchasing CDs and DVDs, but instead renting content from companies like Spotify and Netflix. We think that the same thing should happen in health-care, where organizations are less reliant on traditional vendors that require big upfront costs and disruptive replacements.”
Wise agrees, adding that once APIs are used more routinely, the costs of technology should drop, but so should other operational costs.
“When we have true interop-erability, not only should we see lower technology costs, but gains in shared information and care co-ordination should cut costs also,” Wise says.
Donna Marbury is a writer in Columbus, Ohio.
Post-EHR Productivity DropFor the past several years, Managed Healthcare Executive’s sister publication, Physicians Practice journal, has asked its readers to identify their “most pressing information technology problem.”
In 2012, 2013, and 2014, the most common response among survey takers was “EHR adoption and implementation.” In 2015, for the first time, “a drop in productivity due to our EHR,” and a “lack of interoperability between EHRs,” received the highest percentages of responses.
Other key EHR related survey findings from the 2015 survey include:
of respondents said EHR use has improved documentation.
of respondents said EHR use has led to a return on investment.
of respondents said EHR use had caused them to see fewer patients per day.
67% 32% 37%WEBSTER

MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com22
BEST PRACTICES FOR OPTIMAL OUTCOMES
Health Management
iabetes is a silent disease—most of these patients feel fine, even if their sugar levels are dangerously high. Because
they don’t feel ill, many dia-betic patients aren’t motivated
to change their lifestyles or follow prescribed medical treatment.
In fact, as few as 60% of patients with type 2 diabetes take prescribed medications, according to a study in the American Journal of Managed
Care. Another study, in Diabetes
Therapy, showed that less than 50% of diabetic patients achieve recom-mended glycemic goals.
Furthermore, direct risk reduc-tion for diabetes-related kidney disease, stroke, heart disease, and amputation were estimated for 100% compliance with diabetes treatment, as reported in a study in Innovations in Pharmacy. Risk, case, and yearly cost reduction calculated for 100% compliance with diabetes treatment were 13.6%, 0.9 million, and $9.3 billion, respectively.
Given this, it’s obvious that adhering to treatment protocols can significantly benefit diabetes patients. So how can providers—who are ultimately responsible for motivating patients to improve compliance—achieve the goal of
better compliance among these patients? Here, experts offer solu-tions for some common noncom-pliance issues.
1Failure to adhere to treatment
recommendationsFirst and foremost, patients need to understand the long-term implications of not taking care of their diabetes. “Educating patients and their families about what diabetes does to the body, and how medication counters those effects,
is critical to inciting behavior change,” says Diana O’Keefe, RN, CDTC, CDE, clinical coordi-nator, Diabetes and Endocrine Institute, Morris-
town Medical Center, Morristown, New Jersey.
Serge Jabbour, MD, FACP, FACE, professor of medicine and director, Division of Endocrinology, Diabe-tes & Metabolic Diseases, Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, believes discussing American Dia-betes Association (ADA) guidelines in regard to HbA1c, lipids, and so
forth with patients, is important. “When patients learn that a nation-al association recommends specific goals to achieve based on major studies, their compliance improves, especially when they hear that achieving target goals would lower complications regarding kidney disease, eye disease, nerve disease, heart attack, and stroke,” he says. In addition, providers can improve patient compliance by setting re-alistic goals and expectations. For example, when discussing weight loss, patients should be reminded that results are expected over months rather than days or weeks.
A focus on the individual pa-tient is also imperative. “Providers need to understand who their pa-tients are and the factors that may influence their compliance,” says Deena Adimoolam, MD, assistant professor of medicine, Endocrinol-ogy, Diabetes, and Bone Disease, at the Icahn School of Medicine at Mount Sinai, New York, New York. “These might include socio-economic limitations, educational background, cultural differences, and language barriers.” Treatment plans and goals should be tailored to patients based on their unique
circumstances including their age, underlying medical condi-tions, and risk for hypoglycemia.
Kristi Hender-son, DNP, NP-BC, FAEN, chief tele-
health and innovation officer, Uni-versity of Mississippi Medical Cen-ter, Jackson, Mississippi, stresses the importance of using technology to interact with patients daily to encourage adherence to treatment plans. “Health coaches and nurses can provide education, motivation,
D
ADIMOOLAM
O’KEEFE
Five reasons diabetic patients don’t adhere… and solutions from experts by KAREN APPOLD
Health Management
Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 23
and tools to empower patients to manage their health through text messaging, video chats, and elec-tronic health sessions delivered on the phone, tablets, or computers, so it is convenient and easy to access,” she says.
2Failure to comply with medication
guidelinesPoor health literacy is a major bar-rier to medication adherence, Adi-moolam maintains. Health literacy is a patient’s ability to accurately comprehend medical information, and can be limited due to one’s level of education or inability to understand a non-native language.
Adimoolam assesses a patient’s
health literacy with a simple survey. Then, she tailors patients’ treatment plans and clinic visits accordingly (e.g., would a patient benefit from more frequent follow-up visits or the help of a diabetes educator?).
Open communication is key when patients aren’t taking medications as recommended, says Adimoolam. Ask the patient directly why his or her control is suboptimal, she says. “Some barriers to medication adherence may include inability to pay for medications, lack of understand-ing on how to take them, and social stressors.”
Alan M. Delamater, PhD, profes-sor of pediatrics and psychology
and the director of clinical psychol-ogy, Department of Pediatrics, University of Miami Miller School of Medicine, Miami, Florida, says research shows that patients who have good relationships with their doctors better adhere to therapy
regimens. “Physi-cians should use active listen-ing techniques and work with patients on goal setting,” he says.
