Embed Size (px)
Citation preview

Breast Cancer Research and Treatment 81: 107–115, 2003.© 2003 Kluwer Academic Publishers. Printed in the Netherlands.
Report
Mammography surveillance following breast cancer
Berta M. Geller1, Karla Kerlikowske2,3, Patricia A. Carney4, Linn A. Abraham5, BonnieC. Yankaskas6, Stephen H. Taplin5, Rachel Ballard-Barbash7, Mark B. Dignan8, RobertRosenberg9, Nicole Urban10, and William E. Barlow5,11
1Health Promotion Research, College of Medicine, University of Vermont, Burlington, VT; 2Department ofEpidemiology and Biostatistics, 3General Internal Medicine Section, Department of Veterans Affairs, University ofCalifornia, San Francisco, CA; 4Norris Cotton Cancer Center/Dartmouth-Hitchcock Medical Center/Departmentof Community and Family Medicine, Dartmouth Medical School, Lebanon, NH; 5Center for Health Studies,Group Health Cooperative, Seattle, WA; 6Department of Radiology, University of North Carolina, Chapel Hill,NC; 7Applied Research Branch, CSRP, DCCPS, National Cancer Institute, Bethesda, MD; 8AMC Cancer Center,Denver, CO; 9Department of Radiology, University of New Mexico, Albuquerque, NM; 10Fred Hutchinson CancerResearch Center, Division of Public Health; 11Department of Biostatistics, University of Washington, Seattle,WA, USA
Key words: breast cancer, mammography, recurrence, screening, surveillance
Summary
Background. To describe when women diagnosed with breast cancer return for their first mammography, and toidentify factors predictive of women returning for mammographic surveillance.
Methods. Women who underwent mammography at facilities participating in the National Cancer Institute’sBreast Cancer Surveillance Consortium (BCSC) during 1996 and who were subsequently diagnosed with ductalcarcinoma in situ or invasive breast cancer were included in this study. Data from seven mammography registrieswere linked to population-based cancer and pathology registries. Kaplan–Meier curves were used to depict thenumber of months from the breast cancer diagnosis to the first mammogram within the defined follow-up period.Demographic, disease and treatment variables were included in univariate and multivariate analyses to identifyfactors predictive of women returning for mammography.
Results. Of the 2503 women diagnosed with breast cancer, 78.1% returned for mammography examinationbetween 7 and 30 months following the diagnosis. Mammography facilities indicated that 66.8% of mammographyexaminations were classified as screening. Multivariate analyses found that women were most likely to undergosurveillance mammography if they were diagnosed at ages 60–69 with Stage 0, I or II breast cancer and hadreceived radiation therapy in addition to surgery.
Conclusions. While the majority of women return for mammographic surveillance following breast cancer,some important subgroups of women at higher risk for recurrence are less likely to return. Research is needed todetermine why some women are not undergoing mammography surveillance after a breast cancer diagnosis andwhether surveillance increases the chance of detecting tumors with a good prognosis.
Introduction
Women with a history of primary unilateral breast can-cer have a 5-year risk of contralateral breast cancer(CBC) approaching 4% [1]. Risk of local recurrence is5–10% at 5 years and increases to 10–15% at 10 years[2–4]. To improve survival, at least one professional
organization concerned with breast cancer care, theAmerican Society of Clinical Oncology, recommendsannual mammographic surveillance for women with ahistory of breast cancer to promote early detection ofnew and recurring breast cancers [5].
Women who have experienced breast cancermay not be sufficiently utilizing surveillance

108 BM Geller et al.
mammography [6, 7]. A 1994 survey of women with ahistory of breast cancer in rural Washington showedthat 30% of the women reported not having had amammographic examination in the past year [8]. Pre-dictors of subsequent mammography use included aphysician recommendation to undergo mammographyscreening and whether the original breast cancer wasmammographically detected. In a study using insur-ance claims data linked with the state cancer registry,as many as 79% of the women under 64 years old diag-nosed in 1989–1991 had follow-up mammographywithin 18 months of breast cancer surgery [9]. In astudy of older breast cancer survivors using Medicareclaims and Surveillance, Epidemiology and End Re-sults (SEER) data for women with cancers diagnosedin 1991, 85% had mammography claims within 2years after treatment [6].
