Embed Size (px)
Citation preview
Mammography Outcomes Audit
D U K E E L D R I D G E , M . S .
M E D I C A L P H Y S I C I S T

Mammography Medical Outcomes Audit
An audit is required by MQSA…
The ultimate QC test… Outcomes

The Current Law
Quality assurance-mammography medical outcomes audit. Eachfacility shall establish and maintain a mammography medical outcomes auditprogram to follow-up positive mammographic assessments and to correlatepathology results with the interpreting physician's findings. This program shallbe designed to ensure the reliability, clarity, and accuracy of the interpretationof mammograms.
(1) General requirements. Each facility shall establish a system to collectand review outcome data for all mammograms performed, including follow-upon the disposition of all positive mammograms and correlation of pathologyresults with the interpreting physician's mammography report. Analysis ofthese outcome data shall be made individually and collectively for allinterpreting physicians at the facility. In addition, any cases of breast canceramong women imaged at the facility that subsequently become known to thefacility shall prompt the facility to initiate follow-up on surgical and/orpathology results and review of the mammograms taken prior to the diagnosisof a malignancy.

The current Law
(2) Frequency of audit analysis. The facility's first audit analysis shall beinitiated no later than 12 months after the date the facility becomes certified, or12 months after April 28, 1999, whichever date is the latest. This audit analysisshall be completed within an additional 12 months to permit completion ofdiagnostic procedures and data collection. Subsequent audit analyses will beconducted at least once every 12 months.
(3) Reviewing interpreting physician. Each facility shall designate at leastone interpreting physician to review the medical outcomes audit data at leastonce every 12 months. This individual shall record the dates of the auditperiod(s) and shall be responsible for analyzing results based on this audit. Thisindividual shall also be responsible for documenting the results, notifying otherinterpreting physicians of their results and the facility aggregate results. Iffollow-up actions are taken, the reviewing interpreting physician shall also beresponsible for documenting the nature of the follow-up.

You have to answer these questions
Current FDA Inspector’s Audit Questions…

Basic Audit Elements
The basic elements of a mammography medical audit system:
(1) definition of positive mammograms requiring follow-up,
(2) a method to follow-up positive mammograms
(3) a system to attempt to collect pathology results for all biopsies performed,
(4) methods to correlate pathology results with the final assessment category indicated by the interpreting physicians,
(5) a method to include any cases of breast cancer among patients imaged at the facility that subsequently became known to the facclity, and
(6) review of medical outcomes audit data for the aggregate of interpreting physicians as well as each individual interpreting physician at least once every 12 months.

PGHS
PGHS Subtopics

FDA Guidance for MMOA

KansasRadiationPhysics.com

D. Eldridge, M.S.
12
1994 DHS Publication
Lawrence W. Bassett, M.D(Co-chair)
E. Edward Hendrick, PhD(Co-chair)
Tamsen L. Bassford, MD
Priscilla F. Butler,MS
Darryl Carter,MD
Marydale DeBor, JD
Carl J. D’Orsi, MD
Carol J. Garlinghouse, MSN, RNC
Richard F. Jones III, MD
Amy S. Langer, MBA
J. Leonard Lichtenfeld, MD
Janet R. Osuch, MD
Lynda N. Reynolds, BS,RT
Ellen Shaw de Paredes, MD
Richard E. Williams, MD
US Dept of Health and Human Services
Public Health Service
Agency for Health Care Policy and Research
Rockville, Maryland
AHCPR Publication No. 95-0632
October 1994

