Embed Size (px)
Citation preview
145
MALIGNANT TUMOURS OF THE TESTISBy M. D. SNELLING, F.R.C.S., M.R.C.P., D.M.R., and D. M. T. CONES, D.M.R.T.
From the Meyerstein Institute of Radiotherapy, Middlesex Hospital
Malignant testicular tumours fall into two maingroups; seminoma, otherwise known as carcinomaor spermatocytoma, and teratoma, incorporatingthe more malignant and rapidly growing chorio-nepithelioma. Sertoli cell tumours are rare andinterstitial cell tumours are more commonly be-nign; secondary malignant tumours are rare, therebeing less than 50 reported cases in the literature.9We are most concerned here with seminoma andteratoma, and this article is based upon I66 casestreated and followed up at the Middlesex Hospitalbetween 1929 and i95I. Of these, 67 per cent.were seminoma and 33 per cent. teratoma. Thisfigure corresponds exactly with the series reportedby Gordon-Taylor and Wyndham,7 and althougha number of our cases are included in their seriesthey also included cases from other hospitals inLondon, the South-East of England and Australia.The percentage of seminoma is rather higherthan is usually given, figures varying from 59 percent. to 65 per cent. having been previouslyreported.
It is not within the scope of this article tocomment on the difference of opinion regardingthe histogenesis of seminoma, nor would we pre-sume to do so. Ewing6 has stated that seminomadoes not arise from seminal epithelium, but is anembryonal carcinoma arising in a teratoma.Willisl5 is equally definite in his theory thatseminoma arises from seminal epithelium and is aseparate entity from teratoma, and his argumentsare now widely accepted on both sides of theAtlantic.
Morbid AnatomyThe cut section of a seminoma of the testis
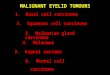
shows a soft opaque tumour, white or yellowish incolour, invading and destroying the body of thetestis. A thin layer of testicular tissue may berecognizable surrounding the tumour. Thetumour itself is structureless and homogeneous,sometimes with areas of haemorrhage and necrosis;fibrous trabeculae may sometimes be presentgiving a lobulated appearance (Fig. i).
Histologically, diffuse masses of large polygonalcells with a clear or finely granular cytoplasm are
FIG. I. Naked eye appearance of a seminoma.
seen, with a well-marked cell boundary and small,somewhat rounded, hyperchromatic nuclei withprominent acidophile nucleoli. These cells re-semble spermatocytes. In some cases the cells aresmall with large nuclei resembling spermatoblasts,and may give the appearance of lymphosarcoma.
C1
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
146 POSTGRADUATE MEDICAL JOURNAL March I952
'., '"I E #1,:__~.
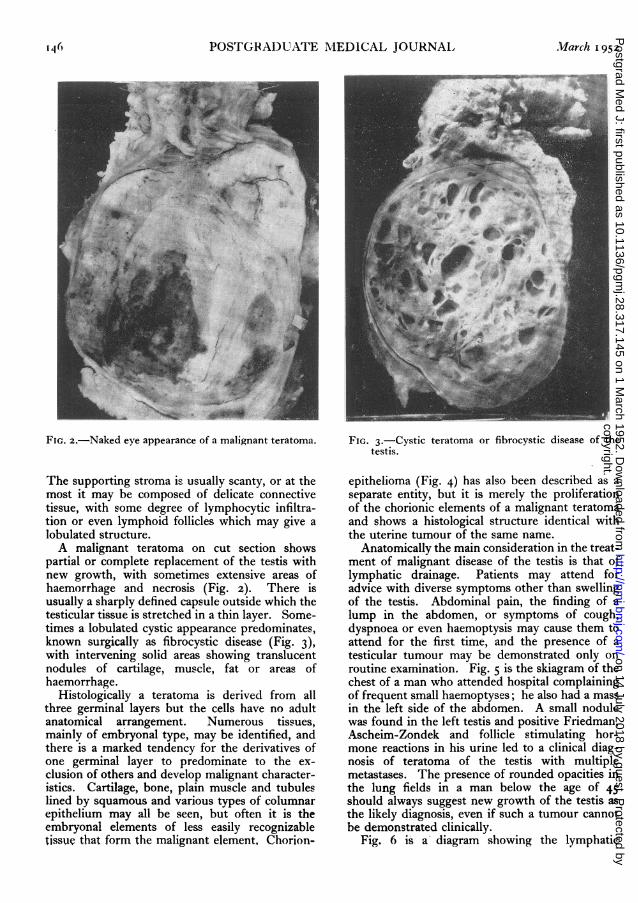
r11FIG. 2.-Naked eye appearance of a malignant teratoma.
The supporting stroma is usually scanty, or at themost it may be composed of delicate connectivetissue, with some degree of lymphocytic infiltra-tion or even lymphoid follicles which may give alobulated structure.A malignant teratoma on cut section shows
partial or complete replacement of the testis withnew growth, with sometimes extensive areas ofhaemorrhage and necrosis (Fig. 2). There isusually a sharply defined capsule outside which thetesticular tissue is stretched in a thin layer. Some-times a lobulated cystic appearance predominates,known surgically as fibrocystic disease (Fig. 3),with intervening solid areas showing translucentnodules of cartilage, muscle, fat or areas ofhaemorrhage.
Histologically a teratoma is derived from allthree germinal layers but the cells have no adultanatomical arrangement. Numerous tissues,mainly of embryonal type, may be identified, andthere is a marked tendency for the derivatives ofone germinal layer to predominate to the ex-clusion of others and develop malignant character-istics. Cartilage, bone, plain muscle and tubuleslined by squamous and various types of columnarepithelium may all be seen, but often it is theembryonal elements of less easily recognizabletissue that form the malignant element, Chorion-
FIG. 3.-Cystic teratoma or fibrocystic disease of thetestis.
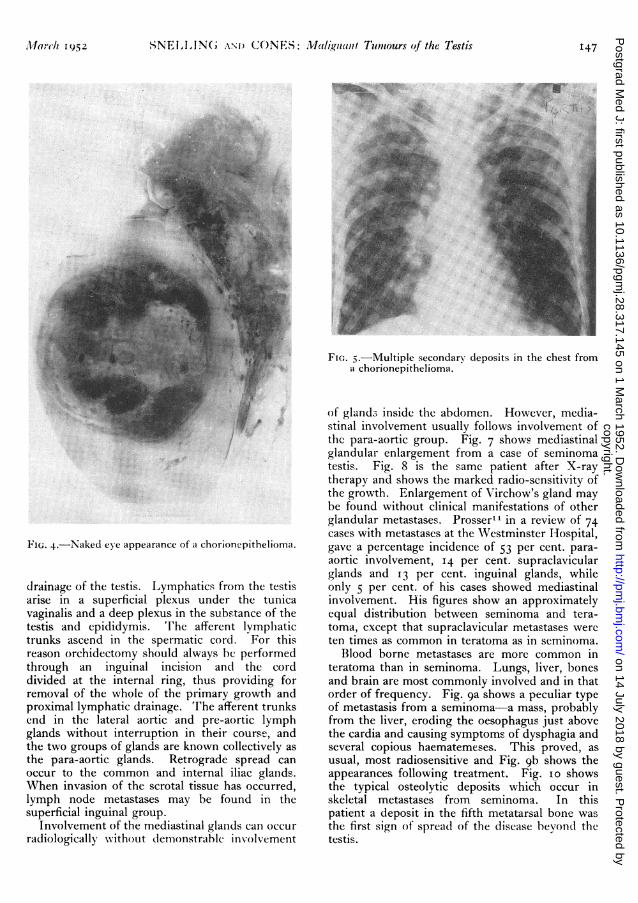
epithelioma (Fig. 4) has also been described as a
separate entity, but it is merely the proliferationof the chorionic elements of a malignant teratomaand shows a histological structure identical withthe uterine tumour of the same name.