This paper extends what has been previously re-ported by studying a population that includes wo-men of all ages and their subsequent mammographicfollow-up as recorded in the Breast Cancer Surveil-lance Consortium (BCSC) database [10]. Using a largeethnically diverse population, we examined demo-graphic and clinical characteristics that may be relatedto whether or not women returned for surveillancemammography within 7–30 months following a breastcancer diagnosis. Our objectives for this study areto describe when women who were diagnosed withbreast cancer return for their first mammography, howmammography facilities categorize mammographicsurveillance following breast cancer, and to discoverthe factors potentially predictive of women returningfor mammographic surveillance.
Methods
The National Cancer Institute established the BCSC(http://breastscreening.cancer.gov) [10] in 1994, withthe primary objectives being to enhance our under-standing of both breast cancer screening practices andthe natural history of breast cancer in the UnitedStates. Data are pooled from seven mammography re-gistries located in Colorado, New Hampshire, NewMexico, North Carolina, San Francisco, Vermont andwestern Washington state. Data from each BCSCmammography registry are sent without personal iden-tifiers to a central statistical coordinating center forpooled analyses. Data collection methods at all BCSCregistries have been approved by the appropriate Insti-tutional Review Boards, and each registry has received
a certificate of confidentiality issued by the UnitedStates Public Health Service. Confidentiality proce-dures for the protection of data are similar at eachregistry and are described elsewhere [11].
Study population
Women were included in this study if they had screen-ing or diagnostic mammography (index examination)in 1996 and were diagnosed with their first ductal car-cinoma in situ (DCIS) or invasive breast cancer within1 year of that mammography examination associatedwith the detection. Because some breast imaging fa-cilities have closed, merged or stopped participatingin registries, only women seen at mammography fa-cilities that contributed data for five consecutive yearsfrom 1996–2000 were included for analysis. Womenwith a diagnosis of lobular carcinomas in situ wereexcluded from this analysis. Women who reported aprevious history of breast cancer at the time of indexmammography (N = 151), women who had a bilateralmastectomy (N = 13), and women with stage IV dis-ease (N = 38) were excluded from the study. Womenwho were known to have died from any cause duringthe follow-up period were censored at the time of theirdeath in the survival analyses and excluded from uni-variate and multivariate analyses. If vital status wasunknown and no information indicating surveillancemammography existed, we assumed that a woman didnot have an examination.
Measurement and definitions
Characteristics measured at the time of index mam-mography included mammography registry location,race, education, family history of breast cancer, meno-pausal status, and Hispanic origin. Level of educationwas dichotomized into high school graduate or lessversus more than high school. To determine if a breastcancer was detected during screening mammographyor diagnostic mammography, we used the indicationfor the index examination as assigned by the mammo-graphy facility staff. If the indication for examinationwas screening and the mammographic assessment waspositive (BI-RADS assessment category 0, 4 or 5, [12]or 3 with a recommendation for immediate work-up),the cancer was considered screen-detected.
Age at diagnosis, American Joint Committee onCancer (AJCC) stage of breast cancer (TNM patholog-ical staging), receipt of radiation therapy, and typeof cancer-directed surgery (breast-conserving surgerywith and without radiation and unilateral mastectomy

Mammography after breast cancer 109
with and without radiation) were ascertained fromcancer and pathology registries. Breast conservingsurgery (BCS) was defined as anything less than atotal mastectomy. If surgery was categorized as nocancer-directed surgery we coded these cases as miss-ing (5.9% of cases). Receipt of chemotherapy wasnot included in the analyses because the data arenot complete in cancer registries [13]. Most variableswere collected as categorical. Age at diagnosis wascategorized into 10-year age groups.
The follow-up period was defined as 7–30 monthsafter a woman’s breast cancer diagnosis date. Weconsidered up to 7 months post-diagnosis as the treat-ment period and excluded mammography examina-tions done during this time period. It is recommendedto start surveillance mammography 6 months after thecompletion of treatment. We did not know when treat-ment began or ended, so we defined the follow-upperiod up to 30 months after diagnosis to allow forvariation in the timing of treatment. Any screening ordiagnostic examination during the defined follow-upperiod was considered surveillance.
Statistical analysis
Kaplan–Meier curves for the study population and bystage of cancer were used to depict the number ofmonths from the breast cancer diagnosis to the firstsurveillance mammography examination within thedefined follow-up period. Log-rank tests were usedto determine whether the Kaplan–Meier curves weresignificantly different from each other.