1994 Clinical Determinants

MMOA Results at selected sites

2013 BIRADS 5TH Edition

Bi-Rads 5th Edition, 2013

BIRADS

Mammography Medical Outcomes Audit
Lead Interpreting Physician:________________________, M.D. has the general responsibility of ensuring that the quality assurance program meets all theFDA requirements. No individual shall be assigned or shall retain responsibility for quality assurance tasks unless the lead interpreting physician hasdetermined that the individual’s qualifications for, and performance of, the assignment are adequate.
Audit Interpreting Physician:________________________, M.D. will review the medical outcomes audit data at least once every 12 months, recording thedates of the audit period(s) and shall be responsible for analyzing results based on this audit. This individual shall also be responsible for documenting theresults, notifying other interpreting physicians of their results and the facility aggregate results. If follow-up actions are taken, the reviewing interpretingphysician shall also be responsible for documenting the nature of the follow-up.
Interpreting Physicians:
___________________________, M.D. ___________________________, M.D.
___________________________, M.D. ___________________________, M.D.
___________________________, M.D. ___________________________, M.D.
All interpreting physicians must follow the facility procedures for corrective action when the images they are asked to interpret are of poor quality. They must allparticipate in the facility's medical outcomes audit program.
QC Technologist: ___________________________, R.T.(M) is responsible for all individual tasks within the quality assurance program not assigned to thelead interpreting physician or the medical physicist. The tasks are to be performed by the quality control technologist or by other personnel qualified to performthe tasks. When other personnel are utilized for these tasks, the quality control technologist shall ensure that the tasks are completed in such a way as to meetthe FDA requirements.
MMOA Outcomes/Recall: _________________________, R.T.(M) will assist the Lead Interpreting Physician with tasks pertaining to the keeping of totals forall positive readings on patients and for patients who were initially read as negative but were later found out to have pathology(False Negatives). Patients willbe tracked until all follow-up is completed and documented as required by the MQSA.
Medical Physicist: ___________________________, M.S., will perform the mammography equipment survey and oversee the equipment-related qualityassurance practices of the facility. At a minimum, the medical physicist shall be responsible for performing the surveys and mammography equipmentevaluations and providing the facility with the reports as required within 1 month after the survey.

D. Eldridge, M.S. 19
Transferred to Another Facility
for Work-up & Audit Purposes
B
Utilize Orig. Flow Sheet,
Adding "O" Before Each Class
e.g. OA, OS+, etc.
Follow-up
Unavailable
C
Category 0
"Additional Imaging Required"
CANCER
within 1 Year
A+ . . .
Categories 1 & 2
"Negative" or "Benign"
A
CANCER
within 1 Year
D+ . . .
Follow-up Result:
Category 1 or 2
D
Follow-up Result:
Continue to Follow as Cat. 3
E
CANCER
within 1 Year
H+ . . .
Biopsy Recommended,
but not Done
H
Return Follow-up
in 3-6 months
JF
CANCER
within 1 Year
J+ . . .
Benign
J
CANCER
K . . .
Core Biopsy
Follow-up
Unavailable
I
CANCER
within 1 Year
L+ . . .
Benign
L
CANCER
M . . .
Surgical Biopsy
Follow-up Result:
Category 4 or 5
Biopsy Recommended
Transfer to Another Facility
for Work-up & Audit Purposes
F
Follow-up
Unavailable
G
Category 3
"Probably Benign"
Additional Follow-up Recommended
CANCER
within 1 Year
P+ . . .
Biopsy Recommended,
but not Done
P
Follow-up in
3-6 Months
SF
CANCER
within 1 Year
S+ . . .
Benign
S
CANCER
T . . .
Core Biopsy
CANCER
within 1 Year
U+ . . .
Benign
U
CANCER
V . . .
Surgical Biopsy
Follow-up
Unavailable
R
Categories 4 & 5
"Suspicious or Highly Suggestive of Malignancy"
Biopsy Recommended
Screening Algorithm
Category 6, Categories 4A, 4B,
& 4C:
The 2003 ACR BI-RADS
reporting system has a new
“Category 6” for “known
biopsy-Proven malignancy,
with no therapy undergone by
the patient”. This was added
so that screening patients
already known to have cancer
would not skew detection
rates. The ACR has also
added subcategories for
Category 4: 4A, 4B, and 4C to
encourage pathologists to
initiate further evaluation of
benign results and should
allow clinicians to better
understand follow-up
recommendations after biopsy
for findings placed in Category
4 subsets. Some other
nomenclature changes have
been made.

Mammography Medical Outcomes Audit
Must follow all patients who “end up” being classified as Category 4 or 5.