Providers can underestimate
the important role education takes in medication adherence. At the Diabetes and Endocrine Institute, each patient is educated about
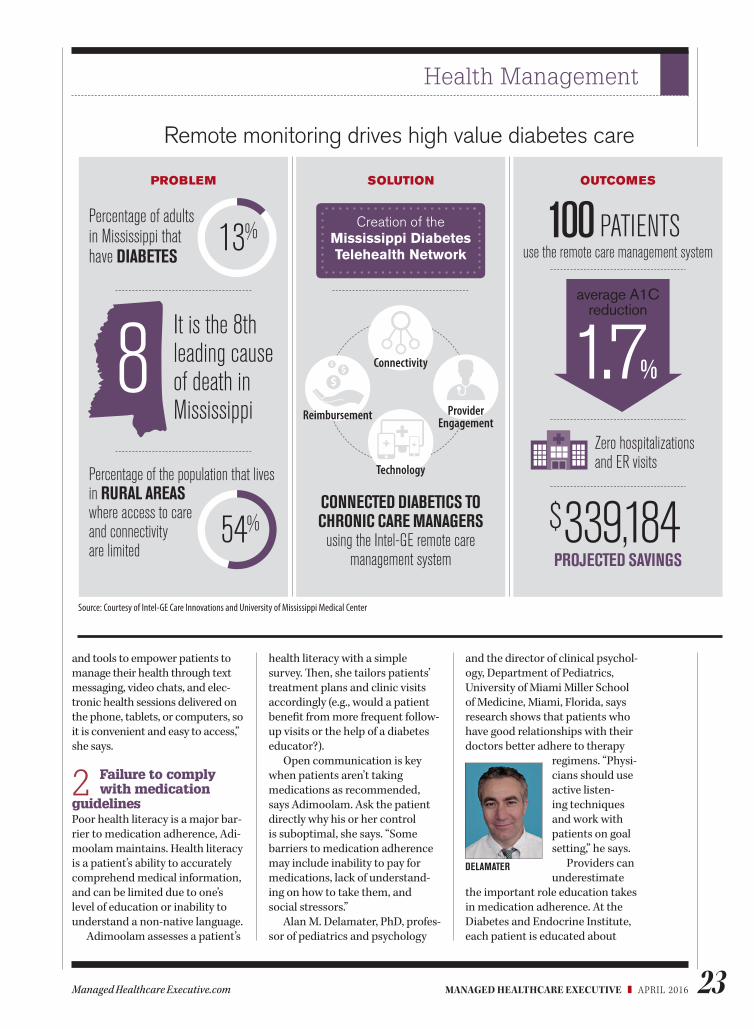
Remote monitoring drives high value diabetes care
Percentage of the population that lives in RURAL AREAS where access to care and connectivity are limited
Percentage of adults in Mississippi that have DIABETES
CONNECTED DIABETICS TO CHRONIC CARE MANAGERS
using the Intel-GE remote care management system
Technology
Connectivity
Reimbursement Provider Engagement
OUTCOMES
$339,184PROJECTED SAVINGS
use the remote care management system100 PATIENTS
Source: Courtesy of Intel-GE Care Innovations and University of Mississippi Medical Center
It is the 8th leading cause of death in Mississippi
8
PROBLEM SOLUTION
Creation of the Mississippi Diabetes Telehealth Network
Zero hospitalizations and ER visits
average A1C reduction
1.7%
DELAMATER
13%
54%

MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com24
Health Management
each medication’s mechanism of action in layman’s terms. “If patients understand the basics of why their doctor prescribed their medication, they’re more apt to take it as prescribed,” O’Keefe says.
The same technology that helps patient adhere to their treatment
plans can also be employed to send reminders and alerts to support medica-tion adherence. “Our technology has daily health questions that
the patient answers telling us why he or she isn’t taking a medica-tion (e.g., ran out of it, needs a new prescription, has bad side effects), so we can intervene appropriately,” says Henderson, who has seen compliance rates as high as 96% using the technology.
3Failure to commit to lifestyle changes
Adherence rates for diet and exercise are even worse than for taking medications, with studies reporting less than 65% and less than 20% respectively. “It’s easy to just take a pill, but changing your diet and exercising are much more obtrusive,” Delamater says.
Again, communication is the key to convincing patients to make lifestyle changes. “Providers should ask patients what types of exercise they enjoy,” Adimoolam says. “If patients are unable to engage in physical activity, find out why and uncover these barriers. Some patients may have significant pain limiting their ability to exercise. These patients should have their pain evaluated and treated to allow for improved mobility and exercise. If they have chronic pain that is difficult to control, providers should look for alterna-tive forms of exercise that may be
associated with less pain, such as aqua aerobics.”
Regarding diet, providers need to be realistic with expectations, and suggest patients eat less of certain bad foods rather than eliminate them completely. “Allow the patient to take time to make changes. Slow change is better than no change,” Adimoolam says.
Jabbour advises referring patients to a dietitian or diabetes educator. “By attending diabetes education classes, patients will better understand the importance
of diet and exercise in the management of their diabe-tes and overall health,” he says.
Group classes can be incredibly motivating be-
cause everyone in attendance talks about the same issues and has the same challenges, O’Keefe says. It’s motivating for people to be with others who are also managing their disease.
4Failure to self-monitor
Adimoolam educates patients on the importance of self-monitoring of blood glucose to help them understand and control diabetes in order to prevent complica-tions from the disease. She also educates them on the importance of self-monitoring blood glucose to identify emergency situations such as experiencing hypoglycemia, which can be fatal.
The ADA recommends that type 1 diabetics on multiple-dose insulin or insulin pump therapy monitor blood glucose at least before meals and snacks, occasion-ally postprandially, at bedtime, prior to exercise, after treating low blood glucose (until glucoses are normal), and prior to certain tasks
such as driving. Not all type 2 dia-betics require frequent self-moni-toring; the frequency depends on the severity of the diabetes and treatment goals.
Adimoolam empowers patients to believe that by understanding their fingerstick readings they will be able to gauge how their body will respond to certain foods, situations (such as exercise or stress), and hypoglycemia. “When a patient understands their body, he or she can better predict what to expect in different scenarios,” she says.
5Failure to attend regular check ups
Adimoolam explains to patients the reasons for needing to have regular visits. “The goal is to optimize their diabetes treatment in order to prevent complications,” she says. “The frequency of their appointments will be higher when their condition is poorly con-trolled. Once they are stable, we can decrease the frequency. That way, there is an end in sight.”
O’Keefe believes that check ups should offer multiple benefits. “We schedule visits to ensure that each patient is also able to meet with a diabetes educator, so they can get a better understanding of a medi-cation or discharge instructions. By providing this added education-al benefit, patients want to come back to learn more,” she says.
Diabetes is a complex disease. The key to compliance is education and open communication. “Provid-ers need to listen to their patients to understand their struggles in not achieving optimal diabetes control,” Adimoolam says. “When they listen with an open mind, they can identify key issues that need to be addressed first. Medications aren’t always the answer.”
Karen Appold is a medical writer in Lehigh Valley, Pennsylvania.
HENDERSON
JABBOUR

MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com28
CLIN ICAL CONSIDERATIONS WITH SYSTEMWIDE IMPACT
Hospitals & Providers
hysicians want to do what they went into medicine to do: Take care of patients through building and fos-
tering strong relationships with them. In the fee-for-
service world, however, many independent physicians believe that calling cannot be realized. That’s because in order to stay in business, they need to see as many patients as they can during the day—and that translates into seeing each patient for only about 10 or 15 min-utes, says Jeff Butler, chairman and chief executive officer of Arlington, Virginia-based Privia Health, a national medical group.
Value-based reimbursement, he says, can change that. “The op-portunity for these providers is to come alongside and be the strate-gic partners of health plans … and
really get aligned on managing a population and getting rewarded, not for doing more stuff, not for seeing more patients, but getting rewarded
for keeping people healthy and keeping them out of the acute care setting,” says Butler.
While value-based reimburse-ment presents opportunities for payers and providers, succeeding in such a reimbursement model can be challenging. Here are four things to strive for that could
increase the likelihood of success in a new payment model.
