Embed Size (px)
Citation preview

J Clin Pathol 1986;39:16-21
Malignant histiocytosis complicating rheumatoidarthritis: report of four cases
AS JACK, BF BOYCE, FD LEE
From the Department of Pathology, University of Glasgow, Glasgow Royal Infirmary, Glasgow
SUMMARY Four patients with rheumatoid arthritis developed a similar type of lymphoreticulartumour. The morphology and immunocytochemical findings suggested that this was a form ofmalignant histiocytosis: there may be an important correlation between this tumour and rheumatoidarthritis.
An association between lymphoreticular neoplasmsand diseases affecting the immune system has oftenbeen described. B cell lymphomas are found in associ-ation with Hashimoto's thyroiditis,' Sjogren's syn-drome,2 immunosuppression,3 and the acquiredimmune deficiency syndrome (AIDS).4 The occur-rence of malignant histiocytosis of the intestine inpatients with coeliac disease is now well recognised.5 6
In contrast, lymphoreticular tumours have not beenreported in rheumatoid arthritis or other related con-nective tissue disorders in which there is often evi-dence of lymphoid hyperplasia, autoantibody for-mation, and immune impairment. We describe fourcases in which a distinctive form of lymphoreticularneoplasm occurred in patients with rheumatoidarthritis.
Case reports
CLINICAL DETAILSCase I This patient, a 63 year old man, had beenreceiving treatment with non-steroidal anti-inflammatory drugs and gold for seropositive rheu-matoid arthritis for about two years before death.Gold treatment had induced a good symptomaticresponse. He was admitted to hospital shortly beforehis death with a history of fever and general malaiseof recent onset. Chest radiography, computed tomog-raphy, and abdominal ultrasonography suggested thepresence of disseminated tumour. A laparotomy wasperformed, which confirmed the presence of multipletumour nodules in the liver. The spleen had beenremoved because of accidental surgical trauma.Case 2 This patient, a 54 year old woman, was diag-nosed as having seropositive rheumatoid arthritis six
Accepted for publication 16 September 1985
months before death. She had a symmetrical erosivearthropathy with an erythrocyte sedimentation ratemeasured at 130 mm/hour. This had been treated withnon-steroidal anti-inflammatory drugs. She wasadmitted to hospital with rapidly progressive renalfailure and died shortly after. A diffuse infiltrate hadbeen noted on the chest x-rayCase 3 This patient, a 56 year old woman, had nod-ular seropositive rheumatoid arthritis that hadresulted in a flexion deformity of both knees. This hadbeen present for more than five years. She had beentreated with non-steroidal anti-inflammatory drugs.She was admitted to hospital with severe joint pain,jaundice, and vomiting. On examination she wasshocked and hypoxic. She died a few hours later.Case 4 This patient, a 77 year old woman, wasknown to have had seropositive rheumatoid arthritisfor more than five years, resulting in a moderatedegree of joint deformity. She had received treatmentwith gold and penicillamine. She was admitted to hos-pital complaining of upper abdominal pain which hadstarted during the previous few days. Cholecystitiswas diagnosed and a laparotomy was performed. Thegall bladder was thickened and- adherent, and the liverhad a finely mottled appearance. Cholecystectomyand liver biopsy were performed. She was alive threemonths later.Postmortem examinations were performed on cases
1-3. The gall bladder and liver were examined incase 4.