Anatomically the main consideration in the treat-ment of malignant disease of the testis is that oflymphatic drainage. Patients may attend foradvice with diverse symptoms other than swellingof the testis. Abdominal pain, the finding of alump in the abdomen, or symptoms of cough,dyspnoea or even haemoptysis may cause them toattend for the first time, and the presence of atesticular tumour may be demonstrated only onroutine examination. Fig. 5 is the skiagram of thechest of a man who attended hospital complainingof frequent small haemoptyses; he also had a massin the left side of the abdomen. A small nodulewas found in the left testis and positive Friedman,Ascheim-Zondek and follicle stimulating hor-mone reactions in his urine led to a clinical diag-nosis of teratoma of the testis with multiplemetastases. The presence of rounded opacities inthe lung fields in a man below the age of 45should always suggest new growth of the testis asthe likely diagnosis, even if such a tumour cannotbe demonstrated clinically.
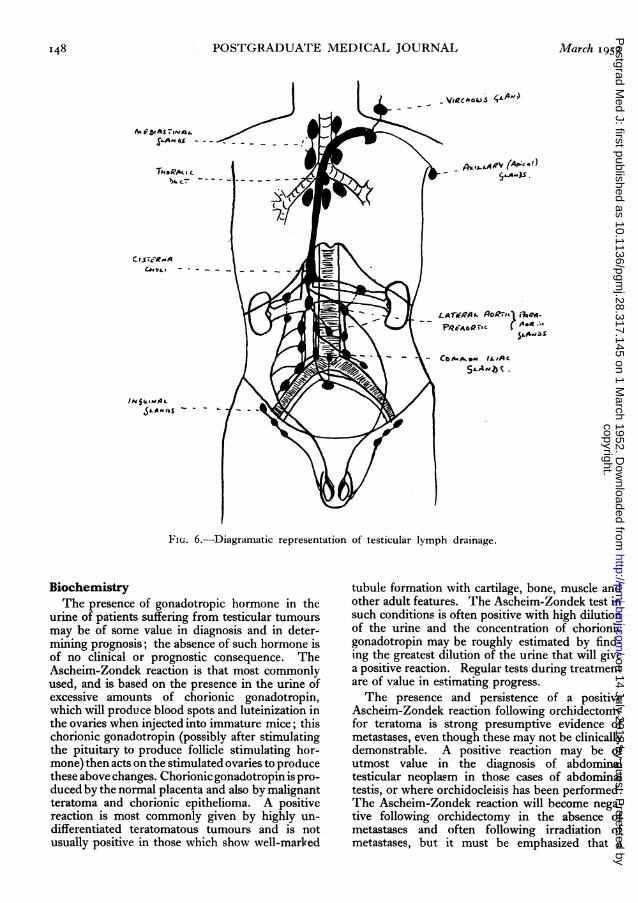
Fig. 6 is a diagram showing the lymphatic
ofthco ioni elmet .famlgattrtmand..hows .-..hitloia stucur ·dnia .....ith..
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
M1/arc]Th I952 SNE,I,IN(; A;N) CO'NES: Maligntaut Tumours of the Testis 147
:' ...........:i.:i!FIG. 4.-Naked eye appearance of a chorionepithelioma.
drainage of the testis. Lymphatics from the testisarise in a superficial plexus under the tunicavaginalis and a deep plexus in the substance of thetestis and epididymis. The afferent lymphatictrunks ascend in the spermatic cord. For thisreason orchidectomy should always be performedthrough an inguinal incision and the corddivided at the internal ring, thus providing forremoval of the whole of the primary growth andproximal lymphatic drainage. The afferent trunksend in the lateral aortic and pre-aortic lymphglands without interruption in their course, andthe two groups of glands are known collectively asthe para-aortic glands. Retrograde spread canoccur to the common and internal iliac glands.When invasion of the scrotal tissue has occurred,lymph node metastases may be found in thesuperficial inguinal group.
Involvement of the mediastinal glands can occurradiologically without demonstrable involvement
FIG. 5.-Multiple secondary deposits in the chest froma chorionepithelioma.
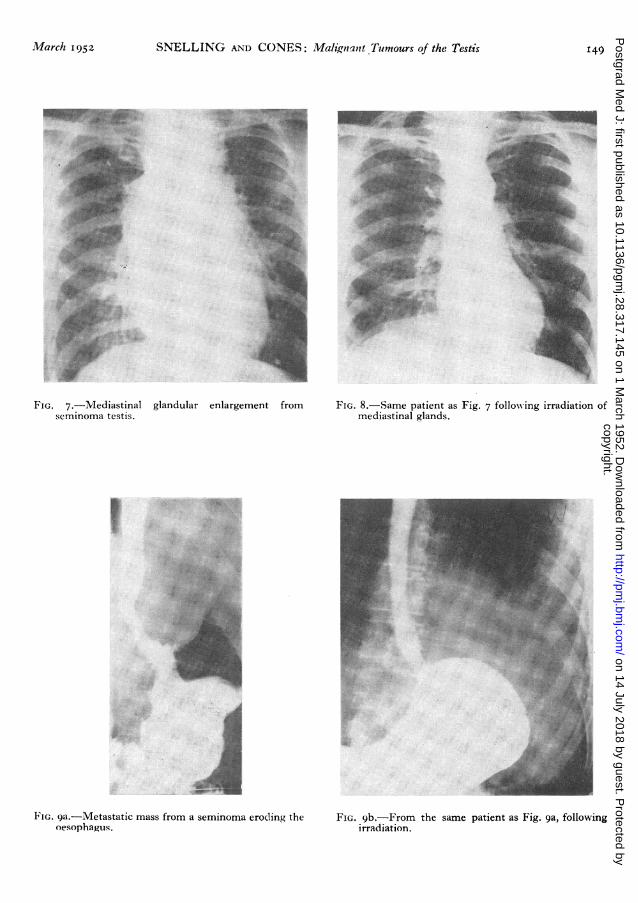
of gland, inside the abdomen. However, media-stinal involvement usually follows involvement ofthe para-aortic group. Fig. 7 shows mediastinalglandular enlargement from a case of seminomatestis. Fig. 8 is the same patient after X-raytherapy and shows the marked radio-sensitivity ofthe growth. Enlargement of Virchow's gland maybe found without clinical manifestations of otherglandular metastases. Prosserl4 in a review of 74cases with metastases at the Westminster Hospital,gave a percentage incidence of 53 per cent. para-aortic involvement, 14 per cent. supraclavicularglands and I3 per cent. inguinal glands, whileonly 5 per cent. of his cases showed mediastinalinvolvement. His figures show an approximatelyequal distribution between seminoma and tera-toma, except that supraclavicular metastases wereten times as common in teratoma as in seminoma.