1/ Stronger partnershipsTo take advantage of value-based care payment models, such as accountable care organizations, independent physicians must align with other providers.
That alignment requires adapt-ing to common technology, com-mon platforms, common work flow, and common systems, says Butler. “They don’t have to be geographi-cally located next to each other. But they need to be on a common platform that allows them to get the efficiencies and [economies] of scale, and to benefit from the technology and the people and the expertise that are needed in order to be able to take on risk.”
For larger healthcare systems and managed care organizations that are onboarding new physi-cians, that means a critical aspect of alignment is providing physi-cians with the resources necessary to adjust to the broader organiza-tion’s technology platforms.
When onboarding new prac-tices, Privia Health, for example, introduces physicians to popula-tion health and risk management systems that enable them to focus on providing patient care, says Butler. After about four to five months using these systems, physicians can spend an hour with patients who have many com-plex co-morbidities—instead of
the typical 10 or 15 minutes they could spend in the fee-for-service model, says Butler. It makes sense to invest time in these patients, because it could prevent a costly ER visit later, he says.
Conversely, if patients need something minor addressed, such as a prescription refill, they can see a nurse or communicate with the practice via secure e-mail—instead of having to come in and take up an appointment slot with the physician, says Butler.
2/ Unlimited primary careTo succeed in value-based care, payers and providers have to provide as much primary-care as necessary to enrollees, says Linde Wilson, executive advisor for L.E.K. Consulting’s Healthcare Services Practice. “That way, primary care providers can capture issues early and they can prevent patients from going to specialist care. Providers can also use innovative models that include [advanced practitio-ners] and nurses,” she says.
Harken Health, an affiliate of UnitedHealthcare, has developed a model that provides unlimited primary care to all of its enrollees—with no copays, says Wilson. “The idea is that if you really want to manage care, you have to provide as much primary care as is necessary to enrollees so you can capture issues early—and you can prevent them from going to specialty care.”
In exchange for a monthly
Four characteristics of successful organizations by AINE CRYTS
Advancing collaborative care models
P
BUTLER
Hospitals & Providers
Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 29
membership fee, enrollees pay no copays for visits to Harken Health Centers in Illinois and Georgia, according to the company. Mem-bers receive 24/7 access to their doctor and can have questions or concerns addressed in an offi ce visit or by phone, e-mail, or video chat. Th ey also have access to a health coach and behavioral health specialists for short-term counsel-ing, assessments, and referrals.
Th is approach allows the prac-tice to be innovative and incorpo-rate nurse practitioners and physi-cian assistants, she says. “My belief is if they’re not always going to use physicians, and they’re going to have people practicing at the top of their licenses, [Harken Health] could really have something here that could help keep patients healthier.”
3/ Expanded servicesAnother model Wilson is particu-larly excited about is the Camden Coalition of Healthcare Providers in Camden, New Jersey. In this model, patients with frequent hos-pital admissions are identifi ed us-ing information from the Camden Health Information Exchange. Th e Camden Coalition’s staff members meet patients while they’re in the hospital and off er access to care-coordination services with a community-based team of nurses, social workers, community health workers, and health coaches for about 90 days, according to the organization. Th e organization’s staff also works with patients to navigate behavioral and social bar-riers to wellness. Th e belief is that access to primary care, transporta-tion, and housing can help prevent readmissions.
4/ Empowered physiciansMark Wagar is president of North-ridge, California-based Heritage Medical Systems, an affi liate of the Heritage Provider Network, which
is one of the country’s largest pio-neer accountable care organiza-tions. He says that for many years, physicians have lacked insight into the total cost and quality of care when their patients use a particu-lar healthcare delivery system for a surgical procedure, for example.
Heritage Provider Network is now combining claims informa-
tion with quality information and providing physicians access to that information. Th at way, a physi-cian can identify, for example, in which hospital a patient in need of a particular procedure will likely have a more positive outcome at a lower cost.
Aine Cryts is a writer based in Boston.
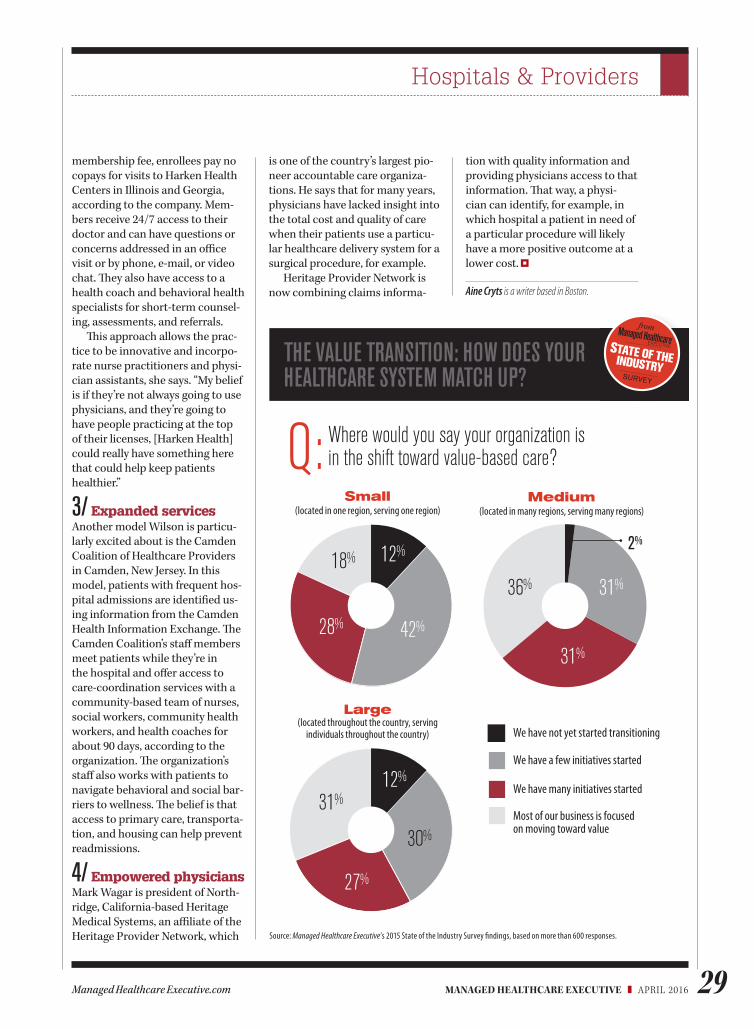
Source: Managed Healthcare Executive’s 2015 State of the Industry Survey fi ndings, based on more than 600 responses.
Where would you say your organization is in the shift toward value-based care?Q:
Small (located in one region, serving one region)
12%
42%28%
18%
Medium (located in many regions, serving many regions)
2%
31%
31%36%
INDUSTRY
STATE OF THE
from
SURVEY
THE VALUE TRANSITION: HOW DOES YOUR HEALTHCARE SYSTEM MATCH UP?
