Embed Size (px)
Citation preview

_ SPECIAL PATIENT CARE--=-=- """-=-;;;?P-:0. /n~/5-U'''*/7;;~'HCREDIT
Malignant hyperthermia and its implicationsin general dentistryErik F. Reifenstahl, DMD • Henry H. Rowshan, DDS
Malignant hyperthermia (MH) is an uncommon and potentially lif..threatening pharmacogenetic disorder. This abnormality in musclemetabolism can be triggered by avariety of agents (particularlygeneral anesthetics and stress), resulting in a rapid heart rateincrease, muscle rigidity, acidosis, temperature elevation, rhab~
domyolysi~ and renal failure. Immediate discontinuing of triggeringagents, oxygenation, cooling, and dantrolene are necessary totreat an episode. MH·susceptible patients often indicate apositive
family history of experiencing an adverse event during anesthesia,Few diagnostic tests are available to screen patients; the mostaccurate test is a skeletal muscle biopsy. MH'susceptible patientscan undergo surgical procedures as necessary. Careful explorationof the medical history will allow the clinician to make the necessarymodifications to treat and manage an episode expedientty.
Received: June 10, 2008Accepted: July 10, 2008
First teported in 1900 as hyper.pyrexia (an extreme devationin body temperature as a
reaction to anesthesia), malignanthyperthetmia (MH) is characterizedby a hypetcatabolic teaction in themuscles ofgenetically susceptibleindividuals, induced by certain drugsOt by physical Ot emotional sttCss.\ Atthe dental office, an MH-susttptiblepatient exposed to excessive stresses(such as pain, rear, Ot othet triggering agents) may exhibit signs·andsymptoms of MH.' Dentists must beaware ofthe disease's pathophysiology to'prepare fot, and hopefullyprevent, an MH episode.
The cs(imatcd incidence ofMH is 1:15,000 fot children and1:50,000 fot adults.' It OCCUlS motefrequently between the ages 60and 30 and is predominant in men.3
When MH was first recogni7..ed a.~
a complication of anesthesia, itsmortality rate was 70%; however.a 2003 article reported that diagnostic testing. increased awarenessofthe condition, and the use ofappropriate treatment medicationshad loweted the mortality rate roapproximately 5%.'
MH has an autosomal dominant
inheritance. The gene responsiblefOt MH is located on the long armofchromosome 19.5 More than40 mutations have been found inthe gene encoding fot the skeletalmuscle calcium telease channel,known as the ryanodine receptor(RYRJ).' These mutations allowan abnormal response to triggeringagents, tesulting in MH.
A triggering agent has an abnormaleffect on the skeletal muscles of asusceptible patient, as calcium ionconcentration rises suddenly withinthe sarcoplasmic teticulum ofskeletalmuscles, resulting in muscle oontrac~
tion.' Subsequent tigidity indicatesdepletion ofadenosine triphosphate(ATP) stOtes, which are crucial fOtthe ceuptake ofcalcium and tevelSingme condition. The disruption ofcellular membranes allows potas·siwn. calcium. creatine kinase, andmyoglobin to enret extracellularfluid, n:sulting in metabolic acidosis,myoglobinuria. and disseminatedintravasculat coagulation (DIe). Ifuntreated, MH could result in organf.illure and death.'
A review of me literature usingMEDLINE reveals sevetal casesofMH related to dental treat-
ment. A 2006 article by Noguchiet al desctibed a case offatalMH in which a J2-yeat-old boywith cetebtal palsy experiencedextreme stress during the appointment. The patient wa.~ con~ciOlL<j:
during the appointment and wasadministeted 0.5 mL oflidocaineprior to the extraction of a primarymolar. Muscle spasms occurredshortly afret the ptoceduue. Dentalanesthesiologists administeredoxygen, intravenous diazepam,and diclofenac and transfetredthe patient to a general hospital.Despite additional treatment(including heparin, dantrolene, andblood transfusions), the parient'scondition deteriorated over the next13 days, resulting in thabdomyolysis, DIe, and multiple organfailure.'