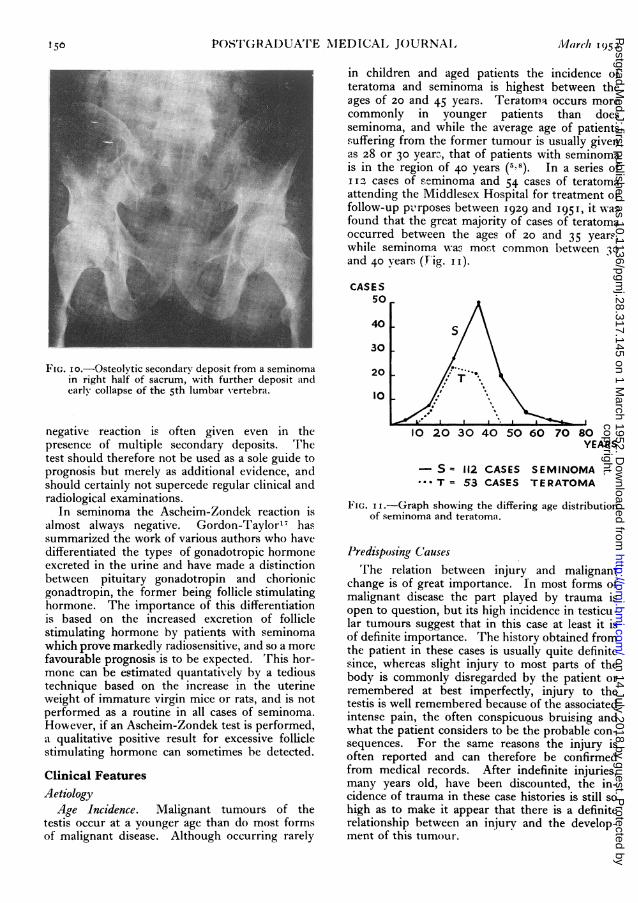
Blood borne metastases are more common interatoma than in seminoma. Lungs, liver, bonesand brain are most commonly involved and in thatorder of frequency. Fig. ga shows a peculiar typeof metastasis from a seminoma-a mass, probablyfrom the liver, eroding the oesophagus just abovethe cardia and causing symptoms of dysphagia andseveral copious haematemeses. This proved, asusual, most radiosensitive and Fig. 9b shows theappearances following treatment. Fig. io showsthe typical osteolytic deposits which occur inskeletal metastases from seminoma. In thispatient a deposit in the fifth metatarsal bone wasthe first sign of spread of the disease beyond thetestis.
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
148 POSTGRADUATE MEDICAL JOURNAL March 1952
Alcl - VrC ASoO )'A - -, - - -
.
N5kASL
. \D a t \r dr^a a e.C
F'IG. 6.-Diagramatic representation of testicular lymph drainage.
BiochemistryThe presence of gonadotropic hormone in the
urine of patients suffering from testicular tumoursmay be of some value in diagnosis and in deter-mining prognosis; the absence of such hormone isof no clinical or prognostic consequence. TheAscheim-Zondek reaction is that most commonlyused, and is based on the presence in the urine ofexcessive amounts of chorionic gonadotropin,which will produce blood spots and luteinization inthe ovaries when injected into immature mice; thischorionic gonadotropin (possibly after stimulatingthe pituitary to produce follicle stimulating hor-mone) then acts on the stimulated ovaries to producethese above changes. Chorionic gonadotropin is pro-duced by the normal placenta and also by malignantteratoma and chorionic epithelioma. A positivereaction is most commonly given by highly un-differentiated teratomatous tumours and is notusually positive in those which show well-marked
tubule formation with cartilage, bone, muscle andother adult features. The Ascheim-Zondek test insuch conditions is often positive with high dilutionof the urine and the concentration of chorionicgonadotropin may be roughly estimated by find-ing the greatest dilution of the urine that will givea positive reaction. Regular tests during treatmentare of value in estimating progress.The presence and persistence of a positive
Ascheim-Zondek reaction following orchidectomyfor teratoma is strong presumptive evidence ofmetastases, even though these may not be clinicallydemonstrable. A positive reaction may be ofutmost value in the diagnosis of abdominaltesticular neoplasm in those cases of abdominaltestis, or where orchidocleisis has been performed.The Ascheim-Zondek reaction will become nega-tive following orchidectomy in the absence ofmetastases and often following irradiation ofmetastases, but it must be emphasized that a
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
March I952 SNELLING AND CONES: MalignantTurmours of the Testis 149
FIG. 7.--Mediastinal glandular enlargement fromseminoma testis.
:ai,i,j
: I:^|. - *;; 3. .::Z ^^
.... .E
":!..~it.
...::
·. :
E'IG. 9a.--Metastatic mass from a seminoma erod!ing: the
oesophaus.....
:.'..:
;.s,.-: .' :. ·
.4 ,::.:" ..'::',...
Fit;. 9a.-Metastatic mass from a seminoma erocling theoesophagus.
FIG. 8.-Same patient as Fig. 7 following irradiation ofmediastinal glands.
FIG. gb.-From the same patient as Fig. 9a, followingirradiation.
:-:
irradliation .
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
156 POSTGRADUATE MEDICAL JOURNAL March 1952
FIG. io.-Osteolytic secondary deposit from a seminomain right half of sacrum, with further deposit andearly collapse of the 5th lumbar vertebra.
negative reaction is often given even in thepresence of multiple secondary deposits. Thetest should therefore not be used as a sole guide toprognosis but merely as additional evidence, andshould certainly not supercede regular clinical andradiological examinations.
In seminoma the Ascheim-Zondek reaction isalmost always negative. Gordon-Taylor,7 hassummarized the work of various authors who havedifferentiated the types of gonadotropic hormoneexcreted in the urine and have made a distinctionbetween pituitary gonadotropin and chorionicgonadtropin, the former being follicle stimulatinghormone. The importance of this differentiationis based on the increased excretion of folliclestimulating hormone by patients with seminomawhich prove markedly radiosensitive, and so a morefavourable prognosis is to be expected. This hor-mone can be estimated quantatively by a tedioustechnique based on the increase in the uterineweight of immature virgin mice or rats, and is notperformed as a routine in all cases of seminoma.However, if an Ascheim-Zondek test is performed,a qualitative positive result for excessive folliclestimulating hormone can sometimes be detected.