Manually following biopsies…

D. Eldridge, M.S. 22
PatientName:_________________________________________________I.D.#:__________________
(Last) (First) (Middle)
Address:_____________________________________________________Phone#:__________
Primary Physician:___________________________________________Office#:___________
Date of positive mammogram:___________ Dates of priormammograms:_________________
Done by:________________R.T.(M) Read by:________________M.D. on_______________
(date)Patient information, history, and other information attached.
Mammography Reports attached? Initial Reading Category: 0, 1, 2, 3, 4 ,or 5
Additional interpretivecomments:________________________________________________
Details of Follow-up
(U=Ultrasound, S=Surgical consult, B=Radiological Biopsy,C(months)=Clinical Exam, X=eXtra views)
A. Date:____________ Type Follow-up:_______ Doneby:________________________M.D.
Results:_______________________________________________________________________
_____________________________________________________________________________
Future Follow-up: ______________________Date:______________ Recordedby:__________
B. Date:___________ Type Follow-up:_______ Doneby:________________________M.D.
Results:_______________________________________________________________________
Details of Follow-up
(U=Ultrasound, S=Surgical consult, B=Biopsy, C(months)=Clinical Follow-up Exam)
PatientName:____________________________________________I.D.#:_________________
(Last) (First) (Middle)
C. Date:___________ Type Follow-up:_______ Doneby:________________________M.D.
Results:______________________________________________________________________
_____________________________________________________________________________
Future Follow-up: ______________________Date:______________ Recordedby:__________
D. Date:___________ Type Follow-up:_______ Doneby:________________________M.D.
Results:_______________________________________________________________________
_____________________________________________________________________________
Future Follow-up: ______________________Date:______________ Recordedby:__________
E. Date:___________ Type Follow-up:_______ Doneby:________________________M.D.
Results:_______________________________________________________________________
_____________________________________________________________________________
Future Follow-up: ______________________Date:______________ Recordedby:__________

Mammography Medical Outcomes Audit
# Screenings/year: _______
# Biopsies Recommended: _______
# Biopsies Done: _______
# Cancers Found: _______
Cancer Stage when found: _______

Mammography Medical Outcomes Audit
# Screenings: 6408
# Biopsies Recommended: 190
# Biopsies Done: 164
# Cancers Found: 25

Mammography Medical Outcomes Audit
Biopsy Completion Rate (85%): 86.3%
Biopsies Rec./1000 patients(32): 29.7
Cancers found/1000 patients(6): 3.9

Mammography Medical Outcomes Audit
Test +
Test -
Disease + Disease -
True PositiveFalse
Positive
False
Negative
True
Negative

Mammography Medical Outcomes Audit
Categories
4, 5, 0+,3+
Categories
1,2,3, & 0
Disease + Disease -
True
Positive
False
Positive
False
Negative
True
Negative

D. Eldridge, M.S. 28
True Positives (TP). Cancer diagnosed within 1 year after biopsy recommendation based on abnormal mammogram.
*True Negative (TN). No known cancer diagnosed within 1 year of normal mammogram.
*False Negative (FN). Cancer diagnosed within 1 year of a normal mammogram. Although other definitions of false negative exist, this definition is the most widely applied.
*False Positive (FP). Benign disease found at biopsy within 1 year after an abnormal mammogram and recommendation for
biopsy or surgical consultation.

D. Eldridge, M.S. 29
*Sensitivity. The probability of detecting a cancer when a cancer exists,or the percentage of all patients found to have breast cancer within 1year of screening who were correctly diagnosed at the screeningsession.
Sensitivity = TP/(TP+FN)
85-90%
*Specificity. The probability of a normal mammogram report when nocancer exists, or the percentage of all patients not found to have breastcancer within 1 year of screening who were correctly identified asnormal at the time of screening.
Specificity = TN/(FP+TN).

D. Eldridge, M.S. 30
Categories
4, 5, 0+,3+
Categories
1,2,3, & 0
Disease + Disease -
True
Positive
False
Positive
False
Negative
True
Negative
Sensitivity=TP/(TP+FN) Specificity=TN/(FP+TN)

Magview

Mammography Medical Outcomes Audit

Mammography Medical Outcomes Audit
Analyzing Biopsy Data

Mammography Medical Outcomes Audit
Positive predictive value (PPV). Three definitions may be applied, depending on the practice conditions.