All of the above mentioned characteristics wereused to predict which women did and did not havesurveillance mammography using univariate logisticregression models. Odds ratios and 95% confidenceintervals were calculated for each variable in separatelogistic regression models. The variables that weresignificant at p < 0.05 in the univariate analyses werethen combined in a multivariate logistic regressionmodel. To create the most parsimonious multivariatemodel, we removed variables that were not statisti-cally significantly associated with return for screeningmammography or did not affect the magnitude of theassociation of other factors with outcomes. We alsoexamined whether the relationship between BCSCregistry and the probability of returning for a mam-mogram was related to a woman’s age at diagnosis.The interaction between age and registry was exploredextensively. Age could not be fit as a continuousvariable in the interaction term due to the non-linear
relationship between age group and the probability ofreturning for follow-up mammography. Therefore, agewas included in the interaction term using indicatorvariables for each age group. The interaction was notfound to be statistically significant but this could bethe result of sparse data due to the large number ofcategories. Because of the lack of statistical signifi-cance, we do not present these interaction terms in thefinal model. If a BCSC mammography registry did notcollect a demographic, risk factor or treatment vari-able, the registry data were omitted from any analysesthat included that variable. Two-sided p-value < 0.05was considered statistically significant in all of theseanalyses.
Results
There were 2595 women diagnosed with breast can-cer within 1 year of a mammography examinationperformed in 1996 who met the inclusion criteria.Of these 2595 women, 92 died before or duringthe follow-up period and were excluded from Tables1–3 and censored at their time of death when com-puting the Kaplan–Meier curves. Of the remaining2503 women, 1955 (78.1%) returned for at least onemammography examination between 7 and 30 monthsfollowing the diagnosis. Approximately two percentof women had mammography examinations duringthe 0–6-month period but did not appear again formammography. An additional 2% returned after the30-month time period for surveillance mammographybut did not appear during the 7–30-month follow-upperiod. Five women had mammography before andafter the designated follow-up but not during the 7–30month time period. The indication for examinationassigned by staff at the radiology facility for the first
Table 1. Mammography facility’s indication for first follow-upmammogram∗
Indication N %
Routine screening 1305 66.8
Additional evaluation 101 5.2
Short interval follow-up 169 8.6
Evaluation of breast problem 295 15.1
Other procedures 5 0.3
Missing 80 4.1
Total 1955 100.0
∗ Only women with a follow-up mammogram are included.

110 BM Geller et al.
Table 2. Characteristics of study population by pattern of follow-up mammography
Characteristics Total Any follow-up Odds ratio 95% CI p-value
(2503) mammogram (N = 1955)
N %
Age at diagnosis <0.001
<40 128 77 60.2 0.52 0.35–0.78 0.002
40–49 496 369 74.4 1.00 Referent group
50–59 618 478 77.3 1.18 0.89–1.55 0.252
60–69 586 514 87.7 2.46 1.79–3.39 <0.001
70–79 478 387 81.0 1.46 1.08–1.99 0.014
80+ 197 130 66.0 0.67 0.47–0.96 0.027
Race (1.00% missing) 0.482
white 2261 1762 77.9 1.00 Referent group
black 138 104 75.4 0.87 0.59–1.31 0.482
Native Amer/Eskimo/Aleutian 17 15 88.2 2.12 0.60–13.50 0.318
Asian/Pacific islander 55 47 85.5 1.66 0.83–3.83 0.187
Other/mixed 7 5 71.4 0.71 0.15–4.95 0.680
Hispanic (23.2% missing)
Yes 191 145 75.9 1.00 Referent group
No 1731 1363 78.7 1.18 0.82–1.66 0.368
Education∗ (33.6% missing)
HS grad/GED or less 543 433 79.7 1.02 0.77–1.34 0.917
College/Tech/Post-grad 727 578 79.5 1.00 Referent group
Family history of breast cancer∗ (8.7% missing)
Yes 345 271 78.6 1.00
No 1471 1203 81.8 1.23 0.91–1.63 0.168
Postmenopausal (14.0% missing)
Yes 1766 1422 80.5 1.61 1.25–2.06 <0.001
No 386 278 72.0 1.00 Referent group
Cancer detected by positive screening (1.3% missing)
Yes 1218 975 80.0 1.25 1.04–1.52 0.021
No 1252 954 76.2 1.00 Referent group
Stage of breast cancer (17.7% missing) 0.037
0 349 275 78.8 1.72 1.05–2.80 0.030
I 1030 827 80.3 1.89 1.20–2.93 0.005
II 579 448 77.4 1.59 0.99–2.50 0.051
III 101 69 68.3 1.00 Referent group
Received radiation therapy (9.2% missing)
Yes 1008 865 85.8 2.28 1.84–2.83 <0.001
No 1265 919 72.6 1.00 Referent group
Cancer-directed surgery∗∗ (5.9% missing) <0.001
Mastectomy with radiation 136 107 78.7 1.00 Referent group
Mastectomy without radiation 697 517 74.2 0.78 0.49–1.20 0.269
BCS∗∗∗ with radiation 752 671 89.2 2.25 1.39–3.56 0.001
BCS∗∗∗ without radiation 286 224 78.3 0.98 0.59–1.60 0.934
∗ Excludes one registry because data not collected.∗∗ Excludes one registry because of high amount of missing data.∗∗∗ Breast conserving surgery.