Clinical Features
AetiologyAge Incidence. Malignant tumours of the
testis occur at a younger age than do most formsof malignant disease. Although occurring rarely
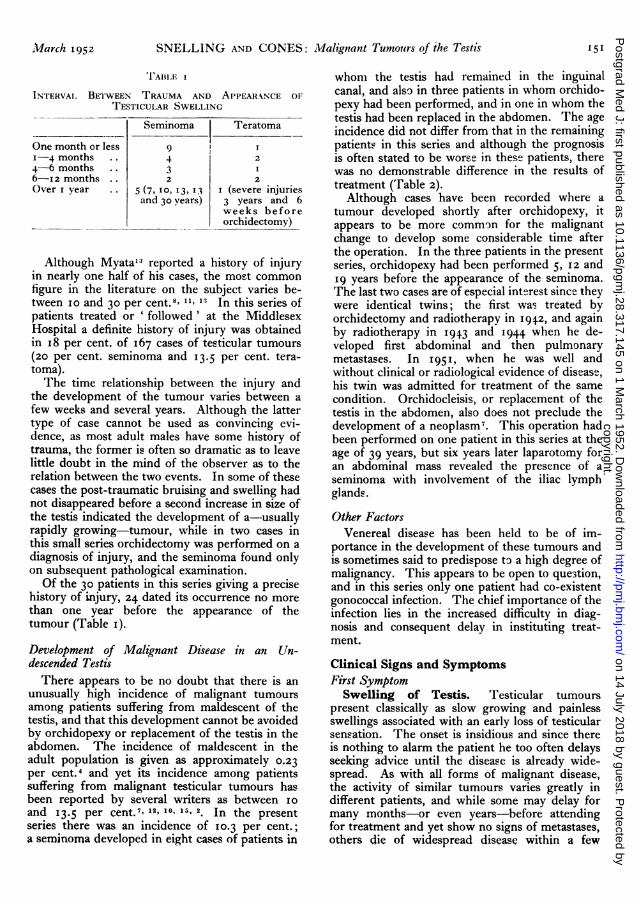
in children and aged patients the incidence ofteratoma and seminoma is highest between theages of 20 and 45 years. Teratoma occurs morecommonly in younger patients than doesseminoma, and while the average age of patientssuffering from the former tumour is usually givenas 28 or 30 years, that of patients with seminomais in the region of 40 years (5,8). In a series ofII2 cases of seminoma and 54 cases of teratomaattending the Middlesex Hospital for treatment orfollow-up pvrposes between I929 and I951, it wasfound that the great majority of cases of teratomaoccurred between the ages of 20 and 35 years,while seminoma was most common between 3oand 40 years (Fig. 1 ).CASES
50
40 s
30
2010' \
10 20 30 40 50 60 70 80YEARS
-S = 112 CASES SEMINOMA- T = 53 CASES TERATOMA
FIGe. I .-Graph showing the differing age distributionof seminoma and teratoma.
Predisposing CausesThe relation between injury and malignant
change is of great importance. In most forms ofmalignant disease the part played by trauma isopen to question, but its high incidence in testicu-lar tumours suggest that in this case at least it isof definite importance. The history obtained fromthe patient in these cases is usually quite definitesince, whereas slight injury to most parts of thebody is commonly disregarded by the patient orremembered at best imperfectly, injury to thetestis is well remembered because of the associatedintense pain, the often conspicuous bruising andwhat the patient considers to be the probable con-sequences. For the same reasons the injury isoften reported and can therefore be confirmedfrom medical records. After indefinite injuries,many years old, have been discounted, the in-cidence of trauma in these case histories is still sohigh as to make it appear that there is a definiterelationship between an injury and the develop-ment of this tumour.
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
iMarch 1952 SNELLING AND CONES: Malignant Tumours of the Testis 151
1TABIII 1
INTERVAI BETWEEN TRAUMA AND APPEARANCE OFTESTICULAR SWELLING
Seminoma Teratoma
One month or less 9 X1-4 months .. 4 24-6 months 3 I6-12 months . 2 2Over I year . 5 (71, i3, 13 I (severe injuries
and 30 years) 3 years and 6weeks beforeorchidectomy)
Although Myata13 reported a history of injuryin nearly one half of his cases, the most commonfigure in the literature on the subject varies be-tween io and 30 per cent.8, 11,' In this series ofpatients treated or ' followed' at the MiddlesexHospital a definite history of injury was obtainedin i8 per cent. of i67 cases of testicular tumours(20 per cent. seminoma and I3.5 per cent. tera-toma).The time relationship between the injury and
the development of the tumour varies between afew weeks and several years. Although the lattertype of case cannot be used as convincing evi-dence, as most adult males have some history oftrauma, the former is often so dramatic as to leavelittle doubt in the mind of the observer as to therelation between the two events. In some of thesecases the post-traumatic bruising and swelling hadnot disappeared before a second increase in size ofthe testis indicated the development of a-usuallyrapidly growing-tumour, while in two cases inthis small series orchidectomy was performed on adiagnosis of injury, and the seminoma found onlyon subsequent pathological examination.Of the 30 patients in this series giving a precise
history of injury, 24 dated its occurrence no morethan one year before the appearance of thetumour (Table i).Development of Malignant Disease in an Un-descended TestisThere appears to be no doubt that there is an
unusually high incidence of malignant tumoursamong patients suffering from maldescent of thetestis, and that this development cannot be avoidedby orchidopexy or replacement of the testis in theabdomen. The incidence of maldescent in theadult population is given as approximately 0.23per cent.4 and yet its incidence among patientssuffering from malignant testicular tumours hasbeen reported by several writers as between ioand 13.5 per cent.7' 12, 10, 1 2. In the presentseries there was an incidence of 10.3 per cent.;a seminoma developed in eight cases of patients in
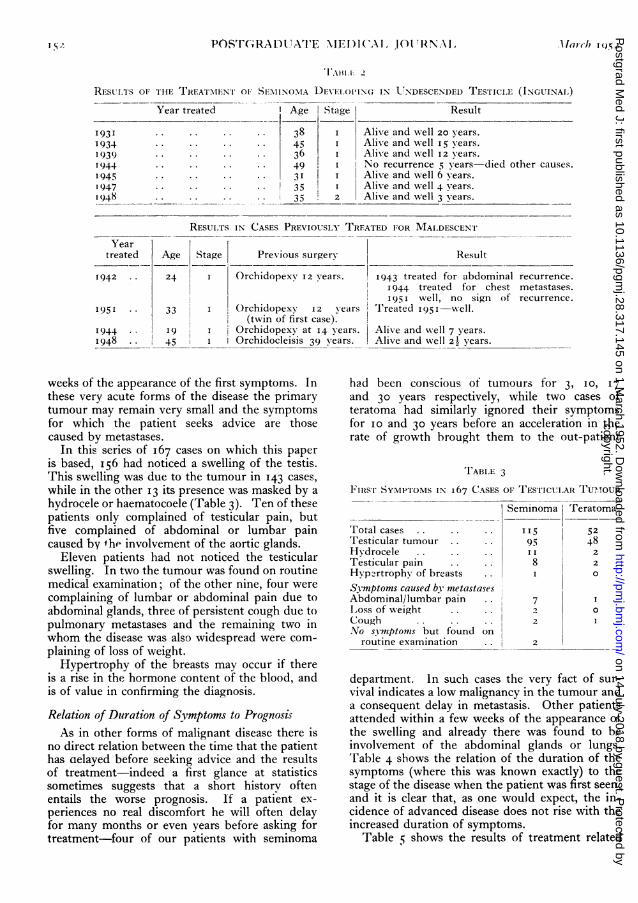
whom the testis had remained in the inguinalcanal, and also in three patients in whom orchido-pexy had been performed, and in one in whom thetestis had been replaced in the abdomen. The ageincidence did not differ from that in the remainingpatients in this series and although the prognosisis often stated to be worse in these patients, therewas no demonstrable difference in the results oftreatment (Table 2).Although cases have been recorded where a
tumour developed shortly after orchidopexy, itappears to be more common for the malignantchange to develop some considerable time afterthe operation. In the three patients in the presentseries, orchidopexy had been performed 5, I2 and19 years before the appearance of the seminoma.The last two cases are of especial interest since theywere identical twins; the first was treated byorchidectomy and radiotherapy in 1942, and againby radiotherapy in I943 and 1944 when he de-veloped first abdominal and then pulmonarymetastases. In I951, when he was well andwithout clinical or radiological evidence of disease,his twin was admitted for treatment of the samecondition. Orchidocleisis, or replacement of thetestis in the abdomen, also does not preclude thedevelopment of a neoplasm7. This operation hadbeen performed on one patient in this series at theage of 39 years, but six years later laparotomy foran abdominal mass revealed the presence of aseminoma with involvement of the iliac lymphglands.Other Factors
Venereal disease has been held to be of im-portance in the development of these tumours andis sometimes said to predispose to a high degree ofmalignancy. This appears to be open to question,and in this series only one patient had co-existentgonococcal infection. The chief importance of theinfection lies in the increased difficulty in diag-nosis and consequent delay in instituting treat-ment.