We have not yet started transitioning
We have a few initiatives started
We have many initiatives started
Most of our business is focused on moving toward value
Large (located throughout the country, serving
individuals throughout the country)
31%12%
30%
27%
MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com30
INDUSTRY EXPERTS WEIGH IN
Q&A
ccording to the “Eco-nomic Costs of Diabetes” study by the American Diabetes Association
(ADA), the total esti-mated cost of diagnosed
diabetes in the United States is $245 billion, including $176 bil-lion in direct medical costs and $69 billion in reduced productiv-ity. Individuals with diagnosed diabetes incur, on average, medi-cal expenditures of about $13,700 per year, of which about $7,900 is attributed to diabetes. These individuals also, on average, have medical expenditures approxi-mately 2.3 times higher than those without diabetes.
Given this, Managed
Healthcare Executive asked Andrew S. Rhinehart, MD, chief medical officer, Glytec, Greenville, South Carolina, and Jay LaBine, MD, chief medical officer, Priority Health, Grand Rapids, Michigan, how new treatments, technologies, and services might help reduce costs and improve the quality of care for diabetes patients.
Q: Managed Healthcare Executive (MHE):
How might emerging new treatments for diabetes improve
the quality of care while reducing costs?
Rhinehart: Scores of data show that improved glycemic control reduces the overall cost of care for people with diabetes. The cost of prescription medications and diabetes supplies accounts for merely 12% of the $245 billion spent annually. The majority of costs come from treating diabe-tes related hospitalizations, com-plications, and indirect costs (i.e., increased absenteeism and re-duced productivity while at work, reduced productivity for those not in the labor force, inability to work as a result of disease-relat-ed disability, and lost productive capacity due to early mortality). Preventing these complications, improving patients’ lives, and keeping individuals with diabetes healthier with the use of the new-est and best therapies should in turn lower costs.
Q: MHE: How can new technology impact costs
and quality for diabetic patients?
LaBine: Smart devices offer many benefits to individuals who are responsible for consistent self monitoring. Utilizing technol-ogy such as phone and computer apps that log blood sugar and foods consumed, smart pumps that give insulin as the body needs it, and text and e-mail reminders to test or take medi-cations will make it easier for diabetic patients to control and maintain their disease.
Rhinehart: By using today’s tech-nologies, large amounts of data can be collected. Moving forward, providers need to better capital-ize on this large data set by glean-ing actionable insights through the use of predictive analytics and decision-support software to as-sist with medication dosing.
Impact of emerging treatments, technologies by KAREN APPOLD
CALCULATING DIABETES COSTS
A
“Many payers finally are understanding that paying for medications and provider office visits is not enough for patients with diabetes.” —ANDREW S. RHINEHART, MD, GLYTEC

Q&A
Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 31
“Utilizing technology such as phone and computer apps that log blood sugar and foods consumed ... will make it easier for diabetic patients to control and maintain their disease.”—JAY LABINE, MD, PRIORITY HEALTH
Q: MHE: What services should health plans offer that will
help patients stick to treatment plans and adhere to lifestyle modifications?
Rhinehart: Many payers finally are understanding that paying for medications and provider office visits is not enough for patients with diabetes. To improve care, payers need to provide additional coverage for diabetes self-man-agement education and support through a recognized diabetes education center, such as the American Association of Diabetes Educators or the ADA. Without proper education and support, patients are less likely to manage their own care outside of the hos-pital. Organizing patient incentive programs that motivate them to comply with therapy is another method that payers can use to help patients better manage their disease. These can be financial incentives (e.g., no copays for medications and testing supplies in addition to lower or no office visit copays) or support incentives through disease management
provided either directly from the provider, payer, or from a third party, such as pharmacists provid-ing medication therapy manage-ment.
Q: MHE: What else should healthcare executives know
about diabetes care from a financial perspective?
Rhinehart: The most important thing to understand regarding diabetes is that early action is key. Although treatments, educa-tion, technologies, and support are expensive, study after study demonstrates that better glucose control improves outcomes and is cost effective. The cost of poor control increases logarithmically over time due to hospitaliza-tions, complications, the need for more medications to treat these complications, morbidity, disability, decreased produc-tivity, and the list goes on. It’s simple—diagnose early, educate, and treat aggressively to achieve proper glycemic control and reap the rewards.
LaBine: If can we can create programs that remove barriers, and align support at home and at work—we may be able to miti-gate the long-term costs associ-ated with diabetes.
Karen Appold is a medical writer in Lehigh Valley,
Pennsylvania.
For information on advancements in diabetes care go to bit.ly/diabetes-improvements
MORE INFO
Three steps to manage diabetes❚ Diagnose early
❚ Educate
❚ Treat aggressively to achieve proper glycemic control
MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com32
LEGISLATIVE / POLICY DEVELOPMENTS, TRENDS AND IMPACTS
Policy Outlook
rescription drug abuse is an epidemic across the U.S., with an average of 44 people dying every day
as a result of prescription opioid overdoses, accord-
ing to the Centers for Disease Control and Prevention (CDC).
Nearly 2 million Americans abuse or are dependent on opioids, and abuse of these drugs costs the U.S. almost $56 billion each year in lost productivity, healthcare costs, and criminal justice costs, according to the CDC.
Diversion is another major problem. Fifty five percent of peo-ple who abuse prescription medi-cations get them from friends or relatives, while only 17.3% abuse their own prescription, according to the CDC. The rest of abusers obtain medications by theft or illegal purchase.
There are many ways politi-cians and healthcare providers are working to combat these abuses, and the epidemic has even caught the attention of the White House, with President Barack Obama pledging $500 million in his 2017 budget to fight prescription drug abuse. A portion of those funds could go to helping states expand
their prescription drug monitor-ing programs (PDMPs).
PDMP overview PDMPs, which are already in use in some capacity in 49 states and are electronic databases used to track the prescribing and dispens-ing of controlled prescription drugs to patients, can be very ef-fective, especially when used with other interventions, says Heather Gray, legislative director of the National Alliance for Model State Drug Laws.
“Not only can these programs help identify potential doctor shoppers (individuals receiv-ing multiple prescriptions from multiple providers) they can also help healthcare providers iden-tify patients who may be at risk of developing a substance use disorder or even overdose,” Gray says. “It is difficult to quantify the impact that these programs have had on the prescription drug abuse problem, as oftentimes the enacting state legislation was passed as part of an overall revi-sion of prescription drug laws. However, no one doubts that they have an important role to play in the fight against prescription drug abuse.”
PDMPs are primarily used by physicians and pharmacists to ensure that their patients are not receiving duplicate prescrip-tions or showing any other signs of abuse, misuse, or diversion. If abuse is suspected, the hope is that the physician will refer the patient for treatment or further evaluation.
Many state guidelines strongly suggest that if a physician suspects a patient is abusing prescription drugs, the physician should refer the patient for evalu-ation and treatment.