In 2005, a 5-year-<>ld boyexpetienced MH duting a closedreduction procedure to (feat amandihular fracture. The hoy hada histoty of uneventful genetalanesthesia and no famJly history ofMH. Anesthesia was obtained usinginhalational halothane and nItrousoxide; at rhat point, 20 mg of intravenous lidocaine was administered
242 MaylJune 2009 General Dentistry www.agd.org

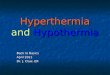
Sarcnplasmic reticulum
RYRI
, _, 'iJM~ action potential propag;rted
i,!i ..
~Ca" released into cytosol
~Ca" triggers binding of cross bridgee: I I
Ca"
0Filamentsslide +Ca2+
~in filament) ,
Fig. 1. Adiagram of the steps within a muscle cell leading to MH.
and nitrous oxide was discontinued.Surgeons administered 7.2 mL of2% lidocaine locally and proceededwith arehOOr placement. Theprocedure was stopped once thesymptoms of muscle rigidity, hypercarbia, taehypnea, and tachycardiawere recognized.. The incident wasmanaged successfully by stoppingthe rriggering agent, administeringdantrolene, and applying coolingmeasures, including placing icepacks in the axillary and groin areas,switehing co ice-cold IV fluids, andcold ga.~[Tic lavage. The patient wa.~
transferred to a local hospital, whetehis symptoms resolved overnight.8
Inads et al reported the case ofan II-year-<>Id girl who underwentan alveolar eleft bone graft undergeneral anesthesia. which resulted inpersistent hyperthermia that lastedfor five days postoperatively. Thepatient had undergone general anes~
thesia befOre without any complication. In this case, anesthesia wasinduced with the rapidly acring gen-
eral anesthetic propofol followed bythe non-depolarizing neuromuscularblocking agent vecuronium bromideand maintained with nitrous oxide.Local anesthesia at surgical sites wasobtained using 16.5 mLofl% lidocaine with 1:100,000 epinephrineand 25 mL of 1% lidocaine withoutepinephrine. Attempts to managethe hypenhermia with the NSA/Ddiclofenac were unsuccessful; theepisode was resolved by using oraldantrolene.'
Monaghan and Hindle presented acase involving a 30-year-<>ld womanwith a history ofsuccessful genetalanesthesia who experienced MHonc hour into an orthognathic surgical procedure. The surgeons firstrecognized tachycardia, warmth ofthe skin, and cyanotic appearance ofthe blood. The patient was managedsuccessfully through cooling and theadministration ofdantrolene. 1O
Nitrous oxide was implicatedas the triggering agent in a 1985report in whieh a 15-year-old boy
with cerebral palsy and a historysignificant for MH experienced thecondition during dental treatment,despite being premedicated withdantrolene when nitrous oxide wasutilized. Anesthesia was uneventfulat a subsequent appointment whenthe same premedication protocolswere utUi.zed and nitrous oxide wasnot administered. ll
Choung described a postoperativevariant ofMH termed human stress.ryndrome."Characterized by motesubtle manifestations ofMH without any extreme elevation in bodytemperature, human stress syndromecan result from exposure to physicalor emotional stress outside a medicalsetting. Choung reponed the case ofa 17-ycar-<>ld boy with no sigrlificanthistoty who underwent onhognathicsurgery. Postoperatively, his temperature was slightly elevated and anelectrocardiogram (ECG) showedT-wave inversiom. The patient complained only ofgeneralized musclesoreness. His condition resolved
www.agd.org General Dentistry May/June 2009 243

SPECIAL PATIENT CARE Malignant hyperthermia in general dentistry
Table 1. Drug therapy andmalignant hyperthermia.-4
Trigger agents
Depolarizing muscle relaxants(succinylcholine)
Volatile anestheticagentsHalothane
Isoflurane
Enflurane
Sevoflurane
Methoxyflurane
Des:flurane
Safe agents
Non-depolarizing musde relaxants
Nitrous oxide"Intravenous anesthetks
Ketamine
PropofolEtomidate
Thiopental
Vasopressors
local anesthetics"
Opiates
BMZOdiazep;nes
Barmturates
*Have_betn implicated In triggering MH
in 48 hoU!1i; further questioningrevealed that the patient experieneedfrequent muscle cramps during timesofemotional srress.12
Pathophysiology of diseaseIn MH-susceptible people, theRYRl is in a more open resting state(greatly reducing the calcium ionbonding capaci<y) and the intracellular calcium ion release rate is threetimes greater man in a normalindividual. The devated cytoplasmiccalcium concentration results incontinued interaction betweenactin and myosin filaments. withsustained contracture. Biochemicalpathways are activated to reuptake
the calcium, without suca:ss. Theresult is a breakdown ofATp, lacticacidosis, hypercarbia, and hyper~
thermia.' The pathway that !<:ads toMH is depicted in Figure I.