Clinical Signs and SymptomsFirst Symptom
Swelling of Testis. Testicular tumourspresent classically as slow growing and painlessswellings associated with an early loss of testicularsensation. The onset is insidious and since thereis nothing to alarm the patient he too often delaysseeking advice until the disease is already wide-spread. As with all forms of malignant disease,the activity of similar tumours varies greatly indifferent patients, and while some may delay formany months-or even years-before attendingfor treatment and yet show no signs of metastases,others die of widespread disease within a few
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
TI\AlI.I: 2
RESULTS OF THE TREATMENT OF SEMINOMA DEVEL)OPIN(G IN UNDESCENI)ED TESTICLE (INGUINAL)Year treated Age Stage Result
1931 . .. . . 38 I Alive and well 20 years.1934 . . 45 I Alive and well 15 years.1939 36 Alive and well 12 years.194 .. .. .. . 49 No recurrence 5 years-died other causes.1945 .. .. .. .. I Alive and well 6 years.1947 . . .. . 35 I Alive and well 4 years.1948 . . 35 2 Alive and well 3 years.
RESUITS IN CASES PREVIOUSLY TREATED FOR MALDESCENTYear
treated Age Stage Previous surgery Result
1942 .. 24 I Orchidopexy I2 years. 1943 treated for abdominal recurrence.1944 treated for chest metastases.! 951 well, no sign of recurrence.
1951 · · 33 ()rchidopexy 12 years T'Ireated I95I-well.(twin of first case).
1944 .. 9 Orchidopexy at 14 years. Alive and well 7 years.1948 . 45 Orchidocleisis 39 years. Alive and well 2z years.
weeks of the appearance of the first symptoms. Inthese very acute forms of the disease the primarytumour may remain very small and the symptomsfor which the patient seeks advice are thosecaused by metastases.
In this series of 167 cases on which this paperis based, I56 had noticed a swelling of the testis.This swelling was due to the tumour in 143 cases,while in the other 13 its presence was masked by ahydrocele or haematocoele (Table 3). Ten of thesepatients only complained of testicular pain, butfive complained of abdominal or lumbar paincaused by he involvement of the aortic glands.
Eleven patients had not noticed the testicularswelling. In two the tumour was found on routinemedical examination; of the other nine, four werecomplaining of lumbar or abdominal pain due toabdominal glands, three of persistent cough due topulmonary metastases and the remaining two inwhom the disease was also widespread were com-plaining of loss of weight.
Hypertrophy of the breasts may occur if thereis a rise in the hormone content of the blood, andis of value in confirming the diagnosis.Relation of Duration of Symptoms to PrognosisAs in other forms of malignant disease there is
no direct relation between the time that the patienthas celayed before seeking advice and the resultsof treatment-indeed a first glance at statisticssometimes suggests that a short history oftenentails the worse prognosis. If a patient ex-periences no real discomfort he will often delayfor many months or even years before asking fortreatment-four of our patients with seminoma
had been conscious of tumours for 3, 10, 17and 30 years respectively, while two cases ofteratoma had similarly ignored their symptomsfor io and 30 years before an acceleration in therate of growth brought them to the out-patient
TABLE 3
FIISTr SYMPTOMS IN 167 CASES OF TEST'ICUIARI TUM.OUR
Seminoma Teratoma
Total cases .. .. . 115 52Testicular tumour .. .. 95 48Hydrocele .. .. .. 2Testicular pain .. 8 2
Hyp2rtrophy of breasts .. 0oSymptoms caused by metastasesAbdominal/lumbar pain 7Loss of weight ...2 .Cough . .. 2 INo symptomss but found on
routine examination 2
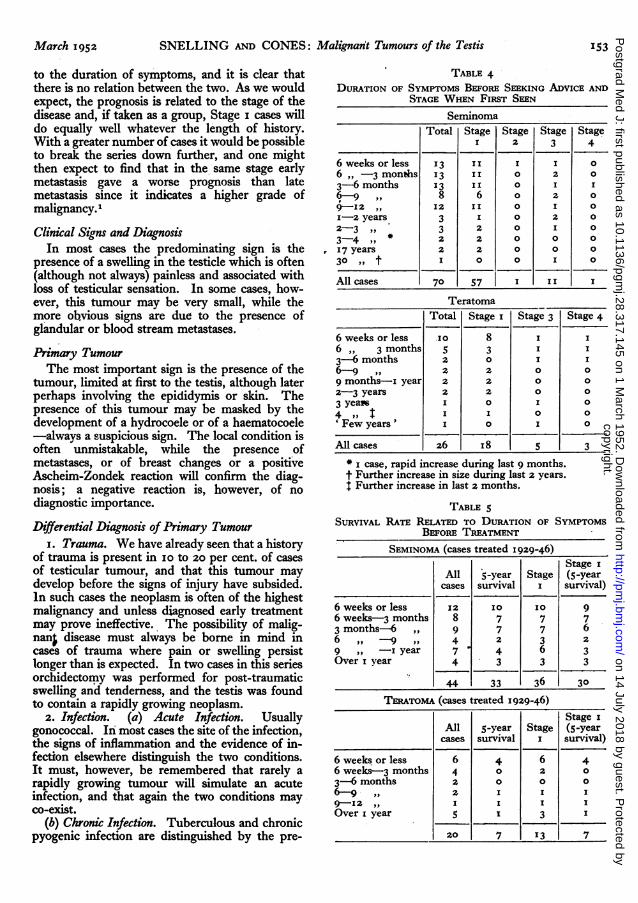
department. In such cases the very fact of sur-vival indicates a low malignancy in the tumour anda consequent delay in metastasis. Other patientsattended within a few weeks of the appearance ofthe swelling and already there was found to beinvolvement of the abdominal glands or lungs.Table 4 shows the relation of the duration of thesymptoms (where this was known exactly) to thestage of the disease when the patient was first seen,and it is clear that, as one would expect, the in-cidence of advanced disease does not rise with theincreased duration of symptoms.
Table 5 shows the results of treatment related
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
March 1952 SNELLING AND CONES: Malignant Tumours of the Testis53
to the duration of symptoms, and it is clear thatthere is no relation between the two. As we wouldexpect, the prognosis is related to the stage of thedisease and, if taken as a group, Stage I cases willdo equally well whatever the length of history.With a greater number of cases it would be possibleto break the series down further, and one mightthen expect to find that in the same stage earlymetastasis gave a worse prognosis than latemetastasis since it indicates a higher grade ofmalignancy.1Clinical Signs and Diagnosis
In most cases the predominating sign is thepresence of a swelling in the testicle which is often(although not always) painless and associated withloss of testicular sensation. In some cases, how-ever, this tumour may be very small, while themore obvious signs are due to the presence ofglandular or blood stream metastases.