D. Eldridge, M.S. 35
*PPV1 (Abnormal Reading). The percentage of all screening mammography cases that result in a diagnosis of cancer based on abnormal screening examination.
PPV1 = TP/(number of abnormal screening exams), or
PPV1 = TP/(TP+FP1).
*PPV2 (Biopsy recommended). The percentage of all screening mammography cases that result in a diagnosis of cancer based on a recommendation of consideration for biopsy.
PPV2 = TP/(# of cases recommended for biopsy after abnormal screening exams), or
PPV2 = TP/(TP+FP2).
*PPV3 (Biopsy done). The percentage of all screening mammography cases that result in a diagnosis of cancer based on biopsies performed. This is also known as the biopsy yield of malignancy, or the positive biopsy rate.
PPV3 = TP/(number of biopsies), or
PPV3 = TP/(TP+FP3).

Staging Cancers
AJCC Staging of Breast Cancers . . .
T . . .
N . . .
M . . .
is difficult w/o a mandatory regional tumor registry.

D. Eldridge, M.S. 37
Stage 0 Tis N0 M0
Stage 1 T1 N0 M0
Stage IIA T0 N1 M0
T1 N1 M0
T2 N0 M0
Stage IIB T2 N1 M0
T3 N0 M0
Stage IIIAT0 N2 M0
T1 N2 M0
T2 N2 M0
T3 N1 M0
T3 N2 M0
Stage IIIBT4 N0 M0
T4 N1 M0
T4 N2 M0
Stage IIICAny T N3 M0
Stage IV Any T Any N M1
American Joint Committee On Cancer (AJCC) Staging of Breast Cancer
revised: 1/1/03

D. Eldridge, M.S. 38
Tumor
T0: No evidence of primary tumor
Tis: Carcinoma in situ
T1: Tumor > 2 cm
T2: 2 cm < Tumor < 5 cm
T3: Tumor > 5 cm
T4: Tumor (any size) extending to Chest wall or Skin
Also: TX, Tis(CDIS), Tis(LCIS), Tis(Paget’s), T1mic, T1a, T1b, T1c, T4a, T4, T4c, T4d
Lymph Nodes
N0: No regional lymph node metastases
N1: Mets to ipsilateral axillary lymph nodes fixed or matted, or in clinically apparent ipsilateral internal mammography nodes in the absence of clinically evident axillary lymph node metastasis
N3: Mets in ipsilateral infraclaviculary lymph node(s) with or without axillary lymph node involvement, or in clinically apparent ipsilateral internal mammary lymph node(s) and in the presence of clinically evident axillary lymph node mets; or mets in ipsilateral SCLNs with or without axillary or internal mammary lymph node involvement;
Also: NX, N2a, N2b, N3a, N3b, N3cpNX, pN0, PN0(I-), PN0(I+), PN0(mol-), PN0(mol+), PN1, PN1mi, PN1a, PN1b, PN1c, pN2, pN2a, pN2b,pN3, pN3a, pN3b, pN3c
Metastasis
MX: Distant metastasis cannot be assessed
M0: No distant metastasis
M1: Distant metastasis

D. Eldridge, M.S. 39
In Situ Carcinomas
NOS (not otherwise specified)
Intraductal
Paget’s disease and intraductal
Invasive Carcinomas
NOS (not otherwise specified)
Ductal
Inflammatory
Medullary, NOS
Medullary with lymhoid stroma
Mucinous
Papillary
Tubular
Lobular
Paget’s disease and infiltrating
Undifferentiated
Squamous cell
Adenoid cystic
Secretory
Cribriform

EZ Staging

EZ Staging

D. Eldridge, M.S. 42
-
Nodes
Ca1
+
Nodes
Ca2
Nodes
not sampled
Ca3
< 1 cm.
-
Nodes
Ca4
+
Nodes
Ca5
Nodes
not sampled
Ca6
> 1 cm.
DCIS
-
Nodes
Ca7
+
Nodes
Ca8
Nodes
not sampled
Ca9
< 1 cm.
-
Nodes
Ca10
+
Nodes
Ca11
Nodes
not sampled
Ca12
> 1 cm.
Invasive Ca
Ductal/Lobular
MamtreeTM Malignant Code
1 0,1,2,3,4,5
2 0,1,2,3,4,5
3 0,1,2,3,4,5
4 0,1,2,3,4,5
5 0,1,2,3,4,5
6 0,1,2,3,4,5
7 0,1,2,3,4,5
8 0,1,2,3,4,5
9 0,1,2,3,4,5
10 0,1,2,3,4,5
11 0,1,2,3,4,5
12 0,1,2,3,4,5
Initial Category Malignancy Code CommentsPatient #
Breast Cancer