IMMUNOCYTOCHEMICAL STUDIESAll cases were studied using standard indirect immu-noperoxidase methods with the following antibodies:antileucocyte common antigen (Dako Ltd), anti-alpha-l-antitrypsin (Dako Ltd), anti-alpha-l-anti-chymotrypsin (Dako Ltd), antimuramidase (DakoLtd), anti-leu-Ml (Becton-Dickinson), anti-S100
16
on March 24, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.1.16 on 1 January 1986. Dow
nloaded from
Malignant histiocytosis complicating rheumatoid arthritis
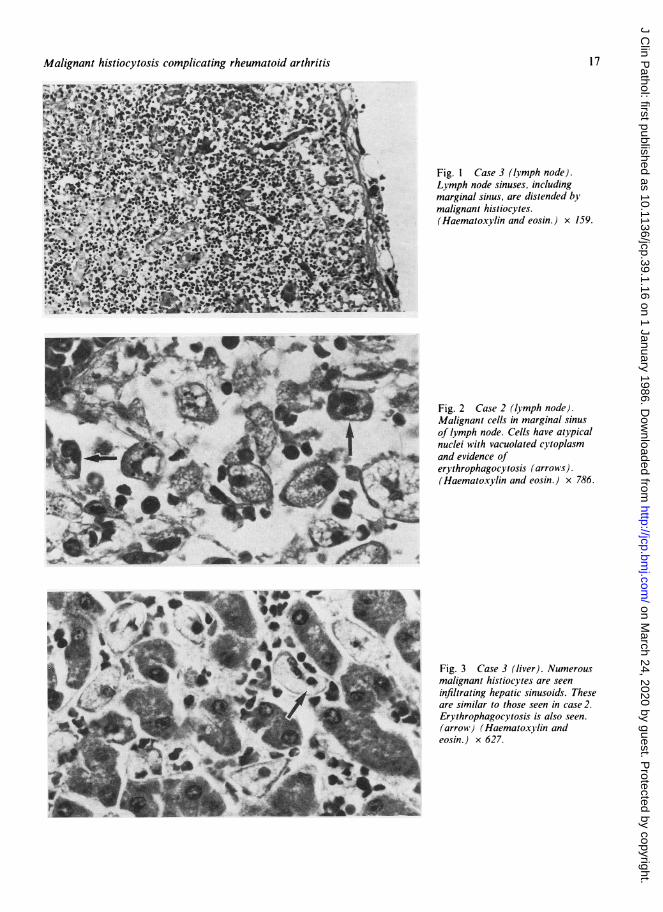
Fig. I Case 3 (lymph node).Lymph node sinuses, includingmarginal sinus, are distended bymalignant histiocytes.(Haematoxylin and eosin.) x 159.
Fig. 2 Case 2 (lymph node).Malignant cells in marginal sinusof lymph node. Cells have atypicalnuclei with vacuolated cytoplasmand evidence oferythrophagocytosis (arrows).(Haematoxylin and eosin.) x 786.
Fig. 3 Case 3 (liver). Numerousmalignant histiocytes are seeninfiltrating hepatic sinusoids. Theseare similar to those seen in case 2.Erythrophagocytosis is also seen.(arrow) (Haematoxprlin andeosin.) x 627.
17
on March 24, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.1.16 on 1 January 1986. Dow
nloaded from
Jack, Boyce, Lee
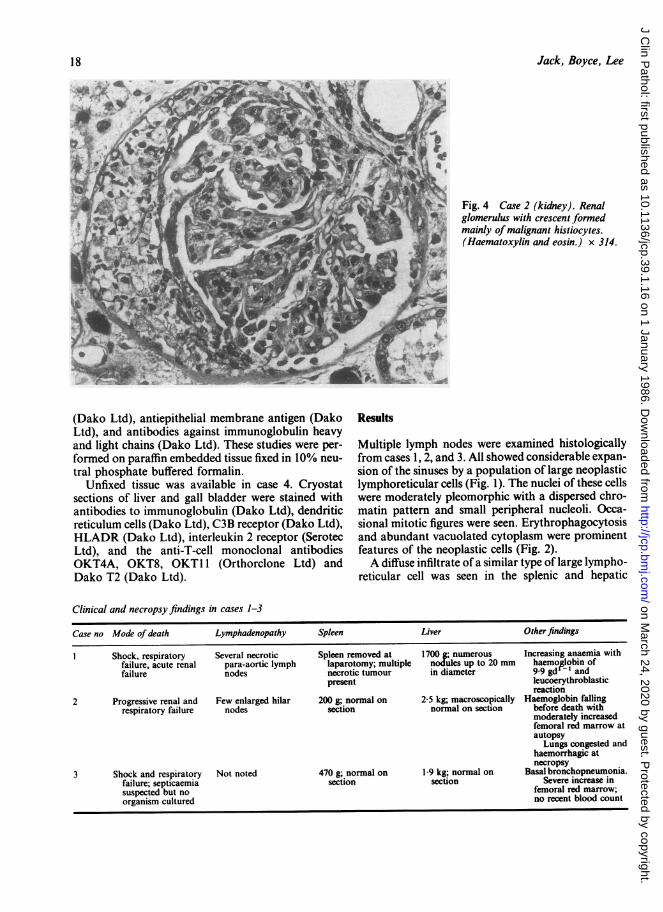
Fig. 4 Case 2 (kidney). Renalglomerulus with crescent formedmainly of malignant histiocytes.(Haematoxylin and eosin.) x 314.