Primary TumourThe most important sign is the presence of the
tumour, limited at first to the testis, although laterperhaps involving the epididymis or skin. Thepresence of this tumour may be masked by thedevelopment of a hydrocoele or of a haematocoele-always a suspicious sign. The local condition isoften unmistakable, while the presence ofmetastases, or of breast changes or a positiveAscheim-Zondek reaction will confirm the diag-nosis; a negative reaction is, however, of nodiagnostic importance.Differential Diagnosis of Primary Tumour
I. Trauma. We have already seen that a historyof trauma is present in 10 to 20 per cent. of casesof testicular tumour, and that this tumour maydevelop before the signs of injury have subsided.In such cases the neoplasm is often of the highestmalignancy and unless diagnosed early treatmentmay prove ineffective. The possibility of malig-nan; disease must always be borne in mind incases of trauma where pain or swelling persistlonger than is expected. In two cases in this seriesorchidectomy was performed for post-traumaticswelling and tenderness, and the testis was foundto contain a rapidly growing neoplasm.
2. Infection. (a) Acute Infection. Usuallygonococcal. In most cases the site of the infection,the signs of inflammation and the evidence of in-fection elsewhere distinguish the two conditions.It must, however, be remembered that rarely arapidly growing tumour will simulate an acuteinfection, and that again the two conditions mayco-exist.
(b) Chronic Infection. Tuberculous and chronicpyogenic infection are distinguished by the pre-
TABLE 4DURATION OF SYMPTOMS BEFORE SEEKING ADVICE AND
STAGE WHEN FIRST SEENSeminoma
Total Stage Stage Stage StageI 2 3 4
6 weeks or less 13 II I I O6 ,, -3 months 13 II o 2 o3-6 months 13 I o I6-9 ,, 8 6 o 29-12 ,, 12 II Ix-2 years 3 I O 2 o2-3 ,, 3 2 0 I 0
3-4 ,, 2 2 0 0 0
I7 years 2 2 0 0 0
30 ,, t I O O I O
All cases 70 57 I II I
TeratomaTotal Stage I Stage 3 Stage 4
6 weeks or less 10 8 i I6 ,, 3 months 5 3 I 1
3-6 months 2 0 I I6-9 ,, 2 2 0 0
9 months-i year 2 2 0 0
2-3 years 2 2 0 0
3 yeas I 0 I 0
4 ,, i I o o' Few years ' I I 0
All cases 26 I8 5 3* case, rapid increase during last 9 months.t Further increase in size during last 2 years.t Further increase in last 2 months.
TABLE 5SURVIVAL RATE RELATED TO DURATION OF SYMPTOMS
BEFORE TREATMENTSEMINOMA (cases treated 1929-46)
Stage IAll 5-year Stage (5-yearcases survival I survival)
6 weeks or less 12 10 10 96 weeks-3 months 8 7 7 73 months-6 ,, 9 7 7 66 ,, -9 ,, 4 2 3 2
9 ,, - year 7 4 6 3Over I year 4 3 3 3
44 33 36 30
TERATOMA (cases treated 1929-46)Stage i
All 5-year Stage (5-yearcases survival I survival)
6 weeks or less 6 4 6 46 weeks-3 months 4 o 2 0
3-6 months 2 0 0 0
6-9 , 2 I I I9-12 ,, I I I IOver I year 5 I 3 I
20 7 13 7
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
154 POSTGRADUATE MEDICAL JOURNAL March 1952
sence of epididymitis and other evidence of in-fection, although in some cases nodules due to aneoplasm may present a very similar appearance.
(c) Syphilis causes a painless, although usuallynodular, enlargement of the testicle which may beindistinguishable from an early neoplasm. Anegative Wasserman reaction is of importance indiagnosis-a positive one may be misleading.Clinical Signs Caused by Metastases
I. General Signs. Anorexia, loss of weight,etc., appear only when the disease is far advancedand multiple metastases are already present. Theyare, therefore, of little value in diagnosis.
2. Local Spread. In late cases there is infiltra-tion of the scrotal skin, sometimes associated withfungation. Spread up the cord is shown by theinvolvement of the lymphatics which may be onlyfound on microscopical examination, or may resultin thickening of the cord or the formation ofpalpable nodules.
3. Distant Lymphatic Spread. (a) AbdominalGlands. Lymphatics lead from the testes to thepre-aortic and lateral aortic glands below the renalvessels. These glands are therefore involved earlyin cases of testicular tumour, and an abdffminalmass was present in a fifth of the cases in thisseries. Such a mass may cause abdominal orlumbar pain or may, if large enough, produceobstructive symptoms suggesting a carcinoma ofthe colon or, by involving the ureter, cause firsthydronephrosis and later suppression of the func-tion of one or both kidneys. It is often verydifficult to palpate a glandular mass in the abdomenof a muscular young man, and examination underanaesthesia is always advisable in such cases, whilean intravenous pyelogram is also of value as aroutine mevsure.
(b) Involvement of Other Lymph Glands. Theiliac or pre-sacral glands may be directly involvedfrom the primary tumour, but such involvement israre unless the abdominal or inguinal glands arealready extensively involved. The inguinal glandsare also rarely affected unless the primary growthis very advanced and has extended through thecoverings of the testis, or in cases where thewound has been contaminated at operation and aresidual growth remains in the scrotum or inguinalregion.
(c) Changes in the Second Testicle. (i) A secondprimary growth is possible but is a rare oc-currence.7 (2) An advanced primary growth mayinvolve the second testicle by direct extension.(3) Following involvement of the abdominal lym-phatics, a secondary deposit may occur by retro-grade lymphatic spread to the contralateraltesticle. (4) In widespread disease blood streammetastasis may occur. (5) A varicocoele may de-
velop in the left testicle as a result of the presenceof a mass of abdominal glands.
(d) Extra-Abdominal Spread. (I) Lymphaticspread. There may be enlargement of the supra-clavicular or axillary glands, or X-rays may showmediastinal involvement. (2) Blood stream meta-stasis. The most common metastases occur in theparenchyma of the lungs where X-rays showmultiple rounded shadows (Fig. 5). Less com-monly deposits occur in the bones, subcutaneoustissues, liver and other organs.Treatment of Testicular TumoursGeneral Principles
In the present state of our knowledge malignantdisease, in most cases, can be cured only by thecomplete surgical removal of all malignant cells,or by their complete destruction by X-rays orby y-radiation. Treatment, therefore, depends onthe 'block' removal of the growth, efferent lym-phatics and involved glands together with a marginof normal tissue, or in the adequate irradiation ofthe same volume of tissue.. Since both seminomaand teratoma are very malignant growths whichtend to metastasize early, it must always be as-sumed that lymphatic spread has extended for atleast one stage beyond the area clinically involved.This means that treatment of an early neoplasmapparently localized to the testis includes removalor irradiation of the testicular lymphatics and ofthe abdominal lymph glands while, theoretically,if the abdominal glands are involved treatmentshould also be given to the mediastinum and tothe supraclavicular glands-in practice, as we shallsee, the volume of tissue to be irradiated islimited by the general reaction of the patient.Methods of Treatment AvailableThese tumours may be treated by surgery or by
radiotherapy alone, or by a combination of bothmethods. The method chosen depends on thestage of the disease, its surgical accessibility andoperability, the radiosensitivity of the neoplasmand on the general reaction of the patieit toirradiation.
i. Surgical Methods. Simple and Radical Or-chidectomy.