Mammography View Abbreviations

Assessment Category Meanings

http://breastscreening.cancer.gov/statistics/benchmarks/screening/
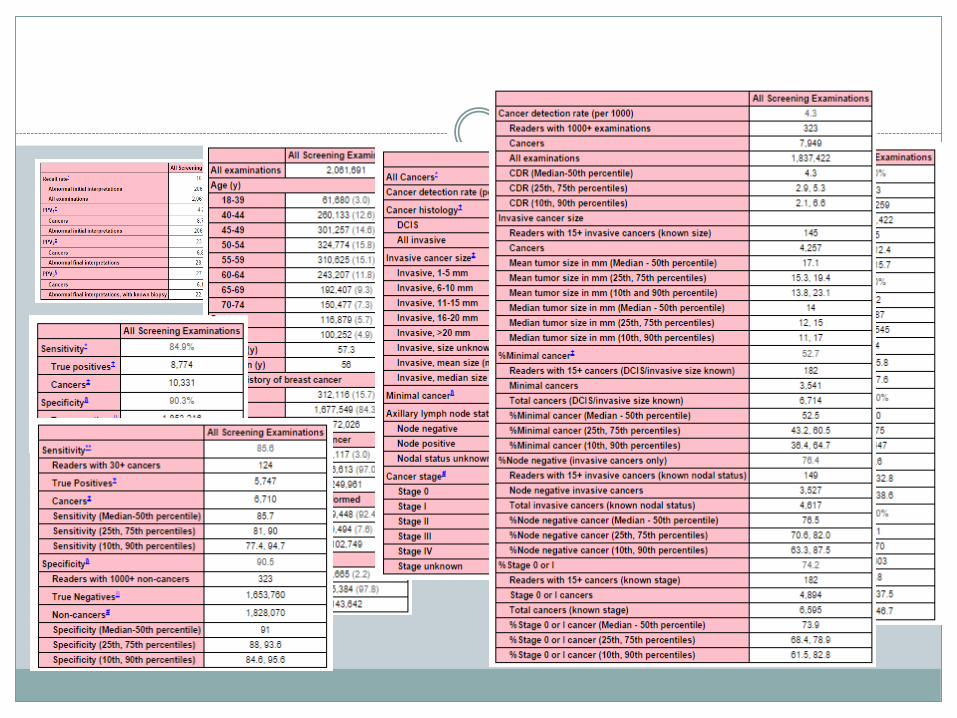

Cancer Detection Rate/Age
2009 BCSC Benchmarks
Cancer Detection Rate: 4.7/1000
Median size of invasive Ca: 14.0 mm
% Node-negative of invasive Ca: 77.3%
% Minimal Ca: 52.6%
Abnormal Recall Rate: 10.6%
PPV1 (abnormal interpretation): 4.4%
PPV2 (rec. for tissue diagnosis): 25.4%
PPV3 (biopsy performed): 31.0%
Sensitivity: 79.0%
Specificity: 89.8%

Large Facility

What does the Lead Radiologist Want?
However, before a “complete” audit system can beimplemented, patient confidentiality and protection ofmedical audit information from discovery must beinsured.
Current State peer review statutes protecting peer reviewactivities, such as collection of medical audit data, applyto inpatient facilities.
In many States, there is virtually no protection fromdiscovery of quality assurance activities in ambulatoryand outpatient settings, where most mammographyfacilities function.

Mammography Medical Outcomes Audit
MAMMOGRAPHY
We are performing a complex imaging procedure,
Mammograms are difficult to interpret, but
Patient follow-up might be the toughest part.

Mammography Medical Outcomes Audit
FOLLOW-UP
The mammography medical audit is a systematic collection and analysis of mammography results, which are compared with outcomes data. The result should help ensure quality mammography is done.

Mammography Medical Outcomes Audit
The MMOA relates technical and interpretive aspects of mammography performance to outcomes.

Mammography Medical Outcomes Audit
If done correctly, the audit will help.

Most Importantly…
Don’t “lose” a patient who has been recommended for biopsy.
Do the best you can.

The End
Thank you!
Duke Eldridge, M.S.
KansasRadiationPhysics.com