(Dako Ltd), antiepithelial membrane antigen (DakoLtd), and antibodies against immunoglobulin heavyand light chains (Dako Ltd). These studies were per-
formed on paraffin embedded tissue fixed in 10% neu-
tral phosphate buffered formalin.Unfixed tissue was available in case 4. Cryostat
sections of liver and gall bladder were stained withantibodies to immunoglobulin (Dako Ltd), dendriticreticulum cells (Dako Ltd), C3B receptor (Dako Ltd),HLADR (Dako Ltd), interleukin 2 receptor (SerotecLtd), and the anti-T-cell monoclonal antibodiesOKT4A, OKT8, OKT1 1 (Orthorclone Ltd) andDako T2 (Dako Ltd).
Results
Multiple lymph nodes were examined histologicallyfrom cases 1, 2, and 3. All showed considerable expan-sion of the sinuses by a population of large neoplasticlymphoreticular cells (Fig. 1). The nuclei of these cellswere moderately pleomorphic with a dispersed chro-matin pattern and small peripheral nucleoli. Occa-sional mitotic figures were seen. Erythrophagocytosisand abundant vacuolated cytoplasm were prominentfeatures of the neoplastic cells (Fig. 2).A diffuse infiltrate of a similar type of large lympho-
reticular cell was seen in the splenic and hepatic
Clinical and necropsy findings in cases 1-3
Case no Mode of death Lymphadenopathy Spleen Liver Other findings
I Shock, respiratory Several necrotic Spleen removed at 1700 g; numerous Increasing anaemia withfailure, acute renal para-aortic lymph laparotomy; multiple nodules up to 20 mm haemollobin offailure nodes necrotic tumour in diameter 9.9 gd' and
present leucoerythroblasticreaction
2 Progressive renal and Few enlarged hilar 200 g; normal on 2-5 kg; macroscopically Haemoglobin fallingrespiratory failure nodes section normal on section before death with
moderately increasedfemoral red marrow atautopsy
Lungs congested andhaemorrhagic atnecropsy
3 Shock and respiratory Not noted 470 g; normal on 1 9 kg; normal on Basal bronchopneumonia.failure; septicaemia section section Severe increase insuspected but no femoral red marrow;organism cultured no recent blood count
18
on March 24, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.1.16 on 1 January 1986. Dow