Mammography after breast cancer 111
Table 3. Final model of predictors for returning for surveillancemammography
Characteristics Odds 95% CI p-value
ratios∗
Age at diagnosis
<40 0.80 0.42–1.55 0.489
40–49 1.00 Referent
group
50–59 1.11 0.75–1.64 0.614
60–69 1.88 1.22–2.89 0.004
70–79 1.21 0.80–1.81 0.370
80+ 0.90 0.54–1.53 0.693
Stage of breast cancer (17.7% missing)
0 1.70 0.88–3.26 0.112
I 1.63 0.89–2.92 0.108
II 1.65 0.90–2.95 0.099
III 1.00 Referent
group
Cancer-directed surgery∗∗ (5.9% missing)
Mastectomy with radiation 1.00 Referent
group
Mastectomy without 0.54 0.29–0.96 0.044
radiation
BCS∗∗∗ with 1.44 0.74–2.66 0.263
radiation
BCS∗∗∗ without 0.65 0.33–1.25 0.208
radiation
∗ Adjusted by mammography registry in addition to all variables inthe table.∗∗ Excludes one registry because of high amount of missing data.∗∗∗ Breast conserving surgery.
follow-up mammography is shown in Table 1. A totalof 66.8% of women returned for a routine screeningexamination, while 23.7% returned for a short intervalfollow-up or evaluation of a breast problem.
Of those women who returned for surveillancemammography during the 7–30 months followingdiagnosis, 74.3% (1453/1955) had two or more mam-mography examinations, and 25.7% (502/1955) hadonly one during that time period. Women who re-ceived breast conserving surgery (715), rather than aunilateral mastectomy (434) were significantly morelikely to have received two or more mammograms dur-ing the follow-up period (69% vs. 52%, p < 0.0001).
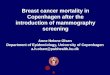
Within 12 months of diagnosis approximately 50%of women had their first surveillance mammography(Figure 1). At this time the proportion of womenreturning for surveillance mammography begins todiffer by registry, and by the end of the 30-month
Figure 1. Kaplan–Meier curve for time to first follow-up surveil-lance mammography. Probability that a woman returned for fol-low-up mammography during the 7–30 months after diagnosis ofbreast cancer.
follow-up period, the proportion ranges from 68 to87% among BCSC registries. The log-rank test com-paring BCSC registries to each other resulted in ap-value <0.001, showing that registries are statisti-cally different in the number of women who returnedfor follow-up mammography visits.
Univariate odds ratios showed that, compared towomen ages 40–49, those diagnosed before age 40and age 80 or older were least likely to return forsurveillance mammography (Table 2). Women ages60–79 years were more likely to return. Neither race,nor Hispanic origin, or level of education was as-sociated with returning for mammography. Womenwho were postmenopausal (vs. premenopausal) andthose whose breast cancer was screen-detected weremore likely to return for mammographic surveillancethan women whose cancers were not screen-detected.Women with early stage disease were 60–90% morelikely to return for surveillance mammography com-pared to women with stage III disease. Only 20.8%(21/101) of cancers diagnosed at stage III were screen-detected compared with 64.4% (224/348) of stage0,53.1% (541/1018) of stage I, and 34.5% (197/571)of stage II cancers that were screen-detected in thisstudy. Treatment also influenced return for surveil-lance mammography. Women who received radiationtherapy were approximately 2.3 times more likely toreturn for mammography than those who did not. Ofthose who received radiation therapy, women who hadBCS were more likely to have a follow-up mammo-gram than women who had a unilateral mastectomy(OR = 2.3; CI 1.39–3.56).