PDMPs also help identify any potential drug interactions that could be harmful to a patient. For example, if a patient is receiv-ing benzodiazepines from one physician and opioids from another, the physician checking the PDMP will be alerted to that and may choose to reduce the dosage of opioids prescribed or might change to another pain reliever because of the high risk of overdose for patients taking both types of drugs.
An in-depth look at state initiatives
by RACHAEL ZIMLICH
Do prescription drug monitoring programs work?
P
Nearly 2 million Americans abuse or are dependent on opioids. Abuse of these drugs costs the U.S. almost $56 billion each year.—CDC

Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 33
Policy Outlook
PDMP effectiveness The success of a state’s PDMP depends on the particulars of the program, but states with strong participation requirements seem to have robust positive results.
Woody McMillin, of the Ten-nessee Department of Health, says the state’s Controlled Substance Monitoring Database Program (CSMD) became mandatory in 2013, and appears to be helping.
“We have seen positive changes, including a reduction in the morphine milligram equiva-lents dispensed, a reduction in the number of doctor and pharmacy shoppers going to multiple outlets to obtain drugs, an increase in queries to the CSMD by prescrib-ers and extenders, and a change in practices, with some 41.4% less likely to prescribe certain con-trolled substances,” McMillin says.
Research from various organi-zations also points to promising results. In Florida, deaths related to oxycodone overdose dropped 25% after Florida implemented its PDMP in late 2011, accord-ing to a team of University of Florida Health researchers. New York experienced a 75% decrease in prescriptions issued through “doctor shopping” as a result of a 2012 requirement that prescribers check the PDMP before writing a prescription, according to the PDMP Center of Excellence at Brandeis University. Also accord-ing to the PDMP Center of Excel-lence, 74% of California physicians reportedly changed their prescrib-ing practices as a result of patient activity reports created using the state’s PDMP.
PDMP opposition The only state that hasn’t adopted a PDMP is Missouri. Sen. Robert Schaaf is a long-time opponent of such a system.
“The people of Missouri do not want one,” Schaaf says. “There have been polls taken and I’ve had many people express concern about their right to privacy of their medical information. People don’t want their private medical information on a government database.”
Schaaf doesn’t believe that PDMPs have been shown to reduce deaths from opioids, only from diversion, and there were even mixed results on that front. He adds: “The problem is that in states that have passed and PDMP, the usage of heroin has been known to increase.”
In 2014, the CDC showed that overdose deaths related to opioid pain relievers quadrupled since 1999 and were at a historic high. The problem began, according to the CDC, in the 1990s when opioid pain relievers were increasingly prescribed to treat what was be-lieved to be a widespread problem of undertreated pain. As prescrip-tions for opioids climbed, so did overdose deaths.
Then, in recent years, heroin use began to climb as well, more than doubling from 2007 to 2012, according to the Substance Abuse and Mental Health Services Administration. Many healthcare providers attribute the rise in heroin addiction to opioid abuse, particularly when the prescription pipeline is shut off or becomes too costly.
“CDC’s analysis has found that more than three out of four people who reported both past-year opioid abuse and heroin use said they used opioids non-medical-ly—that is, without a prescription or for the feeling or experience the drugs cause prior to heroin initiation,” said Daniel Sosin, MD, MPH, FACP, acting director of the National Center for Injury Preven-
$72.5 BILLIONThe amount of money
nonmedical use of
prescription painkillers costs
health insurers annually.
500,000The number of emergency
department visits in 2009
due to people misusing
or abusing prescription
painkillers.
15,000The number of people who
died of overdoses involving
prescription painkillers in
2008.
1 IN 20The number of people in the
U.S. (ages 12 or older) who
reported using prescription
painkillers for nonmedical
reasons in 2010.
Source: CDC
High cost of prescription painkillers
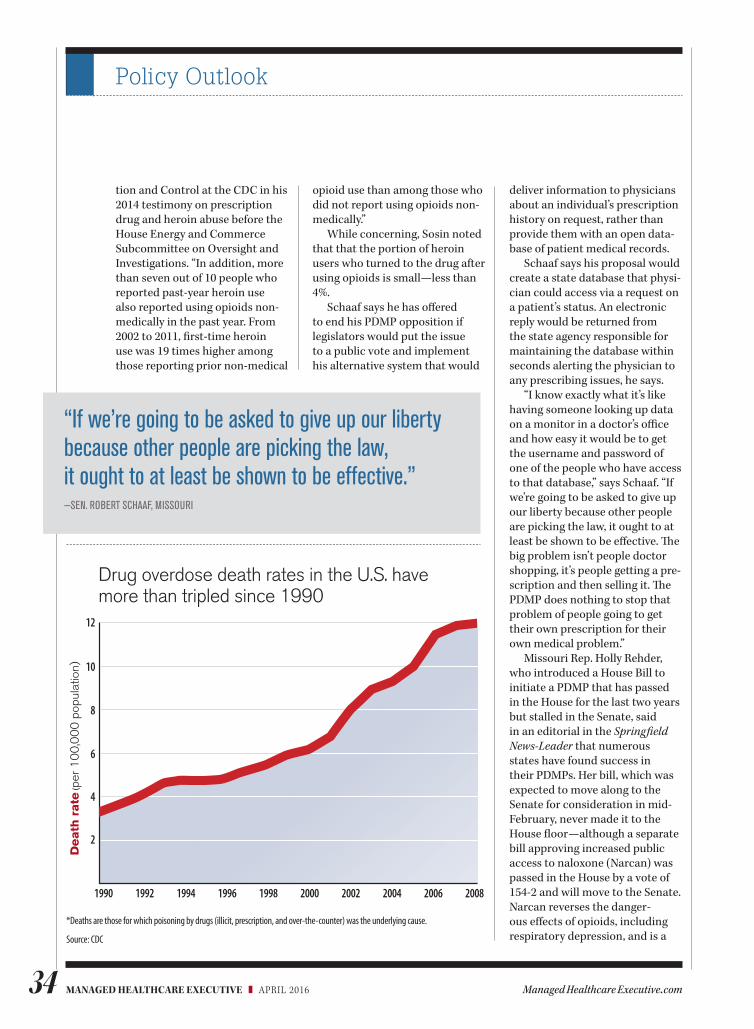
MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com34
Policy Outlook
tion and Control at the CDC in his 2014 testimony on prescription drug and heroin abuse before the House Energy and Commerce Subcommittee on Oversight and Investigations. “In addition, more than seven out of 10 people who reported past-year heroin use also reported using opioids non-medically in the past year. From 2002 to 2011, fi rst-time heroin use was 19 times higher among those reporting prior non-medical
opioid use than among those who did not report using opioids non-medically.”
While concerning, Sosin noted that that the portion of heroin users who turned to the drug after using opioids is small—less than 4%.
Schaaf says he has off ered to end his PDMP opposition if legislators would put the issue to a public vote and implement his alternative system that would
deliver information to physicians about an individual’s prescription history on request, rather than provide them with an open data-base of patient medical records.