Simple orchidectomy is the treatment of choicefor the primary tumour. This operation shouldalways be performed through an inguinal incision,the cord should be divided at the internal ring andthe testis and cord should be removed in onepiece, care being taken to avoid contamination ofthe scrotum or wound with neoplastic cells. Thisminor operation provides the simplest and mostrapid method of treating the primary tumour andhas certain added advantages. The diagnosis is
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
March 1952 SNELLING AND CONES: Malignant Tumours of the Testis 155
thus completely established and from the histologyof the neoplasrm its radiosensitivity can bejudged-of importance in planning further treatment-andalso the prognosis of the patient. Providing thatremoval is complete, it also renders unnecessaryany subsequent irradiation of the scrotum itselfand therefore the risk of irradiating the remainingtestis and producing sterility.
Radical orchidectomy includes the removal of thelymphatics accompanying the testicular vein andof the regional pre-aortic and lateral aortic glands.This operation was not attended by a high mor-tality,9 but adequate dissection of the glands wasnot always possible. A great improvement in re-sults has been achieved by a combination of simpleorchidectomy with irradiation of the lymphaticsand of the inguinal, iliac and aortic glands withdeep X-rays, a procedure which has now sup-planted the radical operation. A case can still bemade for the use of this operation in the treatmentof early cases of radio-resistant teratoma, but ingeneral there is no doubt that the results of treat-ment have been greatly improved since theintroduction of the combined method as a routinetreatment.
RadiotherapyThe response to radiation varies greatly in
different tumours, and while a seminoma respondsquickly to radiation, some teratomata are more re-sistant. The amount of radiation which can begiven to any patient is limited by the generalreaction of the patient and the effect produced onthe normal tissues surrounding the neoplasticcells. The general reaction varies with site andthe total volume of tissue to be irradiated, and inthese cases this volume of tissue comprises a largeproportion of the abdomen, irradiation of whichusually tends to cause radiation ' sickfess.' Thevertebrae are also irradiated, the effect on themarrow sometimes producing a severe fall in thewhite cell count. These general reactions limit thetotal quantity of radiation which can be given andthe rate at which it is administered and are of fargreater importance than the reactions of thenormal tissue directly surrounding the tumourcells and of the skin. The effect of this generalreaction is such that although an adequate dosagecan be administered to destroy the radiosensitiveseminoma, we cannot deal so adequately with therelatively insensitive teratoma-a fact well illus-trated by the survival figures of the two diseases.
This general reaction also limits our treatmentof Stage 3 cases where, theoretically, mediastinaland supraclavicular glands should also be ir-radiated. In practice the general reaction makes itimpossible to administer an adequate quantity ofradiation to all areas and it is therefore our usual
practice to irradiate the abdomen to a satisfactorilyhigh dosage and to give further treatment onlyshould signs of recurrence appear elsewhere.
Patients may not attend for treatment untilmetastases are already present in the lungs. Insuch cases treatment must be given to the wholetrunk and the general reaction following the ir-radiation of such a large volume limits the dosageseverely. Even so, there are occasional caseswhere the radiosensitivity is so great that all lesionswill disappear-at least for many months or evenyears-and therefore treatment should be in-stituted with a view to ascertaining the radio-sensitivity of the tumour and so of identifying thepatients who can still be benefited. In other caseslung metastases develop months or years after thecompletion of the first treatment. In such casesonly the chest requires treatment and the generalreaction is therefore less severe and a moreadequate dosage can be employed. In this seriesalone three patients suffering from seminoma arewell and without clinical or radiological evidenceof metastases several years after the treatment ofmultiple pulmonary metastases. The results interatoma are far less encouraging, but here againa trial should be made of the radiosensitivity of thelesion before deciding that all treatment must beabandoned. The following combinations of treat-ment is used in different stages of the disease:-
Stage i.-Limited to testis. Orchidectomy,with division of cord at internal ring, followed bydeep X-ray treatment to inguinal wound andglands, iliac glands and aortic glands up to thelevel of the diaphragm.
Stage Ia.-Patients in whom there is residualneoplasm in the scrotum following orchidectomy.As Stage i, but with the addition of irradiation ofthe affected side of the scrotum, the contralateraltestis being shielded as much as possible.
Stage 2.-Involvement of inguinal or iliacglands. As Stage I.
Stage 3.-Patients with clinical involvement ofthe abdominal glands. As Stage i but followed ifpossible by irradiation of the mediastinum andsupraclavicular glands (rarely possible owing togeneral reactions).
Stage 4.-Distant metastases by lymphatics orblood stream. (a) ' Curative' method of irradia-tion of whole of tissue involved, i.e. whole trunk(rarely possible). (b) 'Palliative' irradiation ofmetastases producing symptoms.Results of TreatmentThe results of the treatment of testicular
tumours improved greatly following the intro-duction of the combination of surgery and deepX-ray treatment. The results of treatment de-pend on the type of tumour, its malignancy and
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from
156 POSTGRADUATE MEDICAL JOURNAL March 1952
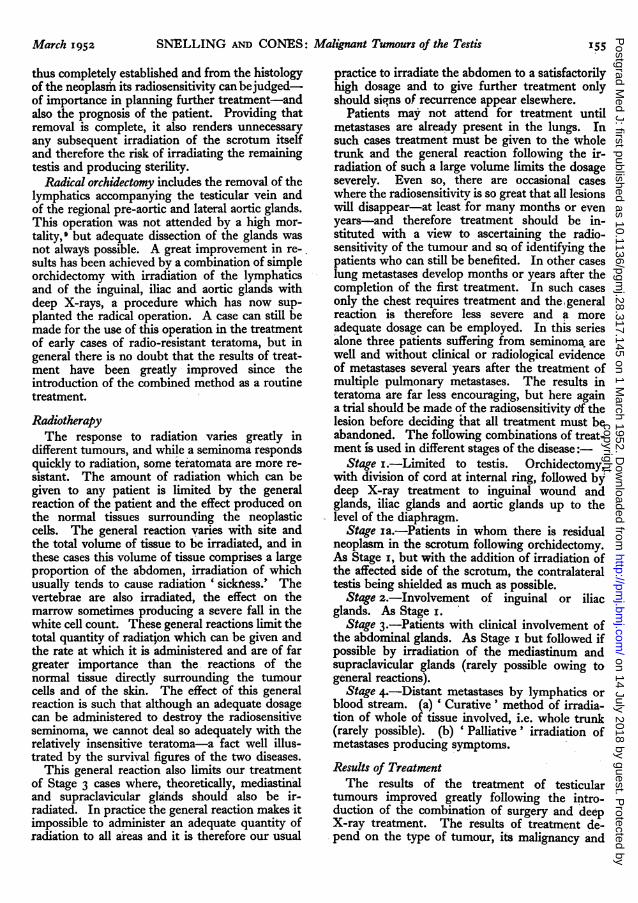
TABLE 6RESULTS OF' TREATMENT OF SEMINOMA AND TERATOMA
All new cases treated I929-50Stage I .. Disease limited to testis.Stage 2 .. Involvement of inguinal/iliac glands.Stage 3 .. Involvement of aortic glands.Stage 4 .. Distant metastases.