Multivariate results are presented in Table 3. Thefinal prediction model included only age at diagnosis,stage, and receipt of cancer directed surgery. As stage

112 BM Geller et al.
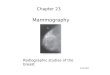
Figure 2. Kaplan–Meier curves for time to follow-up by stage.Probability that a woman returned for follow-up mammographyduring the 7–30 months after diagnosis of breast cancer.
was associated with both type of treatment and like-lihood of returning for a follow-up mammogram, itremained in the final model although it was not stat-istically significant. In addition to being aged 60–69,only one other factor, treatment with mastectomywith radiation, was statistically significantly associ-ated with return for surveillance mammography, withabout a 50% reduction in return for women who weretreated with mastectomy without radiation. While notstatistically significant, women with an earlier stageof diagnosis (stage 0, OR = 1.7; stage I, OR = 1.6;stage II, OR = 1.7) were more likely to return for sur-veillance mammography during the 7–30-month timeperiod.
Figure 2 gives the Kaplan–Meier curves illustrat-ing the time to first surveillance mammography forwomen at different stages of diagnosis. The conclu-sions drawn from these curves agree with those fromthe multivariate models; women who have an earlierstage of disease return more quickly than women withstage III breast cancer. The curves are almost parallelfor stages 0, I and II, and are more divergent fromstage III at about 12 months from diagnosis. Over 35%of women with late-stage breast cancer did not returnfor mammography by the end of the follow-up period.The p-value for a log-rank test comparing the threeKaplan–Meier curves for stage was <0.001.
Discussion
We found that women with a recent personal history ofbreast cancer were most likely to undergo surveillancemammography if they were diagnosed at ages 60–69years, with stage 0, I or II breast cancer, and received
radiation therapy in addition to surgery. Women whohave been diagnosed with breast cancer are at high riskfor CBC and disease recurrence. It is important thatwomen who have been diagnosed with breast cancerwith good long-term prognosis undergo surveillancefor early detection of CBC and local recurrent disease.Although mammography will not detect all new andrecurrent breast cancers it will identify a significantproportion.
The ability of mammography alone to detect recur-rent disease varies in previous studies depending onthe interval of screening, time period of the study, andstages of breast cancer included in the study [14–16].Recurrent DCIS is more frequently detected mammo-graphically than recurrent invasive breast cancers; inthis study all six of the DCIS recurrences were mam-mographically detected compared to only 14 of the 20subsequent invasive breast cancers [14].
Size and tumor stage may influence detection ofa recurrent or new primary breast cancer. Womenwith recurrent stage I and II breast cancers who weretreated with BCS and radiation therapy had a favorableprognosis if the tumors were smaller than 2 cm andconfined to the breast [4]. Another study found that re-currences detected by mammography alone were lesslikely to develop further relapses compared to recur-rences detected by clinical examination. Patients withDCIS or locally invasive recurrences were more likelyto have had the recurrence detected mammographi-cally than women with regional or distant invasive dis-ease (71 and 33%, respectively) [18]. In a more recentstudy, recurrence detected by mammography alone orcombined with clinical examination was significantlymore likely to be associated with prolonged survivalthan detection by clinical examination alone [19]. Thissurvival advantage may be explained by lead-time biasfrom earlier diagnosis by mammography. In additionto mammography being able to detect early, non-palpable recurrences [20], imaging also contributesclinically relevant information for surgical treatmentplanning [21].