Schaaf says his proposal would create a state database that physi-cian could access via a request on a patient’s status. An electronic reply would be returned from the state agency responsible for maintaining the database within seconds alerting the physician to any prescribing issues, he says.
“I know exactly what it’s like having someone looking up data on a monitor in a doctor’s offi ce and how easy it would be to get the username and password of one of the people who have access to that database,” says Schaaf. “If we’re going to be asked to give up our liberty because other people are picking the law, it ought to at least be shown to be eff ective. Th e big problem isn’t people doctor shopping, it’s people getting a pre-scription and then selling it. Th e PDMP does nothing to stop that problem of people going to get their own prescription for their own medical problem.”
Missouri Rep. Holly Rehder, who introduced a House Bill to initiate a PDMP that has passed in the House for the last two years but stalled in the Senate, said in an editorial in the Springfi eld
News-Leader that numerous states have found success in their PDMPs. Her bill, which was expected to move along to the Senate for consideration in mid-February, never made it to the House fl oor—although a separate bill approving increased public access to naloxone (Narcan) was passed in the House by a vote of 154-2 and will move to the Senate. Narcan reverses the danger-ous eff ects of opioids, including respiratory depression, and is a
“If we’re going to be asked to give up our liberty because other people are picking the law, it ought to at least be shown to be effective.” —SEN. ROBERT SCHAAF, MISSOURI
*Deaths are those for which poisoning by drugs (illicit, prescription, and over-the-counter) was the underlying cause.
Source: CDC
Drug overdose death rates in the U.S. have more than tripled since 1990
1990 200820062004200220001998199619941992
2
4
6
8
10
12
Death
rate
(per
10
0,0
00
pop
ulat
ion)
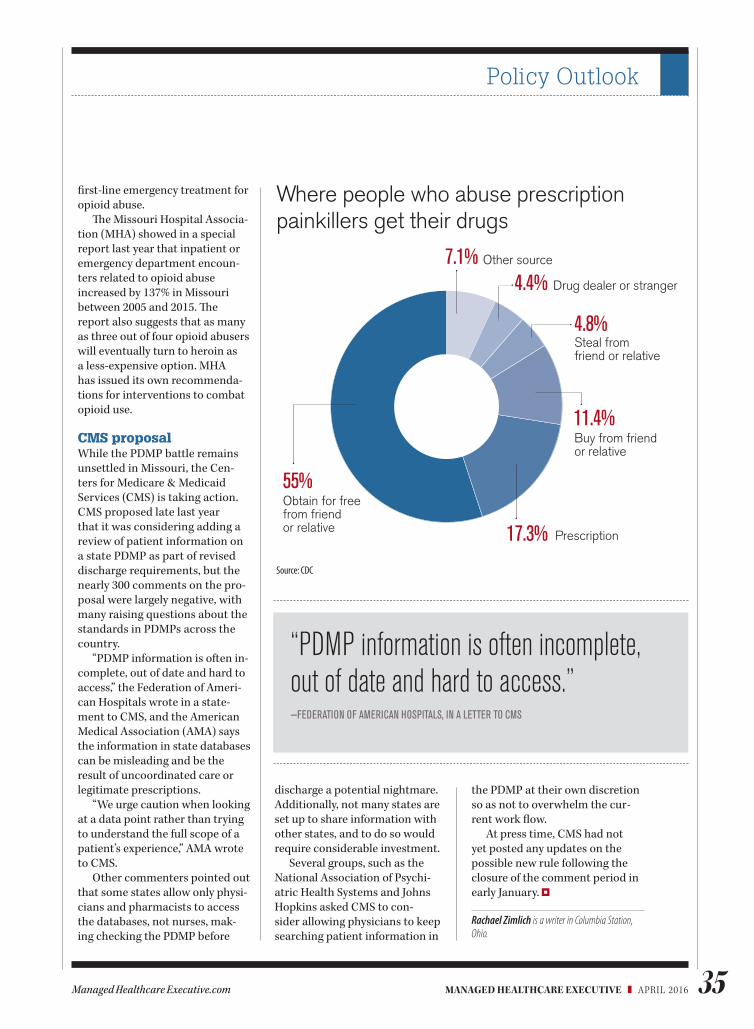
Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 35
Policy Outlook
first-line emergency treatment for opioid abuse.
The Missouri Hospital Associa-tion (MHA) showed in a special report last year that inpatient or emergency department encoun-ters related to opioid abuse increased by 137% in Missouri between 2005 and 2015. The report also suggests that as many as three out of four opioid abusers will eventually turn to heroin as a less-expensive option. MHA has issued its own recommenda-tions for interventions to combat opioid use.
CMS proposal While the PDMP battle remains unsettled in Missouri, the Cen-ters for Medicare & Medicaid Services (CMS) is taking action. CMS proposed late last year that it was considering adding a review of patient information on a state PDMP as part of revised discharge requirements, but the nearly 300 comments on the pro-posal were largely negative, with many raising questions about the standards in PDMPs across the country.
“PDMP information is often in-complete, out of date and hard to access,” the Federation of Ameri-can Hospitals wrote in a state-ment to CMS, and the American Medical Association (AMA) says the information in state databases can be misleading and be the result of uncoordinated care or legitimate prescriptions.
“We urge caution when looking at a data point rather than trying to understand the full scope of a patient’s experience,” AMA wrote to CMS.
Other commenters pointed out that some states allow only physi-cians and pharmacists to access the databases, not nurses, mak-ing checking the PDMP before
discharge a potential nightmare. Additionally, not many states are set up to share information with other states, and to do so would require considerable investment.
Several groups, such as the National Association of Psychi-atric Health Systems and Johns Hopkins asked CMS to con-sider allowing physicians to keep searching patient information in
the PDMP at their own discretion so as not to overwhelm the cur-rent work flow.
At press time, CMS had not yet posted any updates on the possible new rule following the closure of the comment period in early January.
Rachael Zimlich is a writer in Columbia Station, Ohio.
Where people who abuse prescription painkillers get their drugs
Source: CDC
“PDMP information is often incomplete, out of date and hard to access.” —FEDERATION OF AMERICAN HOSPITALS, IN A LETTER TO CMS
Other source
Drug dealer or stranger
Steal fromfriend or relative
Buy from friendor relative
Prescription
Obtain for free from friendor relative
7.1%4.4%
4.8%
11.4%
17.3%
55%
MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com36
Drugs In The Pipeline
iabetes is an epidemic that drives a great deal of costs associated with medica-tions and treatment. About
9% of the U.S. population has diabetes and $176 billion
in direct medical costs are associ-ated with the condition, according to the American Diabetes Associa-tion.
Diabetes trend continues to increase. Prime Therapeutics saw greater than 30% trend in this category in 2015 compared to 2014, according to David Lassen, chief clinical officer at Prime. The average cost of a branded product was approximately $275; almost 20% higher than the year before. Prime also saw utilization increase by more than 10%.