Tachycardia is the most consistentearly sign ofMH. An unexplainedincrease in end-tidal carbon dioxidelevels is a sensitive indicator ofMH.' Generalized erythema and anincreased respiratory rate often areobserved. Muscle rigidi<y develops(usually noted first in the massetermuscles) and will vary in terms oftime ofonset and severity, depend~ing on the trigger agent. Biochemical changes include acidosis and anincrease in levels ofserwn potassium, phosphate, and creatine phosphokinase (CPK) due to lactic acidproduction and muscle breakdown.Patients often will experience severemuscle soreness for several days afteran MH crisis.13
Several trigger agents (see Table 1)have been identified in MH. Triggeragents that are bdieved to beresponsible for a majority ofthecases include the depolarizingmuscle relaxant succinylcholine andthe volatile anesthetic agent halothane.2 Nitrous oxide and amidelocal anesthetics also have beenimplicated. in MH.6,1I.,,, Though
some believe nitrous oxide to be atrigger of MH, its frequent use asan anesthetic agent with susceptiblepatients would seem to discountthis theory. I As nitrous oxide hasgeneral anesthetic properties, it isappropriate to use it with cautionfor patients with personal or familyhistories ofMH. 15,[6 Contraindica~
tion fut the use of amide localanesthetics is based on in vitromuscle contracture studies.6 Amideanesthetics have been demonstratedto cawe muscle contraction, whileester anesthetics caused relaxationof muscle tissue. which inhibitscontracture.J,6.lJ Reviews of the
literature have not demonstrateda clear link between amide anesthetics and MH and it generallyis accepted that amide anesthetics are safe ror MH-susceptiblepatients.6.17.18
DiscussionIt is essential fur dentists to identifYa patient's susceptibility to MH priorto treatment. MH may occur outside the operating room and resultfrom factors untelated to drugs,either emotional (excitement andstress) or physical (mild infections,vigorous exercise, and elevated. environmental temperatures).19 Patientswith a significant p<:fsonal or familyanesthetic history may be susceptibleto MH. In addition, patienrs witha musculoskeletal disorder (suchas myotonia congenita, myotonicdysttophy, joint hypermobility,ptosis, squint, thoracic kyphosis,lumbar lordosis, or scoliosis), with orwithout a history of MH, must besuspected for the condition. t~
MH is a genetic condition; as aresult, a careful examination ofthepatient's medical history and f.unilyhisto<y (particularly where anesthesia is concerned) is revealing. In twoof the case reports described above.details concerning significant familyhistory were revealed only alter thefact. 9,10 Most episodes occur on the
patient's first exposure to triggeragents; however, a personal historyof uneventful general anesthesiadoes not rule out the possibility ofan MH crisis occurring.2
•10
There are few simple diagnostictests [0 identifY an MH-susceptiblepanent. 20 Muscle biopsies withcontraction studies are needed todefinitivdy diagnose MH.!' Thisprocedure begins by talting a biopsyofapproximately 2 g of muscletissue from the vastus lateralisor medialis. The muscle tissue isexposed to caffeine or halothane
244 May/June 2009 General Dentistry www.agd.org

Table 2. Patient assessment for MH.3
Athorough medical history. to include family history with anesthesia, is essential
Apositive diagnosis can be:Unequivocally posItive based on apositive muscle biopsy, or aconfirmed reaction in thepatient or immediate family member
EqujllOcaHy posItive based on afamily history of unexplained death from generalanesthesia, positive CPI( blood test, or if patient has central core disease. Duchennemuscular dystrophy, myoadenyfate deaminase deficiency, other myopathies, or heat stroKe
Consider degree of anticipated stress at appointment Astressful appointment can bedefined as:
Arry treatment on an apprehensive patient
Aprolonged or.extensive appointment
Atraumatic surgical procedure
Based on degree of susceptibility to MH and stress, the clinldan should make necessarymodification.> to treatment
and the force of muscle contractureis measured. This (esc: has a currenc:sensitivity of 97-99% and specificity of85--90%.' This tcst cum:ndyis available in eight medical centersin the U.S. and Canada."