Stage Stage StageTotal Stage I 2 3 4
Seminoma I07 87 (8I.3%) 4 10 6Teratoma 53 39 (73.6%) o 7 7
TABLE 7RESULTS OF TREATMENT 1929-48
SURVIVALI o-year 5-year 3-year
1 (1929-41) (I929-46) (x929-48)Seminoma
Allcases 2I1/38 (55.3 %) 52/77 (67.5%) t66/92 (71.7%)Stage I 21/29 (72.4%) 49/6I (8o.3%) 60/73 (82.2%)Stage z 0/2 1/3 2/4Stage 3 0/4 I/7 3/9Stage 4 o/3 I/6 /6
TeratomaAllcases 3/18(I6.7%) II/39(28.2%) 15/44(34.I%)Stage I 2/13 10/28(35.7%) 13/31 (41.9%)Stage 2 - ---Stage 3 i/3 I/6 2/7Stage 4 0/2 0/5 o/6
* 2 cases lost to follow-up.t 3 cases lost to follow-up.
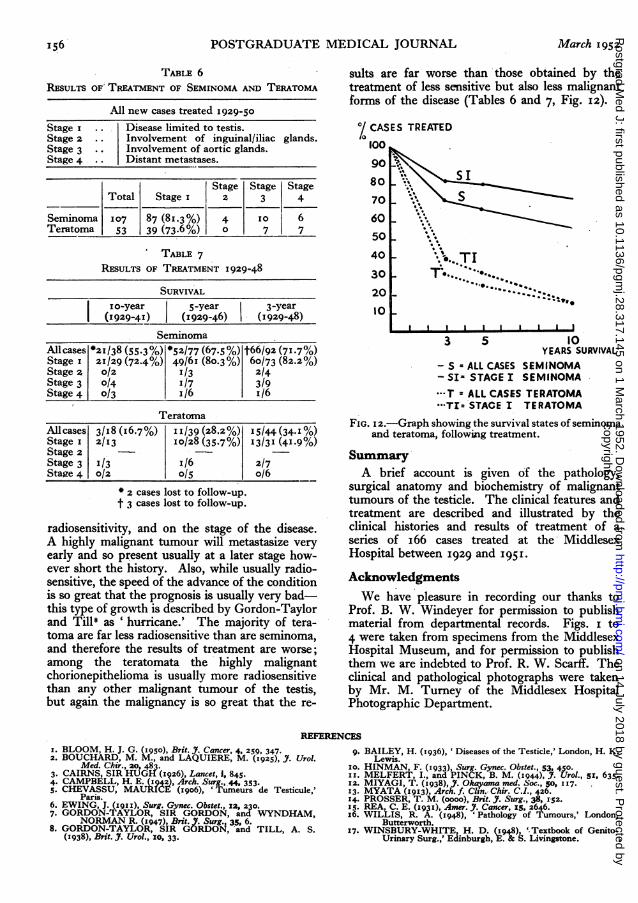
radiosensitivity, and on the stage of the disease.A highly malignant tumour will metastasize veryearly and so present usually at a later stage how-ever short the history. Also, while usually radio-sensitive, the speed of the advance of the conditionis so great that the prognosis is usually very bad-this type of growth is described by Gordon-Taylorand Till8 as 'hurricane.' The majority of tera-toma are far less radiosensitive than are seminoma,and therefore the results of treatment are worse;among the teratomata the highly malignantchorionepithelioma is usually more radiosensitivethan any other malignant tumour of the testis,but again the malignancy is so great that the re-
suits are far worse than those obtained by thetreatment of less sensitive but also less malignantforms of the disease (Tables 6 and 7, Fig. I2).
°/ CASES TREATED100
9O8070 S6050 \
'"'...40 ... TI
30 T.20- :..10
I I I I I I I I I I
3 5 10YEARS SURVIVAL
- S a ALL CASES SEMINOMA- SI- STAGE I SEMINOMA--T = ALL CASES TERATOMA·-*TI= STAGE I TERATOMA
FIG. I2.-Graph showing the survival states of seminomaand teratoma, following treatment.
SummaryA brief account is given of the pathology,
surgical anatomy and biochemistry of malignanttumours of the testicle. The clinical features andtreatment are described and illustrated by theclinical histories and results of treatment of aseries of i66 cases treated at the MiddlesexHospital between 1929 and I95 .
AcknowledgmentsWe have pleasure in recording our thanks to
Prof. B. W. Windeyer for permission to publishmaterial from departmental records. Figs. i to4 were taken from specimens from the MiddlesexHospital Museum, and for permission to publishthem we are indebted to Prof. R. W. Scarff. Theclinical and pathological photographs were takenby Mr. M. Turey of the Middlesex HospitalPhotographic Department.
REFERENCESx. BLOOM, H. J. G. (1950), Brit. J. Cancer, 4, 259, 347.2. BOUCHARD, M. M., and LAQUIERE, M. (1925), J. Urol.
Med. Chir., 20, 483.3. CAIRNS, SIR HUGH (1926), Lancet, 1, 845.4. CAMPBELL, H. E. (1942), Arch. Surg., 44, 353.5. CHEVASSU, MAURICE (1906), 'Tumeurs de Testicule,'Paris.6. EWING, J. (1911), Surg. Gynec. Obstet., x2, 230.7. GORDON-TAYLOR, SIR GORDON, and WYNDHAM,NORMAN R. (I947), Brit. Y. Surg., 35. 6.8. GORDON-TAYLOR, SIR GORDON, and TILL, A. S.
(1938), Brit. J. Urol., i0, 33.
9. BAILEY, H. (I936), ' Diseases of the Testicle,' London, H. K.Lewis.
xo. HINMAN, F. (933), Surg. Gynec. Obstet., 53, 450.xx. MELFERT, I., and PINCK, B. M. (944), . Urol., 5s, 635.12. MIYAGI, T. (1938), J. Okayama med. Soc., 50, 117.13. MYATA (x913), Arch. f. Clsn. Chir. C.I., 426.14. PROSSER, T. M. (oooo), Brit. J. Surg., 38, 152.I5. REA, C. E. (I931), Amer. J. Cancer, IS. 2646.x6. WILLIS, R. A. (I948), 'Pathology of Tumours,' London,
Butterworth.17. WINSBURY-WHITE, H. D. (1948), 'Textbook of Genito-
Urinary Surg.,' Edinburgh, E. & S. Livingstone.
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.317.145 on 1 March 1952. D
ownloaded from






![Malignant mesothelioma of the tunica vaginalis testis: a ...testis. Mesothelioma of the tunica vaginalis testis repre-sent only 0.3–5% of all mesothelial neoplasms [7]. Ac-cording](https://img.pdfslide.us/doc/110x75/60ab9ecd88f9ad6c0664e638/malignant-mesothelioma-of-the-tunica-vaginalis-testis-a-testis-mesothelioma.jpg)
![Malignant tumours of temporomandibular joint · 2020. 10. 6. · Temporomandibular joint (TMJ) disorders are very common and can be easily diagnosed [1, 2]. However, malignant tumours](https://img.pdfslide.us/doc/110x75/609cf658aa942f17d538f23e/malignant-tumours-of-temporomandibular-joint-2020-10-6-temporomandibular-joint.jpg)