“With the aging population and obesity epidemic in the United States, we would anticipate this trend to continue,” Lassen says. “The use of medication is grow-ing across both generic and brand products; however, brand infla-tionary price hikes and expensive new-to-market products are sig-nificantly impacting trend. Manag-ing diabetes is now exceeding 10% of Prime’s total drug spend.”
Patients with type 2 diabetes can adapt their lifestyle to manage the disease by changing their diet, exer-cising and optimizing their weight, says Cynthia Ambres, MD, KPMG Strategy partner and member of the firm’s Global Healthcare Center of
Excellence. “We understand that type 2 actually can be eliminated for many with these lifestyle changes, unfortunately, many patients don’t commit to these changes and have additional risks associated with high blood pressure and high cholesterol.”
Between 33% and 49% of patients still do not meet targets for glycemic, blood pressure, or cholesterol con-trol, and only 14% meet targets for all three measures and nonsmoking status, according to a position state-ment published in Diabetes Care.
Patients who do not manage the disease well are at high risk for stroke, blindness, kidney failure, and peripheral artery disease.
“The sheer volume of diabetes patients has made it a big driver of medication spending. However, multiple studies examined diabe-tes costs and generally support a correlation of increased adherence
and reduced cost related to avoidable hospi-talizations,” says Ash Shehata, advisory leader for health plans at KPMG. “So health plans,
pharmacy benefit managers and other managed care organizations will place a great deal of emphasis upon medication adherence to save money and also to protect the quality of life of their members.”
Formulary considerationsAll diabetes drugs need to be on managed care’s radar, according to Lassen. “It is important to manage the patient population to the most cost-effective and clinically appro-priate drugs. Trying generics—such as metformin—is an appropriate first-line therapy. Watching the new drugs coming to market and the cost implications is also vital.”
Although growth continues in the diabetes pipeline, many of the upcoming therapies are “me-too” drugs or new combinations of existing therapies, he says. “Given there are a number of drugs in each category, we can deploy preferred product management and exclu-sion strategies to help drive use of the most effective medicines.”
“Many diabetics have fairly complex medication regimens,” Ambres says. “The need to bal-
ance medica-tions, timing and continued monitoring of blood sugar is an ongoing struggle. Newer medica-tions have helped make it easier to
stick to a treatment plan because they have longer-acting formula-tions or act in combination with other drugs. Some of the drugs that are in the pipeline only need to be administered once a week, which is a significant advance, but they will carry higher price tags for both the insurer and on the part of the patient reflected in their self-pay components.”
New DPP-4 (dipeptidyl pepti-dase-4) and human glucagon-like peptide (GLP) drugs are both aimed at treating type 2 diabetes and are gaining traction in the market, according to Ambres.
Several DPP-4 drugs, which
D
Diabetes drug pipelinePatient volume, price increases contribute to rising drug spend by TRACEY WALKER
AMBRES
SHEHATA

Drugs In The Pipeline
Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 37
decrease blood glucose levels, have been on the market since 2006 and more are being introduced.
“The benefit of the DPP-4s is that the drugs show little risk of causing hypoglycemia [low blood sugar], which can lead to a trip to the emergency department,” says Am-bres. “GLP-1 drugs improve insulin sensitivity and have helped patients lose some weight, so some of these diabetes treatments have been mentioning that in their marketing.”
Sodium-glucose co-transport-er-2 [SGLT-2] inhibitors lower blood sugar by blocking reabsorp-tion of glucose by the kidney and increasing its excretion in urine, but FDA said it is requiring label changes because of the risk of uri-nary tract infections and the blood becoming too acidic.
Cost implicationsNewer drugs typically cost health plans more money in terms of pharmacy costs, but the formula-tions coming out now can improve medication adherence, Shehata says. “Biosimilar versions of insulin could lower some of the costs, but we have not seen them hit the mar-ket in the U.S.,” he says.
The injectable drugs, including the insulins and GLP-1 agonists, are expensive therapies, accord-ing to Lassen. There are new combinations coming to market that combine basal insulins with a GLP-1 agonist.
“These combinations are likely to cost thousands of dollars per month,” he says. “The cost of these therapies is not likely going to offset any medical savings from events associated with diabetes. This issue
has been brought to the forefront many times recently—making pay-ers and patients ask, ‘What is the true value of these therapies?’ Many new resources are being developed [e.g., The Institute for Clinical and Economic Review (ICER) reports] to try to quantify the value and appropriate pricing of newer agents. Payers are reviewing these recommendations as well as the incremental clinical value to make tough formulary choices.”
Many first-line drugs used for treating diabetes currently are now generic, such as metformin (Glucophage and Glucophage XR extended-release) and glyburide (Micronase, DiaBeta, and Glynase), according to Kimberly White, senior consultant at Numerof & Associ-ates, a healthcare consulting firm.
“A big focus of R&D is finding ways to improve adherence, like inhaled insulin and once-daily insulin, such as recently launched Tresiba, or once-weekly dosing of oral medicines, such as Trulicity,” White says.
Future considerationsAn aging population that will need more management of diabetes, as well as growing prevalence of type 2 diabetes among younger people be-cause of the obesity epidemic, will keep this category of drug spending and medical management very ac-tive, according to Ambres.
“Science could lead this category in very interesting directions, but that will be farther in the future as stem cell treatments are developed and as research on the artificial pancreas makes progress,” she says.
For example, Clinicaltrials.gov
has counted 113 different studies on research for an artificial pancreas.
Prime anticipates a continued increase of drug spend in this category. “Payers will likely be more aggressive with formulary decisions, utilization management programs and exclusion strategies to try to mitigate the trend while providing appropriate therapy options for their members,” says Lassen. “Health plans may provide additional incentives for their mem-bers to prevent the development of diabetes as a way to offset both pharmacy and medical spending.”
Type 2 diabetes is a health prob-lem that can be effectively managed
as a chronic disease, accord-ing to White. “It will take patients, providers and payers work-ing together to ensure that the patient gets the
right intervention at the right time to minimize the long-term cost impact of the disease,” she says.
Type 2 diabetes is no longer just a concern for the elderly, White points out. “Increasingly, people are being diagnosed with the dis-ease at younger ages,” she says. “As younger people are diagnosed with type 2 diabetes, managed care will need to work with patients and providers to ensure good diabetes management. This may include providing diet and nutritional services, supporting exercise and/or covering medications.”
Tracey Walker is content manager for Managed Healthcare Executive.
WHITE
“Health plans may provide additional incentives for their members to prevent the development of diabetes as a way to offset both pharmacy and medical spending.”DAVID LASSEN, CHIEF CLINICAL OFFICER, PRIME THERAPEUTICS

MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 Managed Healthcare Executive.com38
INNOVATIVE IDEAS FOR DRUG UTILIZATION AND MANAGEMENT
Pharmacy Best Practices
hile the high cost of specialty pharmacy is no surprise in the healthcare industry—commonly
cited problems include pricey R&D, unscrupulous
manufacturers, patents and insufficient competition—infus-ibles have additional challenges. At the top of the list is broad variation in cost depending on site of administration; for example, a hospital outpatient setting is more expensive than an infusion center or home infusion.