Molecular genetic diagnosticshold great promise lOr a noninvasive diagnostic test that is highlyreproducible and requires minimalbiological material. As mutationsin the gene encoding the calciumrelease gene in skeletal muscle havebeen described as causal for MH,guidelines have been developed lOrclinical molecular testing:~
Approximately 8oo!o off.lmilymembers who are susceptible toMH have significantly elevated CPKlevels; a substantially higher correlation exists ifmyopathy is present. 14
Though not a specific indicatoT) CPKlevels (combined with patient histotyand muscle biopsy) may help toidentiJY MH-susceptible subject<. "
Haas et al described a proto-col for patient assessment thatprovides the clinician with anobjective framework to evaluatean MH-susceptible patient basedon medical history, diagnosis, andanticipated stress (see Table 2).'Modifiutions to treatme1lt can bemade according to degree ofsusceptibility. An important dementofthis protocol is an evaluationof the stress the patient is likely toexperience during the procedure. Ina survey of patients who had experienced MH-like reactions duringdental treatment, the presence ofstress before the reaction-eitherbecause ofanxiety or the procedurebeing performed-was a commontheme.6 Haas a at recommendedperforming any stressful treatmentin a f.lcility with an appropriateMH protocol in place.'
Cenual to resolving an MH crisisis dantrolene sodium, a musclerelaxant that effeetively blocks
the release of calcium from thesarcoplasmic reticulum.22 Discontinuing triggering agents, combinedwith cooling measures and theadministration of pure oxygen anddantrolene sodium can be effectivein resolving an MH crisis. Management of a susceptible patient mayinvolve the preoperative use of dantrolene. l9,20 Once MH is resolved,symptoms such as tachycardia, rigidity, acidosis, and hyperthermia mayreturn. Following a crisis, patientsneed to be monitored carefully inan intensive care setting, as 25%of cases have reported recrudescentMH within 48 hours of an episode.'
SummaryMH is an uncommon and potentially life-threatening pharmacogenetic disorder. Characterized by ahypercatabolic reaction in muscleinduced by cerrain drugs or byphysical or emotional stress, MHcan adversely affect the quality ofand access to dental care. Patientswith a history ofMH may bedenied treatment or receive carein an inappropriate setting. At thedental office, an MH-susceptible
patient exposed to excessive stresses(such as pain and fear) may exhibitsymptoms of MH. The dentist'sf.lmiliarity with the disease canenable MH-susceptible patients toreceive dental treatment in a safeand reasonable manner.
DisclaimerThe views expressed in this artide
do not reflect the views of theUnited States Army or any government agency thereofand are solelythe views of the authors.
Author informationCPT Reifensrahl is a resident in anAdvanced Education in GeneralDentistry program, Schofield Barracks, Hawaii. Dr. Rowshan is anassociate professor of the Oral andMaxillofacial Surgery and AdvancedEducation in General Surgerytwo-year programs at Tripier ArmyMedical Center, Hawaii.
References1. Eslambolchi S. Malignant hyperthermia: It5 im
portance with respect to dentistry. UTor Dent J1991;5(1):24-30.