nloaded from
Malignant histiocytosis complicating rheumatoid arthritis
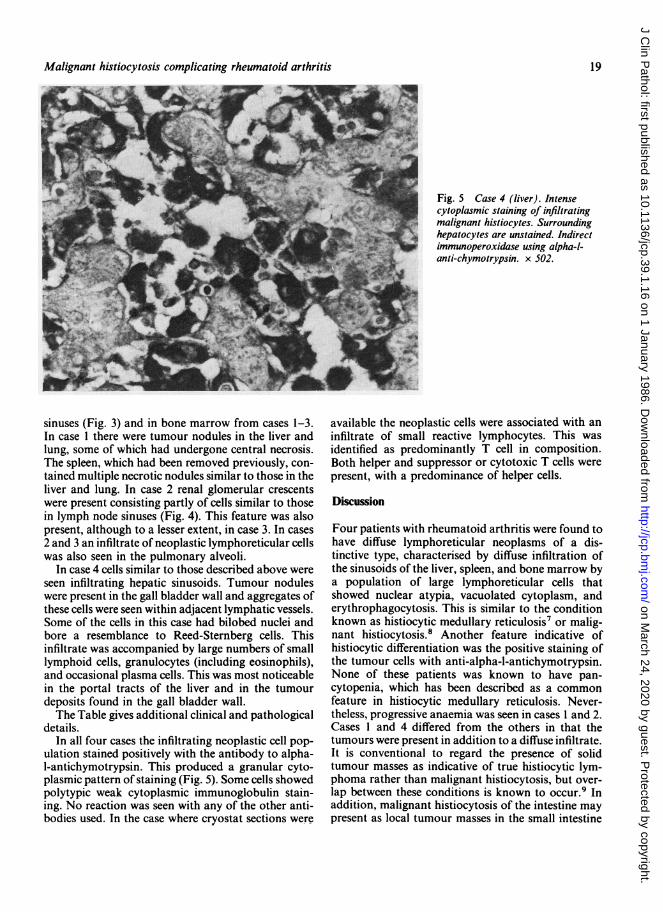
Fig. 5 Case 4 (liver). Intensecytoplasmic staining of infiltratingmalignant histiocytes. Surroundinghepatocytes are unstained. Indirectimmunoperoxidase using alpha-l-anti-chymotrypsin. x 502.
sinuses (Fig. 3) and in bone marrow from cases 1-3.In case I there were tumour nodules in the liver andlung, some of which had undergone central necrosis.The spleen, which had been removed previously, con-tained multiple necrotic nodules similar to those in theliver and lung. In case 2 renal glomerular crescentswere present consisting partly of cells similar to thosein lymph node sinuses (Fig. 4). This feature was alsopresent, although to a lesser extent, in case 3. In cases2 and 3 an infiltrate of neoplastic lymphoreticular cellswas also seen in the pulmonary alveoli.
In case 4 cells similar to those described above wereseen infiltrating hepatic sinusoids. Tumour noduleswere present in the gall bladder wall and aggregates ofthese cells were seen within adjacent lymphatic vessels.Some of the cells in this case had bilobed nuclei andbore a resemblance to Reed-Sternberg cells. Thisinfiltrate was accompanied by large numbers of smalllymphoid cells, granulocytes (including eosinophils),and occasional plasma cells. This was most noticeablein the portal tracts of the liver and in the tumourdeposits found in the gall bladder wall.The Table gives additional clinical and pathological
details.In all four cases the infiltrating neoplastic cell pop-
ulation stained positively with the antibody to alpha-I-antichymotrypsin. This produced a granular cyto-plasmic pattern of staining (Fig. 5). Some cells showedpolytypic weak cytoplasmic immunoglobulin stain-ing. No reaction was seen with any of the other anti-bodies used. In the case where cryostat sections were
available the neoplastic cells were associated with aninfiltrate of small reactive lymphocytes. This wasidentified as predominantly T cell in composition.Both helper and suppressor or cytotoxic T cells werepresent, with a predominance of helper cells.