“Primarily, the challenges of managing infusible medications arise from the fact that they’re of-ten administered in a professional setting rather than being picked up at a pharmacy by the patient,” says Jim Carlson, vice president, clinical pharmacy services for OmedaRx. “That means that billing is often done after the fact, but it also means that pricing and associated fees vary greatly from one location to the other.
“Further complicating mat-ters is the fact that most infusion claims are billed under a patient’s medical insurance plan, whereas traditional PBMs manage only the pharmacy plan,” he says.
Research by Prime Therapeu-tics, a pharmacy benefits manager, found that it would be appropri-ate for 20% of members receiv-ing infusible/injectable drugs in a hospital setting to receive these medications in a clinic. The
research indicates that for Prime’s clients, transitioning members to a less-expensive setting would result in more than $80 million in annual savings.
Cause and effectJohn Kalada, senior director, strate-gic accounts and market access for Xcenda, says that as payers better manage infusibles through estab-lished clinical and dosing guide-lines that lower reimbursement, physicians are referring patients to hospital outpatient settings to com-pensate for a decrease in payment.
When payments cover proce-dures with little-to-no variability, Kalada says physicians receive a comprehensive “management” or “encounter” fee for each infusion and the corresponding proce-dure—a type of bundled payment. However, plans often mandate
that a designated specialty phar-macy that works directly with the health plan on reimbursement provides the medication to the physician.
“This arrangement removes finan-cial incentive for a physician to use a specific treatment based on potential revenue from an infused option,” he says.
Renee Rayburg, senior director of clinical consulting for Arte-metrx, recommends that payers
gain insight into the vast differenc-es in costs for infusibles adminis-tered at different sites of care and develop programs to enforce use of the most appropriate locations.
Data disconnectsBecause the majority of infusibles fall under the medical benefit, data capture presents another barrier to effectively managing these drugs. “The data are not as clean, rich, or transmitted electronically as phar-macy data are,” Kalada says.
Carlson says there also is minimal available data about new products and urges payers to invest in rigorous clinical review of new medications that hit the market to determine their comparative value against other treatment options.
“Over the long run, plans that maximize the value of their infusion drug spend by carefully selecting the very best medications for their members will experience a total cost of care that stays below national trends,” Carlson says. “With a sound clinical evaluation methodology, plans can then pursue other cost stewardship initiatives, such as prior authorization and site of care.”
Rayburg points to confusion over different billing codes and reimbursement calculations de-pendent on site of administration as another barrier to managing in-fusibles. Physician offices, infusion clinics and home health (agencies or in-home) rely on the Health Care Financing Administration (HCFA)
W
Top challenges and how to navigate them by MARI EDLIN
Managing costs: specialty infusibles
KALADA

Pharmacy Best Practices
Managed Healthcare Executive.com MANAGED HEALTHCARE EXECUTIVE ❚ APRIL 2016 39
claim form, Medicare’s standard form, and use codes unique to a drug or drug class based on the average sales price. If an infusible is delivered in a hospital outpa-tient setting, billing is based on a percent of billed charges and relies on revenue and codes unique to infusions only.
“Because the outpatient codes are unique only to infusions, they do not indicate which drug is being used, making codes less precise,” Rayburg says. “There is a lack of understanding data, how to read reports and how to decipher which medications, how many and what dose. This makes it impor-tant to have someone who can understand all of the codes and translate them.”
Other strategiesIn line with most specialty drugs, infusibles often require prior authorization, which Kalada says is intrinsic to these products. Prior authorization is used extensively to ensure that only patients with a well-documented need are using a specific treatment. If the request meets specific criteria, the plan will approve access and payment.
With certain disease states, Kalada adds, plans sometimes add specialty prescriber restrictions as part of the prior authorization pro-cess. This requires that a designat-ed specialist prescribe the therapy. Plans believe that a specialist in a particular disease area may be better versed in the overall use of a specific therapy, as well as treating those patient types.
As part of the prior-authoriza-tion process, he says some plans require that patients try non-infused therapeutics and demon-strate that a therapy is not effective before using an infused medica-tion. Clinical guidelines also shape treatments at particular points of care and provide a roadmap for therapeutic utilization.
Carlson says that while tra-ditional prior authorization still
plays an important role, other programs such as site-of-care optimization, case management, adherence and billing controls are also necessary to properly manage the cost of treatment over time.
He supports benefit design as a meaningful tool for achieving savings; however, he says that it has been muted by the enormous cost of some of the new specialty medications.
“Generally speaking, patients in need of costly care will certainly max out their benefit every year, which means that the traditional financial reward/incentive/de-terrents that plan designs have wielded become somewhat less meaningful,” Carlson says. “How-ever, plans are beginning to model some interesting designs based on lump sum and health savings account benefit frameworks that may hold some promise.”
Artemetrx recommends the use
of prior authorization, ensuring patients utilize the most cost-effective site of care from the start, along with step therapy, duration of therapy and quantity limits, as an effective tool for managing utilization of infusibles. Evidence-based criteria ensure the right patient with the right diagnosis gets the right drug at the right dose in the right frequency for the right duration, Rayburg says.
Besides prior authorization, the company offers its payer clients a variety of cost-saving oppor-tunities: 1) not paying for drugs administered in an outpatient setting; 2) requiring infusible drugs to be administered at home or in a provider office; and 3) approv-ing drugs based on sites. Most of these protocols are voluntary, but payers may decide to make them mandatory.
Its Specialty Drug Advisor solu-tion provides plan sponsors with advanced analytics, specialty drug expertise and proprietary technol-ogy to manage specialty drug spend across both the pharmacy and medical benefits, helping to reduce clinically inappropriate use, manage reimbursement, optimize sites of care and audit vendor performance through data-driven identification and review. It also offers a site of care program that helps payers transition patients to a more cost-effective site.
Mari Edlin is a frequent contributor to Managed Healthcare Executive. She is based in Sonoma, California.
The amount of money Prime Therapeutics determined it would save annually if 20% of its members receiving infusible/injectable drugs in a hospital setting received these medications in a clinic.
$80 MILLION
ADVERT ISER INDEXThe following is a list of the advertisers in this issue. Although every effort is made to ensure accuracy, this publication assumes no liability for errors or omissions.
Allergan Viberzi 25-27
Athenahealth Corporate 6-7
Bristol-Myers Squibb Corporate CV2-1
Merck & Co., Inc. Zepatier CV4
Advertiser Name Brand Name Page No

For more information, visit zepatier.com.
NOW APPROVED
Copyright © 2016 Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc.
All rights reserved. INFC-1164679-0000 12/15