2. Ma~med S. Handbook of lorai anesthesia, ed.4.It.lQuis: MQsby: 1997.
www.agd.org General Dentistry MaylJune 2009 245

SPECIAL PATIENT CARE Malignant hyperthermia in general dentistry
3. Haas DA. Young ER Harper DG. Malignant hyperthermia and the general dentist Current re<:·ommendatioo< J Can Denl Assoc 1992;5811):28·33.
4. Ali 5Z, Taguchi A Rosenberg H. Malignant hyperthermia. Best Pratt Res Clin Anaesthesiol2003;1714):519-533.
5. Slavkin HC, Benefit:5 and risks of medications:Challenges for the 21st century. j Am Dent Assoc 1997;128181:1157-116ll.
6. Minasian A. Yagiela JA The use of amide kKalanesthetics in patients susceptible to malignanthjp<rthermia. Ofal Surg Ofal Moo Or~ Path~
Oral RadiolI988;66(4):405-415.7. Noguchi I, Ohno H, Takana K, Shimada R, Sasaa
M, Shimonaka H. Fatal hyperthermia due todental treatment Oral Surg Oral Med OralPathol Oral Radiol Endod 2006;101(3):061-064.
8. Fukami Me. Ganzberg SI.A me report of martgnant hyperthermia in adental cnni( operatingroom.Anelth Prog 2005;52(1):24-28.
9. Inada H, Jinna S, Kohase H. Fukayama H, UminoM. Post"f)erativl! hyperthermia of unknownorigin treated with dantrolene sodium. Anesthfrog 2005;52(1):21-23.
10. Monaghan A. Hindle I. MaHgnilnt hyperpyrexiain oralsurgery--Case report and literature review. 8r j Oral Maxillofa, Su", 1994;32(3): 190193.
11, Waite PO, Ballard lB, YoofaA, Malignant hyper~
thermia in a patient receiving nitrous oxide. j
Oral Maxillofac 5urg 1985;43111):907-909.12. Choung R. Post-operative variant of malignant
hyperthermia: Report of il case, JOral MaxUlolac 5urg 1992;50(11):1235-1237.
13, Robertson GR. Malignant hyperthermia. JCanDentAs",c 1987;53111:33-35.
14, Carson JM, Van Sickels JE, Preoperative determi·nation of suscepnbility to malignant hyperthermia. j Oral Maxillofac Su", 1982;40(7):432·435.
15. Duncan GH, Moore P. Nitrous oxide and thedental patient Areview of adverse reactions. jAm DenlAssoc 1984;108(2):213-219.
16. Galanter·Mosielski MM, Hardie J, Canran C8,Malignant hyperthermia and the dental pratt\tione<. Jcan DenlAssoc 1987;53141:295-296.
17, Haas DA.An,update 00 local anesthetics in den·tistry. j Can Dent As\o' 2002;68(9):546-551.
18, D'Ambrosio l, Adragna MG. Guidelines for theuse of local anesthetics in the dental treatmentof patients who are susceptIble to malignanthyperthermia. Spec Care Dentist 1988;8(2):61·63.
t9, Adriani J, Sundin R. Malignant hyperthermia indental patients. j Am Dent""oc 1984;10812,180-184.
20. Warrington RD, Kocnansky CY, 8ach DE. Treat·ment of apatient susceptible to malignant hyperthermia. Clin Prev Dent 1986;8(1):27-29.
21. Testing for susceptibiflty to MH: Muscle contrac·tion or muscular genetics? Available at http://w.YW.mhaus.orglindex.cfmlfuseactionlOniineBrocnures.DisplayJ8TOchurePKI71 AIAFFC-18C7-4A36-970C6FD827999FE5.am, Accessed January 2009.
22. Cantin RY, Poole A. Ryan J1. Malignant hyperthermia. Oral Surg Oral Med Oral Patho11986;6214):389-392.
Published with permission by the Academy ofGeneral Dentistry.@Copyright 2009 by the Academyof General Dentistry. All righB reserved.
-------------------0-------------------
246 MaylJune 2009 General Dentistry www.agd.org











![Malignant hyperthermia [final]](https://img.pdfslide.us/doc/110x75/58ceb1b71a28abb2218b5123/malignant-hyperthermia-final.jpg)