Discussion
Four patients with rheumatoid arthritis were found tohave diffuse lymphoreticular neoplasms of a dis-tinctive type, characterised by diffuse infiltration ofthe sinusoids of the liver, spleen, and bone marrow bya population of large lymphoreticular cells thatshowed nuclear atypia, vacuolated cytoplasm, anderythrophagocytosis. This is similar to the conditionknown as histiocytic medullary reticulosis7 or malig-nant histiocytosis.8 Another feature indicative ofhistiocytic differentiation was the positive staining ofthe tumour cells with anti-alpha-l-antichymotrypsin.None of these patients was known to have pan-cytopenia, which has been described as a commonfeature in histiocytic medullary reticulosis. Never-theless, progressive anaemia was seen in cases I and 2.Cases I and 4 differed from the others in that thetumours were present in addition to a diffuse infiltrate.It is conventional to regard the presence of solidtumour masses as indicative of true histiocytic lym-phoma rather than malignant histiocytosis, but over-lap between these conditions is known to occur.9 Inaddition, malignant histiocytosis of the intestine maypresent as local tumour masses in the small intestine
19
-!l'.r
on March 24, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.1.16 on 1 January 1986. Dow
nloaded from
20
but may infiltrate diffusely in other organs.5 6Identifying histiocytic tumours has been a contro-
versial matter for many years. This has-been partlydue to the use of the term histiocytic by the Rappaportclassification for tumours of B or T cell.'0 The inci-dence of histiocytic tumours has been variouslyquoted as less than I% " or 1015%. 2 13 The causeof this discrepancy is related to the importanceattached to alpha-l-antitrypsin staining as a reliablemarker of histiocyte differentiation and the use of theHodgkin's disease related monoclonal antibodies,Ki-l and Leu Ml." The difficulties have beenexacerbated by a recent report on monotypic surfaceimmunoglobulin staining in malignant histiocytosis ofthe intestine using the immuno-gold-silver method.'4In the cases described above the term malignanthistiocytosis is a useful description, but clearly somedoubt must remain as to the true histogenesis of theselesions.Two other differential diagnoses should be consid-
ered in these cases. A benign virus induced histiocyticproliferation with erythrophagocytosis has beendescribed. This is associated with a high mortality.'5The cases we described were differentiated from thiscondition by the presence of conspicuous nuclearatypia and by tumour formation in cases I and 4. Thesecond possible differential diagnosis is the hae-mophagocytic T cell lymphoma or leukaemia,described by Kadin.'6 None of the cases describedwas leukaemic, but a T cell origin of the lesion cannotbe excluded in the absence of appropriate markers inthree cases. It has been proposed that malignanthistiocytosis and haemophagocytic T cell lymphomaare closely related, with several patients beingdescribed who have features of both conditions.'7The cases were collected over four years during
which time only one other case of malignanthistiocytosis was diagnosed in this department,excluding coeliac related malignant histiocytosis ofthe intestine. This points to a true rather than a fortu-itous correlation with rheumatoid arthritis. The manand three women described reflect the sex preferenceof rheumatoid arthritis; the age range, however(54-77 years) is older than the usual age of onset ofrheumatoid arthritis, the third to fourth decade. Twoof the patients had relatively short histories of jointdisease, but the other patients had been receivingtreatment for over five years. There seems to be noconsistency between patients as regards treatmentother than non-steroidal anti-inflammatory drugs. Allfour patients presented with an acute illness, followedin cases 1-3 with rapid deterioration and death. Onepatient (case 4) is alive three months afterpresentation and is being treated with chemotherapy.An interesting feature ofcase 2 was the presentation
with renal failure and the subsequent finding of glo-
Jack, Boyce, Lee
merular crescents partly composed of neoplastic cells.This has been previously reported in malignanthistiocytosis"8 and is consistent with the presence ofnormal histiocytes in Bowman's capsule.'9
It would be interesting to know if similar cases havebeen recognised elsewhere, so that the incidence ofmalignant histiocytosis as a complication of rheu-matoid arthritis could be assessed. If tissue were tobecome available from other cases it may be possible,using immunocytochemical markers and gene rear-rangement studies, to further characterise the cellspresent in these tumours. Such studies could elucidatefurther what seems to be a link between the immu-nological abnormalities of rheumatoid arthritis andthe development of lymphoreticular tumours. Thisassociation is also interesting in view of the rheu-matoid induced proliferation of the mononuclearphagocyte component of the synovial"lining,20 whichoccurs in affected joints.
We thank Dr R Madhok, department of medicine,Glasgow Royal Infirmary, for helpful discussions. Weare grateful to Mrs I Main for typing the manuscriptand Mr T Parker for preparing the illustrations. ASJis supported by the Wellcome Trust.
References
l Anscombe AM, Wright DH. Primary malignant lymphomas of thethyroid-a tumour ofmucosa associated lymphoid tissue: reviewof seventy-six cases. Histopathology 1985;9:81-97.