We would expect mammography to be as goodat detecting CBC as it is in detecting primary tu-mors. Recurrences in the same breast are more difficultto diagnose with mammography than CBC due totreatment-induced changes to the breast [14]. In astudy that compared detection of asynchronous CBCfrom two cities in the Netherlands, one with and onewithout mammography screening [22], 70% of theCBCs were detected by mammographic screening inthe city using both mammography and clinical breast

Mammography after breast cancer 113
examination. Thirty-five percent of these mammo-graphically detected tumors were ≤10 mm or in situdisease compared with 7% that were detected by clin-ical breast examination in the other city. In addition,75% of the mammographically detected CBC’s werenode negative compared with 57% detected by clinicalexamination. Their follow-up period was insufficientto measure survival. Another study found that evenwhen mammography surveillance led to a more favor-able stage at diagnosis, they were unable to realize animprovement in breast cancer mortality [23]. In twomore recent studies mammography alone was able todetect 37–40% of the CBCs [24, 25], slightly lowerthan the 49% of primary tumors reported here. Onestudy found that women whose CBC was diagnosedby mammography were statistically more likely tosurvive than women whose CBC was diagnosed byother means [24]. A second study reported that 83%of the tumors detected by mammography had goodprognostic features compared with 38% of those diag-nosed by routine clinical examination [25]. Thesestudies suggest that among women with breast cancerregular mammography surveillance may help in theearlier diagnosis of CBC. This is certainly an area forfurther study.
While women who are treated with BCS withoutradiation therapy are less likely to return for sur-veillance mammography, they are at elevated risk oflocal recurrence [26]. As many as 35% of womenwho do not receive radiation therapy may have re-current disease, and 80% of these recurrences willoccur during the first 5 years after treatment [26].Women who were not treated with radiation maybe less likely to have access to medical care or beengaged with the medical system, or follow phy-sician recommendations. Women who had radiationtherapy for breast cancer, regardless of the type ofsurgery, were more likely to have four consecutivemammography examinations and most were orderedby the radiation oncologist [7]. Our results are sim-ilar to a SEER-Medicare study that [6] found 22%of women who had BCS and no radiotherapy didnot return for surveillance mammography. However,we found a higher percentage (11%) of women withBCS and radiation therapy not receiving mammo-graphy during the follow-up period compared withthe SEER-Medicare study (4%). This may be due tothe age difference in the populations studied. Anothersimilarity in results between the two studies is thatwomen who had BCS with radiation therapy weresignificantly more likely than women with mastec-
tomy and radiation therapy to return for surveillancemammography.
We found women with a diagnosis of late stagebreast cancer were less likely to return for surveil-lance mammography than women with earlier stagediagnoses. The two studies that used insurance claimsdata only included women diagnosed with an AJCCstage of II or less [6, 9]. The SEER-Medicare studyfound that receipt of mammography did not differbetween women diagnosed with stage 0 and stage I,and that women with stage II cancers were less likelyto return for surveillance mammography than womenwith in situ disease (OR 0.66, 95% CI: 0.47–0.93).Similarly, we found that women with stage II wereslightly less likely to return for mammography thanwomen diagnosed with stage 0 disease. Women in ourstudy with late stage disease were almost half as likelyto have had their breast cancer detected by screen-ing mammography suggesting that these women maynot have confidence that a disease recurrence wouldbe visible on a mammogram. We found no publishedresearch that shows that early detection of recurrentmetastatic disease or detection of a new primary inthe contralateral breast of a woman with metastaseswill improve survival. Therefore, there may be no in-dication for physicians to recommend mammographicsurveillance for women with late stage disease. This isan area that requires further exploration.
Our follow-up period for surveillance mammo-graphy started at 7 months after the diagnosis ofbreast cancer. The American Society for ClinicalOncology (ASCO) recommends surveillance mammo-graphy start 6 months after the completion of radi-ation therapy [5]. At some institutions surveillancebegins 9–12 months after radiation therapy becausemost benign changes to the breast following treat-ment are expected to stabilize by that time [15]. Wedo not have data on when treatment began or endedso we defined the follow-up period up to 30 monthsafter diagnosis to allow for variation in the timingof treatment. Most women returned for at least onemammographic examination during that time periodand 74% of the women who returned had two ormore mammograms. Although ASCO does not re-commend biannual surveillance mammography, manyproviders are following women after treatment withBCS with mammography every 6 months for the first2–3 years [14]. While we focused on any surveillancein our study, we also found that women who haveBCS rather than mastectomy were more likely to havehad multiple mammography examinations during the

114 BM Geller et al.
follow-up period. For example, the prevalence of 1 and2 or more mammography examinations in the follow-up period was 17 and 69%, respectively, in womenwith BCS compared to only 23 and 52%, respectively,in women with mastectomy.