2Zulman J, Jaffe R, Talal N. Evidence that the malignant lymphomaof Sjogren's syndrome is a monoclonal B-cell neoplasm. NewEngl J Med 1978;299:1215-20.
'Cleary ML, Sklar J. Lymphoproliferative disorders in cardiactransplantation recipients are multiclonal lymphomas. Lancet1984;ii:489-93.
'Reichert CM, O'Leary TJ, Levens DL, Simrell CR, Macher AM.Autopsy pathology in the acquired immune deficiency syn-drome. Am J Pathol 1983;112:357-82.
-'Isaacson P, Wright DH. Intestinal lymphoma associated with mal-absorption. Lancet 1978;i:67-70.
6Isaacson P, Wright DH. Malignant histocytosis of the intestine. Itsrelationship to malabsorption and ulcerative jejunitis. HumPathol 1978;9:661-77.
'Scott RB, Robb-Smith AHT. Histiocytic medullary reticulosis.Lancet 1939;ii: 194-8.
8Rappaport H. Tumours of the hematopoietic system. Atlas oftumour pathology. Washington DC: Armed Forces Institute ofPathology, 1966:36-43.
9Warnke RA, Kim H, Dorfman RF. Malignant histiocytosis(histiocytic medullary reticulosis). I. Clinico-pathologic study of29 cases. Cancer 1975;35:215-30.
'0Nathwani BN. A critical analysis of classifications of non-Hodgkin's lymphoma. Cancer 1979;44:347-8.
l Stein H, Lennert K, Feller AC, Masson DY. Immunohistologicalanalysis of human lymphoma: correlation of histological andimmunological categories. Adv Cancer Res 1985;42:67-143.
"Van der Valk P, Meijer CJLM, Willemze R, Van Oosterom AT,Spaander PJ, TeVelde J. Histiocytic sarcoma (true histiocyticlymphoma) a clinicopathological study of 20 cases. Histo-pathology 1984;8:105-23.
on March 24, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.1.16 on 1 January 1986. Dow
nloaded from

Malignant histiocytosis complicating rheumatoid arthritis
3 Van der Valk P, Herman J, Brand R, Cornelisse CJ, Spaander PJ,Meijer CJLM. Morphometric characterisation of diffuse largecell (histiocytic) lymphomas. Am J Pathol 1982;107:327-55.
'4Morgan DR, Holgate CS, Dixon MF, Bird CC. Classification ofsmall bowel lymphoma by immunogold silver technique:relationship with coeliac disease. J Paihol 1985;146:241A.
s Risdall RJ, McKenna RW, Nesbit ME, et al. Virus associatedhaemophagocytic syndrome: a benign histiocytic proliferationdistinct from malignant histiocytosis. Cancer 1979;44:993-1002.
16Kadin ME, Kamoun M, Lamberg J. Erythrophagocytic T-gammalymphoma. A clinicopathologic entity resembling malignanthistiocytosis. N Engi J Med 1981;304:648-9.
'"Kadin ME. T-gamma cells: a missing link between malignanthistiocytosis and T-cell leukaemia-lymphoma? Hum Pathol198 1;12:771-2.
18Aozasa K, Tsujimoto M, Inoue A. Malignant histiocytosis. Reportof twenty five cases with pulmonary, renal and/or gastro-intestinal involvement. Histopathology 1985;9:39-49.
Thomson WM, Holdworth SR, Glasgow EF, Atkin RC. The mac-rophage in the development of experimental crescentic glomeru-lonephritis. Studies using tissue culture and electron microscopy.Am J Pathol 1979;94:223-40.
20Ghadially FN. The articular territory of the reticuloendothelialsystem. Ultrastruct Pathol 1980;1:249-58.
Requests for reprints to: Dr AS Jack, Department of Pathol-ogy, Royal Infirmary, Glasgow G40SF, Scotland.
21
on March 24, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.1.16 on 1 January 1986. Dow
nloaded from