Unlike the two previous studies that used insur-ance claims data, our study population spanned all agegroups. Women diagnosed with breast cancer duringtheir sixth decade of life are more likely to have sur-veillance mammography than both older and youngerwomen. Women in their sixties may be in better healththan older women and therefore are able to receiveand benefit from mammography. They may be lessbusy and they may be more likely to have their mam-mography covered by insurance than younger women.This is an area worthy of further research.
There are several limitations of this study. Co-morbidity data were not available for the women inthis study, which may influence whether women returnfor mammography [6]. We are missing vital status fora very few women at one registry, and may be missingsome mammograms performed for surveillance. Thecompleteness of mammographic ascertainment variesamong registries, which can lead to an underestimateof the proportion of women undergoing surveillance.In addition, we can assume some loss of follow-upmammography if women receive care outside of thecatchment areas of each registry. Despite these limita-tions, our results are very similar to the two previouslypublished reports that used claims databases and can-cer registries and had similar limitations [6, 9], aswell as a third study that used medical record ab-straction and phone interviews [7]. Our results showeda higher proportion of women returning for surveil-lance mammography than reported in the telephonesurvey conducted in Washington state [8], however ourfollow-up period was 6 months longer.
We found that despite recommendations by at leastone professional organization, many women have notreturned for mammography after treatment for breastcancer. Some of these women were diagnosed at a latestage and most likely will not benefit from surveil-lance mammography. Other women not returning forsurveillance mammography did not received radiationtherapy with BCS. These women did not receive thestandard recommended therapy for breast cancer andhence are at higher risk for recurrence and may bene-fit from surveillance mammography. It is notable thatthey are also not receiving surveillance mammographyas advised by at least one professional organization,suggesting a pattern of receipt of non-standard care.
All physicians involved in breast cancer care need tobe more active in evaluating the need for surveillanceand discussing this with women. Research is neededto determine why some women are not undergoingmammography surveillance after a breast cancer dia-gnosis and whether surveillance increases the chanceof detecting tumors with a good prognosis.
Acknowledgements
This work was supported by cooperative agree-ments UO1CA63731, UO1CA63736, UO1CA63740,UO1CA69976, UO1CA70013, UO1CA70040,UO1CA86076, and UO1CA86082 from the NationalCancer Institute, as part of the NCI’s Breast CancerSurveillance Consortium, and by RO1CA63146.
References
1. Broet P, de la Rochefordiere A, Scholl S, Fourquet A, MosseriV, Durand JC, Pouillart P, Asselain, B: Contralateral breastcancer: annual incidence and risk parameters. J Clin Oncol13: 1578–1583, 1995
2. Fowble B, Solin LJ, Schultz DJ, Weiss MC: Breast recurrenceand survival related to primary tumor location in patients un-dergoing conservative surgery and radiation for early-stagebreast cancer. Int J Radiat Oncol Biol Phys 23: 933–939, 1992
3. Recht A, Silen W, Schnitt SJ, Connolly JL, Gelman RS, RoseMA, Silver B, Harris JR: Time-course of local recurrence fol-lowing conservative surgery and radiotherapy for early stagebreast cancer. Int J Radiat Oncol Biol Phys 15: 255–261, 1988
4. Kurtz J, Amalric R, Ayme HB, Jacquemier J, Pietra J, HansD, Pollet JF, Bressac C, Spitalier JM: Local recurrenceafter breast-conservation surgery and radiotherapy. Cancer 63:1912–1917, 1989
5. Smith T, Davidson N, Schapira D, Grunfeld E, Muss H,Vogel V, Somerfield MR: American Society of Clinical Oncol-ogy 1998 update of recommended breast cancer surveillanceguidelines. J Clin Oncol 47: 1080–1082, 1999
6. Schapira M, McAuliffe T, Nattinger A: Underutilization ofmammography in older breast cancer survivors. Med Care 38:281–289, 2000
7. Lash T, Sillman R: Medical surveillance after breast cancerdiagnosis. Med Care 39: 945–955, 2001
8. Andersen M, Urban N: The use of mammography by survivorsof breast cancer. Am J Public Health 88: 1713–1715, 1998
9. Hillner B, McDonald K, Penerthy L, Desch C, Smith T,Maddux P, Glasheen WP, Retchin SM: Measuring standardsof care for early breast cancer in an insured population. J ClinOncol 15: 1401–1408, 1997
10. Ballard-Barbash R, Taplin S, Yankaskas B, Ernster V,Rosenberg R, Carney PA, Barlow, W, Geller B, KerlikowskeK, Edwards B, Lynch C, Urban N, Chrvala C, Key C, PoplackS, Worden JK, Kessler L: Breast Cancer Surveillance Con-sortium: a national mammography screening and outcomesdatabase. AJR 169: 1001–1008, 1997

Mammography after breast cancer 115
11. Carney PA, Geller B, Moffett H, Ganger M, Sewell M, BarlowWE, et al.: Medico-legal issues and protective policies andprocedures for data integrity and confidentiality in a largemulti-center research program: The National Cancer Insti-tute’s Breast Cancer Surveillance Consortium. Am J Epi-demiol 152: 371–378, 2000
12. D’Orsi C, Bassett L, Feig S, Jackson VP, Kopans DB, LinverMN, Sickles EA, Stelling CB: Illustrated breast imaging re-porting and data system: Illustrated BI-RADSTM. 3rd edn,American College of Radiology, Reston, VA, 1998
13. Bickell N, Chassin M: Determining the quality of breast can-cer care: do tumor registries measure up? Ann Intern Med 132:705–710, 2000
14. Giess C, Keating D, Osborne M, Rosenblatt R: Local tu-mor recurrence following breast-conservation therapy: cor-relation of histopathologic findings with detection methodand mammographic findings. Radiology 212: 829–835,1999
15. Orel S, Troupin R, Patterson E, Fowble B: Breast cancer recur-rence after lumpectomy and irradiation: role of mammographyin detection. Radiology 183: 201–206, 1992
16. Ashkanani F, Sarkar T, Needham G, Coldwells A, Ah-SeeA, Gilbert F, Hutcheon AW, Eremin O, Heys SD: What isachieved by mammographic surveillance after breast conser-vation treatment for breast cancer? Am J Surg 182: 207–210,2001
17. Muss H: Postoperative follow-up after early-stage breast can-cer. Breast J 2: 281–285, 1996
18. Abner A, Recht A, Emberlein T, Come S, Shulman L, HayesD, Connolly JL, Silver B, Harris JR: Prognosis followingsalvage mastectomy for recurrence in the breast after con-servative surgery and radiation therapy for early-stage breastcancer. J Clin Oncol 11: 44–48, 1993
19. Doyle T, Schultz D, Peters C, Harris E, Solin L: Long-termresults of local recurrence after breast conservation treatment
for invasive breast cancer. Int J Radiat Oncol Biol Phys 51:74–80, 2001
20. Grosse A, Schreer I, Frischbier H, Maass H, Loening TB,Ahnsen J: Results of breast conserving therapy for early breastcancer and the role of mammographic follow-up. Int J RadiatOncol Biol Phys 38: 761–767, 1997
21. Dershaw D: Mammography in patients with breast cancertreated by breast conservation (lumpectomy with or withoutradiation). AJR 164: 309–316, 1995
22. Mellink W, Holland R, Hendriks J, Peeters P, Rutgers E,van Daal W: The contribution of routine follow-up mammo-graphy to an early detection of asynchronous contralateralbreast cancer. Cancer 67: 1844–1848, 1991
23. Ciatto S, Ambrogetti D, Bonardi R, Bravetti P, Del Tureo M:Prognostic impact of early detection of contralateral primarybreast cancer. Tumori 76: 370–373, 1990
24. Kaas R, Hart A, Besard A, Peterse J, Rutgers E: Impact ofmammographic interval on stage and survival after the diag-nosis of contralateral breast cancer. Br J Surg 88: 123–127,2001
25. Kollias J, Evans A, Wilson R, Ellis I, Elston C, Blamey R:Value of contralateral surveillance mammography for primarybreast cancer. World J Surg 24: 983–989, 2000
26. Fisher B, Anderson S, Redmond C, Wolmark N, WickerhamD, Cronin W: Re-analysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomywith lumpectomy with or without irradiation in the treatmentof breast cancer. N Engl J Med 333: 1456–1461, 1995
Address for offprints and correspondence: Berta M. Geller,Ed.D., University of Vermont, Office of Health PromotionResearch, 1 South Prospect Street, Burlington, VT 05401-3444,USA; Tel.: +1-802-656-4187; Fax: +1-802-656-8826; E-mail:[email protected]